Back to Journals » Nature and Science of Sleep » Volume 12
Pitolisant to Treat Excessive Daytime Sleepiness and Cataplexy in Adults with Narcolepsy: Rationale and Clinical Utility
Authors Guevarra JT ![]() , Hiensch R
, Hiensch R ![]() , Varga AW
, Varga AW ![]() , Rapoport DM
, Rapoport DM ![]()
Received 23 May 2020
Accepted for publication 13 August 2020
Published 12 October 2020 Volume 2020:12 Pages 709—719
DOI https://doi.org/10.2147/NSS.S264140
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sutapa Mukherjee
Jay T Guevarra, Robert Hiensch, Andrew W Varga, David M Rapoport
Division of Pulmonary, Critical Care, and Sleep Medicine, Mount Sinai Integrative Sleep Center, Icahn School of Medicine at Mount Sinai, New York, NY 10029, USA
Correspondence: Jay T Guevarra
Division of Pulmonary, Critical Care, and Sleep Medicine, Mount Sinai Integrative Sleep Center, Icahn School of Medicine at Mount Sinai, One Gustave L. Levy Place, New York, NY 10029, USA
Tel +1 646 339-3862
Fax +1 212 876 5519
Email [email protected]
Abstract: Narcolepsy is a sleep disorder marked by chronic, debilitating excessive daytime sleepiness and can be associated with cataplexy, sleep paralysis and sleep-related hallucinations. Pharmacological therapy for narcolepsy primarily aims to increase wakefulness and reduce cataplexy attacks. Pitolisant is a first-in-class agent utilizing histamine to improve wakefulness by acting as an antagonist/inverse agonist of the presynaptic histamine 3 receptor. This review summarizes the clinical efficacy, safety and tolerability of pitolisant in treating the symptoms of narcolepsy. Randomized and observational studies demonstrate pitolisant to be effective in treating both hypersomnolence and cataplexy while generally being well tolerated at prescribed doses. The most common adverse reactions include headache, insomnia and nausea.
Keywords: narcolepsy, pitolisant, histamine 3 receptor, excessive daytime sleepiness, cataplexy
Plain Language Summary
Narcolepsy is a rare chronic sleep disorder associated with debilitating excessive daytime sleepiness, cataplexy, sleep-related hallucinations and sleep paralysis. It affects approximately 0.02%-0.05% of various populations in European, USA and Asian countries. In addition to physical symptoms, patients often have a decreased quality of life, with daytime sleepiness affecting their social and work productivity. The deficiency of a brain neuropeptide, hypocretin, has been implicated as a main cause of narcolepsy. Histamine works alongside hypocretin in regulating an individual’s sleep/wake cycle. Increased histamine levels are found during wakefulness and return to lower levels during sleep. Pitolisant is the first drug in its class that increases levels of histamine by targeting the histamine 3 receptor. This review goes over the clinical outcomes, safety and tolerability of using pitolisant to treat narcolepsy.
Introduction
Narcolepsy is a clinical syndrome marked by chronic, debilitating excessive daytime sleepiness (EDS) and the presence of arousal state instability where the thresholds between the various stages of sleep and wake are easily crossed.1,2 There are two types of narcolepsy, differentiated by the presence of cataplexy (recurrent brief episodes of sudden, usually symmetrical loss of muscle tone with retained consciousness precipitated by strong emotions) and cerebral spinal fluid (CSF) hypocretin-1 levels.3 Narcolepsy type 1 (often referred to as narcolepsy with cataplexy) is distinguished by either the presence of cataplexy or low CSF hypocretin-1 levels (=<110 pg/mL) and is estimated to have a prevalence of 14–50 per 100,000 people and an incidence of 4.87 per 100,000 person-years.4–6 Narcolepsy type 2 has absent cataplexy and either normal (>110 pg/mL) or unmeasured CSF hypocretin-1 levels.2 The prevalence of narcolepsy type 2 is not well studied, but estimated to be about 20–65 per 100,000 people.6,7 Other symptoms common to both narcolepsy types 1 and 2 include fragmented, disrupted sleep, hypnogogic and hypnopompic hallucinations (vivid auditory or visual dreamlike perceptions at sleep onset or offset), automatic behaviors (activities performed without awareness) and sleep paralysis (temporary inability to move while falling asleep or awakening).4,8 Patients with narcolepsy may enter rapid eye movement sleep (REM) earlier (<90 min) after nighttime sleep initiation and have sleep-onset REM periods that occur during daytime naps. Other sleep abnormalities are also common, including sleep-disordered breathing, periodic limb movements of sleep, and REM sleep behavior disorder. Depression, anxiety, and obesity also are frequently comorbid. Narcoleptic patients have a reduced quality of life, as the diagnosis affects many aspects of their day-to-day functioning, including work/school performance, social relationships and mental health. The onset of narcolepsy occurs most often between ten and 25 years of age but can occur as early as 5 years or after 40 years of age. The observation of onset during late adulthood may be confounded by delays in diagnosis.1
Pathophysiology of Narcolepsy
Wakefulness is promoted by multiple interconnected brain circuits that control ascending arousal systems. These originate from multiple nuclei that coordinate the release of wake-promoting neurotransmitters including norepinephrine, serotonin, dopamine, histamine and acetylcholine. Lateral hypothalamic neurons containing hypocretin-1 and −2, also known as orexin A and B, sustain wakefulness by activating wake-promoting neurons in other hypothalamic regions, including the tuberomammillary nucleus, and project both rostrally to the cortex, basal forebrain and thalamus and caudally to brainstem monoaminergic nuclei, most prominently the locus coeruleus.9 Hypocretins also stimulate brain areas that inhibit REM sleep. There are only 10,000–20,000 neurons that produce hypocretin, and the selective loss of these neurons due to a presumed autoimmune etiology is implicated as the main cause of EDS and cataplexy in narcolepsy type 1.10,11 Two receptors, hcrtr1 and hcrtr2, mediate the effects of hypocretin in mammals.12 The absence of hcrtr2 receptors in mice results in cataplexy and disruption during wake compared to wild-type.13,14 Dogs that lack hcrtr2 receptors also have the canine form of narcolepsy with cataplexy and have decreased histamine and increased dopamine concentrations in the cortex and thalamus.15
The hypocretin system acts in conjunction with histamine, which also has a pivotal role in the wake-promoting pathway in the brain by regulating the light/dark circadian cycle. It increases during wakefulness and returns to lower levels during sleep.16 Histamine originates from the tuberomammillary nucleus in the posterior hypothalamus and projects to multiple brain regions from the brainstem to the cortex. There are four different histamine receptor subtypes (H1-H4). The wakefulness activity of histamine is mediated by H1 receptors (H1R), which is targeted by classical antihistamines resulting in a sedating effect. The presynaptic H3 receptor (H3R) has a unique role as an autoreceptor due to its inhibitory effect on histamine release and formation.17 While concentrated in the central nervous system (CNS), the H3R can also be found in the pulmonary, gastrointestinal and cardiovascular systems.18 It is also present on axon terminals of non-histaminergic neurons (heteroreceptors) and has an inhibitory effect on the release of other neurotransmitters, particularly norepinephrine, γ-aminobutyric acid (GABA), dopamine, serotonin, acetylcholine and glutamate. H3Rs remain constitutively active resulting in a continued inhibitory effect even in the absence of histamine.19
