")
Back to Journals » Drug Design, Development and Therapy » Volume 18
Plants with Anti-Ulcer Activity and Mechanism: A Review of Preclinical and Clinical Studies
Authors Prayoga DK, Aulifa DL , Budiman A, Levita J
Received 29 October 2023
Accepted for publication 23 January 2024
Published 1 February 2024 Volume 2024:18 Pages 193—213
DOI https://doi.org/10.2147/DDDT.S446949
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Deshanda Kurniawan Prayoga,1,* Diah Lia Aulifa,2,* Arif Budiman,3,* Jutti Levita4,*
1Master Program in Pharmacy, Faculty of Pharmacy, Padjadjaran University, Sumedang, West Java, 45363, Indonesia; 2Department of Pharmaceutical Analysis and Medicinal Chemistry, Faculty of Pharmacy, Padjadjaran University, Sumedang, 45363, Indonesia; 3Department of Pharmaceutics and Pharmaceutical Technology, Faculty of Pharmacy, Padjadjaran University, Sumedang, 45363, Indonesia; 4Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Padjadjaran University, Sumedang, 45363, Indonesia
*These authors contributed equally to this work
Correspondence: Jutti Levita, Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Padjadjaran University, Sumedang, West Java, 46363, Indonesia, Tel +6222-84288888 Ext 3510, Email [email protected]
Abstract: Ulcer disorders including the oral mucosa, large intestine, and stomach mucosa, cause significant global health burdens. Conventional treatments such as non-steroid anti-inflammatory drugs (NSAIDs), proton pump inhibitors (PPIs), histamine H2 receptor antagonists (H2RAs), and cytoprotective agents have drawbacks like mucosal injury, diminish gastric acid secretion, and interact with concurrent medications. Therefore, alternative therapeutic approaches are needed to tackle this health concern. Plants are rich in active metabolites in the bark, roots, leaves, fruits, and seeds, and have been utilized for medicinal purposes since ancient times. The use of herbal therapy is crucial, and regulations are necessary to ensure the quality of products, particularly in randomized studies, to assess their efficacy and safety in treating ulcer disorders. This study aims to explore the anti-ulcer activity of medicinal plants in treating peptic ulcer disease, ulcerative colitis, and aphthous ulcers. Articles were searched in Scopus and PubMed, and filtered for publication from 2013 to 2023, resulting in a total of 460 from Scopus and 239 from PubMed. The articles were further screened by title and abstract and resulted in 55 articles. Natural products, rich in active metabolites, were described to manage ulcer disease by protecting the mucosa, reducing ulcer effects, inhibiting pro-inflammatory factors, and reducing bacterial load, thus improving patients’ quality of life. Natural extracts have proven effective in managing other health problems, including ulcers by reducing pain and decreasing lesions. This review provides an overview of preclinical and clinical studies on medicinal plants, focusing on their effectiveness in treating conditions like peptic ulcers, ulcerative colitis, and aphthous ulcers.
Keywords: anti-ulcers, aphthous ulcer, botanical drugs, peptic ulcer disease, ulcerative colitis
Introduction
The need to replace certain drugs due to their adverse effects exemplifies the universal role of plants in the treatment of disease and the maintenance of health. The utilization of medicinal plants for the treatment of various ailments has been practiced since ancient times and is commonly referred to as phytotherapy.1 The healing effects of medicinal plants come from the fact that they accommodate a wide range of secondary metabolites, called phytochemicals, which can be synthesized again and again in nature. The richest sources of active metabolites are contained in seeds, bark, roots, leaves, and fruits of plants. Therefore, a multitude of plants have employed these phytochemicals as a defense mechanism against pathogens.
Phytochemicals have been used since ancient times for the treatment of various disorders and are generally considered safer as compared to synthetic medicines.2–4 They are widely available in nature, and apart from therapeutic purposes, they are also consumed in the form of nutritional supplements.5 Several plant-derived chemical constituents have been reported to possess anti-ulcerative properties in various preclinical studies. These constituents belong to the class of alkaloids, tannins, flavonoids, terpenoids, glycosides, carotenoids, and saponins.6–8 Numerous botanical products have been confirmed to exhibit antiulcer activity although most studies focused on pharmacological action in animal models.
Ulceration is a crater-shaped lesion or wound that can form on the oral mucosa, large intestine (colon), and stomach mucosa. The formation of an ulcer may cause the region to bleed or discharge unpleasant materials, creating a painful sore that is susceptible to infection. Ulceration can be characterized by flaws in the epithelium, underlying connective tissue, or both. The diagnosis of ulcerative lesions may be difficult due to the wide range of potential causes and presenting characteristics of every organ.9 Despite the existence of various conventional and non-conventional treatment modalities for ulcer management, each approach is associated with certain limitations, including toxicity, low efficacy, and high cost.10 It is crucial to highlight the fact that botanical products may contain a multitude of active constituents that possess both hazardous and advantageous effects. Thus, it is important to use herbal therapy and put in place regulations to ensure the quality of herbal products, especially when it comes to doing more randomized studies to find out how effective and safe different products are at treating ulcer disorders.1
Taking all into consideration, this review aims to provide an in-depth exploration of plants possessing anti-ulcer activity, elucidating their mechanisms of action through a combination of preclinical and clinical studies. By consolidating the current body of knowledge, this review aims to shed light on the potential of plant-based interventions as viable alternatives for the management of gastrointestinal ulcers. This review will encompass a thorough analysis of preclinical studies investigating various plant species and their active metabolites with demonstrated anti-ulcerative properties, as well as a critical evaluation of clinical trials investigating the efficacy and safety of plant-based interventions in ulcer management. Special emphasis will be placed on elucidating the underlying mechanisms, including their impact on gastric mucosal protection, modulation of acid secretion, anti-inflammatory effects, assessments of symptom relief, ulcer healing rates, and potential preventive effects on ulcer recurrence.
Methods
Initially, the search included references published from 2013 until 2023. Articles were searched in Scopus and PubMed, in addition to Google Scholar. Throughout the search process, synonyms and related terms were used interchangeably as keywords, and the Boolean operator “AND” was utilized to combine and exclude terms as follows: (1) in the Scopus database using the keywords Plants AND Anti-ulcerative Activity AND Clinical Studies, searched within Article title, Abstract, and Keywords, resulted in n = 6; using the keywords Plants AND Anti-ulcerative Activity searched within Article title, Abstract, and Keyword, resulted in n = 90; and using the keywords Plants AND Antiulcer AND Activity searched within Article title, Abstract, Keywords, resulted in n = 364, with a total of 460 articles from Scopus database; (2) in the PubMed database using the keywords Plants AND Anti-ulcerative Activity searched within Abstract, free full text, and in the last 10 years, resulted in n = 239.
