Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Plasma Fetuin-B Levels are Associated with Nervous Symptoms and Conduction Velocity in Patients with Painful DPN
Authors Lin K ![]() , Wang X, Gu T, Feng K, Zeng W, Yang L
, Wang X, Gu T, Feng K, Zeng W, Yang L
Received 11 August 2024
Accepted for publication 24 January 2025
Published 13 March 2025 Volume 2025:18 Pages 785—793
DOI https://doi.org/10.2147/DMSO.S485853
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rebecca Baqiyyah Conway
Ke Lin,1,* Xiaocui Wang,2,* Tao Gu,3,* Keduo Feng,1 Wang Zeng,1 Liu Yang1
1Department of Neurology, Chongqing University Central Hospital, Chongqing Emergency Medical Center, Chongqing, People’s Republic of China; 2Department of Endocrinology, Translational Research of Diabetes Key Laboratory of Chongqing Education Commission of China, Second Affiliated Hospital of Army Medical University, Chongqing, People’s Republic of China; 3Department of Radiology, Second Affiliated Hospital of Army Medical University, Chongqing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ke Lin; Liu Yang, Department of Neurology, Chongqing University Central Hospital, Chongqing Emergency Medical Center, Chongqing, People’s Republic of China, Email [email protected]; [email protected]
Aim: To assess the plasma concentrations of the novel hepatokine fetuin-B in individuals with type 2 diabetes with or without diabetic peripheral neuropathy (DPN), and to evaluate the relationship among fetuin-B levels, nervous function, and metabolic parameters.
Methods: A total of 333 participants were recruited and divided into three groups: DPN, painful DPN (pDPN), and non-DPN. Metabolic parameters, peripheral neuropathy-associated indices, and general biochemical parameters were also measured.
Results: Compared with the non-DPN group, general parameters, including age, SBP, BUN, Cr, and ALT, were significantly higher in the DPN and pDPN groups, and FPG, HbA1c, TC, TG, LDL, BUN, Cr, and UA levels were higher in the pDPN group. The neuropathy symptom score (NSS), neuropathy disability score (NDS), and Douleur Neuropathique en 4 Questions (DN4) were highest in the pDPN group, followed by the DPN group, and lowest in the non-DPN group. Moreover, fetuin B levels showed the same trends as peripheral neuropathy indices. Additionally, oxidative stress markers showed a decrease in total antioxidant capacity (TAC) and an increase in malondialdehyde (MDA) across all groups, with the most pronounced changes observed in pDPN patients. Bivariate correlation analysis showed that fetuin B levels were positively correlated with FPG, TC, LDL, NSS, NDS, DN4, and MDA levels, and negatively associated with TAC after adjusting for age and sex. Furthermore, nerve conduction velocity, including MLT, MRT, SRS, and SLT, showed decreasing trends among tertiles of fetuin B levels.
Conclusion: The current study suggests that circulating fetuin-B levels may be associated with the progression of pDPN and highlights the effects of hepatokine-mediated liver-to-peripheral nervous system crosstalk in DPN.
Keywords: diabetes, diabetic peripheral neuropathy, fetuin-B, glucose, lipids
Introduction
The diabetes pandemic is growing worldwide; 537 million adults are living with diabetes, and this number is predicted to rise to 783 million by 2045 according to the IDF Diabetes Atlas.1 As a common complication of diabetes, peripheral neuropathy affected approximately 30–51% of people with diabetes and is defined as symmetrical, length-dependent sensorimotor polyneuropathy induced by diabetes.2,3 Depending on the affected nerves, diabetic peripheral neuropathy (DPN) symptoms include numbness in a stocking-glove pattern that progresses proximally from the feet and hands, tingling, and/or burning in the extremities.3,4 Some patients manifesting distressing painful neuropathic symptoms are defined as having painful DPN (pDPN), which affects 13–35% of patients with diabetes and has a notable impact on daily functioning, depression, sleep disturbance, financial instability, and decreased quality of life.4,5 However, there is still a lack of effective interventions for pDPN in clinical practice, owing to a lack of understanding of the mechanisms and timely diagnosis.
Several risk factors have been proposed for pDPN, including hyperglycemia, dyslipidemia, and oxidative stress; thus, appropriate therapies have been applied in routine clinical practice.4,6 However, the occurrence and development of pDPN have not been effectively curbed, indicating that the underlying pathogenesis requires urgent elucidation. Hepatokine fetuin-B is secreted by hepatocytes and is released in large amounts in patients with diabetes. It is reported that fetuin B promotes insulin resistance, impairs glucose metabolism, and exacerbates liver steatosis.7,8 Recently, fetuin-B has been reported to participate in the development of nervous system diseases such as Alzheimer’s disease and ischemic stroke by increasing oxidative stress.9,10 In addition to the central nervous system, hepatokines such as FGF21 also play a regulatory role in the peripheral nervous system.11 These findings suggest that fetuin-B is associated with DPN.
