Back to Journals » Journal of Healthcare Leadership » Volume 18
Pitfalls and Mitigation Strategies for Dyad Leadership Practice and Implementation in Healthcare
Received 15 October 2025
Accepted for publication 25 December 2025
Published 7 January 2026 Volume 2026:18 570839
DOI https://doi.org/10.2147/JHL.S570839
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Russell Taichman
Anurag Saxena,1 Grant Yao2
1Department of Pathology and Laboratory Medicine, College of Medicine, University of Saskatchewan, Saskatoon, SK, Canada; 2College of Medicine, University of Saskatchewan, Saskatoon, SK, Canada
Correspondence: Anurag Saxena, University of Saskatchewan, Rm 3870, Department of Pathology and Laboratory Medicine, Royal University Hospital, 103 Hospital Drive, Saskatoon, SK, S7N 0W8, Canada, Tel +1 306-655-2157, Fax +1 306-655-2223, Email [email protected]
Abstract: Dyad leadership (co-leadership between a physician and another clinical, eg, nurse or an administrative leader) is being increasingly adopted in healthcare to leverage diverse competencies required and achieve coherence between administrative and clinical governance. The challenges and success strategies of this model have been described. However, the organizations and leaders struggle with its implementation and actual practice. The purpose of this paper is to describe the pitfalls and suggest mitigation strategies for the practice and implementation of dyad leadership model. The insights were derived through inductive thematic analysis and constant comparison of the “text” that included a narrative review of extant peer-reviewed (PUBMED, MEDLINE, CINAHL, PsychInfo, Scopus) and grey literature on dyad leadership (2000– 2025), interdisciplinary perspectives on relevant theories, findings through research in a health region (2010– 2011), and reflections on experiences in a dyad leadership role. The pitfalls at the individual and dyad partner level include a lack of “shared” leadership literacy, suboptimal relational dynamics (spurious harmony, not switching switch leader-follower roles, and not allowing time for the relationship to mature), and ineffective collaboration (unresolved role ambiguity, lack of information sharing, ineffective decision-making, and counterproductive actions). At the organizational level the pitfalls are lack of organizational preparation and non-strategic implementation, lack of support for and accountability of dyad leaders, and not selecting the right people for dyad leadership roles. Mitigation involves becoming adept at the required behavioral complexity relying on a deeper understanding of shared leadership, nurturing a mutually valued relationship aimed at collective identity, and leveraging collective efficacy, inter-dependencies, complementary strengths, and positive effects of psychological ownership and territoriality. Strategic organizational implementation includes criteria-based selection, appropriate support and clear accountability mechanisms, and monitoring leaders’ behaviors and effectiveness of the model. Navigating these pitfalls would help agency and well-being, fulfilled relationships and effective collaborative work to utilize the full potential of the dyad leadership model.
Keywords: dyad leadership, pitfalls, health leadership, leadership in healthcare, mitigation strategies, shared leadership
Introduction
Dyad leadership, a sharing of leadership and management functions amongst two individuals, has been variably adopted in healthcare organizations (HCOs). It is based on the assertions that a) the competencies required to lead in a complex adaptive system (CAS) such as healthcare, are too broad to reside in one individual1 and b) there is a coexistence of professional and bureaucratic logics and cultures in HCOs,2 which require coherence through integration of administrative and clinical governance.3 Similarly, in medical education institutions, there are academic and administrative leaders (and managers) who work together on different aspects to achieve organizational outcomes, although the partnerships may not be on equal footing with possible hierarchical relationships and parallel siloed reporting to higher organizational levels; eg, co-leadership at the senior leadership level in the universities.4 Sometimes, working groups for specific projects may adopt a co-leadership model, eg, a faculty and student co-chair to address inequities.5
The dyad model has robust support from various leadership theories including shared leadership,6 distributed leadership,7 connective leadership,8 collaborative leadership,9 and collectivist leadership.10
In HCOs, both the dyad partners could have clinical expertise, eg, a physician and a nurse,11 but more commonly the partnership is between a physician and a leader with an administrative background.12 There is extensive grey literature (books, blogs, webpages, and dissertations) and somewhat limited peer-reviewed literature (empirical studies, reviews, and commentaries) on dyad leadership. The peer-reviewed literature highlights the rationale and structure and design elements including shared and overlapping roles and responsibilities,13,14 suggestions for development and implementation,11 necessity of team- and general-leadership competencies as a foundation for the partnership,15 challenges and success strategies across individual and organizational domains,16,17 and strategies for effective collaboration between the dyad partners.15
There is a paucity of literature on the effectiveness of the dyad model with only occasional reports on the factors linked with successful outcomes.18,19 However, its success can be inferred from its continued use and reliance in some high-performance organizations, eg the Mayo Clinic.20 The promise of the dyad model is reflected in its consideration and increasing adoption in HCOs across the world.21–23
Successful implementation and utilization of dyad leadership requires knowledge of challenges and strategies for success. These span personal/interpersonal (mindsets, competencies, interpersonal relationship including communication, resources including time and support, and collaboration) and organizational (strategy, operation, implementation, culture, support, and evaluation) domains.2,15,16,22 Despite its appeal and literature on success strategies, organizations struggle with implementation and practice of this model.13,15,16 Further, finding a balance in this model is hard24 likely reflecting the dysfunction observed in teams across organizational boundaries25 and balancing institutional logics.2
The exercise of agency and organizational implementation of this model requires consideration of certain pitfalls that need to be mitigated or navigated successfully. Our aim was to identify the pitfalls and put forward mitigation strategies and actions based on insights drawn from multiple sources including a narrative literature review, research identifying dyad leaders’ perceptions, reflections on experiences of being in a dyad leadership role and conversations with organizational leaders, and interdisciplinary literature on theories informing sharing of leadership.
Methods
The literature review strategy, research on perceptions of dyad and senior leaders in a health region, reflections on experiences and conversations with organizational leaders and analysis are described below.
Literature Search Strategy
The literature review, limited to English language peer-reviewed literature spanning 2000–2025, was conducted from June to September 2025; it utilized Medical Subject Headings, keywords and free text related to dyad leadership in healthcare and medical education. The full search strategy is described in Table S1. The databases searched included (number of articles identified are given in brackets): PUBMED (81), CINAHL (22), MEDLINE (7), Google Scholar (22), Web of Science (169), PsychInfo (2), and Scopus (69). Inclusion criteria were studies limited to dyad leadership, English language, and any article type (empirical studies, reviews and commentaries); the exclusion criteria were (no full-length paper available, and duplicates). When identified through the systematic and scoping reviews, articles prior to 2000 were also included. The grey literature search (white papers, webpages, presentations, workshop summaries, books, ProQuest Dissertations and Theses and Google Scholar) identified 156 “texts”. Grey literature was included to leverage information not published in peer-reviewed literature (especially those with null or negative results), enhance comprehensiveness, and tap into current information.26 After reading all abstracts, full-length manuscripts of the articles with descriptions of dyad leadership implementation and practice full-length manuscripts were read. Given the small number of studies in peer-reviewed literature and heterogeneity in study designs, a narrative review was performed, and the quality of evidence was not determined. A total of 195 documents were considered for this review.
