Back to Journals » Journal of Inflammation Research » Volume 18
Platelet Indices and ApoA1 as Predictive Markers in Neoadjuvant Immunochemotherapy for Locally Advanced Esophageal Squamous Cell Carcinoma: A Retrospective Study
Authors Zeng T ![]() , Liu YC, Wang XH, Yan J, Li SB, Deng D, Xing S
, Liu YC, Wang XH, Yan J, Li SB, Deng D, Xing S
Received 2 October 2025
Accepted for publication 16 November 2025
Published 3 December 2025 Volume 2025:18 Pages 16967—16980
DOI https://doi.org/10.2147/JIR.S567945
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Junhao Wang
Tao Zeng,1,2,* Yue-chang Liu,1,2,* Xiang-hui Wang,1,2,* Jun Yan,3 Shi-bing Li,1,2 Danning Deng,1,2 Shan Xing4
1Department of Clinical Laboratory, The Sixth Affiliated Hospital, Sun Yat-Sen University, Guangzhou, 510655, People’s Republic of China; 2Biomedical Innovation Center, The Sixth Affiliated Hospital, Sun Yat-sen University, Guangzhou, 510655, People’s Republic of China; 3Department of Clinical Laboratory, Guangdong Medical University, Zhanjiang, 524023, People’s Republic of China; 4Department of Clinical Laboratory, State Key Laboratory of Oncology in South China, Guangdong Provincial Clinical Research Center for Cancer, Sun Yat-Sen University Cancer Center, Guangzhou, 510060, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Danning Deng, Department of Clinical Laboratory, the Sixth Affiliated Hospital, Sun Yat-sen University, No. 26 Erheng Road of Yuancun, Tianhe District, Guangzhou, 510655, People’s Republic of China, Email [email protected] Shan Xing, Department of Clinical Laboratory, State Key Laboratory of Oncology in South China, Guangdong Provincial Clinical Research Center for Cancer, Sun Yat-Sen University Cancer Center, 651 Dongfeng East Road, Guangzhou, 510060, People’s Republic of China, Email [email protected]
Purpose: To evaluate the predictive value of baseline and preoperative blood parameters for treatment efficacy and prognosis in patients with locally advanced esophageal squamous cell carcinoma (LA-ESCC) undergoing neoadjuvant chemoimmunotherapy (nCIT) followed by radical surgery.
Patients and Methods: This retrospective study analyzed clinical data from patients with LA-ESCC patients treated with nCIT followed by surgery (October 2019-November 2024). Patients were categorized based on pathological response (pathological complete response [pCR] and major pathological response [MPR]). Univariate and multivariate analyses identified factors associated with pCR and MPR. Cox regression and Kaplan-Meier methods were used to evaluate overall survival (OS) and disease-free survival (DFS). Nomograms and Receiver Operating Characteristic (ROC) curves were created for prognostic prediction.
Results: Among 236 patients, the pCR rate was 31.8%, and the MPR rate was 51.7%. pCR was associated with improved DFS (Hazard Ratio [HR] = 0.27, 95% CI: 0.16– 0.43, p < 0.0001) but not OS (p = 0.058). MPR was significantly correlated with both DFS (HR=0.27, 95% CI: 0.17– 0.44, p < 0.0001) and OS (HR=0.38, 95% CI: 0.21– 0.71, p = 0.0023). Identified predictors of treatment response included baseline and preoperative platelet indices (mean platelet volume [MPV], platelet distribution width [PDW], platelet-large cell ratio [P-LCR]) for both pCR and MPR, along with preoperative Apolipoprotein A1 (ApoA1) specifically for MPR (all identified as independent predictors on univariate and multivariate analysis, p < 0.05), reflecting their role in modulating the inflammatory response. A predictive model combining MPV (HR = 0.86, 95% CI: 0.61– 1.22) and ApoA1 (HR = 0.24, 95% CI: 0.07– 0.81) demonstrated good accuracy in forecasting DFS (30 months: AUC = 0.71, 95% CI: 0.60– 0.81).
Conclusion: Baseline and preoperative blood parameters (MPV, PDW, P-LCR) and preoperative ApoA1 are valuable predictors of treatment response and prognosis in LA-ESCC. Nomograms incorporating these markers offer reliable prognostic insights for DFS.
Keywords: esophageal squamous cell carcinoma, neoadjuvant therapy, pathological complete response, prognosis, inflammation, biomarkers
Introduction
Esophageal cancer is a prevalent and aggressive malignancy of the upper gastrointestinal tract.1 Globally, it ranks as the 11th most prevalent cancer and the seventh leading cause of cancer-related death, with an estimated 510,716 new cases and approximately 445,129 deaths in 2022.2 In China, esophageal cancer ranks seventh in incidence and fifth in mortality among all malignant tumors.3 Histologically, esophageal squamous cell carcinoma (ESCC) is the most common subtype, accounting for over 90% of cases.4,5 Neoadjuvant chemoradiotherapy combined with surgery has been established as the standard treatment for locally advanced esophageal cancer, based on landmark studies such as CROSS and NEOCRTEC5010.6–8
In recent years, clinical trials including KEYNOTE-181, KEYNOTE-590, and ESCORT-1st have confirmed that immunotherapy combined with chemotherapy serves as a first-line treatment for metastatic esophageal cancer, significantly improving overall survival (OS) and progression-free survival (PFS).9,10 More recently, the ESCORT-NEO trial in 2024 evaluated the efficacy of neoadjuvant immunotherapy (nICT) combined with chemotherapy in resectable locally advanced esophageal squamous cell carcinoma (LA-ESCC). This trial demonstrated a substantial increase in the pathological complete response (pCR) rate (28%) and major pathological response (MPR) rate (59.1%), indicating promising potential for improving patient outcomes.11
However, not all patients with esophageal cancer benefit from immunotherapy. Clinically validated biomarkers for ESCC include programmed death-ligand 1 (PD-L1) expression, tumor mutational burden (TMB), microsatellite instability-high (MSI-H) or mismatch repair deficiency (dMMR), and nutritional status.12 In addition, emerging biomarkers such as gene mutation profiles, gut microbiota composition, and peripheral blood markers have shown potential predictive value.13,14 As nearly one-third of LA-ESCC patients exhibit limited radiologic response to nICT, radiologic staging alone is insufficient to predict pCR.15 Even among biomarker-selected patients, the predictive accuracy of existing clinicopathologic factors remains limited. For example, in the ESCORT-1st study, more than 27% of PD-L1 positive (CPS ≥10) patients showed no objective response to immunochemotherapy, while in the KEYNOTE-181 trial, up to 65% of TMB-high patients failed to respond to immunotherapy.9,10 Additionally, MSI-H/dMMR and TMB-H are rarely present in esophageal cancer.12,16 These findings underscore the current accuracy limits of clinicopathologic predictors and highlight the unmet need for reliable pretreatment biomarkers.12–15 Previous studies have demonstrated that platelets express PD-L1 and can upregulate PD-L1 expression on tumor cells, thereby inducing exhaustion of cytotoxic CD8⁺ T cells.17 In addition, platelet-derived proteins such as ADAM10, ADAM17, and TGF-β suppress natural killer (NK) cell activity, suggesting that platelet-related parameters may serve as accessible and biologically relevant biomarkers of immunotherapy response.18 Furthermore, lipid accumulation within the tumor microenvironment drives metabolic reprogramming of myeloid-derived suppressor cells (MDSCs) from glycolysis to fatty acid oxidation (FAO), enhancing their immunosuppressive function.19 Given these mechanisms, circulating markers such as platelet indices and lipid indicators may reflect the host’s immune and metabolic status. By using conventional blood indicators, which are easily accessible and low-cost, rapid assessment can be conducted before surgery.20
This study integrates data from the entire hospital focusing on patients with LA-ESCC who underwent surgical resection following nICT. The aim is to evaluate the predictive value of baseline and preoperative blood-based biomarkers for treatment response and survival in patients with LA-ESCC receiving nICT.
