Back to Journals » Cancer Management and Research » Volume 11
Plasma long noncoding RNAs PANDAR, FOXD2-AS1, and SMARCC2 as potential novel diagnostic biomarkers for gastric cancer
Authors Yang Z, Sun Y ![]() , Liu R
, Liu R ![]() , Shi Y, Ding S
, Shi Y, Ding S ![]()
Received 17 January 2019
Accepted for publication 11 June 2019
Published 4 July 2019 Volume 2019:11 Pages 6175—6184
DOI https://doi.org/10.2147/CMAR.S201935
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xueqiong Zhu
Ziwei Yang,1 Yanfei Sun,2 Rongfeng Liu,3 Yanyan Shi,4 Shigang Ding5
1Department of Clinical Laboratory Medicine, The First Affiliated Hospital of China Medical University, Shenyang, Liaoning, People’s Republic of China; 2Department of Emergency, The First Affiliated Hospital of China Medical University, Shenyang, Liaoning, People’s Republic of China; 3Department of Clinical Laboratory Medicine, Beijing Anzhen Hospital, Capital Medical University, Beijing, People’s Republic of China; 4Research Center of Clinical Epidemiology, Peking University Third Hospital, Beijing, People’s Republic of China; 5Department of Gastroenterology, Peking University Third Hospital, Beijing, People’s Republic of China
Background: Gastric cancer is still a common cancer worldwide. Investigation of potential plasma biomarkers for gastric cancer diagnosis is essential for prevention strategies and early intervention for gastric cancer-control planning.
Objectives: This study was aimed to explore the lncRNAs’ promoter of CDKN1A antisense DNA-damage-activated RNA (PANDAR), FOXD2-AS1, and SMARCC2 as potential novel diagnostic biomarkers for gastric cancer.
Method: 109 gastric cancer patients and 106 healthy controls were involved in this study. Plasma lncRNAs PANDAR, FOXD2-AS1, and SMARCC2 were detected by real-time PCR. Student’s t-test, Mann-Whitney U test, and Chi-square test were used to verify the differences of clinical variables between two groups. Receiver operating characteristic curve (ROC) was used to evaluate the diagnostic value of every biomarker. Multivariable analysis of risk factors for gastric cancer was performed using logistic regression analysis.
Results: There were significant differences in age, gender, carcinoembryonic antigen (CEA), carbohydrate antigen (CA) 153 between gastric cancer and healthy controls (P<0.05). Compared with healthy subjects, the levels of plasma lncRNAs PANDAR, FOXD2-AS1, and SMARCC2 were all significantly higher in gastric cancer patients (P<0.05). These lncRNAs were significantly associated with clinicopathological parameters of gastric cancer, like pathological differentiation, TNM stage, and/or lymph nodes metastasis, and/or invasion depth (P<0.05). The AUC for lncRNA PANDAR was 0.767, for FOXD2-AS1 was 0.700, for SMARCC2 was 0.748, and the AUC of the combinative diagnostic value of these three lncRNAs was 0.839. Adjusted by other variables, these lncRNAs’ expressions were significantly associated with gastric cancer.
Conclusions: Plasma lncRNAs PANDAR, FOXD2-AS1, and SMARCC2 might be appropriate diagnostic biomarkers for gastric cancer.
Keywords: gastric cancer diagnosis, long noncoding RNA, PANDAR, FOXD2-AS1, SMARCC2
Introduction
Gastric cancer remains a common cancer worldwide with a considerable health burden.1 The morbidity and mortality of gastric cancer are still high. It is reported to be responsible for more than 1 million new cases and about 783,000 deaths in 2018 for gastric cancer, which is the fifth most frequently diagnosed cancer and the third leading cause of cancer death.2 Although the technologies for gastric cancer diagnosis have advanced recently, gastric cancer patients’ prognosis is still poor. Approximately 70% gastric cancer patients died from this disease globally after 5 years follow-up.3 Pathological examination for biopsy tissues is the golden standard for gastric cancer diagnosis.4 However, endoscopy is invasive and uncomfortable, which is performed less frequently than blood test. If blood biomarkers are able to diagnose gastric cancer, the detection rate of gastric cancer should be increased effectively. The positive rates of current serum cancer biomarkers for gastric cancer diagnosis are relatively low, like carcinoembryonic antigen (CEA), alpha fetoprotein (AFP), carbohydrate antigen (CA) 199, and CA125.5,6 It is necessary to investigate other novel biomarkers with high sensitivity and specificity.
Noncoding RNAs (ncRNAs) compose up to 75% of the human genome, which play important roles in regulating multiple biological processes.7 Long noncoding RNAs (lncRNAs) are a kind of noncoding RNAs longer than 200 nucleotides and lack protein-coding ability. It has been reported that lncRNA may regulate the tumor formation process.8 Some studies indicate that plasma lncRNAs can serve as potential biomarkers for gastric cancer detection.9 It is still far from clinical application because of the lack of large-range validation and consensus among researchers.
LncRNAs PANDAR, FOXD2-AS1, and SMARCC2 have been reported to be able to promote gastric carcinogenesis.10–12 The previous studies investigated the lncRNA expression profiles and researched the mechanisms of the three lncRNAs in gastric cancer, indicating the three lncRNAs should play important part in gastric carcinogenesis. However, it has not been clear whether lncRNAs PANDAR, FOXD2-AS1, and SMARCC2 in patients’ plasma are potential biomarkers for gastric cancer diagnosis. In this study, we investigated the diagnostic value of plasma lncRNAs PANDAR, FOXD2-AS1, and SMARCC2 in gastric cancer patients comparing with healthy controls.
