Back to Journals » International Journal of General Medicine » Volume 12
Pilot study to explore the prophylactic efficacy of oral probiotic Streptococcus salivarius K12 in preventing recurrent pharyngo-tonsillar episodes in pediatric patients
Authors Marini G, Sitzia E, Panatta ML ![]() , De Vincentiis GC
, De Vincentiis GC
Received 14 March 2018
Accepted for publication 14 March 2019
Published 5 June 2019 Volume 2019:12 Pages 213—217
DOI https://doi.org/10.2147/IJGM.S168209
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Giulia Marini, Emanuela Sitzia, Maria Laura Panatta, Giovanni Carlo De Vincentiis
Department of Otorhinolaryngology, IRCCS Bambino Gesù Pediatric Hospital, Rome, Italy
Background: In the pediatric population, acute pharyngo-tonsillitis represents one of the most frequent causes of access to outpatient treatment and use of antibiotics. In frequent tonsillitis, the pharmacological approach is no longer effective, and, therefore, surgery becomes the treatment of choice.
Methods: This study compares the prophylactic efficacy of Streptococcus salivarius K12 (Bactoblis®) in children with recurrent pharyngo-tonsillitis treated vs untreated, with a 12 -month follow-up. The primary objectives are: The incidence of recurrence of pharyngo-tonsillar episodes and the concomitant use of other drugs. Secondary objectives are: tolerability of the treatment, the effectiveness in terms of clinical improvement, days of absence from school, reduction of the use of standard therapies, and cancellation from the surgical planning list.
Results: Patients belonging to group A (treated with K12 for 90 days) were 24 males and 26 females, mean age 6.6 years (SD=1.57), those belonging to group B (untreated) were 23 males and 27 females, average age 6.8 years (SD=1.72). In the follow-up, group A reported 26 inflammatory pharyngo-tonsillary episodes in the first trimester, unlike group B, who reported 72 in the second trimester. This has shown a lower incidence (3.38%) of the disease compared to group B (6.66%), for a total of 169 inflammatory pharyngo-tonsillary episodes in group A against 333 in group B. A reduction in days of school absence of 429 days in group A and 927 days in the control group (P<0.01) was also noted. Finally, 14 children of group A (28%) underwent adenotonsillectomy, against the whole group B. No adverse events were reported.
Conclusion: The efficacy of K12 on the prevention of pharyngo-tonsillar infections, the decrease in the use of antibiotics and the improvement of the overall quality-of-life was confirmed, with a decreased number of absences from school and fewer patients undergoing surgery.
Keywords: Blis K12, pediatric pharyngo-tonsillitis, adenotonsillectomy, children, probiotics
Introduction
Among the most common upper respiratory tract infections in the pediatric population, acute pharyngotonsillitis represents one of the most frequent causes of access to outpatient treatment and use of antibiotics.
These infections particulary affect children, up to an age of about 10 years, and are more frequently caused by viruses (respirators, enteroviruses, and herpes); only 30% of them are of bacterial origin.
The most serious types of pharyngitis are attributed to bacterial etiologies, such as group A β-haemolytic Streptococcus pyogenes (GAS).1,2
In bacterial tonsillitis, the first choice therapy is the antibiotic therapy with frequent use of penicillins, ampicillin and amoxicillin, alone or with clavulanic acid, in particular. The use of non-steroidal anti-inflammatory drugs (paracetamol and ibuprofen) is effective in reducing symptoms such as fever and pharingodynia.3
In the case of particularly frequent tonsillitis or chronic tonsillitis, the pharmacological approach is no longer effective. The patient in these cases will be referred to surgery: in particular, the surgical removal of the tonsils (tonsillectomy) will be considered.
The criteria proposed for the inclusion in the surgical planning list are those described by the PNLG edition of 2008 (SNLG – Appropriateness and safety of tonsillectomy and/or adenoidectomy) for recurrent inflammation (five or more episodes of tonsillitis in a year, episodes incapacitating such as to prevent normal activities, symptoms persisting for at least 1 year).
An improvement in the quality-of-life after tonsillectomy has been reported in subjects undergoing repeated cycles of antibiotic therapy, but no randomized controlled trials evaluating the effect of tonsillectomy on the general well-being, development, and behavior of the child are available. These measures, however, represent important treatment outcomes to be inserted in future clinical research.4,5
With the aim of reducing the prescription of antibiotic therapies and surgical referrals, the use of specific probiotic therapy for the oral cavity has been proposed, based on the studies of Dr. J. Tagg and colleagues. The Australian microbiologist finally succeeded in isolating a Streptococcus salivarius, called Blis K12®.
