Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 12
Plaque Fluoride Levels as a Predictor of Caries Development in Early Childhood with High Sugar Exposure – A Preliminary Study
Authors Rizzardi KF, Rodrigues LKA ![]() , Steiner-Oliveira C
, Steiner-Oliveira C ![]() , Nobre-dos-Santos M, Parisotto TM
, Nobre-dos-Santos M, Parisotto TM
Received 12 September 2019
Accepted for publication 28 December 2019
Published 9 March 2020 Volume 2020:12 Pages 71—78
DOI https://doi.org/10.2147/CCIDE.S230809
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Karina Ferreira Rizzardi, 1 Lidiany Karla Azevedo Rodrigues, 2 Carolina Steiner-Oliveira, 3 Marines Nobre-dos-Santos, 3 Thaís Manzano Parisotto 1
1Laboratory of Molecular and Clinical Microbiology, University São Francisco, Bragança Paulista, SP, Brazil; 2Faculty of Pharmacy, Dentistry and Nursing, Federal University of Ceará, Fortaleza, CE, Brazil; 3Piracicaba Dental School, University of Campinas, Piracicaba, SP, Brazil
Correspondence: Thaís Manzano Parisotto
Laboratory of Molecular and Clinical Microbiology, University São Francisco, Av. São Francisco de Assis, 218, Bragança Paulista, SP 12916-900, Brazil
Tel +55 11 24548474
Email [email protected]
Objective: This longitudinal study aimed to investigate if the plaque fluoride (PF) concentration can predict the early childhood caries onset. Design: As part of a larger study, 188 preschoolers were clinically evaluated for early childhood caries diagnosis, at baseline and after 1-year follow-up. After that, the final sample comprised: 1. children who had already caries at baseline (decayed, missing or filled surfaces, as well as white chalky white spot lesions adjacent to gingival margins) and developed at least one more cavitation after one year (n=16), and 2. children who never had or developed any caries lesions, including active white spots lesions (n=15). Before the clinical examinations, dental plaque was collected. PF concentration was determined with an ion-specific electrode. A chart was used to estimate the mean daily sugar exposure. The results were statistically analyzed by Spearman correlation and logistic regression analyses (α=0.05).
Results: After one year, a positive significant correlation between caries development and liquid sucrose, total sugar and total sucrose consumption increments was found (p< 0.05). Moreover, the solid sugar, solid sucrose and total sugar exposure at baseline were positively correlated with the presence of dental plaque at follow-up (p< 0.05). To top it all, children with PF concentrations ≤ 0.1 μg/mg at baseline were 10 times more likely to develop caries.
Conclusion: In conclusion, this study demonstrated for the first time in vivo that low PF concentration is a predictor of caries development in primary teeth.
Keywords: dental caries, preschool child, fluoride, biofilm
Introduction
In the past decades, dental caries has declined and is restricted to some segments of the population.15 However, early childhood caries (ECC), which affects children under 6 years of age, continues to be highly prevalent, especially in developing countries.21,29–31
The development of carious lesions reflects a prolonged imbalance between episodes of de- and remineralization with progressive net tooth mineral loss, which could lead to tooth-surface cavitation.13,26,27 This dynamic bacteria-mediated de- and remineralization relationship reflects the consumption frequency of cariogenic substrates, such as sugars, which are the main substrate for acid lactic production.33
Even when the plaque/plaque fluid pH is under the critical value for hydroxyapatite, but not lower than pH 4.5, a certain amount of calcium and phosphate can be recovered by enamel/dentin as fluorapatite. Thus, in the following situation: 4.5<pH<5.5, hydroxyapatite dissolves from the subsurface and fluorapatite/fluorhydroxyapatite forms in the surface layer.2,4
The availability and maintenance of F constant in the oral cavity is crucial for caries control,8,25 as higher amounts of plaque F decrease dental hard tissues solubility following a logarithmic pattern.2,5 Consequently, a low F concentration in the dental plaque would be a predisposing factor for ECC, and exactly how much F in the dental plaque might be capable to predict caries development in young children has never been explored before. This finding could influence the appropriate decision-making regarding preventive measures to control the disease, as well as its unpleasant consequences.
Furthermore, not many in vivo studies1,16,17 have been conducted focusing on F and dental caries in primary teeth, especially considering a follow-up research. Longitudinal investigations are important because they consider the response of the child to certain factors during the disease process.
Thus, this study aimed to assess if the plaque fluoride (PF) concentration can predict the early childhood caries.
Materials and Methods
Ethical Considerations
This longitudinal study was formally approved by the Ethical Committee in Research of Piracicaba Dental School – University of Campinas, Brazil (Protocol 017/2008) and was conducted in full accordance with the World Medical Association Declaration of Helsinki. The parents of the children granted written informed consent for the study and the authors have anonymized them, without identifying them in any way. The preschools and nurseries also granted permission. In addition, all mandatory clinical/laboratory health and safety procedures have been complied within the course of conducting any work reported in the present paper.