Both the hypocretin and histaminergic system play coinciding roles in the control of wakefulness.20 The hypocretin system innervates histamine neurons, as proven in the rodent and zebrafish model.21–23 Histaminergic neurons receive hypocretinergic input through hcrtr2 receptors.24,25 Hypocretin-1 and hypocretin-2 depolarize the histaminergic tuberomammillary neurons and increase their firing rate through action on postsynaptic receptors. Immunocytochemical studies show that histamine and hypocretin neurons are located very close to each other.21 Hypocretin neurons are also heavily innervated by histaminergic neurons. Histamine also has an essential role in the development of the hypocretin system in zebrafish larvae, which is mediated through H1R.23 In knockout mice without H1R, hypocretin concentration in the CSF was decreased compared to control.26 In narcoleptic patients with reduced hypocretin neurons, histamine concentration in the CSF was also lower than healthy controls.27–29
Available Narcolepsy Medications
There are several nonpharmacologic interventions that can help manage the symptoms of narcolepsy. These include scheduled napping, good sleep hygiene, and avoidance of drugs that can worsen daytime sleepiness.30 Most patients, however, require medications to reduce sleepiness and cataplexy. The wake-promoting agents modafinil and its R-enantiomer armodafinil are first-line medications for the treatment of EDS in narcolepsy. Their exact mechanism of action in promoting wakefulness is not fully understood but appears to be mediated by increased dopaminergic signaling by blocking dopamine reuptake.31 Stimulants, including amphetamines and methylphenidate, are second-line agents due to abuse potential and sympathomimetic side effects. Methylphenidate also inhibits dopamine and norepinephrine reuptake in the CNS while amphetamines increase both the release of dopamine and norepinephrine in the CNS and block their reuptake. Solriamfetol, a novel dopamine and norepinephrine reuptake inhibitor, was recently approved by the United States Food and Drug Administration (FDA) as a first-line treatment for adult patients with EDS in the setting of narcolepsy.32 The only drug approved by the FDA for the treatment of cataplexy is sodium oxybate whose mechanism is poorly understood but seems to be related to stimulation of GABAB receptors. It also improves EDS and can be considered a first-line therapy when cataplexy is coexistent and requires therapy. Off-label medications used for cataplexy include tricyclic antidepressants (TCAs), selective serotonin reuptake inhibitors, and serotonin and norepinephrine reuptake inhibitors.33 Many of the available treatments for narcolepsy either only partially treat its symptoms (ie wake-promoting agents without effect on cataplexy) or require complex dosing schedules and self-discipline (sodium oxybate). There is a need for new therapeutics that have limited side effects, abuse potential and efficacy on the predominant symptoms narcolepsy.34 Pitolisant (brand name Wakix®) is approved to treat narcolepsy without cataplexy in the United States and narcolepsy with cataplexy in Europe. It is a first-in-class agent to uniquely utilize the role of histamine in regulating wakefulness. This review aims to discuss the safety, efficacy, and tolerability of pitolisant in the management of narcolepsy.
Pitolisant
Mechanism of Action
The blockage of H3R has become a target in the management of disorders of hypersomnia, including narcolepsy. The H3R’s participation in the tonic control of histamine release requires prospective antagonists to have potent intrinsic activity as inverse agonists in order to fully reverse its highly constitutive activity.17 Pitolisant, previously known as BF2.649 and tiprolisant, is the first non-imidazole-based H3R antagonist/inverse agonist to progress into clinical development.
Pitolisant is an N-piperidyl derivative that acts as a high-affinity competitive antagonist and an inverse agonist with an EC50 of 1.5 nM and an inhibitor constant, Ki, of 1 nM, consistent with high potency. It blocks the auto-inhibiting activity of histamine and H3R agonists on endogenous histamine release (See Figure 1). It also increases histamine release above the basal level. At a low concentration of 100 nm, it has no significant interaction with almost a hundred other human receptors and channels.35 It also increases acetylcholine release in the prefrontal cortex and hippocampus as proven in rats, enhancing arousal. Pitolisant preferentially increases dopamine in the prefrontal cortex but not in the striatal complex that comprises the nucleus accumbens.17 Pitolisant’s selectivity of dopamine release was confirmed in rat models compared to modafinil, which increased dopamine release in the nucleus accumbens. This likely explains the lack of psychomotor activity and drug-abuse liability of pitolisant.36 Pitolisant is the first FDA-approved drug to treat hypersomnolence in narcolepsy without being scheduled as a controlled substance as studies in humans demonstrated that it was found to have an abuse profile similar to placebo and significantly lower than that of a phentermine, a mild stimulant.37
 |
Figure 1 Chemical Structure of Pitolisant (C17H26ClNO).39 Notes: National Center for Biotechnology Information. PubChem Database. Pitolisant, CID=9948102, https://pubchem.ncbi.nlm.nih.gov/compound/Pitolisant (Accessed April 29, 2020) |
Pharmacokinetics
Pitolisant was initially approved by the European Medicines Agency for narcolepsy at a dose range of 4.5–36 mg/day.38 It was then FDA-approved for the treatment of daytime sleepiness in adults with narcolepsy in August 2019 at a recommended dose range of 17.8–35 mg/day. The FDA-recommended dose titration starts at 8.9 mg/day, increasing to 17.8 mg/day and then 35.6 mg/day at 1-week intervals based on tolerability. It is available in film-coated tablets, with dosage forms of 4.45 mg and 17.8 mg.32,38 Pitolisant has a high affinity for H3R (Ki = 1 nM) compared to other histamine receptors (H1R, H2R, or H4R, Ki >10 µM). In addition, pitolisant binds to the mouse sigma-1 receptor similar to that for the H3R, which could theoretically contribute to its cognitive and mood effects. However, this interaction with the sigma-1 receptor is not entirely understood. Sigma 1-receptor agonists increase dopamine levels in the nucleus accumbens, whereas pitolisant preferentially increases its concentration in the prefrontal cortex. Pitolisant also antagonizes the sigma-2 receptor and may diminish the effects of cocaine.39–41 Pitolisant is readily absorbed and reaches peak plasma concentration in 3 hrs. After a dose of pitolisant 35.6 mg once daily, the steady-state Cmax is 73 ng/mL and the area under the curve (AUC) is 812 ng*hr/mL. Pitolisant has a plasma half-life of 7.5–24.2 hrs and it reaches steady state in 5 to 6 days, and almost always by day 7 (See Table 1).
