Back to Journals » International Medical Case Reports Journal » Volume 16
Pituitary Macroadenoma with Optic Cupping Masquerading as Normal Tension Glaucoma
Authors Cheng AM ![]() , Schecter S
, Schecter S ![]() , Komotar RJ, Tsai J, Gupta SK
, Komotar RJ, Tsai J, Gupta SK
Received 22 May 2023
Accepted for publication 5 July 2023
Published 14 July 2023 Volume 2023:16 Pages 419—423
DOI https://doi.org/10.2147/IMCRJ.S422426
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Anny M Cheng,1– 3,* Scott Schecter,4,* Ricardo Jorge Komotar,5 Joby Tsai,1,2 Shailesh K Gupta1,2
1Department of Ophthalmology, Broward Health, Fort Lauderdale, FL, USA; 2Specialty Retina Center, Coral Springs, FL, USA; 3Department of Ophthalmology, Florida International University, Herbert Wertheim College of Medicine, Miami, FL, USA; 4South Florida Vision, Fort Lauderdale, FL, USA; 5Department of Neurosurgery, University of Miami, Miami, FL, USA
*These authors contributed equally to this work
Correspondence: Shailesh K Gupta, Department of Ophthalmology, Broward Health, Fort Lauderdale, FL & Specialty Retina Center, 6280 W Sample Road# 202, Coral Springs, FL, 33067, USA, Tel +1 561 322-3588, Fax +1 754 812-5993, Email [email protected]
Abstract: When non-glaucomatous disease with disc cupping mimics normal-tension glaucoma (NTG), diagnosis is challenging. The typical optic disc features of glaucomatous disease are often subjective, and often overlap with disc changes in compressive intracranial lesions. Ancillary diagnostic testing such as retinal nerve fiber layer (RNFL) analysis and visual field testing can elevate the index of suspicion of an underlying non-glaucomatous process. We present a case of a nonfunctional macroadenoma coexisting with NTG, although it is unclear if the concurrent brain lesion aggravated or caused it. This case highlights the diagnostic challenge of recognizing optic cupping and non-matching abnormalities in the visual field from a coexisting intracranial lesion, even in the absence of other neurological signs.
Keywords: cupping, normal tension glaucoma, pituitary macroadenoma, visual field defects
Introduction
Normal-tension glaucoma (NTG) is characterized by optic nerve head cupping, retinal ganglion cell (RGC) loss, and visual field defects, whereas intraocular pressure (IOP) is within the normal range. Diagnosis is challenging when normal pressure non-glaucomatous disorders with disc cupping mimic NTG. Optic nerve cupping is an important diagnostic feature of glaucoma; however, it is not pathognomonic and may occur in non-glaucomatous diseases. The typical characteristics of glaucomatous changes include deepening of the optic cup, appearance of the optic nerve head, neuroretinal rim notching, disc hemorrhage, parapapillary atrophy, and symmetric retinal nerve fiber layer loss.1,2 Cupping with out-of-proportional neuroretinal rim pallor is more common in non-glaucomatous eyes. However, all of these funduscopic signs are subjective, and similar clinical cupping observations have been found in glaucoma and compressive intracranial lesions.
Patients with intracranial tumors have been reported to have normal IOP but glaucomatous-like optic discs.3–6 Studies show that the neuroradiological presence of a mass lesion in patients diagnosed with glaucoma varies from 0 to 14.2%.2,7 While part of the possible work-up, routine neuroimaging is not recommended for patients with presumed NTG, because of the low yield of intracranial pathological detection.2,8 Instead of imaging studies, the pattern of the visual field defect can be a diagnostic clue to identify the intracranial etiology if optic disc neuroretinal rim pallor is absent in examinations.6 Studies show that visual field defects related to vertical alignment are significantly associated with compressive intracranial pathology.2,6 This is an important clinical finding in isolated or coexisting intracranial masses and glaucoma, where the diagnosis of brain lesions may be overlooked. Therefore, a detailed record of visual field pattern changes is crucial. Herein, we present the identification of an associated brain mass in a NTG patient with significant optic disc cupping. Institutional approval was waived as our single case report involves retrospective medical record review of one patient and the only interaction with the patient has been for purposes of treating the patient and does not meet the Common Rule definition of research (45 CFR 164.501). Although institutional approval was not required to publish the case details, we obtained written informed consent from the patient for the publication of his case and any accompanying images.