Sample
The sample size calculation (α=5%; β=90%) was based on a previous study17 using a similar methodology, which found 56% of difference in the fluoride concentration in dental plaque when caries free and pit and fissure caries children were compared. The calculated sample size was of 11 children per group; however, as this was a longitudinal study, we decided to include at least 15 children per group.
As part of a larger study, 188 preschoolers were clinically evaluated for early childhood caries diagnosis, at baseline and after 1-year follow-up.19,20 Preschoolers in good general health, 3–4 years old at baseline, were selected to take part in the study. The exclusion criteria included children with syndromes, having enamel hypoplastic lesions, taking medications for chronic disease, and children who were subjected to topical fluoride application, in the two-month period before plaque collection. Then, two groups of children were formed: 1. the caries group (CA, n=16, 8 girls and 8 boys), in which children had already caries at baseline (decayed, missing or filled surfaces, as well as white chalky white spot lesions adjacent to gingival margins) and developed at least one more cavitation or filling after one year. It should be emphasized that new fillings were considered only when a new carious lesion was developed and filled during the one year follow-up period; and 2. the no caries development group (NC, n=15, 10 girls and 5 boys), in which the children never had or developed any caries lesions, including active white spots lesions.
The children were from both genders, all of low socioeconomic backgrounds, and were attending public preschools in the urban area of Itatiba, in the state of São Paulo, Brazil. They stayed a minimum of 4 hrs per day at the preschools, having their main meals there, as well as having their teeth brushed at least once a day with 1100 ppm fluoridated dentifrice (provided by the Secretary of Health of the city of Itatiba in the period that the research was developed). The urban area of Itatiba has been fluoridated since 1980. Heterocontrol of the fluoridation process revealed that the concentration of F in the tap water was 0.5–0.8 ppm during the study.
Clinically Visible Dental Plaque Recording
The presence or absence of clinically visible plaque on the maxillary incisors was recorded under artificial light with the child lying on a table. After that, the children had their teeth cleaned for the clinical examinations.22
Clinical Examination
Dental examinations of each child were performed at baseline and after one year. After receiving instructions regarding the caries diagnosis criteria, one pedodontist was calibrated by re-examination of 12 children with a one-week interval period. The baseline Kappa value at the surface level was of 0.78, and the follow-up Kappa value at the surface level was of 0.82. The pedodontist conducted all the examinations following rigorous cross-infection control measures. The examinations were performed at the preschools with the child lying on a table and the examiner sitting behind the child. A focusable flashlight, a ball-ended dental probe, a mouth mirror and gauze for cleaning and drying the teeth were used. The criteria from the World Health Organization were used for ECC diagnosis with an additional measurement of active white spot lesions/early caries lesions (ECL)20,21,34 to assure that caries free children did not have active non-cavitated caries lesions, leading to a misclassification. The units of evaluation were decayed, missing and filled surfaces, as well as the white chalky spot lesions close to the gingival tissue.
Dental Plaque Collection and Fluoride Assay
Pooled supragingival plaque samples were collected at baseline and after one year from smooth surfaces (buccal and palatine) from all primary teeth, except from the interiors of the cavities, at least one hour after food intake and tooth brushing in the afternoon period. A wooden stick was employed for the plaque collection, which was placed into a microcentrifuge tube. The tubes were then transported in refrigerated boxes (4°C) to the Pediatric Dentistry Laboratory at Piracicaba Dental School, where they were frozen (–20 °C) until the analysis. Dental plaque was dried for 24 h in vacuum over P2O5, and the dry weight was obtained using an analytical balance (BelEngineering, Via Venezia Giulia, Monza). Then, 0.5 M HCl was added to the tube in the proportion of 0.1 mL/mg plaque dry weight. After extraction for 3 h at room temperature under constant agitation, the same volume of TISAB II (Total Ionic Strength Adjustor Buffer), pH 5.0 (containing 20 g NaOH/L), was added to the tube as a buffer.17 The samples were centrifuged (12,000 g) for 3 min, and the supernatant was retained for determination of the acid-soluble F concentration. Fluoride determination was performed using an Orion 96–09 ion-selective electrode (Orion Research Inc., Boston, MA, USA) and an Orion EA-940 digital ion analyzer that were previously calibrated with various F standard solutions (0.025 to 2.00 μg F/mL). The readings were expressed in millivolts (mV) and were then transformed to μg F/mL through linear regression of the calibration curve. The results were expressed as μg F/mg of plaque dry weight.
Dietary Sugar Exposure Evaluation
Mothers and health agents of the preschoolers that took part in this study were asked to fill out a diet chart for three consecutive days during the work week,22 at baseline and at follow-up. This chart included the times of day that the children ate and drank anything and the contents of all meals/snacks. The daily frequencies of total (solid + liquid) sugar and total (solid + liquid) sucrose exposure, solid sucrose, solid sugar exposure and liquid sucrose exposure were calculated using this chart by dividing the total number of sugar/sucrose exposure during the 3 days by the number of days. Whether the child slept with a baby bottle containing sweetened liquids was also recorded.