To elucidate this potential association, we assessed plasma fetuin-B concentration in patients with or without painful DPN and DNP. Our study found that patients with pDPN had the highest levels of plasma fetuin-B, followed by patients with DPN and non-DPN. Moreover, total antioxidant capacity (TAC) decreased and malondialdehyde (MDA, a marker of oxidative stress) increased in the DPN group and was highest in the pDPN group. In addition, plasma fetuin-B levels were positively correlated with FPG, TC, LDL, NSS, NDS, DN4, and MDA and negatively associated with TAC after adjusting for age and sex. Furthermore, nerve conduction velocity, including MLT, MRT, SRS, and SLT, showed increasing trends among tertiles of fetuin-B levels. These findings indicate a strong correlation between plasma fetuin-B level and DPN severity.
Methods
Subjects and Exclusion Criteria
A total of 333 patients with type 2 diabetes mellitus (T2DM) were recruited for this study. Of these, 139 T2DM patients were without DPN, 93 patients were diagnosed with DPN (without pDPN), and 101 patients were diagnosed with pDPN. T2DM was diagnosed according to the 1999 diagnostic criteria of the World Health Organization using oral glucose tolerance tests (OGTT). DPN was diagnosed according to the criteria established by the Toronto Diabetic Neuropathy Expert Group, as outlined in the article “Diabetic neuropathies: update on definitions, diagnostic criteria, estimation of severity, and treatments”.12 The diagnostic criteria for confirmed DPN involved a comprehensive assessment that included the presence of abnormalities in nerve conduction velocity (NCV, sensory nerve conduction velocity (SNCV) below 40 m/s, motor nerve conduction velocity (MNCV) below 50 m/s were considered indicative of significant neuropathy), neuropathy symptom scores (NSS, ranging from 0 to 9, with a threshold set at a value greater than 5 to define the presence of neuropathy), and neuropathy disability scores (NDS, ranging from 0 to 10, with neuropathy defined as a value exceeding 6). The clinical diagnosis of pDPN followed the NeuPSIG grading system and was customized for painful DPN.13,14 It was identified by pain in both feet and legs, sensory signs in the feet and legs, the presence of abnormal NCV, and a Douleur Neuropathique en 4 Questions (DN4) score of ≥ 3/7 (which exhibits a sensitivity and specificity of 84% in identifying clinically confirmed pDPN).15 All the patients received oral antidiabetic agents and/or () insulin therapies according to their physician’s prescription.
The exclusion criteria were as follows: (1) acute diabetic complications; (2) hypertension at stage 2 or beyond (resting blood pressure ≥ 160/100 mmHg); (3) neuropathy attributed to alternative factors, including but not limited to cervical and lumbar spine lesions (nerve root compression, spinal canal stenosis, or cervical and lumbar degeneration), cerebral infarction, and Guillain-Barré syndrome (GBS); (4) arteriovenous vascular disease (venous thrombosis or lymphangitis); (5) individual affected by neurotoxicity resulting from chemotherapy drugs or nerve damage associated with metabolic toxins due to renal insufficiency; (6) presence of acute inflammatory diseases indicated by clinical symptoms of infection or a blood leukocyte count exceeding 7 X 109/L; (7) ongoing renal or hepatic disease and recent systemic corticosteroid treatment within the last 6 months; and (8) currently pregnancy or breastfeeding. The Ethics Committee of Chongqing University Central Hospital approved all the study protocols (2021–55), and each participant signed an informed consent form. This study complied with the principles of the Declaration of Helsinki.
Clinical Parameters Measurements
The clinical parameters of the participants were evaluated following protocols established in previous studies.16 Specifically, height, weight, and blood pressure were measured by trained investigators using standardized procedures. Height was recorded to the nearest 0.1 cm, body weight with an accuracy of ± 0.2 kg, and blood pressure was measured twice using a standard mercury manometer. Subsequently, body mass index (BMI) was calculated using a standardized formula: weight in kilograms (kg) divided by height in meters squared (m2).
Blood samples were obtained after overnight fasting to assess various biochemical markers including hemoglobin A1c (HbA1c), triglyceride (TG), total cholesterol (TC), high-density lipoprotein cholesterol (HDL-c), low-density lipoprotein cholesterol (LDL-c), blood urea nitrogen (urea), creatinine (Cr), uric acid (UA), alanine aminotransferase (ALT), aspartate aminotransferase (AST), total bilirubin (TBIL), and direct bilirubin (DBIL). All blood samples were separated within 30 min and then frozen at −20°C until use in this study, within a one-month period. Biochemical analyses were conducted using a biochemical autoanalyzer (Beckman CX-7 Biochemical Autoanalyzer; Brea, CA, USA).
For oxidative stress status evaluation, total antioxidant capacity and malondialdehyde (MAD, a biomarker of oxidative stress) were assessed using commercial kits according to the manufacturer’s instructions (Solarbio, Beijing, China).
Neuropathy Symptom Score/Neuropathy Disability Score (NSS/NDS) Evaluation
NSS and NDS assessments were conducted for each participant in accordance with methodologies established in previous studies.16,17 The NSS, employed for the evaluation of neuropathic symptoms, encompasses a comprehensive range of symptoms, including unsteadiness in walking, numbness, burning or tingling sensations, fatigue, cramping, aching, and prickling. The scoring scale for NSS ranges from 0 to 9, with a threshold set at a value greater than 5 to define the presence of neuropathy. The NDS evaluation comprised assessments of the ankle reflex, vibration perception, temperature sensation, and pinprick responses. The scoring scale for NDS ranges from 0 to 10, with neuropathy defined as a score exceeding 6.
