Back to Archived Journals » Open Access Surgery » Volume 8
Pilonidal sinus – challenges and solutions
Received 21 June 2015
Accepted for publication 27 August 2015
Published 25 September 2015 Volume 2015:8 Pages 67—71
DOI https://doi.org/10.2147/OAS.S54939
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Cataldo Doria
Ali Guner, Arif Burak Cekic
Department of General Surgery, Karadeniz Technical University, Farabi Hospital, Trabzon, Turkey
Abstract: Although it is clinically asymptomatic in some cases, pilonidal sinus disease may also present as a complicated disease, characterized by multiple sinus tracts, leading to severe impairment of patient quality of life. Although clinical studies of pilonidal sinus have been conducted for approximately a century, the gold standard for treatment is undefined. The ideal treatment requires a shorter hospital stay, requires less wound care, results in rapid recovery, maintains quality of life, and has low recurrence rates. In this review, we aim to discuss the challenges and possible solutions for the management of pilonidal sinus disease.
Keywords: pilonidal sinus disease, surgery, management, complications, recurrence
What is sacrococcygeal pilonidal sinus disease and what causes it?
The history of sacrococcygeal pilonidal sinus disease (PSD) began in the early 19th century. The disease was first reported by Herbert Mayo in 1833 and first defined as “pilonidal sinus” by Richard Manning Hodges in 1880.1 It is common, particularly in young adults. The disease may be associated with sex hormones because it is most commonly observed between puberty and 40 years of age; furthermore, it may be associated with a more hirsute nature because it is more frequently observed in males than in females.2,3
Having treated thousands of PSD cases over 35 years of practice, Karydakis stated that various factors predispose patients to hair insertion, which results in PSD.4 Factors such as the H-factor (hair), F-factor (forces such as depth and narrowness of the natal cleft), and V-factor (vulnerability) act together and cause first hair insertion, which is followed by the easy insertion of other hairs and, finally, development of PSD. Different from this theorem, Bascom noted that the primary pathology of pilonidal sinus originates from the follicle and the normal follicle becomes a stretched follicle and an epithelial tube over time; a chronic abscess cavity and hair insertion develop secondary to these changes.5,6 Consistent with this hypothesis, it has been demonstrated that hair was detected in histopathological examinations in only 65% of PSD cases.7
PSD is a heterogeneous disease group with varied presentations. Although it may be incidentally detected after an asymptomatic course, it could present as a complicated chronic form that develops fistulization in different gluteal regions.8 Furthermore, acute abscess formation is a frequently encountered presentation.
Management of sacrococcygeal PSD
The results of surgical treatment for incidentally detected PSD are not superior to the outcomes obtained for chronic fistulized PSD.7 Thus, observation alone is appropriate in asymptomatic patients. Furthermore, the incidence of symptoms in previously asymptomatic patients is not known. Recommendations such as epilation of the gluteal region, cleaning the hairs, and frequent bathing can be administered to reduce the risk of disease progression during the observation period.9
Whether primary or recurrent, PSD can present as an acute abscess. Similar to abscesses anywhere on the body, simple abscess drainage can be performed. In addition, curettage and debridement provide greater healing and lower recurrence rates.10,11 Alternatively, needle aspiration of the abscess can be performed together with antibiotic therapy. It has been demonstrated that an emergency situation can be delayed and treated with elective surgery.12 Problems caused by abscess drainage, such as functional work loss and slow recovery, can be prevented in 95% of these patients by this approach.