Materials and Methods
Patients
All patients were consecutively enrolled from the Department of Thoracic Surgery at Sun Yat-sen University Cancer Center (Guangzhou, China). This was a single-center, retrospective study. Between October 2019 and November 2024, a total of 305 patient records were initially reviewed. After applying predefined inclusion and exclusion criteria, data from 236 patients with locally advanced esophageal squamous cell carcinoma (LA-ESCC) who underwent neoadjuvant chemoimmunotherapy (nCIT) followed by radical surgery were analyzed. Clinical characteristics, preoperative blood parameters, and follow-up data (with follow-up completed on July 31, 2025) were retrospectively extracted from patient records (CONSORT flowchart, see Figure S1).
Inclusion Criteria
- Patients with pre-treatment clinical staging according to the 8th edition of the AJCC/UICC staging system, specifically T1b-4aN1-3M0 or T2-4aN0M0 resectable ESCC, with pathological diagnosis as the gold standard.21
- Patients who had not received any prior anti-tumor treatment.
- Age ≥18 years, regardless of gender.
- Performance Status (PS) score of 0–1.22
Exclusion Criteria
- Patients who had previously received anti-tumor treatment (including chemotherapy, radiotherapy, surgery, immunotherapy, etc).
- Patients who received radiotherapy combined with immunotherapy.
- Patients with distant organ metastases.
- Patients who did not undergo surgery or lacked surgical pathological results.
- Patients with a history of malignant tumors other than esophageal cancer.
- Patients with incomplete clinical data or follow-up information.
Immunotherapy Drugs
The following immunotherapy drugs were used: camrelizumab, sintilimab, toripalimab, tislelizumab, and pembrolizumab.
Immunotherapy Efficacy Assessment
The pathological outcomes of nCIT were evaluated by two experienced pathologists, using resected tissue specimens. Pathological complete response (pCR) was defined as the absence of residual cancer cells in the tumor specimen and lymph nodes. Major pathological response (MPR) was defined as ≤10% viable tumor cells remaining in the surgically resected specimen. Tumor regression grade (TRG) was used as follows: Grade 0: No residual cancer cells (pCR); Grade 1: ≤10% viable tumor cells; Grade 2: 10–50% viable tumor cells; Grade 3: >50% viable tumor cells. TRG 0–1 was considered achieving MPR, while TRG 2–3 was considered not achieving MPR.23
Follow-Up
The follow-up cutoff date was July 31, 2025. The median follow-up duration was 25.5 months. Disease-free survival (DFS) was defined as the time from the initiation of immunotherapy to confirmed progressive disease or cancer-related death. Overall survival (OS) was defined as the time from the initiation of treatment to death from any cause.24
Methods
General Clinical Information
The following clinical parameters were collected: gender, age, body mass index (BMI), smoking history, alcohol consumption history, and family history of cancer.
Tumor Information
Data collected included tumor location, degree of differentiation, T stage, N stage, clinical TNM stage, and information on the treatment drugs used.
Hematological Indicators
A total of 114 hematological indicators were collected at baseline and prior to surgery following nCIT. These included data from blood cell analysis, biochemical and tumor marker tests, coagulation parameters, inflammation-related markers (eg, C-reactive protein [CRP], serum amyloid A [SAA]), and derived metrics (eg, neutrophil-to-lymphocyte ratio [NLR], derived NLR [dNLR], systemic immune-inflammation index [SII], etc). Peripheral venous blood samples were collected at baseline (within 1 week prior to neoadjuvant therapy) and preoperatively (1–3 days before surgery). The interval between the last neoadjuvant cycle and surgery followed current Chinese clinical practice (4–6 weeks).11 Complete blood count parameters were measured using Sysmex XN-9000 analyzers; serum biochemical parameters were measured using the Roche cobas 8000 series (module c702); and tumor markers were measured using the Roche cobas 8000 series (module e801).
Statistical Analysis
Data analysis was performed using R software (version 4.5.0) and Python (version 3.11.4). Univariate analyses were conducted using the Chi-square test or Fisher’s exact test for qualitative data. Normally distributed continuous data were compared using the t-test, while non-normally distributed data were analyzed with non-parametric tests. Multivariate analysis was conducted using logistic regression. OS and DFS were assessed using univariate and multivariate Cox regression models. Kaplan-Meier curves were generated, and survival differences between groups were compared using the log-rank test. A p-value of less than 0.05 was considered statistically significant. Optimal cut-off values for continuous hematologic parameters were defined using ROC curves based on the Youden index for pCR prediction (“pROC” package), and were determined with the “survival” and “survminer” packages for survival outcomes. Multicollinearity was evaluated by Spearman correlation with Bonferroni correction and VIF calculation (“corrplot” and “car” packages).
Results
Patient Characteristics
A total of 236 patients with LA-ESCC who received nICT were included in this study. The baseline characteristics of the patients are summarized in Table 1. The median age of the participants was 60 years (interquartile range [IQR], 39–76 years); 198 patients (83.9%) were male, and 38 patients (16.1%) were female. Clinical staging was as follows: stage II in 37 cases (15.7%), stage III in 172 cases (72.9%), stage IVA in 25 cases (10.6%), and 2 cases (0.8%) with indeterminate staging between stage II and III. Tumor location was classified as upper esophagus in 13 cases (5.5%), middle esophagus in 123 cases (52.1%), and lower esophagus in 100 cases (42.4%).