Nerve Conduction Testing
Nerve conduction testing was performed using electromyography/evoked potential equipment (NDI-092, Shanghai, China) according to the manufacturer’s protocols and guidelines. The testing procedures were uniformly administered by a single experienced neurologist, ensuring methodological consistency and minimizing inter-operator variability. Bilateral tibial and peroneal nerve motor conduction velocities and bilateral tibial and sural nerve sensory conduction velocities were assessed in current study.
Plasma Fetuin-B Concentration Assessment
Plasma concentrations of fetuin-B were quantified using ELISA, employing a specific antibody targeting fetuin-B sourced from Proteintech (Wuhan, China), in accordance with established and standardized protocols. To ensure the robustness and accuracy of the results, all samples underwent duplicate analyses, with repetitions initiated in cases in which a disparity exceeding 15% between duplicate measurements was identified. The ELISA procedure demonstrated negligible cross-reactivity and interference, confirming the specificity and reliability of the assay for the accurate measurement of plasma fetuin-B concentrations.
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics for Windows, version 22 (IBM) and GraphPad Prism 8.0 for figure generation. Normality testing of all quantitative variables was conducted using the Shapiro–Wilk test in SPSS. Variables that followed a normal distribution are presented as means ± standard deviations (SD), while non-normally distributed data are expressed as medians and interquartile ranges (IQR). Comparisons between the three groups were performed using one-way analysis of variance (ANOVA) for normally distributed data, and the Mann–Whitney U-test was applied for non-normally distributed data. Post hoc pairwise comparisons were conducted using Tukey’s test for normally distributed data or the Bonferroni test for non-normally distributed data.
Bivariate correlation analyses were conducted using Spearman correlation test with partial correlation adjustments for age and sex. Multiple logistic regression analysis was performed to evaluate the relationship between fetuin-B levels and pDPN or its parameters, which were adjusted for potential confounders including MAD, TAC, FPG, HbA1c, TC, and LDL-c. Statistical significance was set at a threshold of P < 0.05.
Results
Patients’ General Characteristics, Glucose, Lipid, Renal and Hepatic Profiles and Oxidative Status
As shown in Table 1, 333 patients with diabetes were recruited for the current study, including 194 (58.3%) males and 139 (41.7%) females. The participants were divided into three groups (non-DPN, DPN, and pDPN), and the average ages of the DPN and pDPN groups were older than those of the non-DPN group but showed no difference between the DPN and pDPN groups. In addition, the SBP was higher in the pDPN group than in the non-DPN group. The remaining general parameters, such as DBP and BMI, were similar across all the three groups. As for glucose and lipid indices, FPG, HbA1c, and lipid profiles, including TC, TG, and LDL-c, were higher in the pDPN group than in the DPN and non-DPN groups (P < 0.05, P < 0.01, respectively; Table 1). For renal and liver parameters, the pDPN group showed the highest levels of urea, creatinine, and UA (P < 0.05, P < 0.01, Table 1), while the non-DPN group showed the highest level of ALT (P < 0.05, P < 0.01, Table 1). The remaining parameters showed no significant differences among the three groups. As for peripheral neuropathy-associated indices, NDS, NSS, and ND4 showed similar trends among these groups, that is, the highest in the pDPN group, followed by the DPN group, and the lowest in the non-DPN group (P < 0.05, P < 0.01, Table 1). As mentioned above, apart from glucose and lipid dysregulation, oxidative stress is also considered a potential mechanism for pDPN. Therefore, we assessed the oxidative status of all participants. As shown in Figure 1, TAC levels decreased and MAD levels increased in the three groups, indicating that stronger oxidative stress was induced in patients with DPN, especially in those with pain.
