Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 16
Platelet-Rich Fibrin (PRF) Analyzed for Cytokine Profiles - A Misguided Hope for Osteogenesis in Jawbone Defects? Research and Clinical Observational Study
Authors Lechner J ![]() , vonBaehr V, Doebis C, Notter F, Schick F
, vonBaehr V, Doebis C, Notter F, Schick F ![]()
Received 4 September 2024
Accepted for publication 15 November 2024
Published 19 November 2024 Volume 2024:16 Pages 467—479
DOI https://doi.org/10.2147/CCIDE.S488206
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Johann Lechner,1 Volker vonBaehr,2 Cornelia Doebis,3 Florian Notter,4 Fabian Schick4
1Department of Osteoimmunology, Clinic for Integrative Dentistry, Munich, Germany; 2Department of Immunology and Allergology, Institute for Medical Diagnostics, Berlin, Germany; 3Department of Analysis, Institute for Medical Diagnostics, Berlin, Germany; 4Department of Implantology, Clinic for Integrative Dentistry, Munich, Germany
Correspondence: Johann Lechner, Department of Osteoimmunology, Clinic for Integrative Dentistry, Gruenwalder Str. 10A, Munich, 81547, Germany, Tel +49 89 697 0129, Fax +49 89 692 5830, Email [email protected]
Background: Platelet-rich fibrin (PRF) blood concentrates are used in oral implantology and defect surgery to promote osteoneogenesis in Bone Marrow Defects in Jawbone (BMDJ), according to the morphology of fatty-degenerative osteonecrosis also called FDOJ.
Question: Can the benefit of PRF on alveolar osteoneogenesis be confirmed by cytokine analysis?.
Methods: The cytokine expressions of the PRF samples in 26 patients undergoing BMDJ/FDOJ surgery in the same session were analysed for seven cytokines (RANTES/CCL5; FGF-2; IL-1RA; Il-6; IL-8; MCP-1; TNF-a) by multiplex (Luminex). The FDOJ samples of these 26 BMDJ/FDOJ patients were analysed for the RANTES/CCL5 expression only.
Results: Cytokine expression in PRF is compared to reference values for healthy medullary bone of the jaw and BMDJ/FDOJ and shows that the cytokine expressions of the PRF samples do not compensate or counteract prima vista for the cytokine dysregulations present in the BMDJ/FDOJ areas.
Discussion: To define the aid of cytokines studied in PRF in the restoration of the immunological dysregulation in areas of BMDJ/FDOJ, literature is reviewed comparing RANTES/CCL5, IL-1ra, TNF-α and MCP-1/CCL2 expression in PRF and BMDJ/FDOJ. Immunoregulatory properties of PRF in alveolar bone restoration are evaluated.
Summary: PRF was mistakenly thought to be a cure for bone healing, which is here shown to be incorrect. Enoral Ultrasound Sonography of bone density is available for the clinical measurement of individually developed osteoneogenesis by PRF.
Conclusion: The multiplex analysis of PRF shows a dynamic and cytokine-based interaction with osteoneogenesis that is not yet fully clarified.
Keywords: platelet-rich fibrin, multiplex analysis, cytokines, bone marrow defects of the jaw, osteoneogenesis, enoral transalveolar ultrasonograph
Graphical Abstract:

Introduction
Osteoimmunology of Wound Healing
Bone regeneration is an important pillar of wound healing in oral surgery and implantology procedures in dentistry. The tissues involved in wound healing may be regarded as an immunologically active microenvironment whose immunological parameters are primarily modulated by macrophages and T cells. An initial immune-mediated and controlled inflammatory response is essential.1 The relationship between inflammation, the immune system and bone has led to a new field that may be termed “maxillo-mandibular osteoimmunology”2 and encompasses the science related to osteoclast development and osteoneogenesis in the jawbone.3 Alveolar macrophages also play a special role during the early stages of the osseointegration of implants.4 In the case of immune and inflammatory reactions to biomaterials, “inflammation” is associated with an undesirable defence. At the same time, however, inflammatory reactions are necessary initial processes in the regulation of wound healing and osteoneogenesis. The primary phase of inflammation is therefore of critical importance to a successful osteoimmunological dynamic.5 However, an osteo-immune dysbalance may result not only from local and systemic oxidative stress,6,7 but also from undesirable immune responses that are connected to the failure of wound healing in implantology.8
Blood Concentrates in Osteoimmunology
Blood concentrates are increasingly being used in oral surgery as autologous products to support wound healing and bone regeneration. These concentrates are prepared by centrifugation of the patient’s own peripheral blood.9 To date, there has been research into the composition of cells and growth factors found in these blood-derived products and scientific explanations of their respective bioactivity. The platelet-rich fibrin (PRF) procedure is considered to be an entirely autologous system. PRF is the body’s own fibrin-rich matrix, which is an important component of blood and is obtained by centrifuging the patient’s own blood.10 The protein fibrin serves as a natural protective barrier against germs and contributes to blood clotting. When closing wounds, fibrin acts as a kind of natural adhesive. The matrix also contains a particularly large number of white blood cells which store information for tissue regeneration.11 In addition, PRF contains platelets, whose growth factors promote wound healing.12 It has been shown that the bioactivity and composition of blood concentrates depend directly on the centrifugal force applied. By reducing the centrifugal force, both leukocytes and thrombocytes are concentrated in the PRF matrix, thereby increasing the bioactivity of PRF. Leukocytes and their subgroups play an important role in initial wound healing and can therefore accelerate and support regeneration.13,14 The innovative concept for improved wound healing by the application of PRF was developed in 2001 by Dr Joseph Choukroun and his colleagues15 and has become established in the daily practice of oral surgery and implantology based on evidence-based practice.16 Previous research on PRF has mainly focussed on tissue regeneration via M1/M2 macrophage activity.
