Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Physiotherapy Practice for Management of Patients Undergoing Upper Abdominal Surgery in United Arab Emirates – A National Survey
Authors Aldhuhoori FZ, Walton LM, Bairapareddy KC, Amaravadi SK ![]() , Alaparthi GK
, Alaparthi GK ![]()
Received 8 July 2021
Accepted for publication 24 August 2021
Published 14 September 2021 Volume 2021:14 Pages 2513—2526
DOI https://doi.org/10.2147/JMDH.S328528
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Fatima Zaid Aldhuhoori,1 Lori Maria Walton,2 Kalyana Chakravarthy Bairapareddy,1 Sampath Kumar Amaravadi,3 Gopala Krishna Alaparthi1
1Department of Physiotherapy, College of Health Sciences, University of Sharjah, Sharjah, United Arab Emirates; 2Department of Physiotherapy, University of Scranton, Scranton, PA, USA; 3Department of Physiotherapy, College of Health Sciences, Gulf Medical University, Ajman, United Arab Emirates
Correspondence: Gopala Krishna Alaparthi
Department of Physiotherapy, College of Health Sciences, University of Sharjah, Sharjah, United Arab Emirates
Tel +971 504899323
Email [email protected]
Background: The main goal of physiotherapy post-upper abdominal surgery (UAS) is to expedite recovery from the surgery by avoiding or remediating postoperative pulmonary complications (PPCs) and offering physical rehabilitation to ease the process of returning to premorbid status. The present study aimed to survey physiotherapists in the United Arab Emirates (UAE) about their clinical practice in the assessment and management of patients having upper abdominal surgery.
Methods: The current study adopted a novel anonymous online survey to explore the current practice among physiotherapists in the UAE. The Research Ethics Committee approved the study, and a questionnaire was borrowed from a previous study with similar objectives completed in Australia. The questionnaire had 51 questions cutting across 7 sections that investigated the assessment tools and interventions and explored current practice amongst physiotherapists treating patients following abdominal surgery in UAE hospitals.
Results: A survey of 42 post-UAS physiotherapy practitioners across the UAE was conducted with a 42% response rate and 57.5% completion rate. The mean age of physiotherapists who were working in the UAE is 35 years, most of whom have more than five years of general ward experience. Most patients were not seen on day zero (day of surgery). Respondents in the UAE are almost universally preferred prescribing deep breathing exercises, incentive spirometry (IS), mobility from the bedside, and education as their primary intervention either “often” or “always” in the consecutive days post-UAS. Spo2, visual analog scale, respiratory rate and fatigue are used as key outcome measures.
Conclusion: Research work on physiotherapy postoperatively has shown demonstrated prominence of mobilization but is not yet reflected in current practice among physiotherapists caring for post-UAS cohorts in the UAE. The vast difference in the choice of screening tools preferred by physiotherapists in diagnosing high-risk patients postoperatively reflects a lack of corroborating evidence available to physiotherapists.
Keywords: abdominal surgery, postoperative pulmonary complications, laparotomy, lung function
Introduction
Abdominal surgery is an umbrella term used to refer to surgical procedures undertaken in the abdominal area to diagnose and possibly treat a presenting medical problem.1 Different technique and medical procedures may be used depending on the abdominal organ involved and the type of condition being explored. Most of these procedures traditionally require opening the abdomen with a large incision and are referred to as open abdomen surgeries or laparotomies.1,2 Upper abdominal surgery was defined as any surgical procedure performed through an incision above or extending above the umbilicus. The recovery journey after upper abdominal surgery is often a multifaceted process that requires multi-practitioners input to be successful. Recovery remains a nebulous concept, lacking a clear definition among both health-care professionals and patients.2
Early postoperative days are associated with fatigue and limited respiratory movements.3 Pathophysiological changes post abdominal surgery cause respiratory muscle dysfunction due to altered muscle integrity, length-tension relationship, and thoracoabdominal mechanism, leading to postoperative pulmonary complications (PPCs).4 Respiratory muscle function and diaphragmatic movements are affected due to the anesthetic effect, site of the surgical incision reduced physical activity, and positional dependence.5 Surgical duration, anesthesia, and nociception impair respiratory function, exacerbate mucociliary clearance depression, and suppress the cough reflex leading to secretion retention and reduced lung volumes, thereby contributing to atelectasis and the development of infection.6
General anesthesia and peri-operative drugs affect breathing regulation by altering neural drive, further reducing functional residual capacity postoperatively and disrupting ventilation-perfusion ratio by decreasing pulmonary compliance, eventually causing hypoxemia and an increase in respiratory rate.3,7 Due to reflex inhibition of the phrenic nerve and nerve innervating abdominal muscles, surgical incisions near the diaphragm and abdominal muscles cause postoperative pain and limit respiratory movement.4 Similarly, the length of the incision has an additional effect on the development of PPC, as the peritoneal area near the abdominal viscera is severely affected as the length of the incision increases. As a result, open abdominal surgery has a higher rate of PPC development than laparoscopic surgery.7
The primary goal of physiotherapy is to facilitate recovery from surgery by preventing or treating postoperative complications and providing physical rehabilitation to aid in returning to premorbid physical function. While physiotherapy primarily focuses on physical rehabilitation, it may impact several other domains. Rehabilitation begins preoperatively and continues throughout the acute and subacute postoperative periods and may extend beyond hospital discharge into community-based or ambulatory care to assist with a return to normal activities of daily living and function.8
Chest physiotherapy includes deep breathing techniques, splinted active coughing, incentive spirometry (IS), inspiratory muscle training, and education regarding early mobilization. Practical training improves respiratory function preoperatively and benefits in improving lung expansion postoperatively than no intervention.9
There is no published consensus on the best assessment tool(s) to screen patients for the risk of PPC development and evaluate the efficacy of physiotherapeutic treatment after UAS. Similarly, there is currently no consensus on intervention effectiveness, with recent research unable to demonstrate that one physiotherapy technique is superior to another in preventing PPC.6 Several high-quality studies that have enhanced the efficacy of physiotherapy intervention for patients undergoing abdominal surgery have recently been published.10,11,18
Current postoperative UAS physiotherapy management within the United Arab Emirates (UAE) has not been documented. Therefore, the study aimed to establish current clinical physiotherapy assessment and management practice with patients undergoing upper abdominal surgery in UAE and whether this follows current best evidence recommendations.
Methods
Study Design
The current study adopted a novel anonymous online survey to explore the current practice among physiotherapists in the United Arab Emirates. The study also sought the consent of Patman et al6 to modify their original tool to reflect the healthcare landscape of the UAE.
Ethics Approval
This study was performed in accordance with the ethical standards of the Declaration of Helsinki. This study was approved by the Research Ethics Committee at the University of Sharjah (REC-20-05-13-04-S).
Research Tool and Piloting
A questionnaire was borrowed from Patman et al,6, a previous study with similar objectives completed in Australia. The questionnaire was modified slightly with the consent of the origin to produce the final version. The questionnaire had 51 questions cutting across 7 sections that investigated the assessment tools and interventions and explored current practice amongst physiotherapists treating patients following abdominal surgery in UAE hospitals. The questionnaire collected participants’ information, patient demographics, patient-physiotherapy factors for commencing treatment, prescription and dosage of interventions, mobility prescription following abdominal surgery (frequency, intensity, and duration of mobility prescription), and discharge planning. The questionnaire is generally close ended, incorporating a ranking system and matrix scale.
Survey Participants
Physiotherapists with a one-year Bachelor of Physiotherapy degree or higher who work or have worked in a licensed UAE hospital or health-care facility were eligible to participate in this study. Physiotherapists who were not treating patients following abdominal surgery were excluded from the survey.