He found it from the throat of a child whose medical history revealed that he had never been infected with pharyngo-tonsillar infections; this pathogen, then, was able to kill the dreaded Streptococcus pyogenes, known to be responsible for most of the pharyngo-tonsillar infections of bacterial etiology, and a significant share of acute average otitis.
With this study we propose to explore the prophylactic efficacy of oral Streptococcus salivarius K12 in the pediatric population affected by recurrent pharyngitis-tonsillitis.
Aims of the study
In the present study we propose to compare the prophylactic efficacy of oral Streptococcus salivarius K12 in children with recurrent pharyngo-tonsillitis treated for 3 months with oral discoid Streptococcus salivarius K12 with patients not treated with K12/or standard care for a period of 12 months. We evaluated the prophylactic efficacy with the capability of Streptococcus salivarius K12 in reducing the recurrence rate of pharyngeal and tonsillar episodes and the concomitant use of other drugs as the primary objective. Secondary objectives are: to evaluate the tolerability of the treatment, the effectiveness in terms of clinical improvement, days of absence from school, reduction of the use of standard therapies, and cancellation from the surgical planning list.
Materials and methods
The project was submitted and approved by the Ethics Committee of the Bambino Gesù Pediatric Hospital (registration number 867_OPBG_2014).
The study is prospective, randomized, open, and monocentric. Recruited subjects are of both sexes; aged between 5 and 10 years; enrolled in the surgical planning list, since 2014 at the U.O.C. of Otorhinolaryngology of the Bambino Gesù Pediatric Hospital of Palidoro, for adenotonsillectomy according to the criteria described by the 2008 PNLG for recurrent inflammation; not being treated with Streptococcus salivarius K12 in the 3 months prior to inclusion.
Diagnosis was confirmed by clinical exam by one of the four authors.
Parents provided written consent to the medical treatment and the divulging of personal data for scientific research purposes.
The children were divided into two groups:
- group A (50 patients) were treated with Streptococcus salivarius K12 discoid; and
- group B (50 patients) were not treated with Streptococcus salivarius K12 discoid.
All subjects included in the study were treated, as needed, with NSAIDs, Antibiotics, Steroids, according to good clinical practice.
The exclusion criteria are: the presence of comorbidity; the presence of complicated manifestations of suppurative type and the presence of sleep disorder. The duration of the study was 18 months, 6 for enrollment and 12 for therapy and follow-up. Parents were asked to complete a clinical diary describing the inflammatory episodes and possible drug treatment. A clinical evaluation of the patient was performed quarterly, and the pharyngo-tonsillar episodes and the relative therapies were noted. No pharyngeal swabs were performed during the inflammatory episodes, because all patients enrolled had previously been diagnosed with chronic tonsillitis by GAS.
Statistic analysis
The proposed study is an exploratory pilot study, whereby the sample size of 100 subjects (50 per group) was chosen purely for convenience and adequate for feasibility.
Data are expressed as mean and standard deviation and compared with the Mann-Whitney test, Kruskall Wallis, or 2-way variance analysis. The analysis will be “intention to treat”, leaving each patient in the original randomization arm. The data, possibly missing, are therefore not taken into consideration.
Results
Patients belonging to group A (treated with oral discoid Streptococcus salivarius K12 for 90 days) were 24 males and 26 females, mean age 6.6 years (SD=1.57), those belonging to group B (untreated) were 23 males and 27 females, average age 6.8 years (SD=1.72). In the 12 months of follow-up, group A reported in the first trimester, that of treatment with Streptococcus salivarius K12, 26 inflammatory pharyngo-tonsillary episodes unlike group B which reported 72, in the second trimester, despite the absence of treatment group A has showed a lower incidence (3.38%) of the disease compared to group B (6.66%) for a total in the year of observation of 169 EFT in group A against 333 of group B (Table 1).
 | Table 1 Number of inflammatory pharyngo-tonsillary episodes in two groups in 12 months of follow-up |
We also evaluated the consumption, by dose, of NSAIDs and antibiotic drugs, with a reduction in the use of group A drugs, especially in the quarter of treatment with Streptococcus salivarius K12 (Table 2).
 | Table 2 Consumption, by dose, of NSAIDs and antibiotic drugs in 12 months of follow-up |
In the 12 months of observation we also noticed a reduction in days of school absence of 429 days in group A and 927 days in the control group (P<0.01) (Table 3).
