Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 14
Platelet Indices and Its Association with Microvascular Complications Among Type 2 Diabetes Mellitus Patients in Northeast Ethiopia: A Cross-Sectional Study
Authors Taderegew MM ![]() , Woldeamanuel GG
, Woldeamanuel GG ![]() , Emeria MS
, Emeria MS ![]() , Tilahun M
, Tilahun M ![]() , Yitbarek GY
, Yitbarek GY ![]() , Zegeye B
, Zegeye B ![]()
Received 5 January 2021
Accepted for publication 4 February 2021
Published 25 February 2021 Volume 2021:14 Pages 865—874
DOI https://doi.org/10.2147/DMSO.S300460
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Mitku Mammo Taderegew,1 Gashaw Garedew Woldeamanuel,1 Mamo Solomon Emeria,2 Melkamu Tilahun,3 Getachew Yideg Yitbarek,4 Betregiorgis Zegeye5
1Department of Biomedical Sciences, College of Medicine and Health Sciences, Wolkite University, Wolkite, Ethiopia; 2Department of Nursing, College of Medicine and Health Sciences, Wolkite University, Wolkite, Ethiopia; 3Department of Biomedical Sciences (Medical Physiology), College of Medicine and Health Sciences, Debre Markos University, Debre Markos, Ethiopia; 4Department of Biomedical Sciences, College of Health Sciences, Debre Tabor University, Debre Tabor, Ethiopia; 5HaSET Maternal and Child Health Research Program, Shewarobit Field Office, Shewarobit, Ethiopia
Correspondence: Mitku Mammo Taderegew
Department of Biomedical Sciences, School of Medicine, College of Medicine and Health Sciences, Wolkite University, PO Box 07, Wolkite, Ethiopia
Email [email protected]
Purpose: Platelet indices have been shown to be associated with complications of diabetes mellitus (DM). However, the clinical relevance of platelet indices for assessing the risk of being microvascular complications among patients with DM is largely overlooked. Hence this study aimed to determine the association of platelet indices with microvascular complications among type 2 DM patients.
Patients and Methods: A hospital-based cross-sectional study was conducted among 352 type 2 DM patients from April 1 to May 30/2019 at Debre Berhan Referral Hospital. Data were collected by interview, physical measurements, document review, and laboratory tests. Then the data were entered into Epi-data manager-4.4.1.0 and exported into SPSS-25 for analysis. Platelet indices were compared between participants with and without microvascular complications using an independent t-test. A logistic regression model was used to assess the association between microvascular complications and platelet indices. All inferences were considered statistically significant at P< 0.05.
Results: One hundred seventeen (33.2%) of participants were suffering from at least one microvascular complications. The mean platelet volume (MPV), platelet distribution width (PDW), and platelet-large cell ratio (P-LCR) were significantly increased in DM patients with complications as compared to without complications (13.57± 2.17fl vs. 11.76± 1.93fl), (16.57± 2.49fl vs. 14.97± 2.41fl) and (28.09± 7.58% vs. 24.19± 6.46%), respectively (all are P˂0.001). In multivariate logistic regression analysis, MPV (AOR=1.68, 95% CI: 1.37– 2.05), PDW (AOR=1.37, 95% CI: 1.15– 1.63), P-LCR (AOR=1.07, 95% CI: 1.01– 1.14), age (AOR=1.07, 95% CI: 1.01– 1.12), and duration of DM (AOR=1.31, 95% CI: 1.18– 1.46) were significantly associated with the presence of microvascular complications.
Conclusion: MPV, PDW, and P-LCR were significantly higher among type 2 DM patients with microvascular complications. This indicates that platelet indices can be used as prognostic markers of vascular complications and can be used as simple and cost-effective parameters to predict microvascular complications particularly in patients with old age and long duration of DM.
Keywords: platelet indices, microvascular complication, type 2 DM, Ethiopia
Introduction
Diabetes mellitus (DM) is a complex metabolic disorder of great impact worldwide with a central theme of chronic hyperglycemia arising from insulin deficiency or insulin resistance or both.1 Type 2 diabetes mellitus is the predominant form of diabetes worldwide, accounting for 90% of cases globally.2
Diabetes mellitus has been growing rapidly as a worldwide public health problem. According to International Diabetes Federation (IDF) estimation, as of 2019, 463 million (8.8%) adults had DM worldwide. These global prevalence is estimated to be increased to 700 million (10.9%) by the end of 2045. It is estimated that the middle and low-income countries will bear the brunt of the diabetes epidemic to the extent of 80% of the global burden.3
The chronic hyperglycemia and attendant metabolic deregulation of DM resulting in long-term diabetes-related complications in multiple organ systems of the body.4 These complications are responsible for the majority of morbidity and mortality associated with the disorder which impairs the quality of life of the patient and imposes significant cost implications for the patient, relatives, and the healthcare system.5
If microvascular complications are detected at the earlier stages it will be useful in controlling them and protecting the patients from associated adverse events.6 However, screening all DM patients for all microvascular complications has an economic burden since they involve multiple specialties and need lifelong follow-up. At this juncture, it may be helpful if there is a parameter that can find out DM patient who is at higher risk of developing these complications.5,7
Due to metabolic abnormality, platelets in DM are larger, hyperactive, and release more granules, and have an increased tendency to thrombotic events leading to both macrovascular and microvascular complications which in turn increases morbidity and mortality.7–9
Hence, platelet indices which commonly available from the routine hematological analysis may provide important information for early detection and evaluation of diabetes-related complications so that timely intervention could be taken from earlier stages.10
Nevertheless, measurements of platelet indices are simple, inexpensive, and easily available from routine laboratories investigation and are done nearly for every patient coming to the hospital via a routine complete blood count test, clinicians were not routinely considered platelet parameters for assessing the status of the patients. Besides data on platelet parameter and their association with vascular complications are scarce in sub-Saharan countries particularly in Ethiopia.
Hence, in view of this, the study was conducted to assess platelet indices and its association with the microvascular complications among type 2 DM patients attending Debre Berhan Referral Hospital, North-East Ethiopia. To the best of our knowledge, this is the first study in Ethiopia that investigates the relationships between platelet indices and diabetes-related complications.