Recruitment of Survey Participants
All hospitals identified as performing UAS in the UAE were identified via publicly accessible profiles. Hospitals were contacted to establish if UAS was performed and whether the facility provided a physiotherapy service to patients post-UAS. Phone calls were directed to the Physiotherapy Head of Department, who provided further contact details and email addresses of physiotherapists. An outline of the study’s objectives was discussed during the phone calls, emphasizing the necessity for physiotherapists treating patients undergoing UAS to be involved. Participants were encouraged to forward the email to other relevant clinicians, increasing the response rate via the snowball effect.
Sample Size
As this study was descriptive and did not test any hypotheses, no sample size calculations were undertaken. All hospitals performing UAS in the UAE were targeted and contacted with an invitation to the survey. Not all facilities performed UAS or had physiotherapists treating these patients, while others did not want to provide contact details due to security and confidentiality reasons. The study invited 100 physiotherapists from hospitals where UAS is performed across the UAE to participate in the survey. Of the 100, 42 physiotherapists were responded from whom the completed survey was distributed and retrieved via google forms—voluntarily opening and completing the survey implied consent.
Data Analysis
The data for the study were anonymously gathered from physiotherapists across the UAE using the Google Forms platform, and the survey responses were retrieved in MS Excel format. The data was then exported SPSS (version 240; IBM Corp, Armonk, New York, USA) for cleaning and analysis. Data categories and respective frequencies and proportions were tabulated and are reported as percentages and averages relative to the total response rate, symbolized as “n.” Averages were used to summarize the matrix-styled questions. A 5-point Likert scale with levels ranging from “never” to ‘always’ was predominantly used for ordinal-weighted responses. Quantitative analyses were performed to highlight patterns in responses to the survey's closed-ended questions. Rates of incidence or frequencies for quantitative responses were calculated and rationalized to total responses.
Results
The present survey was initiated in January 2021 and carried out till July 2021. The study invited 100 physiotherapists from hospitals where UAS is performed across the UAE to participate in the survey. Of the 100 invites sent, 73 were opened, providing a 73% consenting rate. There were seven failed deliveries, and among the 73 surveys that were opened, 42 were completed presenting a 42% response rate and 57.5% completion rate. The remainder 31 physiotherapists, despite opening the surveys, did not progress to respond to the survey questions. Figure 1 is a flowchart of participant recruitment and participation in the survey. The respondents did not need to complete all the questions in the survey, necessitating the use of only the valid sample for the question in the survey. The survey exhibited a slight variance in the Likert scale responses; hence, for better interpretation, responses with “never” and “rarely” were collapsed and reported together, as were “always” and “often.” Responses with “sometimes” were interpreted as such, resulting in three categories. The demographic characteristics of the respondents and an overview of the hospitals participating in the survey are shown in Table 1.
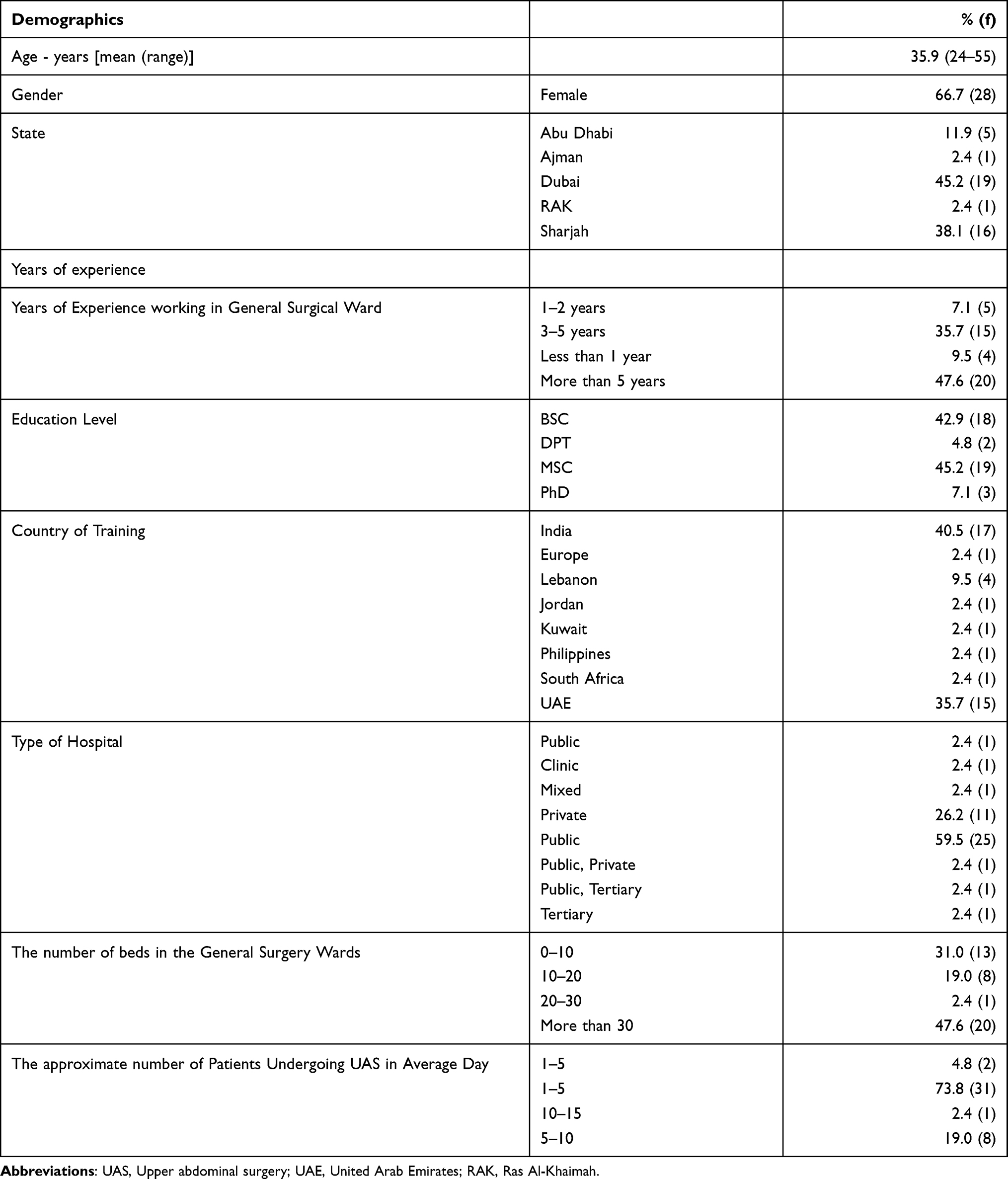 |
Table 1 Participant and Hospital Demographics |
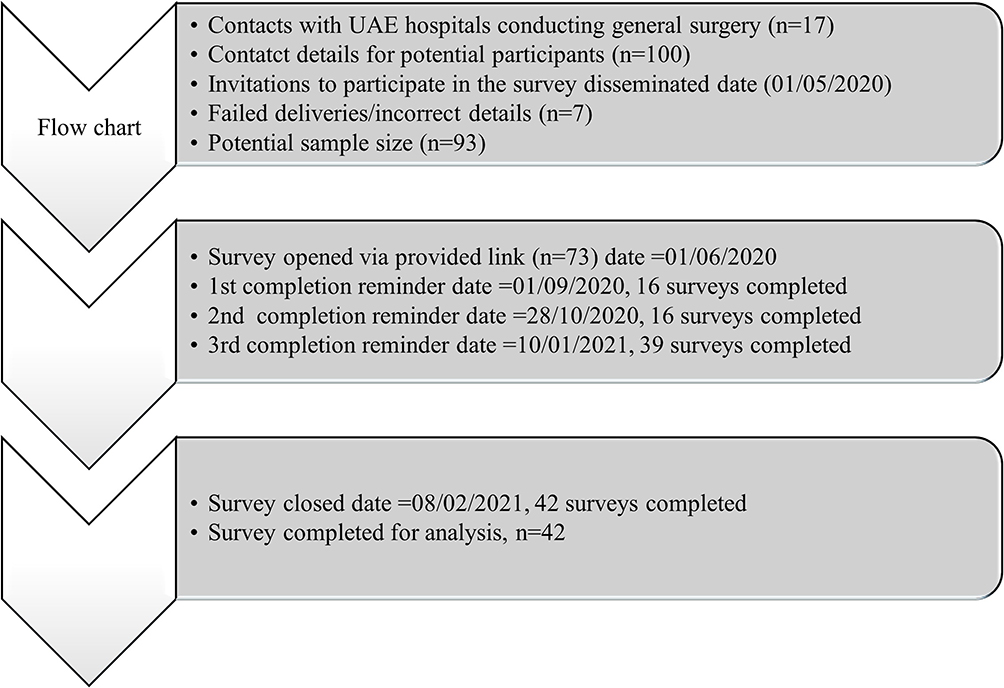 |
Figure 1 Flowchart of participants recruitment and participation in the survey. |
Screening of Patients for Pre-Existing and Postoperative Risk Factors Before Commencing Treatment