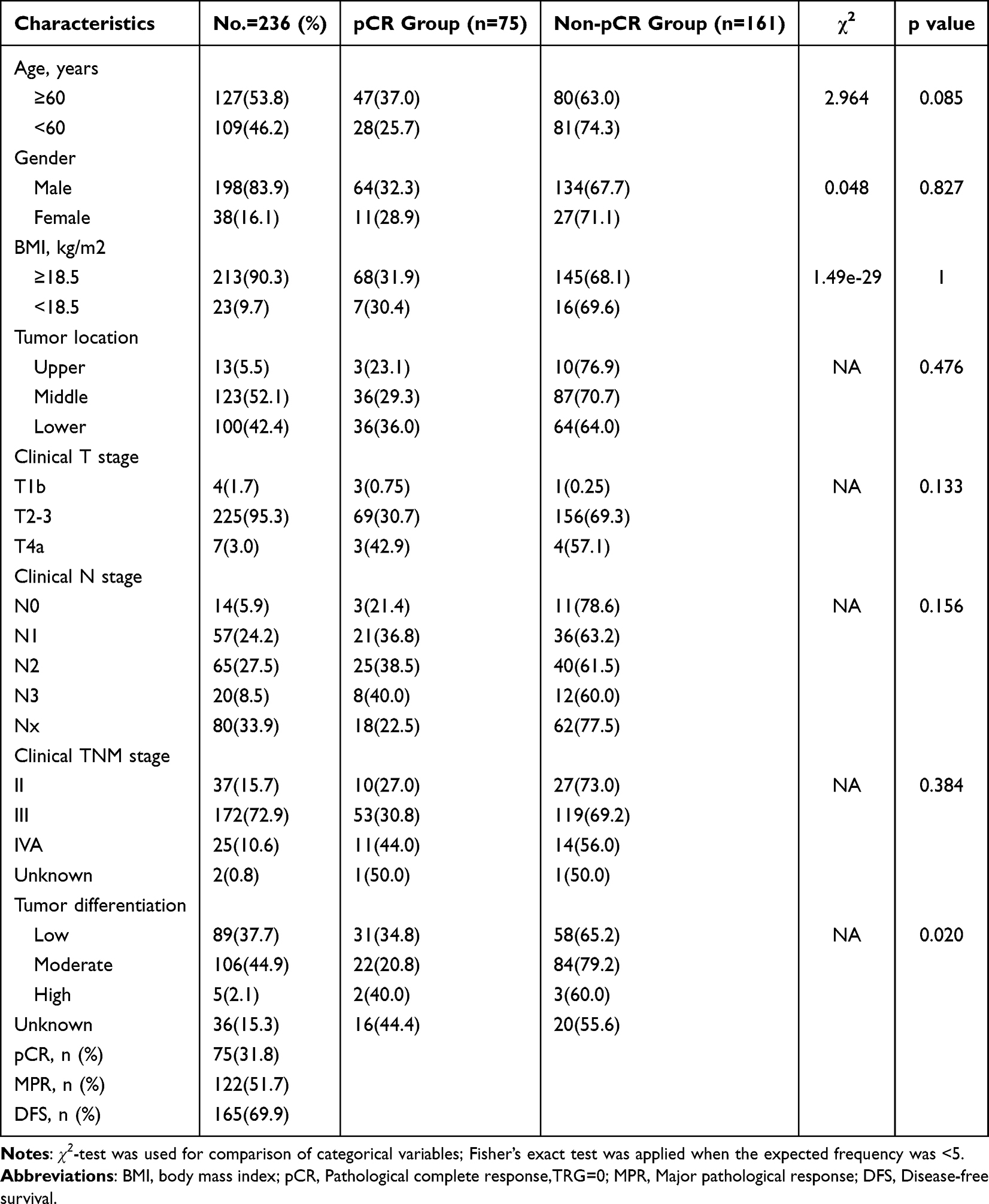 |
Table 1 Baseline Demographics and Clinical Information |
Postoperative pathology revealed that 75 patients (31.8%) achieved pCR and 161 patients (68.2%) were non-pCR, while 122 patients (51.7%) achieved MPR and 114 patients (48.3%) were non-MPR. Tumor differentiation was categorized as low in 89 cases (37.7%), moderate in 106 cases (44.9%), high in 5 cases (2.1%), and unknown in 36 cases (15.3%).
Clinical follow-up data showed a median follow-up duration of 25.5 months (95% confidence interval [CI], 23.2–27.2 months), with a maximum follow-up time of 68.9 months. The median OS and DFS had not yet been reached. The 1-year and 2-year OS rates were 95.6% (95% CI: 93.0–98.3) and 86.7% (95% CI: 82.1–91.6), respectively (Figure 1A). The 1-year and 2-year DFS rates were 86.5% (95% CI: 82.2–91.1) and 71.7% (95% CI: 65.8–78.1), respectively (Figure 1B).
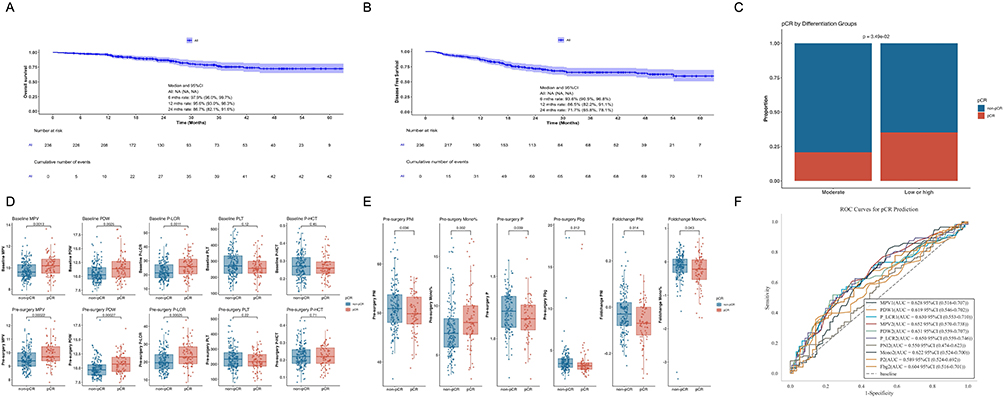 |
Figure 1 Survival curves and comparison of pCR across different indicators. (A) Kaplan-Meier curves of OS for patients who received immunochemotherapy followed by surgery (n=236). (B) Kaplan-Meier curves of DFS for patients who received immunochemotherapy followed by surgery (n=236). (C) Stacked bar chart of pCR rates according to different tumor differentiation levels (n=200). (D) Box plots of platelet counts and related parameters among different pCR groups (n=236). (E) Box plots of other significantly different indicators among different pCR groups (n=154). (F) ROC curves for predictors of pCR identified in univariate analysis (n=154), 1 indicates baseline levels, and 2 indicates preoperative levels. |
Univariate and Multivariate Analysis of Predictors for pCR
A significant association was observed between tumor differentiation and pCR rate (Table 2). When using the low differentiated group as a reference, the moderately differentiation group showed a significantly reduced odds of pCR (Odds Ratio [OR] = 0.49, 95% CI: 0.26–0.93, p < 0.05). As shown in Figure 1C, patients with moderately differentiated tumors were less likely to achieve pCR compared to those with high or low differentiation (20.8% vs 35.1%, χ2=4.45, p < 0.05). We observed significant differences in three baseline platelet parameters (n=236, Univariate analysis). These are mean platelet volume (MPV, OR = 1.65, 95% CI: 1.21–2.25, p = 0.002), platelet distribution width (PDW, OR = 1.27, 95% CI: 1.10–1.46, p = 0.001), and platelet-large cell ratio (P-LCR, OR = 1.07, 95% CI: 1.03–1.11, p = 0.001). Notably, similar significant differences in MPV (OR = 1.84, 95% CI: 1.29–2.63, p = 0.001), PDW (OR = 1.36, 95% CI: 1.14–1.62, p = 0.001), and P-LCR (OR = 1.08, 95% CI: 1.04–1.13, p < 0.001) were found when comparing preoperative data following nICT, with these differences being even more pronounced (higher ORs and smaller p-values, n=235). However, no significant differences were observed in platelet count (PLT) or platelet hematocrit (P-HCT) (Figure 1D).