Statistics
The statistical analyses were performed using the Statistical Package for Social Science 13.0 (SPSS Inc., Chicago, IL, USA). The comparison between the two groups (CA x NC) at baseline and at follow-up was performed using the Mann–Whitney U-test. When the same groups were compared at different time points (baseline x follow-up), the Wilcoxon matched pairs signed ranks test was used. To assess the correlation between caries increment and sugar/sucrose consumption increment, the Spearman correlation was used. This test was also used to evaluate the correlation between the sugar/sucrose exposure, dental plaque presence and dental plaque F concentration at baseline with these same variables at follow-up. Logistic regression was also employed to individually identify risk factors for early childhood caries development. All analyses were conducted using a level of significance of 5% and a confidence interval of 95%.
Results
Children in the caries group exhibited a mean dmfs score of 8.0±4.9 at baseline and 10.4±4.9 at follow-up (increment=2.4); ECL lesions were the most prevalent lesions. The means, medians and standard errors of dental plaque F concentration and sugar/sucrose consumption frequency in the solid, liquid and total forms are displayed in Table 1. This table also shows the statistical differences (p<0.05) between groups regarding total sucrose, total sugar and liquid sucrose consumption at follow-up. Within the two groups, significant increases at follow-up were revealed for the following variables: NC – solid sugar and solid sucrose consumption; CA – solid sugar, solid sucrose, total sugar and total sucrose consumption. A significant decrease in dental plaque F concentration and liquid sucrose consumption was identified only in the NC group. No statistically significant differences were identified between the CA and NC groups regarding sugar/sucrose consumption increments and plaque fluoride increments (Table 1).
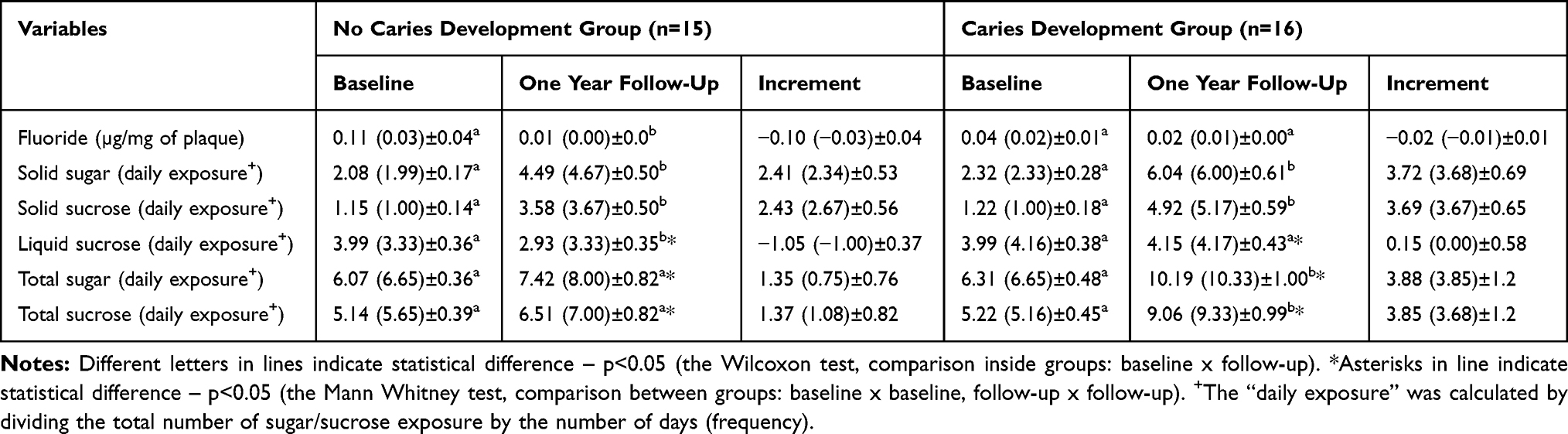 |
Table 1 Means, Medians and Standard Errors of Fluoride Concentration in Dental Plaque and Sugar/Sucrose Consumption Frequencies at Baseline and at Follow-Up in the Group of Children Who Developed Caries and in the Group, Who Did Not Develop Caries |
Table 2 indicates a positive significant correlation between caries increment and liquid sucrose, total sugar and total sucrose consumption increments. The correlations among variables evaluated at baseline versus variables evaluated at follow-up are shown in Table 3. This table also reveals that the solid sugar, solid sucrose and total sugar exposure at baseline were positively correlated with the presence of dental plaque at follow-up (p<0.05).