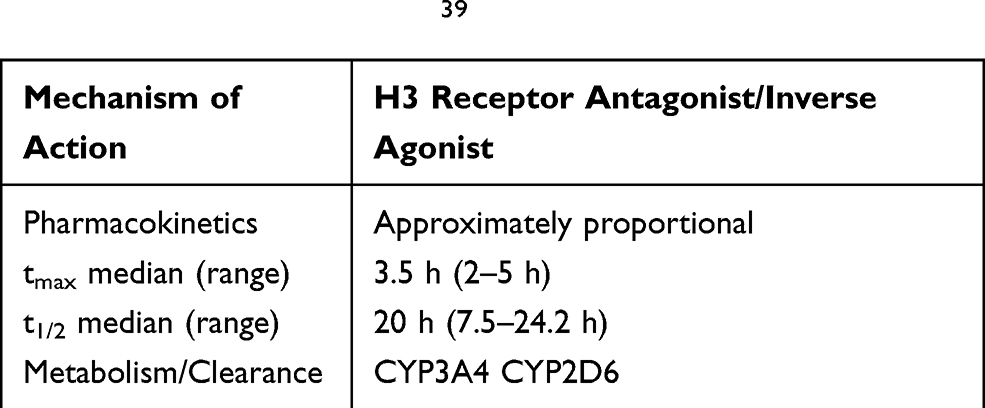 |
Table 1 Pitolisant Overview39 |
Due to its long half-life, it is recommended to take pitolisant early in the morning in order to prevent insomnia. When absorbed, pitolisant is equally distributed between red blood cells and plasma due its high serum protein binding. Metabolism of pitolisant occurs under the action of CYP3A4 and CYP2D6 and is eliminated as inactive metabolites. These metabolites are eliminated mainly through the urine (63%), expired air (25%) and in the feces (<3%).38,42 Pitolisant dose adjustments may be needed in individuals taking medicines that impact CYP3A4 and CYP2D6.
Pitolisant dosing varies in certain populations. The plasma concentration of pitolisant is increased in patients with renal failure (stage 2–3), and the maximum daily dose recommended for these patients is 18 mg. It is not recommended for patients with end-stage renal disease. No dose change is needed for mild hepatic impairment. For patients with moderate hepatic impairment (Child-Pugh B), there was a 2.4 increase in AUC and the half-life doubled. In these patients, treatment should be initiated for 2 weeks before increasing the daily dose to a similar maximum of 18 mg. Pitolisant is contraindicated in patients with severe hepatic impairment.42 Although one small study demonstrated that pitolisant at therapeutic doses does not have any inducer activity on CYP3A4, the drug’s manufacturer suggests that women of reproductive potential on hormonal contraception should still use an alternative nonhormonal contraceptive during and up until 21 days after treatment due to the drug’s long half-life. The effects of in utero exposure to pitolisant are unknown, but it does cross the placenta and teratogenicity was seen in some animal studies. Data collection via a pregnancy registry is ongoing to monitor pregnancy and infant outcomes following in utero exposure to pitolisant. Animal studies have demonstrated that pitolisant passes into breast milk, and its use should, therefore, be avoided in breastfeeding mothers until human studies are available.42 There are limited data on the safety and efficacy of pitolisant in elderly and pediatric populations.
CYP2D6 inhibitors such as paroxetine, fluoxetine, venlafaxine, quinidine, duloxetine, bupropion, terbinafine and cinacalcet may increase the serum concentration of pitolisant and require a 50% dose reduction of pitolisant. CYP3A4 inducers decrease levels of pitolisant and necessitate an increased dose. Antihistamines and TCAs should be avoided as they may decrease the effect of pitolisant.
Cost
Following FDA approval of pitolisant, its manufacturer Harmony Biosciences estimated an annual price tag of about $140,000.43 In a Swedish study, the cost per additional quality-adjusted life-year (QALY) was estimated at SEK 356,337 (~€35,600) and SEK 491,128 (~€49,000) for pitolisant as an adjunctive treatment. Healthcare utilization and QALYs were calculated assuming no treatment effect on survival.44
Efficacy
Lin et al first tested the histamine hypothesis in hypocretin -/- mice by enhancing its release through administering tiprolisant, a precursor of pitolisant.45 The study found tiprolisant enhanced histamine levels and noradrenergic neuron activity. When these mice were given modafinil alone, histamine cortical concentration increased by about 42% with no major difference in noradrenergic activity. In contrast, the co-administration of tiprolisant and modafinil resulted in a significant increase of about 216% cortical histamine concentration, as well as a 121% increase in noradrenergic activity. Clinically, tiprolisant promoted wakefulness and decreased abnormal direct onsets of REM sleep from wakefulness (DREMs), akin to a human sleep-onset REM period. Total REM sleep was decreased by tiprolisant and modafinil, but only tiprolisant considerably decreased the number and duration of DREMs episodes. The group also performed a pilot, prospective, comparative, sequential placebo-controlled, single-blind, multi-center study of a single dose of pitolisant (40 mg) in 22 patients. The patients received placebo followed by tiprolisant for 1 week and were found to have a reduced Epworth Sleepiness Scale (ESS) score from baseline by 1.0 with placebo (p > 0.05) and 5.9 with tiprolisant (p < 0.001). Patient sleep diaries suggested no differences in nocturnal sleep, including duration and wake after sleep onset number, compared to placebo.