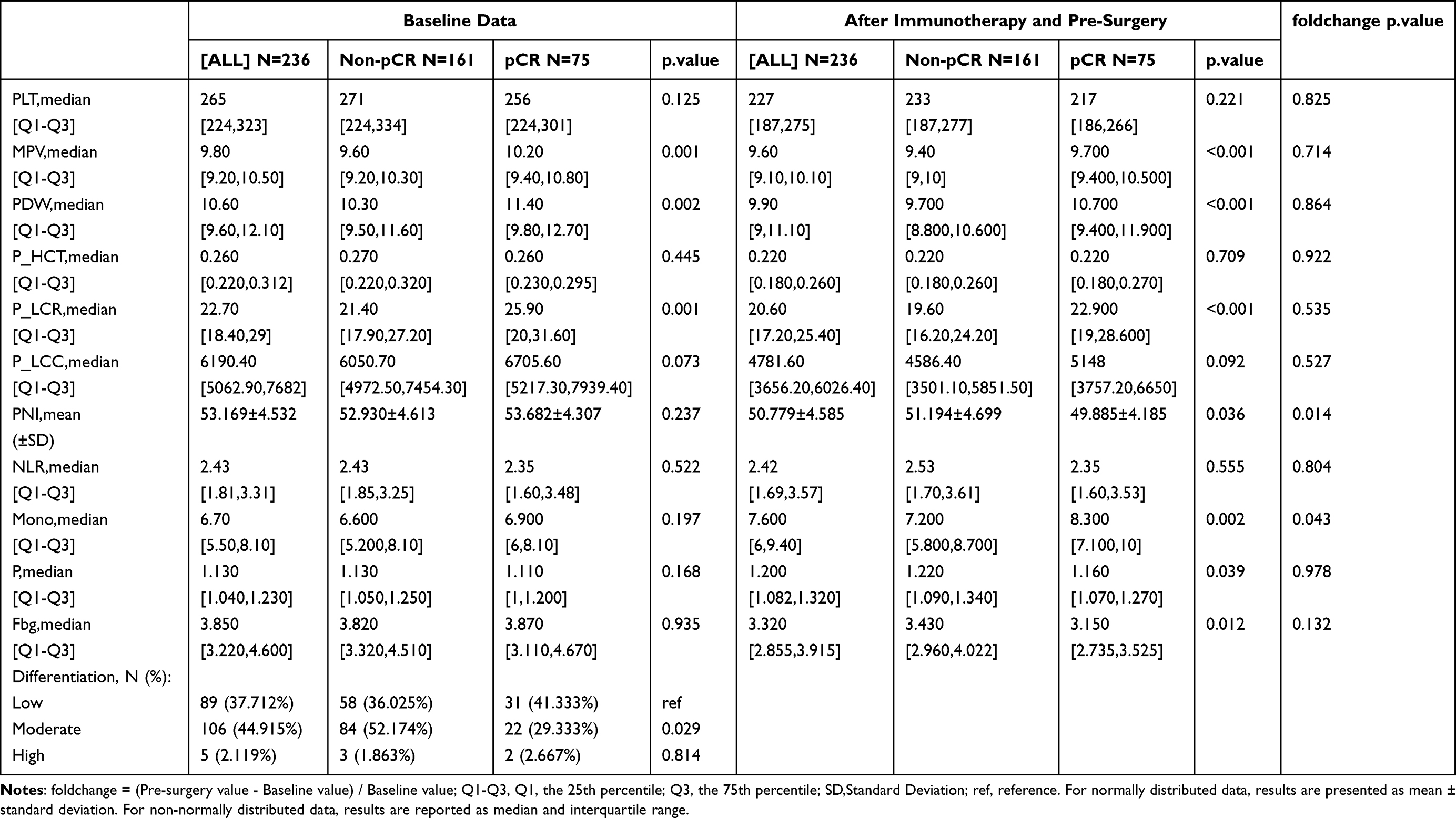 |
Table 2 Dynamic Changes in Blood Test Results: From Baseline to Pre-Surgery |
Analysis of all hematological indicators showed that preoperative prognostic nutritional index (PNI, p = 0.036), monocyte percentage (Mono%, p = 0.002), phosphorus (P, p = 0.039), and fibrinogen (Fbg, p = 0.012) differed significantly between groups (Figure 1E), although the differences were less marked than those observed for platelet-related parameters. When analyzing the change in values between preoperative and baseline data, only PNI (p = 0.014) and Mono% (p = 0.043) showed significant differences.
Multivariate logistic regression analysis including age, sex demonstrated that both baseline and preoperative MPV, PDW, and P-LCR were independent predictors of pCR and MPR (all p < 0.05). The baseline values of MPV (OR = 1.64, 95% CI: 1.20–2.24, p = 0.002), PDW (OR = 1.27, 95% CI: 1.10–1.47, p = 0.001), and P-LCR (OR = 1.07, 95% CI: 1.03–1.11, p = 0.001) were independent predictors of pCR. Similarly, the preoperative values of these platelet parameters also showed significant independent associations with pCR, with further strengthened effect sizes after nICT (MPV: OR = 1.84, 95% CI: 1.29–2.63; PDW: OR = 1.35, 95% CI: 1.14–1.61; P-LCR: OR = 1.08, 95% CI: 1.03–1.13; all p < 0.001). ROC curve analysis revealed that preoperative MPV, PDW, and P-LCR showed higher AUC values for predicting pCR (AUC of MPV = 0.65, 95% CI: 0.57–0.74, cutoff = 9.70, Figure 1F). These three platelet-related variables were highly correlated, with preoperative MPV showing a strong correlation with P-LCR and PDW (all Spearman’ r > 0.9, p < 0.001), preventing the construction of a combined multivariate prediction model.
Survival Outcomes and Impact of pCR
Kaplan-Meier (KM) curves, log-rank tests, and Cox regression analyses were employed to evaluate survival outcomes. Although the median OS and DFS have not yet been reached due to the excellent efficacy of nICT, we explored whether achieving pCR influences short-term and long-term survival (n=236). The KM curves demonstrated a significant difference in DFS between the pCR and non-pCR groups (Hazard Ratio [HR] = 0.27, 95% CI: 0.16–0.43, log-rank p < 0.0001), as shown in Figure 2A. However, the difference in OS was not statistically significant (HR=0.50, 95% CI: 0.26–0.94, log-rank p = 0.058) (Figure 2B). These results suggest that achieving pCR after nICT is primarily associated with improved short-term survival, with a more limited impact on long-term survival.