Materials and methods
Patients and plasma sample collections
We enrolled 109 GC patients and 106 normal healthy subjects between December, 2017 and October, 2018 at The First Hospital of China Medical University. All enrolled patients with GC were diagnosed by histopathological examination after radical resection or endoscopic biopsy. Clinicopathological data were obtained from the medical records. Healthy controls consisted of patients with benign diseases such as hernias, stones, or varicose veins who had no evidence of any stomach disease or other malignancy. All clinical parameters were estimated according to the 8th AJCC/TNM staging system. The present study was approved by the Research Ethics Committee of The First Hospital of China Medical University. We confirmed that all participants provided written informed consent, and that this study was conducted in accordance with the Declaration of Helsinki.
Blood sampling was standardized. All blood samples were collected from each enrolled individual and held in a purple-top EDTA tube before subjects had received any surgery, chemotherapy, or radiation therapy. Plasma samples were separated within 4 hrs after collection following a two-step centrifugation protocol (3,000 g for 10 mins at 4°C, 12,000 g for 10 mins at 4°C) to thoroughly remove cellular nucleic acids, transfer to RNase/DNase-free tubes and immediately frozen and store at −80°C until total RNA extraction.
RNA extraction from plasma
Total RNA was extracted from plasma using the blood total RNA isolation kit (BioTeke). 300 μL plasma was thoroughly mixed with an equal volume of denaturing solution and incubated on ice for 5 mins. 600 μL acid-phenol:chloroform was added and thoroughly mixed via vortex, then centrifuged at 12,000× g for 10 mins at room temperature. The upper aqueous phase was transferred to a fresh RNase-free tube. Washing steps were performed according to the manufacturer’s protocol, and the RNA was finally eluted with 30 μl RNase-free water pre-heated to 65°C. Plasma samples for evaluating the internal control were randomly selected and processed under identical conditions.
Reverse transcription (RT) and real-time PCR
The cDNA was synthesized using a PrimeScript RT reagent kit (TaKaRa) according to the manufacturer’s protocol. The relative expression levels of lncRNAs in all samples were determined using SYBR Premix Ex TaqTM (TaKaRa) on a Light Cycler 480 Real-time PCR system (Roche). The reactions were incubated at 95°C for 30 seconds and then underwent 45 cycles of 95°C for 5 seconds, 59°C for 10 seconds and 72°C for 30 seconds. Samples were analyzed in triplicate, and the products were confirmed by melting curve analysis following each reaction. GAPDH was used as an internal control. The sequences of the primers for real-time PCR are shown in Table S1. All qRT-PCR reactions were performed in triplicate.
Statistical analysis
Statistical analyses were performed by SPSS 22.0 computer software, GraphPad Prism 5, and MedCalc statistical software.ΔCT, which is the difference between CT values of the target and the endogenous reference GAPDH (ΔCT = CTlncRNA-CTGAPDH), was estimated to reflect the expression of lncRNA. Descriptive statistics are given as mean ± s.d., median (minimum, maximum), and percentage. A parametric comparison was performed using Student’s t-test, and a non-parametric comparison was conducted using the Mann–Whitney U test. Chi-square test was used to verify the differences of nominative variables between the two groups. Multivariable analysis of risk factors for gastric cancer was performed using logistic regression analysis. Variables including patients’ gender, age, CEA, AFP, CA125, CA153, and CA199 were adjusted in the multivariable logistic regression analysis. Receiver operating characteristic curve (ROC) and area under curve (AUC) were used to evaluate the diagnostic value of every biomarker. A combined ROC was calculated based on the logistic regression model. P-values less than 0.05 were considered to be statistically significant.
Results
General characteristics of gastric cancer patients compared with normal participants
In the healthy control group, there were a total of 106 individuals, and 55 individuals were female, 51 male. Among them, 80 individuals were younger than 65 years old. In gastric cancer group, there were a total of 109 individuals, and 27 individuals were female, 82 male. Among them, 66 individuals were younger than 65 years old. There were significant differences in both age and gender between these two groups. The levels of serum biomarkers including CEA, AFP, CA125, CA153, and CA199 were shown in Table 1. There were significant differences in CEA and CA153 between the two groups (Table 1). These variables were adjusted in the following logistic regression analysis.
 |
Table 1 General characteristics of gastric cancer patients compared with health controls |
Expression of plasma lncRNAs PANDAR, FOXD2-AS1, and SMARCC2 and its relationship with clinicopathological features in gastric cancer patients
A total of 106 healthy subjects and 109 gastric cancer patients were enrolled in this study. Levels of plasma lncRNAs PANDAR, FOXD2-AS1, and SMARCC2 in these samples were measured using real-time PCR. Compared with healthy subjects, the levels of plasma lncRNAs PANDAR, FOXD2-AS1, and SMARCC2 were all significantly higher in gastric cancer patients (P<0.05). The results were shown in Figure 1.
 |
Figure 1 Expression levels of plasma lncRNAs PANDAR (A), FOXD2-AS1 (B), and SMARCC2 (C) in gastric cancer (GC) and healthy subjects (Normal) evaluated by real-time PCR. *When compared with healthy subjects, a P<0.05 was considered statistically significant. |
Then we analyzed the association between clinicopathological parameters of gastric cancer and the levels of plasma lncRNAs PANDAR, FOXD2-AS1, and SMARCC2 (Table 2). The results showed that for plasma lncRNA PANDAR, the levels were significantly higher in female than in male, higher in poor pathological differentiation than in well and moderate differentiation, higher in TNM III and IV stage than in I and II stage. For lncRNA FOXD2-AS1, the levels were significantly higher in poor pathological differentiation than in well and moderate differentiation, higher in patients with lymph nodes metastasis than without lymph nodes metastasis, higher in TNM III and IV stage than in I and II stage. For lncRNA SMARCC2, the levels were significantly higher in poor pathological differentiation than in well and moderate differentiation, higher in T4 invasion depth than in T1+T2+T3 invasion depth, higher in TNM III and IV stage than in I and II stage.