Although clinical studies of chronic pilonidal sinus have been conducted for approximately a century, the gold standard treatment is undefined. Although most investigations have analyzed surgical treatment, the effectiveness of nonsurgical methods has been investigated recently. The absence of an ideal treatment method results in suboptimal outcomes. The ideal treatment entails shorter hospital stays, requires less wound care, results in rapid recovery, maintains quality of life, and has low recurrence rates. However, no current treatment ensures all of these factors. Furthermore, the heterogeneous nature of the chronic disease limits the applicability of a single treatment approach to all patients.13–16
Primary PSD most frequently begins as a single-follicle disease and advances by incorporating other hair follicles. Later, the disease may fistulize to the gluteal region unilaterally or bilaterally. Because the size of the defect after surgical excision and method used to close this defect are directly associated with the clinical outcomes, the treatment approach varies according to the development stage of the disease.17,18 There is no staging system that has been defined for PSD. Although different authors have developed classification systems, these classifications have generally considered clinical presentations of the disease, independent of its progressive course.19,20 An ideal classification system should differentiate an acute abscess from chronic sinus disease, asymptomatic from symptomatic, and primary from recurrent. According to our institutional approach, we classify the chronic disease that is restricted to the midline as single/multiple-pit disease, whereas we classify the disease outside the midline as unilateral/bilateral; therefore, different treatment protocols exist for each disease stage. Furthermore, together with this staging approach, it is possible to share more accurate data among investigators, and the ideal treatment for each stage can be determined. As this staging approach becomes widespread in clinical practice, an ideal treatment approach can be developed.
Which technique should be used in surgical treatment?
The application of a single treatment approach to all cases with chronic symptomatic PSD would result in suboptimal outcomes. An individualized approach is desirable to avoid both overtreatment and undertreatment. To date, a comparative clinical study of stage-based treatment approaches has not been performed. The only consensus from several studies is that off-midline treatment is more appropriate.14
The two Cochrane meta-analyses that were published in 2007 and 2010 compared primary closure and secondary healing: the first meta-analysis included 18 studies and the second included 26 studies by adding eight more to the first analysis.21,22 Although wound healing was faster in the primary closure group, recurrence rates were higher. Neither approach was clearly superior.
Primary closure after removal of diseased tissue is the most common approach in clinical practice. Both edges of the wound are approximated. However, approximation of wound edges at the midline would cause high pressure and more traction. Thus, different off-midline and flap techniques can decrease wound tension, prevent separation, and avoid associated complications in the early stages of recovery.23,24 Furthermore, the flattening of the natal cleft is an important issue.25–27 Elimination of negative pressure and a vacuum effect in the midline, which are risk factors for PSD, may decrease future recurrences. Thus, in addition to off-midline treatment, flattening of the midline may help guide treatment choice.
The techniques that meet these criteria may be classified as advancing flaps and rotation flaps. The Karydakis flap, Bascom flap, and V-Y flap are classified as advancing flaps.28–30 Rotation flaps included the Limberg flap, modified Limberg flap, Dufourmentel flap, Z-plasty, and gluteus maximus fasciocutaneous flap.31–34 Outcomes of randomized studies for these techniques are presented in Table 1. Different endpoints have been used in the studies, and the superiority or noninferiority of each technique is mentioned. Overall, no evidence demonstrates definite superiority of one method over the others.