The finding of the study is helpful in establishing the association between platelet indices and microvascular complications among type 2 DM patients so as to know whether platelet indices can be of any help in the early screening of complications which would reduce morbidity and healthcare costs of the patients. The study also provides input for other researchers, as baseline data for further investigations.
Patients and Methods
Study Setting and Design
A cross-sectional study was conducted among type 2 DM patients at Debre Berhan referral hospital which is located 130 km North-East of Addis Ababa, the capital city of Ethiopia from November-1 to December 30/2019. Debre Berhan Referral Hospital provides DM follow-up services along with other inpatient and outpatient health care and medical services. Besides the routine follow-up care practice, the diabetes follow-up clinic provides diabetes-related complications screening service for all DM patients for the first contact. Then every 6 months patients were screened for these complications.
Study Population and Sampling Techniques
All type 2 DM patients attending the hospitals during the study periods were eligible for the study, whereas patients with a history of blood transfusion in the last three weeks, taking drugs that cause bone marrow suppression, participants with a history of blood loss (gastrointestinal or genitourinary bleeding), pregnancy mothers, male patients with hemoglobin below 13 g/dl and female patients below 12 g/dl, and patients on antiplatelet drugs were excluded. Participants with other known chronic diseases (hematologic diseases, malignancies, kidney disease, and chronic liver disease) were also excluded to rule out any other causes of reactive platelets.
The required sample size of the study was estimated using a statistical formula for single population proportion by taking the prevalence of microvascular complications as 38.5%,11 a confidence interval of 95% (Z a/2=1.96), and 5% level of precision. Hence, the final sample size was 364. A systematic random sampling technique based on the order of their visit was used for selecting the study participants. The first participant was randomly selected by writing down the medical record numbers of the first two participants in separate papers and thereafter selecting one randomly. Then, every other patient that meets the inclusion criteria was enrolled in the study.
Data Collection Procedures and Operational Definitions
Data were collected by a face-to-face interview, review of patient’s medical records, physical measurements, and collecting laboratory investigation using a pre-tested structured questionnaire. A detailed history was taken regarding the socio-demographic and clinical characteristics of the study participants. Data regarding the presence of hypertension, duration of DM, current treatment for DM, and diabetes-related microvascular complications were collected from each study participant’s via review of their medical records.
Regarding anthropometric measurements, weight and height were measured using an electronic weight scale and a portable standard stadiometer with proper calibrations to calculate the body mass index (BMI) as weight in kilograms divided by the square of height in meters.12,13 Waist circumference was measured to the nearest 0.1 cm with a non-extensible inelastic measuring tape at the midpoint between the last rib and the iliac crest at the end of the normal expiration, with keeping the participant standing up straight, parallel legs and arms hanging down on the sides. The measurement was repeated and the average value was recorded for analysis. Then abdominal obesity was defined as a waist circumference of greater than 88 cm for females and greater than 102 cm for males.14
Blood pressure (BP) was measured twice (5 minutes apart) using a standard digital sphygmomanometer with appropriate cuffs in a sitting position after at least 5-minutes of rest. An average of two measurements was recorded for analysis. If the difference between the two readings was >5mm Hg, the measurement was repeated and the average of the two closest readings was considered for classifying blood pressure. Then participants with systolic/diastolic blood pressure levels ≥130/80 mmHg or with antihypertensive medication regardless of the current BP were defined as having hypertension.15
After overnight fasting, 4 mL of venous blood samples were drawn with aseptic precautions from the antecubital vein from each study participant by trained data collectors. Then 2 mL of the samples were taken in the Ethylene diamine tetraacetic acid (EDTA) tube for complete blood count for determination of platelet indices and the remaining 2 mL into a plain tube for plasma glucose analysis.
Analysis of platelet indices was performed by using the ABX Micros 60 automated hematology cell counter (Horiba- ABX, Montpellier, France). Plasma glucose levels were analyzed with a glucometer. The analysis was done according to standard operating procedures within 2 hours of sample collection to avoid changes due to aging of the blood sample.
To ensure data quality, the questionnaire was initially prepared in English and translated to Amharic language (local language) by an expert who has a good ability of the two languages. The Amharic language version again was retranslated back into English by another expert to ensure consistency. The questionnaire was pre-tested on 19 type 2 DM patients (5% of the actual sample size) in the Debre Sina Hospital before it was administered to the study participants. Based on the pre-test some modifications have been done to the questionnaire and the modified questionnaire was used for the final data collection. Three data collectors (one nurse and two laboratory technicians) and one supervisor were recruited and one-day training was given for them by the principal investigator regarding the objectives of the study, the data collection procedures, and the confidentiality of the information. The data collection procedures were checked frequently through supervision by the investigators and supervisor for its consistency. Additionally, the collected data were checked daily by the principal investigator to safeguard its completeness and clarity.
Statistical Analysis
Before entry, data were cleaned and checked for any missing values. Then, it entered into Epi-data manager version 4.4.1.0 and exported to SPSS version-25 software for statistical analysis. The data were also checked; for its distribution and outliers before analysis. The normality test of variables was evaluated by using the Kolmogorov–Smirnov and Shapiro–Wilk tests. Then the data were processed by using descriptive analysis, including frequency distribution, cross-tabulation, and summary measures.
Data were expressed as mean ± standard deviation (±SD) for all normally distributed continuous variables and as frequency and percentage for categorical variables. Independent t-test and chi-square test were used to evaluate the differences in the distribution of continuous and categorical variables with respect to the presence or absence of microvascular complications, respectively.
Binary logistic regression analysis was performed to assess the association between microvascular complications and platelet indices as the main predictors. In the regression analysis, other known conventional risk factors for diabetic microvascular complications were included as covariates in the model. To identify the predictors that were independently associated with microvascular complications, only independent variables with a P-value <0.25 in the unadjusted model of logistic regression analysis were included in the multivariate logistic regression model. All inferences were considered statistically significant at P<0.05.
