Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Plasma RBP4 Level in Association with Body Composition, Metabolic Profile, STRA6 and RBP4 Gene Polymorphisms in Obese Romanian Children
Authors Boaghi A ![]() , Pop RM
, Pop RM ![]() , Vasilache SL
, Vasilache SL ![]() , Banescu C, Hutanu A, Marginean OC, Pascanu IM
, Banescu C, Hutanu A, Marginean OC, Pascanu IM
Received 26 July 2020
Accepted for publication 19 September 2020
Published 27 November 2020 Volume 2020:13 Pages 4643—4650
DOI https://doi.org/10.2147/DMSO.S273146
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Anastasia Boaghi,1 Raluca-Monica Pop,1,2 Simona Loredana Vasilache,3 Claudia Banescu,4 Adina Hutanu,5 Oana Cristina Marginean,6 Ionela Maria Pascanu1,7
1Department of Endocrinology, Mures County Hospital, Tȃrgu Mureș 540139, Romȃnia; 2Research Methodology Department, George Emil Palade University of Medicine, Pharmacy, Science, and Technology of Tȃrgu Mureș, Tȃrgu Mureș 540139, Romȃnia; 3Doctoral School, George Emil Palade University of Medicine, Pharmacy, Science, and Technology of Tȃrgu Mureș, Tȃrgu Mureș 540139, Romȃnia; 4Genetics Department, George Emil Palade University of Medicine, Pharmacy, Science, and Technology of Tȃrgu Mureș, Tȃrgu Mureș 540139, Romȃnia; 5Center for Advanced Medical and Pharmaceutical Research, LC/MC Laboratory, George Emil Palade University of Medicine, Pharmacy, Science, and Technology of Tȃrgu Mureș, Tȃrgu Mureș, 540139, Romȃnia; 6Pediatrics Department, George Emil Palade University of Medicine, Pharmacy, Science, and Technology of Tȃrgu Mureș, Tȃrgu Mureș 540139, Romȃnia; 7Endocrinology Department, George Emil Palade University of Medicine, Pharmacy, Science, and Technology of Tȃrgu Mureș, Tȃrgu Mureș 540139, Romȃnia
Correspondence: Raluca-Monica Pop
Research Methodology Department, George Emil Palade University of Medicine, Pharmacy, Science, and Technology of Tȃrgu Mureș, 38 Gheorghe Marinescu Street, Tȃrgu Mureș 540139, Romȃnia
Tel +40 744326976
Fax +40 265210407
Email [email protected]
Background: Pediatric obesity continues to remain a serious health concern which has significantly increased the morbidity risk in adulthood. Recent studies have analyzed the impact of the two adipokines, RBP4 (retinol binding protein 4) and STRA6 (stimulated by retinoic acid 6) in pediatric obese subjects with contradictory results.
Methods: An observational study was conducted in the Pediatric and Endocrinology Departments, Targu-Mures, Romania, including 213 children between 5– 17 years of age, divided into two groups according to body mass index (BMI) standard deviation score (SDS): case (overweight or obese) and control (normal SDS). Age, sex, basic anthropometric and biochemical measurements and genotype of rs3758539, and rs10882280 for RBP4 gene and rs974456 and rs351224 of STRA6 gene were analyzed. Statistical analysis used SPSS v. 25.0, with a level of significance α = 0.05.
Results: There is no association between the two gene’s polymorphisms and obesity in our pediatric population. In regression analysis, with HOMA IR (homeostatic model assessment of insulin resistance) as the outcome, the plasmatic level of RBP4 and fat mass percentage are significant predictors, with the model explaining 42% of the HOMA variability. Hypercholesterolemia was significantly associated with male sex, carrying variant allele and heterozygote status of rs10882280 RBP4 gene and wild-type allele rs351224 of STRA6 gene.
Conclusion: There is no significant association between obesity and SNPs of the RBP4 and STRA6 in our population, but they seem to play a role in insulin resistance and hypercholesterolemia.
Keywords: pediatric obesity, RBP4, STRA6, polymorphisms
Introduction
Overweight and obesity have become a global public health problem in the last decade, with its prevalence increasing at an alarming step, especially in the pediatric population. The World Health Organization (WHO) estimated that in 2016, 340 million children and adolescents aged 5–19 years were overweight or obese.1 The most recent data for Romania showed that one in four children was overweight or obese with male gender and school-aged groups being more affected.2,3 This condition leads to a higher propensity towards developing metabolic syndrome, diabetes mellitus, hypertension, cardiovascular disease, and sleep apnea both during childhood and later in adulthood.