All articles found through these searches were further screened and those that met the review’s inclusion criteria (open access, written in English, related to antiulcer activity studied in animal models and humans, not studied in cells or computational simulation), were retrieved and evaluated by the authors. Finally, 55 articles were selected, as depicted in Figure 1. However, during the process, an additional search was conducted to obtain more articles to support the discussion.
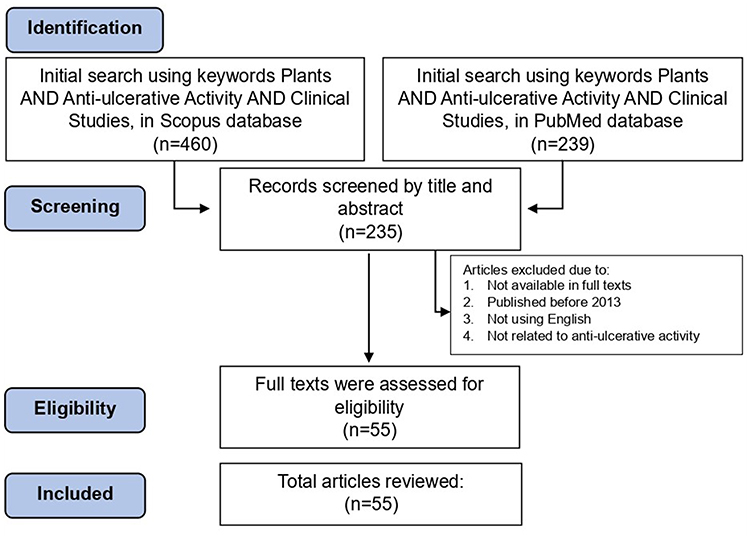 |
Figure 1 The study design of the review. |
Results
Of the 55 articles, 50 discussed in vivo (preclinical) methods (Table 1) and 5 discussed clinical (human) studies (Table 2). For example, 16 articles described the mechanisms for peptic ulcer disease, 33 articles described the mechanisms for ulcerative colitis, and 3 articles described the mechanisms for aphthous ulcer. Moreover, 33 articles discussed the active metabolites that demonstrated mechanisms for healing ulcers. Of these studies, 5 confirmed the importance or empirical history of the plants that had mechanisms for healing ulcers.
 |
Table 1 The Anti-Ulcerative Properties of Various Plants in Preclinical Studies |
 |
Table 2 The Anti-Ulcerative Properties of Various Plants in Clinical Studies |
Most of the studies described Brazil (South America) and China as the origin locations of the plant collection, although other countries such as Iran, Egypt, Pakistan, Cameroon (Central Africa), Bangladesh, Poland, Malaysia, Korea, Nigeria (West Africa), and Indonesia were also mentioned.
In the preclinical studies, various types of ulcer inducers were used, eg, ethanol (9 articles), dextran sulfate sodium (8 articles), bethanechol (6 articles), acetic acid (6 articles), indomethacin (3 articles), histamine (2 articles), trinitrobenzene sulfonic acid (2 articles), and other inducers (pentagastrin, piroxicam, Helicobacter pylori, and a burnisher). Of those, rats (Rattus norvegicus) were more selected (54.54%) as the animal model than mice (Mus musculus) (45.45%). The description of the diseases is presented below.
Nine plants were confirmed for their strong anti-peptic ulcer disease activity in animal models, twenty plants have shown strong anti-ulcerative colitis activity, and no plant exhibited strong anti-aphthous ulcer activity. Studies in humans indicated that Nicotiana tabacum (Solanaceae), Glycyrrhiza glabra (Fabaceae), and Zingiber officinale (Zingiberaceae) possessed strong antiulcer activity.
Peptic Ulcer Disease (PUD)
Peptic ulcer disease (PUD) is characterized by the presence of damage or ulcers in the mucosal lining of the gastrointestinal tract (GI), which leads to the excessive secretion of gastric acid or pepsin. Typically, these symptoms appear within the gastric region and the proximal segment of the duodenum.50 Peptic ulcer disease (PUD) is a global problem with a lifetime risk of development ranging from 5–10%.51 In general, there has been a global decline in the prevalence of peptic ulcer disease (PUD) as a result of enhanced hygienic and sanitary practices, as well as the implementation of effective treatment strategies and the cautious utilization of non-steroidal anti-inflammatory drugs (NSAIDs). Therefore, epidemiological studies have demonstrated a reduction in peptic ulcer incidence, hospital admissions, and death but the case fatality rate has stabilized at 5–10%.52
PUD has various multiple factors. Traditionally, mucosal disruption in patients with peptic disease is considered to be a result of a hypersecretory of acid together with dietary factors or stress. The primary risk factors associated with gastric or peptic ulcers are infection with H. pylori and the utilization of nonsteroidal anti-inflammatory drugs (NSAIDs).53,54 Nevertheless, the incidence of PUD is relatively low among individuals affected by H. pylori or those who use NSAIDs. This suggests that individual susceptibility affects the initial onset of mucosal damage.
The primary goal of presently antiulcer medications is not only limited to controlling the progression of the disease. It also aims to induce remission as quickly as possible and to maintain it for a long time The management of PUD currently uses a variety of conventional treatment modalities, but it’s crucial to remember that each of these treatments has one or more negative side effects. The primary goal of currently used anti-ulcerative medications is not simply to manage the advancement of the ailment. It also aims to promptly initiate and sustain a state of remission over an extended period.55,56 The primary negative consequences encompass gastrointestinal disruptions such as feelings of nausea, vomiting, constipation, and diarrhea, as well as impacts on the cardiovascular system.10
Based on the findings, it has been reported by the World Health Organization (WHO) that approximately 80–85% of the global population relies on natural products for disease management and nutritional supplementation. Botanical products are being utilized as alternative medicines for the treatment of various diseases due to their perceived safety in comparison to synthetic medicines.57 An in vivo or preclinical study of the active metabolites in a plant showed that the metabolites treat peptic ulcer disease by protecting the gastrointestinal mucosa wall, reducing the effects of ulcers, decreasing or reducing the lesion area caused by ulcers, inhibiting cytokine pro-inflammatory factors such as TNF-α, IL-1β, and IL-6, an ulcerative agent, and reducing the bacterial load on the gastric mucosa caused by Helicobacter pylori in the test animal, and clinical studies of the active metabolites showed that the combination of metabolites as a supplement makes a better treatment for PUD.