This led to two further Phase II studies that demonstrated clinical efficacy in humans.46 Both found significant improvement in ESS score with pitolisant treatment. They also supported a titration scheme for pitolisant by starting at a lower dose and titrating upwards based on normalization of symptomatology and lack of adverse events.
Pivotal Trials
Four major Phase III studies, three of which were randomized, have evaluated the efficacy of pitolisant in patients with narcolepsy (See Table 2).
 |
Table 2 Efficacy of Pitolisant for Narcolepsy: Randomized Control Trials |
Harmony I
Harmony I was the first Phase III, randomized, double-blind placebo-controlled trial investigating pitolisant for narcolepsy.47 It assessed the safety and efficacy of pitolisant against placebo and modafinil. Patients older than 18 years of age meeting the International Classification of Sleep Disorders 2 criteria of narcolepsy with or without cataplexy were recruited from 32 centers in five European countries. Eligible patients had a baseline ESS score of ≥14. Psychostimulants were stopped for 14 or more days prior to initiation, but anti-cataplectic drugs, including sodium oxybate and antidepressants besides TCAs, were continued. Participants were randomly assigned to receive pitolisant, modafinil or placebo (1:1:1). The primary endpoint studied was a difference in change in ESS after an 8-week treatment period between pitolisant and placebo group. Secondary and additional endpoints include a variety of objective and subjective measures of sleepiness and health-related quality of life.
Patients were included if they had at least one dose of the study drug and provided at least one post-baseline value in the intention-to-treat population. Of the 94 patients that were included in the intention-to-treat analysis, 76 (81%) had cataplexy, 42 (45%) had previously taken psychostimulants, and 33 (35%) were on anti-cataplectic drugs. Treatment lasted for 8 weeks and ranged from 10 to 40 mg/day of pitolisant and 100–400 mg of modafinil. For the first 3 weeks, doses were adjusted at the discretion of the investigator followed by a stable dose for the last 5 weeks. At the 8-week result period, the pitolisant group (−5.8 ± 6.2) had a greater reduction in the ESS score compared to the placebo group (−3.4 ± 4.2), but less than the modafinil group (−6.9 ± 6.2). After adjustment for baseline differences, pitolisant was superior to placebo, but not noninferior to modafinil. When specifically looking at the responder rate (defined as an ESS ≤ 10 at treatment conclusion), there was also a significant reduction in ESS score compared to placebo (Figure 2).
 |
Figure 2 Epworth Sleepiness Scale Responder Rate (%)A.47–49 Notes: AESS ≤ 10 or Baseline ESS – final ESS ≥ 3 in I Harmony IBIS. BTreatment Effect Size. *p ≤ 0.05. **p ≤ 0.001.Abbreviations: ESS, Epworth Sleepiness Scale; PIT, pitolisant; PBO, placebo. |
Pitolisant was also superior to placebo in most of the studied secondary efficacy endpoints, including the maintenance of wakefulness test (MWT), sustained attention to response task (SART), and modified clinical global impression of change scale (CGI-C). There was no difference between pitolisant and modafinil in these measures. A post hoc analysis demonstrated pitolisant to be superior to placebo in reduction of cataplexy rate from baseline and noninferior to modafinil as assessed through sleep diaries but no difference among treatment arms when cataplexy was assessed by the CGI-C.
In summary, Harmony I demonstrated that pitolisant reduced EDS as assessed by the ESS compared to placebo, but was not noninferior to treatment with modafinil.
Harmony IBIS
Harmony Ibis followed Harmony I with a similar study design.46 One hundred and sixty-three narcoleptic patients with ESS ≥ 14 with and without cataplexy were randomized to pitolisant, modafinil and placebo (2:2:1) over an 8-week period. Pitolisant doses were lower compared to Harmony I at 5–20 mg/day and modafinil doses ranged from 100 to 400 mg/day. The mean ESS score reductions were −3.6 ± 5.6 in the placebo group, −4.6 ± 4.6 in the pitolisant group, and −7.8 ± 5.9 in the modafinil group. In contrast to Harmony I, pitolisant was not superior to placebo (difference −1.94, 95% CI: −4.005 to −0.07; p = 0.065) and was again not noninferior to modafinil (difference −2.75, 95% CI: −4.48 to −1.02, <3 points) for the primary outcome of improving mean ESS score. Patients receiving pitolisant did have a higher ESS responder rate score compared to placebo (OR 9.24 [95% CI: 3.82 to 22.35]; p = 0.001) and a similar rate to modafinil (OR 1.06 [0.44 to 2.54]; p = 0.894) (See Figure 2). In post hoc sensitivity analysis, a superiority test demonstrated modafinil as superior to placebo in final ESS. MWT scores were significantly increased in the pitolisant group (Δ = +1.14 min) with a decrease in the placebo group (Δ = −1.39 min) during the final visit. Other secondary endpoints including SART, CGI-C, subjective EDS symptoms confirmed previous positive efficacy data seen in pitolisant in comparison to placebo.
Unlike Harmony I, pitolisant was not demonstrated to reduce cataplexy rate in comparison to placebo. In both studies, pitolisant, modafinil and placebo recipients did not differ significantly with respect to the quality of life from baseline.
Harmony CTP
Harmony CTP was a randomized, double-blind, placebo-controlled trial focusing on the safety and efficacy of pitolisant on cataplexy events in patients with narcolepsy with cataplexy.48 Patients with a history of at least three cataplexy episodes per week and EDS (ESS ≥ 12) were recruited from 16 sleep centers in nine countries and randomly assigned to receive either pitolisant or placebo once per day. Treatment duration was 7 weeks with the first 3 weeks used for flexible dosing based on tolerance and efficacy by clinical assessment (range 5–20 mg/day) followed by 4 weeks of stable dosing (5–40 mg/day). The primary endpoint was the change in an average number of cataplexy attacks per week (ie weekly cataplexy rate (WCR)) from baseline (WCRbaseline) to the WCR during 4 weeks of stable treatment (WCRfinal).
A total of 54 patients were randomized into the pitolisant group and 51 to the placebo group in the intention-to-treat analysis. Pitolisant reduced the WCR compared to baseline by 75% (WCRfinal = 2.27; WCRbaseline = 9.15; WCRfinal/baseline = 0.25), while in the placebo group, the reduction was only 38% (WCRfinal = 4.52; WCRbaseline = 7.31; WCRfinal/baseline = 0.62). The rate ratio was 0.512 and statistically significant in favor of pitolisant (95% CI 0.43–0.6; p < 0.0001). Pitolisant was also associated with significant improvement in comparison to placebo in secondary outcomes including ESS and MWT.