 |
Table 2 Spearman Correlation Coefficients (r) Between Caries Increment and Sugar/Sucrose Consumption Frequency Increment |
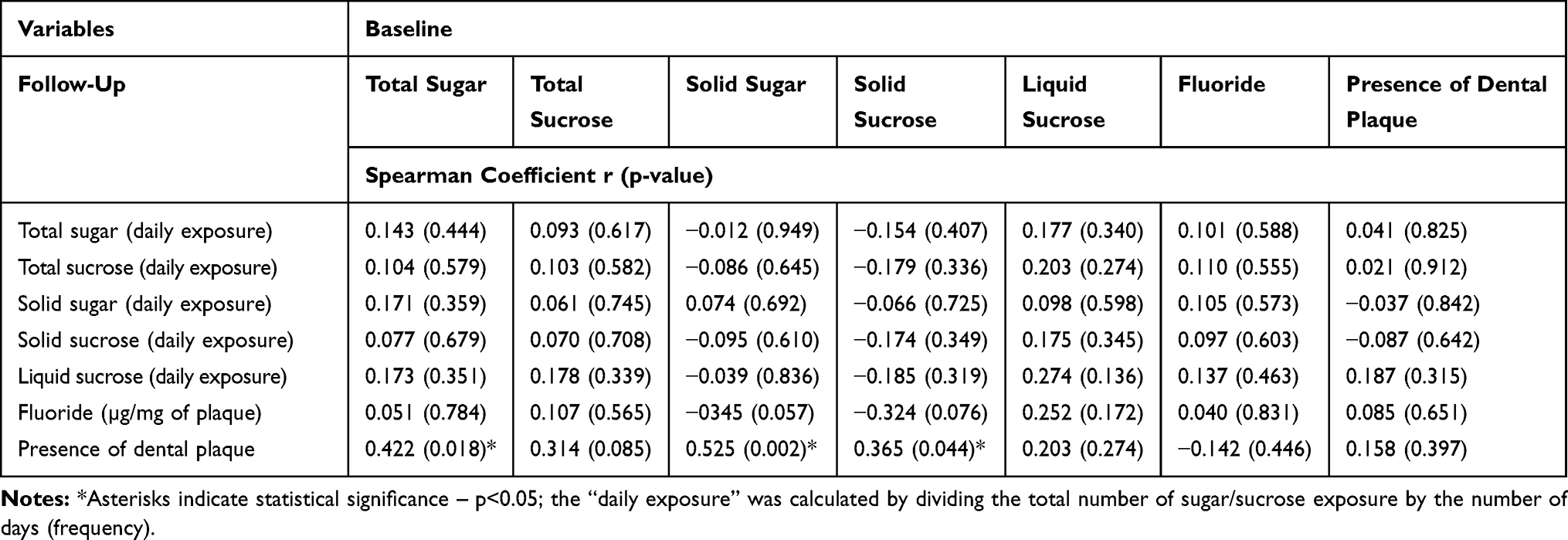 |
Table 3 Correlations Between Fluoride Concentrations in Dental Plaque, Sugar/Sucrose Consumption Frequency and Presence of Dental Plaque at Baseline versus These Same Variables at Follow-Up |
Finally, Table 4 shows that children with plaque F concentrations ≤0.1 μg/mg at baseline were more likely to develop caries in one year. This table also shows that sugar/sucrose exposure and the practice of sleeping with a baby bottle containing sugary liquids at baseline were not able to influence caries development in the studied population.
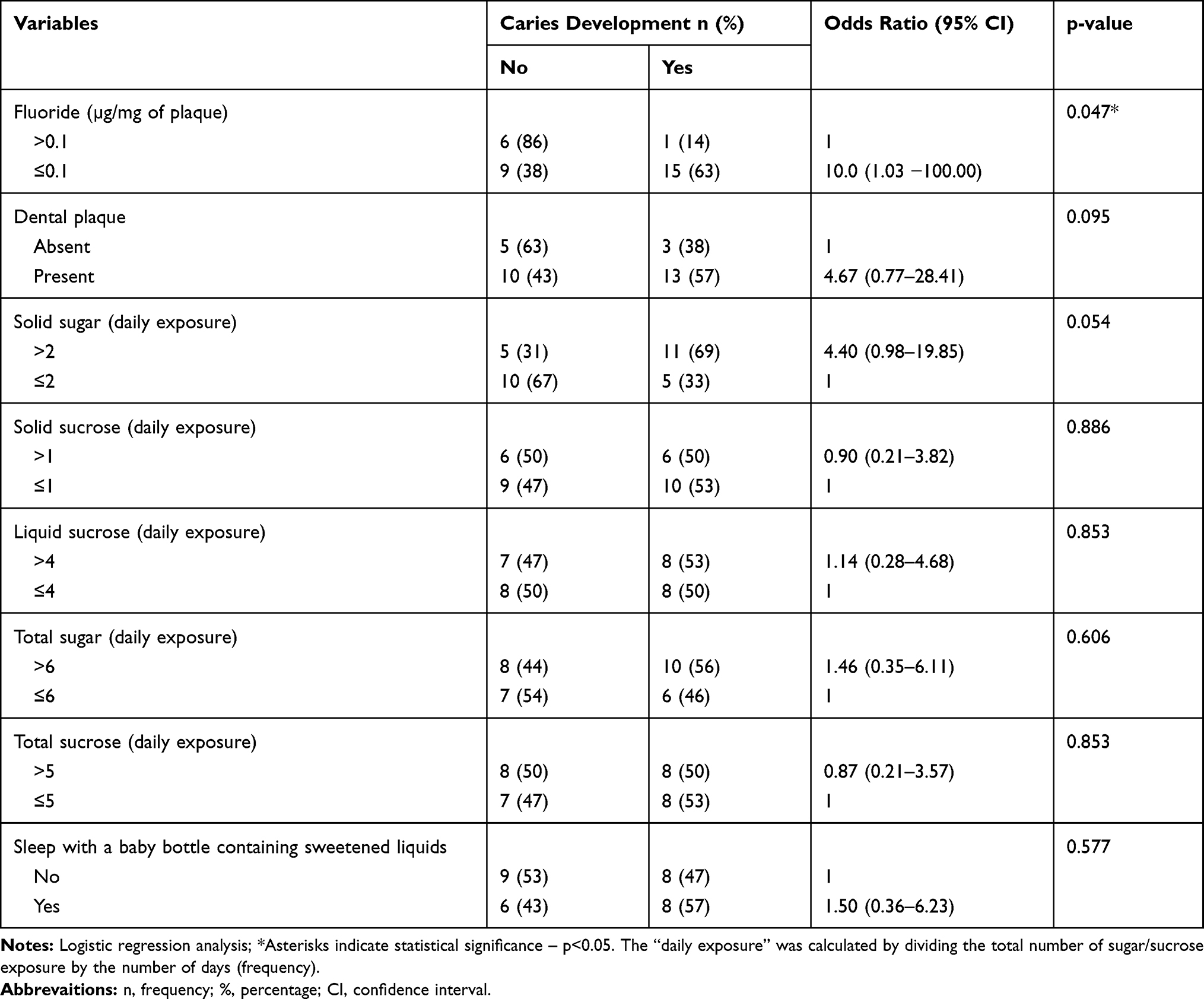 |
Table 4 Risks for Caries Development, Considering Fluoride Concentration, Sugar/Sucrose Consumption Frequency, and Presence of Dental Plaque |
Discussion
Fluoride is a critical ion involved in the dynamics of de- and remineralization of dental tissues. To our knowledge, for the first time, this study demonstrated longitudinally and in vivo that preschool children with plaque F concentrations lower than 0.1 μg/mg at baseline were 10 times more likely to develop caries lesions in primary teeth in a one-year follow-up period than those who had higher F concentrations (Table 4). One explanation for these findings could be that during a cariogenic challenge, fluoride present in dental plaque/plaque fluid will penetrate along with the acids to the subsurface, being adsorbed to the crystal protecting enamel surface from dissolution.2 It is well known that, in the presence of F, there is a decrease in the dissolution of