The survey enquired if patients in the UAE were screened or assessed before their UAS. The findings from the survey suggest that screening of patients before UAS by physiotherapists was not performed routinely. 26.2% of the respondents (n = 11/42) reported that this was “never” part of the procedure, with an additional 23.8% (n = 10/42) indicating that they “rarely” screened/assessed patients before undergoing UAS. As part of the survey where screening or assessment of patients as part of the physiotherapy intervention procedure, physiotherapists were asked to identify the frequently used parameters in identifying pre-existing risk factors that predispose the patients to an elevated risk of developing a PPC. Unlike in Australia, where, according to Patman et al (2017) “advanced age” and “smoking history” were both recognized by 98% (n = 54/55) of respondents, post-UAS physiotherapists in the UAE identified physician referral (69%, n=29/42), mobility status (73.8%, n=31/42), and fitness level or exercise tolerance (66.7%, n= 28/42) as the “always” and “often” used to screen patients before undergoing UAS. The findings of the study further revealed that patients’ past clinical experience (61.9%, n=26/42), smoking history (57.1%, n=24/42), and body mass index (BMI) (47.6%, n=20/42) were also prevalent factors for screening patients for PPC risk preoperatively. Among the least popular preoperative screening factors among physiotherapists in the UAE were the Melbourne Risk Prediction Tool (7.1%), American Association of Anaesthesiology (ASA) Score (7.1%), and National Surgical Quality Improvement Project (NSQIP) (9.5%).
Postoperatively, physiotherapist across the UAE most popularly use pain (high VAS) (85.7%, n=36/42), decreased saturation of oxygen (SpO2)’ (80.9%, n=34/42), and patient appearance (80.9%, n=34/42) as parameters to screen for high priority patients. Also, among the most commonly used parameters were high temperature (78.5%, n=33/42), amount of assistance required in mobilizing the patient (73.8%, n=31/42), high rate of perceived exertion (BORG) (66.7%, n=28/42), and raised respiratory rate (59.5%, n=25/42). However, respondents did not rate “sputum classification” (38.1%), high BORG (40.5%), anxiety level (33.3%), and increased ABGs (42.8%) as the commonly used postoperative screening tools among physiotherapists in the UAE.
Treatment
The survey required the physiotherapists to comment on what they concentrated on as primary goals or foci in managing patients in the consecutive days post-UAS. The study observed that most patients were not seen on day zero (day of surgery). On average, 47.6% (n = 20/42) of physiotherapists in general surgical wards treated their post-UAS patients once daily, starting on day one postoperatively. The primary of the majority of the physiotherapists on day one postoperatively was improved circulation (90.5%, n=38), improved exercise tolerance (85.7%, n=36), and allowing patients to be discharged from the hospital (78.6%, n=33). Also, a majority of the physiotherapists in the UAE aimed at preventing pneumonia and developing PPC (71.4%, n=30), improved airway clearance (71.4%), and increased lung volumes (71.5%, n=30). “Always” and “often,” 64.3%, 57.1%, and 64.3%, of the surveyed physiotherapists in the UAE would aim to normalize blood pressure, improve bladder and bowel function, and fulfill hospital protocols, respectively, in post-UAS patients on each consecutive days postoperatively. Physiotherapists’ expectations of patient milestones achieved each consecutive day post-UAS are given in Table 2.
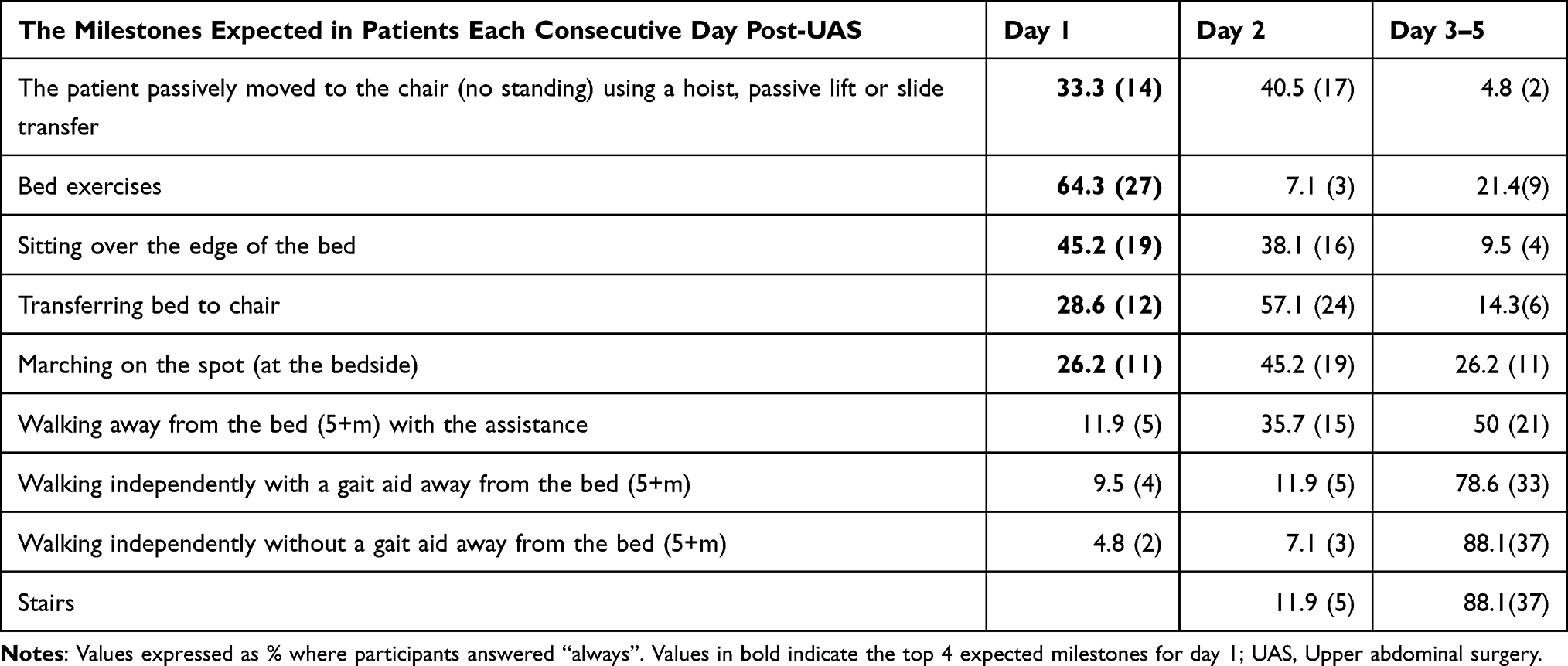 |
Table 2 Milestones Expected to Be Achieved Post-UAS |
Physiotherapists in the UAE almost universally prefer prescribing deep breathing exercises (thoracic expansion exercises, sustained maximal inspiration and pursed lip breathing) (64.3%, n=27/42), incentive Spirometry (IS) (64.3%, n=27/42), mobility from bedside (66.7%, n=28/42), and education (76.2%, n =32/42) as their primary intervention either “often” or “always” in the consecutive days post-UAS. Upper limb exercises (57.1%), ambulation or walking (52.4%), and upright sitting on the edge of the bed 57.1 (%) are also among the “always” or “often” used by above half of the surveyed physiotherapists (Table 3). Among the standard components of deep breathing exercises incorporated by physiotherapists postoperatively were inspiratory hold (66.7%), huff (less or with cough) (6.6%), incentive spirometry (73.8%), thoracic expansion exercises (71.4%), breathing control (71.4%), and positioning (76.2%) (Table 4).