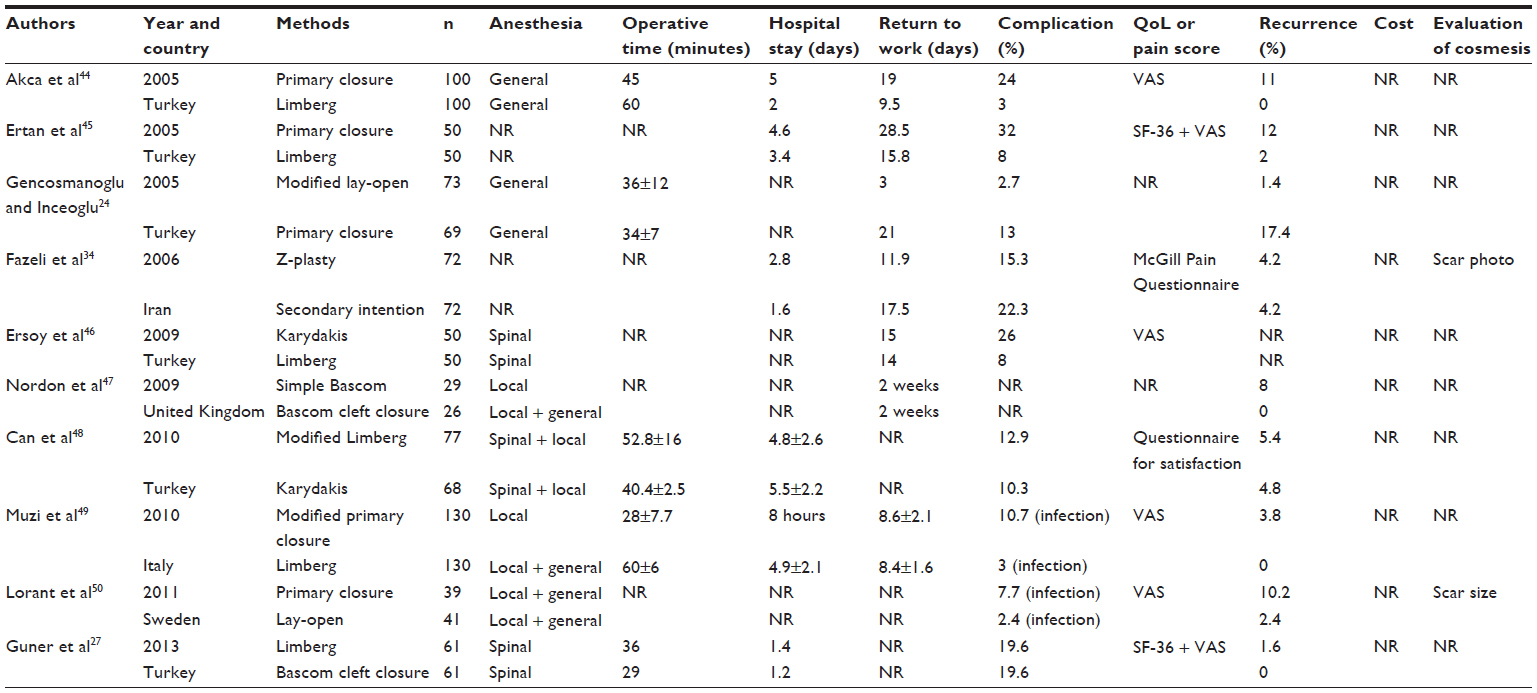 | Table 1 Outcomes of randomized studies comparing different techniques |
Symptomatic PSD sometimes can be presented as single-follicle disease. In those cases, flap procedures can be considered an aggressive approach. Therefore, minimally invasive techniques such as sinusectomy or a pit-picking technique would be a better approach to avoid overtreatment.5,35 Minially invasive techniques can be performed under local anesthesia as a day-case procedure and provide early recovery with acceptable morbidity.
Recurrent disease requires different management than primary disease
Recurrent disease is defined as a PSD case that has undergone curative therapy, completely healed, and recurred. Although unhealed wounds are defined as recurrent disease by some authors, these two are different clinical entities.16,36–38 The treatment of recurrent disease is more difficult than that of primary disease. The anatomical changes following prior treatment, the removed tissue, and the invasiveness of the current disease dictate the preferred treatment approach.26,39 Recurrent cases are separately evaluated from primary cases in our institutional algorithm. After the assessment of multiple factors, the appropriate approach is determined. Although the application of flap techniques is recommended in the literature, favorable results can be obtained with minimally invasive treatments in an individualized approach.25,27 Because it is difficult to define the progressive course of the primary disease for the recurrent disease, there is a requirement for a different classification system.
Nonsurgical treatment
Among the nonsurgical treatment options, crystallized phenol application is frequently used.40,41 Although it requires a long recovery period, it could be used in both primary and recurrent cases because it results in earlier return to work, low morbidity, and high success rates. However, there is a requirement for further studies on this subject. No randomized trials on this subject exist, and long-term results are unknown. Some studies have reported successful results after cryosurgery with liquid nitrogen or fibrin glue application after cleaning the sinus content.42,43 However, these studies are limited in number and methodologically weak.