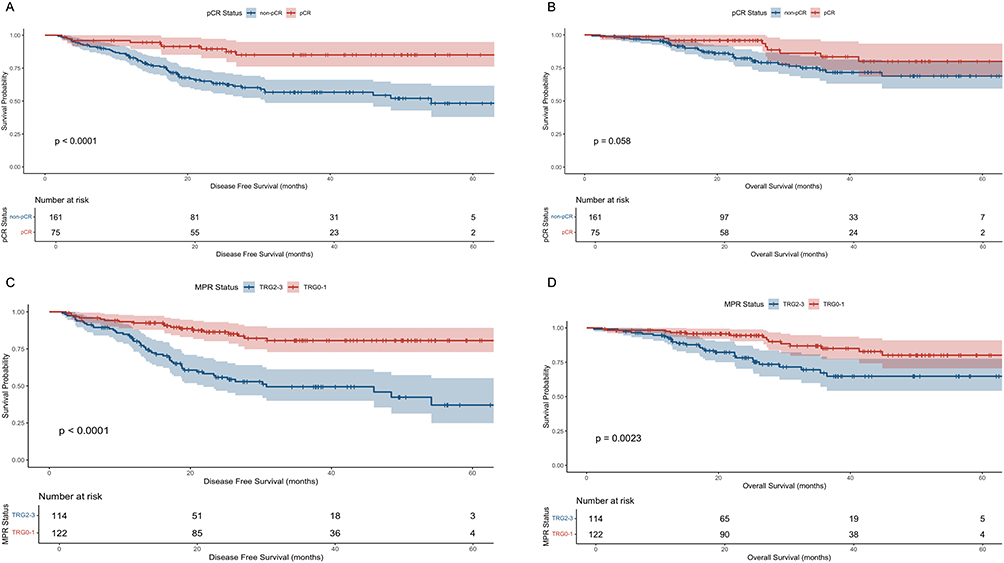 |
Figure 2 Kaplan-Meier survival curves of DFS and OS stratified by pCR and MPR status. (A) Kaplan-Meier curves for DFS in patients stratified by pCR status (n=236). (B) Kaplan-Meier curves for OS in patients stratified by pCR status (n=236). (C) Kaplan-Meier curves for DFS in patients stratified by MPR status (n=236). (D) Kaplan-Meier curves for OS in patients stratified by MPR status (n=236). |
Stratified Survival Analysis and Multivariate Cox Regression
Stratified survival analysis and multivariate Cox regression were performed to evaluate the influence of various predictors on OS and DFS. Univariate Cox regression analyses revealed that indicators such as MPV, PDW, and P-LCR did not significantly impact OS or DFS (all p > 0.05). Consequently, subgroup survival comparisons based on these factors were not feasible. Similarly, other variables previously associated with pCR, including PNI, Mono%, P, and Fbg, also showed no significant association with OS or DFS (all p > 0.05).
Impact of MPR on Survival Outcomes
We further evaluated whether achieving MPR could improve both short-term and long-term survival outcomes (n=236). Kaplan-Meier curve analysis revealed a significant difference in DFS between patients with TRG 0–1 and TRG 2–3 (HR=0.27, 95% CI: 0.17–0.44, log-rank p < 0.0001). Notably, OS was also significantly improved in the TRG 0–1 group compared to the TRG 2–3 group (HR=0.38, 95% CI: 0.21–0.71, log-rank p = 0.0023), as shown in Figure 2C and D. These findings suggest that achieving MPR is associated with favorable short- and long-term survival outcomes. In contrast to pCR, MPR appears to be a more suitable predictor of nICT efficacy and survival benefit. In other words, a TRG score of 1 indicates a survival benefit from immunotherapy, even in the absence of complete tumor eradication.
Univariate logistic regression analysis demonstrated that preoperative MPV (OR = 1.62, 95% CI: 1.15–2.26, p = 0.005), PDW (OR = 1.31, 95% CI: 1.10–1.55, p = 0.003), and P-LCR (OR = 1.07, 95% CI: 1.02–1.11, p = 0.003) differed significantly between MPR groups (n=235). Additionally, preoperative apolipoprotein A1 (ApoA1, OR = 4.19, 95% CI: 1.14–15.39, p = 0.031) levels were significantly different between MPR groups (n = 169). Multivariate logistic regression analyses demonstrated that preoperative MPV (OR = 1.71, 95% CI: 1.14–2.57, p = 0.01), PDW (OR = 1.35, 95% CI: 1.09–1.68, p = 0.006), and P-LCR (OR = 1.07, 95% CI: 1.02–1.13, p = 0.007) were independent predictors of MPR. Univariate Cox regression analysis for DFS showed that preoperative ApoA1 was significantly associated with DFS (HR=0.23, 95% CI: 0.07–0.78, log-rank p = 0.018), whereas baseline ApoA1 levels were not (p > 0.05, Figure 3A and B).
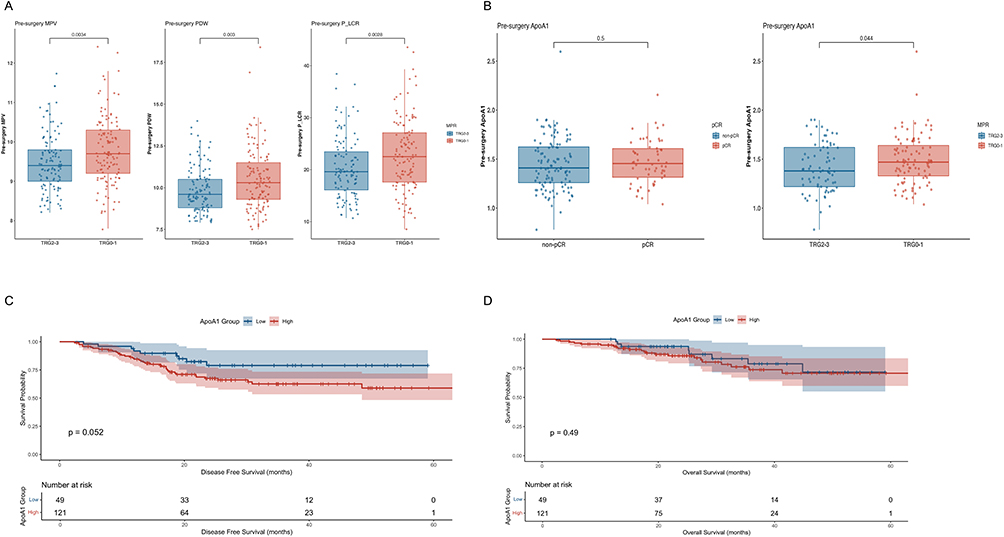 |
Figure 3 Comparative analysis among MPR subgroups and survival curves by ApoA1 levels. (A) Boxplots of platelet-related parameters across different MPR subgroups (n=235). (B) Boxplots of ApoA1 levels in patients stratified by pCR and MPR status (n=169). (C) Kaplan-Meier curves for DFS in patients stratified by ApoA1 levels (cutoff = 1.4, n=169). (D) Kaplan-Meier curves for OS in patients stratified by ApoA1 levels (cutoff = 1.4, n=169). |
Although the median survival for OS and DFS was not reached, survival analysis for MPV, PDW, and P-LCR revealed no statistically significant differences (all p > 0.05). While the log-rank test for DFS and ApoA1 approached significance (ApoA1 cutoff = 1.4 mmol/L, log-rank p = 0.052), KM analyses for OS did not show a significant association for ApoA1 (p > 0.05, Figure 3C and D).
Cox Regression and Predictive Model for DFS
We employed a Cox proportional hazards model with the “all” method for multivariable adjustment to assess the impact of preoperative MPV combined with ApoA1 on DFS (n=169). The results indicated that ApoA1 remained a significant predictor of DFS (HR = 0.24, 95% CI: 0.07–0.81, p=0.021), whereas MPV did not show significance (HR = 0.86, 95% CI: 0.61–1.22, p = 0.4, Figure 4A). Our model demonstrated a moderate predictive performance with a C-index of 0.622 (95% CI: 0.548–0.697).