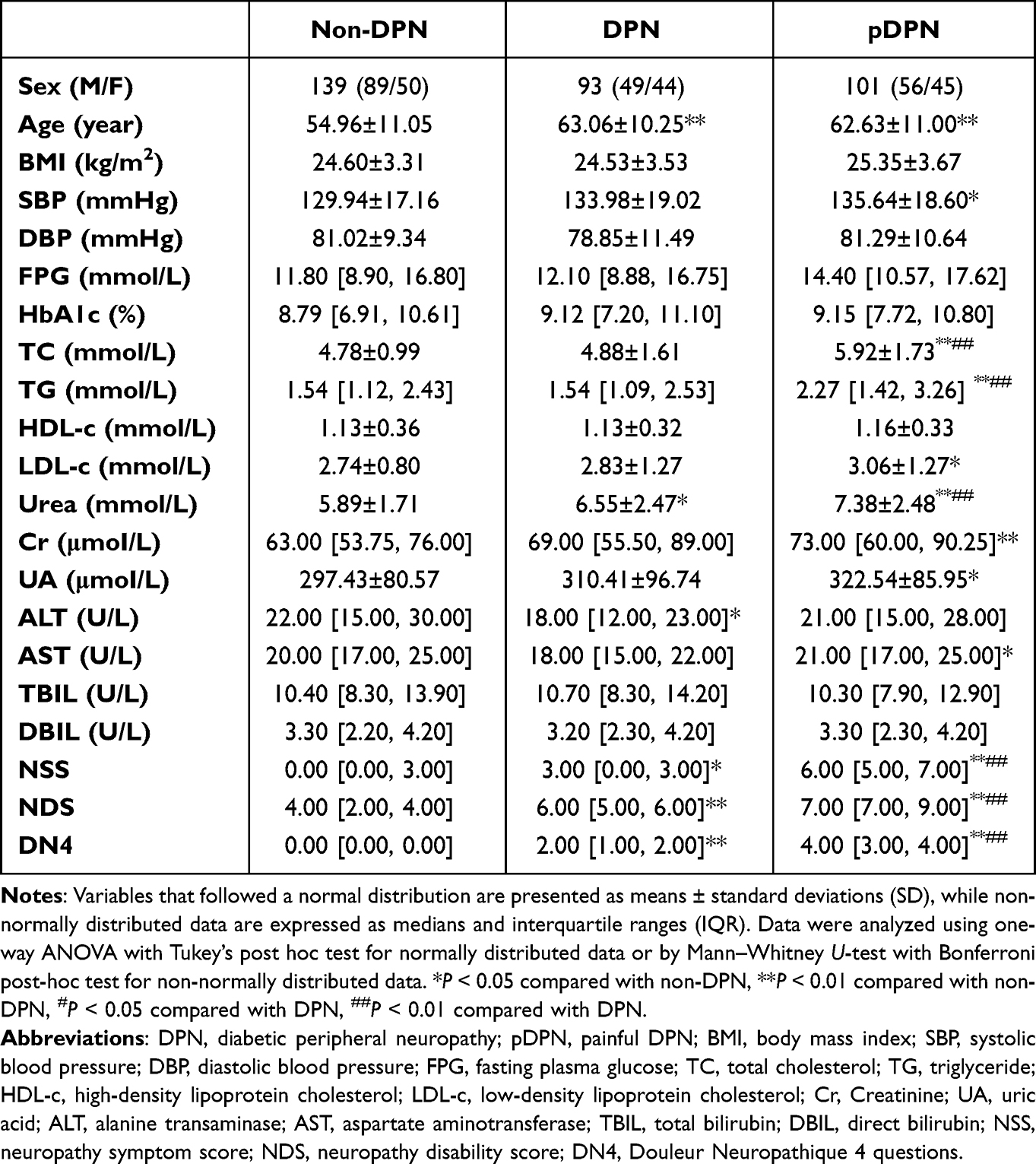 |
Table 1 Clinical Characteristics of the Three Groups |
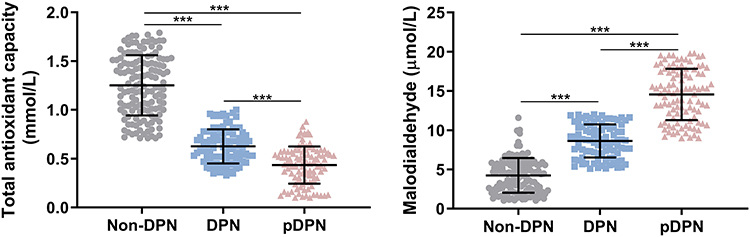 |
Figure 1 Circulating antioxidative and oxidative stress status in diabetic controls, DPN, and pDPN patients. Total antioxidant capacity (TAC) and malondialdehyde (MDA) levels were measured in all participants to assess the antioxidative or oxidative stress status. Data are presented as mean ± SD. Data were analyzed using one-way ANOVA with Tukey’s post hoc test. ***P < 0.001. n = 139, 92, 101 in the non-DPN, DPN, and pDPN groups, respectively. |
Plasma Fetuin-B Concentrations Were Positively Correlated with Neuropathy Symptoms and Were Negatively Related to Nerve Conduction Velocity
As shown in Figure 2, plasma fetuin-B levels were highest in the pDPN group, followed by the DPN group, and were lowest in the T2DM group. Spearman correlation analyses were conducted to further assess the interrelationships between fetuin-B concentrations and DPN. The results showed that plasma fetuin-B levels were positively associated with neuropathy symptom indices NSS, NDS and DN4, and were negatively correlated with nerve conduction velocity, including MLT, MRT, SRS, and SLT (Table 2). After adjusting for age and sex, these correlations remained significant (Table 2). Moreover, after dividing all participants by fetuin-B levels, both motor and sensory conduction velocities showed decreasing trends among the tertiles of fetuin-B levels (Table 3). These results indicated a strong link between fetuin-B and neuropathy.