dental tissues. This is the case because even when the plaque/plaque fluid pH is under the critical value for hydroxyapatite, but not lower than pH 4.5, a certain amount of calcium and phosphate is recovered by enamel/dentin. Additionally, remineralization is favored when the pH rises, enhancing the redeposition of these ions on demineralized tissues.4 Thus, the key point in the availability and maintenance of F in the oral cavity is to reduce the mineral potential of demineralization during acid attacks and to promote mineral transfer into the tooth following acid attacks. This main effect of how fluoride controls caries development occurs at the interface between the tooth surface and the adjacent dental plaque.2 However, regarding dental plaque F concentrations at baseline or at follow-up, no statistically significant difference could be observed between the group that developed caries and the group that did not. These findings are in line with studies by Bayrak, Okte and Fidanci1 assessing primary and permanent dentitions and Pearce et al23 assessing permanent dentition. However, they do not corroborate the results obtained by Gaugler and Bruton6 (1982) and Dos Santos et al17 Compared to the study of Dos Santos et al17 the caries diagnosis criteria used in their study did not include ECL. Therefore, the caries index of their caries group might have been much higher than it appeared, which might have favored achieving a significant difference. Regarding the Gaugler and Bruton6 (1982) study, the difference in the target population of the study could be a possible reason for the difference compared to this study, as their report involved adults.