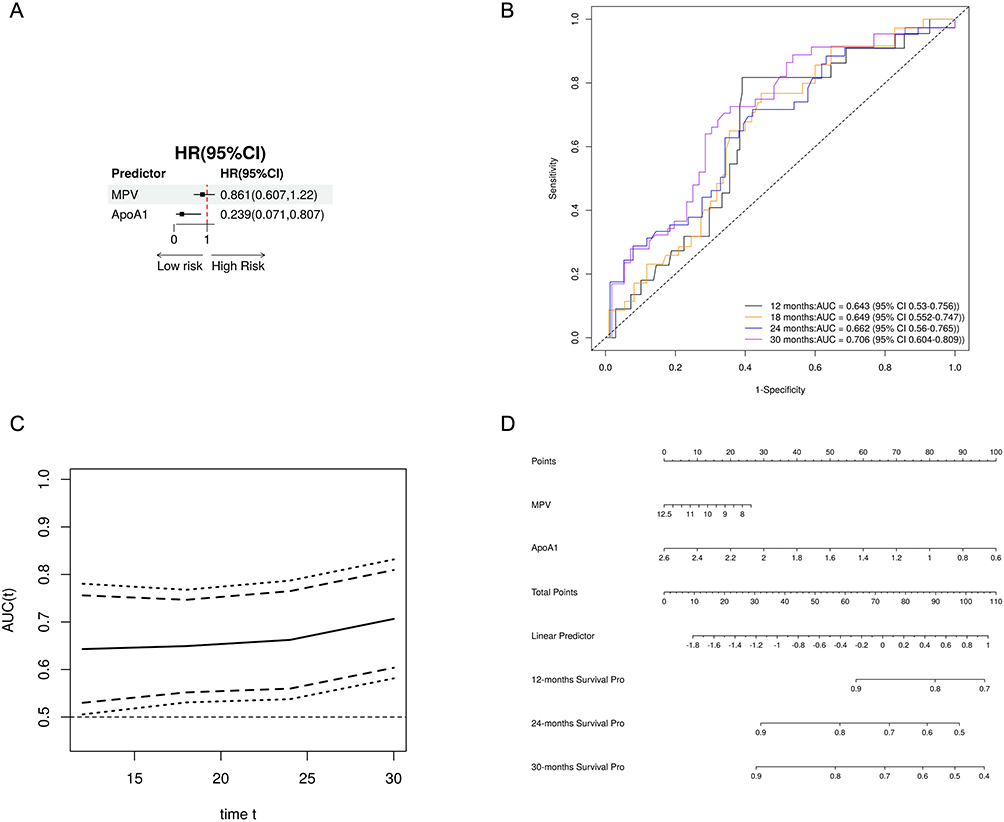 |
Figure 4 Prognostic value of preoperative MPV combined with ApoA1 for DFS. (A) Forest plot illustrating the prognostic value of preoperative MPV combined with ApoA1 for DFS (n=169). (B) Time-dependent ROC curves for DFS prediction using preoperative MPV combined with ApoA1 (n=169). (C) Continuous time-dependent ROC curves for DFS prediction using preoperative MPV combined with ApoA1 (n=169). (D) Nomogram for predicting DFS based on preoperative MPV combined with ApoA1 (n=169). |
The model’s Wald test, log-rank test, and likelihood ratio test all yielded p-values < 0.05, confirming the model’s robustness. The predictive performance for DFS at 12, 18, 24, and 30 months demonstrated AUC values of 0.643 (95% CI: 0.53–0.756), 0.649 (95% CI: 0.552–0.747), 0.662 (95% CI: 0.56–0.765), and 0.706 (95% CI: 0.604–0.809), respectively (Figure 4B and 4C). Additionally, we constructed nomograms to predict 12-, 24-, and 30-month DFS, which may facilitate clinical prediction of DFS in patients with LA-ESCC (Figure 4D). Calibration curves and decision curve analyses are shown in Figure S2 and Figure S3, respectively.
Discussion
This study aimed to investigate the blood parameters that influence the therapeutic efficacy and prognosis of nCIT in LA-ESCC. Through a retrospective analysis of routinely assessed hematological indices, clinical data, pathological findings, and prognostic outcomes from stage II/III ESCC patients treated at our institution, we identified important predictive biomarkers.
Our multivariate analyses revealed that both baseline and preoperative MPV, PDW, and P-LCR were independent predictors of pCR, with preoperative values showing even more pronounced differences (all p < 0.001). These findings suggest that platelet-related parameters may serve as useful indicators of treatment response in LA-ESCC patients undergoing nCIT. Furthermore, preoperative MPV, PDW, P-LCR, and ApoA1 exhibited significant differences across MPR groups (all p < 0.05). Notably, preoperative ApoA1 was independently associated with DFS in both univariate and multivariate Cox regression analyses (all p < 0.05).
A predictive model combining preoperative MPV and ApoA1 demonstrated promising performance in predicting DFS, with AUC values for 12, 18, 24, and 30 months of 0.643 (95% CI: 0.53–0.756), 0.649 (95% CI: 0.552–0.747), 0.662 (95% CI: 0.56–0.765), and 0.706 (95% CI: 0.604–0.809), respectively. These results underscore the potential clinical utility of combining these readily available hematological markers to predict patient outcomes and personalize treatment strategies for LA-ESCC.
In our cohort, pCR was associated with improved DFS (p < 0.0001) but showed no significant impact on OS (p = 0.058). In comparison, MPR was significantly associated with both better DFS (p < 0.0001) and OS (p = 0.0023). This discrepancy may be attributed to the fact that the median OS and DFS have not yet been reached, coupled with a relatively short median follow-up of 25.5 months. Although OS remains the gold standard endpoint for assessing clinical benefit in cancer therapeutics, recent evidence from nCIT in lung cancer has shown superior 5-year survival rates for patients achieving pCR compared to those without (95.3% vs 55.7%) with a median follow-up of 68.4 months.25 The median OS and DFS were not reached, limiting the analysis of long-term survival outcomes. The conclusion regarding the impact of pCR on OS may therefore be premature. However, long-term OS data for nCIT in ESCC remain unavailable.
One study cautioned against using pCR as a surrogate for OS in resectable ESCC, while another suggested recurrence-free survival (RFS) could serve as a more appropriate surrogate for OS to expedite clinical trial timelines in ESCC.26,27 The Keystone-001 trial evaluated preoperative nCIT for LA-ESCC, The trial chose MPR as the primary endpoint instead of pCR. This choice was based on evidence that MPR in resected specimens may better predict long-term survival.24,28
Our observed pCR and MPR rates were 31.8% and 51.7%, respectively, slightly lower than those reported in the Keystone-001 trial (41% and 72%).24 In comparison, our 1-year OS rate was modestly higher (95.6% vs 91.3%), while the 2-year OS rate was lower (86.7% vs 91.3%). These differences may be attributed to variations in sample size (n = 236 vs n = 46) or treatment regimens (multi-drug versus pembrolizumab). Given these discrepancies, determining the optimal surrogate endpoint for long-term survival in nCIT-treated ESCC will require extended follow-up in larger patient cohorts.