Bone Marrow Defects and Fatty-Degenerative Osteonecrosis of the Jawbone
The death of local bone marrow cells due to chronic stimulation resulting from unfavourable factors such as inflammation of the jawbone may lead to chronic osteoimmune dysregulation. In previous publications, we defined this chronic inflammatory process in bone marrow defects of the jaw (BMDJ) as fatty-degenerative osteonecrosis of the jaw (FDOJ) that is associated with chronic overexpression of the proinflammatory cytokine RANTES/CCL5 (R/C).17–19 BMDJ/FDOJ is also primarily defined in the literature as “bone marrow edema” or silent or subclinical inflammation, without the typical signs of acute inflammation.20,21 Figure 1 shows one of the tissue samples obtained during a surgical procedure to excise a bone marrow defect of the jaw.19 We also further investigated 128 additional BMDJ/FDOJ samples to measure the levels of various cytokines using a cytokine panel consisting of FGF-2, IL-1ra, IL-8, IL-6, IL-10, MCP-1, TNF-α and R/C (Figure 1).18 It is clinically remarkable that, with the exception of cases of atypical facial pain and trigeminal neuralgia, BMDJ/FDOJ does not elicit pain in most patients. The absence of a painful inflammatory response may be explained by the decreased expression of TNF-α and IL-6 in BMDJ/FDOJ, with TNF-α expression reduced by one-third and IL-6 expression reduced by one-tenth compared to the expression levels of 19 samples of healthy bone marrow. Thus, the levels of these acute inflammatory mediators are insufficient to drive acute and painful inflammation for proper wound healing in most cases of BMDJ/FDOJ.19 Graphical statistics of Figure 1 in Figure 2 show the the mean value of the respective cytokine in 128 BMDJ/FDOJ samples (MV FDOJ, n = 128) and the mean value of each cytokine in 19 healthy jaw bone samples (Norm = 19) including the standard deviation (StDEv±).19
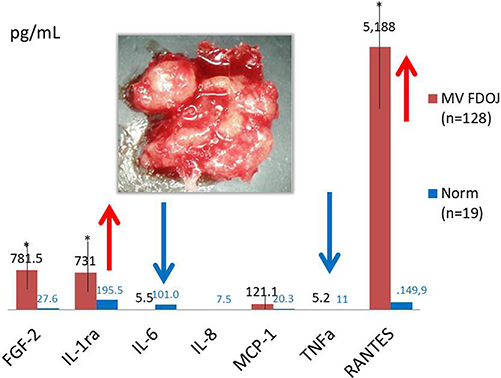 |
Figure 1 Legend: Columns in red (MV) show the mean value of the respective cytokine in 128 BMDJ/FDOJ samples; columns in blue (Norm) show the mean value of each cytokine in 19 healthy jaw bone samples. The distribution of the multiplex analyses of 128 BMDJ/FDOJ samples shows marked singular overexpression of R/C, mild overexpression of IL-1ra (red arrows) and highly downregulated TNF-α and IL-6 expression (blue arrows). (*) Indicate medium values of cytokine expressions in BMDJ/FDOJ samples. The inset image shows one of the characteristic samples of fatty-degenerative osteonecrosis of the jaw (FDOJ) which was evaluated using a cytokine panel analysis.19 |
 |
Figure 2 Graphical statistics of. Figure 1: MV FDOJ = 128 show the mean value of the respective cytokine in 128 BMDJ/FDOJ samples; Norm = 19 show the mean value of each cytokine in 19 healthy jaw bone samples.19 |
The Aim of the Application of PRF in Osteoimmunology
Ideally, the aim of the application of PRF in osteoimmunology following the excision of BMDJ/FDOJ is to compensate for the dysregulated cytokine patterns that are characteristic of this condition in order to induce optimal wound healing and neogenesis in jawbone. Wound healing in bone begins with an inflammatory response which is usually the response of vascularized living tissue to trauma.22 The consistent lack of proinflammatory cytokines found in samples of fatty-degenerative BMDJ indicates failed wound healing.18,19 This is so since inflammation is considered to be a useful mechanism in the early days of bone healing. When the inflammatory process is prolonged, however, the beneficial effect is reversed and the process becomes detrimental.23 In jawbone samples that were previously investigated, the downregulation of angiogenic cytokines resulted in the absence of angiogenesis, finally resulting in ischemia and hypoxia in the BMDJ/FDOJ areas concerned.24,25 In contrast there has been very limited research into the osteoimmunological effects of PRF application in surgery of the jaw. In addition to macrophages, CD4+ T helper cells with cell-specific secreted cytokines play a key role in the osteoimmunology of bone regeneration. To clarify the cytokine release in PRF blood concentrate, we investigated this in patients’ individual PRF centrifugate.
Objectives
To wheather serve the cytokine levels present in PRF samples to compensate for the pathological expression patterns of BMDJ/FDOJ? Does the PRF cytokine concentration measured provide the expected positive osteoimmunological regeneration stimulus at the surgical site in comparison with BMDJ/FDOJ cytokine concentration?
Hitherto no cytokine analysis of PRF in comparison to cytokine expression in BMDJ/FDOJ has been published. We try to enlighten this in this paper (see graphical abstract).