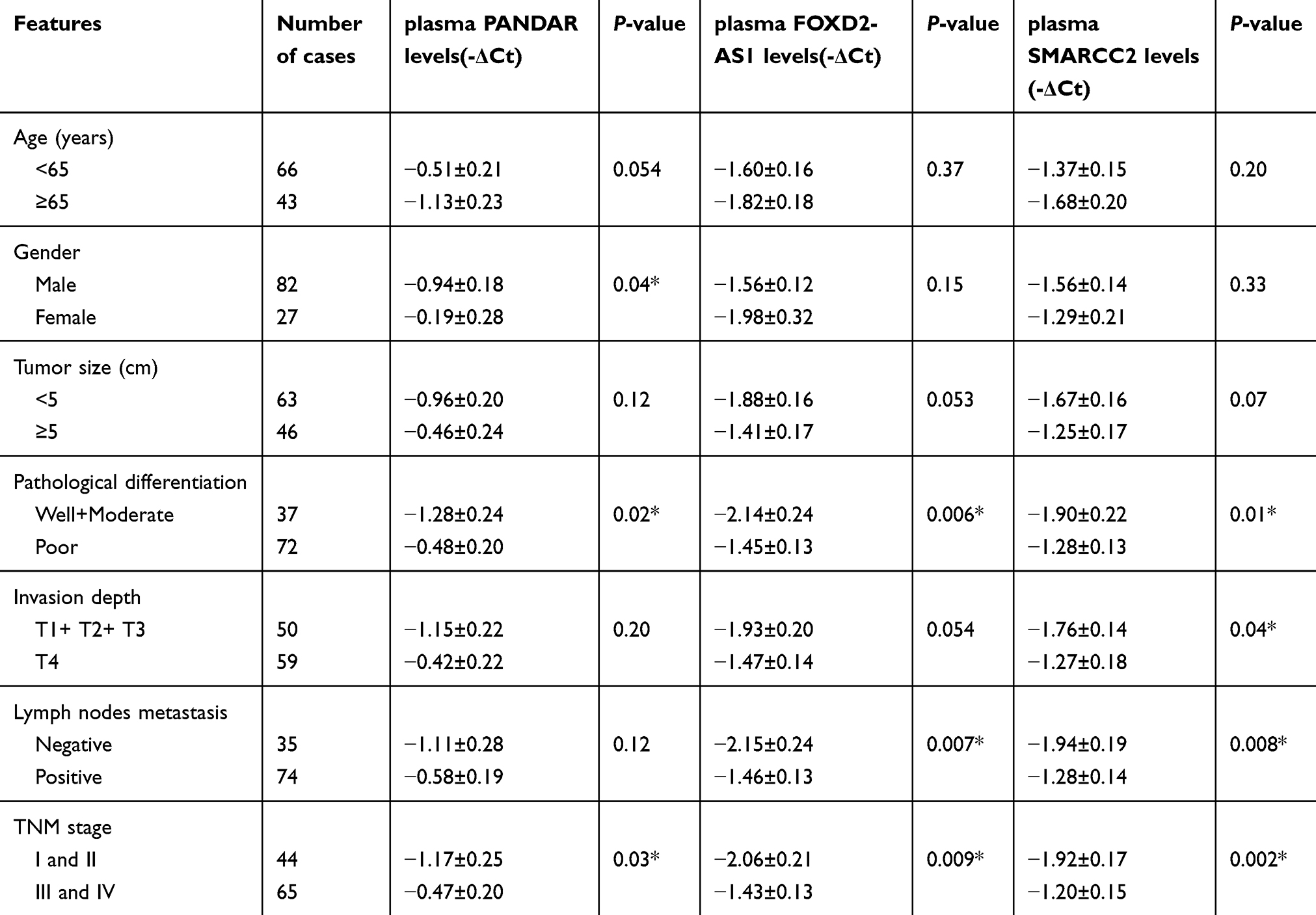 |
Table 2 Correlation between plasma lncRNAs and clinicopathological parameters of gastric cancer (n=109) |
Diagnostic value of plasma lncRNAs PANDAR, FOXD2-AS1, and SMARCC2 for gastric cancer patients
ROC curves were used to evaluate the potential diagnostic capacity of each biomarkers for gastric cancer detection. Relative expression levels of the lncRNAs were obtained using real-time PCR as described previously. The area under the curve (AUC) for CEA was 0.661 (95% CI, 0.592–0.724, P<0.05). The AUC for CA153 was 0.589 (95% CI, 0.520–0.657, P<0.05). The AUC for AFP was 0.536 (95% CI, 0.467–0.604, P>0.05). The AUC for CA125 was 0.558 (95% CI, 0.489–0.626, P>0.05). The AUC for CA199 was 0.533 (95% CI, 0.464–0.602, P>0.05). We calculated the combinative diagnostic value of CEA, CA153, AFP, CA125, and CA199, and the AUC was 0.709 (95% CI, 0.639–0.779, P<0.05). The results are shown in Figure 2.