Our findings further suggest that elevated levels of MPV, PDW, and P-LCR are associated with a higher likelihood of achieving pCR and MPR following nCIT. Specifically, a increase in MPV reflects larger platelet volumes in peripheral blood, which likely indicates the presence of freshly released, immature, or activated platelets.29–32 Similarly, an elevated PDW signifies increased heterogeneity in platelet size, indicative of a higher proportion of activated platelets. An increase in P-LCR means more platelets are larger than the normal volume threshold, which is usually greater than 12 fL. This increase is also a marker for freshly activated or reactive platelets. The platelet indices MPV, PDW, and P-LCR together show systemic platelet activation. Platelet activation is commonly seen in inflammation, thrombosis, tumor growth, and cardiovascular diseases. Although MPV, PDW, and P-LCR were associated with treatment response (pCR/MPR), their direct correlation with OS or DFS was not significant. This may be because pathological response serves as a stronger surrogate endpoint for long-term survival, overshadowing the effect of baseline hematologic parameters. These markers may therefore influence survival indirectly through their impact on treatment response. In addition, the short follow-up and limited survival events might have reduced the statistical power to detect their prognostic value.
ApoA1, the principal protein component of high-density lipoprotein (HDL), is crucial in lipid metabolism, modulation of inflammation, and immune response regulation.33 Previous studies have shown that serum ApoA1 levels are significantly reduced in ESCC patients compared to healthy controls, with low levels of ApoA1 correlating strongly with poor prognosis and serving as an independent predictor of adverse OS.34–36 In our study, preoperative ApoA1 levels had a significant effect on DFS. Lower preoperative ApoA1 levels were linked to better DFS outcomes. However, this counterintuitive result may be explained by metabolic and immune interactions. Hypercholesterolemia, often accompanied by reduced ApoA1 levels, has been associated with better outcomes in patients receiving immunotherapy.37 It may reflect a pro-inflammatory state that enhances tumor immunogenicity and responsiveness to immunotherapy. Moreover, cholesterol and mature HDL particles can modulate the tumor immune microenvironment by promoting M1-like macrophages and activated CD8⁺ T cells, thereby improving antitumor immunity.35,38
Despite the valuable insights provided by our study, several limitations warrant consideration. Firstly, this was a retrospective, single-center study with a relatively modest sample size, which may limit the generalizability of the results. The follow-up duration was not yet sufficient to reach the median OS or DFS, restricting the interpretation of long-term outcomes. Additionally, treatment regimens were not fully homogeneous, introducing potential confounding effects. Commonly utilized biomarkers, such as PD-L1 expression, were not included in the current analysis, and external validation cohorts were unavailable, which may reduce the robustness of the findings.
Nevertheless, our study retains several strengths, including consecutive patient enrollment and the systematic, protocol-driven approach to extracting laboratory data from the clinical database, which support the consistency and reliability of the results. In future studies, we aim to include larger cohorts of patients with LA-ESCC, integrate a wider range of biomarkers (eg, PD-L1, cytokines), and conduct multicenter validation with longer follow-up periods to further confirm and broaden the applicability of our conclusions.39 Furthermore, mechanistic investigations will be essential to explore the role of platelets in modulating the tumor microenvironment in ESCC, specifically their interactions with tumor cells, T lymphocytes, and other immune effector cells.
Conclusion
Baseline and preoperative MPV, PDW, and P-LCR serve as valuable predictors of response and prognosis to nCIT in LA-ESCC. Nomograms integrating these with preoperative ApoA1 show promising performance in prognosticating DFS, offering clinical utility.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethics Statement
The study was conducted in accordance with the ethical standards outlined in the Declaration of Helsinki and received ethical approval from the Ethics Committee of Sun Yat-sen University Cancer Center of Sun Yat-sen University (Approval Number: B2025-394-01). Given the retrospective design, the Ethics Committee granted a waiver of informed consent after thoroughly reviewing the study protocol and confirming that the criteria for exemption were met. Patient privacy was strictly protected, and data confidentiality was fully maintained.
Acknowledgments
We thank all colleagues in the Department of Clinical Laboratory, The Sixth Affiliated Hospital and Sun Yat-sen University Cancer Center of Sun Yat-sen University.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Tao Zeng, Yue-chang Liu, Xiang-hui Wang: Conceptualization, Data curation, Formal analysis, Project administration, Visualization, Writing – original draft. Jun Yan: Data curation, Formal analysis, Project administration, Writing – review and editing; Shi-bing Li: Conceptualization, Formal analysis, Project administration, Funding acquisition, Writing – review and editing; Danning Deng, Shan Xing: Conceptualization, Formal analysis, Project administration, Visualization, Funding acquisition, Writing – review and editing.
Funding
Supported by the program of Guangdong Provincial Clinical Research Center for Digestive Diseases (2020B1111170004), Guangdong Esophageal Cancer Institute Science and Technology Program (Q202404), National Natural Science Foundation of China (82203259), Natural Science Foundation of Guangdong Province (2023A1515010398 and 2024A1515013021) and Science and Technology Projects in Guangzhou (2023A04J2246).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Siegel RL, Kratzer TB, Giaquinto AN, Sung H, Jemal A. Cancer statistics, 2025. CA Cancer J Clin. 2025;75(1):10–45. doi:10.3322/caac.21871
2. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
3. Han B, Zheng R, Zeng H, et al. Cancer incidence and mortality in China, 2022. J Natl Cancer Cent. 2024;4(1):47–53. doi:10.1016/j.jncc.2024.01.006
4. Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66(2):115–132. doi:10.3322/caac.21338
5. Morgan E, Soerjomataram I, Rumgay H, et al. The global landscape of esophageal squamous cell carcinoma and esophageal adenocarcinoma incidence and mortality in 2020 and projections to 2040: new estimates from GLOBOCAN 2020. Gastroenterology. 2022;163(3):649–658e2. doi:10.1053/j.gastro.2022.05.054
6. Yang H, Liu H, Chen Y, et al. Neoadjuvant chemoradiotherapy followed by surgery versus surgery alone for locally advanced squamous cell carcinoma of the esophagus (NEOCRTEC5010): a Phase III multicenter, randomized, open-label clinical trial. J Clin Oncol. 2018;36(27):2796–2803. doi:10.1200/JCO.2018.79.1483