Research on Dyad Leaders’ Perceptions
The research on dyad leadership in healthcare (in the then Saskatoon Health Region) included specific questions on the pitfalls and how to navigate these. The health region included 10 hospitals, 29 long-term facilities, 12 primary healthcare sites, 14 public health sites, and small centres in communities and business locations and private residencies to provide hospital-, ambulatory-, mental health-, community health-, long-term care-, and rehabilitation services through approximately 847 physicians, 13000 staff and 8000 volunteers to approximately 300,000 population (urban and rural) spread over 32000 sq km. The other findings from this research, eg, structural aspects and challenges and success strategies have been published,14,16 but the pitfalls have never been published. The perceptions of 32 leaders in dyad leadership roles (15 physician leaders and 17 administrative co-leaders) at three organizational levels (front-line, mid-level and senior-level) and five senior leaders (members of the senior leadership team responsible for implementation of dyad leadership model) were gathered through an open-ended survey and focus groups (leaders in dyad roles) and semi-structured interviews (senior leaders). The question asked was, “what are the pitfalls dyad leaders should be aware of and what can be done about these?” The University of Saskatchewan Behavioral Research Ethics Board (Beh# 09–09, approval from 2009 to 2013) and the Saskatoon Health Region Research Project Ethics Committee (EC#B2009-09) had approved the study. All participants had provided written consent prior to their participation by reviewing and signing the approved consent form.
Reflections on Dyad Leadership
The corresponding author’s reflections on experiences of being in a dyad leadership role for three years and conversations with senior organizational leaders were documented. Further, preparatory work and debriefs for five workshops on various aspects of dyad leadership led to additional journal writing and reflections over the last eight years (2018–2025).
Analysis and Synthesis of Findings
The “text” gathered through the above modalities was analyzed by inductive thematic analysis (familiarization, first and second round coding followed by categorization looking for overlaps and patterns, generating themes by identifying bigger picture or deeper meaning, reviewing themes, naming themes and report writing).27 Including non-traditional data sources (grey literature and reflections on lived experiences), in addition to literature review and empirical research, is likely to have enhanced contextual understanding in the complex systems of healthcare and medical education.28 Extant interdisciplinary literature on relevant theoretical perspectives (eg, shared-, collective-, connective-, distributed- leadership) was simultaneously reviewed. Following initial coding and second-level coding, constant comparison was used iteratively to form broad categories until the categories were separate and non-overlapping. The themes generated after the final round were then named. The conceptual work includes critically examining notions and constructs of shared leadership.
Findings
There are pitfalls at the individual-, dyad partner-, and organizational levels. In addition, the pitfalls inherent in sharing leadership – the so-called dark side of shared leadership – also exist. A brief summary of the findings (pitfalls and suggestions for mitigating and navigating these pitfalls) is shown in Table 1. The source for these (literature review with relevant references cited, research in the health region or reflection – supported by direct quotes) is indicated in the Table.
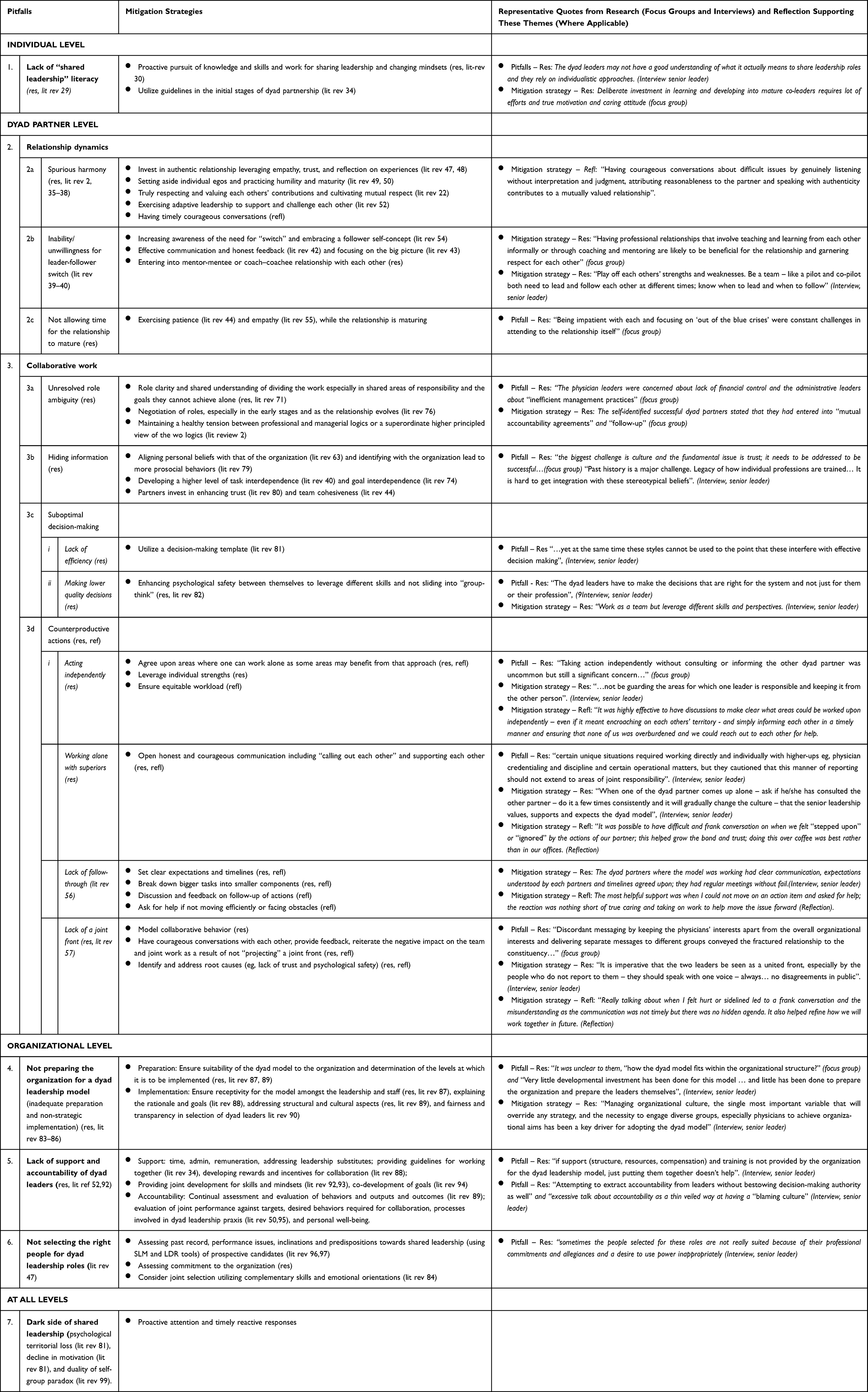 |
Table 1 Pitfalls and Mitigation Strategies Identified Through Literature Review, Research and Reflections on Lived Experiences. Sources are Identified as Follows: Lit Rev x (Literature Review, Reference Number; Res – Research, Refl – Reflection)’ SML: shared leadership mapping, LDR: Leader Developmental Readiness |
Insights and Discussion
The salient features of pitfalls, their manifestations, and the impact (individual and organizational) of not addressing these pitfalls, insights (reflecting the role of underlying factors and considerations relevant to solutions), and explanations of suggestions for mitigating and navigating the pitfall(s) are discussed below. Only representative references are cited.