Results
Socio-Demographic Characteristics of the Participants
A total of 364 study participants were invited and 352 of them fulfilled the inclusion criteria and volunteered to participate in the study making the response rate 97.1%. The mean age (±SD) of the study participant was 54.2 (±8.5) years, ranging from 36 to 76 years. Out of 352 study participants, 184 (52.3%) were females and 225 (63.9%) were from an urban area (Table 1).
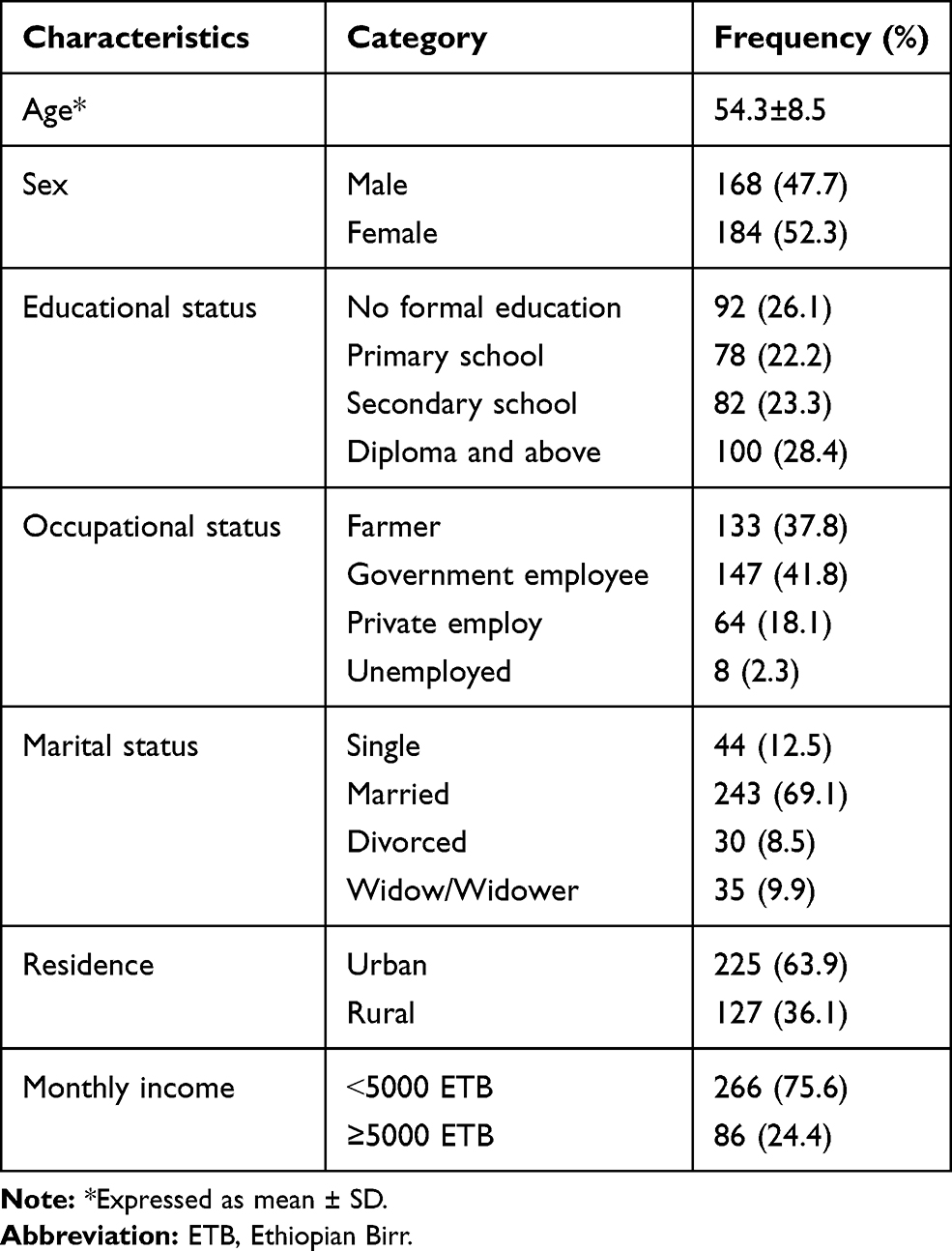 |
Table 1 Socio-Demographic Characteristics of the Study Participants (n=352) |
Clinical Characteristics of the Participants
More than half (54.5%) of the study participants were suffering from diabetes for 1–7 years duration. The mean (±SD) of BMI and waist circumference were found to be 23.3 (±3.7) kg/m2 and 84.7 (±6.9) cm, respectively. The Mean (±SD) of SBP and DBP were also found to be 132.99 (±13.99) mmHg and 82.57 (±11.04) mmHg, respectively, and 139 (39.5%) were hypertensive. Three-fourths (76.7%) of the study participants were on oral hypoglycemic agents and the remaining were on combined treatments of insulin and oral hypoglycemic agents (Table 2).