Endocrine Society recommends using body mass index (BMI) standard deviation scores (SDS) to categorize obesity in research studies, based on the WHO standards.4 Normal BMI is considered between −1 and +1 standard deviation score SDS for age and sex, overweight as a BMI between +1 and +2 SDS and obesity as a BMI above +2 SDS for age and sex.5 Genetic, socioeconomic, behavioral, and environmental factors are involved in this disorder’s etiology.6 In obese humans, adipose tissue secretes an impressive number of adipokines with local and systemic effects and it is responsible for insulin resistance with proinflammatory response.7
RBP4 (retinol binding protein 4) is a plasma transporter protein for vitamin A, which has been recently described as a possible mediator for obesity and type 2 diabetes mellitus through its ability to increase insulin resistance.8,9 The RBP4 gene is located on chromosome 10 (10q23–q24), has a molecular mass of ~21 kDa and it encodes a protein of 201 amino acids.10 Yang et al observed higher levels of RBP4 in the blood of several mouse models of obesity and insulin resistance.11
STRA6 (stimulated by retinoic acid 6) is a membrane retinol transporter, which transfers vitamin A from blood into target cells and it was identified as the RBP4 membrane receptor.12,13 STRA6 activates a JAK2 (Janus kinases 2)/STAT5 (Signal transducer and activator of transcription 5) cascade which continues with induction of STAT target genes. It induces the inhibitor of insulin signaling SOCS3 (Suppressor of cytokine signaling 3) with insulin resistance as final result.11,14 The role of RBP4 and STRA6 in children’s obesity and its comorbidities was investigated in different populations such as the Chinese, Caucasian, American, Canadian, but as to date, there is no available data regarding Romanian children.15–20
The studies analyzing the impact of various adipokines on metabolic consequences are important for their correct and early management. Apart from prevention strategies which include physical activity, lifestyle and diet changes, the treatment for confirmed cases is difficult and novel therapeutic strategies targeting adipokine milieu might become the key for tackling this condition. In order to “flatten the curve,” new approaches to prevent and address obesity must be devised. Using adipokines as target for future pharmacological interventions might prove to be the key for treating obesity, but the exact relationship between the adipokines, their genes and obesity development has yet to be fully understood.21
Recently, studies analyzing RBP4 plasmatic levels in pediatric populations showed that higher values were associated with increased cardiovascular and obesity risk, with the underlying mechanism hypothesized to be increased levels of oxidative stress markers, such as glutathione.16,22–24 Apart from plasma levels, single nucleotide polymorphisms have been analyzed, yielding an association between rs3758539 and rs10882280 of the RBP4 and insulin resistance, metabolic syndrome, obesity and diabetes mellitus.20,25,26 rs974456 of the STRA6 was significantly associated with diabetes mellitus in the adult population.27,28 Therefore, RBP4 and STRA6 gene polymorphism might be involved as susceptibility genes in obesity.
The aim of this study was to analyze the association of two specific single nucleotide polymorphism (SNPs) rs3758539 and rs10882280 of the RBP4 and rs974456 and rs351224 of the STRA6 with anthropometric and biochemical markers of obesity in children.
Materials and Methods
Study Design
An observational study was conducted in the Endocrinology and Pediatric Clinic of Târgu Mures, Romania, including 213 children, between 5–17 years of age, selected and evaluated between 2016 and 2018. Subjects were divided into two groups according to BMI SDS, based on WHO standards:29 control group: −1 SDS and + 1 SDS, and case group (overweight: > +1 SDS and obese > +2 SDS). Subjects in the control group were represented by children with normal BMI and without any of the exclusion criteria, referred for a pediatric or endocrine consult and in whom any pathology was excluded. The following exclusion criteria were used: age below 5 years; secondary causes of obesity, such as genetic, hypothalamic disorders, endocrine severe disorders; history of severe chronic diseases (chronic kidney disease, heart failure, liver failure, and malabsorption syndrome); pharmacological causes; or parents and children’s refusal to participate in the study. For the case group, all consecutive children presenting for consult with a BMI SDS >1 SDS and none of the exclusion criteria were considered eligible and were proposed participation in the study.
Ethics Statements
The study protocol was approved by the Ethics Committee for Scientific Research of “George Emil Palade” University of Medicine, Pharmacy, Science and Technology of Targu Mures (decision no.7/11th of January 2016). Written informed consent was obtained from the parents/legal representatives and a verbal consent from children.
Upon written consent, the study visit was scheduled, during which all anthropometric measurements were repeated, body composition analysis was performed and blood was drawn for biochemical and genetic analysis. We analyzed age, sex and basic anthropometric measurements: height SDS, BMI SDS, abdominal circumference SDS, tricipital skin-fold thickness SDS, waist circumference/height ratio (WHtR), body composition such as fat mass, muscle mass performed with bioimpedance analysis (Tanita BC-420) which is a safe method based on electrical resistance of different type of tissue and can be influenced by age, sex or race. We used standardized tools and measurement protocols.30,31
Metabolic Analysis
Biochemistry parameters, serum levels of glucose (normal value: 70–105 mg/dl), total cholesterol (normal value: <170 mg/dl), HDL-c (normal value: 40–60 mg/dl), uric acid (normal value: 2.6–6 mg/dl), triglycerides (TG, normal value: <150 mg/dl) were evaluated by routine laboratory procedures on analyzer Architect C 4000.
HOMA IR (homeostatic model assessment for insulin resistance) was calculated according to formula: fasting insulin levels x fasting glucose/405.
For insulin and RBP4, blood samples were collected on EDTA as anticoagulant, during the morning after 10–12 hours overnighting fasting. Tubes were centrifuged at 1500g for 15 minutes and plasma aliquoted and stored at −80 °C until analyzed. Plasma levels of insulin and RBP4 were assessed using the ELISA method on automated analyzer ELISA Dynex DSX (Dynex Technology, USA).