Ulcerative Colitis (UC)
Ulcerative colitis is a long-lasting inflammatory condition of the colon that causes the wall of the colon to become easily detached and wear away at the surface, often with bleeding. Typically, this condition is characterized by inflammation that is localized to the mucosal and submucosal layers of the colon. In general, the onset of the disease occurs within the rectum and progresses in a contiguous manner towards more proximal regions. Ulcerative has no cure and is a lifelong disorder with a significant impact on both physical and mental health.58 The etiology of inflammatory bowel disease remains uncertain. The prominent independent risk factor of familial disease history, which is present in about 8% to 14% of affected people, suggests that a primary genetic component plays a significant role. Individuals who have a family diagnosed with ulcerative colitis are at a significantly elevated risk, approximately four times higher, of developing the same disease.59
There is a growing emphasis in treatment strategies on achieving intestinal healing rather than solely focusing on symptomatic relief, to mitigate the likelihood of long-term complications and the need for surgical interventions.60,61 Treatments can be broadly categorized as those employed to initiate remission, either at the time of diagnosis or during a subsequent flare-up.62 Currently, the dietary management is to improve symptoms while offering support. In recent years, there has been a notable shift in dogma toward the utilization of dietary therapies that target specific mechanisms to induce disease remission.63–65 Most research has focused on how the immune system changes in the early stages, but over the past 20 years, a lot of evidence has shown that ulcerative colitis (UC) is mostly a disease of the epithelial tissue.66 The pathogenesis of the colonic epithelium is mostly caused by metabolic defects, which play a key role and may contribute to the breakdown of the mucosal barrier. Consequently, the epithelium may experience additional harmful effects due to the presence of microbial metabolites, such as hydrogen sulfide (H2S) and nitric oxide (NO), which can be toxic when present in excessive amounts.67
People with UC can get relief from their symptoms through a variety of pharmacological interventions. However, a large number of these therapeutic medications are linked to serious side effects.68 Therefore, researchers are currently placing increased emphasis on natural compounds,69 as they have the potential to mitigate adverse effects. A clinical study of gingerol and shogaol, which are the active metabolites in the Zingiber officinal plants, found that they were more likely to cause a clinical response and significantly improve a patient’s quality of life.70 Recent research has shown that using natural lipid nanoparticles (nLNP) loaded with 6-shogaol (6S/nLNP) can effectively change the types of bacteria in the gut, cause metabolic changes in feces, and reduce inflammation in a model of acute colitis caused by DSS.71 An in vivo or preclinical study of the active metabolites in a plant showed that the active metabolites inhibited cytokine pro-inflammatory factors such as TNF-α, IL-1β, and IL-6, an ulcerative agent, in the test animal, also the metabolites protected colon mucosa from ulceration through their strength aspect, such as antioxidant, or anti-inflammatory. According to preclinical and clinical studies.
Aphthous Ulcer (Mouth Ulcer)
Aphthous ulcers, also known as mouth ulcers, show inflamed spots with a white-reddish appearance that develop on the mucous membrane that lines the oral cavity. Despite being painful, these injuries generally undergo spontaneous healing and do not result in any complications. There is variation in the recurrence of canker sores, with certain individuals experiencing a reoccurrence within a few weeks, while others may encounter them after months or even years.72
Aphthous stomatitis is estimated to impact around 20% of the overall population. The prevalence of this phenomenon is slightly higher among females and individuals from affluent socioeconomic backgrounds and countries. Most people get them for the first time when they are a teenager or young adult. The age of onset may be during childhood, but more commonly in the second and third decades of life, becoming less common with advancing age. This disease is more common in women than in men. The cause of aphthous stomatitis is idiopathic and multifactorial but likely involves activation of the cell-mediated immune system. Since acute infections are not the cause of aphthous ulcers, they are not contagious. Local trauma, emotional or physiological stress, allergy or sensitivity, menstruation, or changes in the oral microbiome can all cause aphthous stomatitis. Aphthous ulcers are more prevalent in nonsmokers and smokers who quit and less common in individuals with good oral hygiene practices.73–75
The present treatment plan for this disease primarily focuses on managing symptoms, aiming to alleviate pain, facilitate lesion resolution, and extend the duration between episodes.76 The primary strategy for the treatment is to control the inflammation, suppress the inflammation-associated cells’ activity, reduce the pain of the lesion, and accelerate the healing process.77 The most commonly used anti-inflammatory agents to treat oral cavity inflammations are topical corticosteroids.78
Biological and laser therapies have emerged as novel therapeutic modalities for the treatment of mucosal diseases, garnering considerable anticipation in the medical community. Changes in oral microbiota have been linked to the development,79 which paves the way for probiotic treatments that can be put directly in the mouth. However, long-term exposure to these medications may cause drug resistance, oral flora imbalance, and secondary fungal infections.80
Natural extracts have already been proven effective for managing other oral health problems, apart from ulcers. Several clinical studies have shown the positive effects of natural extracts in reducing the pain and duration of mouth ulcers.45,79,80 A clinical study revealed that patients with aphthous ulcers treated with Nicotiana tabacum E. metabolites were likely to show reduced ulcer lesions compared to placebo, which was the control of the randomized control trial. The metabolites contributed to the suppression of pro-inflammatory cytokines and decreased the size of lesions on oral mucosa.46
Discussion
The investigation of anti-ulcerative activity has also encompassed the study of isolated metabolites derived from plants. The phytochemical constituents in plants have a variety of functions in anti-ulcerative activity, for example, alkaloids were reported for their anti-ulcerative effects by modulating the gastric acid secretion and cytoprotective properties.81 Flavonoids exhibit potent anti-inflammatory and antioxidant activity, contributing to ulcer healing and mucosal protection.82 Saponin has been found to inhibit gastric mucosal injuries induced by factors such as ethanol or indomethacin.83 Tannins, a type of phytochemical can form protective barriers on the mucosal surface,84 and polyphenols, which are also found in plants have multifaceted actions, such as anti-secretory and anti-inflammatory effects.82 Hence, plants are paving the way for the development of targeted and efficacious treatments for ulcerative disorders. The assessment of potential anti-ulcerative activities in plants that are often used to treat ulcers is a very important step in proving that these plants work as medicines. Various plant materials may exhibit multiple types of anti-ulcer effects, including safeguarding the mucosa against ulcers and impeding pro-inflammatory cytokine activity. This is attributed to the fact that individuals with chronic wounds, such as ulcers, tend to have elevated systemic and local levels of TNF-α.