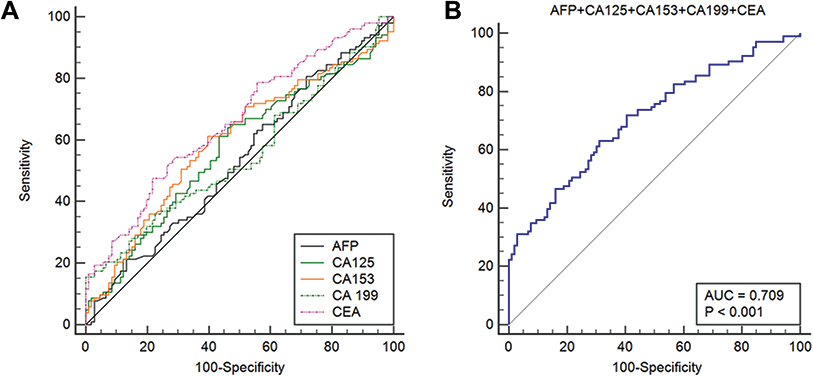 |
Figure 2 The ROC curves of current biomarkers including CEA, CA153, AFP, CA125, and CA199. (A) The ROC curves of each current biomarker. The area under the curve (AUC) for CEA was 0.661. The AUC for CA153 was 0.589. The AUC for AFP was 0.536. The AUC for CA125 was 0.558. The AUC for CA199 was 0.533. (B) The ROC curve of combined CEA, CA153, AFP, CA125, and CA199. The AUC was 0.709, P<0.001. |
For the lncRNAs, the AUCs are generally larger than the above biomarkers. For lncRNA PANDAR, the AUC was 0.767 (95% CI, 0.703–0.822, P<0.05). For lncRNA FOXD2-AS1, the AUC was 0.700 (95% CI, 0.629–0.772, P<0.05). For lncRNA SMARCC2, the AUC was 0.748 (95% CI, 0.682–0.815, P<0.05). We calculated the combinative diagnostic value of the three lncRNAs, and the AUC was 0.839 (95% CI, 0.785–0.894, P<0.05). The results are shown in Figure 3. These results indicated that plasma lncRNAs PANDAR, FOXD2-AS1, and SMARCC2 might be appropriate diagnostic biomarkers for gastric cancer.
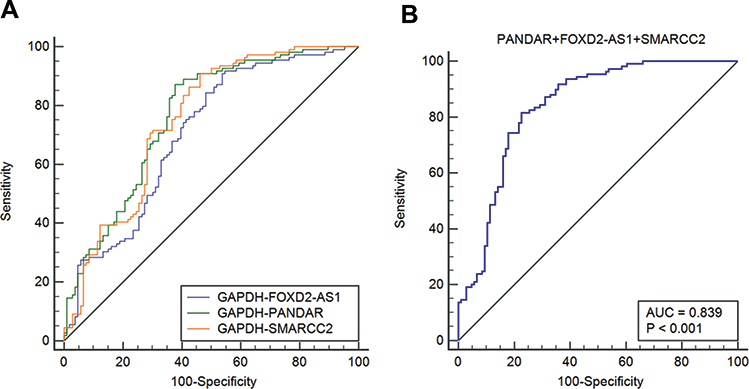 |
Figure 3 The ROC curves of plasma lncRNAs PANDAR, FOXD2-AS1, and SMARCC2. (A) The ROC curves of each plasma lncRNA. The AUC for PANDAR was 0.767. The AUC for FOXD2-AS1 was 0.700. The AUC for SMARCC2 was 0.748. (B) The ROC curve of combined lncRNAs PANDAR, FOXD2-AS1, and SMARCC2. The AUC was 0.839, P<0.001. |
Multivariate analysis of risk factors for gastric cancer
Logistic regression analysis was used to analyze the risk factors for gastric cancer. The 10 variables including gender, age, current biomarkers (CEA, AFP, CA125, CA153, CA199), and the three lncRNAs investigated in this study (PANDAR, FOXD2-AS1, SMARCC2) were analyzed by multivariate logistic regression analysis. The results in Table 3 showed that gender (OR, 0.219; 95% CI, 0.090–0.532; P<0.01), CEA (OR, 0.022; 95% CI, 1.032–1.496; P<0.05), and lncRNA PANDAR (OR, 1.690; 95% CI, 1.313–2,176; P<0.001), FOXD2-AS1 (OR, 1.358; 95% CI, 1.032–1.787; P<0.05), SMARCC2 (OR, 1.681; 95% CI, 1.293–2.186; P<0.001) were significantly associated with gastric cancer.