For insulin (DRG International Inc., USA) a quantitative solid-phase enzyme-linked immunosorbent assay (ELISA) based on the sandwich principle was used, according to the manufacturer instructions. Patient samples (containing endogenous insulin) were incubated with enzyme conjugate containing biotin-conjugated anti-insulin antibody in the wells coated with monoclonal anti-insulin antibody. After incubation and washing steps, the addition of the streptavidin peroxidase complex followed by substrate, allow revelation of the antigen-antibody complex. The intensity of color developed was proportional to the insulin concentration in the sample. Performance characteristics for Insulin detection kit: sensitivity 1.76 μUI/mL, intra- and inter-assay CVs were < 2.6 % and < 6% respectively.
For RBP4, a captured quantitative ELISA immunoassay was used, according to manufacturers’ instructions (Sigma-Aldrich Co, USA). The capture antibody coated on wells were incubated with samples and standards (with known concentrations). After an overnight incubation step at 4 °C, the target protein from the sample binds on the immobilized antibody from the bottom of the wells. After the addition of the secondary biotinylated detection antibody followed by peroxidase-streptavidin solution and substrate (3,3′,5,5′-Tetramethylbenzidine) the color developed was proportional to RBP4 concentration from the samples. The performance characteristics of the test were: minimum detectable dose 0.1 ng/mL and intraassay reproducibility < 10%.
Fresh blood, collected in an EDTA tube, was used for isolation of genomic DNA (gDNA) by using Quick-DNA miniprep kit (from ZymoResearch, USA). The obtained gDNA was quantified by using BioSpectrometer basic (Eppendorf AG). For genotyping of rs3758539, and rs10882280 for RBP4 gene and rs974456 and rs351224 of STRA6 gene we used the 7500 Fast Real-Time PCR system from ThermoFisher Scientific (USA) and the specific TaqMan assays as follows: C_11756910_10, C_11756899_10 (for RB4 SNPs) and C___3152257_20, C___3152256_10 (for STRA6 SNPs).
Statistical Analysis
The statistical analysis was performed using SPSS v. 25.0 (SPSS Inc, Chicago, IL, USA). For descriptive statistics, we used the mean and standard deviation for normally distributed variables and median and interquartile range for non-gaussian distribution. The Shapiro Wilk test was used to assess distribution. Unpaired independent samples t-test or Mann–Whitney test were used for mean/median comparison. Spearman’s nonparametric correlation analysis was used to determine the relationships between continuous variables and chi-square test for associations’ evaluation. Linear and logistic regression models were constructed, using the continuous or categorical BMI classification, as well as metabolic parameters as outcomes and the various anthropometric and metabolic parameters as predictors. The level of significance used was α=0.05.