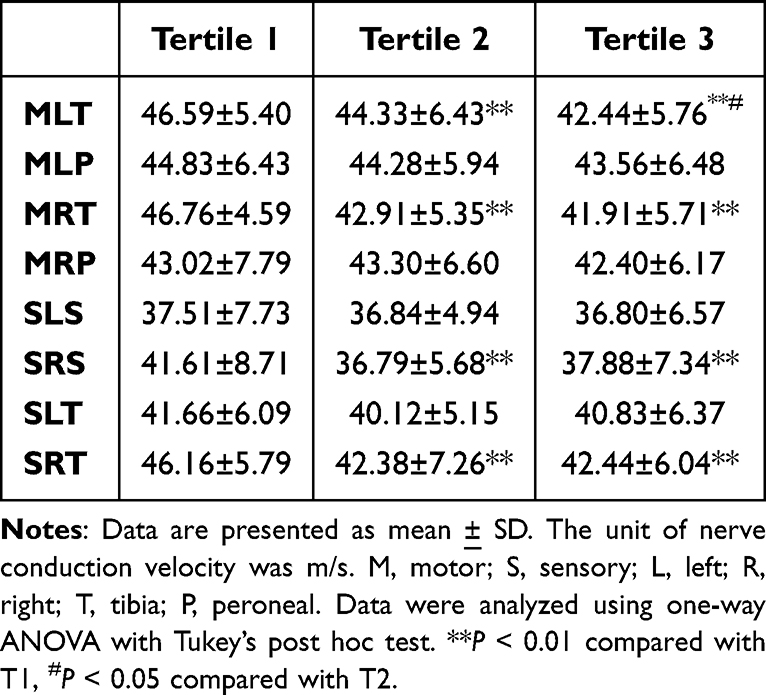 |
Table 2 Subjects with Nerve Conduction Velocity Were Divided According to Plasma Fetuin-B Tertiles |
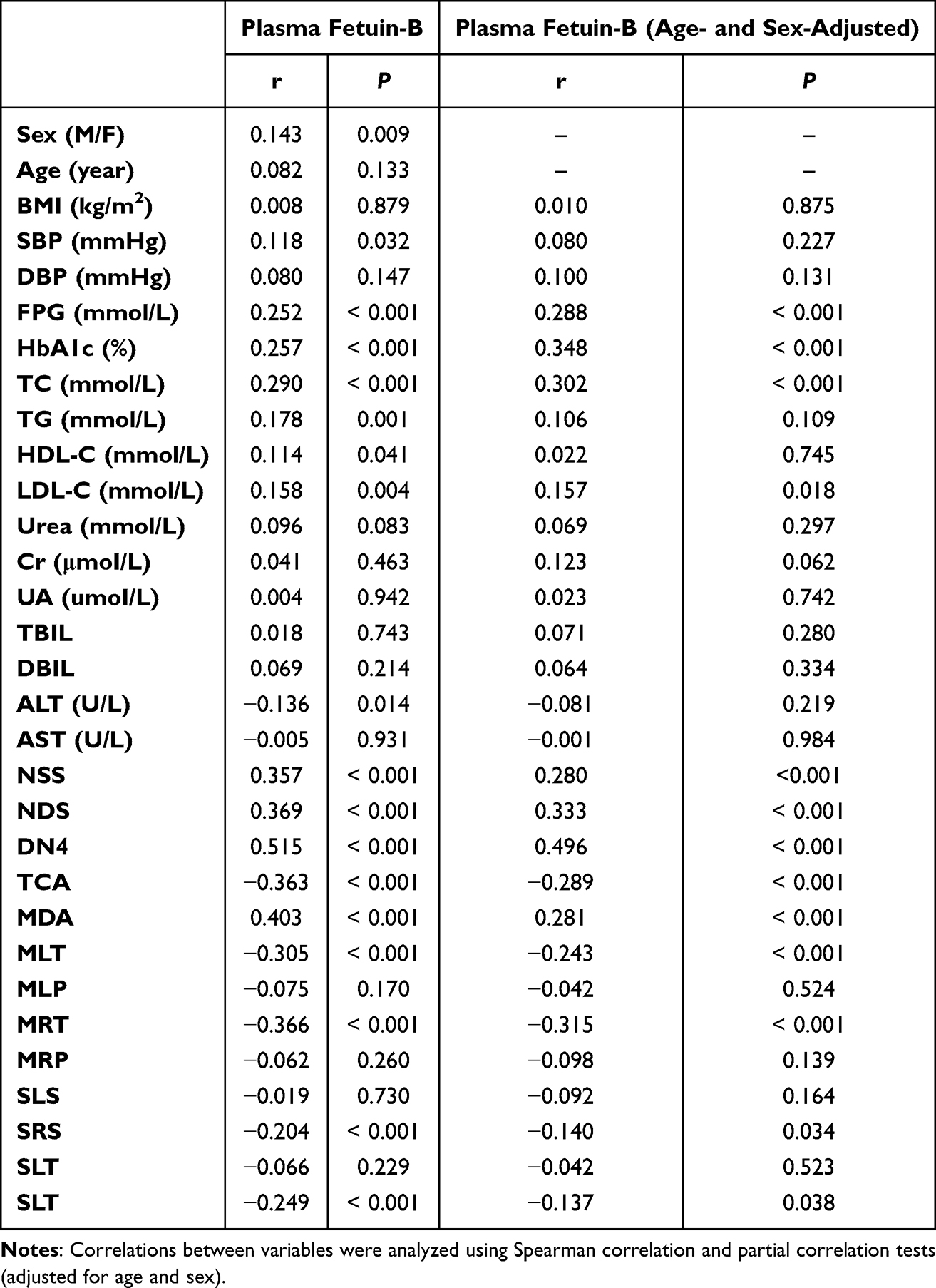 |
Table 3 Correlation Analysis of Parameters Related to Plasma Fetuin-B Level in All Participants |
 |
Figure 2 Plasma fetuin-B concentrations in diabetic controls, DPN and pDPN patients. Data are presented as mean ± SD. Data were analyzed using one-way ANOVA with Tukey’s post hoc test. *P < 0.05, **P < 0.01, ***P < 0.001. n = 139, 92, 101 in the non-DPN, DPN, and pDPN groups, respectively. |
Oxidative Stress as a Potential Confounder in the Relationship Between Fetuin-B and pDPN
As mentioned above, oxidative stress is considered to be a potential mechanism for the development of pDPN. Therefore, we evaluated the relationship between fetuin-B level and oxidative stress markers. Spearman correlation analysis showed that plasma fetuin-B levels were positively correlated with MAD concentration and negatively correlated with TAC (Table 2). Furthermore, after adjusting for MAD and TAC, multiple logistic regression analysis showed that the relationship between fetuin-B levels and pDPN (compared to the rest of the sample) was attenuated (OR = 1.38, 95% confidence interval = 0.27–7.18, P = 0.70). We further explored the potential impact of oxidative stress on the relationship between fetuin-B and the pDPN parameters (NSS, NDS, and DN4). In unadjusted models, fetuin-B levels were significantly associated with these parameters. However, after adjusting for oxidative stress markers (MAD and TAC), these associations were no longer statistically significant (eg, NSS: OR = 2.75, 95% CI = 0.73–10.35, P = 0.14; NDS: OR = 2.53, 95% CI = 0.33–19.38, P = 0.37; ND4: OR = 1.89, 95% CI = 0.57–6.20, P = 0.29). These findings highlight the complex interplay among oxidative stress, fetuin-B, and pDPN. Although our results suggest a role for oxidative stress as a confounding factor, further studies are necessary to confirm and clarify these observations.
Influence of Glucose and Lipid Metabolism on the Association Between Fetuin-B and pDPN
In addition to oxidative stress, the relationship between fetuin-B levels and general biochemical parameters was also assessed. Consistent with previous reports, circulating fetuin-B levels were positively associated with glucose and lipid parameters such as FPG, HbA1c, TC, and LDL-c (Table 2). Moreover, it appeared to be correlated with SBP and TG, HDL, and ALT levels (Table 2). However, these associations were not statistically significant after controlling for sex or age (Table 2). Additionally, we assessed whether the association between fetuin-B and pDPN was affected by the glucose and lipid parameters. After adjusting for FPG, HbA1c, TC, and LDL-c, multiple logistic regression analysis showed that the previously observed relationship between fetuin-B levels and pDPN (compared to the rest of the sample) was attenuated and no longer statistically significant (OR = 1.134, 95% confidence interval = 0.50–2.59, P = 0.77), suggesting that the association may be influenced by glucose and lipid metabolism, rather than being an independent factor.