The mitogen-activated protein kinase (MAPK) pathway plays a crucial role in the regulation of pro-inflammatory cytokine production, including interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α). This substance is classified as a proinflammatory cytokine that is rapidly secreted in response to an inflammatory stimulus. It plays a critical role in initiating various intracellular processes and is involved in the development of both acute and chronic inflammatory responses. This leads to the activation of nuclear factor kappa B (NF-kappaB), as well as the promotion of the release of additional pro-inflammatory cytokines, chemokines, and proteases.85 The overproduction of TNF-α has a direct correlation with various inflammatory disorders, including arthritis and inflammatory bowel disease. Consequently, regulating TNF-α levels can serve as an effective therapeutic approach for managing these diseases.86
Cytokine proinflammatory factors, such as IL-1, TNF-α, IL-6, and IFN-γ, were found to be upregulated.87 These factors are known to be involved in gastric inflammation caused by H. pylori. The involvement of the acute phase response pathway and NF-kappaB signaling pathways was also suggested.88 TNF-α plays a key role in mediating inflammatory events, involved in both acute and chronic responses.89 IL-6 produces an acute phase response, promoting the induction of intracellular signaling cascades, which give rise to the production of other inflammatory cytokines.90 At first, proinflammatory cytokines help acute wounds heal by boosting the growth of keratinocytes and making them make more antimicrobial peptides. Nevertheless, excessive production of proinflammatory cytokines can result in the persistence of inflammation and impaired wound healing.91,92 Hence, the therapeutic efficacy of chronic wound healing can be attributed to the inhibition of excessive proinflammatory cytokines.93 The extract contained phenolic compounds that demonstrated antioxidant properties by inhibiting oxidative stress, reducing the production of nitric oxide (NO), and preventing the activation of p38. Consequently, this inhibition led to the suppression of tumor necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6), thereby exhibiting anti-inflammatory and antiulcerogenic effects.16
The suggested mechanisms of action are explained through cytoprotective mechanism (causing an increase in gastric mucus), antioxidant activity (preventing depletion of sulfhydryl groups and reducing levels of lipid peroxidation and myeloperoxidase activity in the gastric mucosa), and finally healing ability.94,95 The small size of metabolites facilitates their passage through the mucus layer, enabling them to interact with colonic cells and initiate immune responses.91,93,96,97 Hence, metabolites derived from plants possess the potential to modulate the advancement of intestinal inflammation, thereby offering translational prospects.71 Ulcer, being a chronic inflammatory disease, exhibits distinct characteristics during the progression of chronic inflammation in the colon.98 Notably, the integrity of the mucus layer remains largely unaffected, and the permeability of the epithelial lining undergoes minimal alterations. In contrast, the acute colitis model demonstrates significant compromise to both the mucus layer and the permeability of the epithelial lining.71
In the present study, we found two plants with double anti-ulcerative activities, ie, T. erecta (strong anti-peptic ulcer disease and anti-ulcerative colitis) and M. citrifolia (strong anti-ulcerative colitis and weak anti-aphthous ulcer), thus presuming their potential to be further developed as anti-ulcer botanical drugs.
Conclusion
This review elaborates on an overview of the preclinical and clinical studies that have been done on medicinal plants. It focuses on how well they work to treat conditions such as peptic ulcer disease (PUD), ulcerative colitis (UC), and aphthous ulcers. The phytochemicals and pharmacological properties have also been elucidated. These active metabolites, derived from various plant sources such as alkaloids, flavonoids, tannins, saponins, and polyphenols, have a variety of functions in the treatment of ulcers and contribute synergistic interactions to the anti-ulcerative efficacy of plant extracts. For most of the plants that have been looked at, however, there is a clear lack of anti-H. pylori activity and clinical studies on metabolites derived from plant studies. The opportunity to conduct such studies is available to determine whether these plants possess both clinical and non-clinical properties. Also, there is a limitation of the study, we found that not all articles explain the controls used in preclinical and clinical studies, not all articles explain where and when the plants were collected, and not all articles explain the extraction method and solvent used which makes this article a constraint. More pharmacological activity assays are needed to figure out the mechanism of how each metabolite works, for example, by studying what proteins, pathways, or genes are altered by the plant extract or metabolite. These studies will be essential to validate the potential use of these metabolites in the treatment of ulcers. From a future perspective in the realm of plants, we can anticipate the isolation and synthesis of the active metabolites from plants for their capability as targeted therapies with enhanced efficacy and reduced potential for adverse effects. This review provides a piece of scientific evidence supporting the utilization of plant metabolites as a potential therapeutic approach for the treatment of ulcers.
Acknowledgments
The authors thank the Rector of Universitas Padjadjaran for funding the APC via the Directorate of Research and Community Engagement.
Disclosure
The authors declared no potential conflicts of interest to the research, authorship, or publication of this article.
References
1. Kuna L, Jakab J, Smolic R, Raguz-Lucic N, Vcev A, Smolic M. Peptic ulcer disease: a brief review of conventional therapy and herbal treatment options. J Clin Med. 2019;8(2):179. doi:10.3390/jcm8020179
2. Choi W, Choi CH, Kim YR, Kim SJ, Na CS, Lee H. HerDing: herb recommendation system to treat diseases using genes and chemicals. Database. 2016;2016:baw011. doi:10.1093/database/baw011
3. Lin LT, Hsu WC, Lin CC. Antiviral natural products and herbal medicines. J Tradit Complement Med. 2014;4(1):24–35. doi:10.4103/2225-4110.124335
4. Gupta M, Kapoor B, Gupta R, Singh N. Plants and phytochemicals for treatment of peptic ulcer: an overview. South Afr J Bot. 2021;138:105–114. doi:10.1016/j.sajb.2020.11.030
5. Zhang L, Zhuang H, Zhang Y, et al. Plants for health: an ethnobotanical 25-year repeat survey of traditional medicine sold in a major marketplace in North-west Yunnan, China. J Ethnopharmacol. 2018;224:119–125. doi:10.1016/j.jep.2018.05.029
6. Aslam B, Awan T, Javed I, Khaliq T, Khan JA, Raza A. Gastroprotective and antioxidant potential of Glycyrrhiza glabra on experimentally induced gastric ulcers in albino mice. Int J Curr Microbiol App Sci. 2015;4:451–460.