Results
Anthropometric and biochemical characteristics of the study groups are presented in Table 1. Median age of the control group was 12.0 years (10.9–12.3) and for case group was 11.5 years (10.9–11.9), with no significant difference between median age (p=0.635). The two groups were age and sex matched, with 130 subjects in the case group and 83 in the control group. Sex ratio male: female was 0.8 for control group and 1.1 for the case group. There are significant differences for clinical parameters: height SDS, BMI SDS, waist SDS, skinfold SDS, fat mass, and muscle mass. Except for glucose, all the metabolic parameters were significantly different between case and control groups.
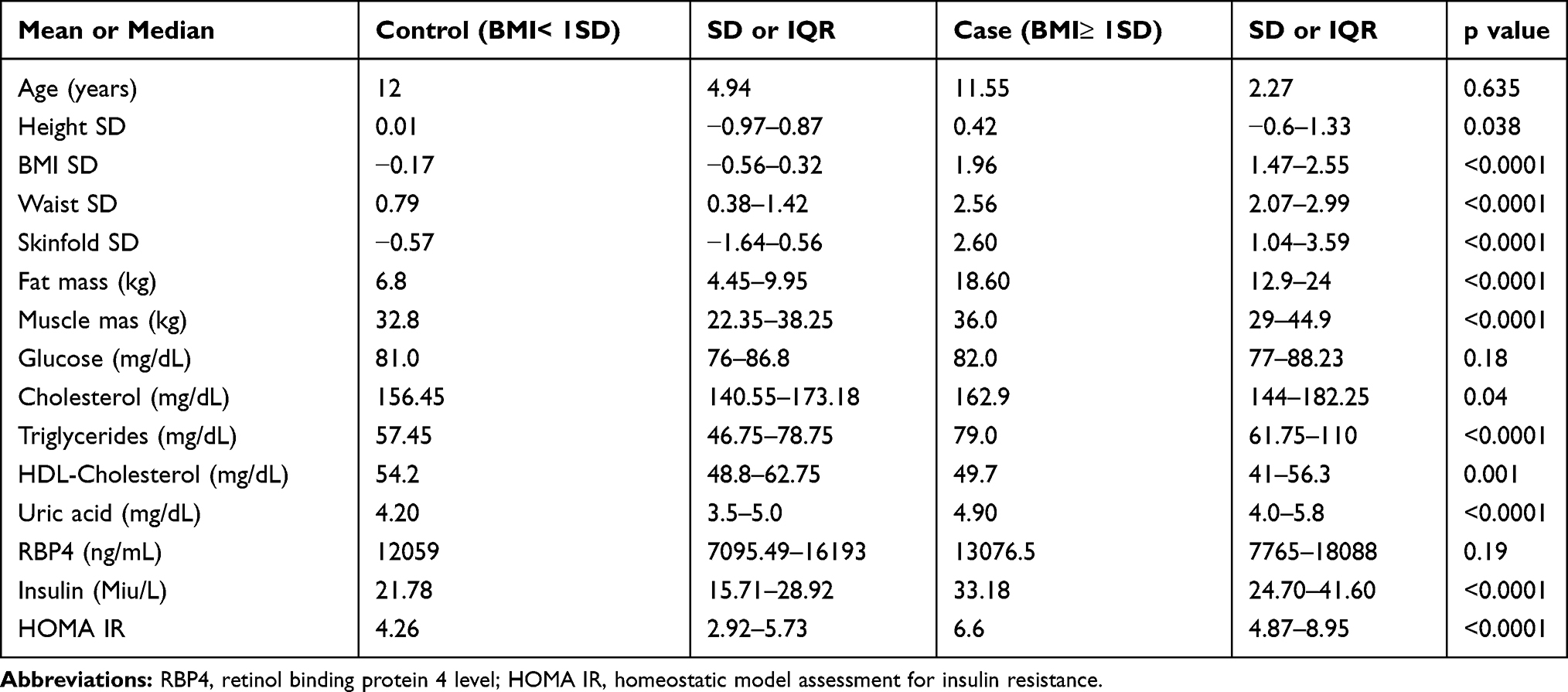 |
Table 1 General Characteristics of the Normal vs Overweight obese Children |
HOMA IR, significantly correlated with BMI SDS (rs=0.426, p=0.001), waist circumference SDS (rs= 0.426, p=0.001), fat mass (rs= 0.501, p=0.001), muscle mass (rs=0.375, p=0.001), glucose (rs= 0.285, p=0.001), triglycerides (rs= 0.33, p= 0.001), HDL-cholesterol (rs 0.199, p=0.007), uric acid (rs= 0.221, p= 0.016) and insulin (rs= 0.973, p=0.001).
After adjusting for age, sex and BMI SDS, the plasmatic level of RBP4 does not correlate with the components of the metabolic, body composition or anthropometric profile.
In regression analysis, with HOMA IR as the outcome, the plasmatic level of RBP4 (β=0.153, 95% CI 0.02–0.285, p=0.024), age (β=0.193, 95% CI 0.062–0.325, p=0.004) and fat mass percentage (β=0.338, 95% CI 0.188–0.488, p<0.001) are significant predictors, with the model explaining 42% of the HOMA variability and BMI SDS and sex having no significant influence.
The frequency of minor alleles corresponds to the general data for each polymorphism, and the frequency of the genotypes is in the Hardy-Weinberg equilibrium (RBP4 rs3758539 Χ2=0.1, RBP4 rs10882280, Χ2=0.07, STRA6 rs351224 Χ2=0.45, p>0.05), except for STRA6 rs974456(Χ2=4.45, p<0.01). There is an association between sex and STRA6 rs974456 (p=0.021), and the genotype frequency for boys is in Hardy Weinberg equilibrium (Χ2=0.97, p>0.05). Using logistic regression, with low HDL or high triglycerides as the outcome, there is no association with the RBP4 or STRA6 SNP. When using hypercholesterolemia as the outcome, male sex (OR 2.197, 95% CI 1.132–4.266, p=0.020), allele A of the rs10882280 (OR 0.274, 95% CI 0.125–0.604, p=0.001), heterozygote status of the RBP4 rs10882280 (OR 3.643, 95% CI 1.657–8.012, p=0.001) and allele T of the STRA6 rs351224 (OR 2.368, 95% CI 1.044–5.368, p=0.039) are significantly associated with it.
There is no significant association between the genotypes and obesity (Table 2).