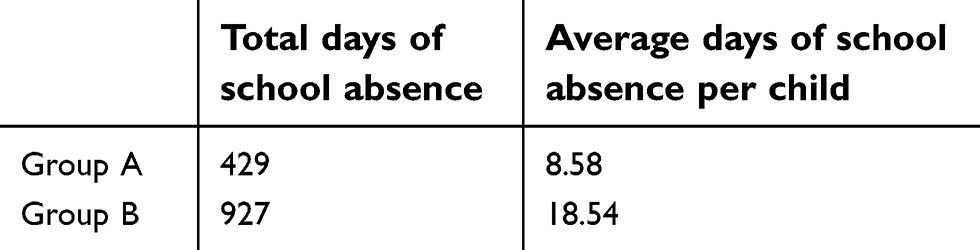 | Table 3 Days of school absence in two groups in 12 months of follow-up (P<0.01) |
Finally, based on the results obtained and after having subjected all the patients enrolled to clinical control, 14 children of group A (28%) underwent adenotonsillectomy, against the whole group B. No adverse events were reported after use of oral Streptococcus salivarius K12 (Table 4).
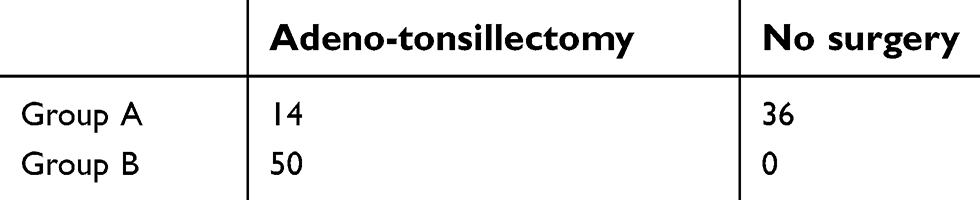 | Table 4 Patients who underwent surgery or not |
Discussion
Interest in probiotic therapy has gained considerable importance in the treatment of bacterial infections in recent years, so that in the past antibiotic therapy existed as the only alternative. After John Tagg’s results, in the following years a number of different strains of Streptococcus pyogenes were tested and collected in microbiological laboratories around the world. The testing, to date, has given excellent results. In fact, all tested strains were killed by Blis K12®.6
The analysis of the genome of Blis K12® shows the mechanism behind this anti-streptococcal action. In its cell body is in fact identified a megaplasmide of 190 kilobases coding for two bacteriocins belonging to the group of lantibiotics: salivaricin A2 and salivaricin B. These, also isolated, effectively determine the death of Streptococcus pyogenes and also some other strains involved in infectious processes that affect the middle ear or periodontitis with halitosis.
The secretion of the two bacteriocins, however, is not the only mechanism of action of its potential clinical effects.
In fact, it has been observed that the administration of K12 down modulates, in the host, the expression of some genes involved in the inflammatory cascade, as well as the release of some pro-inflammatory lymphokines (IL-6 and IL-8). The overall action resulting from the oral administration of Streptococcus salivarius K12 is probably the result of an integrated mechanism where a targeted action against other streptococci (pyogenes in particular) is associated with an anti-inflammatory capacity of promoting host-microbe homeostasis.7,8
For this purpose, a study was carried out, the results of which were published in the International Journal of General Medicine, which showed that, in a group of patients treated for 90 days with K12, there was a statistically significant decrease in the incidence of pharyngo-tonsillitis by SBEA and otitis.9
The efficacy results, in terms of incidence of streptococcal-pharyngeal disease during the study compared to the previous year, confirmed that prophylaxis with Bactoblis® reduced the incidence of β-hemolytic streptococcal oropharyngeal infections of about 96% and viral infections of 80%. Treatment was well tolerated, with no notable side-effects. Compliance was very good. Other studies on the preventive efficacy of K12 on the pediatric population10–13 and on adults followed, and all showed a significant decrease in pharyngo-tonsillary infectious episodes.14
With this study, we have confirmed that the treatment with oral Streptococcus salivarius K12 prevents the onset of pharyngo-tonsillary infections, is a valid alternative to antibiotic therapy and, above all, never taken into account in the previously cited studies, avoids the use of adenotonsillectomy, non-surgical intervention of risks, such as postoperative hemorrhage, and lethal complications.15
The limitations of these studies are the number of patients enrolled (50 per study group), pharyngo-tonsillar infections during follow-up were diagnosed and treated by the treating physician and without the execution of a throat swab and the absence of double blind randomization. Future investigations are needed to confirm these results in a bigger sample size.