Case Report
A healthy 65-year-old man presented with occasional blurred vision for one week. At the initial presentation, his best-corrected visual acuity was 20/25 bilaterally, and intraocular pressure was 16 mmHg in both eyes. Motility revealed a slight limitation of abduction in the left eye. Pupils were round and reactive without a relative afferent pupillary defect. Slit-lamp examination revealed mild bilateral nuclear cataracts. Fundus examination revealed clear media, normal color, and asymmetric optic nerve head cupping of 0.55 horizontally in the right eye and 0.85 horizontally in the left eye (Figure 1A). An initial diagnosis of “normal tension glaucoma” was made, and he was not treated with any topical glaucomic medications at the initial presentation. Optical coherence tomography (OCT) of the retinal nerve fiber layer (RNFL) showed bilateral superior and inferior thinning, which is consistent with glaucomatous changes; however, the left eye also showed temporal thinning (Figure 1B). Automated perimetry revealed bilateral nasal steps associated with temporal defects with respect to the vertical meridian (Figure 1C and D), raising the suspicion of an intracranial lesion other than glaucomatous change. Magnetic resonance imaging (MRI) of the brain (Figure 2) confirmed a 3.1×2.3 x 2.8 cm mass arising from the pituitary fossa, consistent with a macroadenoma, with mass effect on the optic chiasm, protrusion into the left cavernous sinus, and lateral displacement of the left internal carotid artery. The brain tumor was removed uneventfully after evaluation by a neurosurgeon (R.J.K.). Postoperative best-corrected visual acuity was 20/25 bilaterally, and visual field testing demonstrated resolution of bitemporal defects. Follow-up evaluation at 12 months revealed an intraocular pressure of 12 mmHg bilaterally under Lumigan (bimatoprost ophthalmic solution 0.01%, Allergan, AbbVie, USA) treatment for NTG, and cupping remained 0.55 in the right eye and 0.85 in the left eye, respectively.
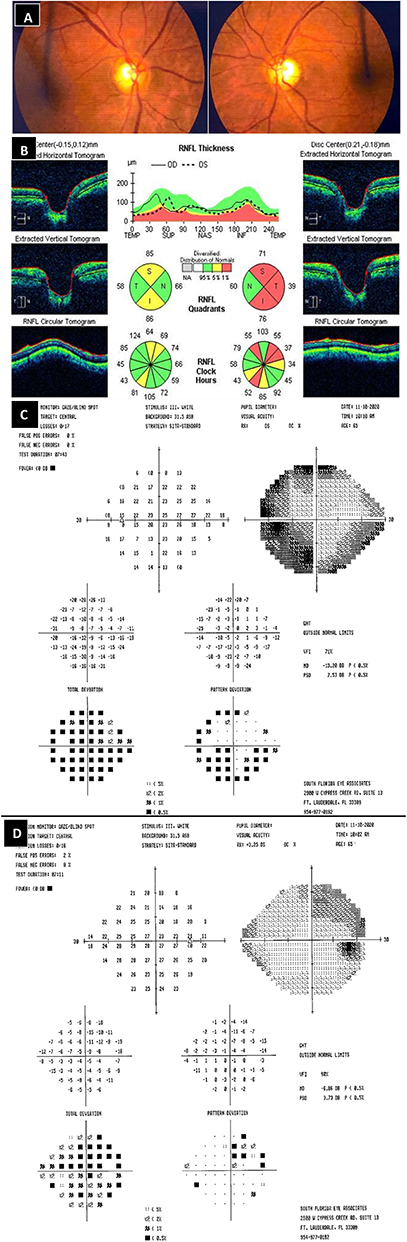 |
Figure 1 Asymmetric optic nerve head cupping of 0.55 horizontally in the right eye (left panel) and 0.85 horizontally in the left eye (right panel) (A). Optical coherence tomography of the retinal nerve fiber layer showed atrophy of the left optic nerve not only in the superior and inferior but also in the temporal portion (B). Pre-operative automated perimetry showed a bitemporal visual field defect respect to vertical meridian associated with nasal steps in the left eye (C) and right eye (D). |
 |
Figure 2 MRI sagittal (A) and coronal (B) T1 showed heterogeneous enhancing mass arising from pituitary fossa consistent with macroadenoma. |
Discussion
We present a case of a nonfunctional macroadenoma coexisting with glaucoma that highlights the importance of identifying nonglaucomatous visual field defects in the presence of concurrent glaucomatous changes. To avoid mismanagement of glaucoma, in particular NTG, we emphasize the importance of considering more than merely the morphology of the optic disc. It is not uncommon to interpret intracranial optic lesions as glaucomatous changes based on fundus examinations and, therefore, miss the diagnosis.9 Patients may have signs that raise suspicion about the presumptive diagnosis of NTG.