7. Ghosh V, Sugumar S, Mukherjee A, Chandrasekaran N. Neem (Azadirachta indica) Oils. In: Essential Oils in Food Preservation, Flavor and Safety. Academic Press; 2016:593–599.
8. Kim KH, Lee D, Lee HL, Kim CE, Jung K, Kang KS. Beneficial effects of Panax ginseng for the treatment and prevention of neurodegenerative diseases: past findings and future directions. J Ginseng Res. 2018;42(3):239–247. doi:10.1016/j.jgr.2017.03.011
9. Mortazavi H, Safi Y, Baharvand M, Rahmani S. Diagnostic features of common oral ulcerative lesions: an updated decision tree. Int J Dent. 2016;2016:1–14. doi:10.1155/2016/7278925
10. Scally B, Emberson JR, Spata E, et al. Effects of gastroprotectant drugs for the prevention and treatment of peptic ulcer disease and its complications: a meta-analysis of randomised trials. Lancet Gastroenterol Hepatol. 2018;3(4):231–241. doi:10.1016/S2468-1253(18)30037-2
11. Bento EB, de B. Júnior FE, de Oliveira DR, et al. Antiulcerogenic activity of the hydroalcoholic extract of leaves of Annona muricata Linnaeus in mice. Saudi J Biol Sci. 2016;25(4):609–621. doi:10.1016/j.sjbs.2016.01.024
12. da Silvada Silvada Silva LM, de M. Burci L, Crestani S, et al. Acid-gastric antisecretory effect of the ethanolic extract from Arctium lappa L. root: role of H+, K+-ATPase, Ca2+ influx and the cholinergic pathway. Inflammopharmacology. 2018;26(2):521–530. doi:10.1007/s10787-017-0378-4
13. Boeing T, de Souzade Souza J, da Silva RCV, et al. Gastroprotective effect of Artemisia absinthium L.: a medicinal plant used in the treatment of digestive disorders. J Ethnopharmacol. 2023;312:116488. doi:10.1016/j.jep.2023.116488
14. Kouitcheu Mabeku LB, Eyoum Bille B, Tchouangueu TF, Nguepi E, Leundji H. Treatment of Helicobacter pylori infected mice with Bryophyllum pinnatum, a medicinal plant with antioxidant and antimicrobial properties, reduces bacterial load. Pharm Biol. 2017;55(1):603–610. doi:10.1080/13880209.2016.1266668
15. de Oliveira BMM, Serpa PZ, da Costa Zanatta ME, et al. Gastroprotective and gastric healing effects of the aqueous extract of Casearia sylvestris in rodents: ultrasound, histological and biochemical analyzes. J Ethnopharmacol. 2022;298:115660. doi:10.1016/j.jep.2022.115660
16. Dörr JA, Majolo F, Bortoluzzi L, et al. Antiulcerogenic potential of the ethanolic extract of Ceiba speciosa (A. St.-Hil.) ravenna evaluated by in vitro and in vivo studies. Int J Mol Sci. 2022;23(24):15634. doi:10.3390/ijms232415634
17. Azaba SS, Abdel Jaleelb GA, Eldahshanc OA. Anti-inflammatory and gastroprotective potential of leaf essential oil of Cinnamomum glanduliferum in ethanol-induced rat experimental gastritis. Pharm Biol. 2017;55(1):1654–1661. doi:10.1080/13880209.2017.1314512
18. Ajaib M, Ishtiaq S, Ishtiaq M, et al. Analysis of antidiabetic, antiulcer and analgesic potential of traditional ethnomedicinal plant Emex spinosa (L.) Campd. from Azad Jammu and Kashmir. PLoS One. 2022;17(10):1–21. doi:10.1371/journal.pone.0274706
19. Saberi A, Abbasloo E, Sepehri G, et al. The effects of methanolic extract of Melissa Officinalis on experimental gastric ulcers in rats. Iran Red Crescent Med J. 2016;18(7). doi:10.5812/ircmj.24271
20. Mostofa R, Ahmed S, Begum MM, et al. Evaluation of anti-inflammatory and gastric anti-ulcer activity of Phyllanthus niruri L. (Euphorbiaceae) leaves in experimental rats. BMC Complement Altern Med. 2017;17(1):1–10. doi:10.1186/s12906-017-1771-7
21. Brito SA, de Almeidade Almeida CLF, de Santana TI, et al. Antiulcer Activity and Potential Mechanism of Action of the Leaves of Spondias mombin L. Oxid Med Cell Longev. 2018;2018:1–20. doi:10.1155/2018/1731459
22. Meurer MC, Mees M, Mariano LNB, et al. Hydroalcoholic extract of Tagetes erecta L. flowers, rich in the carotenoid lutein, attenuates inflammatory cytokine secretion and improves the oxidative stress in an animal model of ulcerative colitis. Nutri Res. 2019;66:95–106. doi:10.1016/j.nutres.2019.03.005
23. Silva LP, De Angelis CD, Bonamin F, et al. A medicinal plant from the Caribbean pharmacopeia with anti-Helicobacter pylori and antiulcer action in experimental rodent models. J Ethnopharmacol. 2015;159:285–295. doi:10.1016/j.jep.2014.11.025
24. Rodriguez-Canales M, Jimenez-Rivas R, Canales-Martinez MM, et al. Protective effect of amphipterygium adstringens extract on dextran sulphate sodium-induced ulcerative colitis in mice. Mediators Inflamm. 2016;2016:1–12. doi:10.1155/2016/8543561
25. Deng X, Wang Y, Tian L, et al. Anneslea fragrans Wall. ameliorates ulcerative colitis via inhibiting NF-κB and MAPK activation and mediating intestinal barrier integrity. J Ethnopharmacol. 2021;278:114304. doi:10.1016/j.jep.2021.114304
26. Szandruk M, Merwid-Ląd A, Szeląg A. The impact of mangiferin from Belamcanda chinensis on experimental colitis in rats. Inflammopharmacology. 2018;26(2):571–581. doi:10.1007/s10787-017-0337-0
27. Sharma A, Tirpude NV, Kulurkar PM, Sharma R, Padwad Y. Berberis lycium fruit extract attenuates oxi-inflammatory stress and promotes mucosal healing by mitigating NF-κB/c-Jun/MAPKs signalling and augmenting splenic Treg proliferation in a murine model of dextran sulphate sodium-induced ulcerative colitis. Eur J Nutr. 2020;59(6):2663–2681. doi:10.1007/s00394-019-02114-1
28. Dou YX, Zhou JT, Wang TT, et al. Self-nanoemulsifying drug delivery system of bruceine D: a new approach for anti-ulcerative colitis. Int J Nanomed. 2018;13:5887–5907. doi:10.2147/IJN.S174146