Harmony III
Harmony III, a phase III, pragmatic, prospective, open-label study was an uncontrolled trial designed to assess the long-term safety of pitolisant in the treatment of EDS (ESS ≥ 12) in narcolepsy patients with or without cataplexy regardless of previous treatment.49 Of the 102 patients who received pitolisant, 29 were treatment naïve. Concomitant stimulants, H1 antagonists, and anti-cataplectic agents, except for TCAs, were allowed. A total of 68 patients (51 with cataplexy) completed the 12 months of treatment and had a mean decrease in ESS score of 4.6±0.6. Two-thirds of patients were considered responders, defined as a final ESS ≤ 10 or an ESS decrease ≥3 points. The 1-year response rate (final ESS score ≤10 and/or decrease ≥3) was 64.7% (44/68), and ESS score normalized (≤10) in 36.8% (25/68). The largest improvement was seen in patients taking pitolisant monotherapy de novo (−6.5 ± 1.3), although mean ESS score was higher in these patients at baseline. In patients with generalized and partial cataplexy, cataplexy rates decreased by 88% and 71%, respectively (p = 0.055). Frequency of hallucinations, sleep paralysis and sleep attacks were reduced by 54%, 63%, and 27%, respectively.
The limitations of Harmony III, including its open-label design, lack of reference therapy, concomitant presence of drug-naïve and already-treated patients, and lack of objective measures of EDS do not allow for impartial conclusions of its efficacy. Nevertheless, it was the first pragmatic trial looking at the long-term effects of pitolisant in a realistic population and in conjunction with other therapies. It supports pitolisant as a relatively well-tolerated medication for narcoleptics with or without cataplexy.
Safety and Tolerability
Adverse Reactions
The randomized, placebo-controlled Harmony trials, a US-based pitolisant expanded access clinical evaluation (PEACE) program, and supportive data from clinical trials studying the efficacy of pitolisant in other hypersomnia-related diagnoses have informed the safety profile of pitolisant (See Table 3).50 Placebo-controlled trials best identify adverse reactions directly attributable to treatment therapy. Adverse reactions that occurred at least twice the rate of placebo and were seen in ≥5% of patients include insomnia (6%), nausea (6%), and anxiety (5%). Other adverse reactions common to both pitolisant and placebo included headache (18% in pitolisant vs 15% in placebo), upper respiratory tract infection (5% vs 3%), musculoskeletal pain (5% vs 3%), and anxiety (5% vs 1%).42 The Harmony III study suggested that the frequency of adverse events decreases during the course of treatment: 54% reported adverse events over the first 3 months versus 12.5% during the last 3 months. 13.1% of adverse events in this study were considered severe but only half considered related to the study drug, and all but one patient had complete resolution of the adverse event. Patents who were taking additional anti-narcoleptic agents had a twice greater frequency of adverse events compared to patients who took pitolisant alone (53.7% versus 29.2%, p = 0.012). A recent abstract integrating the safety and tolerability data from four randomized, placebo-controlled trials corroborated these findings.51 Adverse events for pitolisant and placebo occurred in 49.4% and 41.2% patients, respectively. Only two in the pitolisant group were considered serious. No clinically significant effects were seen in vital signs, laboratory findings, or ECG parameters. Pitolisant was determined to be generally safe and well tolerated. The PEACE program further substantiated tolerability and safety. Despite most patients (91.1%) taking maximal dose and many (60.1%) taking additional narcolepsy medications, only 8.2% patients discontinued therapy – 5.3% from adverse events and 1.1% for lack of efficacy. The most reported adverse events included headache (8.1%), anxiety (3.8%) and nausea (3.4%).52 The incidence of adverse effects does appear to be related to dose. A large study involving over 1800 subjects taking pitolisant for a variety of etiologies (including off-label conditions) found that the incidence of adverse events was dose-dependent (11.1% at 4.5 mg/d; 20.3% at 9 mg/d; 32.5% at 18 mg/d; 36.4% at 36 mg/d). Again, the most common adverse effects were neuropsychiatric, including insomnia (8.4%), headache (7.7%), anxiety (2.1%), irritability (1.8%), dizziness (1.4%), depression (1.3%), tremor (1.2%), sleep disorders (1.1%) and vertigo (1.0%). Gastrointestinal effects including nausea (4.8%), vomiting (1%) and diarrhea (1%) were also observed.53