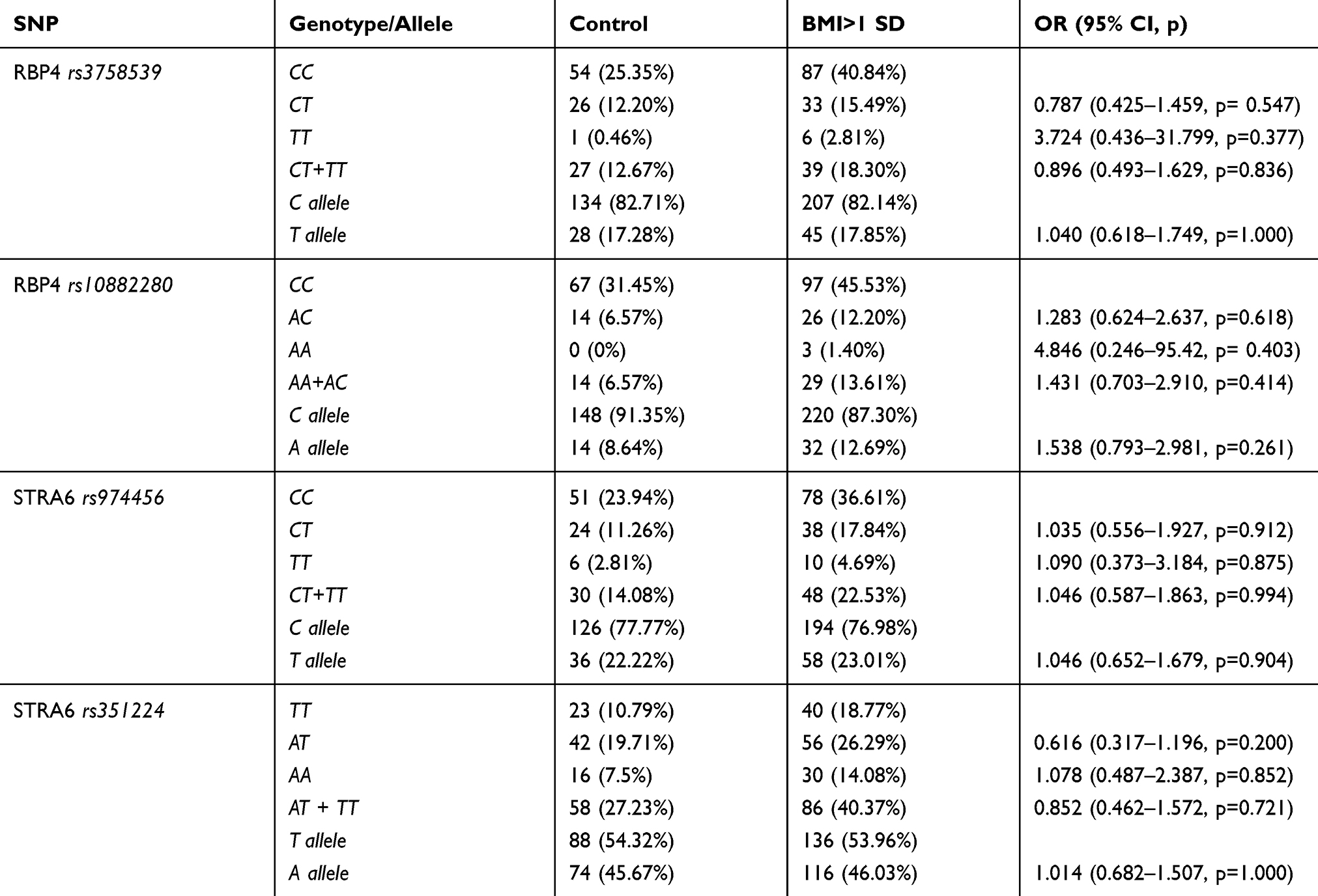 |
Table 2 Genotype and allele Distributions of Investigated SNPs in Pediatric Population |
Discussions
Pediatric obesity continues to remain a serious health concern which has significantly increased the risk of comorbidities in adulthood. This disorder is caused by the interaction between genetic and environmental factors.4,32,33 Abdominal obesity by itself is an independent risk factor for insulin resistance and the development of type 2 diabetes mellitus.34
Our study found significant higher levels of both insulin and HOMA IR in the obese group, results concordant to the study of 173 obese and multi-ethnic adolescents which concluded that gender, pubertal stage, BMI, WC, and body fat percentage had significant, positive correlations with fasting insulin and HOMA IR.35 Recently, a study on a Romanian elderly population has also described significant higher levels of HOMA-IR in the obese group.36
The direction of the relationship between concentrations of RBP4 blood levels and obesity is still controversial. In the study performed by Li et al on a Chinese population, BMI and waist to hip ratio (WHR) were positively correlated with RBP4.18 In cross-sectional study of 98 Indian obese/overweight children higher values of RBP4 were present in 81% of boys and 56.8% of girls with a significant difference between genders.23 Another study found higher RBP4 blood levels in obese American adolescents (by 36%) compared with normal weight children which positively correlated with HOMA IR, fat mass and fasting insulin levels.16 Klisic et al demonstrated significant correlation between cardiovascular risk score in Serbian overweight/obese adolescent girls aged 16–19 years and BMI, WC, LDL cholesterol, insulin, HOMA IR and plasma RBP4. They concluded that a higher cardiovascular risk score positively correlates with RBP4 levels in this age group.24
We have not obtained significant correlations of plasma RBP4 with BMI and WHtR and there were no significant differences between the two groups regarding RBP4 level. Similar to our results, another study analyzing the blood level of RBP4 in American pediatric population found no differences in obese or overweight vs normal weight children.37 Korek et al did not observe in adult population significant correlation between RBP4 and anthropometric markers, such as body weight, BMI, WHR.38 There are also contradictory studies which described that RBP4 correlated with age, anthropometric parameters and fat mass percentage.15,24,39 Friebe et al observed that values of RBP4 were increasing with pubertal stage.39 Pubertal status was not reported in our study, but we also found significant correlations between RBP4 and HOMA IR levels, with RBP4, age and fat mass explaining 42% of the HOMA IR variability.
Hyperinsulinemia may lead to an increase in triglycerides levels and subsequently stimulates the synthesis and secretion of RBP4 from the liver or the ectopic adipose tissue, and there are studies which proved positive correlations between plasma RBP4 and elevated triglycerides both in pediatric and adult population.24,38,40 Kim et al found that the positive association between RBP4 and triglycerides levels was maintained even after adjusting for confounding factors such as age and BMI.41 Kwanbunjan et al concluded that RBP4 levels were significantly higher among 167 adult subjects with high triglycerides levels and the associations of RBP4 with hypertriglyceridemia and insulin resistance may have important implications for the risk of heart disease and stroke.42 Although we found the already mentioned significant correlations between RBP4 and HOMA IR, in our sample there was no significant correlation between RBP4 and triglycerides levels, results concordant with those from Friebe et al on 129 Caucasian children and adolescents.39 Thiruvengadam et al concluded that RBP4 was significantly correlated only with LDL levels and CRP (C reactive protein) levels in children.23 To sum up, RBP4 levels seem to correlate with some markers of metabolic syndrome, more often with glucose metabolism (as our results showed), but no definitive conclusion can be drawn from the available small observational data on different ethnic populations, opening the field for the hypothesis of genetic factors determinism.