29. Mahmoud TN, El-Maadawy WH, Kandil ZA, Khalil H, El-fiky NM, El Alfy TSMA. Canna x generalis L.H. Bailey rhizome extract ameliorates dextran sulfate sodium-induced colitis via modulating intestinal mucosal dysfunction, oxidative stress, inflammation, and TLR4/ NF-ҡB and NLRP3 inflammasome pathways. J Ethnopharmacol. 2021;269:113670. doi:10.1016/j.jep.2020.113670
30. Li H, Chen X, Liu J, et al. Ethanol extract of Centella asiatica alleviated dextran sulfate sodium-induced colitis: restoration on mucosa barrier and gut microbiota homeostasis. J Ethnopharmacol. 2021;267:113445. doi:10.1016/j.jep.2020.113445
31. Sudirman S, Hsu YH, He JL, Kong ZL, Nakano H. Dietary polysaccharide-rich extract from Eucheuma cottonii modulates the inflammatory response and suppresses colonic injury on dextran sulfate sodiuminduced colitis in mice. PLoS One. 2018;13(10):1–15. doi:10.1371/journal.pone.0205252
32. Shen P, Zhang Z, Zhu K, et al. Evodiamine prevents dextran sulfate sodium-induced murine experimental colitis via the regulation of NF-κB and NLRP3 inflammasome. Biomed Pharmacother. 2019;110:786–795. doi:10.1016/j.biopha.2018.12.033
33. Kim TW, Shin JS, Chung KS, Lee YG, Baek NI, Lee KT. Anti-inflammatory mechanisms of koreanaside a, a lignan isolated from the flower of forsythia koreana, against LPS-induced macrophage activation and DSS-induced colitis mice: the crucial role of AP-1, NF-κB, and JAK/STAT signaling. Cells. 2019;8(10):1163. doi:10.3390/cells8101163
34. Farombi EO, Adedara IA, Ajayi BO, Ayepola OR, Egbeme EE. Kolaviron, a natural antioxidant and anti-inflammatory phytochemical prevents dextran sulphate sodium-induced colitis in rats. Basic Clin Pharmacol Toxicol. 2013;113(1):49–55. doi:10.1111/bcpt.12050
35. Wang Y, Wang Y, Shen W, et al. Grape seed polyphenols ameliorated dextran sulfate sodium-induced colitis via suppression of inflammation and apoptosis. Pharmacology. 2020;105(1–2):9–18. doi:10.1159/000501897
36. Aleisa AM, Al-Rejaie SS, Abuohashish HM, Ola MS, Parmar MY, Ahmed MM. Pretreatment of Gymnema sylvestre revealed the protection against acetic acid-induced ulcerative colitis in rats. BMC Complement Altern Med. 2014;14(1):1–11. doi:10.1186/1472-6882-14-49
37. Le Song J, Qian Y, Li GJ, Zhao X. Anti-inflammatory effects of kudingcha methanol extract (Ilex kudingcha C.J. Tseng) in dextran sulfate sodium-induced ulcerative colitis. Mol Med Rep. 2013;8(4):1256–1262. doi:10.3892/mmr.2013.1635
38. Batista JA, de Aguiar Magalhães D, Sousa SG, et al. Polysaccharides derived from Morinda citrifolia Linn reduce inflammatory markers during experimental colitis. J Ethnopharmacol. 2020;248:112303. doi:10.1016/j.jep.2019.112303
39. Elmaksoud HAA, Motawea MH, Desoky AA, Elharrif MG, Ibrahimi A. Hydroxytyrosol alleviate intestinal inflammation, oxidative stress and apoptosis resulted in ulcerative colitis. Biomed Pharmacother. 2021;142:112073. doi:10.1016/j.biopha.2021.112073
40. Ayaz M, Junaid M, Ullah F, et al. GC-MS analysis and gastroprotective evaluations of crude extracts, isolated saponins, and essential oil from Polygonum hydropiper L. Front Chem. 2017;1–11. doi:10.3389/fchem.2017.00058
41. Meurer M, Gonçalves B, Cury BJ, et al. Extract of Tagetes erecta L., a medicinal plant rich in lutein, promotes gastric healing and reduces ulcer recurrence in rodents. J Ethnopharmacol. 2022;293:115258. doi:10.1016/j.jep.2022.115258
42. Ding A, Wen X. Dandelion root extract protects NCM460 colonic cells and relieves experimental mouse colitis. J Nat Med. 2018;72(4):857–866. doi:10.1007/s11418-018-1217-7
43. Gautam MK, Goel S, Ghatule RR, Singh A, Nath G, Goel RK. Curative effect of Terminalia chebula extract on acetic acid-induced experimental colitis: role of antioxidants, free radicals and acute inflammatory marker. Inflammopharmacology. 2013;21(5):377–383. doi:10.1007/s10787-012-0147-3
44. Rezeki S, Vidirachmilla N. The effect of noni leaves extract (Morinda citrifolia L) on wound healing percentage of traumatic ulcer in oral mucosa of Wistar rats (rattus norvegicus) by in vivo. Biomed Pharmacol J. 2017;10(4):1735–1740. doi:10.13005/bpj/1286
45. Gavanji S, Larki B, Bakhtari A. The effect of extract of Punica granatum var. pleniflora for treatment of minor recurrent aphthous stomatitis. Integr Med Res. 2014;3(2):83–90. doi:10.1016/j.imr.2014.03.001
46. Vaziri S, Mojarrab M, Farzaei MH, Najafi F, Ghobadi A. Evaluation of anti-aphthous activity of decoction of Nicotiana tabacum leaves as a mouthwash: a placebo-controlled clinical study. J Tradit Chin Med. 2016;36(2):160–164. doi:10.1016/s0254-6272(16)30022-x
47. Hajiaghamohammadi AA, Zargar A, Oveisi S, Samimi R, Reisian S. To evaluate of the effect of adding licorice to the standard treatment regimen of Helicobacter pylori. Brazilian J Infect Dis. 2016;20(6):534–538. doi:10.1016/j.bjid.2016.07.015
48. Zhang M, Viennois E, Prasad M, et al. Edible ginger-derived nanoparticles: a novel therapeutic approach for the prevention and treatment of inflammatory bowel disease and colitis-associated cancer. Biomaterials. 2016;101:321–340. doi:10.1016/j.biomaterials.2016.06.018
49. Ansari M, Hashemipour M, Farsinejad A, et al. Clinical efficacy of a buccoadhesive paste from Fenugreek seeds (Trigonella foenum graecum L.) on recurrent aphthous stomatitis: in-vitro assessment of non-toxic concentration and pilot trial. Adv Integr Med. 2022;9(1):17–21. doi:10.1016/j.aimed.2021.06.001
50. Malik T, Singh K, Gnanapandithan K. Peptic Ulcer Disease. StatPearls Publishing; 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK534792/.