Conclusion
Achieving the ideal management of PSD requires:
- A staging system. It is necessary to define a staging system consistent with the varied clinical presentations of the disease, resulting in a stage-specific treatment approach. Furthermore, by applying different treatment approaches to different stages, data sharing among investigators would improve.
- Primary endpoints for future clinical studies. Although several clinical studies evaluate recurrence rates, a low recurrence rate alone is not sufficient to determine the ideal treatment. Similar to recurrence rate, early morbidity plays an important role. Therefore, in future clinical studies, data such as complication rates, work loss, cosmetic results, quality of life, and cost should be evaluated in addition to recurrence rates.
- A definition of ideal treatment. Currently, there is no standard, recommended treatment for all patients with PSD. An individualized approach that assesses the extent of disease, social status, and expectations of the patient would be ideal. The gold standard for treatment would not only produce excellent cosmetic results, but also remove predisposing factors for PSD by flattening the natal cleft and enabling tension-free repair.
Disclosure
The authors report no conflicts of interest in this work.
References
Humphries AE, Duncan JE. Evaluation and management of pilonidal disease. Surg Clin North Am. 2010;90(1):113–124. | |
Raffman RA. A re-evaluation of the pathogenesis of pilonidal sinus. Ann Surg. 1959;150:895–903. | |
Søndenaa K, Andersen E, Nesvik I, Søreide JA. Patient characteristics and symptoms in chronic pilonidal sinus disease. Int J Colorectal Dis. 1995;10(1):39–42. | |
Karydakis GE. Easy and successful treatment of pilonidal sinus after explanation of its causative process. Aust N Z J Surg. 1992;62(5):385–389. | |
Bascom J. Pilonidal disease: origin from follicles of hairs and results of follicle removal as treatment. Surgery. 1980;87(5):567–572. | |
Bascom J. Pilonidal sinus: experience with the Karydakis flap. Br J Surg. 1998;85(6):874. | |
Doll D, Friederichs J, Boulesteix AL, Düsel W, Fend F, Petersen S. Surgery for asymptomatic pilonidal sinus disease. Int J Colorectal Dis. 2008;23(9):839–844. | |
Abdelrazeq AS, Rahman M, Botterill ID, Alexander DJ. Short-term and long-term outcomes of the cleft lift procedure in the management of nonacute pilonidal disorders. Dis Colon Rectum. 2008;51(7):1100–1106. | |
Ersoy OF, Karaca S, Kayaoglu HA, Ozkan N, Celik A, Ozum T. Comparison of different surgical options in the treatment of pilonidal disease: retrospective analysis of 175 patients. Kaohsiung J Med Sci. 2007;23(2):67–70. | |
Jensen SL, Harling H. Prognosis after simple incision and drainage for a first-episode acute pilonidal abscess. Br J Surg. 1988;75(1):60–61. | |
Vahedian J, Nabavizadeh F, Nakhaee N, Vahedian M, Sadeghpour A. Comparison between drainage and curettage in the treatment of acute pilonidal abscess. Saudi Med J. 2005;26(4):553–555. | |
Hussain ZI, Aghahoseini A, Alexander D. Converting emergency pilonidal abscess into an elective procedure. Dis Colon Rectum. 2012; 55(6):640–645. | |
Petersen S, Koch R, Stelzner S, Wendlandt TP, Ludwig K. Primary closure techniques in chronic pilonidal sinus: a survey of the results of different surgical approaches. Dis Colon Rectum. 2002;45(11):1458–1467. | |