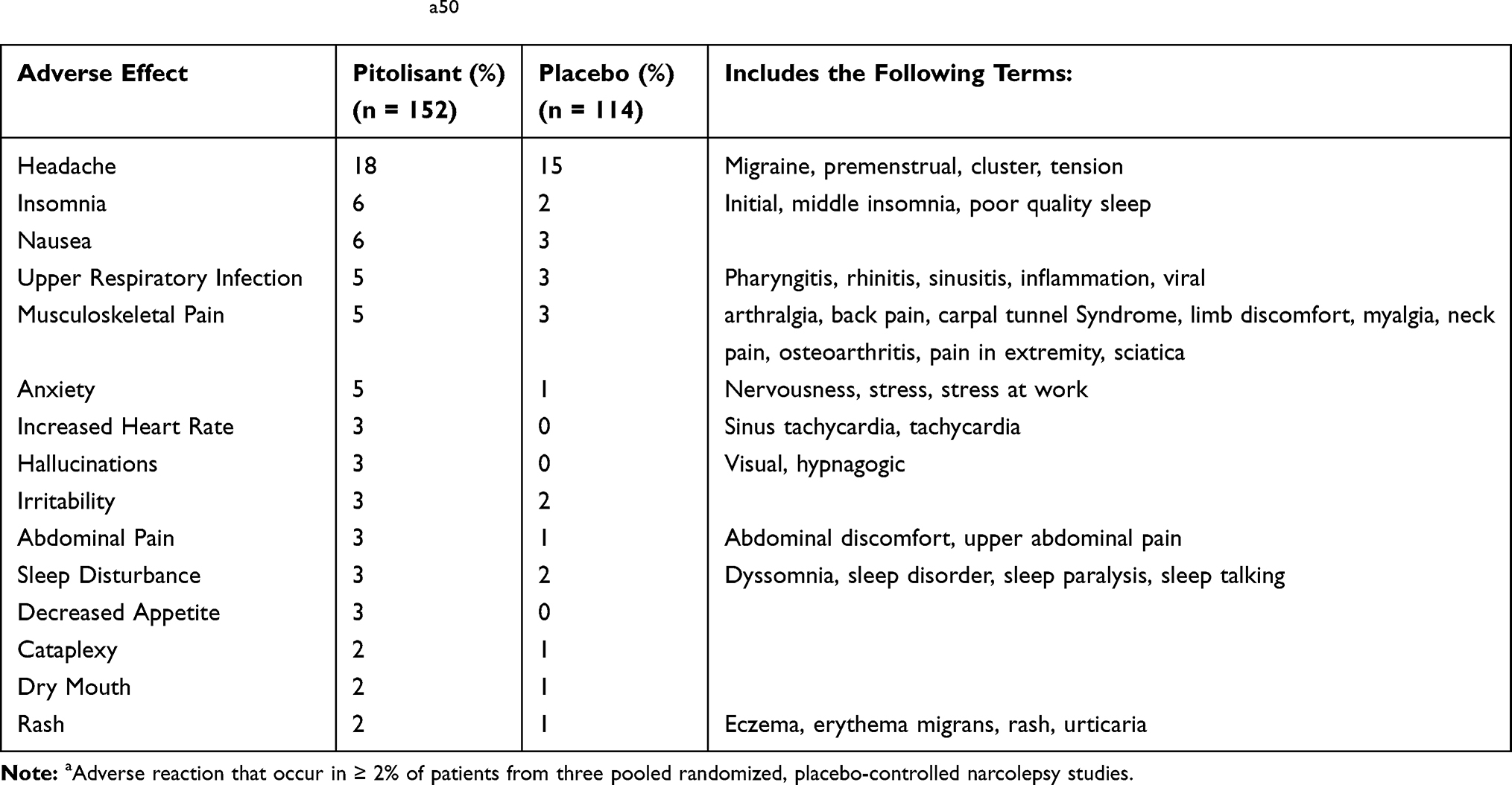 |
Table 3 Pitolisant Adverse Reactionsa50 |
QTc Prolongation
The package insert for pitolisant states that it prolongs the QT interval, and it recommends that patients with known QT prolongation, taking medications that prolong the QT, or those otherwise at risk for arrhythmias avoid its use. Randomized studies that look at pitolisant prescribed at recommended doses (40 mg), however, have not demonstrated a significant increase in the QTc in comparison to placebo.46 In contrast, various supratherapeutic doses (120–240 mg) increased the QTc by about 10 ms. While clinical trials using therapeutic doses did not identify any cardiac safety issues, caution is advised in at-risk patients.46
Nighttime Sleep
The effect of pitolisant on nighttime sleep with narcolepsy was recently studied.54 Data collected included the subjective Pittsburgh Sleep Quality Index (PSQI) and objective overnight polysomnography (PSG). Post-treatment and baseline PSG parameters were similar including total recorded sleep time (354.1 vs 365.9 min), sleep efficiency (79.6 vs 78.9%) and arousal index (17.2 vs 18.1 arousals/hour). No change was observed on the overall PSQI, although the component of sleep efficiency was negatively affected.
Abuse Potential
Animal studies of pitolisant demonstrate a low potential of abuse.36,55 This was validated in a human study in a randomized, double-blind, active- and placebo-controlled four-period crossover study.37 Nondependent recreational stimulant users able to distinguish a known drug of abuse, phentermine, from placebo in a drug discrimination test were recruited and randomized to receive pitolisant at therapeutic (35.6 mg) and supratherapeutic doses (213.6 mg), phentermine 60 mg, and placebo. Using the primary endpoint of maximum effect (Emax) on the 100-point Drug Liking visual analog scale, Emax was similar between both pitolisant doses and placebo and significantly greater for phentermine, supporting a minimal abuse potential for pitolisant.
Pitolisant and Other Narcolepsy Medications
Comparative studies investigating different medications and optimal drug doses for patients with narcolepsy types 1 and 2 are sparse. A meta-analysis looked at 14 randomized controlled trials in an attempt to compare the efficacy between multiple treatments for narcolepsy using a random model that assumed heterogeneity between studies and corrected for multi-arm studies.56 Medications included sodium oxybate (6 and 9 g/d), modafinil (between 200 and 400 mg/d), and pitolisant (up to 20 and up to 40 mg/d). Although significant heterogeneity (>50%) was found between 12/14 studies for almost all endpoints, between-design consistency was present. The meta-data analysis determined that pitolisant up to 40 mg/d, sodium oxybate 9 g/d, and modafinil 200–400mg/d had similar efficacy for EDS as determined by the ESS and MWT. For cataplexy, pitolisant 40 mg/d and sodium oxybate 9 g/d had similar efficacy. Although the effects between medications on average were comparable, it remains to be determined whether patients who do not respond well to any given medicine will respond to medicines in another class or whether a medicine’s effects may be potentiated by combination with a medicine from another class.
Summary
Narcolepsy is a debilitating sleep disorder marked by EDS and, in many patients, cataplexy. The pharmacological treatment options are slim but expanding. Modafinil and armodafinil have historically been considered first-line options for EDS. Sodium oxybate is the only FDA-approved medication to treat cataplexy secondary to narcolepsy and is effective in reducing sleep fragmentation.57 Pitolisant is a new addition to the pharmacological armamentarium to treat EDS in narcolepsy, with several trials suggesting efficacy in cataplexy as well. Pitolisant is a first-in-class wake-promoting medication that works as an antagonist/inverse agonist of the H3R and is the only narcolepsy drug not scheduled as a controlled substance. It is generally well tolerated, with headache, insomnia, nausea and anxiety being the most common adverse reactions. Large, longitudinal studies of pitolisant’s effect on both EDS and cataplexy in narcolepsy as well as comparative and medication combination studies are needed to help guide the overall rationale for physicians in narcolepsy management. Pitolisant certainly will develop a niche in the treatment algorithm in patients with narcolepsy, who often remain with symptoms despite current recommended therapy.