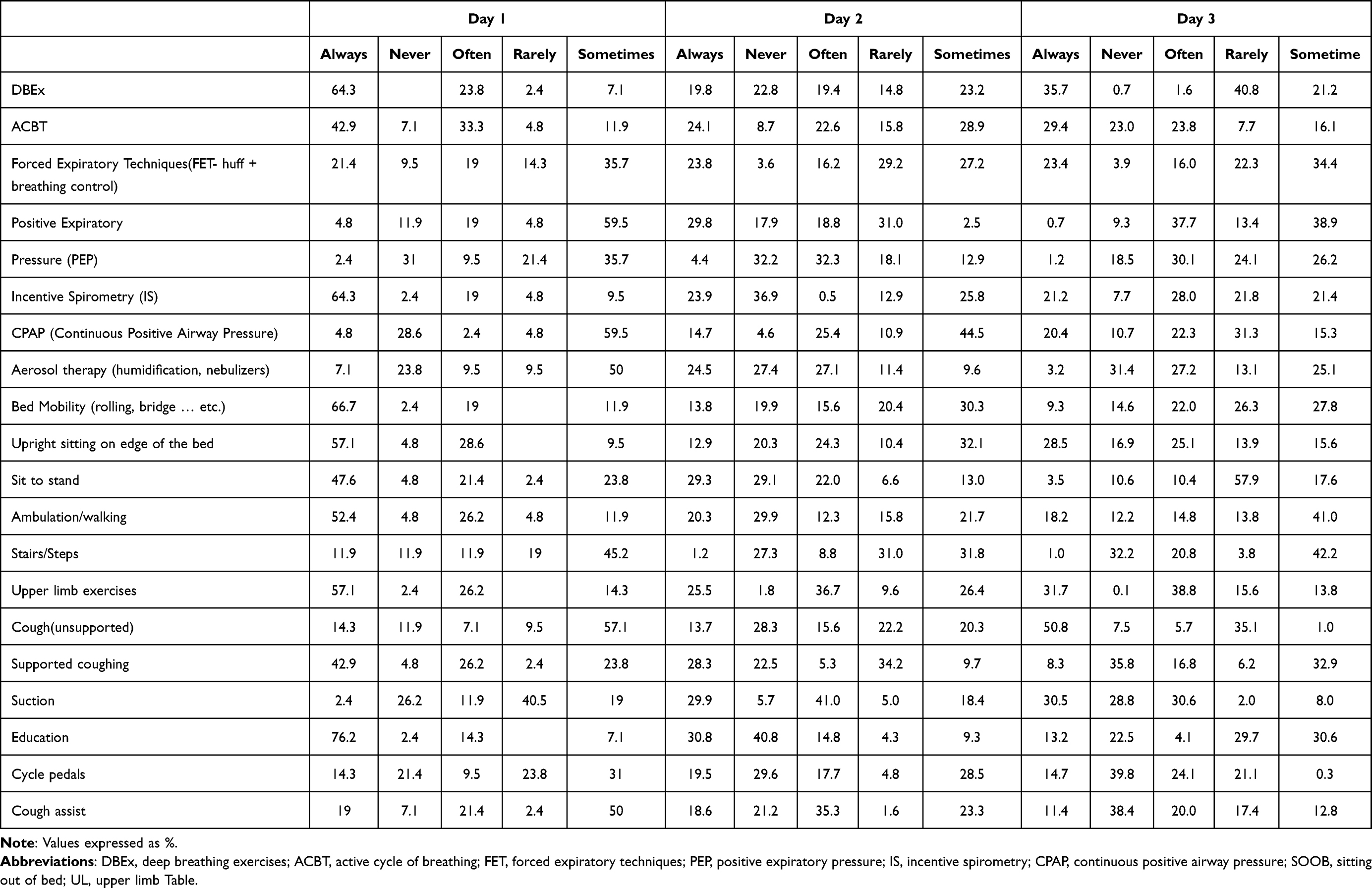 |
Table 3 Frequently Prescribed Interventions Over Consecutive Days Post-UAS |
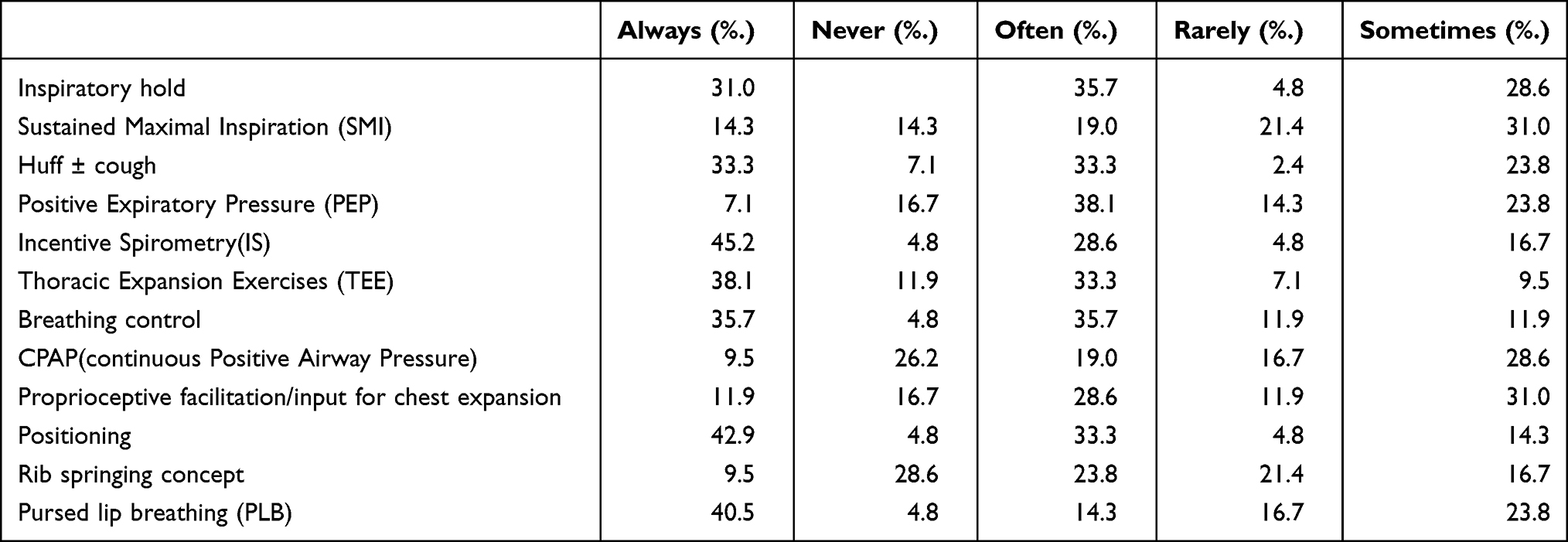 |
Table 4 Components of Breathing Exercises |
Outcome Measures
Physiotherapists in the UAE “always” and “often” use SpO2 (83.4%), progression of assistance required (76.2%), pain (VAS) (76.2%), and respiratory rate (71.5%) as the key outcome measures for monitoring the effectiveness of physiotherapy interventions, postoperatively. Also used “often” or “always” by over a half of the physiotherapists surveyed are blood pressure (59.6%), heart rate (54.8%), distance mobilized (64.3%), the readiness of discharge (61.9%), rate of perceived exertion (RPE) (52.3%), anxiety level (57.2%), and patient appearance (61.9%). Table 5 also shows that Clinical Pulmonary Infection Score (CPIS) (40.5%), ABGs (33.4%), chest x-ray (35.7%), and BORG score (33.3%) were among the minor popular measures used to monitor the effectiveness of physiotherapist interventions on post-UAS patients among practitioners in the UAE.