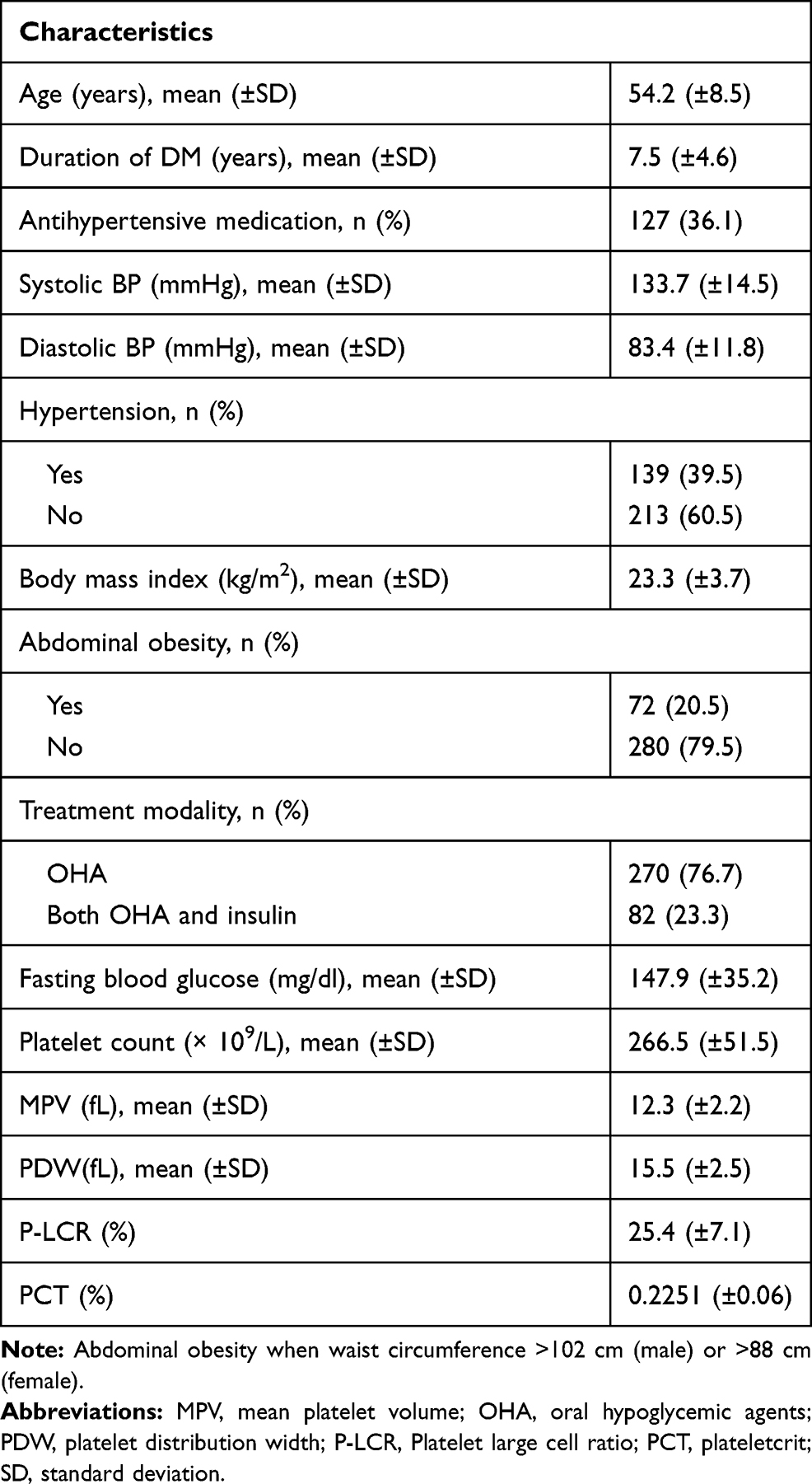 |
Table 2 Clinical Characteristics of the Study Participants (n=352) |
Platelet Indices Among the Study Participants with or without Microvascular Complications
From the total of the study participants, 117 (33.2%) were presented with at least one documented record of diabetes-related microvascular complications, namely retinopathy, neuropathy, and nephropathy. Among the microvascular complications, retinopathy, nephropathy, and neuropathy were seen in 66 (18.8%), 39 (11.1%), and 23 (6.5%) participants, respectively. One hundred six participants (30.1%) had only one microvascular complication while 11 participants (3.1%) had more than one complications.
Diabetic patients with microvascular complications showed significantly higher mean platelet volume (MPV), platelet distribution width (PDW), and platelet-large cell ratio (PLCR) than DM patients without microvascular complications (P˂0.05). Diabetic patients with microvascular complications also showed higher plateletcrit (PCT) than those without microvascular complications; however, these differences were not found to be statistically significant. On the other hand, diabetic patients with microvascular complications showed lower mean platelet count than those without microvascular complications, however, these differences were also not found to be significant (P >0.05). Concerning demographic, clinical, and biochemical indices among the study participants with or without complications, participants with complications had significantly higher mean age and duration of diabetes as compared to patients without complications (P <0.05). The mean value of BMI, SBP, DBP, and FBS was also found to be higher among participants with complications as compared to participants without complication, but only BMI and FBS were found to be statistically significant (P <0.05) (Table 3).