Disclosure
Dr. Jay T. Guevarra and Dr. Robert Hiensch have no disclosures. Dr. Andrew W. Varga has previously served as a consultant for Merck and Eisai Pharmaceuticals and reports grants, personal fees, and non-financial support from Merck, and personal fees from Eisai, outside the submitted work. He is supported by: NIH/NIA R01AG056682, R01AG066870, R21AG059179, the Alzheimer’s Association, the McClung Foundation, and the Merck Investigators Studies Program. Dr. David M. Rapoport receives patent royalties from Fisher & Paykel Healthcare Limited and Sefam Medical, Ltd for CPAP modifications; consulting fees and grant support from Fisher & Paykel Healthcare Limited; and consulting fees from BioMarin Pharmaceutical Inc, Morphy, Inc, and Jazz Pharmaceuticals plc. The authors report no other potential conflicts of interest for this work.
References
1. Scammell TE. Narcolepsy. N Engl J Med. 2015;373(27):2654–2662. doi:10.1056/NEJMra1500587
2. Thorpy MJ. Narcolepsy, a Clinical Guide.
3. Darien I. International Classification of Sleep Disorders.
4. Longstreth WT, Koepsell TD, Ton TG, Hendrickson AF, van Belle G. The epidemiology of narcolepsy. Sleep. 2007;30(1):13–26. doi:10.1093/sleep/30.1.13
5. Hale L, Guan S, Emanuele E. Narcolepsy: A Clinical Guide.
6. Scheer D, Schwartz SW, Parr M, Zgibor J, Sanchez-Anguiano A, Rajaram L. Prevalence and incidence of narcolepsy in a US health care claims database, 2008-2010. Sleep. 2019;42.
7. Silber MH, Krahn LE, Olson EJ, Pankratz VS. The epidemiology of narcolepsy in Olmsted County, Minnesota: a population-based study. Sleep. 2002;25(2):197–202. doi:10.1093/sleep/25.2.197
8. Guilleminault C, Billiard M, Montplaisir J, Dement WC. Altered states of consciousness in disorders of daytime sleepiness. J Neurol Sci. 1975;26(3):377–393. doi:10.1016/0022-510X(75)90209-9
9. Scammell TE, Arrigoni E, Lipton JO. Neural circuitry of wakefulness and sleep. Neuron. 2017;93(4):747–765. doi:10.1016/j.neuron.2017.01.014
10. Mahoney CE, Cogswell A, Koralnik IJ, Scammell TE. The neurobiological basis of narcolepsy. Nat Rev Neurosci. 2019;20(2):83–93. doi:10.1038/s41583-018-0097-x
11. Nishino S, Ripley B, Overeem S, Lammers GJ, Mignot E. Hypocretin (orexin) deficiency in human narcolepsy. Lancet. 2000;355(9197):39–40. doi:10.1016/S0140-6736(99)05582-8
12. Sakurai T. The neural circuit of orexin (hypocretin): maintaining sleep and wakefulness. Nat Rev Neurosci. 2007;8(3):171–181. doi:10.1038/nrn2092
13. Willie JT, Chemelli RM, Sinton CM, et al. Distinct narcolepsy syndromes in Orexin receptor-2 and Orexin null mice: molecular genetic dissection of Non-REM and REM sleep regulatory processes. Neuron. 2003;38(5):715–730. doi:10.1016/S0896-6273(03)00330-1
14. Willie JT, Renthal W, Chemelli RM, et al. Modafinil more effectively induces wakefulness in orexin-null mice than in wild-type littermates. Neuroscience. 2005;130(4):983–995. doi:10.1016/j.neuroscience.2004.10.005
15. Lin L, Faraco J, Li R, et al. The sleep disorder canine narcolepsy is caused by a mutation in the hypocretin (orexin) receptor 2 gene. Cell. 1999;98(3):365–376. doi:10.1016/S0092-8674(00)81965-0
16. Haas HL, Sergeeva OA, Selbach O. Histamine in the nervous system. Physiol Rev. 2008;88:1183–1241.
17. Schwartz JC. The histamine H3 receptor: from discovery to clinical trials with pitolisant. Br J Pharmacol. 2011;163(4):713–721. doi:10.1111/j.1476-5381.2011.01286.x
18. Ghamari N, Zarei O, Arias-Montaño JA, et al. Histamine H. Pharmacol Ther. 2019;200:69–84. doi:10.1016/j.pharmthera.2019.04.007
19. Schlicker E, Kathmann M. Role of the Histamine H. Handb Exp Pharmacol. 2017;241:277–299.
20. Sundvik M, Panula P. Interactions of the orexin/hypocretin neurones and the histaminergic system. Acta Physiol (Oxf). 2015;213(2):321–333. doi:10.1111/apha.12432
21. Eriksson KS, Sergeeva O, Brown RE, Haas HL. Orexin/hypocretin excites the histaminergic neurons of the tuberomammillary nucleus. J Neurosci. 2001;21(23):9273–9279. doi:10.1523/JNEUROSCI.21-23-09273.2001
22. Kaslin J, Nystedt JM, Ostergård M, Peitsaro N, Panula P. The orexin/hypocretin system in zebrafish is connected to the aminergic and cholinergic systems. J Neurosci. 2004;24(11):2678–2689. doi:10.1523/JNEUROSCI.4908-03.2004
23. Sundvik M, Kudo H, Toivonen P, Rozov S, Chen YC, Panula P. The histaminergic system regulates wakefulness and orexin/hypocretin neuron development via histamine receptor H1 in zebrafish. FASEB J. 2011;25(12):4338–4347. doi:10.1096/fj.11-188268
24. Marcus JN, Aschkenasi CJ, Lee CE, et al. Differential expression of orexin receptors 1 and 2 in the rat brain. J Comp Neurol. 2001;435(1):6–25. doi:10.1002/cne.1190
25. Yamanaka A, Tsujino N, Funahashi H, et al. Orexins activate histaminergic neurons via the orexin 2 receptor. Biochem Biophys Res Commun. 2002;290(4):1237–1245. doi:10.1006/bbrc.2001.6318
26. Lin L, Wisor J, Shiba T, et al. Measurement of hypocretin/orexin content in the mouse brain using an enzyme immunoassay: the effect of circadian time, age and genetic background. Peptides. 2002;23(12):2203–2211. doi:10.1016/S0196-9781(02)00251-6
27. Nishino S, Sakurai E, Nevsimalova S, et al. Decreased CSF histamine in narcolepsy with and without low CSF hypocretin-1 in comparison to healthy controls. Sleep. 2009;32(2):175–180. doi:10.1093/sleep/32.2.175
28. Bassetti CL, Baumann CR, Dauvilliers Y, Croyal M, Robert P, Schwartz JC. Cerebrospinal fluid histamine levels are decreased in patients with narcolepsy and excessive daytime sleepiness of other origin. J Sleep Res. 2010;19(4):620–623. doi:10.1111/j.1365-2869.2010.00819.x
29. Kanbayashi T, Kodama T, Kondo H, et al. CSF histamine contents in narcolepsy, idiopathic hypersomnia and obstructive sleep apnea syndrome. Sleep. 2009;32(2):181–187. doi:10.1093/sleep/32.2.181