Individual Level
At the individual level, the pitfall is a lack of “shared leadership” literacy, or a superficial understanding without internalization of its nuances and intricacies. This may manifest in actions consistent with a short-term perspective limited to one dyad partner’s own areas of responsibility and allegiance to their profession.
Indeed, a lack of understanding of shared leadership was found to be a significant concern for the work amongst collaboratives between different organizations.29 The importance of literacy is highlighted by the observation that effective shared leadership rests on the foundation of cognition (mental models), learning (through training, education and development), and consequent behaviors (complexity of social influence on the partner).30 In addition to being capable of general leadership skills – especially ethical underpinnings to serve the collective (demonstrating character, exercising moral courage, treating each other and people with respect and upholding organizational values)31,32 – and team leadership skills,15 dyad leaders must be competent in other domains. Proficiency in broader systems thinking, leading across boundaries, simultaneously upholding multiple (and sometimes oppositional) realities, and higher-level thinking such as strategic, critical, systems and expert thinking is required. The latter are particularly relevant for creating value.33
Suggested solutions: Investing in gaining the knowledge, utilizing personal initiatives and organizational opportunities and engaging in reflective practice are essential to gain a deeper understanding. Since this understanding and its translation into practice takes time, access to guidelines – through one’s organizational resources or general literature – would be helpful, especially in the early stages of dyad partnerships.34
Dyad-Partner Level
There are two aspects that are potentially vulnerable, relationship dynamics and collaborative work.
Relationship Dynamics
A mutually valued relationship is the foundation of an effective dyad leadership partnership with trust and respect at its core. The three pitfalls affecting the relationship quality are spurious harmony, not being able to switch leader-follower roles, and not allowing time needed for the relationship to mature.
Spurious Harmony
While internally shaky, on the surface there may be “spurious harmony” and lukewarm interactions between dyad leaders with an ever-present risk of the relations sliding into an abrasive and overtly confrontational relationship. Examples of some actions (whether done unconsciously or deliberately) that can damage the relationship are, a) ignoring the co-leader (eg, not responding to requests in a timely manner), b) leaving the work largely on the partner’s shoulders, and c) the domineering leader subduing the other partner, eg, a physician leader dominating the nurse partner35 for personal gains and justifying the action in terms of organizational goal achievement.36 This can lead to the partnership metamorphosing into a state of “assimilation” of the weaker partner by the other.2 The other alternative is time being inefficiently spent in power struggles and conflicts and in pushing personal agendas.
The underlying factors are likely to include a lack of respect, poor communication, not having shared core values, and how the dyad partners view each other’s overall competence and the ability to complete the tasks.37 One partner’s disposition towards “power and authority” may result in decreased involvement in the relationship. It is likely that one or both partners, although having been assigned to the formal roles, have not psychologically granted leadership to the other partner and have reluctantly accepted them in the dyad role.38
Leader-Follower Switch
The pitfall is the inability or unwillingness to switch the leader-follower roles within the dyad partnership and insists on a leadership position. Some situations require one of the dyad partners to take the lead and the other one to be in the follower role in the shared areas of responsibility, eg, the administrative partner leading the work on maintaining services within budget. The switch involves both cognitive and behavioral dimensions,39 and it may be difficult to manage across the blurred boundaries.40 Rooted in the notion of “collective intentionality”,41 the cooperation between the partners and leader-follower switch can be enhanced by effective communication42 and a focus on the “big picture”.43
Time for Developing the Relationship
The pitfall is not allowing time to develop a strong relationship, and thinking that the formation of the dyad alone is enough to effectively work together. The dyad is a two-person team and like other teams, goes through stages of forming, storming, norming, and performing. Further, it is a long-term proposition and takes time for the partners to adjust and the relationship to mature. Indeed, prolonged partnerships have been shown to increase the cohesion and the likelihood of knowledge sharing.44
The cumulative effects of these pitfalls on the partners are negative. These include: a) detrimental effect on individual well-being, eg, psychological toll – as people are not able to live with their values, do not feel psychologically safe, and experience increased stress,45 b) negative reinforcing of professional boundaries, with leaders strengthening their world view, ideology, and authority,46 and c) an unconscious or deliberate “tilting away” from joint work. Consequently, the dyad leaders are unable to give their best to the organization and may resort to exertion of power.
Suggested solutions: To develop and nurture a mutually valued relationship, leaders must recognize the time and deliberate investment required for the relationship’s evolution. Based on social exchange theory, the commitment of the dyad partners can be enhanced by role clarity, clear delineation of structures and processes and the experiences in the relationship.47,48 Setting aside individual egos, and exhibiting maturity and humility in working towards a collective identity, ie, a strong identification with the collective team49 and collective dedication50 would foster harmony and cohesion. Understanding the value that each partner brings to the relationship and leveraging each other’s strengths are likely to contribute to cultivating mutual respect, when complemented by timely authentic conversations and undergirded by a foundation of shared values.22 The concept of OBREAU triad (observation, reasonableness and authenticity) is a useful and simple template in having courageous conversations on difficult topics.51 Adaptive leadership, that entails leaders helping others face the challenges and successfully motivate and mobilize,52 is directly relevant to the dyad partners exhibiting these abilities towards each other. Other strategies that would be helpful include team-building activities and social events.53
Switching of leader-follower roles can be facilitated by leadership development interventions aimed at increasing the awareness of the need to transition between leader and follower roles and embracing a follower-self-concept54 and providing honest feedback to each other associated with reflective practice. The dyad partners could also enter mentor-mentee or teacher/facilitator-learner roles with each other, thus relying on and accepting each other’s knowledge, expertise and wisdom. These multiple relationships will enhance “fluidity” when role switching.
Being aware of the need for time required to develop a mature relationship and settle into an “artful leadership dance” where they easily switch leader-follower roles and work as true partners will help in being patient, cut some slack, and have empathy for the other partner. Empathy has been shown to be key in developing the relationship.55
Collaborative Work
There are four pitfalls in working together, unresolved role ambiguity, lack of information sharing, suboptimal decision-making, and indulging in counterproductive actions. These are discussed below.