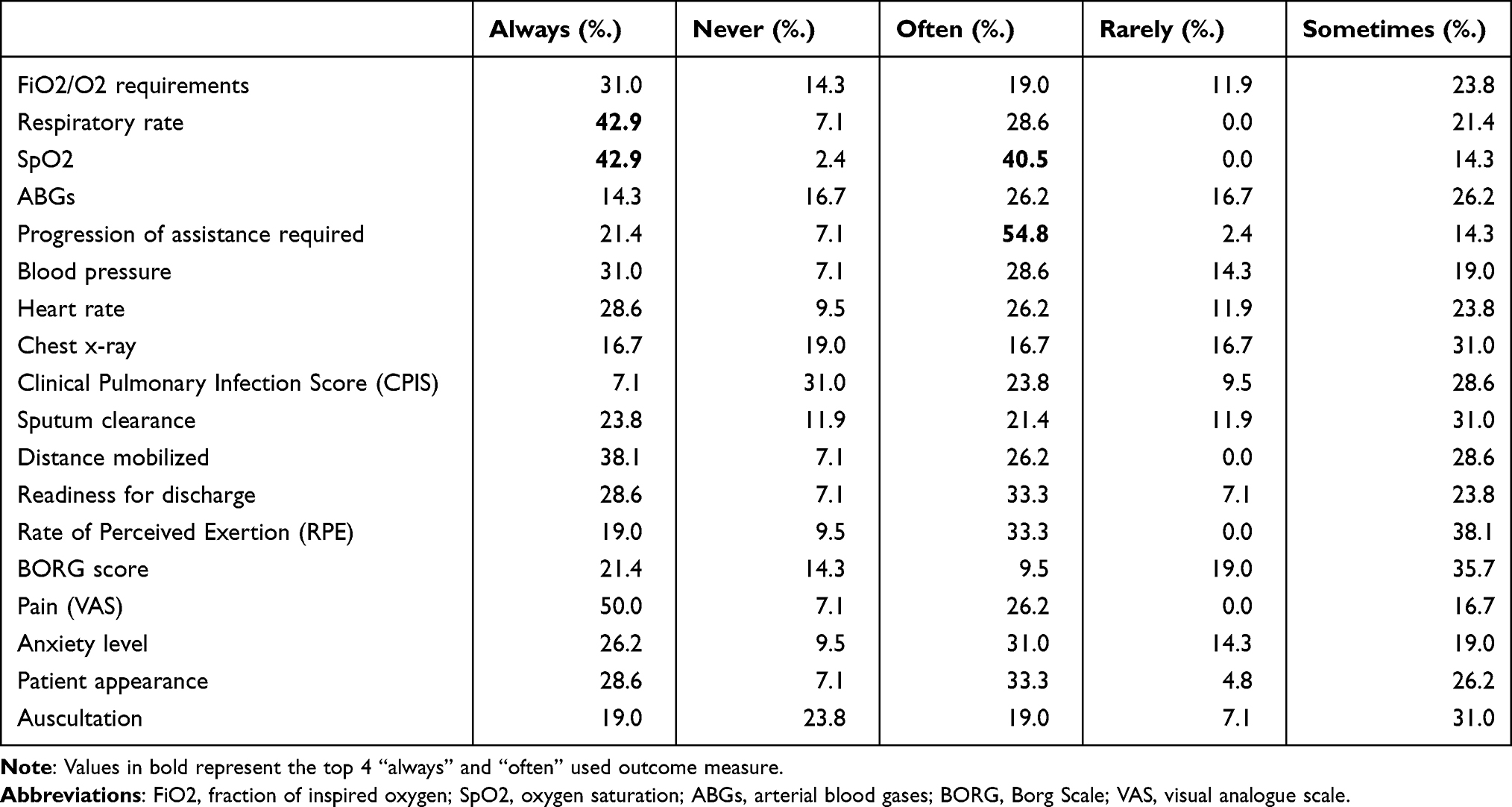 |
Table 5 Outcome Measures Used to Monitor the Effectiveness of Your Interventions |
Barriers to Treatment
As can be seen in Table 6, physiotherapists across the UAE identify pain (VAS) (64.3%), decreased SpO2 (66.7%), and fatigue (61.9%) as “always” and “often” the key barriers limiting the commencement of physiotherapy interventions postoperatively. In addition, the physio judgment of medical stability (52.4%) and blood pressure (52.4%) would also be among the factors leading to over half of the delayed physiotherapy interventions in post-UAS patients. The rarest of the factors contributing to delayed physiotherapy interventions include the number of attachments (catheter, Intravenous drip, O2 therapy) (40.5%), and VO2 max (38.1%), while BORG would sometimes cause significantly delayed treatment.