Materials and Method
Preparation of PRF Samples
For each of the 26 patients, 10mL of venous blood was drawn from a peripheral vein into PRF blood tubes via a butterfly needle (Figure 3). Centrifugation was performed using a PRF Duo Centrifuge (Mectron) according to the instructions. In this study, the low-speed centrifugation concept (LSCC) was used to precisely determine the PRF composition (UPM = 1300; RCF = 208g; 8 min).
 |
Figure 3 From left to right: PRF clot frozen transport to laboratory for Multiplex analysis (Luminex) for a seven cytokine panel (RANTES/CCL5, FGF-2, IL1-RA, Il-6, IL-8, MCP-1, and TNF-α: See Figure 2). |
Following this, the PRF clot was taken in a standardised manner immediately after phase separation from the yellow PRF layer, directly adjacent to the phase transition.15,26 On collection, pea-sized lumps of PRF samples samples were immediately placed in a sterile collection vessel (Sarstedt Micro-Tube Ref. 72.692.005) and hermetically sealed. Each sample was stored at –20°C until transported individually to the laboratory for Multiplex analysis (Luminex) for a seven cytokine panel (RANTES/CCL5, FGF-2, IL1-RA, Il-6, IL-8, MCP-1, and TNF-α. (See Figure 3).
Preparation and Laboratory Analyses of PRF and BMDJ/FDOJ Samples
Pea-sized lumps of PRF samples from each of the 26 participants were sent frozen from our clinic, as well as corresponding samples of BMDJ/FDOJ from same patients to a laboratory (IMD-Berlin*) for analysis using a cytokine panel of FGF-2, IL1-RA, IL-6, IL-8, MCP-1, TNF-α, RANTES (R/C). On collection, PRF and BMDJ/FDOJ samples were immediately placed in a sterile collection vessel (Sarstedt Micro-Tube Ref. 72.692.005) and hermetically sealed. Each sample was stored at –20°C until transported individually to the laboratory where the tissue material was mechanically processed in 200 µL of protease buffer (Complete Mini Protease Inhibitor Cocktail, Roche, D) and homogenized. The homogenate was centrifuged for 15 minutes at 13,400 rpm and the supernatant was then removed and centrifuged for an additional 25 minutes at 13,400 rpm. The quantification of R/C was determined in the supernatant of the tissue homogenate using the Human Cytokine/Chemokine Panel I (HCYTOMAG-60K, Merck KGaA, Darmstadt, D) according to the manufacturer’s protocol and using Luminex 200TM with xPonent© software (Luminex, Austin, TX, USA).
Patient Cohort
The clinical samples of BMDJ/FDOJ obtained in this study were provided by 26 patients who underwent surgical treatment at the authors’ clinic. All of the participants in this study had chronic immune diseases and were referred to the authors’ clinic following appropriate specialist diagnoses. These patients sought to resolve chronic inflammatory bone defects of the jaw by restoring these immunologically altered BMDJ/FDOJ areas. The elimination and resolution of the chronic inflammatory cascades occurring in these regions was also associated with the prospect of reversing the patients’ systemic immune imbalance and associated symptom relief.27 The potential links between BMDJ/FDOJ and R/C-driven immune diseases, particularly those associated with the singular overexpression of R/C, have been presented in previous studies.2,17–19,19
All patients gave written informed consent (as described in the PLOS informed consent form) to participate in this study and for publication of the results. All patient data were de-identified. Each patient expressed an interest in determining whether chronic inflammation in the jawbone was present and, if so, associated with a diagnosis of chronic immune dysfunction or systemic disease. All investigations of the samples obtained from human participants in this study were performed and approved by the forensically accredited Institute for Medical Diagnostics, Nikolaistr. 22, D-12247 Berlin (IMD-Berlin). The approval decision was reached independently of Dr. Volker vonBaehr by IMD Berlin, in accordance with DIN EN 15198/DIN EN 17025 and in compliance with the Declaration of Helsinki of 1975 as amended in 2013 or comparable ethical standards. Figure 4 shows a tissue sample obtained in the course of a surgical procedure to remove a bone marrow defect of the jaw (BMDJ). In previous publications, we described the pathological morphology alteration of such areas.18,19
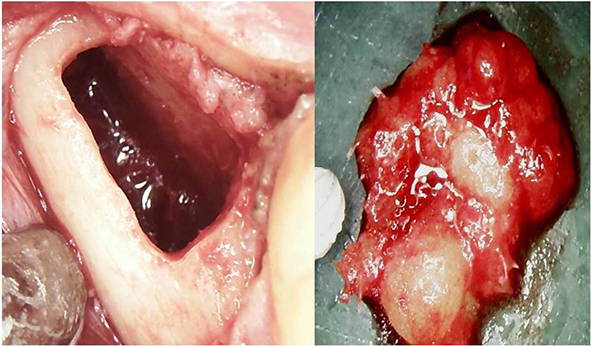 |
Figure 4 Areas of BMDJ/FDOJ. The left panel shows a hollow cavity in areas 38–39 after curettage of a softened, spongy bone marrow defect of the jaw (BMDJ). The right panel shows a clump of tissue displaying fatty degeneration of bone marrow (FDOJ) with the typical yellowish coloring characteristic of this fatty transformation. |
Results
Cytokines in PRF
For comparison with the available cytokine profiles for samples of BMDJ/FDOJ, the laboratory (IMD-Berlin*) assessed the PRF samples from the patient cohort provided with a cytokine panel including RANTES/CCL5, FGF-2, IL1-RA, Il-6, IL-8, MCP-1, and TNF-α (Figure 5).