Unresolved Role Ambiguity
A lack of clarity of the roles may, either inadvertently or deliberately, lead to neglecting one’s responsibilities or overstepping the boundaries. This would not only be unhelpful but may have negative impact on the outputs and outcomes.
Lack of Information Sharing
The dyad partner(s) may not engage in full transparent sharing of information and indulge in knowledge hiding leading to non-cooperation.
Suboptimal Decision-Making
While many decisions made jointly are likely to be better, decision-making dyad leadership dynamics can also negatively affect decision-making and manifest as either a lack of efficiency or poor decisions being made.
Lack of Efficiency
Less efficient decision- making can stem from, a) competing personal agendas and turf battles driving the work, b) overreliance on collaborative and affiliative styles (too much collaboration), or c) “paralysis by analysis”.
Quality of Decisions
Suboptimal decisions may arise when partners lose sight of long-term goals by neglecting client needs and focusing on short-term impacts relevant to their portfolio and individual areas of responsibility or a desire for consensus to preserve harmony. Another contributory factor may be “groupthink”, because critical thinking is often suppressed in this process.
Counterproductive Actions
There are four pitfalls.
Acting Independently
Guarding the areas for which one leader is responsible while withholding it from the partner, although could be rationalized, as efficiency, is a pitfall.
Working Separately with Their Superiors
Although certain unique situations would require working directly and individually with higher-ups eg, physician credentialing and discipline, and certain operational matters, extending this reporting to areas of joint responsibility is a pitfall that may run the risk of sliding into developing parallel streams of work and accountability.
A Lack of Follow-Through
This lack on specific issues may be particularly evident in the dyad model because of the so-called “diffusion of responsibility”, which refers to a “diminished sense of responsibility in groups and social collectives”.56 Role ambiguity and a suboptimal relationship are highly likely to contribute to this phenomenon.
Presenting a Disjointed Front to the Constituents
Discordant messaging by keeping one group’s interests (eg, physicians) apart from the overall organizational interests and delivering separate messages to different groups would convey the fractured relationship to the constituents and fail to achieve group cohesion. Due to the selection processes, especially for physician leaders, where there is a democratic element for input from their peers, the physician leaders may feel opposing tensions between their peers’ interests and the organizational interests. This tension, especially if the dyad leadership is not strong, may pull them towards putting a higher attention and value to the interests of their peers, the so-called “conundrum of accountability”.57
The impact of these pitfalls is emotional exhaustion58 attributable to poor resource exchange and loss of reciprocity,59 and an increase in anxiety.50 Further, poor collaboration may negatively impact the joint performance. For example, working under time pressures, especially in a setting where the collective efficacy of the dyad partners is weak, leads to poor task performance.50
The constructs of psychological ownership and territoriality are relevant to deciphering these pitfalls. Psychological ownership at the individual level defined as a, “state of mind where an individual feels as though the target of ownership (material or immaterial in nature) or a piece of it is “theirs”60 can have both positive61 and negative impact.62 This distinction is most likely linked to the underlying motivation;63 eg, low prosocial motivation64 and high avoidance motivation65 are linked to hiding the knowledge and not sharing the information.
Territoriality defined as exclusive ownership of something (aspects such as physical, social, people, and ideas) and efforts to convey and defend the claim66 is an evolutionary preservation mechanism and has four effects – autonomy, privacy, security, and self-identity.67 Similar to psychological ownership, it can have both negative impacts, eg, knowledge hiding68 and poor team outcomes,69 as well as positive outcomes, eg, increased knowledge sharing associated with territorial expanding.70
Suggested solutions: Collaboration, which involves sharing of information and decision-making, partnership and interdependency, and responsibility and power71 would be enhanced by considering the following suggestions.
Building on the foundation of a mutually valued relationship, the dyad partners need to work towards a state of high collective efficacy, which is an emergent property and more than the sum of individual self-efficacy.72 Continuous attention to and leveraging the common factors underlying effective collaboration – common core values, collaborative working relationships, clear and transparent communication, a mutual respect and complementary competencies – are integral to working together.22 Leveraging each other’s strengths by allocating tasks aligned with these strengths fosters both individual and team performance.73
Considerations for developing a common understanding of responsibilities and their enactment include, a) sharing responsibilities to reach the goals that they alone cannot achieve,71 b) developing a higher level of task-interdependence – especially relevant to designing work distribution in shared areas of responsibility,40 and c) ensuring goal interdependence.74 Healthcare and medical education are known complex adaptive systems and interdependence, entanglement, emergence and self-organization are essential attributes of complexity leadership that need to be understood and leveraged for effective leadership practice.75 Developing a nuanced crafting of role boundaries within the constraints of “official job descriptions” is especially important in the early stages of dyad partnership and requires cultural sensitivity, negotiation skills, and cognizance of the organizational processes.76 Further, true integration of professional and managerial institutional logics requires maintaining a health tension between them or a joint effort by the dyad partners to transcend both logics in pursuit of a higher level overarching purpose.2
Human beings ascribe social meanings to the territories and have an innate need to maintain boundaries and this has implications in the proxemic patterns of interactions with others.77 The insights from the work on psychological ownership and territoriality can be leveraged by exploiting those predispositions and conditions that enhance information and knowledge sharing. Sharing of information can be enhanced when, a) an individual’s personal beliefs are aligned with that of the organization and there is encouragement of knowledge exchange,63 b) practices that promote knowledge sharing are rewarded,78 c) leaders identify themselves with the organization that leads to more prosocial behaviors,79 and d) the partners have invested in developing team cohesiveness44 including enhancing trust.80
Developing a robust evidence-informed decision-making framework and referring to it would help avoid the pitfalls related to decision-making.81 In addition, there needs to be a degree of healthy tension between the two partners where they feel safe enough to voice disagreement and find ways to work through differences, leverage different skills and perspectives without sliding into groupthink.82
Both leaders need to be diligent in presenting a united front to the constituents and the leaders they report to and receive directives from, especially when the other partner is not “in the room”. The adage, “we judge ourselves by our intentions and others by their actions” is highly relevant here; the constituents/followers of the dyad leaders are multiple groups with diverse interests, and the leaders are being watched continuously for cohesion and fractures.
Organizational Level
There are three pitfalls at the organizational level, a lack of preparation for the implementation of the dyad model, inadequate support and ineffective accountability mechanisms for the dyad leaders, and selection of individuals unsuited for dyad leadership roles.