Regarding the analysis of the relationship between SNP and obesity, our results did not confirm significant association between SNPs rs3758539 and rs10882280 of the RBP4 and obesity in the studied population. Also, we did not find any significant association between SNPs and metabolic factors, except total cholesterol.
In a study analyzing the same SNPs as we did in 180 Caucasian children, Codoner-Franch et al identified a significant association between the RBP4 rs3758539 and insulin and HOMA IR and observed that children carrying variant allele had higher insulin levels and HOMA IR than carriers of the wild-type allele.26 They did not find other significant association of RBP4 rs3758539 with metabolic risk such as BMI, WHR, triglycerides, HDL-cholesterol and mean arterial pressure.26 Similarly, Fribe et al did not notice an association between rs3758539 of RBP4 and total cholesterol, triglycerides, HDL-cholesterol and LDL-cholesterol in Caucasian children.20 They did confirm significant association between the carriers of wild-type allele of RBP4 rs3758539 and the variant allele with BMI, WHR, blood pressure and insulin sensitivity index.20 Shea et al, in a study of 1836 Canadian population, analyzed five SNPs and concluded that SNPs rs10882280 was significantly associated with HDL cholesterol, without any associations with other parameters of lipid metabolism.25 Another study on Canadian population found that the risk allele C of RBP4 rs3758539 genotype CT had significant association with HDL-cholesterol and dyslipidemia.43 Shajarian et al did not find any significant association between RBP4 rs3758539 and total cholesterol, HDL-cholesterol, LDL- cholesterol, triglycerides, glucose, insulin and HOMA IR.44 Minor allele of RBP4 rs3758539 had an increased effect on BMI from GG to AA genotype and from CC to AA genotype for RBP4 rs10882280.44 Studies of two SNPs (rs10882283 and rs10882273 of RBP4 gene) were associated with increased BMI and WHR.45 Thus, different ethnic backgrounds might be a cause of the discrepancies between our results and literature data.
A previous research that included 571 type 2 diabetes adult patients and 632 healthy subjects and analyzed rs974456 of the STRA6 gene concluded that genotype TT was associated significantly with diabetes; subjects with CC homozygous genotype have a significantly higher risk of diabetes than those with variant (TT+TC) genotype in the case of rs974456.28 Nair et al demonstrated that STRA6 rs974456 is also associated with diabetes in Indian adult population.27 We noticed no association between rs974456 and rs351224 of the STRA6 gene and obesity or overweight in our pediatric population from central part of Romania, but there was an association between hypercholesterolemia and wild-type allele of STRA6 rs351224 gene.
Considering the fact that the previous studies were performed only on adult population and no data are available regarding the role of the rs3758539 and rs10882280 of the RBP4 gene and rs974456 and rs351224 of the STRA6 gene in children, we may consider the present research a unique and valuable study. However, there are some study limitations to be taken into account. The sample size was small, and the control group included children presenting for consultations for other mild disorders, which might have had an unknown influence on the metabolic profile or even RBP4 levels. A larger study, including subjects at a national level and using controls from the general population might yield different results.
Conclusion
In the current study, we described no correlation between RBP4 value and components of the anthropometric or metabolic profile in obese children, but RBP4 levels are significant predictors for insulin resistance. There is no association between rs3758539 and rs10882280 of the RBP4 and rs974456 and rs351224 for STRA6 and obesity in our population. Two of the 4 SNPs analyzed (carrying variant allele and heterozygote status of rs10882280 RBP4 gene and wild-type allele rs351224 of STRA6 gene) seem to be associated with hypercholesterolemia, but additional genetic studies are needed.
Statement of Ethics
The research was approved by the University’s Ethics Committee (no.7/11th of January 2016). All procedures performed in this study were ethically in accordance with the World Medical Association Declaration of Helsinki.
Acknowledgment
This study was supported by an internal research grant from the University of Medicine and Pharmacy Tirgu-Mures, Romania (Nr. 17802/1/22.12.2015).
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
No competing financial interests exist. The authors report no conflicts of interest for this work.