 |
Figure 5 Distribution of cytokine expression of PRF samples from 26 patients as determined by multiplex analysis of the following cytokines in pg/mL: R/C, FGF-2, IL1-RA, IL-6, IL-8, MCP-1 and TNF-α. |
RANTES/CCL5 in PRF (n = 26) and in BMDJ/FDOJ (n = 26)
Portions of PRF samples were collected from the same 26 patients after preoperative blood sampling, and immediately sent frozen for laboratory analysis. Afterwards, the corresponding patient`s BMDJ/FDOJ area was opened intraoperatively and the BMDJ/FDOJ sample was also sent frozen for laboratory analysis. Figure 6 shows the results of R/C expression for the 26 PRF samples from Figure 5 on the left and the R/C expression from 26 BMDJ/FDOJ samples on the right.
 |
Figure 6 Graphical statistics to Figure 5: Left picture: Results of RANTES/CCL5 expression in 26 PRF samples (MV = 9.212,19 pg/mL; StDev = ±7.352,03 pg/mL). Right picture: Results of RANTES/CCL5 expression in 26 BMDJ/FDOJ samples of same patients as PRF (MV = 2.766,88 pg/mL; StDev = ±3.399,78 pg/mL). |
Statistical Analysis
The quantitative data of the new research were analyzed using descriptive statistics, which was calculated using IBM SPSS, version 19 (IBM Corporation, Armonk, NY, USA). The median, the arithmetic mean value, and data distribution were calculated. Differences between cohorts were computed with Student’s t-test or Spearman’s rho. The two-sided unpaired t-test was used to determine differences within groups, whereas Spearman’s coefficient was used to analyze correlations among the results of the cytokine profile analyses. The significance level was set at P<0.05.
Discussion
The increasing prevalence of the application of PRF in oral surgery attests to the obvious benefits of this technique for tissue regeneration. The results of this study therefore challenge us to reconsider the clinical evidence with the conflicting laboratory data.
Cytokines in BMDJ/FDOJ
As shown in Bone Marrow Defects and Fatty-Degenerative Osteonecrosis of the Jawbone BMDJ/FDOJ areas show an absence of the classic markers of inflammation and their significantly reduced expression in the cytokine pattern (see Figure 1). On average, TNF-α is downregulated to one-third, and IL-6 to one-tenth, of the levels found in healthy cancellous bone. This feature of BMDJ/FDOJ18 impedes an appropriate inflammatory defense response. At the same time, the lack of acute medullary tissue reaction may lead to the cryptic symptomatology that is often characteristic of BMDJ/FDOJ, namely the failure to elicit a pain response in most patients. The reduced expression of TNF-α and IL-6, however, contrasts with the singular overexpression of the proinflammatory chemokine R/C that is found in BMDJ/FDOJ.
Comparison of Cytokines in PRF to Reference Values for Healthy Medullary Bone of the Jaw and BMDJ/FDOJ
The hypothetical mechanism of the postoperative application of PRF blood concentrate is to aid in the restoration of the immunological dysbalance in areas of BMDJ/FDOJ. One way in which this may occur is that the pattern of PRF cytokine expression counteracts the effects of both the up- and down-regulated cytokines found in BMDJ/FDOJ and thus leads to the immunological revision of the inflammatory dysregulation in the jawbone defects (see Figure 1). Ideally, this would lead to optimal wound healing in osteoimmunological and osseointegrative procedures. Figure 7 compares the cytokine analyses of PRF samples (blue columns) with previously collected data from 128 BMDJ/FDOJ samples, where we added the new R/C of 26 actually debrided BMDJ/FDOJ samples (red columns) and 19 samples of healthy medullary bone of the jaw (green columns).17–19
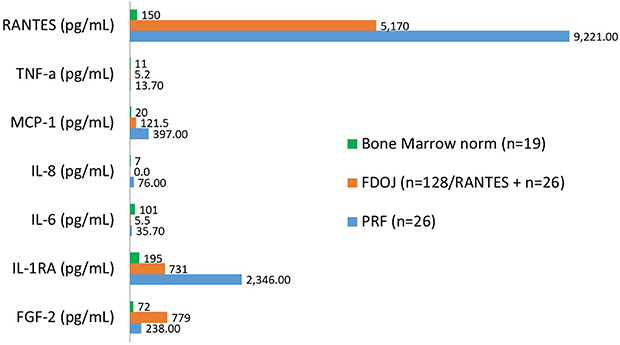 |
Figure 7 Comparison of cytokine expression patterns observed in the 7-cytokine panel for 19 samples of healthy medullary bone of the jaw (green columns), for 128 BMDJ/FDOJ samples where we added the new R/C of 26 actually debrided BMDJ/FDOJ samples (red columns), and 26 PRF samples (blue columns). |
Figure 7 clearly shows that the cytokines R/C and IL-1RA, which are already elevated in the bone marrow defects, are expressed at even nearly double higher levels in the PRF. In contrast, the desired initial starter function for osteogenic wound healing of TNF-α, MCP-1 and IL-6 is only slightly promoted.
Lack of Counteraction to Cytokine Imbalance in BMDJ/FDOJ in PRF
One of the hypothetical aims in applying PRF postoperatively in this context is to counteract the effects of the pathogenetic BMDJ/FDOJ cytokine patterns with the introduction of compensatory cytokine concentrates present in PRF (see Figure 8). a) The downregulated TH-1 acute cytokines IL-6, MCP-1 and TNF-α should be upregulated (red arrows) by PRF application (yellow columns); b) the upregulated TH-2 cytokines should be downregulated (blue arrows); c) However, this is clearly not the case (Figure 8).