Organizational Readiness and Implementation
Inadequate preparation and non-strategic implementation with little development investment are the pitfalls. The premise of dyad leadership is sharing of leadership; however, most organizations are still hierarchical with centralized top-down governance and linear control83 and there may be resistance and scepticism for the dyad model at various levels of organizational leadership and front-line staff.84 The initial determination would involve suitability of the dyad leadership model to the organization’s mission and vision and its life cycle. Another consideration is which hierarchical levels of leadership/management would benefit from a dyad model, as “shared leadership is not ideal for every team environment”85 and not appropriate for certain situations and contexts.86
Suggested solutions: Ensuring that the organization (structures, processes and people – especially diverse groups) are ready to accept the dyad leadership model requires extensive preparatory work87 for successful joint leadership across professional boundaries. Explaining the rationale and goal,88 addressing structural and cultural aspects,89 and ensuring fairness and transparency in the selection of dyad leaders90 are critical. Clear communication across inter-professional organizational boundaries in complex healthcare contexts is critical as it affects the interdisciplinary discourse, which affects the outcomes of implementation.91 Measuring and evaluating implementation fidelity (including activities and outputs) and outcomes attributable to dyad leadership model (individual and dyad-level effectiveness, leadership experience measures, performance, process improvements, leadership capacity, realized benefits, and return on investment) at the unit, departmental and organizational level, utilizing appropriate evaluation frameworks and instruments are essential.
Support for and Accountability of Dyad Leaders
There are two pitfalls: a) putting people in dyad leadership roles without proper development and support and b) not holding them accountable for joint performance.
Leadership Development and Support
Not providing tailored and contextualized leadership development and ongoing appropriate support (structure, resources, and compensation) and simply assigning dyad leadership roles is a pitfall.
Providing foundational training and education, especially jointly to both the partners, is critical to address the purpose, knowledge and dynamics of sharing leadership – including team’s collective identification - and in developing skills on how to achieve cohesion.92 Investing in enhancing collective efficacy through “efficacy beliefs training” utilizing enactive mastery, vicarious experiences, verbal persuasion and reducing emotional threats of rejection93 is a prudent initial step in getting the leaders prepared for the roles. In addition to training in “team development”, activities that empower leaders to co-design and co-develop their goals and work have been shown to be highly effective.94 Articulating guidelines for sharing leadership is important since internalization of the shared leadership model takes time.34 These guidelines could include goals, roles and responsibilities, implementation and evaluation aspects.
The organizations usually do not reward the exact behaviors required for team success (eg, team development, empowering people, sharing information, providing help from the background and promoting organizational learning);52 instead reward “heroic leadership behaviors” and accomplishments. This sends a mixed message and impacts leadership performance steering the leaders towards individual heroic practices rather than collaborative team behaviors. Developing rewards and incentives that promote collaboration and desired behaviors88 need to be adopted by the organization.
Accountability Through Assessment and Evaluation
Lack of robust mechanisms for ensuring accountability is a pitfall. Since the sharing of leadership has elements of emergence and ongoing evolutionary aspects, it is important to measure its processes and effectiveness and impact on the leaders. The need for “continual assessment and evaluation” has been stressed.89 Given that political realities and conflicts with underlying power and authority issues are part of organizational life, suboptimal dyad partnerships (with their own conflicts and power struggles) can add further complexity, making measurement even more important. In addition to evaluating performance against targets, evaluation of desired behaviors (required for collaboration), processes, foundational elements (eg, density of social networks),95 collective efficacy,50 and impact on personal well-being (eg, psychological health, collective anxiety and collective engagement) using validated cost-effective tools and instruments can allow for timely interventions.
Selecting Individuals for Dyad Leadership Roles
Putting people in dyad relationships when they do not have inclinations/predispositions towards collaboration, empathy and great communication or have a track record of poor performance in these domains is a pitfall. While most capabilities can be acquired through appropriate training and education the role of inherent attributes cannot be overlooked. Further, insecurity or deliberate undermining by a dyad partner cannot just damage the relationship but also negatively impact performance.47
The organizations would benefit by identifying high potential candidates through assessing not only individual leadership attributes and past successes but also factors such as collective orientation, trusting disposition, and the ability to work together with others. There are instruments that may be helpful. The shared leadership mapping (SLM) based on social network analysis assesses other’s perception of an individual’s leadership qualities.96 Validated instruments for the construct of leader developmental readiness (LDR) assess components of motivation and ability.97
Equally important is the need to assess whether the candidates for leadership development are sufficiently committed to the efforts and whether the organization would benefit from the investment. Finally, there is a need for joint selection considering complementary skills and emotional orientations and mechanisms for coordination.84
At All Levels - The Dark Side of Shared Leadership
Not being aware that shared leadership has a dark side and needs to be watched for is a significant pitfall at all levels. There are inherent features in shared leadership that may negatively impact the leaders and the team.98 These include, a) psychological territorial loss (a reduction in the power and influence of a leader who need to accept the leadership of others),81 b) decline in motivation (due to the realization that their ability to provide benefits to the followers is reduced as a result of reduced power and influence),81 and c) navigating the duality of self- and group-paradox (simultaneously be part of the group and different).99 In addition, stress, power struggles, interpersonal conflicts are known adverse effects. These aspects require cognizance, proactive attention and timely reactive responses to benefit from the advantages of shared leadership.
For a seamless implementation across the organization and the practice of dyad leadership at the partner level, following leadership perspectives have been referred to above: for sharing leadership (shared, distributed, connective, collaborative, and collectivist perspectives) and individual actions guided by (ethical, adaptive, and complexity perspectives). In addition, systems leadership, defined as, “the concerted effort of many people working together at different places in the system and at different levels” and it crosses boundaries, both physical and virtual, “existing simultaneously in multiple dimensions”100 is directly relevant to dyad leadership implementation and practice.
Strengths and Limitations
The strengths of this study include triangulation from multiple data sources (extant literature on dyad leadership, interdisciplinary literature on sharing leadership, research in one health region on its experiences in implementation and dyad leadership practice and reflections on “lived” experiences as a dyad leader). This has allowed for combining practical experience with theoretical framing. The findings and insights are based on the somewhat limited peer-reviewed literature on dyad leadership, findings derived from research at one institution and reflections of one individual. This is further constrained by a paucity of studies on dyad leadership effectiveness that can inform required processes and behaviors.
Conclusions and Implications
The pitfalls dyad leaders may encounter are largely rooted in mental frames and shaped by perceptions of power. Further, the underlying factors are likely to intersect and contribute to creating a “mesh” of inefficient and ineffective dynamics and processes. Leaders can use positional power and leadership language to defend their actions that might have been drawn from lower-level non-collaborative and non-relational perspectives. The organizational pitfalls bring into focus the necessity of robust implementation and ongoing commitment at the senior leadership level to the organizational change they have initiated. If unaddressed, there is a high likelihood of significant damage to the dyad relationship and poor organizational performance. Navigating these pitfalls would help agency and well-being, fulfilled relationships and effective collaborative work to utilize the full potential of the dyad leadership.