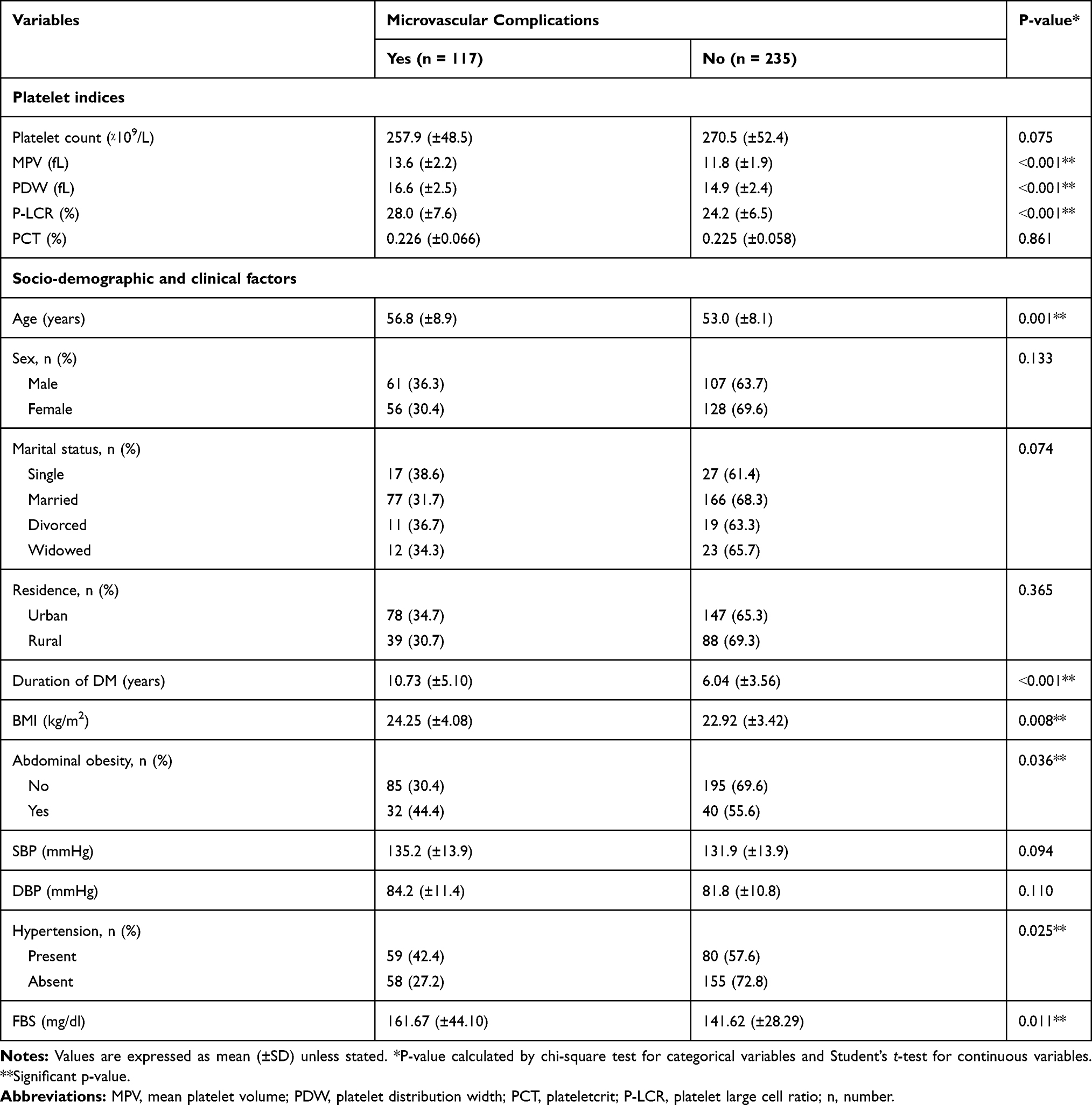 |
Table 3 Comparison of Mean Platelet Indices and Clinical Characteristics with the Presence of Microvascular Complication Among the Study Participants (n=352) |
Regarding the types of microvascular complications, MPV, PDW, and P-LCR were found to be significantly increased in diabetic retinopathy (P<0.001), (P<0.001), and (P=0.005), respectively and only P-LCR was significantly increased in diabetic neuropathy (P<0.001). MPV and PDW were also significantly higher in diabetic nephropathy as compared to their counterparts (P<0.05) (Table 4).
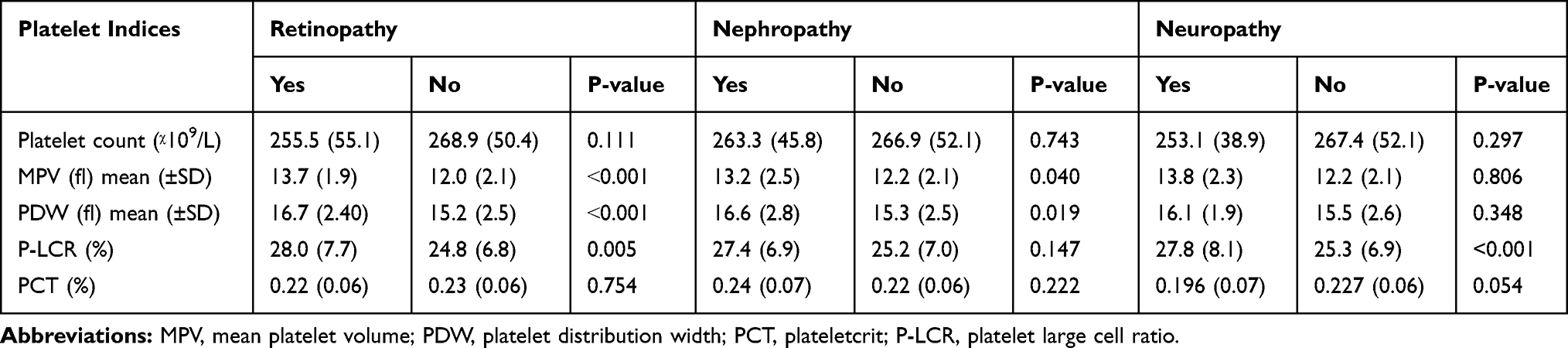 |
Table 4 Comparison of Platelet Indices According to the Types of Microvascular Complications Among the Study Participant (n=352) |
Factors Associated with Microvascular Complications Among the Study Participants
In univariate logistic regression analysis, MPV (COR=1.56, 95% CI: 1.34–1.81, P ˂0.001), PDW (COR=1.32, 95% CI: 1.16–1.48, P ˂0.001), and P-LCR (COR=1.09, 95% CI: 1.04–1.13, P˂0.001) were significantly associated with the presence of diabetes-related microvascular complications among type 2 DM patients. After adjustment for age, sex, duration of DM, BMI, waist circumference, systolic and diastolic blood pressure, hypertension, and FBS of the study participants within multiple logistic regression, MPV (AOR=1.68, 95% CI: 1.37–2.05), PDW (AOR=1.37, 95% CI: 1.15–1.63), and P-LCR (AOR=1.07, 95% CI: 1.01–1.14) remained significantly associated with the presence of microvascular complications and the associations were more strengthened. Other independent predictors of microvascular complications in the study were age (AOR=1.07, 95% CI: 1.01–1.12), and duration of DM (AOR=1.31, 95% CI: 1.18–1.46) (Table 5).