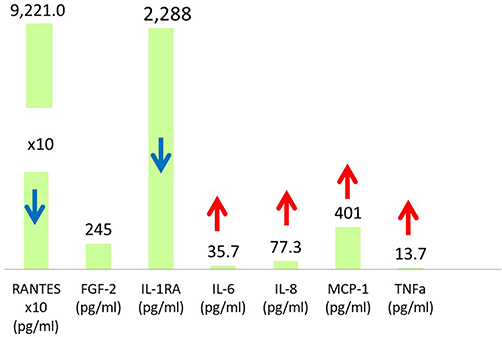 |
Figure 8 Hypothetical mechanism of aim of PRF (yellow columns), ie, balancing the pathological cytokine profile of BMDJ/FDOJ by upregulating TH-1 acute cytokines IL-6, MCP-1 and TNF-α, (red arrows), and downregulating TH-2 cytokines, (blue arrows). |
Osteoneogenetic Effect of RANTES/CCL5 Overexpression in PRF
Our data show that the PRF samples have an R/C expression of 9.221 pg/mL, a level twice as high as that found postoperatively in the corresponding BMDJ/FDOJ areas, ie, 5.218 pg/mL. At first glance, this could mean that with the application of PRF, the chemokine R/C is reintroduced in BMDJ/FDOJ surgical sites - or prepared implant sites - in double the concentration. From this perspective, the purpose of PRF application following the surgical removal of an area of chronic R/C expression due to BMDJ/FDOJ appears to be called into question. Interestingly, an increase in R/C has been associated with decreased vitamin D levels.22,28 An increased level of R/C in PRF may, therefore, be associated with reduced osteoneogenesis.
What, then, is the evidence against this obvious conclusion? On the one hand, R/C alone is highly expressed in PRF, which is not surprising given the concentrated number of platelets. However, it should be borne in mind that R/C present in PRF has different osteoimmunological significance than R/C found in BMDJ/FDOJ tissue which has been expressed continuously over years. In BMDJ/FDOJ areas, which are characterised by chronic impaired wound healing, the chemotactic advantage of R/C with respect to immunological rebalancing does not apply. The question remains as to why the high level of R/C in BMDJ/FDOJ is unable to resolve the chronic osteoimmune disorder found in these areas, even over years.29 The one-off application of PRF with an extremely high concentration of R/C contrasts with the chronic expression of R/C in BMDJ/FDOJ areas, which is also strikingly elevated.
Research shows that suppression of endogenous CCL5 expression inhibits osteogenesis.23 Downregulation of the chemokine receptors CCR1 and CCL5 receptors significantly reduces the osteogenesis of human mesenchymal stem cells (MSCs).23 Both R/C and the associated receptors (CCR1/CCR5) are required for the osteogenesis of MSCs. However, the function of R/C in osteogenesis, especially the effects of R/C on the process of differentiation of MSC into osteoblasts, has not yet been investigated in human cells and the regulatory mechanisms of R/C in the osteogenesis of human MSC are still unknown.30 Higher levels of R/C are associated with normal wound healing29 and both MCP-1 and R/C recruit macrophages to the site of injury.31 R/C has also been shown to be significantly increased in the wounds of younger burn patients compared to older patients.32 R/C thus appears to have two sides: At the same time, R/C is fundamentally required for osteogenesis and the high expression of this chemokine is generally regarded as conducive to positive wound healing.19,30,33 Thus, the favourable effects of PRF application may be since the R/C concentration is increased and osteoneogenesis is promoted.
Literature Review Comparing IL-1ra Expression in PRF and BMDJ/FDOJ
IL-1, a key proinflammatory cytokine, triggers the induction of a broad spectrum of other proinflammatory cytokines, including IL-6.31,34 Interleukin 1 mediates bone resorption and cartilage destruction. The cytokines IL-1 and TNF-α (see section 5.6) are the main proinflammatory signaling agents. These two cytokines are released by tissue macrophages when exposed to an inflammatory stimulus (such as bacteria, fungi and autoantigens, as well as foreign substances).35 The main proinflammatory effects of IL-1 and TNF-α are stimulation of T- and B- cells and macrophages, activation of the vascular endothelium and induction of the acute phase response.36 Research shows that the interleukin 1 (IL-1)-interleukin 1 receptor antagonist (IL-1ra) is an anti-inflammatory cytokine that selectively inhibits the effect of IL1, ie, IL-1ra blocks IL1-mediated inflammatory reactions.32,35
In this study, upregulated IL-1ra in PRF counteracts the activities of proinflammatory triggers IL-1 and IL-6 that are necessary for osteoneogenetic wound healing. Our data show that PRF has an IL-1ra expression of 2.346 pg/mL, an approximately 3-fold increase compared to the level in BMDJ/FDOJ (731 pg/mL).19 The overexpressed concentration of IL-1ra in PRF (2.346 pg/mL) appears to be counterproductive to optimal wound healing with an initial promotion of inflammation in the context of osseointegration and osteoimmunological rebalancing.
Literature Review Comparing TNF-α Expression in PRF and BMDJ/FDOJ
The inflammatory response plays a crucial role in the early phase of fracture healing. In a fracture, the immune cells, eg macrophages, lead to the secretion of inflammatory cytokines such as tumour necrosis factor-alpha (TNF-α), which controls the healing processes mediated by MSCs. In the first 24 hours after fracture, TNF-α expression is significantly increased under normal conditions and its influence on the concentration of MSCs and cell differentiation becomes significant three days after fracture.37 The absence of TNF-α signalling reduces the concentration of MSC in the callus by more than 20%. Thus, an optimal TNF-α concentration is required to promote the early phase of healing. Excessive or insufficient secretion of TNF-α may significantly hinder this process.36,37 The initial stage of BMDJ/FDOJ is characterised by having only one third of the TNF-α activity as healthy cancellous bone of the jaw. As TNF-α plays an essential role in promoting wound healing in the early phase of osteoneogenesis,28,32 the reduced TNF-α activity in BMDJ/FDOJ explains the deficient ossification present in these areas of the jaw.