There are practical and research implications of this study. These findings have implications for governance, policy, strategy and tactics for implementation, the latter including ensuring implementation fidelity and evaluating the effectiveness of implementation itself. Further, evaluating the effectiveness of the dyad leadership model would entail measurement of individual and dyad-level effectiveness, leadership experience measures, performance, process improvements, leadership capacity, and return on investment. Given that the empirical component of this study is based on findings from one health region, the findings need to be interpreted in the context of individual settings. Inclusion of these pitfalls and mitigation strategies in educational curricula for dyad leaders is likely to be of practical relevance and inform daily practice. Further research, especially empirical studies, on the prevalence and role of these pitfalls in dyad leadership practice and the impact on individuals and organizations and underlying mechanisms would contribute to evidence-informed practice.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Self-funded.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pearce CL. The future of leadership; Combining vertical and shared leadership to transform knowledge work. Acad Manag Executive. 2004;18(1):47–16. doi:10.5465/ame.2004.12690298
2. Gibeau É, Langley A, Jean-Louis D, van Schendel N. Bridging competing demands through co-leadership? potential and limitations. Human Relations. 2020;73(4):464–489. doi:10.1177/0018726719888145
3. Dobrow MJ, Sullivan T, Sawka C. Shifting clinical accountability and the pursuit of quality: aligning clinical and administrative approaches. Review. Healthcare Manag Forum/Canadian College Health Service Executives. 2008;21(3):6–19. doi:10.1016/S0840-4704(10)60269-4
4. Edge K. A tale of two leaders: rflecting on senior co-leadership in higher education. In: Netolicky DM, editor. Future Alternatives for Educational Leadership: Diversity, Inclusion, Equity, and Democracy.
5. Kumar C, Lowrie DJ, Pritchard T, Kelly L. Incorporating faculty and student co-leadership in workgroup structures. Med Sci Educ. 2024;34(6):1521–1526. doi:10.1007/s40670-024-02129-2
6. Pearce CL, Conger JA. Shared Leadership: Reframing the Hows and Whys of Leadership. SAGE Publications; 2003.
7. Gronn P. Distributed leadership as a unit of analysis. Leadersh Q. 2002;13(4):423–451. doi:10.1016/S1048-9843(02)00120-0
8. Lipman-Blumen J. The Connective Edge: Leading in an Interdependent World. Jossey-Bass Publishers; 1996.
9. Chrislip DD, Larson CE. Collaborative Leadership. Jossey-Bass Publishers; 1994.
10. Yammarino FJ, Salas E, Serban A, Shirreffs K, Shuffler ML. Collectivistic leadership approaches: putting the “we” in leadership science and practice. Industrial Organizational Psychol. 2012;5(4):382–402. doi:10.1111/j.1754-9434.2012.01467.x
11. Baldwin KS, Dimunation N, Alexander J. Health care leadership and the dyad model. Physician Exec. 2011;37(4):66–70.
12. Sanford KD, Moore S. Dyad Leadership in Healthcare: When One Plus One Is Greater Than Two. Wolters Kluwer; 2015.
13. Zismer DK, Brueggemann J. Examining the “dyad” as a management model in integrated health systems. Physician Exec. 2010;36(1):14–19.
14. Saxena A, Davies M, Philippon D. Structure of healthcare dyad leadership; an organization’s experience. Leadersh Health Serv. 2018;31(2):238–253. doi:10.1108/LHS-12-2017-0076
15. Linhardt R, Holladay CL, Shah A, Rustagi A, Salas E. Dyad leadership blueprint: nine strategies for effective collaboration. BMJ Lead. 2025;leader–2024–001094. doi:10.1136/leader-2024-001094
16. Saxena A. Challenges and success strategies for dyad leadership model in healthcare. Healthcare Manag Forum / Canadian College Health Service Executives. 2021;34(3):137–148. doi:10.1177/0840470420961522
17. Loving V. Optimising doctor-administrator leadership dyads in healthcare organisations. BMJ Lead. 2025;leader–2024–001127. doi:10.1136/leader-2024-001127
18. MacTavish M, Norton P. Redesign of a health science centre: reflections on co-leadership. Healthcare Manag Forum / Canadian College Health Service Executives. 1995;8(4):45–48. doi:10.1016/S0840-4704(10)60932-5
19. Clouser JM, Vundi NL, Cowley AM, et al. Evaluating the clinical dyad leadership model: a narrative review. J Health Organiz Manag. 2020;34(7):725–741. doi:10.1108/JHOM-06-2020-0212
20. Didehban R, Caine NA, Glenn SW, Hasse CH. Role of the administrative partner and the physician-administrator partnership. Mayo Clin Proc Mayo Clin. 2020;95(9s):S38–s40. doi:10.1016/j.mayocp.2020.06.043
21. Leach L, Hastings B, Schwarz G, et al. Distributed leadership in healthcare: leadership dyads and the promise of improved hospital outcomes. Leadersh Health Serv. 2021;34(4):353–374. doi:10.1108/lhs-03-2021-0011
22. Waida E, Harper C, Harris D, Hundal H, Scheepers M, Burrows A. Can we dance together? The dyadic leadership model in physician quality improvement. British Columbia Med J. 2024;66(2):42–45.
23. Comstock NH. Better together: most healthcare leaders report using a dyad leadership model; 2019. Available from: https://www.mgma.com/mgma-stats/better-together-most-healthcare-leaders-report-using-a-dyad-leadership-model.
24. Daiker BL. Shared leadership in a medical practice: keys to success. J Med Pract Manag. 2009;25(2):111–117.
25. Tabrizi B. 75% cross functional teams are dysfunctional. Harvard Business Rev. 2015;23:2–4.
26. Paez A. Gray literature: an important resource in systematic reviews. J Evid Based Med. 2017;10(3):233–240. doi:10.1111/jebm.12266
27. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
28. Al-Quraishi T, Mahdi OA, Abusalem A, et al. Transforming Amazon’s operations: leveraging oracle cloud-based ERP with advanced analytics for data-driven success. Applied Data Sci Analysis. 2024;2024:108–120. doi:10.58496/ADSA/2024/010
29. Kang S, Svensson PG. The benefits and challenges of shared leadership in sport for development and peace collaboratives. Sport Manage Rev. 2023;26(3):383–404. doi:10.1080/14413523.2022.2085430
30. van Knippenberg D, Pearce CL, van Ginkel WP. Shared leadership – vertical leadership dynamics in teams. Organizational Psychol Rev. 2024;15(1):44–67. doi:10.1177/204138662412923
31. Kidder RM. Moral courage, digital distrust: ethics in a troubled world. Bus Soc Rev. 2005;110(4):485–505. doi:10.1111/j.0045-3609.2005.00026.x
32. Gini A. Moral leadership and business ethics. In: Ciullia JB, editor. Ethics: The Heart of Leadership. Praeger Publishers; 2004.
33. Grant H, McCann S. The 4 types of thinking leaders need to practice—and teach. Harvard Business Review. Harvard Business School Publishing; 2025:1–10. Available from: https://hbr.org/2025/02/the-4-types-of-thinking-leaders-need-to-practice-and-teach.