Discussion
pDPN is a common and distressing complication of diabetes and is characterized by chronic and often severe neuropathic pain in the extremities.6,15 The prevalence of this condition is on the rise globally, paralleling the increasing incidence of diabetes.13,17 The impact of pDPN on patients’ quality of life, emotional well-being, and functional status necessitates a deeper understanding of the underlying pathophysiology. Emerging evidence suggests that dysregulation of cytokines within the peripheral nervous system creates an oxidative stress status, perpetuating nerve damage and amplifying pain signals.18 In the current study, we found that fetuin-B, a hepatokine, is strongly associated with pDPN. Specifically, plasma fetuin-B levels were higher in patients with pDPN than in patients with painless DPN and T2DM without DPN. It is significantly associated with neuropathy symptoms and nerve conductive velocity. Additionally, our study demonstrated that oxidative stress status, as reflected by decreased TAC and elevated MDA levels, was significantly worse in patients with DPN and pDPN than in the non-DPN group. This suggests enhanced oxidative damage, particularly in patients with pDPN, potentially contributing to nerve injury. MDA, a marker of lipid peroxidation, indicates damage to neuronal membranes, whereas reduced TAC reflects impaired systemic antioxidant defense.
Fetuin-B, an intriguing glycoprotein encoded by the AHSG gene, functions related to insulin sensitivity, glucose metabolism, and lipid homeostasis.8,19 AHSG encodes both fetuin-A and fetuin-B, and although they share structural similarities, emerging research has indicated unique features and functional differences between these two glycoproteins. The role of fetuin-B in modulating insulin sensitivity is a key player in intricate metabolic regulation.8 Its involvement in glucose metabolism extends beyond its supporting role, contributing to the intricate balance required to maintain optimal blood glucose levels. Consistently, the current study also found a positive relationship between plasma fetuin-B concentration and glucose indices. Moreover, fetuin-B has emerged as a pivotal regulator of lipid homeostasis, influencing processes such as lipid transport, storage, and utilization within the body.20 In the present study, fetuin-B concentration was also related to TG and LDL levels, suggesting that it may be closely related to cholesterol metabolism. Consistently, Xue et al21 conducted a bioinformatics analysis of a population of women with newly diagnosed metabolic syndrome, revealing that most fetuin-B-related core genes are involved in cholesterol metabolism, including cholesterol transporter activity and intermembrane cholesterol transfer activity.