Clinically differentiating glaucomatous and non-glaucomatous etiologies can be challenging, especially in NTG, like in our patient, who presented with cupping and normal IOP without pallor.2,8 Although pallor of the neuroretinal rim is a hallmark non-glaucomatous finding,10 a recent study suggests that the absence of pallor can be due to the difficulty in evaluating patients with little neuroretinal rim left in glaucoma.8 This may explain why we did not appreciate the rim pallor in our patient. In addition, our patient did not present with clinical manifestations such as reduction in central visual acuity, rapid afferent pupillary defect (RAPD), or optic disc edema that have been more easily associated with intracranial lesions.
In addition to studying the appearance of the optic disc and other clinical clues, ancillary diagnostic tests such as RNFL and visual field testing can help increase the index of suspicion for non-glaucomatous disease. A detailed assessment of the optic nerve in relation to visual field defects is critical, as glaucomatous cupping is correlated with visual field deficits. Therefore, non-glaucomatous lesions should be suspected in patients with cupping non-matching visual field defects. Importantly, it is critical to distinguish patients with visual field defects with respect to the vertical meridian from those with typical glaucomatous defects with respect to the horizontal midline. Although unilateral NTG is possible, unilateral or asymmetric cupping may favor a non-glaucomatous cause, such as in our patient. One published report showed that the laminal cribrosa in NTG undergoes significant remodeling, promoting damage to axons that precedes IOP-induced retinal nerve fiber layer loss.11 This suggests that pathologic changes in NTG are more generalized and less likely to be asymmetric or caused by local factors. Additional examinations, such as MRI, can be employed to confirm and localize the underlying cause. Intriguingly, it is unclear whether the coexisting brain macroadenoma, in our case, aggravated or caused NTG. NTG development in our patient may be caused by optic nerve susceptibility to intraocular pressure and/or macroadenoma-induced compression. Regardless of whether the mechanism of NTG in our patient is incidental or casually related, this case highlights the importance of carefully analyzing the visual field deficiency induced by brain lesions that simulate glaucoma cupping, which also coexists with glaucoma, for better time management and surgical planning.
Funding
This study was not supported by any grant.
Disclosure
None of the authors have conflicts of interest.
References
1. Jonas JB, Budde WM. Optic nerve head appearance in juvenile-onset chronic high-pressure glaucoma and normal-pressure glaucoma. Ophthalmology. 2000;107(4):704–711. doi:10.1016/S0161-6420(99)00172-4
2. Greenfield DS, Siatkowski RM, Glaser JS, Schatz NJ, Parrish RK. The cupped disc. Ophthalmology. 1998;105(10):1866–1874. doi:10.1016/S0161-6420(98)91031-4
3. Pellegrini F, Marullo M, Zappacosta A, Liberali T, Cuna A, Lee AG. Suprasellar meningioma presenting with glaucomatous type cupping. Eur J Ophthalmol. 2021;31(6):NP36–NP40. doi:10.1177/1120672120937674
4. Karl D, Gillan SN, Goudie C, Sanders R. Giant prolactinoma mimicking low-tension glaucoma at presentation. Case Rep. 2015;2015(feb06 1):bcr2014207634–bcr2014207634.
5. Drummond SR, Weir C. Chiasmal compression misdiagnosed as normal-tension glaucoma: can we avoid the pitfalls? Int Ophthalmol. 2010;30(2):215–219. doi:10.1007/s10792-009-9308-9
6. Choudhari N, Neog A, Fudnawala V, George R. Cupped disc with normal intraocular pressure: the long road to avoid misdiagnosis. Indian J Ophthalmol. 2011;59(6):491. doi:10.4103/0301-4738.86320
7. Kosior-Jarecka E, Wróbel-Dudzińska D, Pietura R, et al. Results of neuroimaging in patients with atypical normal-tension glaucoma. Biomed Res Int. 2020;2020:1–8. doi:10.1155/2020/9093206
8. Donaldson L, Dezard V, Margolin E. Yield of investigations in patients with questionable nonglaucomatous optic neuropathy. Can J Ophthalmol. 2022;58:219–223. doi:10.1016/j.jcjo.2022.01.013
9. Trobe JD, Glaser JS, Cassady J, Herschler J, Anderson DR. Nonglaucomatous excavation of the optic disc. Arch Ophthalmol. 1980;98(6):1046–1050. doi:10.1001/archopht.1980.01020031036004
10. Lee AG. Differentiating glaucomatous from nonglaucomatous optic atrophy. Ophthalmology. 1999;106(5):855. doi:10.1016/S0161-6420(99)10109-X
11. Kim JA, Kim TW, Lee EJ, Kim JM, Girard MJA, Mari JM. Intereye comparison of lamina cribrosa curvature in normal tension glaucoma patients with unilateral damage. Invest Ophthalmol Vis Sci. 2019;60(7):2423. doi:10.1167/iovs.19-26828
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.