34. Jackson S. A qualitative evaluation of shared leadership barriers, drivers and recommendations. J Manag Med. 2000;14(3–4):166–178. doi:10.1108/02689230010359174
35. Blue I, Fitzgerald M. Interprofessional relations: case studies of working relationships between registered nurses and general practitioners in rural Australia. J Clin Nurs. 2002;11(3):314–321. doi:10.1046/j.1365-2702.2002.00591.x
36. Howard MC, Cogswell JE, Smith MB. The antecedents and outcomes of workplace ostracism: a meta-analysis. J Appl Psychol. 2020;105(6):577–596. doi:10.1037/apl0000453
37. Fransen K, Delvaux E, Mesquita B, Van Puyenbroeck S. The emergence of shared leadership in newly formed teams with an initial structure of vertical leadership: a longitudinal analysis. J Applied Behav Sci. 2018;54(2):140–170. doi:10.1177/0021886318756359
38. Holm F, Fairhurst GT. Configuring shared and hierarchical leadership through authoring. Human Relations. 2017;71(5):692–721. doi:10.1177/0018726717720803
39. Sy T, McCoy T. Being both leaders and followers: advancing a model of leader and follower role switching. In: Lapierre LM, Carsten MK, editors. Followership: What Is It and Why People Follow? Emerald group Publishing Ltd.; 2014: 121–139. chap 7.
40. Nicolaides V, LaPort K, Chen T, et al. The shared leadership of teams: a meta-analysis of proximal, distal, and moderating relationships. Leadersh Q. 2014;25:923–942. doi:10.1016/j.leaqua.2014.06.006
41. Bratman ME. Shared cooperative activity. Philos Rev. 1992;101(2):327–341. doi:10.2307/2185537
42. Balliet D. Communication and cooperation in social dilemmas: a meta-analytic review. J Conflict Resolution. 2009;54(1):39–57. doi:10.1177/0022002709352443
43. Takai A, Fu Q, Doibata Y, et al. Learning acquisition of consistent leader–follower relationships depends on implicit haptic interactions. Sci Rep. 2023;13(1):3476. doi:10.1038/s41598-023-29722-6
44. Lee DS, Lee KC, Seo YW, Choi DY. An analysis of shared leadership, diversity, and team creativity in an e-learning environment. Computers Human Behav. 2015;42:47–56. doi:10.1016/j.chb.2013.10.064
45. Wang H, Peng Q. Is shared leadership really as perfect as we thought? Positive and negative outcomes of shared leadership on employee creativity. J Creative Behav. 2022;56(3):328–343. doi:10.1002/jocb.532
46. Hall P. Interprofessional teamwork: professional cultures as barriers. J Interprofessional Care. 2005;19 Suppl 1:188–196. doi:10.1080/13561820500081745
47. Atencio C, Herbst N. Addressing common obstacles to effective shared leadership: a five-year follow up. J Educ Innovation Commun. 2022;4(1):37–52. doi:10.34097/jeicom-4-1-june2022-3
48. Banai M, Tulimieri P. Contingencies of a leadership symmetric dyad cooperation: the case of the co-CEOs. Leadership Organization Develop J. 2024;45(8):1430–1454. doi:10.1108/LODJ-04-2023-0188
49. Siangchokyoo N, Klinger RL. Shared leadership and team performance: the joint effect of team dispositional composition and collective identification. Group Organ Manag. 2021;47(1):109–140. doi:10.1177/10596011211019928
50. Salanova M, Llorens S, Cifre E, Martínez IM, Schaufeli WB. Perceived collective efficacy, subjective well-being and task performance among electronic work groups: an experimental study. Small Group Res. 2003;34(1):43–73. doi:10.1177/1046496402239577
51. Dunoon D. Mindful OD practice and the Obreau tripod. OD Practitioner. 2014;46(1):18–25.
52. Heifetz R, Laurie D. Mobilizing adaptive work: beyond visionary leadership. In: Conger JA, Spreitzer G, Lawler EE, editors. The Leader’s Change Handbook. Jossey-Bass; 1999.
53. Hannum KM. Social Identity: Knowing Yourself, Knowing Others. John Wiley & Sons.; 2007.
54. Falls A, Allen S. Leader-to-follower transitions: flexibility and awareness. J Leadership Stud. 2020;14(2):24–37. doi:10.1002/jls.21696
55. Abson E, Schofield P. Exploring the antecedents of shared leadership in event organisations. J Hospitality Tourism Manag. 2022;52:439–451. doi:10.1016/j.jhtm.2022.08.003
56. APA. Diffusion of responsibility. Available from: https://dictionary.apa.org/diffusion-of-responsibility.
57. Gill SL. Can doctors and administrators work together? Physician Exec. 1987;13(5):11–16.
58. Thomas CH, Lankau MJ. Preventing burnout: the effects of LMX and mentoring on socialization, role stress, and burnout. Human Resour Manag. 2009;48(3):417–432. doi:10.1002/hrm.20288
59. Bernerth JB, Walker HJ, Harris SG. Rethinking the benefits and pitfalls of leader–member exchange: a reciprocity versus self-protection perspective. Human Relations. 2016;69(3):661–684. doi:10.1177/0018726715594214
60. Pierce JL, Kostova T, Dirks KT. Toward a theory of psychological ownership in organizations. Acad Manag Rev. 2001;26(2):298–310. doi:10.2307/259124
61. Jiang Y, Liao J, Chen J, Hu Y, Du P. Motivation for users’ knowledge-sharing behavior in virtual brand communities: a psychological ownership perspective. Asia Pacific J Market Logistics. 2021;34(10):2165–2183. doi:10.1108/APJML-06-2021-0436
62. Peng H, Pierce J. Job- and organization-based psychological ownership: relationship and outcomes. J Manag Psychol. 2015;30(2):151–168. doi:10.1108/JMP-07-2012-0201
63. Gagné M, Tian A, Soo C, Zhang B, Ho K, Hosszu K. Different motivations for knowledge sharing and hiding: the role of motivating work design. J Organ Behav. 2019;40(7):783–799. doi:10.1002/job.2364
64. Nguyen TM, Malik A, Budhwar P. Knowledge hiding in organizational crisis: the moderating role of leadership. J Bus Res. 2022;139:161–172. doi:10.1016/j.jbusres.2021.09.026
65. Wang L, Law KS, Zhang MJ, Li YN, Liang Y. It’s mine! Psychological ownership of one’s job explains positive and negative workplace outcomes of job engagement. J Applied Psychol. 2019;104(2):229–246. doi:10.1037/apl0000337
66. Brown G, Lawrence TB, Robinson SL. Territoriality in organizations. Acad Manag Rev. 2005;30(3):577–594. doi:10.5465/amr.2005.17293710
67. Leino-Kilpi H, Välimäki M, Dassen T, et al. Privacy: a review of the literature. Int J Nurs Stud. 2001;38(6):663–671. doi:10.1016/s0020-7489(00)00111-5
68. Singh SK. Territoriality, task performance, and workplace deviance: empirical evidence on role of knowledge hiding. J Business Res. 2019;97:10–19. doi:10.1016/j.jbusres.2018.12.034
69. Hernaus T, Sitar AS, Dragicevic N. Evasive (Knowledge) hiding and task performance: the moderating role of job resources. Acad Manag Proceedings. 2022;2022(1):13408. doi:10.5465/AMBPP.2022.13408abstract
70. Chen X, Lee C, Hui C, Lin W, Brown G, Liu J. Feeling possessive, performing well? Effects of job-based psychological ownership on territoriality, information exchange, and job performance. J Applied Psychol. 2023;108(3):403–424. doi:10.1037/apl0001027
71. Clark RC, Greenawald M. Nurse-physician leadership: insights into interprofessional collaboration. J Nurs Administration. 2013;43(12):653–659. doi:10.1097/NNA.0000000000000007