McCallum IJ, King PM, Bruce J. Healing by primary closure versus open healing after surgery for pilonidal sinus: systematic review and meta-analysis. BMJ. 2008;336(7649):868–871. | |
Kulacoglu H, Dener C, Tumer H, Aktimur R. Total subcutaneous fistulectomy combined with Karydakis flap for sacrococcygeal pilonidal disease with secondary perianal opening. Colorectal Dis. 2006;8(2):120–123. | |
Doll D, Krueger CM, Schrank S, Dettmann H, Petersen S, Duesel W. Timeline of recurrence after primary and secondary pilonidal sinus surgery. Dis Colon Rectum. 2007;50(11):1928–1934. | |
de Parades V, Bouchard D, Janier M, Berger A. Pilonidal sinus disease. J Visc Surg. 2013;150(4):237–247. | |
Shabbir J, Chaudhary BN, Britton DC. Management of sacrococcygeal pilonidal sinus disease: a snapshot of current practice. Int J Colorectal Dis. 2011;26(12):1619–1620. | |
Tezel E. A new classification according to navicular area concept for sacrococcygeal pilonidal disease. Colorectal Dis. 2007;9(6):575–576. | |
Irkörücü O, Erdem H, Reyhan E. The best therapy for pilonidal disease: which management for which type? World J Surg. 2012;36(3):691–692. | |
Al-Khamis A, McCallum I, King PM, Bruce J. Healing by primary versus secondary intention after surgical treatment for pilonidal sinus. Cochrane Database Syst Rev. 2010;(1):CD006213. | |
McCallum I, King PM, Bruce J. Healing by primary versus secondary intention after surgical treatment for pilonidal sinus. Cochrane Database Syst Rev. 2007;(4):CD006213. | |
Mentes O, Bagci M, Bilgin T, Ozgul O, Ozdemir M. Limberg flap procedure for pilonidal sinus disease: results of 353 patients. Langenbecks Arch Surg. 2008;393(2):185–189. | |
Gencosmanoglu R, Inceoglu R. Modified lay-open (incision, curettage, partial lateral wall excision and marsupialization) versus total excision with primary closure in the treatment of chronic sacrococcygeal pilonidal sinus: a prospective, randomized clinical trial with a complete two-year follow-up. Int J Colorectal Dis. 2005;20(5):415–422. | |
Mentes BB, Leventoglu S, Cihan A, Tatlicioglu E, Akin M, Oguz M. Modified Limberg transposition flap for sacrococcygeal pilonidal sinus. Surg Today. 2004;34(5):419–423. | |
Theodoropoulos GE, Vlahos K, Lazaris AC, Tahteris E, Panoussopoulos D. Modified Bascom’s asymmetric midgluteal cleft closure technique for recurrent pilonidal disease: early experience in a military hospital. Dis Colon Rectum. 2003;46(9):1286–1291. | |
Guner A, Boz A, Ozkan OF, Ileli O, Kece C, Reis E. Limberg flap versus Bascom cleft lift techniques for sacrococcygeal pilonidal sinus: prospective, randomized trial. World J Surg. 2013;37(9):2074–2080. | |
Petersen S, Aumann G, Kramer A, Doll D, Sailer M, Hellmich G. Short-term results of Karydakis flap for pilonidal sinus disease. Tech Coloproctol. 2007;11(3):235–240. | |
Guner A, Ozkan OF, Kece C, Kesici S, Kucuktulu U. Modification of the Bascom cleft lift procedure for chronic pilonidal sinus: results in 141 patients. Colorectal Dis. 2013;15(7):e402–e406. | |
Nursal TZ, Ezer A, Caliskan K, Törer N, Belli S, Moray G. Prospective randomized controlled trial comparing V-Y advancement flap with primary suture methods in pilonidal disease. Am J Surg. 2010;199(2):170–177. | |
Akin M, Leventoglu S, Mentes BB, et al. Comparison of the classic Limberg flap and modified Limberg flap in the treatment of pilonidal sinus disease: a retrospective analysis of 416 patients. Surg Today. 2010;40(8):757–762. | |