It is recognized that fluoride dentifrice/water can significantly increase fluoride concentration in saliva and biofilm.24 This fluoride enhancement in the oral fluids can shift the balance from enamel demineralization to remineralization a very important issue in the present investigation.2 Fluoride levels in biofilm/biofilm fluid and saliva are mutually interdependent and clearly remarkable in caries prediction.16
Basically, the dental biofilm is composed of a solid (mainly microbial cells and insoluble extracellular polysaccharides) and a liquid phase (liquid fraction permeating cells and extracellular matrix). The biofilm fluid might reflect recent fluoride exposure12 and is of great importance for the understanding of physical-chemical dynamics of the carious process, as a decrease in the ions concentrations, such as calcium, phosphate and fluoride determine the mineral tooth dissolution.14 In addition, the biofilm solids could evidence an equilibrium due to constant and long-term exposure to different fluoride sources12 and systemic fluoride recycling by saliva. In this respect, the study of Lima et al12 did not find statistical difference in the fluoride concentration of the biofilm solid phase right after the intake of food prepared with fluoridated tap water in comparison with a control group. However, in the biofilm fluid, this difference was identified. Still, the findings of Larsen et al9 revealed that an additional 1-h accumulation of fluoride in biofilm solids after a single rinse with 5000 and 1500 ppm fluoride was not different.
In the one-year follow-up period, although the F concentration in dental plaque decreased within groups, this study revealed that the solid sugar/sucrose exposure increased significantly in both groups (Table 1). The group that did not develop caries exhibited a higher plaque F concentration at baseline, probably because caries active individuals might not fill their biofilm fluoride reservoirs during frequent cariogenic challenges.3,9,32 The decrease in F concentration in CA as well as in the NC groups at follow-up may be related to the depletion of the inorganic pools by organic acids as a result of the pH decrease during sugar fermentation, which was a consequence of a higher frequency of sugar exposure. In fact, a 3.1 to 4.0 times higher frequency of solid sucrose exposure was observed from baseline to follow-up in both groups (Table 1). This decrease in fluoride concentration may also be related to possible changes in the structure of dental plaque that may be connected to several factors. Firstly, fluoride uptake by dental plaque fluid into enamel might be involved because, during pH falls, the biofilm fluid would be undersaturated relative to hydroxyapatite but would be still oversaturated relative to fluorapatite, which precipitates on the enamel. Secondly, the fluoride released bound to bacterial cells, which were depleted during the pH falls, might also be a factor. Thirdly, when the frequency of sucrose exposure is increased, a higher concentration of extracellular polysaccharides occupies a larger volume of dental plaque, thereby reducing the cell biomass and the ion-binding sites of bacteria.18
Regarding sugar/sucrose consumption frequency the comparison between CA and NC groups revealed statistically significant differences with respect to total sugar exposure and to sucrose exposure in the total and liquid forms at follow-up (p<0.05, Table 1). This is in line with the positive and significant correlations between dmfs increment and liquid sucrose, total sucrose and the total sugar increments, which are shown in Table 2. These results are also in accordance with studies by Grindefjord et al7 and Law and Seow,10 who also found an association between dental caries development in young children and sugar/sucrose consumption. Interestingly, the baseline conditions of sugar/sucrose exposure and the habit of sleeping with a baby bottle containing sweetened liquids were not able to predict caries development in our study (Table 4). These results were unexpected but emphasize the importance of evaluating a determined variable and its behavior for a certain period of time, as significant correlations of dmfs increments and some sugar/sucrose exposure increments (such as those described above) were identified. The fact that sleeping with a baby bottle was not able to predict caries in our study might be because the parent or responsible party could have included this item in the diet chart according to a prevailing social norm rather than reporting the factual situation, as they might want to adhere to what would be desirable for good oral health.28
The oral hygiene conditions were also evaluated in this study by recording the presence or absence of dental plaque on the maxillary incisors. However, no association between dental caries development and the presence of dental plaque at baseline was identified in this study (Table 4). This finding is not in agreement with the cohort study by Leroy et al11, which used a different criterion for recording the visible dental plaque. These authors investigated plaque accumulation on teeth 52, 55, 72 and 75 in large numbers of preschoolers while, in our study, we recorded the presence or absence of clinically visible plaque on the maxillary incisors. Recognizing the role of dental plaque and sugar exposure in the caries process, especially in its initiation, a significant positive correlation was identified between solid sugar and sucrose exposure at baseline and the presence of dental plaque at follow-up (p<0.05, Table 3). The higher the sucrose consumption, the higher the concentration of insoluble extracellular polysaccharide in dental plaque,17 which favors bacterial adherence to the tooth surface which in turn contributes to the structural integrity of dental biofilm.18
Despite several positive aspects in the present in vivo study, some limitations should be pointed out. Plaque F concentration was only evaluated at baseline and after one year, with no intermediate analysis. This could have been a helpful information to explain F behavior during the follow-up period. Even though children had similar socio-economic and cultural patterns, as they lived in an optimally fluoridated tap water urban area, studied at public schools and used fluoridated toothpastes, it is known that many did not brush their teeth at home, but only once at school, under teacher’s supervision. This could have led to difference in fluoride exposure. Regarding the classical dietary chart, mothers used not report exactly what their children eat and drink, but what is socially accepted; particularly considering that dentists would appraise it. The sporadic use of sugar-containing medications, which are cariogenic, was also not recorded. These aspects might have reduced the fidelity of sugar/sucrose exposure data. In addition, this is a preliminary study and further investigations including larger samples should be stimulated.