72. Bandura A. Self-Efficacy: The Exercise of Control. Freeman; 1997.
73. Meyers MC, van Woerkom M, Bauwens R. Stronger together: a multilevel study of collective strengths use and team performance. J Business Res. 2023;159:113728. doi:10.1016/j.jbusres.2023.113728
74. Fausing M, Jønsson T, Lewandowski J, Bligh M. Antecedents of shared leadership: empowering leadership and interdependence. Leadership Organization Develop J. 2015;36(3):271–291. doi:10.1108/LODJ-06-2013-0075
75. Uhl-Bien M, Marion R, McKelvey B. Complexity Leadership Theory: shifting leadership from the industrial age to the knowledge era. Leadersh Q. 2007;18(4):298–318. doi:10.1016/j.leaqua.2007.04.002
76. Gibeau E. Co-leadership in healthcare organizations: expanding and constricting new senior management roles for physicians. J Health Organiz Manag. 2025;1–17. doi:10.1108/JHOM-12-2024-0510
77. Danesi M. Proxemics. In: Keith B, editor. Encyclopedia of Language & Linguistics.
78. Batool U, Raziq MM, Obaid A, Sumbal M. Psychological ownership and knowledge behaviors during a pandemic: role of approach motivation. Curr Psychol. 2022;1–11. doi:10.1007/s12144-022-03450-y
79. Hart R. Prosocial behaviors at work: key concepts, measures, interventions, antecedents, and outcomes. Behav Sci. 2024;14(1). doi:10.3390/bs14010078
80. Brown G, Crossley C, Robinson SL. Psychological ownership, territorial behavior, and being perceived as a team contributor: the critical role of trust in the work environment. Personnel Psychol. 2014;67(2):463–485. doi:10.1111/peps.12048
81. Zhu J, Liao Z, Yam KC, Johnson RE. Shared leadership: a state-of-the-art review and future research agenda. J Organ Behav. 2018;39(7):834–852. doi:10.1002/job.2296
82. Kezar A. Trying transformations: implementing team‐oriented forms of leadership. New Directions Institutional Res. 1998;25(4):57–72. doi:10.1002/ir.10005
83. Robertson BJ. Holacracy: The New Management System for a Rapidly Changing World. Henry Holt & Company; 2015.
84. O’Toole J, Galbraith J, Lawler III EE. When two (or more) heads are better than one: the promise and pitfalls of shared leadership. California Manage Rev. 2002;44(4):65–83. doi:10.2307/41166143
85. Bligh M, Pearce C, Kohles J. The importance of self- and shared leadership in team based knowledge work: a meso-level model of leadership dynamics. J Manag Psychol. 2006;21(4):296–318. doi:10.1108/02683940610663105
86. Mumford MD, Friedrich TL, Vessey WB, Ruark GA. Collective leadership: thinking about issues vis-à-vis others. Industrial Organizational Psychol. 2012;5(4):408–411. doi:10.1111/j.1754-9434.2012.01469.x
87. Steinert T, Goebel R, Rieger W. A nurse-physician co-leadership model in psychiatric hospitals: results of a survey among leading staff members in three sites. Int J Ment Health Nurs. 2006;15(4):251–257. doi:10.1111/j.1447-0349.2006.00431.x
88. Kim CS, King E, Stein J, Robinson E, Salameh M, O’Leary KJ. Unit-based interprofessional leadership models in six US hospitals. Review. J Hospital Med. 2014;9(8):545–550. doi:10.1002/jhm.2200
89. Scott L, Caress AL. Shared governance and shared leadership: meeting the challenges of implementation. J Nurs Manag. 2005;13(1):4–12. doi:10.1111/j.1365-2834.2004.00455.x
90. Edelmann CM, Boen F, Stouten J, Broek GV, Fransen K. The advantages and disadvantages of different implementations of shared leadership in organizations: a qualitative study. Leadership. 2023;19(6):467–507. doi:10.1177/17427150231200033
91. Mensah GB, Mijwil MM, Abotaleb M, et al. Explainable AI for healthcare: training healthcare workers to use artificial intelligence techniques to reduce medical negligence in Ghana’s public health act, 2012 (Act 851). EDRAAK. 2025;2025:1–6. doi:10.70470/EDRAAK/2025/001
92. Pearce CL, Manz CC. The new silver bullets of leadership: the importance of self- and shared leadership in knowledge work. Organ Dyn. 2005;34(2):130–140. doi:10.1016/j.orgdyn.2005.03.003
93. Bandura A. Social cognitive theory of personality. In: Pervin LA, John OP, editors. Handbook of Personality.
94. De Brún A, O’Donovan R, McAuliffe E. Interventions to develop collectivistic leadership in healthcare settings: a systematic review. BMC Health Serv Res. 2019;19(1):72. doi:10.1186/s12913-019-3883-x
95. Dall’Asta L, Marsili M, Pin P. Collaboration in social networks. Proc Natl Acad Sci. 2012;109(12):4395–4400. doi:10.1073/pnas.1105757109
96. Fransen K, Van Puyenbroeck S, Loughead TM, et al. Who takes the lead? Social network analysis as a pioneering tool to investigate shared leadership within sports teams. Soc Networks. 2015;43:28–38. doi:10.1016/j.socnet.2015.04.003
97. Hannah ST, Avolio BJ. Developmental readiness: a construct to accelerate leader development.
98. Chen W, Zhang J-H. Does shared leadership always work? A state-of-the-art review and future prospects. J Work-Applied Manag. 2022;15(1):51–66. doi:10.1108/JWAM-09-2022-0063
99. Fletcher JK, Kaufer K. Shared leadership: paradox and possibility. In: Pearcce CL, Conger JA, editors. Shared Leadership: Reframing the Hows and Whys of Leadership. Sage; 2003.
100. Ghate D, Lewis J, Welbourn D. Systems leadership: exceptional leadership for exceptional times – synthesis report; 2013. Available from: https://www.leadershipcentre.org.uk/systemsleadership/wp-content/uploads/2017/01/VSC_Synthesis_exec_complete.pd.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.