Our data show a threefold increase in TNF-α expression in PRF compared to the level determined in the cytokine panel for previously obtained BMDJ/FDOJ samples.19 Overall, however, with a value of only 13.7 pg/mL, TNF-α expression in PRF appears to be rather under-regulated compared to the initial phase of osteoneogenesis in healthy jawbone (11,0 pg/mL).19
Literature Review Comparing MCP-1/CCL2 Expression in PRF and BMDJ/FDOJ
MCP-1/CCL2 is a chemokine classically associated with the recruitment of macrophages and monocytes during angiogenesis and also required for the normal progression of wound healing.38,39 MCP-1/CCL2 is CCL2-KO mice exhibited reduced re-epithelialisation associated with reduced macrophage infiltration of wounds.21,39 Acute MCP-1/CCL2 stimulation may facilitate osteogenesis during the initial phase of bone healing, promoting macrophage-MSC crosstalk and, subsequently, by the activation or licensing of MSCs by proinflammatory macrophage cytokines.39 This study demonstrates that MSC-derived MCP-1/CCL2 is required for MSC-induced accelerated wound healing.40 MCP-1/CCL2 expression also promotes osteogenesis. In coincidence with the above research our data show that MCP-1/CCL2 has a level of 397 pg/mL in PRF, which is a threefold higher activation of this inflammatory signal compared to that of BMDJ/FDOJ with 121.5 pg/mL. As a result, MCP-1/CCL2 in PRF may induce osteoneogenesis and compensate for the original deficit of MCP-1/CCL2 expression in BMDJ/FDOJ.
Limitations of the Study
This research is a singular observation, as the question remains open as to whether it may be precisely this mixture of pro- and anti-inflammatory mediators that leads to the activation of osteogenesis in PRF. Since cytokines always interact with each other, their individual effects should not be overestimated in the interpretation of the results of this study. Of course, the individual cytokines in the centrifuged plasma of PRF only have a positive or negative effect on the osteomodulatory target to the extent that the corresponding receptors are also present in the PRF. The question of whether PRF from FDOJ patients could prove a positive effect of PRF in promoting bone healing and osteoimmunological balance and the clinical observation of the application of PRF in the surgery of FDOJ patients need to be analysed in further studies.
Conclusion
Wound healing is an immune-inflammatory process that, ideally, could be stabilised by the application of PRF and brought into osteoimmunological balance. Unfortunately, PRF was mistakenly thought to be a cure for bone healing, which is here shown to be incorrect. Blood concentrates alone cannot heal bone. The centrifugation of serum and the PRF prepared in this way are only restricted capable of triggering a target-orientated dynamic for cytokine regulated osteoneogenesis that has not yet been fully clarified. The positive evidence and widespread use of PRF in dental practices nevertheless necessitates further research into the immune processes associated with PRF. The use of ultrasound-guided measurement of PRF-induced bone density and alveolar osteoneogenesis for the purpose of evaluation and clinical verification is an available and practical chairside technology. The currently available methods of radiographic monitoring do not appear to fulfil these requirements.
The aim of PRF application is to initiate a process of immune surveillance that contributes to the restoration of tissue homeostasis after oral surgery. Previous studies show that the high platelet content of plasma results in an increase in positive growth factors.11–13,15 Under the premises established in Osteoimmunology of Wound Healing, the results of our PRF analysis may be confusing or disappointing. At first glance, the expected immune inducing and counteracting effect of PRF on BMDJ/FDOJ areas does not appear to be direct or immediate. The imbalanced distribution of underexpressed TH-1 cytokines, such as IFN-g, TNF-α, MCP-1/CCL2 and IL-1, compared to overexpressed TH-2 cytokines, such as R/C and IL-1ra, that is originally present in BMDJ/FDOJ also persists in PRF rather than offsetting that distribution. The changing osteoimmunological effects of the cytokines present in PRF that were analysed in this study make it difficult to draw a clear conclusion, but they contribute to the knowledge base on osteoimmunology in jawbone. It is important to acknowledge that the data collected in this study with respect to the analysis of PRF only represent the initial findings regarding the early phase of an osteoimmunological process that takes place over a longer period of time.
Nonetheless a method is necessary for the documentation of success or failure in the application of PRF, preferably in a practical manner and with precise scaling, of the stages of osteoneogenesis and implant osseointegration induced by PRF. Radiation-free trans-alveolar ultrasonography, which is not stressful for the patient, is suitable for this purpose.41,42 This could provide further necessary scientific findings concerning the clinical effects of PRF.43
Institutional Review Board Statement
Included in the manuscript.
Abbreviations
PRF, platelet-rich fibrin; R/C, RANTES/CCL5; BMDJ, bone marrow defects of the jaw; FDOJ, fatty-degenerative osteonecrosis of the jaw.
Data Sharing Statement
The authors declare that all relevant data supporting the findings of this review are included in this article. For further requests, the corresponding author should be contacted.
Informed Consent Statement
Included in the manuscript.
Acknowledgments
The authors would like to thank all the patients who gave their consent to participate.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
Drs Johann Lechner reports a patent Europäisches Patent 3720382 PCT/EP2018/084199 issued to Dr. Johann Lechner. The authors report no other conflicts of interest in this work..