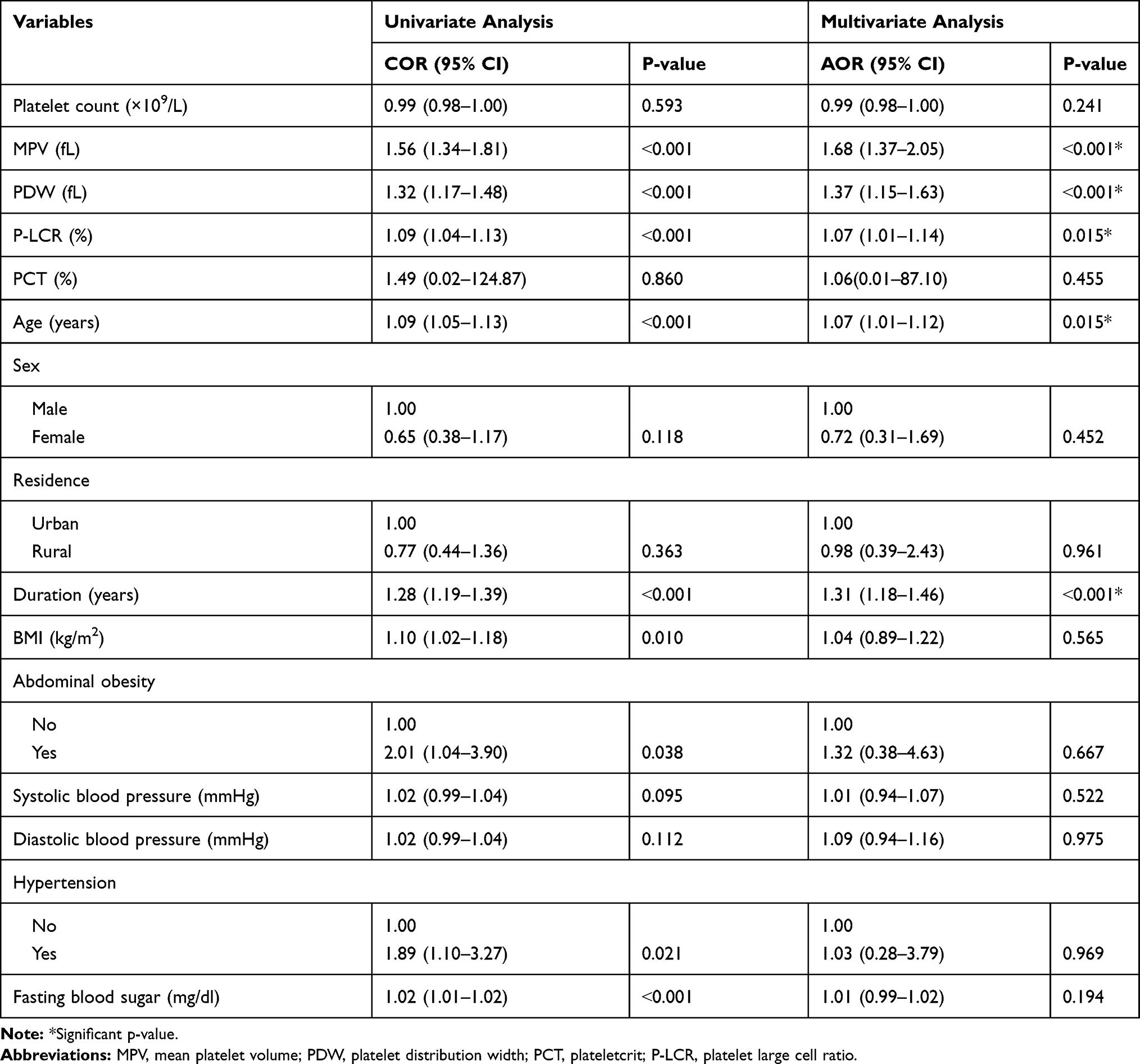 |
Table 5 Factors Associated with Microvascular Complication Among the Study Participants Attending Debre Berhan Referral Hospital, Northeast Ethiopia, 2018 (n=352) |
Discussion
Diabetes is a growing global public health problem associated with an increased risk of microvascular and macrovascular complications.16 With the easy availability of various blood tests such as MPV, efforts are made to identify and prove their utility to act as biomarkers for early detection of diabetic complications.
In this institution based cross-sectional study, platelet indices and its association with microvascular complications among type 2 DM patients at Debre Berhan Referral Hospital Northeast Ethiopia have been assessed. The study was found that MPV, PDW, and P-LCR have significantly increased in type 2 DM patients with microvascular complications as compared to patients without microvascular complications.
After adjusting for potential confounders in multivariate logistic regression, increases in MPV, PDW, and P-LCR levels were significantly associated with the presence of microvascular complications. This was in accordance with studies conducted by Desai et al,17 Tanima Dwivedi and Reshma Davangeri,10 Sushma K and Rangaswamy M,18 Walinjkar et al,19 Pujani et al,20 and Shilpi et al.21
On the other hand, the studies conducted by Alhadas et al,22 and Subashini et al6 have observed that both MPV and PDW were significantly higher in type 2 DM patients with microvascular complications than those without microvascular complications. Moreover, a significantly higher value of MPV has observed in the study results of Yenigün et al.23 Pradeep Nigam et al,24 Dubey et al25 and Buch et al.5 In addition to this, Jindal et al9 showed that PDW was significantly higher in type 2 DM patients with microvascular complications than those without microvascular complications.
An increase in MPV, PDW, and P-LCR is a potential biomarker of an increase in platelet size and reactivity.5,21,26,27 In hyperglycemic condition, the higher blood glucose level increases the production of glycoproteins and causes non-enzymatic glycation of these proteins on the surface of the platelets, which decrease platelets membrane fluidity and causing hyperactive platelets.28,29 Plasma glucose concentration also directly enhances the activation of the arachidonic acid pathway leads to increased thromboxane A2 formation which is one of the potent platelet activators and contributes to hyperactivity of platelets in diabetic patients.30
Hyperactive platelets are larger, highly active, and releases more granules and hence causing increased coagulation, impaired fibrinolysis, and endothelial dysfunction thereby increases the pathogenesis of vascular complications.10,17 In addition, these hyperactive platelets are transformed into the multi-pseudopodia structure and become potentially liable for adhesion and adherence which leads to vascular complications.31
Furthermore, in hyperglycemic conditions, the raised blood glucose level and some glucose metabolites leading to osmotic swelling of platelets which in turn increase platelets reactivity, and perhaps shorten the life span of platelets which reflects the increased release of young and larger platelets from bone marrow. These young and larger platelets are more enzymatically and metabolically active and have an increased tendency to form thrombotic events leading to both macrovascular and microvascular complications which in turn increases morbidity and mortality in diabetic patients.32
In agreement with Dwivedi et al10 and Buch et al5 studies, this study showed that platelet count was lower in patients with microvascular complications than those without microvascular complications but it was not statistically significant. One possible explanation for the decreased in platelet counts in participants with microvascular complications was centered on the rapid consumption of activated platelets in diabetics with complications.7 Oxidative stress, characterized by a disturbance between the production of reactive oxygen species and antioxidant defenses, is a common condition in type 2 DM, may also exert a significant effect on the regulation of platelets life span and platelets homeostasis, thus leading to rapid destruction of the platelets is another possible explanation.33
Besides platelet indices, in this study duration of DM was significantly associated with microvascular complications in which a 1.31-fold increase in the risk of microvascular complications occurrence as the duration of DM increased by one year. This is in accordance with the results of Bui et al,34 and Ramnath et al35 in which long duration of DM was reported to be a non-avoidable risk factor for microvascular complications. This may be due to the effects of prolonged hyperglycemia in the formation of advanced glycation end products which increases the pathogenesis of vascular complications in the different organs of the body.36–38
It was also likely that the difference in the prevalence of microvascular complications might result from differences in the age of the participants in which 1.07-fold increase in the risk of microvascular complications occurrence as the age of the participants increased by one year. This may be due to the presence of other co-morbidities, which are common in the elderly.