References
1. WHO. Obesity and overweight: fact sheet. WHO Media Cent. 2016.
2. Chirita-Emandi A, Barbu CG, Cinteza EE, et al. Overweight and underweight prevalence trends in children from Romania - pooled analysis of cross-sectional studies between 2006 and 2015. Obes Facts. 2016;9(3):206–220. doi:10.1159/000444173
3. Moldovanu F, Nanu M, Ardeleanu I, Stativa E, Nanu I, Bacalearos C. P161 overweight and obesity in romanian children, in European context. 2017. doi:10.1136/archdischild-2017-313273.249
4. Styne DM, Arslanian SA, Connor EL, et al. Pediatric obesity-assessment, treatment, and prevention: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2017. doi:10.1210/jc.2016-2573
5. Barlow SE. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: summary report. Pediatrics. 2007;120:s164–s192. doi:10.1542/peds.2007-2329C
6. Hruby A, Hu FB. The epidemiology of obesity: a big picture. Pharmacoeconomics. 2015;33(7):673–689. doi:10.1007/s40273-014-0243-x
7. Ahima R, Osei S. Adipokines in obesity. Front Horm Res. 2007. doi:10.1159/000115365
8. Kovacs P, Geyer M, Berndt J, et al. Effects of genetic variation in the human retinol binding protein-4 gene (RBP4) on insulin resistance and fat depot-specific mRNA expression. Diabetes. 2007;56(12):3095–3100. doi:10.2337/db06-1647
9. Newcomer ME, Ong DE. Plasma retinol binding protein: structure and function of the prototypic lipocalin. Biochim Biophys Acta - Protein Struct Mol Enzymol. 2000;1482(1–2):57–64. doi:10.1016/S0167-4838(00)00150-3
10. Jaconi S, Rose K, Hughes GJ, Saurat JH, Siegenthaler G. Characterization of two post-translationally processed forms of human serum retinol-binding protein: altered ratios in chronic renal failure. J Lipid Res. 1995;36:1247–1253.
11. Yang Q, Graham TE, Mody N, et al. Serum retinol binding protein 4 contributes to insulin resistance in obesity and type 2 diabetes. Nature. 2005;436(7049):356–362. doi:10.1038/nature03711
12. Kawaguchi R, Yu J, Ter-Stepanian M, et al. Receptor-mediated cellular uptake mechanism that couples to intracellular storage. ACS Chem Biol. 2011;6(10):1041–1051. doi:10.1021/cb200178w
13. Kawaguchi R, Zhong M, Kassai M, Ter-Stepanian M, Sun H. STRA6-catalyzed vitamin a influx, efflux, and exchange. J Membr Biol. 2012;245(11):731–745. doi:10.1007/s00232-012-9463-1
14. Berry DC, Jin H, Majumdar A, Noy N. Signaling by vitamin A and retinol-binding protein regulates gene expression to inhibit insulin responses. Proc Natl Acad Sci U S A. 2011;108(11):4340–4345. doi:10.1073/pnas.1011115108
15. Aeberli I, Biebinger R, Lehmann R, L’Allemand D, Spinas GA, Zimmermann MB. Serum retinol-binding protein 4 concentration and its ratio to serum retinol are associated with obesity and metabolic syndrome components in children. J Clin Endocrinol Metab. 2007;92(11):4359–4365. doi:10.1210/jc.2007-0468
16. Balagopal P, Graham TE, Kahn BB, Altomare A, Funanage V, George D. Reduction of elevated serum retinol binding protein in obese children by lifestyle intervention: association with subclinical inflammation. J Clin Endocrinol Metab. 2007;92(5):1971–1974. doi:10.1210/jc.2006-2712
17. Reinehr T, Stoffel-Wagner B, Roth CL. Retinol-binding protein 4 and its relation to insulin resistance in obese children before and after weight loss. J Clin Endocrinol Metab. 2008. doi:10.1210/jc.2007-2745
18. Li L, Wang C, Bao Y, et al. Serum retinol-binding protein 4 is associated with insulin secretion in Chinese people with normal glucose tolerance. J Diabetes. 2009;1(2):125–130. doi:10.1111/j.1753-0407.2009.00024.x
19. Yeste D, Vendrell J, Tomasini R, et al. Retinol-binding protein 4 levels in obese children and adolescents with glucose intolerance. Horm Res Paediatr. 2010;73(5):335–340. doi:10.1159/000308165
20. Friebe D, Kovacs P, Neef M, et al. The promoter variant −803G>A in the RBP4 gene is not associated with BMI, metabolic parameters or blood pressure in caucasian children. Exp Clin Endocrinol Diabetes. 2011. doi:10.1055/s-0031-1286295
21. Blüher M. Adipokines - removing road blocks to obesity and diabetes therapy. Mol Metab. 2014;3(3):230–240. doi:10.1016/j.molmet.2014.01.005
22. Codoñer-Franch P, Mora-Herranz A, Simó-Jordá R, Pérez-Rambla C, Boix-García L, Faus-Pérez A. Retinol-binding protein 4 levels are associated with measures of liver and renal function and oxidant/antioxidant status in obese children. J Pediatr. 2013;163(2):593–595. doi:10.1016/j.jpeds.2013.03.060
23. Thiruvengadam V, Amperayani S, Babu RP, Uppuluri R. Correlation of childhood obesity and related insulin resistance with leptin and retinol binding protein 4. Indian J Pediatr. 2015. doi:10.1007/s12098-015-1706-6
24. Klisić A, Kavarić N, Bjelaković B, Soldatović I, Martinović M, Kotur-Stevuljević J. The association between retinol-binding protein 4 and cardiovascular risk score is mediated by waist circumference in overweight/obese adolescent girls. Acta Clin Croat. 2017;56:92–98. doi:10.20471/acc.2017.56.01.14
25. Shea JL, Loredo-Osti JC, Sun G. Association of RBP4 gene variants and serum HDL cholesterol levels in the newfoundland population. Obesity. 2010;18(7):1393–1397. doi:10.1038/oby.2009.398
26. Codoñer-Franch P, Carrasco-Luna J, Allepuz P, Codoñer-Alejos A, Guillem V. Association of RBP4 genetic variants with childhood obesity and cardiovascular risk factors. Pediatr Diabetes. 2016;17(8):576–583. doi:10.1111/pedi.12339
27. Nair AK, Sugunan D, Kumar H, Anilkumar G. Case-control analysis of SNPs in GLUT4, RBP4 and STRA6: association of SNPs in STRA6 with type 2 diabetes in a south indian population. PLoS One. 2010;5(7):e11444. doi:10.1371/journal.pone.0011444
28. Huang HW, Liang BY, Li YX. Association of polymorphisms in STRA6 and RARRES2 genes with type 2 diabetes in southern Han Chinese. Biomed Res Int. 2016. doi:10.1155/2016/6589793
29. De Onis M. WHO Child Growth Standards based on length/height, weight and age. Acta Paediatr Int J Paediatr. 2006. doi:10.1080/08035320500495548