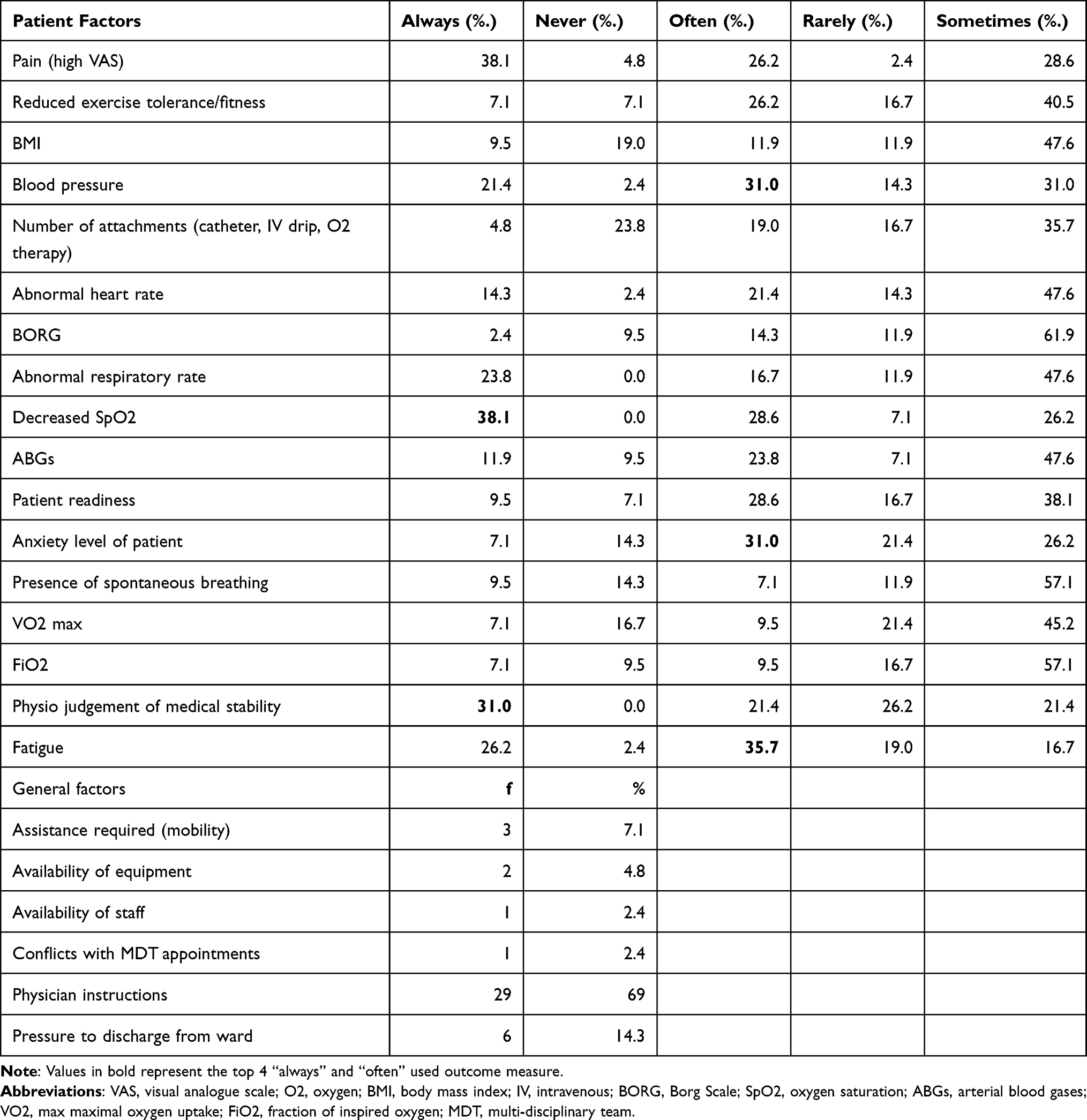 |
Table 6 Patient and General Factors Limiting the Commencement of Physiotherapy Interventions |
Factors that would “always” and “often” interfere with planned interventions, especially mobility, include pain (VAS) physician instructions (85.8%), respiratory rate (88.1%), SpO2 level (88.1%), blood pressure (83.3%), heart rate (83.3%), and mobility as well as the functional status of the patient (83.3%) postoperatively.
Discussion
This study aimed to look into the current physiotherapy management practices for post-UAS patients in the UAE. The survey revealed that physiotherapy interventions for patients undergoing UAS mostly begin postoperatively. In addition, the study noted that it is a common practice among physiotherapists in the UAE to screen patients for PPC exposure using various tools. After screening the patients, the survey also revealed that physiotherapy interventions in the UAE postoperatively included a combination of treatment procedures, amongst which the most popular are deep breathing exercises, bed mobility (rolling, bridge), upright sitting on the edge of the bed, ambulation/walking, and upper limb exercises education.
Screening Patients for Pre-Existing and Postoperative Risk Factors Before Commencing Treatment Pre-Existing Risk Factor Screening
This study observed that preoperative screening was not a routine practice among physiotherapists in the UAE. However, according to the recommendations from the earlier study,10 preoperative interventions such as patient screening and education for psychological preparedness have positively influenced patient outcomes post-UAS. In line with this argument, the findings from this study indicate that significant change in the UAE post-UAS physiotherapy landscape needs to be undertaken to ensure that post-UAS practice benefits from empirical evidence such as Boden et al10,11 concerning preoperative screening. Furthermore, according to Patman et al,6 improved access to patients before UAS increases opportunities for success in postoperative handling by physiotherapists. The authors also noted that empirical reports from the LIPSMAck POP had indicated that preoperative interventions could potentially influence patient treatment outcomes postoperatively.10 Screening of patients, both pre- and postoperatively, helps to identify patients with a high risk of developing a PPC post-UAS. Hence, physiotherapists are better positioned to prioritize their time and resources objectively and with optimal anti-PPC outcomes.
Even with the lack of sufficient preoperative screening for patients in the UAE, physiotherapists across the UAE are assessing/screening patients early postoperatively to determine their level of exposure to the risk of developing a PPC post-UAS. In hospitals where UAS is done in the UAE, this study observed that physiotherapists use a range of dimensions to screen patients for risk of developing a PPC. Among the most assessed parameters are physician referral, smoking history, past clinical experience, mobility status, fitness level/exercise tolerance, with the patient’s mobility status currently being the most screened parameter. These parameters align with those described in a majority of the literature on the handling of patients postoperatively, including Barradell et al.12 Boden et al.10 Fennelly et al.13 Haines et al.14 Lockstone et al15 and Yang et al16 suggest that screening patients based on these parameters help physiotherapists to identify high-priority patients for physiotherapy interventions and possibly avert the danger and cost of developing a PPC. Application of these parameters in the UAE in postoperative physiotherapy practice post-UAS is an indication that physiotherapists in the UAE are accommodating empirical evidence in their current practice. This is important in assisting the physiotherapist in the UAE to allocate and target the patients at high risk of developing a PPC and those that are more likely to benefit from physiotherapy treatment postoperatively.
This study, similar to Patman et al,6 observed risk factors exceeding a score of greater than 2 using the ASA scoring system. Even as such, the findings of this study indicate that the use of the ASA scoring system for screening patients is not routinely done by physiotherapists across the UAE, with only a combined 7.1% of the physiotherapist in the UAE using it to screen patients post-UAS. This could indicate that physiotherapists in the UAE lack awareness of the ASA scoring system as a valuable tool for rating PPC risk exposure, or perhaps, physiotherapists do not regard it as necessary to their practice. On the other hand, it could also indicate that physiotherapists do not consider the ASA scoring system as a well-evidenced and validated screening tool for PPC risk or see it as irrelevant in their physiotherapy practice.
Postoperative Assessment for PPC Risk Factors
Postoperative physiotherapy has undergone tremendous transformations over the years. Diagnostic tools such as ASA and Melbourne Risk Prediction Tool (MRT) have been developed and are very useful to physiotherapists in pinpointing the indicators that elevate the risk of developing a PPC among patients postoperatively.17 Physiotherapists in the UAE did not list high BORG, sputum classification, increased FIO2, ausculation, and anxiety level as frequently used tools even with the extensive recommendation in the literature on their usefulness in identifying risk factors postoperatively. Instead, the physiotherapists responding to the survey rely heavily on pain (high VAS), decreased saturation of oxygen (SpO2), and patient appearance as parameters to screen for high-priority patients postoperatively. Also, among the most commonly used parameters were the high-temperature amount of assistance required in mobilizing the patient, high rate of perceived exertion (RPE), and raised respiratory rate.