In summary, it should be highlighted that evaluating factors involved in caries development, especially in early childhood, can provide a better understanding of caries dynamics, which may favor the implementation of preventive measures for primary teeth. Moreover, the identification of children who are at risk is very relevant for caries prevention. The preventive measures for early childhood caries are important because this disease englobes serious consequences, such as high levels of pain and infection, can impact the quality of life and its prevalence is high/rising in many countries.30
Conclusion
In conclusion, this in vivo longitudinal study demonstrated that in the presence of high sugar exposure, low levels of fluoride in dental plaque increases the risk of developing early childhood caries.
Acknowledgments
We specially thank all the children who participated in this longitudinal study and the Secretary of Education and Health of Itatiba for collaborating with this research. We acknowledge funds by FAPESP (2008/09510-3) and CNPq (480401/2008-0) grants.
Author Contributions
Karina Ferreira Rizzardi took part in the writing of the first draft and in critically reviewing the manuscript, leading to the final version. Thaís Manzano Parisotto also performed the collection of the clinical data, the statistical analysis, the data interpretation, wrote the first draft of the manuscript, designed and coordinate the study. Marines Nobre dos Santos and Lidiany K. A. Rodrigues were responsible for coordinating the study, too, for the design and for writing the paper. Carolina Steiner-Oliveira also helped in data collection and in critically reviewing the manuscript, leading to the final version. All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This work was financially supported by FAPESP under Grant 2008/09510-3; and CNPq under Grant 480401/2008-0.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Bayrak S, Okte Z, Fidanci UR. Relationship between caries and dental plaque composition. Am J Dent. 2011;24:45–48.
2. Buzalaf MA, Pessan JP, Honório HM, Ten Cate JM. Mechanisms of action of fluoride for caries control. Monogr Oral Sci. 2011;22:97–114.
3. Ccahuana-Vasquez RA, Tabchoury CP, Tenuta LM, Del Bel Cury AA, Vale GC, Cury JA. Effect of frequency of sucrose exposure on dental biofilm composition and enamel demineralization in the presence of fluoride. Caries Res. 2007;41(1):9–15. doi:10.1159/000096100
4. Cury JA, Tenuta LM. Enamel remineralization: controlling the caries disease or treating early caries lesions? Braz Oral Res. 2009;23(Suppl 1):23–30. doi:10.1590/S1806-83242009000500005
5. Featherstone JD, Glena R, Shariati M, Shields CP. Dependence of in vitro demineralization of apatite and remineralization of dental enamel on fluoride concentration. J Dent Res. 1990;69:620–625. doi:10.1177/00220345900690S121
6. Gaugler RW, Bruton WF. Fluoride concentration in dental plaque of naval recruits with and without caries. Arch Oral Biol. 1982;27:269–272. doi:10.1016/0003-9969(82)90061-9
7. Grindefjord M, Dahllöf G, Nilsson B, Modéer T. Stepwise prediction of dental caries in children up to 3.5 years of age. Caries Res. 1996;30:256–266. doi:10.1159/000262333
8. Gugnani N, Gugnani S. Remineralisation and arresting caries in children with topical fluorides. Evid Based Dent. 2017;18:41–42. doi:10.1038/sj.ebd.6401234
9. Larsen LS, Baelum V, Tenuta LMA, Richards A, Nyvad B. Fluoride in saliva and dental biofilm after 1500 and 5000 ppm fluoride exposure. Clin Oral Investig. 2018;22::1123–1129. doi:10.1007/s00784-017-2195-y
10. Law V, Seow WK. A longitudinal controlled study of factors associated with mutans streptococci infection and caries lesion initiation in children 21 to 72 months old. Pediatr Dent. 2006;28:58–65.
11. Leroy R, Bogaerts K, Martens L, Declerck D. Risk factors for caries incidence in a cohort of Flemish preschool children. Clin Oral Investig. 2012;16:805–812. doi:10.1007/s00784-011-0579-y
12. Lima CV, Tenuta LM, Cury JA. Fluoride increase in saliva and dental biofilm due to a meal prepared with fluoridated water or salt: a crossover clinical study. Caries Res. 2019;53:41–48. doi:10.1159/000489132
13. Lingström P, Van Houte J, Kashket S. Food starches and dental caries. Crit Rev Oral Biol Med. 2000;11:366–380. doi:10.1177/10454411000110030601
14. Maltz M, Tenuta LMA, Groisman S, Cury JA. Cariology: basic concepts, diagnosis and non-restorative treatment. Artes Medicas. 2016;144.