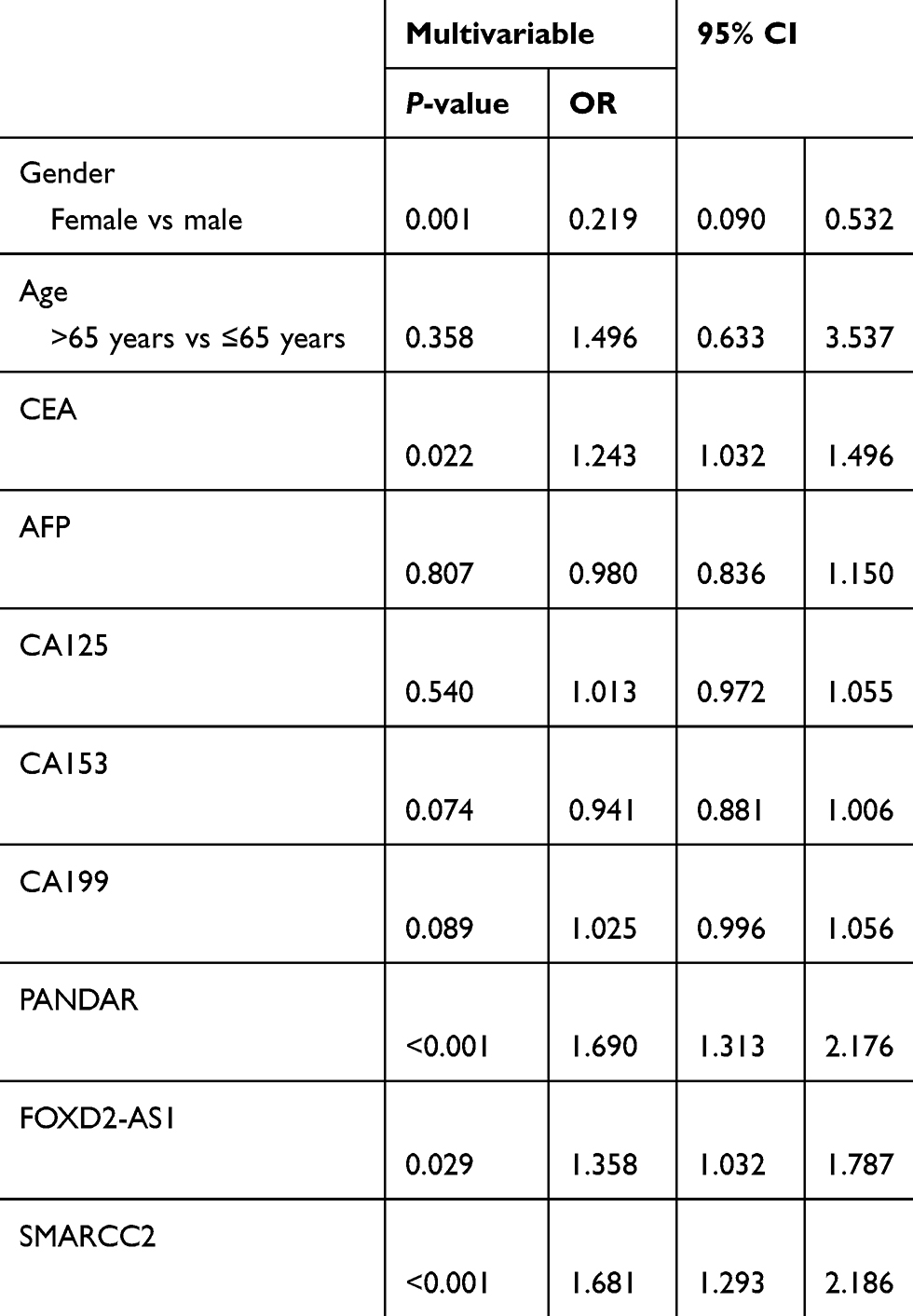 |
Table 3 Multivariable analysis of risk factors for gastric cancer using logistic regression analysis |
Discussion/conclusion
Many patients may be diagnosed with cancer every year in the following years. The number will increase from 14 million a year worldwide in 2012 to 21.6 million a year by 2030. Prompt diagnosis is necessary to improve the patients’ survival. Monitoring the effectiveness of national and regional health systems in treating and caring for patients with cancer becomes ever more crucial.13 Despite a steady decline in gastric cancer incidence and mortality rates observed in developed countries over the past 50 years, gastric cancer is still a considerable global health burden.1,2,14 The incidence rate of gastric cancer is highest in Eastern Asia, including China.2,14 China contributes about 40% of new cases of gastric cancer every year around the world.15 Early detection and timely intervention are considered to be a particularly effective way to fight against cancer. Investigation of the techniques for prompt diagnosis is extremely important for appropriate prevention strategies and prioritization of cancer-control planning.16
In recent years, gastric endoscopy has been rapidly advanced for gastric cancer diagnosis. Endoscopic diagnosis has been revolutionized by dye-based and image-enhanced endoscopic techniques.17 Endoscopic ultrasound-guided needle-based confocal laser endomicroscopy has even been used to improve the diagnostic accuracy.18 However, endoscopy is invasive, uncomfortable, and not suitable for everyone.19 Endoscopy followed by pathological examination are limited by operator’s experience and medical instruments. Serum-based biomarkers are considered to be valuable in cancer diagnosis and monitoring. In our study, we analyzed current serum cancer biomarkers for gastric cancer diagnosis, including CEA, AFP, CA125, CA153, and CA199,20 and their positivity rates showed low, which were consistent with previous studies.21–23 It is urgent to investigate novel biomarkers for diagnosis in gastric cancer patients.21
LncRNAs have been reported to be associated with kinds of diseases,24–26 including cancer phenotypes and carcinogenesis.27–31 Some lncRNAs can regulate the expression of nearby genes through RNA–protein interactions, and other lncRNAs can also act as local regulators.32 LncRNAs play critical roles in genome stability,33 which is considered to be important in carcinogenesis.34 It has been demonstrated that lncRNAs are stable in plasma even in extreme conditions,35 indicating it could be used as diagnostic biomarkers. The relative expression levels of lncRNAs can be measured using real-time PCR. PCR-based testing is widely used for detection of genes in clinics. PCR is often faster and less costly to perform, and can obtain extremely high sensitivities.36 In this study, we measured the expression levels of three plasma lncRNAs using real-time PCR in order to investigate whether plasma lncRNAs PANDAR, FOXD2-AS1, and SMARCC2 could be potential diagnostic biomarkers for gastric cancer.