Kayaalp C, Aydin C, Olmez A. Dufourmentel rhomboid flap for pilonidal disease. Dis Colon Rectum. 2009;52(1):169–170; author reply 170–171. | |
Schrögendorfer KF, Haslik W, Aszmann OC, Vierhapper M, Frey M, Lumenta DB. Prospective evaluation of a single-sided innervated gluteal artery perforator flap for reconstruction for extensive and recurrent pilonidal sinus disease: functional, aesthetic, and patient-reported long-term outcomes. World J Surg. 2012;36(9):2230–2236. | |
Fazeli MS, Adel MG, Lebaschi AH. Comparison of outcomes in Z-plasty and delayed healing by secondary intention of the wound after excision of the sacral pilonidal sinus: results of a randomized, clinical trial. Dis Colon Rectum. 2006;49(12):1831–1836. | |
Soll C, Dindo D, Steinemann D, Hauffe T, Clavien PA, Hahnloser D. Sinusectomy for primary pilonidal sinus: less is more. Surgery. 2011;150:996–1001. | |
Doll D. 5- and 10-year recurrence rate is the new gold standard in pilonidal sinus surgery benchmarking. Med Princ Pract. 2010;19(3):216–217. | |
Bascom J, Bascom T. Failed pilonidal surgery: new paradigm and new operation leading to cures. Arch Surg. 2002;137(10):1146–1150. | |
Bascom J, Bascom T. Prevention of wound healing disorders and recurrence. Am J Surg. 2009;198(2):293–294. | |
Aygen E, Arslan K, Dogru O, Basbug M, Camci C. Crystallized phenol in nonoperative treatment of previously operated, recurrent pilonidal disease. Dis Colon Rectum. 2010;53(6):932–935. | |
Kayaalp C, Aydin C. Review of phenol treatment in sacrococcygeal pilonidal disease. Tech Coloproctol. 2009;13(3):189–193. | |
Dogru O, Camci C, Aygen E, Girgin M, Topuz O. Pilonidal sinus treated with crystallized phenol: an eight-year experience. Dis Colon Rectum. 2004;47(11):1934–1938. | |
Werbin N, Greenberg R. Treatment of pilonidal sinus disease using fibrin glue. Dis Colon Rectum. 2005;48(12):2352–2353. | |
Gage AA, Dutta P. Cryosurgery for pilonidal disease. Am J Surg. 1977;133(2):249–254. | |
Akca T, Colak T, Ustunsoy B, Kanik A, Aydin S. Randomized clinical trial comparing primary closure with the Limberg flap in the treatment of primary sacrococcygeal pilonidal disease. Br J Surg. 2005;92(9):1081–1084. | |
Ertan T, Koc M, Gocmen E, Aslar AK, Keskek M, Kilic M. Does technique alter quality of life after pilonidal sinus surgery? Am J Surg. 2005;190(3):388–392. | |
Ersoy E, Devay AO, Aktimur R, Doganay B, Ozdogan M, Gündogdu RH. Comparison of the short-term results after Limberg and Karydakis procedures for pilonidal disease: randomized prospective analysis of 100 patients. Colorectal Dis. 2009;11(7):705–710. | |
Nordon IM, Senapati A, Cripps NP. A prospective randomized controlled trial of simple Bascom’s technique versus Bascom’s cleft closure for the treatment of chronic pilonidal disease. Am J Surg. 2009;197(2):189–192. | |
Can MF, Sevinc MM, Hancerliogullari O, Yilmaz M, Yagci G. Multicenter prospective randomized trial comparing modified Limberg flap transposition and Karydakis flap reconstruction in patients with sacrococcygeal pilonidal disease. Am J Surg. 2010;200(3):318–327. | |
Muzi MG, Milito G, Cadeddu F, et al. Randomized comparison of Limberg flap versus modified primary closure for the treatment of pilonidal disease. Am J Surg. 2010;200(1):9–14. | |
Lorant T, Ribbe I, Mahteme H, Gustafsson UM, Graf W. Sinus excision and primary closure versus laying open in pilonidal disease: a prospective randomized trial. Dis Colon Rectum. 2011;54(3):300–305. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.