In addition to its metabolic functions, fetuin-B has increasingly been implicated in broader physiological processes. Recent studies have explored its potential involvement in inflammatory responses, offering insights into its role in immune regulation.21,22 Additionally, researchers have aimed to elucidate its impact on various organ systems, including the liver and adipose tissue, to elucidate the diverse effects of fetuin-B on systemic homeostasis.8 In the current study, we observed a positive correlation between fetuin-B level and pDPN. However, after adjusting for potential confounders, such as oxidative stress markers (MDA and TAC) and metabolic factors (FPG, HbA1c, TC, and LDL-c), the direct association was attenuated, suggesting that elevated fetuin-B levels may be influenced by oxidative stress and metabolic dysregulation rather than directly causing pDPN. Notably, the significant correlations between fetuin-B, MDA, and TAC indicated a potential role for fetuin-B in modulating oxidative stress pathways, underscoring the critical role of oxidative stress in fetuin-B-associated effects on DPN progression.
Recently, we reported that the inflammatory factor C1q/tumor necrosis factor-related protein-3 (CTRP3) may serve as a biomarker for patients with DPN. Although both studies investigated biomarkers for DPN, they focused on different aspects of the condition.16 A previous study primarily examined the role of CTRP3 in general DPN, without distinguishing between painful and painless forms.16 However, our current study specifically explored the association of plasma fetuin B levels with nervous symptoms and conduction velocity in patients with painful DPN, which has not been previously reported. Furthermore, the two studies employed different methodologies and focused on distinct patient populations, as elaborated in the Methods and Results sections of our manuscript. Despite sharing the same ethics approval owing to being part of a broader research project on DPN, each paper addresses different research questions and contributes unique insights into the pathophysiology and potential biomarkers of DPN.
This study has several limitations. First, because of the limitations of the cross-sectional design, the exact causal relationship between fetuin-B levels and pDPN could not be ascertained. Second, although renal function and fetuin-B level are not directly linked, renal function plays a role in fetuin-B excretion. This indicates that factors influencing fetuin-B levels may be more complex in patients with renal insufficiency. In our study, we observed elevated levels of UA and Cr in the pDPN group compared with in those the non-DPN and DPN groups. This finding suggests that patients with pDPN are more likely to have concurrent renal dysfunction, which is a common complication of advanced diabetes. Impaired renal function can reduce UA excretion, leading to its accumulation.23 These findings highlight the systemic nature of complications in pDPN and suggest that renal function should be closely monitored in these patients.24 Further studies are needed to explore the precise relationship between pDPN, UA levels, and renal dysfunction.
In conclusion, the current study observed an increased level of the hepatokine fetuin-B in patients with pDPN compared to patients with painless DPN and T2DM without DPN. Moreover, plasma fetuin-B levels were significantly associated with nervous system symptoms and conduction velocity. These findings indicate that fetuin-B may serve as a biomarker for pDPN diagnosis and highlight the effects of hepatokine-mediated liver-to-peripheral nervous system crosstalk on DPN.
Data Sharing Statement
The clinical characteristics of all human subjects used to support the findings of this study have been included in this article.
Funding
This work was supported by the Joint Medical Research Project of the Chongqing Science & Technology Bureau and Chongqing Health Commission (No. 2023MSXM101) and Emergency Medicine Chongqing Key Laboratory Joint Fund for Talent and Development Project (2024RCCX08).
Disclosure
The authors declare no conflict of interest.
References
1. Sun H, Saeedi P, Karuranga S, et al. IDF Diabetes Atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabet Res Clin Pract. 2022;183:109119.