51. Lanas A, Chan F. Peptic ulcer disease. Lancet. 2017;390(10094):613–624. doi:10.1016/S0140-6736(16)32404-7
52. Agreus L, Talley N, Jones M. Value of the “Test & Treat” strategy for uninvestigated dyspepsia at low prevalence rates of helicobacter pylori in the population. Helicobacter. 2016;21(3):186–191. doi:10.1111/hel.12267
53. Narayanan M, Reddy KM, Marsicano E. Peptic ulcer disease and helicobacter pylori infection. Mo Med. 2018;115(3):219–224. doi:10.1097/00001574-199208010-00019
54. Lanas-Gimeno A, Lanas A. Risk of gastrointestinal bleeding during anticoagulant treatment. Expert Opin Drug Saf. 2017;16(6):673–685. doi:10.1080/14740338.2017.1325870
55. Molnar T. Pathogenesis of ulcerative colitis and Crohn’s disease: similarities, differences and a lot of things we do not know yet. J Clin Cell Immunol. 2014;05(04). doi:10.4172/2155-9899.1000253
56. Probert CSJ, Dignass AU, Lindgren S, Oudkerk Pool M, Marteau P. Combined oral and rectal mesalazine for the treatment of mild-to-moderately active ulcerative colitis: rapid symptom resolution and improvements in quality of life. J Crohn’s Colitis. 2014;8(3):200–207. doi:10.1016/j.crohns.2013.08.007
57. Kapoor B, Kaur G, Gupta M, Gupta R. Sub-chronic safety evaluation of aqueous extract of Alangium salvifolium (L.f.) Wangerin leaves in rats. J Adv Pharm Technol Res. 2017;8(3):108–113. doi:10.4103/japtr.JAPTR_69_17
58. Gisbert JP, Chaparro M. Acute severe ulcerative colitis: state of the art treatment. Best Pract Res Clin Gastroenterol. 2018;32–33:59–69. doi:10.1016/j.bpg.2018.05.007
59. Lynch W, Hsu R. Ulcerative Colitis. StatPearls Publishing; 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459282/.
60. Cowie MR. National Institute for Health and Care Excellence. Eur Heart J. 2015;36(4):195.
61. Sz Tun G, Harris A, Lobo AJ. Ulcerative colitis: management in adults, children and young people – concise guidance. Clin Med. 2017;17(5):429–462. doi:10.7861/clinmedicine.17-5-429
62. Trivedi I, Darguzas E, Balbale SN, et al. Patient understanding of “flare” and “remission” of inflammatory bowel disease. Gastroenterol Nurs. 2019;42(4):375–385. doi:10.1097/SGA.0000000000000373
63. Lewis JD, Abreu MT. Diet as a trigger or therapy for inflammatory bowel diseases. Gastroenterology. 2017;152(2):398–414.e6. doi:10.1053/j.gastro.2016.10.019
64. Sarbagili-Shabat C, Sigall-Boneh R, Levine A. Nutritional therapy in inflammatory bowel disease. Curr Opin Gastroenterol. 2015;31(4):303–308. doi:10.1097/MOG.0000000000000178
65. Sigall-Boneh R, Levine A, Lomer M, et al. Research gaps in diet and nutrition in inflammatory bowel disease. A topical review by D-ECCO working group [Dietitians of ECCO]. J Crohn’s Colitis. 2017;11(12):1407–1419. doi:10.1093/ecco-jcc/jjx109
66. Yao CK, Sarbagili-Shabat C. Gaseous metabolites as therapeutic targets in ulcerative colitis. World J Gastroenterol. 2023;29(4):682–691. doi:10.3748/wjg.v29.i4.682
67. Roediger WEW. Causation of human ulcerative colitis: a lead from an animal model that mirrors human disease. JGH Open. 2019;3(4):277–280. doi:10.1002/jgh3.12212
68. Steinhart AH, Fernandes A. Clinical practice guidelines for the medical management of nonhospitalized ulcerative colitis: the patient perspective. Can J Gastroenterol Hepatol. 2015;29(6):294–296. doi:10.1155/2015/214937
69. Ling T, Lang WH, Maier J, Centurion MQ, Rivas F. Cytostatic and cytotoxic natural products against cancer cell models. Molecules. 2019;24(10):2012. doi:10.3390/molecules24102012
70. Shayesteh F, Haidari F, Shayesteh AA, Mohammadi-Asl J, Ahmadi-Angali K. Ginger in patients with active ulcerative colitis: a study protocol for a randomized controlled trial. Trials. 2020;21(1):1–6. doi:10.1186/s13063-020-4193-7
71. Yang C, Sung J, Long D, Alghoul Z, Merlin D. Prevention of ulcerative colitis by autologous metabolite transfer from colitogenic microbiota treated with lipid nanoparticles encapsulating an anti-inflammatory drug candidate. Pharmaceutics. 2022;14(6):1233. doi:10.3390/pharmaceutics14061233
72. InformedHealth.org. Canker Sores (mouth ulcers). Inst Qual Effic Heal Care; 2019. Available from: https://www.ncbi.nlm.nih.gov/books/NBK546250/.