LncRNA PANDAR (promoter of CDKN1A antisense DNA damage activated RNA) has been reported to be overexpressed in cancer tissues and associated with poor prognosis in many types of human cancer, including colorectal cancer,37 renal cell carcinoma,38 and bladder cancer;39 while in lung cancer the correlation of PANDAR is found to be opposite.40 In gastric cancer, PANDAR could promote the malignant progression by regulating CDKN1A gene transcription in a p53-dependent manner.11 LncRNA FOXD2-AS1 might play important roles in kinds of cancer like glioma,41 colorectal cancer.42 It has been found that upregulation of FOXD2-AS1 could promote carcinogenesis and predict poor prognosis in gastric cancer both in vitro and in vivo. Cell cycle and DNA-replication-related genes should be involved in FOXD2-AS1 function. EphB3 downregulation mediated by Zeste homolog 2 (EZH2) and lysine (K)-specific demethylase 1A (LSD1) might promote FOXD2-AS1 leading to gastric cancer.10 LncRNA SMARCC2 has been reported to be involved in gastric carcinogenesis. LncRNA SMARCC2 might inhibit miR-551b-3p expression. TMPRSS4 is reported to be the target gene of miR-551b-3p,12 and could activate NF-kappa B/MMP-9 signaling and promote gastric cancer cells invasiveness.43 However, no study of PANDAR, FOXD2-AS1, and SMARCC2 in gastric cancer plasma has been performed.
In this study, based on the feasibility of real-time PCR testing on plasma lncRNAs and the carcinogenic functions of PANDAR, FOXD2-AS1, and SMARCC2 in gastric carcinogenesis, the levels of three lncRNAs in gastric cancer patients’ plasma were measured using real-time PCR. Our results showed that compared with healthy controls, the levels of plasma lncRNAs PANDAR, FOXD2-AS1, and SMARCC2 were all significantly higher in gastric cancer patients, indicating that these lncRNAs might be valuable for gastric cancer diagnosis. To confirm the hypothesis, diagnostic value of every marker was evaluated using ROC. Our results showed that the AUC of every lncRNA was significantly larger than current serum cancer biomarkers, including CEA, AFP, CA125, CA153, and CA199. The AUC of combinative diagnostic value of the three lncRNAs was up to 0.839, indicating that these lncRNAs are potential biomarkers for gastric cancer diagnosis. To further analyze the risk factors for gastric cancer, multivariable analysis was performed. As well known, gender in our study also showed to be significantly associated with gastric cancer.1 Male might be an independent risk factor for gastric cancer. We did not find the association of age and gastric cancer. Adjusted by gender and age, there were four variables which would be independent risk factors for gastric cancer, including CEA, PANDAR, FOXD2-AS1, and SMARCC2. Elevation of the four markers would independently increase gastric cancer risk. LncRNAs could serve as novel targets for gastric cancer diagnosis.35,44
It is necessary to state that in this study, we used GAPDH as the reference gene. Some reference genes including GAPDH might be deregulated in cancer tissues.45 While in recent researches, GAPDH is still used as a common reference gene.46,47 In the future, the re-recognition of reference genes might be performed with the development of technology and instrument.
In summary, our results showed that lncRNAs PANDAR, FOXD2-AS1, and SMARCC2 in plasma could be used as novel diagnostic biomarkers for gastric cancer detection. The combination of these three lncRNAs could provide a high enough diagnostic accuracy. In this study, we did not have the clinical follow-up survey yet, leading to the lack of prognostic value of the lncRNAs. Further investigation should be performed to complete the follow-up process to study the prognostic value of these biomarkers. As some of these lncRNAs play important effects in many kinds of cancer except for gastric cancer, it should be further studied to identify the specific diagnostic value of these lncRNAs for gastric cancer detection.
Statement of ethics
The study protocol has been approved by the Research Ethics Committee of The First Hospital of China Medical University on human research.
Acknowledgments
This study was funded by the National Natural Science Foundation of China (Grant No. 81700496 and 81870386), and the Beijing Key Laboratory for Helicobacter pylori Infection and Upper Gastrointestinal Diseases (No. BZ0371).