30. NHANES. Anthropometry procedures manual. National Health and Nutrition Examination Survey; 2020.
31. Tanita Corporation of America Inc. Tanita MC-780U Brochure. Tanita Corporation of America Inc.
32. Alkhzouz C, Miclea D, Farcas M, Bucerzan S, Cabau G, Popp RA. Is there a correlation between GAD2 gene-243 A>G polymorphism and obesity? Rev Rom Med Lab. 2019. doi:10.2478/rrlm-2019-0033
33. Vasilache SL, Mărginean CO, Boaghi A, et al. Implications of visfatin genetic variants in the metabolic profile of the Romanian pediatric population. Rev Rom Med Lab. 2020;28(2):163–174. doi:10.2478/rrlm-2020-0015
34. Forkert ECO, Rendo-Urteaga T, Nascimento-Ferreira MV, de Moraes ACF, Moreno LA, de Carvalho HB. Abdominal obesity and cardiometabolic risk in children and adolescents, are we aware of their relevance? Nutrire. 2016;41(1). doi:10.1186/s41110-016-0017-7
35. Ling JCY, Mohamed MNA, Jalaludin MY, Rampal S, Zaharan NL, Mohamed Z. Determinants of high fasting insulin and insulin resistance among overweight/obese adolescents. Sci Rep. 2016;6(1). doi:10.1038/srep36270
36. Mihai G, Gasparik AI, Pascanu IM, Cevei M, Hutanu A, Pop RM. The influence of Visfatin, RBP-4 and insulin resistance on bone mineral density in women with treated primary osteoporosis. Aging Clin Exp Res. 2019;31(6):889–895. doi:10.1007/s40520-019-01206-6
37. Kanaka-Gantenbein C, Margeli A, Pervanidou P, et al. Retinol-binding protein 4 and lipocalin-2 in childhood and adolescent obesity: when children are not just “small adults”. Clin Chem. 2008;54(7):1176–1182. doi:10.1373/clinchem.2007.099002
38. Korek E, Gibas-Dorna M, Chęcińska-Maciejewska Z, et al. Serum RBP4 positively correlates with triglyceride level but not with BMI, fat mass and insulin resistance in healthy obese and non-obese individuals. Biomarkers. 2018;23(7):683–688. doi:10.1080/1354750X.2018.1479770
39. Friebe D, Neef M, Erbs S, et al. Retinol binding protein 4 (RBP4) is primarily associated with adipose tissue mass in children. Int J Pediatr Obes. 2011;6(2):e345–e352. doi:10.3109/17477166.2010.491228
40. Qi Q, Yu Z, Ye X, et al. Elevated retinol-binding protein 4 levels are associated with metabolic syndrome in Chinese people. J Clin Endocrinol Metab. 2007;92(12):4827–4834. doi:10.1210/jc.2007-1219
41. Kim IK, Lee HJ, Kang JH, Song J. Relationship of serum retinol-binding protein 4 with weight status and lipid profile among Korean children and adults. Eur J Clin Nutr. 2011;65(2):226–233. doi:10.1038/ejcn.2010.251
42. Kwanbunjan K, Panprathip P, Phosat C, et al. Association of retinol binding protein 4 and transthyretin with triglyceride levels and insulin resistance in rural thais with high type 2 diabetes risk. BMC Endocr Disord. 2018;18(1). doi:10.1186/s12902-018-0254-2
43. Aref-Eshghi E, Hurley O, Sun G, et al. Genetic associations in community context: a mixed model approach identifies a functional variant in the RBP4 gene associated with HDL-C dyslipidemia. BMC Med Genet. 2018;19(1). doi:10.1186/s12881-018-0719-1
44. Shajarian M, Rafiee L, Naji-Esfahani H, Haghjooy-Javanmard S, Nizal S. Association of RBP4 gene variants with adverse lipid profile and obesity. Gene. 2015;561(1):1–5. doi:10.1016/j.gene.2014.12.071
45. Munkhtulga L, Nagashima S, Nakayama K, et al. Regulatory SNP in the RBP4 gene modified the expression in adipocytes and associated with BMI. Obesity. 2010;18(5):1006–1014. doi:10.1038/oby.2009.358
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.