Conclusions
The results of this study confirmed the efficacy of oral Streptococcus salivarius K12 on the prevention of pharyngo-tonsillar infections, and we were able to show the decrease in the use of antibiotics and the improvement of the overall quality-of-life, with a decreased number of absences from school and fewer patients undergoing surgery of adenotonsillectomy.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Murray RC, Chennupati SK. Chronic streptococcal and non-streptococcal pharyngitis. Infect Disord Drug Targets. 2012;12(4):281–285. doi:10.2174/187152612801319311
2. Bonsignori F, Chiappini E, De Martino M. The infections of the upper respiratory tract in children. Int J Immunopathol Pharmacol. 2010;23(Suppl 1):16–19.
3. Stelter K. Tonsillitis and sore throat in childhood. Laryngorhinootologie. 2014;93(Suppl 1):S84–S102. doi:10.1055/s-0033-1363210
4. Douglas CM, Lang K, Whitmer WM, Wilson JA, Mackenzie K. The effect of tonsillectomy on the morbidity from recurrent tonsillitis. Clin Otolaryngol. 2017;42:1206–1210. doi:10.1111/coa.12850
5. El Hennawi DE, Rifaat Ahmed M. Quality of life after tonsillectomy versus azithromycin. Interv Med Appl Sci. 2016;8(4):141–146. doi:10.1556/1646.8.2016.4.2
6. Wescombe PA, Hale JD, Heng NC, Tagg JR. Developing oral probi- otics from Streptococcus salivarius. Future Microbiol. 2012;7(12):1355–1371. doi:10.2217/fmb.12.113
7. Tagg JR. Prevention of streptococcal pharyngitis by anti-Streptococcus pyogenes bacteriocin-like inhibitory substances (BLIS) produced by Streptococcus salivarius. Indian J Med. 2004;119(Suppl):13–16.
8. Hyink O, Wescombe PA, Upton M, Ragland N, Burton JP, Tagg JR. Salivaricin A2 and the novel lantibiotic salivaricin B are encoded at adjacent loci on a 190-kilobase transmissible megaplasmid in the oral probiotic strain Streptococcus salivarius K12. Appl Environ Microbiol. 2007;73(4):1107–1113. doi:10.1128/AEM.02265-06
9. Di Pierro F, Donato G, Fomia F, et al. Preliminary pediatric clinical evaluation of the oral probiotic Streptococcus salivarius K12 in preventing recurrent pharyngitis and/or tonsillitis caused by Streptococcus pyogenes and recurrent acute otitis media. Int J Gen Med. 2012;5:991–997. doi:10.2147/IJGM.S38859
10. Di Pierro F, Colombo M, Giuliani MG, et al. Effect of administration of Streptococcus salivarius K12 on the occurrence of streptococcal pharyngo-tonsillitis, scarlet fever and acute otitis media in 3 years old children. Eur Rev Med Pharmacol Sci. 2016;20(21):4601–4606.
11. Gregori G, Righi O, Risso P, et al. Reduction of group A beta-hemolytic streptococcus pharyngo-tonsillar infections associated with use of the oral probiotic Streptococcus salivarius K12: a retrospective observational study. Ther Clin Risk Manag. 2016;12:87–92. doi:10.2147/TCRM.S96134
12. Di Pierro F, Di Pasquale D, Di Cicco M. Oral use of Streptococcus salivarius K12 in children with secretory otitis media: preliminary results of a pilot, uncontrolled study. Int J Gen Med. 2015;8:303–308. doi:10.2147/IJGM.S92488
13. Di Pierro F, Colombo M, Zanvit A, Risso P, Rottoli AS. Use of Streptococcus salivarius K12 in the prevention of streptococcal and viral pharyngotonsillitis in children. Drug Healthc Patient Saf. 2014;6:15–20. doi:10.2147/DHPS.S59665
14. Di Pierro F, Adami T, Rapacioli G, Giardini N, Streitberger C. Clinical evaluation of the oral probiotic Streptococcus salivarius K12 in the prevention of recurrent pharyngitis and/or tonsillitis caused by Streptococcus pyogenes in adults. Expert Opin Biol Ther. 2013;13(3):339–343. doi:10.1517/14712598.2013.75871
15. Reusser NM, Bender RW, Agrawal NA, Albright JT, Duncan NO, Edmonds JL. Post-tonsillectomy hemorrhage rates in children compared by surgical technique. Ear Nose Throat J. 2017;96(7):E7–E11. doi:10.1177/014556131709600702
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.