7. Yang H, Liu H, Chen Y, et al. Long-term Efficacy of Neoadjuvant Chemoradiotherapy Plus Surgery for the Treatment of Locally Advanced Esophageal Squamous Cell Carcinoma: the NEOCRTEC5010 Randomized Clinical Trial. JAMA Surg. 2021;156(8):721–729. doi:10.1001/jamasurg.2021.2373
8. Kelly RJ, Ajani JA, Kuzdzal J, et al. Adjuvant nivolumab in resected esophageal or gastroesophageal junction cancer. N Engl J Med. 2021;384(13):1191–1203. doi:10.1056/NEJMoa2032125
9. Kojima T, Shah MA, Muro K, et al. Randomized phase III KEYNOTE-181 study of pembrolizumab versus chemotherapy in advanced esophageal cancer. J Clin Oncol. 2020;38(35):4138–4148. doi:10.1200/JCO.20.01888
10. Luo H, Lu J, Bai Y, et al. Effect of camrelizumab vs placebo added to chemotherapy on survival and progression-free survival in patients with advanced or metastatic esophageal squamous cell carcinoma: the ESCORT-1st randomized clinical trial. JAMA. 2021;326(10):916–925. doi:10.1001/jama.2021.12836
11. Qin J, Xue L, Hao A, et al. Neoadjuvant chemotherapy with or without camrelizumab in resectable esophageal squamous cell carcinoma: the randomized Phase 3 ESCORT-NEO/NCCES01 trial. Nat Med. 2024;30(9):2549–2557. doi:10.1038/s41591-024-03064-w
12. Wang X, Wang P, Huang X, Han Y, Zhang P. Biomarkers for immunotherapy in esophageal cancer. Front Immunol. 2023;14:1117523. doi:10.3389/fimmu.2023.1117523
13. Tong X, Jin M, Wang L, Zhang D, Yin Y, Shen Q. Prognostic biomarkers for immunotherapy in esophageal cancer. Front Immunol. 2024;15:1420399. doi:10.3389/fimmu.2024.1420399
14. Holder AM, Dedeilia A, Sierra-Davidson K, et al. Defining clinically useful biomarkers of immune checkpoint inhibitors in solid tumours. Nat Rev Cancer. 2024;24(7):498–512. doi:10.1038/s41568-024-00705-7
15. Wang M, Wei D, Cui Z, et al. Evaluation of the efficacy and safety of neoadjuvant immunotherapy in locally advanced esophageal squamous cell carcinoma. J Thorac Dis. 2025;17(3):1711–1722. doi:10.21037/jtd-2025-215
16. Jin J, Sun M, Yang X, et al. Incidence of MSI-H esophageal carcinoma and related identification of genomic alterations: a multi-center real-world study. Hum Pathol. 2025;163:105878. doi:10.1016/j.humpath.2025.105878
17. Hinterleitner C, Strahle J, Malenke E, et al. Platelet PD-L1 reflects collective intratumoral PD-L1 expression and predicts immunotherapy response in non-small cell lung cancer. Nat Commun. 2021;12(1):7005. doi:10.1038/s41467-021-27303-7
18. Li S, Lu Z, Wu S, et al. The dynamic role of platelets in cancer progression and their therapeutic implications. Nat Rev Cancer. 2024;24(1):72–87. doi:10.1038/s41568-023-00639-6
19. Li Q, Xiang M. Metabolic reprograming of MDSCs within tumor microenvironment and targeting for cancer immunotherapy. Acta Pharmacol Sin. 2022;43(6):1337–1348. doi:10.1038/s41401-021-00776-4
20. Chang TG, Cao Y, Sfreddo HJ, et al. LORIS robustly predicts patient outcomes with immune checkpoint blockade therapy using common clinical, pathologic and genomic features. Nat Cancer. 2024;5(8):1158–1175. doi:10.1038/s43018-024-00772-7
21. Rice TW, Patil DT, Blackstone EH. 8th edition AJCC/UICC staging of cancers of the esophagus and esophagogastric junction: application to clinical practice. Ann Cardiothorac Surg. 2017;6(2):119–130. doi:10.21037/acs.2017.03.14
22. Oken MM, Creech RH, Tormey DC, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol. 1982;5(6):649–655. doi:10.1097/00000421-198212000-00014
23. Langer R, Becker K. Tumor regression grading of gastrointestinal cancers after neoadjuvant therapy. Virchows Arch. 2018;472(2):175–186. doi:10.1007/s00428-017-2232-x
24. Shang X, Xie Y, Yu J, et al. A prospective study of neoadjuvant pembrolizumab plus chemotherapy for resectable esophageal squamous cell carcinoma: the keystone-001 trial. Cancer Cell. 2024;42(10):1747–1763e7. doi:10.1016/j.ccell.2024.09.008
25. Forde PM, Spicer JD, Provencio M, et al. Overall survival with neoadjuvant nivolumab plus chemotherapy in lung cancer. N Engl J Med. 2025;393(8):741–752. doi:10.1056/NEJMoa2502931
26. Okui J, Nagashima K, Matsuda S, et al. Evaluation of pathological complete response as a surrogate endpoint for overall survival in resectable oesophageal cancer: integrated analysis of individual patient data from phase III trials. Br J Surg. 2025;112(6). doi:10.1093/bjs/znaf131
27. Okui J, Matsuda S, Nagashima K, et al. Recurrence-free survival as a surrogate endpoint for overall survival in resectable esophageal cancer: integrated analysis of individual patient data from phase III trials. Ann Surg. 2025. doi:10.1097/SLA.0000000000006919
28. Weissferdt A, Pataer A, Vaporciyan AA, et al. Agreement on major pathological response in NSCLC patients receiving neoadjuvant chemotherapy. Clin Lung Cancer. 2020;21(4):341–348. doi:10.1016/j.cllc.2019.11.003
29. Joosse SA, Pantel K. Tumor-educated platelets as liquid biopsy in cancer patients. Cancer Cell. 2015;28(5):552–554. doi:10.1016/j.ccell.2015.10.007
30. Best MG, Wesseling P, Wurdinger T. Tumor-educated platelets as a noninvasive biomarker source for cancer detection and progression monitoring. Cancer Res. 2018;78(13):3407–3412. doi:10.1158/0008-5472.CAN-18-0887
31. Xing S, Zeng T, Xue N, et al. Development and validation of tumor-educated blood platelets integrin alpha 2b (ITGA2B) RNA for diagnosis and prognosis of non-small-cell lung cancer through RNA-seq. Int J Biol Sci. 2019;15(9):1977–1992. doi:10.7150/ijbs.36284
32. Murphy L, Inchauspe J, Valenzano G, et al. Platelets sequester extracellular DNA, capturing tumor-derived and free fetal DNA. Science. 2025;389(6761):
33. Georgila K, Vyrla D, Drakos E. Apolipoprotein A-I (ApoA-I), Immunity, Inflammation and Cancer. Cancers. 2019;11(8):1097. doi:10.3390/cancers11081097
34. Wang XP, Li XH, Zhang L, et al. High level of serum apolipoprotein A-I is a favorable prognostic factor for overall survival in esophageal squamous cell carcinoma. BMC Cancer. 2016;16(1):516. doi:10.1186/s12885-016-2502-z
35. Luo F, Cao J, Chen Q, et al. HDL-cholesterol confers sensitivity of immunotherapy in nasopharyngeal carcinoma via remodeling tumor-associated macrophages towards the M1 phenotype. J Immunother Cancer. 2024;12(6):e008146. doi:10.1136/jitc-2023-008146
36. Xiao BJ, Sima XX, Chen G, Gulizeba H, Zhou T, Huang Y. Predictive and prognostic role of early apolipoprotein A-I alteration in recurrent or metastatic nasopharyngeal carcinoma patients treated with anti-PD-1 therapy. Cancer Med. 2023;12(16):16918–16928. doi:10.1002/cam4.6321
37. Perrone F, Minari R, Bersanelli M, et al. The prognostic role of high blood cholesterol in advanced cancer patients treated with immune checkpoint inhibitors. J Immunother. 2020;43(6):196–203. doi:10.1097/CJI.0000000000000321
38. Perrone F, Favari E, Maglietta G, et al. The role of blood cholesterol quality in patients with advanced cancer receiving immune checkpoint inhibitors. Cancer Immunol Immunother. 2023;72(7):2127–2135. doi:10.1007/s00262-023-03398-3
39. Yang Y, Xin D, Wang H, et al. A novel predictor of pathologic complete response for neoadjuvant immunochemotherapy in resectable locally advanced esophageal squamous cell carcinoma. J Inflamm Res. 2023;16:1443–1455. doi:10.2147/JIR.S395231
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.