73. Grimaux X, Leducq S, Goupille P, Aubourg A, Miquelestorena-Standley E, Samimi M. Aphthous mouth ulcers as an initial manifestation of sécukinumab-induced inflammatory bowel disease. Ann Dermatol Venereol. 2018;145(11):676–682. doi:10.1016/j.annder.2018.07.009
74. Borilova Linhartova P, Janos J, Slezakova S, et al. Recurrent aphthous stomatitis and gene variability in selected interleukins: a case–control study. Eur J Oral Sci. 2018;126(6):485–492. doi:10.1111/eos.12577
75. Brignardello-Petersen R. Patients who seek professional treatment of recurrent aphthous stomatitis probably have an increased risk of having head and neck cancer and other types of cancers. J Am Dent Assoc. 2019;150(2):e24. doi:10.1016/j.adaj.2018.09.011
76. Liu H, Tan L, Fu G, Chen L, Tan H. Efficacy of topical intervention for recurrent aphthous stomatitis: a network meta-analysis. Med. 2022;58. doi:10.3390/medicina58060771
77. Sridevi Anjuga EP, Aravindha Babu N. Guidelines for diagnosis and treatment of recurrent aphthous stomatitis for dental practitioners. Indian J Forensic Med Toxicol. 2020;14:1099–1104. doi:10.37506/ijfmt.v14i4.11657
78. Altenburg A, El-Haj N, Micheli C, et al. The treatment of chronic recurrent oral aphthous ulcers. Dtsch Arztebl Int. 2014;111(40):665–673. doi:10.3238/arztebl.2014.0665
79. Yuan H, Qiu J, Zhang T, Wu X, Zhou J, Park S. Quantitative changes of Veillonella, Streptococcus, and Neisseria in the oral cavity of patients with recurrent aphthous stomatitis: a systematic review and meta-analysis. Arch Oral Biol. 2021;129. doi:10.1016/j.archoralbio.2021.105198
80. Rostas A, McLean DI, Wilkinson RD. Management of recurrent aphthous stomatitis - A review. Res J Pharm Technol. 2014;7:1193–1195.
81. Muni Raja Lakshmi K, Kiran M, Sai Prasanna K. A review on natural plants for phytochemical constituents and pharmacological activities. J Drug Delivery Ther. 2021;11(2):232–236. doi:10.22270/jddt.v11i2.4593
82. Cheng YT, Lu CC, Yen GC. Phytochemicals enhance antioxidant enzyme expression to protect against NSAID-induced oxidative damage of the gastrointestinal mucosa. Mol Nutr Food Res. 2017;61. doi:10.1002/mnfr.201600659
83. Jo HJ, Kim N, Nam RH, et al. The effect of cochinchina momordica seed extract on gastric acid secretion and morphologic change in aged rat stomach. Gut Liver. 2013;7(5):560–568. doi:10.5009/gnl.2013.7.5.560
84. Ngoua-Meye-Misso R-L, Sima-Obiang C, Ndong JDLC, Ondo JP, Ovono Abessolo F, Obame-Engonga L-C. Phytochemical screening, antioxidant, anti-inflammatory and antiangiogenic activities of Lophira procera A. Chev. (Ochnaceae) medicinal plant from Gabon. Egypt J Basic Appl Sci. 2018;5:80–86. doi:10.1016/j.ejbas.2017.11.003
85. Sorg C. Macrophages in acute and chronic inflammation. Chest. 1991;100(3):173S–175S. doi:10.1378/chest.100.3.173s
86. Brenner D, Blaser H, Mak TW. Regulation of tumour necrosis factor signalling: live or let die. Nat Rev Immunol. 2015;15(6):362–374. doi:10.1038/nri3834
87. Kanji S, Das H. Advances of stem cell therapeutics in cutaneous wound healing and regeneration. Mediators Inflamm. 2017;2017:1–14. doi:10.1155/2017/5217967
88. Morningstar-Wright L, Czinn SJ, Piazuelo MB, Banerjee A, Godlewska R, Blanchard TG. The TNF-alpha inducing protein is associated with gastric inflammation and hyperplasia in a murine model of helicobacter pylori infection. Front Pharmacol. 2022;13:1–15. doi:10.3389/fphar.2022.817237
89. Coleman JW. Nitric oxide in immunity and inflammation. Int Immunopharmacol. 2001;1(8):1397–1406. doi:10.1016/S1567-5769(01)00086-8
90. Zhang J-M, An J. Cytokines, inflammation, and pain. Int Anesth Clin. 2007;45(2):27–37. doi:10.1097/AIA.0b013e318034194e
91. Xiao T, Yan Z, Xiao S, Xia Y. Proinflammatory cytokines regulate epidermal stem cells in wound epithelialization. Stem Cell Res Ther. 2020;11(1):1–9. doi:10.1186/s13287-020-01755-y
92. Boniakowski AE, Kimball AS, Jacobs BN, Kunkel SL, Gallagher KA. Macrophage-mediated inflammation in normal and diabetic wound healing. J Immunol. 2017;199(1):17–24. doi:10.4049/jimmunol.1700223
93. Ashcroft GS MN, Jeong MJ, Ashworth JJ, Hardman M, Jin W. Tumor necrosis factor-alpha (TNF-α) is a therapeutic target for impaired cutaneous wound healing. Wound Repair Regen. 2012;20(1):38–49. doi:10.1111/j.1524-475X.2011.00748.x
94. Rocha Caldas GF, Oliveira ARDS, Araújo AV, et al. Gastroprotective mechanisms of the monoterpene 1,8-cineole (eucalyptol). PLoS One. 2015;10(8):1–17. doi:10.1371/journal.pone.0134558
95. Al Asmari A, Al Shahrani H, Al Masri N, Al Faraidi A, Elfaki I, Arshaduddin M. Vanillin abrogates ethanol induced gastric injury in rats via modulation of gastric secretion, oxidative stress and inflammation, Toxicol. Reports. 2016;3:105–113. doi:10.1016/j.toxrep.2015.11.001
96. Ahmed I, Roy BC, Khan SA, Septer S, Umar S. Microbiome, metabolome and inflammatory bowel disease. Microorganisms. 2016;4(2):20. doi:10.3390/microorganisms4020020
97. Settanni CR, Ianiro G, Bibbò S, Cammarota G, Gasbarrini A. Gut microbiota alteration and modulation in psychiatric disorders: current evidence on fecal microbiota transplantation. Prog Neuro Psychopharmacol Biol Psychiatry. 2021;109:110258. doi:10.1016/j.pnpbp.2021.110258
98. Keubler LM, Buettner M, Häger C, Bleich A. A multihit model: colitis lessons from the interleukin-10-deficient mouse. Inflamm Bowel Dis. 2015;21(8):1967–1975. doi:10.1097/MIB.0000000000000468
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.