Author contributions
Ziwei Yang performed the research examinations. Yanfei Sun and Rongfeng Liu collated the data. Yanyan Shi performed the statistical analyses and wrote the manuscript. Yanyan Shi and Shigang Ding designed the research. All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ajani JA, Lee J, Sano T, Janjigian YY, Fan D, Song S. Gastric adenocarcinoma. Nat Rev Dis Primers. 2017;3:17036. doi:10.1038/nrdp.2017.36
2. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424. doi:10.3322/caac.21492
3. Verdecchia A, Francisci S, Brenner H, et al. Recent cancer survival in Europe: a 2000-02 period analysis of EUROCARE-4 data. Lancet Oncol. 2007;8:784–796. doi:10.1016/s1470-2045(07)70246-2
4. Yamada S, Hatta W, Gotoda T, et al. Different risk factors between early and late cancer recurrences in patients without additional surgery after noncurative endoscopic submucosal dissection for early gastric cancer. Gastrointest Endosc. 2018. doi:10.1016/j.gie.2018.11.015
5. Shimada H, Noie T, Ohashi M, Oba K, Takahashi Y. Clinical significance of serum tumor markers for gastric cancer: a systematic review of literature by the task force of the Japanese gastric cancer association. Gastric Cancer. 2014;17:26–33. doi:10.1007/s10120-013-0259-5
6. Feng F, Tian Y, Xu G, et al. Diagnostic and prognostic value of CEA, CA19-9, AFP and CA125 for early gastric cancer. BMC Cancer. 2017;17:737. doi:10.1186/s12885-017-3738-y
7. Wang KC, Chang HY. Molecular mechanisms of long noncoding RNAs. Mol Cell. 2011;43:904–914. doi:10.1016/j.molcel.2011.08.018
8. Hu, G. D., Wang CX, Wang HY, et al. Long noncoding RNA CCAT2 functions as a competitive endogenous RNA to regulate FOXC1 expression by sponging miR-23b-5p in lung adenocarcinoma. J Cell Biochem. 2018. doi:10.1002/jcb.28077
9. Liu J, Wang J, Song Y, et al. A panel consisting of three novel circulating lncRNAs, is it a predictive tool for gastric cancer? J Cell Mol Med. 2018;22:3605–3613. doi:10.1111/jcmm.13640
10. Xu TP, Wang W-Y, Ma P, et al. Upregulation of the long noncoding RNA FOXD2-AS1 promotes carcinogenesis by epigenetically silencing EphB3 through EZH2 and LSD1, and predicts poor prognosis in gastric cancer. Oncogene. 2018;37:5020–5036. doi:10.1038/s41388-018-0308-y
11. Liu J, Ben Q, Lu E, et al. Long noncoding RNA PANDAR blocks CDKN1A gene transcription by competitive interaction with p53 protein in gastric cancer. Cell Death Dis. 2018;9:168. doi:10.1038/s41419-017-0246-6
12. Yuan H, Chen Z, Bai S, et al. Molecular mechanisms of lncRNA SMARCC2/miR-551b-3p/TMPRSS4 axis in gastric cancer. Cancer Lett. 2018;418:84–96. doi:10.1016/j.canlet.2018.01.032
13. Allemani C, Matsuda T, Di Carlo V, et al. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet (London, England). 2018;391:1023–1075. doi:10.1016/s0140-6736(17)33326-3
14. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65:87–108. doi:10.3322/caac.21262
15. Torre LA, Siegel RL, Ward EM, Jemal A. Global cancer incidence and mortality rates and trends – an update. Cancer Epidemiol Biomarkers Prev. 2016;25:16–27. doi:10.1158/1055-9965.Epi-15-0578
16. Vineis P, Wild CP. Global cancer patterns: causes and prevention. Lancet (London, England). 2014;383:549–557. doi:10.1016/s0140-6736(13)62224-2
17. Uedo N, Yao K. Endoluminal diagnosis of early gastric cancer and its precursors: bridging the gap between endoscopy and pathology. Adv Exp Med Biol. 2016;908:293–316. doi:10.1007/978-3-319-41388-4_14
18. Zhang, MM, Zhong N, Wang X, et al. Endoscopic ultrasound-guided needle-based confocal laser endomicroscopy for diagnosis of gastric subepithelial tumors: a pilot study. Endoscopy. 2018. doi:10.1055/a-0790-8436
19. Park JY, von Karsa L, Herrero R. Prevention strategies for gastric cancer: a global perspective. Clin Endosc. 2014;47:478–489. doi:10.5946/ce.2014.47.6.478
20. Sakamoto K, Haga Y, Yoshimura R, Egami H, Yokoyama Y, Akagi M. Comparative effectiveness of the tumour diagnostics, CA 19-9, CA 125 and carcinoembryonic antigen in patients with diseases of the digestive system. Gut. 1987;28:323–329. doi:10.1136/gut.28.3.323
21. Subbannayya Y, Mir SA, Renuse S, et al. Identification of differentially expressed serum proteins in gastric adenocarcinoma. J Proteomics. 2015;127:80–88. doi:10.1016/j.jprot.2015.04.021
22. Lim JB, Kim DK, Chung HW. Clinical significance of serum thymus and activation-regulated chemokine in gastric cancer: potential as a serum biomarker. Cancer Sci. 2014;105:1327–1333. doi:10.1111/cas.12505
23. Toiyama Y, Tanaka K, Kitajima T, et al. Serum angiopoietin-like protein 2 as a potential biomarker for diagnosis, early recurrence and prognosis in gastric cancer patients. Carcinogenesis. 2015;36:1474–1483. doi:10.1093/carcin/bgv139