30. Neikrug AB, Ong JC. Narcolepsy: A Clinical Guide.
31. Volkow ND, Fowler JS, Logan J, et al. Effects of modafinil on dopamine and dopamine transporters in the male human brain: clinical implications. JAMA. 2009;301(11):1148–1154. doi:10.1001/jama.2009.351
32. Thorpy MJ. Recently approved and upcoming treatments for narcolepsy. CNS Drugs. 2020;34(1):9–27. doi:10.1007/s40263-019-00689-1
33. Barateau L, Lopez R, Dauvilliers Y. Management of narcolepsy. Curr Treat Options Neurol. 2016;18(10):43. doi:10.1007/s11940-016-0429-y
34. de Biase S, Gigli GL, Valente M. Important decisions in choosing the pharmacotherapy for narcoleptics. Expert Opin Pharmacother. 2019;20(5):483–486. doi:10.1080/14656566.2018.1561861
35. Syed YY. Pitolisant: first global approval. Drugs. 2016;76(13):1313–1318. doi:10.1007/s40265-016-0620-1
36. Uguen M, Perrin D, Belliard S, et al. Preclinical evaluation of the abuse potential of Pitolisant, a histamine H3 receptor inverse agonist/antagonist compared with Modafinil. Br J Pharmacol. 2013;169(3):632–644. doi:10.1111/bph.12149
37. Setnik B, McDonnell M, Mills C, et al.Evaluation of the abuse potential of pitolisant, a selective H3-receptor antagonist/inverse agonist, for the treatment of adult patients with narcolepsy with or without cataplexy. Sleep. 2019.
38. Wakix:Highlights of prescribing information. Plymouth Meeting, PA. 2020
39. Riddy DM, Cook AE, Shackleford DM, et al. Drug-receptor kinetics and sigma-1 receptor affinity differentiate clinically evaluated histamine H(3) receptor antagonists. Neuropharmacology. 2019;144:244–255. doi:10.1016/j.neuropharm.2018.10.028
40. EMA. EMA. Wakix Assessment Report. 2015
41. Lamb YN. Pitolisant: a review in narcolepsy with or without cataplexy. CNS Drugs. 2020;34(2):207–218. doi:10.1007/s40263-020-00703-x
42. Wakix. Summary of product characteristics. Bioprojet Pharma. 2016
43. Emerson E. Newly approved narcolepsy product has a price tag exceeding 100K annually. Crumdale Partners. 2020.
44. Bolin K, Niska P, Pirhonen L, Wasling P, Landtblom AM. The cost utility of pitolisant as narcolepsy treatment. Acta Neurol Scand. 2019.
45. Lin JS, Dauvilliers Y, Arnulf I, et al. An inverse agonist of the histamine H(3) receptor improves wakefulness in narcolepsy: studies in orexin-/- mice and patients. Neurobiol Dis. 2008;30(1):74–83. doi:10.1016/j.nbd.2007.12.003
46. EMA. Wakix assessment. 2020. Available from: https://www.ema.europ.
47. Dauvilliers Y, Bassetti C, Lammers GJ, et al. Pitolisant versus placebo or modafinil in patients with narcolepsy: a double-blind, randomised trial. Lancet Neurol. 2013;12(11):1068–1075. doi:10.1016/S1474-4422(13)70225-4
48. Szakacs Z, Dauvilliers Y, Mikhaylov V, et al. Safety and efficacy of pitolisant on cataplexy in patients with narcolepsy: a randomised, double-blind, placebo-controlled trial. Lancet Neurol. 2017;16(3):200–207. doi:10.1016/S1474-4422(16)30333-7
49. Dauvilliers Y, Arnulf I, Szakacs Z, et al. Long-term use of pitolisant to treat patients with narcolepsy: harmony III Study. Sleep. 2019:42.
50. Solanges M. Pitolisant: Clinical Review. Rev of Safety. Data provided by the U.S. Food and Drug Administration. 2019;332. Available from: https://www.accessdata.fda.gov. Accessed August 18, 2020
51. Scart-Grès C, Momah C, Roy M, Maski K, Piris S, RK B. Safety and tolerability of pitolisant in the treatment of adults. Sleep. 2019;42(Supplement_1):A244–5. doi:10.1093/sleep/zsz067.612
52. Bauer E, Davis C, Patroneva A, Dayno J, Thorpy M. The safety and tolerability of pitolisant in the treatment of excessive daytime sleepiness and cataplexy in adult patients with narcolepsy: an open-label, expanded access program in the United States [abstract no. 0611]. sleep. 2019;42(suppl1):A243. doi:10.1093/sleep/zsz067.609
53. Kollb-Sielecka M, Demolis P, Emmerich J, Markey G, Salmonson T, Haas M. The European Medicines Agency review of pitolisant for treatment of narcolepsy: summary of the scientific assessment by the committee for medicinal products for human use. Sleep Med. 2017;33:125–129. doi:10.1016/j.sleep.2017.01.002
54. Kallweit U, Triller A. Effects of pitolisant on nighttime sleep [abstract no. 0613]. sleep. 2019;42(suppl1):A244. doi:10.1093/sleep/zsz067.611
55. Huyts B, Brabant C, Tirelli E. Pitolisant and intravenous cocaine self-administration in mice. Eur J Pharmacol. 2019;851:63–68. doi:10.1016/j.ejphar.2019.02.019
56. Lehert P, Falissard B. Multiple treatment comparison in narcolepsy: a network meta-analysis. Sleep. 2018;41.
57. Roth T, Dauvilliers Y, Guinta D, Alvarez-Horine S, Dynin E, Black J. Effect of sodium oxybate on disrupted nighttime sleep in patients with narcolepsy. J Sleep Res. 2017;26(4):407–414. doi:10.1111/jsr.12468
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.