2. Hicks CW, Selvin E. Epidemiology of Peripheral Neuropathy and Lower Extremity Disease in Diabetes. Curr Diab Rep. 2019;19(10):86. doi:10.1007/s11892-019-1212-8
3. Feldman EL, Callaghan BC, Pop-Busui R. Diabetic neuropathy. Nat Rev Dis Primers. 2019;5(1):41. doi:10.1038/s41572-019-0092-1
4. Elafros MA, Andersen H, Bennett DL. Towards prevention of diabetic peripheral neuropathy: clinical presentation, pathogenesis, and new treatments. Lancet Neurol. 2022;21(10):922–936. doi:10.1016/S1474-4422(22)00188-0
5. Preston FG, Riley DR, Azmi S, Alam U. Painful Diabetic Peripheral Neuropathy: practical Guidance and Challenges for Clinical Management. Diabetes Metab Syndr Obes. 2023;16:1595–1612. doi:10.2147/DMSO.S370050
6. Sloan G, Selvarajah D, Tesfaye S. Pathogenesis, diagnosis and clinical management of diabetic sensorimotor peripheral neuropathy. Nat Rev Endocrinol. 2021;17(7):400–420. doi:10.1038/s41574-021-00496-z
7. Meex RCR, watt MJ. Hepatokines: linking nonalcoholic fatty liver disease and insulin resistance. Nat Rev Endocrinol. 2017;13(9):509–520. doi:10.1038/nrendo.2017.56
8. Meex R, Hoy A, Morris A. Fetuin B Is a Secreted Hepatocyte Factor Linking Steatosis to Impaired Glucose Metabolism. Cell Metab. 2015;22(6):1078–1089. doi:10.1016/j.cmet.2015.09.023
9. Brazaca LC, Moreto JR, Martin A, Tehrani F, Wang J, Zucolotto V. Colorimetric Paper-Based Immunosensor for Simultaneous Determination of Fetuin B and Clusterin toward Early Alzheimer’s Diagnosis. ACS Nano. 2019;13(11):13325–13332. doi:10.1021/acsnano.9b06571
10. Maglinger B, Frank JA, McLouth CJ. Proteomic changes in intracranial blood during human ischemic stroke. J Neurointerv Surg. 2021;13(4):395–399. doi:10.1136/neurintsurg-2020-016118
11. Wang T, Tyler RE, Ilaka O, Cooper D, Farokhnia M, Leggio L. The crosstalk between fibroblast growth factor 21 (FGF21) system and substance use. iScience. 2024;27(7):110389. doi:10.1016/j.isci.2024.110389
12. Tesfaye S, Boulton AJM, Dyck PJ. Diabetic neuropathies: update on definitions, diagnostic criteria, estimation of severity, and treatments. Diabetes Care. 2010;33(10):2285–2293. doi:10.2337/dc10-1303
13. Finnerup NB, Haroutounian S, Kamerman P. Neuropathic pain: an updated grading system for research and clinical practice. Pain. 2016;157(8):1599–1606. doi:10.1097/j.pain.0000000000000492
14. Baskozos G, Themistocleous AC, Hebert HL. Classification of painful or painless diabetic peripheral neuropathy and identification of the most powerful predictors using machine learning models in large cross-sectional cohorts. BMC Med Inform Decis Mak. 2022;22(1):144. doi:10.1186/s12911-022-01890-x
15. Hazari A, Mishra V, Agouris I. Clinical evaluation of painful diabetes peripheral neuropathy in type 2 diabetes patients: lessons from expatriates in the United Arab Emirates. Diabetes Metab Syndr. 2023;17(9):102832. doi:10.1016/j.dsx.2023.102832
16. Lin K, Yang L, Xiong Y, Feng K, Zeng W, Deng B. Plasma C1q/tumor necrosis factor-related protein-3 concentrations are associated with diabetic peripheral neuropathy. BMJ Open Diabetes Res Care. 2022;10:e002746.
17. Abbott CA, Malik RA, van Ross ER, Kulkarni J, Boulton AJ. Prevalence and characteristics of painful diabetic neuropathy in a large community-based diabetic population in the U.K. Diabetes Care. 2011;34(10):2220–2224. doi:10.2337/dc11-1108
18. Farmer KL, Li C, Dobrowsky RT. Diabetic peripheral neuropathy: should a chaperone accompany our therapeutic approach? Pharmacol Rev. 2012;64(4):880–900. doi:10.1124/pr.111.005314
19. Kralisch S, Hoffmann A, Lössner U. Regulation of the novel adipokines/ hepatokines fetuin A and fetuin B in gestational diabetes mellitus. Metabolism. 2017;68:88–94. doi:10.1016/j.metabol.2016.11.017
20. Singh P, Reza MI, Syed AA, Husain A, Gayen JR. Pancreastatin deteriorates hepatic lipid metabolism via elevating fetuin B in ovariectomized rats. Biochimie. 2023;214:114–122. doi:10.1016/j.biochi.2023.06.006
21. Pasmans K, Goossens GH, Groenhuijzen E. Fetuin B in white adipose tissue induces inflammation and is associated with peripheral insulin resistance in mice and humans. Obesity. 2023;32:517–527.
22. Zhang W, Yao J, Chen C, Wang J, Zhou A. Fetuin-B Overexpression Promotes Inflammation in Diabetic Retinopathy Through Activating Microglia and the NF-kappaB Signaling Pathway. Curr Eye Res. 2023;2023:1–12.
23. Leask MP, Crișan TO, Ji A, Matsuo H, Köttgen A, Merriman TR. The pathogenesis of gout: molecular insights from genetic, epigenomic and transcriptomic studies. Nat Rev Rheumatol. 2024;20(8):510–523. doi:10.1038/s41584-024-01137-1
24. Jeyam A, McGurnaghan SJ, Blackbourn LAK. Diabetic Neuropathy Is a Substantial Burden in People With Type 1 Diabetes and Is Strongly Associated With Socioeconomic Disadvantage: a Population-Representative Study From Scotland. Diabetes Care. 2020;43(4):734–742. doi:10.2337/dc19-1582
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.