References
1. Amengual-Penafiel L, Cordova LA, Constanza Jara-Sepulveda M, Branes- Aroca M, Marchesani-Carrasco F, Cartes-Velasquez R. Osteoimmunology drives dental implant osseointegration: a new paradigm for implant dentistry. Jpn Dent Sci Rev. 2021;57:12–19. doi:10.1016/j.jdsr.2021.01.001
2. Lechner J, Schulz T, von Baehr V. Immunohistological staining of unknown chemokine RANTES/CCL5 expression in jawbone marrow defects—osteoimmunology and disruption of bone remodeling in clinical case studies targeting on predictive preventive personalized medicine. EPMA J. 2019;1–14. doi:10.1007/s13167-019-00182-1
3. Bar-Shavit Z. The osteoclast: a multinucleated, hematopoietic-origin, bone-resorbing osteoimmune cell. J Cell Biochem. 2007;102(5):1130–1139. doi:10.1002/jcb.21553
4. Wang X, Li Y, Feng Y, Cheng H, Li D. The role of macrophages in osseointegration of dental implants: an experimental study in vivo. J BioMed Mater Res A. 2020;108(11):2206–2216. doi:10.1002/jbm.a.36978
5. McDade TW. Early environments and the ecology of inflammation. Proc Natl Acad Sci U S A. 2012;109 Suppl 2:17281–17288. doi:10.1073/pnas.1202244109
6. Negrescu AM, Cimpean A. The state of the art and prospects for osteoimmunomodulatory biomaterials. Materials. 2021;14(6):1357. doi:10.3390/ma14061357
7. Choukroun E. Oxidative stress and osteoimmunology: the two missing pieces of the oral osseointegration puzzle. Immunol Res and Ther J. 2021;3(1):119.
8. Albrektsson T, Becker W, Coli P, Jemt T, Molne J, Sennerby L. Bone loss around oral and orthopedic implants: an immunologically based condition. Clin Implant Dent Relat Res. 2019;21(4):786–795. doi:10.1111/cid.12793
9. Alsousou J, Thompson M, Hulley P, et al. The biology of platelet-rich plasma and its application in trauma and orthopaedic surgery: a review of the literature. J Bone Joint Surg Br. 2009;91(8):987–996. doi:10.1302/0301-620X.91B8.22546
10. Dohan Ehrenfest DM, Pinto NR, Pereda A, et al. The impact of the centrifuge characteristics and centrifugation protocols on the cells, growth factors, and fibrin architecture of a leukocyte- and platelet-rich fibrin (L-PRF) clot and membrane. Platelets. 2018;29(2):171–184. doi:10.1080/09537104.2017.1293812
11. Choukroun J, Diss A, Simonpieri A, et al. Platelet-rich fibrin (PRF): a second-generation platelet concentrate. Part IV: clinical effects on tissue healing. Oral Surg Oral Med Oral Pathol Oral Radiol. 2006;101(3):e56–e60. doi:10.1016/j.tripleo.2005.07.011
12. Ghanaati S, Booms P, Orlowska A, et al. Advanced platelet-rich fibrin: a new concept for cell-based tissue engineering by means of inflammatory cells. J Oral Implantol. 2014;40(6):679–689. doi:10.1563/aaid-joi-D-14-00138
13. Ghanaati S, Herrera-Vizcaino C, Al-Maawi S, et al. Fifteen years of platelet rich fibrin in dentistry and oromaxillofacial surgery: how high is the level of scientific evidence? J Oral Implantol. 2018;44(6):471–492. doi:10.1563/aaid-joi-D-17-00179
14. Damsaz M, Castagnoli CZ, Eshghpour M, et al. Evidence-based clinical efficacy of leukocyte and platelet-rich fibrin in maxillary sinus floor lift, graft and surgical augmentation procedures. Front Surg. 2020;7:537138. doi:10.3389/fsurg.2020.537138
15. Choukroun J, Ghanaati S. Reduction of relative centrifugation force within injectable platelet-rich-fibrin (PRF) concentrates advances patients’ own inflammatory cells, platelets and growth factors: the first introduction. European J Trauma Emerg Surg. 2018;44:87–95. doi:10.1007/s00068-017-0767-9
16. Blatt S, Thiem DGE, Kyyak S, et al. Possible implications for improved osteogenesis? The combination of platelet-rich fibrin with different bone substitute materials. Front Bioeng Biotechnol. 2021;9:640053. doi:10.3389/fbioe.2021.640053
17. Lechner J, Mayer W. Immune messengers in neuralgia inducing cavitational osteonecrosis (NICO) in jaw bone and systemic interference. Eur J Int Med. 2010;2(2):71–77. doi:10.1016/j.eujim.2010.03.004 ISSN 1876-3820.
18. Lechner J, von Baehr V. RANTES and fibroblast growth factor 2 in jawbone cavitations: triggers for systemic disease? Int J Gen Med. 2013;6:277–290. doi:10.2147/IJGM.S43852
19. Lechner J, von Baehr V. Chemokine RANTES/CCL5 as an unknown link between wound healing in the jawbone and systemic disease: is prediction and tailored treatments in the horizon? EPMA J. 2015;6:10. doi:10.1186/s13167-015-0032-4
20. Kong YY, Feige U, Sarosi I, et al. Activated T cells regulate bone loss and joint destruction in adjuvant arthritis through osteoprotegerin ligand. Nature. 1999;402(Suppl 6763):43–47. doi:10.1038/35005552
21. Boyle W, Simonet W, Lacey D. Osteoclast differentiation and activation. Nature. 2003;423:337–342. doi:10.1038/nature01658
22. Yang N, Liu Y. The role of the immune microenvironment in bone regeneration. Int J Med Sci. 2021;18(16):3697–3707. doi:10.7150/ijms.61080
23. Schmidt-Bleek K, Kwee BJ, Mooney DJ, Duda GN. Boon and bane of inflammation in bone tissue regeneration and its link with angiogenesis. Tissue Eng Part B Rev. 2015;21:354–364.