24. Parikshak NN, Swarup V, Belgard TG, et al. Genome-wide changes in lncRNA, splicing, and regional gene expression patterns in autism. Nature. 2016;540:423–427. doi:10.1038/nature20612
25. Engreitz JM, Haines JE, Perez EM, et al. Local regulation of gene expression by lncRNA promoters, transcription and splicing. Nature. 2016;539:452–455. doi:10.1038/nature20149
26. Kotzin JJ, Spencer SP, McCright SJ, et al. The long non-coding RNA morrbid regulates bim and short-lived myeloid cell lifespan. Nature. 2016;537:239–243. doi:10.1038/nature19346
27. Cancer Genome Altas Research Network, Albert Einstein College of Medicine, Analytical Biological Services, et al. Integrated genomic and molecular characterization of cervical cancer. Nature. 2017;543:378–384. doi:10.1038/nature21386
28. Hua JT, Ahmed M, Guo H, et al. Risk SNP-mediated promoter-enhancer switching drives prostate cancer through lncRNA PCAT19. Cell. 2018;174:564–575.e518. doi:10.1016/j.cell.2018.06.014
29. Cho SW, Xu J, Sun R, et al. Promoter of lncRNA gene PVT1 Is a tumor-suppressor DNA boundary element. Cell. 2018;173:1398–1412.e1322. doi:10.1016/j.cell.2018.03.068
30. Huarte M. The emerging role of lncRNAs in cancer. Nat Med. 2015;21:1253–1261. doi:10.1038/nm.3981
31. Zhuo, W., et al. Long non-coding RNA GMAN, upregulated in gastric cancer tissues, is associated with metastasis in patients and promotes translation of ephrin A1 by competitively binding GMAN-AS. Gastroenterology. 2018. doi:10.1053/j.gastro.2018.10.054
32. Joung J, Engreitz JM, Konermann S, et al. Genome-scale activation screen identifies a lncRNA locus regulating a gene neighbourhood. Nature. 2017;548:343–346. doi:10.1038/nature23451
33. Munschauer M, Nguyen CT, Sirokman K, et al. The NORAD lncRNA assembles a topoisomerase complex critical for genome stability. Nature. 2018;561:132–136. doi:10.1038/s41586-018-0453-z
34. Li M, Yu X. The role of poly(ADP-ribosyl)ation in DNA damage response and cancer chemotherapy. Oncogene. 2015;34:3349–3356. doi:10.1038/onc.2014.295
35. Zhang K, Shi H, Xi H, et al. Genome-wide lncRNA microarray profiling identifies novel circulating lncRNAs for detection of gastric cancer. Theranostics. 2017;7:213–227. doi:10.7150/thno.16044
36. Bertoli, H. K., Rasmussen CL, Sand FL, et al. Human papillomavirus and p16 in squamous cell carcinoma and intraepithelial neoplasia of the vagina. Int J Cancer. 2018. doi:10.1002/ijc.32078
37. Rivandi M, Pasdar A, Hamzezadeh L, et al. The prognostic and therapeutic values of long noncoding RNA PANDAR in colorectal cancer. J Cell Physiol. 2019;234:1230–1236. doi:10.1002/jcp.27136
38. Wu Y, Wang Y-Q, Weng W-W, et al. A serum-circulating long noncoding RNA signature can discriminate between patients with clear cell renal cell carcinoma and healthy controls. Oncogenesis. 2016;5:e192. doi:10.1038/oncsis.2015.48
39. Zhan Y, Lin J, Liu Y, et al. Up-regulation of long non-coding RNA PANDAR is associated with poor prognosis and promotes tumorigenesis in bladder cancer. J Exp Clin Cancer Res. 2016;35:83. doi:10.1186/s13046-016-0354-7
40. Han L, Zhang E-B, Yin -D-D, et al. Low expression of long noncoding RNA PANDAR predicts a poor prognosis of non-small cell lung cancer and affects cell apoptosis by regulating Bcl-2. Cell Death Dis. 2015;6:e1665. doi:10.1038/cddis.2015.30
41. Shen, F., Chang H, Gao G, et al. Long noncoding RNA FOXD2-AS1 promotes glioma malignancy and tumorigenesis via targeting miR-185-5p/CCND2 axis. J Cell Biochem. 2018. doi:10.1002/jcb.28208
42. Zhu Y, Qiao L, Zhou Y, Ma N, Wang C, Zhou J. Long non-coding RNA FOXD2-AS1 contributes to colorectal cancer proliferation through its interaction with microRNA-185-5p. Cancer Sci. 2018;109:2235–2242. doi:10.1111/cas.13632
43. Jin J, Shen X, Chen L, Bao LW, Zhu LM. TMPRSS4 promotes invasiveness of human gastric cancer cells through activation of NF-kappaB/MMP-9 signaling. Biomed Pharmacother. 2016;77:30–36. doi:10.1016/j.biopha.2015.11.002
44. Zhang E, He X, Zhang C, et al. A novel long noncoding RNA HOXC-AS3 mediates tumorigenesis of gastric cancer by binding to YBX1. Genome Biol. 2018;19:154. doi:10.1186/s13059-018-1523-0
45. Guo C, Liu S, Sun MZ. Novel insight into the role of GAPDH playing in tumor. Clin Transl Oncol. 2013;15:167–172. doi:10.1007/s12094-012-0924-x
46. Zhao R, Zhang Y, Zhang X, et al. Exosomal long noncoding RNA HOTTIP as potential novel diagnostic and prognostic biomarker test for gastric cancer. Mol Cancer. 2018;17:68. doi:10.1186/s12943-018-0817-x
47. Ichikawa W, Terashima M, Ochiai A, et al. Impact of insulin-like growth factor-1 receptor and amphiregulin expression on survival in patients with stage II/III gastric cancer enrolled in the adjuvant chemotherapy trial of S-1 for gastric cancer. Gastric Cancer. 2017;20:263–273. doi:10.1007/s10120-016-0600-x
Supplementary material
 |
Table S1 Primers for lncRNAs |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.