It is evident from the above results that physiotherapists in the UAE rely on various tools to pinpoint the risk of developing a PPC in post-UAS cohorts. However, there is no evidence of a consensual schema for choosing screening tools among physiotherapists in the UAE. The disparity in the preference accorded to the existing screening tools by physiotherapists across the UAE calls for researchers and practitioners to harmonize physiotherapy practice in the UAE and globally by developing a consensual procedure for screening patients for PPC risks post-UAS. According to Hanekom et al,18 when physiotherapists consensus about post-UAS screening and PPC diagnostic procedures, they can improve efficiency and reduce the PPC incident rate post UAS.
Respiratory Physiotherapy
The study also found that respiratory physiotherapy is one of the most frequently recommended postoperative interventions by physiotherapists in the UAE. Because of the limited research efforts in this area, the available scientific knowledge about the efficacy of respiratory physiotherapy in post-UAS cohorts is essentially inconclusive.18
Physiotherapists in the UAE appear to recognize that post-UAS cohorts are a high-risk population. As a result, it is logical to pursue any benefit of reduced PPC exposure, including the current poorly evidenced prophylactic interventions.19 This makes utmost sense, especially where the pain and cost of PPCs to the health-care systems and individual patients are overwhelming. However, the efficacy of these procedures should be researched thoroughly, not leaving out their cost-benefit analyses. The study noted that physiotherapists in the UAE are almost universally preferred to prescribe deep breathing exercises in conjunction with mobility from the bedside.20 In addition, a majority of the physiotherapists in the UAE indicated the aim to pursue chest treatment on day postoperatively routinely, and almost universally, physiotherapists in the UAE would use deep breathing exercises alongside supported cough. The study’s findings also indicate that positioning and thoracic expansion exercises are also preferred interventions, with over 75% of physiotherapists in the UAE reporting to use them postoperatively. However, earlier study7 notes that these recommendations are entirely based on medical experience even as the contextual literature remains unsatisfying. Other studies have found that mobilization, when used together with chest therapy, effectively reduces the incidence rate of developing a PPC, with a 100% effectiveness in averting atelectasis among patients after undergoing UAS.7,8 Nonetheless, continued research effort is needed to corroborate this suggestion that currently appears widely accepted among physiotherapists in the UAE.
Despite contradictory evidence, clinical experience may be the primary motivator for physiotherapists to continue using chest treatment as a standard practice rather than as required. Although clinical experience is not always untrustworthy, it should be recognized as a potential factor in resistance to change and should be combined with evidence from high-quality studies to promote best practices for UAS patients.
Previous studies21,22 have stated the role of standard chest treatment interventions and translation of evidence from past post-UAS experiences. This would help physiotherapists embrace and consistently implement post-UAS treatment interventions that are empirically viable and most viable in averting PPC risks. It would also be an opportunity to put existing post-UAS physiotherapy resources such as ASA and Melbourne risk prediction in proper use. However, overall the study’s finding did show instances where physiotherapists in the UAE rely on respiratory solely; instead, they would use it alongside assisted early ambulation if the condition of the post-UAS patients allowed.
Mobilization Interventions
Studies have consistently shown that mobilization is an effective therapy for a patient’s recovery post-UAS.11 Early mobilization, both assisted and unassisted, is an effective physiotherapy intervention for patients after undergoing UAS.23,24 The study results indicate that among the milestones “always” and “often” expected by physiotherapist in the UAE are aligned to conventional mobilization goals such as improving circulation, fulfilling hospital protocols, and allowing patient to be discharged as achieving improved exercise tolerance.25,26 On day one postoperatively, where conditions permitted, physiotherapists in the UAE mobilized their patients away from bedside by bridging or rolling, among other strategies. This aligns with physiotherapists’ expectations and primary goals for interventions post-UAS that following day one, post-UAS cohorts should be mobilized, with or without assistance, away from the bedside. This expectation and physiotherapy practice in the UAE conform to the literature that mobilizing patients after undergoing UAS is an effective intervention for reducing PPC risks. As such, the findings demonstrate that physiotherapists in the UAE are aware of treatments recommended in the UAS literature and are translating them into practice by mobilizing patients away from the bedside postoperatively.
Stair climbing was an expected milestone among 88.1% of the UAE’s physiotherapists in three to five days postoperatively. On the contrary, only 22.8% would “always” and “often” consider it a preferred intervention postoperatively. Also, among the least popular interventions used by physiotherapists in the UAE were positive expiratory pressure (PEP), CPAP (continuous positive airway pressure), aerosol therapy (humidification, nebulizers), and suction. Overall, the findings of this study suggest that mobility from the bedside is the “always” and “often” preferred mobilization as the primary focus of physiotherapy interventions post-UAS.
Barriers to Treatment
This study found that physiotherapists across the UAE identify Pain (VAS), decreased SpO2, and fatigue as “always” and “often” the critical barriers to commencement of physiotherapy interventions postoperatively. This highlights some similarities of the UAE and Australian post-UAS physiotherapy landscape. Patman et al6 noted that physiotherapists handling post-UAS cohorts in Australia also site pain as the most prominent barrier to commencement of physiotherapy interventions post-UAS. In addition, the physio judgment of medical stability and blood pressure would also be among the factors leading to over half of the delayed physiotherapy interventions in post-UAS patients. The rarest of the factors contributing to delayed physiotherapy interventions include the number of attachments (catheter, IV drip, O2 therapy), and VO2 max, while BORG would sometimes cause significantly delayed treatment. This study did not primarily focus on the barriers to physiotherapy treatment in the UAE. As a result, the study did not entrench whether the identified barriers affect the efficacy with which physiotherapists in the UAE deliver interventions post-UAS. However, the findings indicate a potential study area, focusing on the impact of some of these barriers on the effectiveness of physiotherapy interventions and the strategies adopted by physiotherapists dealing with post-UAS cohorts.
Research Limitations
The surveyed physiotherapists may have interpreted the questions differently from what was intended. However, while not overlooking this possibility, it is hoped that piloting efforts improved the face validity of the survey tool, and instances of misinterpretation should be minimal. It was not mandatory for the physiotherapist taking part in the survey to respond to all questions to proceed through the survey. This is among the reasons the study recorded varied response rates per question. This limitation was overcome in the analysis by considering only the valid sample per question. The other major limitation is response rate in the present study which is quite poor at <50%, and then the completion rate further still with only just over half of respondents completing the survey.
Recommendations for Future Studies
Despite these limitations, this study was instrumental in identifying critical areas for improvement in future studies and the general physiotherapy landscape in the UAE. More research is needed to develop a consensual screening procedure postoperatively following UAS. This study observed that preoperative screening was not a routine practice among physiotherapists in the UAE. According to the recommendations of Boden et al,10 preoperative interventions such as patient screening and education for psychological preparedness have been shown to influence patient outcomes post-UAS positively. In line with this argument, the finding from this study indicates that significant change in the UAE post-UAS physiotherapy landscape needs to be undertaken to ensure that post-UAS practice benefits from empirical evidence. This study did not primarily focus on the barriers to physiotherapy treatment in the UAE. As a result, the study did not entrench into the possible effects of the identified barriers on the efficacy with which physiotherapists in the UAE deliver interventions post-UAS. However, the findings indicate a potential study area, focusing on the impact of some of these barriers on the effectiveness of physiotherapy interventions and the strategies adopted by physiotherapists while dealing with post-UAS cohorts.