Limitations
Regarding the limitations of our study, the lack of a control group, using plasma glucose levels instead of glycosylated hemoglobin for assessing glycemic control, assessing only microvascular complications, and the use of secondary data for assessing microvascular complications were the limitations of the study. The study was also limited in its ability to identify causal relationships between platelet indices and microvascular complications. Hence, further studies with more strong study design are needed to investigate the cause-effect relationship.
Conclusion
MPV, PDW, and P-LCR have significantly increased in type 2 DM patients with complications as compared to those without complications. The higher values of MPV, PDW, and P-LCR in participants with microvascular complications indicates that platelet indices can be used as better prognostic markers for early detection of diabetic complications and can be used as a simple and cost-effective parameter to monitor and predict the risk of microvascular complications and institute appropriate preventive measures in diabetes.
Abbreviations
BMI, body mass index; BP, blood pressure; CI, confidence interval; DBP, diastolic blood pressure; DM, diabetes mellitus; EDTA, ethylene diamine tetraacetic acid; IDF, International Diabetic Federation; IRB, Institutional Review Board; MPV, mean platelet volume; OHA, oral hypoglycemic agent; PC, plateletcrit; PDW, platelet distribution width; P-LCR, platelet large cell ratio; SBP, systolic blood pressure; SD, standard deviation.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The study was conducted in accordance with the ethical standard of the Helsinki Declaration of 1964 and later versions. The study protocol was approved by the Institutional Review Board (IRB) of Jimma University. Permission and supportive letter were also obtained from Debre Berhan Referral Hospital. The aim of the study was clarified to all eligible study participants who fulfilling inclusion criteria and their consent was sought. Then written informed consent was obtained from all study participants before the study and all the findings of the study were used for the betterment of the study participants.
Acknowledgments
We would like to extend our gratitude to Jimma University for logistic support for this study. We are also very grateful to Debre Berhan Referral Hospital DM clinic staff for their teamwork in the study. Finally, our deepest gratitude goes to the study participants for providing the required information for this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for this study and the study was funded by the authors.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Petersmann A, Nauck M, Müller-wieland D, et al. Definition, classification and diagnosis of diabetes mellitus. Exp Clin Endocrinol Diabetes. 2018;126(7):406–410. doi:10.1055/a-0584-6223
2. Saeedi P, Petersohn I, Salpea P, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the international diabetes federation diabetes atlas, 9th edition. Diabetes Res Clin Pract. 2019;157:107843. doi:10.1016/j.diabres.2019.107843
3. IDF Diabetes Atlas Ninth edition. 2019. Available from: https://www.diabetesatlas.org/upload/resources/material/20200302_133351_IDFATLAS9e-final-web.pdf.
4. American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2009;32(Supplement 1):S62–S67. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2613584/pdf/S62.pdf. Accessed February 11, 2021.
5. Buch A, Kaur S, Nair R, Jain A. Platelet volume indices as predictive biomarkers for diabetic complications in type 2 diabetic patients. J Lab Physicians. 2017;9(2):84–88. doi:10.4103/0974-2727.199625
6. Subramanian S, Green SR, Vaithy A. A prospective observational study of relation between platelet indices and microvascular complications in type 2 diabetic patients in a tertiary care hospital. Int J Recent Sci Res. 2020;11(03):37915–37919.
7. Kodiatte TA, Manikyam UK, Rao SB, et al. Mean platelet volume in type 2 diabetes mellitus. J Lab Physicians. 2012;4(1):5–9. doi:10.4103/0974-2727.98662
8. Ferreiro JL, Gómez-Hospital JA, Angiolillo DJ. Review article: platelet abnormalities in diabetes mellitus. Diabetes Vasc Dis Res. 2010;7(4):251–259. doi:10.1177/1479164110383994
9. Jindal S, Gupta S, Gupta R, et al. Platelet indices in diabetes mellitus: indicators of diabetic microvascular complications. Hematology. 2011;16(2):86–89. doi:10.1179/102453311X12902908412110
10. Dwivedi T, DavangeRi R. Variation of platelet indices among patients with diabetes mellitus attending tertiary care hospital. J Clin Diagn Res. 2018;12:11. doi:10.7860/JCDR/2018/36486.12306
11. Sheleme T, Mamo G, Melaku T, Sahilu T. Prevalence, patterns and predictors of chronic complications of diabetes mellitus at a large referral hospital in Ethiopia: a Prospective Observational Study. Diabetes Metab Syndr Obes. 2020;13:4909. doi:10.2147/DMSO.S281992
12. Barao K, Forones NM. Body mass index: different nutritional status according to WHO, OPAS and lipschitz classifications in gastrointestinal cancer patients. Arq Gastroenterol. 2012;49(2):169–171. doi:10.1590/s0004-28032012000200013
13. World Health Organization. Physical status: the use and interpretation of anthropometry. Report of a WHO expert committee 1995. WHO Technical Report Series. 2017;854. Available from: https://apps.who.int/iris/bitstream/handle/10665/37003/WHO_TRS_854.pdf?sequence=1.