15. Narvai PC, Frazão P, Roncalli AG, Antunes JL. Dental caries in Brazil: decline, polarization, inequality and social exclusion. Rev Panam Salud Publica. 2006;19:385–393. doi:10.1590/S1020-49892006000600004
16. Newby EE, Martinez-Mier EA, Zero DT, et al. A randomised clinical study to evaluate the effect of brushing duration on fluoride levels in dental biofilm fluid and saliva in children aged 4–5 years. Dent J. 2013;63(Suppl 2):39–47.
17. Dos Santos MN, Dos Santos LM, Francisco SB, Cury JA. Relationship among dental plaque composition, daily sugar exposure and caries in the primary dentition. Caries Res. 2002;36:347–352. doi:10.1159/000065959
18. Paes Leme AF, Koo H, Bellato CM, Bedi G, Cury JA. The role of sucrose in cariogenic dental biofilm formation-new insight. J Dent Res. 2006;85:878–887. doi:10.1177/154405910608501002
19. Parisotto TM, King WF, Duque C, et al. Immunological and microbiologic changes during caries development in young children. Caries Res. 2011;45(4):377–385. doi:10.1159/000330230
20. Parisotto TM, Santos MN, Rodrigues LK, Costa LS. Behavior and progression of early carious lesions in early childhood: a 1-year follow-up study. J Dent Child (Chic). 2012;79:130–135.
21. Parisotto TM, Steiner-Oliveira C, De Souza-E-silva CM, Peres RC, Rodrigues LK, Nobre-dos-Santos M. Assessment of cavitated and active non-cavitated caries lesions in 3- to 4-year-old preschool children: a field study. Int J Paediatr Dent. 2012;22:92–99. doi:10.1111/j.1365-263X.2011.01171.x
22. Parisotto TM, Steiner-Oliveira C, Duque C, Peres RC, Rodrigues LK, Nobre-dos-Santos M. Relationship among microbiological composition and presence of dental plaque, sugar exposure, social factors and different stages of early childhood caries. Arch Oral Biol. 2010;55:365–373. doi:10.1016/j.archoralbio.2010.03.005
23. Pearce EI, Dong YM, Yue L, Gao XJ, Purdie GL, Wang JD. Plaque minerals in the prediction of caries activity. Community Dent Oral Epidemiol. 2002;30:61–69. doi:10.1034/j.1600-0528.2002.300109.x
24. Pessan JP, Conceição JM, Grizzo LT, Székely M, Fazakas Z, Buzalaf MA. Intraoral fluoride levels after use of conventional and high-fluoride dentifrices. Clin Oral Investig. 2015;19(4):955–958. doi:10.1007/s00784-015-1426-3
25. Rodrigues E, Delbem AC, Pedrini D, Cavassan L. Enamel remineralization by fluoride-releasing materials: proposal of a pH-cycling model. Braz Dent J. 2010;21:446–451. doi:10.1590/S0103-64402010000500012
26. Rošin-Grget K, Peroš K, Sutej I. The cariostatic mechanisms of fluoride. Acta Med Acad. 2013;42:179–188. doi:10.5644/ama2006-124.85
27. Selwitz RH, Ismail AI, Pitts NB. Dental caries. Lancet. 2007;369:51–59. doi:10.1016/S0140-6736(07)60031-2
28. Sjostrom O, Holst D. Validity of a questionnaire survey: response patterns in different subgroups and the effect of social desirability. Acta Odontol Scand. 2002;60:136–140. doi:10.1080/000163502753740133
29. So M, Ellenikiotis YA, Husby HM, Paz CL, Seymour B, Sokal-Gutierrez K. Early childhood dental caries, mouth pain, and malnutrition in the ecuadorian amazon region. Int J Environ Res Public Health. 2017;14:E550. doi:10.3390/ijerph14050550
30. Splieth CH, Christiansen J, Foster Page LA. Caries epidemiology and community dentistry: chances for future improvements in Caries Risk Groups. Outcomes of the ORCA saturday afternoon symposium, Greifswald, 2014. Part 1. Caries Res. 2016;50:9–16. doi:10.1159/000442713
31. Sutthavong S, Taebanpakul S, Kuruchitkosol C, et al. Oral health status, dental caries risk factors of the children of public kindergarten and schools in Phranakornsriayudhya, Thailand. J Med Assoc Thai. 2010;93:S71–S78.
32. Tenuta LM, Del Bel Cury AA, Bortolin MC, Vogel GL, Cury JA. Ca, Pi, and F in the fluid of biofilm formed under sucrose. J Dent Res. 2006;85(9):834–838. doi:10.1177/154405910608500911
33. Touger-Decker R, Van Loveren C. Sugars and dental caries. Am J Clin Nutr. 2003;78:881S–92S. doi:10.1093/ajcn/78.4.881S
34. World Health Organization. Oral Health Surveys - Basic Methods. Geneva: World Health Organization; 1997.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.