Conclusion
The interventions currently implemented by physiotherapists for patients post-UAS are reflective of the guidelines from the literature. Evidence from recent research efforts validates the use of assisted early mobilization as a standalone treatment but is not yet reflected in current practice among physiotherapists caring for post-UAS cohorts in the UAE. The variability of screening tools used amongst clinicians to identify high-risk patients postoperatively was reflective of the low amount of validated evidence available to physiotherapists. In combination with future research, an agreement amongst physiotherapists is needed to come up with a standard framework for choice of screening tools and physiotherapy interventions to assist practitioners with prioritizing suitably the patients following UAS depending on the presenting level of risk of developing a PPC to ensure physiotherapy treatment time and resources are allocated and utilized efficiently for optimum treatment outcomes.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest for this work and declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Sullivan K, Reeve J, Boden I, Lane R. Physiotherapy following emergency abdominal surgery. Actual Problems Emergency Abdominal Surgery. 2016;1:109.
2. Reeve JC, Boden I. The physiotherapy management of patients undergoing abdominal surgery. N Zealand J Physiotherapy. 2016;44(1):254. doi:10.15619/NZJP/44.1.05
3. Soares SM, Nucci LB, da Silva MM, Campacci TC. Pulmonary function and physical performance outcomes with preoperative physical therapy in upper abdominal surgery: a randomized controlled trial. Clin Rehabil. 2013;27(7):616–627. doi:10.1177/0269215512471063
4. Casali CC, Pereira AP, Martinez JA, de Souza HC, Gastaldi AC. Effects of inspiratory muscle training on muscular and pulmonary function after bariatric surgery in obese patients. Obes Surg. 2011;21(9):1389–1394. doi:10.1007/s11695-010-0349-y
5. Dronkers J, Veldman A, Hoberg E, Van Der Waal C, Van Meeteren N. Prevention of pulmonary complications after upper abdominal surgery by preoperative intensive inspiratory muscle training: a randomized controlled pilot study. Clin Rehabil. 2008;22(2):134–142. doi:10.1177/0269215507081574
6. Patman S, Bartley A, Ferraz A, Bunting C. Physiotherapy in upper abdominal surgery–what is current practice in Australia? Arch Physiotherapy. 2017;7(1):1. doi:10.1186/s40945-017-0039-3
7. Canet J, Gallart L, Gomar C, et al.; ARISCAT group. Prediction of postoperative pulmonary complications in a population-based surgical cohort. J Am Soc Anesthesiologists. 2010;113(6):1338–1350.
8. Reeve J, Anderson L, Raslan Y, Grieve C, Ford J, Wilson L. The physiotherapy management of patients undergoing abdominal surgery: a survey of current practice. N Zealand J Physiotherapy. 2019;47(2):88. doi:10.15619/NZJP/47.2.02
9. Kumar AS, Alaparthi GK, Augustine AJ, Pazhyaottayil ZC, Ramakrishna A, Krishnakumar SK. Comparison of flow and volume incentive spirometry on pulmonary function and exercise tolerance in open abdominal surgery: a randomized clinical trial. J Clin Diagnostic Res. 2016;10(1):KC01.
10. Boden I, Browning L, Skinner EH, et al. LIPPSMAck POP (lung infection prevention post surgery-major abdominal-with preoperative physiotherapy) trial: study protocol for a multi-centre randomised controlled trial. Trials. 2015;16(1):1–5. doi:10.1186/s13063-015-1090-6
11. Boden I, Skinner EH, Browning L, et al. Preoperative physiotherapy for the prevention of respiratory complications after upper abdominal surgery: pragmatic, double blinded, multicentre randomised controlled trial. BMJ. 2018;360.
12. Barradell S, Peseta T, Barrie S. ‘There’s so much to it’: the ways physiotherapy students and recent graduates experience practice. Adv Health Sci Educ. 2018;23(2):387–406. doi:10.1007/s10459-017-9804-z
13. Fennelly O, Blake C, FitzGerald O, et al. Advanced musculoskeletal physiotherapy practice: the patient journey and experience. Musculoskeletal Sci Practice. 2020;45:102077. doi:10.1016/j.msksp.2019.102077
14. Haines KJ, Skinner EH, Berney S. Austin Health POST Study Investigators. Association of postoperative pulmonary complications with delayed mobilisation following major abdominal surgery: an observational cohort study. Physiotherapy. 2013;99(2):119–125. doi:10.1016/j.physio.2012.05.013
15. Lockstone J, Parry SM, Denehy L, et al. Physiotherapist administered, non-invasive ventilation to reduce postoperative pulmonary complications in high-risk patients following elective upper abdominal surgery; a before-and-after cohort implementation study. Physiotherapy. 2020;106:77–86. doi:10.1016/j.physio.2018.12.003
16. Yang CK, Teng A, Lee DY, Rose K. Pulmonary complications after major abdominal surgery: National Surgical Quality Improvement Program analysis. J Surgical Res. 2015;198(2):441–449. doi:10.1016/j.jss.2015.03.028
17. Scholes RL, Browning L, Sztendur EM, Denehy L. Duration of anaesthesia, type of surgery, respiratory co-morbidity, predicted VO2max and smoking predict postoperative pulmonary complications after upper abdominal surgery: an observational study. Australian J Physiotherapy. 2009;55(3):191–198. doi:10.1016/S0004-9514(09)70081-9
18. Hanekom SD, Brooks D, Denehy L, et al. Reaching consensus on the physiotherapeutic management of patients following upper abdominal surgery: a pragmatic approach to interpret equivocal evidence. BMC Med Inform Decis Mak. 2012;12(1):1–9. doi:10.1186/1472-6947-12-5
19. Kokotovic D, Berkfors A, Gögenur I, Ekeloef S, Burcharth J. The effect of postoperative respiratory and mobilization interventions on postoperative complications following abdominal surgery: a systematic review and meta-analysis. Eur J Trauma Emergency Surgery. 2020;2:1–6.
20. Mans CM, Reeve JC, Elkins MR. Postoperative outcomes following preoperative inspiratory muscle training in patients undergoing cardiothoracic or upper abdominal surgery: a systematic review and meta analysis. Clin Rehabil. 2015;29(5):426–438. doi:10.1177/0269215514545350
21. Cook DJ, Thompson JE, Prinsen SK, Dearani JA, Deschamps C. Functional recovery in the elderly after major surgery: assessment of mobility recovery using wireless technology. Ann Thorac Surg. 2013;96(3):1057–1061. doi:10.1016/j.athoracsur.2013.05.092
22. Dorcaratto D, Grande L, Pera M. Enhanced recovery in gastrointestinal surgery: upper gastrointestinal surgery. Dig Surg. 2013;30(1):70–78. doi:10.1159/000350701
23. Silva YR, Li SK, Rickard MJ. Does the addition of deep breathing exercises to physiotherapy-directed early mobilisation alter patient outcomes following high-risk open upper abdominal surgery? Cluster randomised controlled trial. Physiotherapy. 2013;99(3):187–193. doi:10.1016/j.physio.2012.09.006
24. Grams ST, Ono LM, Noronha MA, Schivinski CI, Paulin E. Breathing exercises in upper abdominal surgery: a systematic review and meta-analysis. Br J Physical Therapy. 2012;16:345–353. doi:10.1590/S1413-35552012005000052
25. Boden I, Robertson IK, Neil A, et al. Preoperative physiotherapy is cost-effective for preventing pulmonary complications after major abdominal surgery: a health economic analysis of a multicentre randomised trial. J Physiother. 2020;66(3):180–187. doi:10.1016/j.jphys.2020.06.005
26. Boden I, Peng C, Lockstone J, et al. Validity and utility testing of a criteria-led discharge checklist to determine post-operative recovery after abdominal surgery: an international multicentre prospective cohort trial. World J Surg. 2021;45(3):719–729. doi:10.1007/s00268-020-05873-9
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.