24. Okamoto K, Nakashima T, Shinohara M, et al. Osteoimmunology: the conceptual framework unifying the immune and skeletal systems. Physiol Rev. 2017;97:1295–1349. doi:10.1152/physrev.00036.2016
25. Lechner J, Schuett S, von Baehr V. Aseptic-avascular osteonecrosis: local “silent inflammation” in the jawbone and RANTES/CCL5 over expression. Clin Cosmetic Invest Dentistry. 2017;9:99–109. doi:10.2147/CCIDE.S149545
26. Ghanaati S, Mourao C, Adam E, Sader R, Zadeh H, Al-Maawi S. The role of centrifugation process in the preparation of therapeutic blood concentrates: standardization of the protocols to improve reproducibility. Int J Growth Factors Stem Cells Dent. 2019;2(3):41. doi:10.4103/GFSC.GFSC_15_19
27. Diederich J, Schwagten H, Biltgen G, Lechner J, Müller KE. Reduction of inflammatory RANTES/CCL5 serum levels by surgery in patients with bone marrow defects of the jawbone. Clin Cosmet Investig Dent. 2023;15:181–188. doi:10.2147/CCIDE.S417783
28. Lechner J, Aschoff J, Rudi T. The vitamin D receptor and the etiology of RANTES/CCL- expressive fatty-degenerative osteolysis of the jawbone: an interface between osteoimmunology and bone metabolism. Int J Gen Med. 2018;11:155–166. [pmid:29731660]. doi:10.2147/IJGM.S152873
29. Frank S, Kampfer H, Wetzler C, Stallmeyer B, Pfeilschifter J. Large induction of the chemotactic cytokine RANTES during cutaneous wound repair: a regulatory role for nitric oxide in keratinocyte-derived RANTES expression. Biochem J. 2000;347(Pt 1):265–273. doi:10.1042/bj3470265
30. Liu YC, Kao YT, Huang WK, et al. CCL5/RANTES is important for inducing osteogenesis of human mesenchymal stem cells and is regulated by dexamethasone. Biosci Trends. 2014;8(3):138–143. [pmid:25030847]. doi:10.5582/bst.2014.01047
31. Kobayashi Y. The role of chemokines in neutrophil biology. Front Biosci. 2008;13:2400–2407. doi:10.2741/2853
32. Farinas AF, Bamba R, Pollins AC, Cardwell NL, Nanney LB, Thayer WP. Burn wounds in the young versus the aged patient display differential immunological responses, BURNS. J Int Soc Burn Injuries. 2018;44(6):1475–1481. doi:10.1016/j.burns.2018.05.012
33. Kroeze KL, Jurgens WJ, Doulabi BZ, van Milligen FJ, Scheper RJ, Gibbs S. Chemokine-mediated migration of skin-derived stem cells: predominant role for CCL5/RANTES. J Investigat Dermatol. 2009;129(6):1569–1581. doi:10.1038/jid.2008.405
34. Tahtinen S, Tong AJ, Himmels P, et al. IL-1 and IL-1ra are key regulators of the inflammatory response to RNA vaccines. Nat Immunol. 2022;23(23):532–542. doi:10.1038/s41590-022-01160-y
35. Schiff MH. Schiff MH. Role of interleukin 1 and interleukin 1 receptor antagonist in the mediation of rheumatoid arthritis. Ann Rheumatic Dis. 2000;59:i103–i108. doi:10.1136/ard.59.suppl_1.i103
36. Zhang E, Miramini S, Patel M, et al. Role of TNF-α in early-stage fracture healing under normal and diabetic conditions. Comput Meth Programs Biomed. 2022;213:106536. ISSN 0169-2607. doi:10.1016/j.cmpb.2021.106536
37. Timmen M, Hidding H, Wieskötter B, et al. Influence of antiTNF-alpha antibody treatment on fracture healing under chronic inflammation. BMC Musculoskelet Disord. 2014;15:184. doi:10.1186/1471-2474-15-184 PMID: 24885217; PMCID: PMC4059090.
38. Masakazu T, Zhang N, Tsubosaka M, et al. CCL2 promotes osteogenesis by facilitating macrophage migration during acute inflammation. Front Cell Deve Biol. 2023;11:1213641.
39. Whelan DS, Caplice NM, Clover AJP. Mesenchymal stromal cell derived CCL2 is required for accelerated wound healing. Sci Rep. 2020;10:2642. doi:10.1038/s41598-020-59174-1
40. Hong KH, Ryu J, Han KH. Monocyte chemoattractant protein-1-induced angiogenesis is mediated by vascular endothelial growth factor-A. Blood. 2005;105(4):1405–1407. doi:10.1182/blood-2004-08-3178 Epub 2004 Oct 21. PMID: 15498848.
41. Lechner J, Zimmermann B, Schmidt M, von Baehr V. Ultrasound sonography to detect focal osteoporotic jawbone marrow defects: clinical comparative study with corresponding hounsfield units and RANTES/CCL5 expression. Clin Cosmet Investig Dent. 2020;12:205–216. doi:10.2147/CCIDE.S247345
42. Lechner J, Zimmermann B, Schmidt M. Focal bone-marrow defects in the jawbone determined by ultrasonography—validation of new trans-alveolar ultrasound technique for measuring jawbone density in 210 participants. Ultrasound Med Biol. 2021;12. doi:10.1016/j.ultrasmedbio.2021.07.012.
43. Lechner J, von Baehr V, Notter F, Schick F. Osseointegration and osteoimmunology in implantology: assessment of the immune sustainability of dental implants using advanced sonographic diagnostics: research and case reports. J Int Med Res. 2024;52(1). doi:10.1177/03000605231224161
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.