14. Patry-parisien J, Shields M, Bryan S. Comparison of waist circumference using the World Health Organization and National Institutes of Health protocols. Health Rep. 2012;23(3):53–60.
15. Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. J Am Coll Cardiol. 2018;71(19):e127–e248. doi:10.1016/j.jacc.2017.11.006
16. Dindar S, Cinemre H, Sengul E, Annakkaya AN. Mean platelet volume is associated with glycaemic control and retinopathy in patients with type 2 diabetes mellitus. West Indian Med J. 2013;62(6):519–523. doi:10.7727/wimj.2012.284
17. Desai KN, Lakum NR. An Evaluation Study of Platelet Volume Indices (PVI) in type-2 diabetes mellitus and its micro and macro vascular complications. Ann Pathol Lab Med. 2018;5(5):480–483. doi:10.21276/apalm.1846
18. Sushma KL, Rangaswamy M. Study of platelet indices in type 2 diabetic patients and its correlation with vascular complications. Ann Pathol Lab Med. 2017;4(5):591–598. doi:10.21276/APALM.1297
19. Walinjkar RS, Khadse S, Kumar S, Bawankule S, Acharya S. Platelet indices as a predictor of microvascular complications in type 2 diabetes. Indian J Endocrinol Metab. 2019;23(2):206–210. doi:10.4103/ijem.IJEM_13_19
20. Pujani M, Gahlawat H, Agarwal C, Chauhan V, Singh K, Lukhmana S. Platelet parameters: can they serve as biomarkers of glycemic control or development of complications in evaluation of type 2 diabetes mellitus? Iraq J Hematol. 2018;7(2):72–78. doi:10.4103/ijh.ijh_8_18
21. Shilpi K, Potekar RM. A study of platelet indices in type 2 diabetes mellitus patients. Indian J Hematol Blood Transfus. 2018;34(1):115–120. doi:10.1007/s12288-017-0825-9
22. Alhadas KR, Santos SN, Freitas MM, Viana SM, Ribeiro LC, Costa MB. Are platelet indices useful in the evaluation of type 2 diabetic patients? J Bras Patol Med Lab. 2016;52(2):96–102. doi:10.5935/1676-2444.20160017
23. Yenigün EC, Okyay GU, Pirpir A, Hondur A, Yıldırım İS. Increased mean platelet volume in type 2 diabetes mellitus. Dicle Med J/Dicle Tip Dergisi. 2014;41(1):17–22. doi:10.5798/diclemedj.0921.2014.01.0366
24. Nigam P, Singh B, Yadav AS. Assesment of microvascular complications in type 2 diabetes mellitus patients with special reference to Hba1c and platelet indices (mpv). Paripex Indian J Res. 2019;10:8–11. doi:10.36106/paripex
25. Dubey I, Gaur BS, Singh R. A study to find correlation of platelet indices with HbA1c in diabetic patients with absence/presence of vascular complications. Int J Res Med Sci. 2017;5:1042–1047. doi:10.18203/2320-6012.ijrms20170659
26. Li Z, Wang J, Han X, et al. Association of mean platelet volume with incident type 2 diabetes mellitus risk: the Dongfeng-Tongji cohort study. Diabetol Metab Syndr. 2018;10:29. doi:10.1186/s13098-018-0333-6
27. Ji S, Zhang J, Fan X, et al. The relationship between mean platelet volume and diabetic retinopathy: a systematic review and meta-analysis. Diabetol Metab Syndr. 2019;11(1):25. doi:10.1186/s13098-019-0420-3
28. Kakouros N, Rade JJ, Kourliouros A, Resar JR. Platelet function in patients with diabetes mellitus: from a theoretical to a practical perspective. Int J Endocrinol. 2011;2011:742719. doi:10.1155/2011/742719
29. Akinsegun A, Akinola Olusola D, Sarah JO, et al. Mean platelet volume and platelet counts in type 2 diabetes: mellitus on treatment and non-diabetic mellitus controls in Lagos, Nigeria. Pan Afr Med J. 2014;18:42. doi:10.11604/pamj.2014.18.42.3651
30. Saboor M, Ilyas S. Platelets structural, functional and metabolic alterations in diabetes mellitus. Pak J Physiol. 2012;8(2):40–43.
31. Goyal P, Mahajan S, Parmar C. Evaluation of platelet function in subjects with type-2 diabetes mellitus: a case–control study. Natl J Physiol Pharm Pharmacol. 2020;10(8):667–670.
32. Jaman A, Rezwan S, Alam S, Islam R, Husna AU, Sayeed A. Association of mean platelet volume and platelet distribution width with Hba1c. J Endocrinol Diabetes. 2017;4(4):1–6. doi:10.15226/2374-6890/4/4/00183
33. Folli F, Corradi D, Fanti P, et al. The role of oxidative stress in the pathogenesis of type 2 diabetes mellitus micro- and macrovascular complications: avenues for a mechanistic-based therapeutic approach. Curr Diabetes Rev. 2011;7(5):313–324. doi:10.2174/157339911797415585
34. Bui HDT, Jing X, Lu R, et al. Prevalence of and factors related to microvascular complications in patients with type 2 diabetes mellitus in Tianjin, China: a cross-sectional study. Ann Transl Med. 2019;7(14):325. doi:10.21037/atm.2019.06.08
35. Ramanathan RS. Correlation of duration hypertension and glycemic control with microvascular complications of diabetes mellitus at a tertiary care hospital. J Neurol Exp Neural Sci. 2017;4(1):1–4. doi:10.15761/IMM.1000272
36. Rhee SY, Kim YS. The role of advanced glycation end products in diabetic vascular complications. Diabetes Metab J. 2018;42(3):188–195. doi:10.4093/dmj.2017.0105
37. Singh VP, Bali A, Singh N, Jaggi AS. Advanced glycation end products and diabetic complications. Korean J Physiol Pharmacol. 2014;18(1):1–14. doi:10.4196/kjpp.2014.18.1.1
38. Goh S, Cooper ME. Clinical review: the role of advanced glycation end products in progression and complications of diabetes. J Clin Endocrinol Metab. 2008;93(4):1143–1152. doi:10.1210/jc.2007-1817
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.