Back to Journals » Risk Management and Healthcare Policy » Volume 16
Physiotherapists’ Understanding of Shortwave Diathermy Contraindications: A Questionnaire Survey
Authors Almalty AR ![]() , Abdelnour HM
, Abdelnour HM ![]() , Hawamdeh M
, Hawamdeh M ![]() , Alkhob SA
, Alkhob SA
Received 25 March 2023
Accepted for publication 16 June 2023
Published 26 June 2023 Volume 2023:16 Pages 1171—1185
DOI https://doi.org/10.2147/RMHP.S413806
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mecit Can Emre Simsekler
Abdulmajeed R Almalty,1,2 Hassan M Abdelnour,2 Mohannad Hawamdeh,1 Shadi A Alkhob2
1Department of Physical and Occupational Therapy, College of Allied Health Sciences, The Hashemite University, Zarqa, Jordan; 2Physical Therapy Department, College of Allied Health Sciences, Jerash University, Jerash, Jordan
Correspondence: Abdulmajeed R Almalty, Department of Physical and Occupational Therapy, The Hashemite University, Zarqa, 13133, Jordan, Tel +962-7-97366912, Email [email protected]
Purpose: It is known that electromagnetic fields and heat generated by shortwave diathermy (SWD) can have adverse effects on living tissue. The purpose of this research is to evaluate Jordanian physiotherapists’ knowledge of pulsed and continuous SWD contraindications. And investigate the potential contraindications about which Jordanian physiotherapists may have limited knowledge.
Subjects and Methods: This cross-sectional study investigates Jordanian physiotherapists’ knowledge of SWD contraindications. In 38 private and public hospitals, a self-administered questionnaire survey was carried out. Participants were asked to classify 32 conditions as “always, sometime, or never” contraindicated or “I do not know”. Participants are physiotherapists with two or more years of postgraduate experience. Two forms comprised the survey. The first consisted of assessing their reaction to the contraindications of pulsed shortwave diathermy (PSWD), while the second consisted of continuous shortwave diathermy (CSWD).
Results: Approximately 270 physiotherapists were eligible to participate in this investigation. Only 150 questionnaires were distributed to the therapists who agreed to the study. One hundred twenty-eight were returned for an average response rate of 85.3% (128/150). Respondents had good agreement about using SWD for cardiovascular condition, however, 24 respondents (19%) thought PSWD can be used over venous thrombosis. Only 64% of the respondents was aware that pacemakers are contraindicated for PSWD. Approximately 14% to 32% seem unaware that tuberculosis and osteomyelitis are contraindicated for both CSWD and PSWD. About 21% to 28% have been unaware that the use of PSWD is contraindicated for specialized tissues (eg, eyes, gonads, or malignant tissues) and 29% during pregnancy.
Conclusion: Jordanian physiotherapists generally agreed on the widely acknowledged contraindications of CSWD for specific conditions. However, there was considerable uncertainty among Jordanian physical therapists about the contraindications of PSWD. This discrepancy highlights the need to improve physiotherapist awareness and for more fact-based research to the contraindication of SWD modality.
Keywords: diathermy, electrotherapy, electromagnetic, deep heat
Introduction
Shortwave diathermy (SWD) is one of the agents used in physical therapy. It generates high-frequency electromagnetic energy that has physiological and therapeutic effects on biological tissues.1 SWD can promote vasodilation and tissue healing, decrease inflammation, decrease pain, increase tissue extensibility, decrease muscle spasm and spasticity, reduce swelling, decrease joint stiffness, and control infection.2–8 Like other physical therapy treatments, shortwave is used as a multimodal intervention under specific conditions with the same precautions and contraindications. Furthermore, the improper use of therapeutic SWD can expose patients, physiotherapists, and even bystanders to adverse effects. By turning electromagnetic energy into heat when it enters deep tissues, the SWD elevates tissue temperature, which might be hazardous if not treated correctly. Burns, rashes, increased discomfort, nausea, and fainting are among the potential side effects of SWD treatment,9 even death has been reported as result of mal application of SWD.10
Unfortunately, most of these contraindications were based on expert opinion rather than the findings of scientific studies. Some of these contraindications cannot be studied in humans due to legal or ethical considerations. As a result, a few studies have been conducted to investigate contraindications to SWD in humans.1,3 For example, some researchers were able to examine the dangers of SWD use during pregnancy. The occupational use of microwaves and SWD by physical therapists during conception was evaluated. They found that SWD was associated with an increased incidence of miscarriage and low birth weight.11–13 Other researchers investigated the application of pulsed shortwave diathermy (PSWD) to patients with a metal implant in the treatment field. It has been found to be effective in patients with ankle fractures and internal fixation. It helped them to recover their range of motion without discomfort, pain, or burning during or after treatment.14 However, there is a long list of contraindications that were not investigated. Thus, it is important to exercise caution when using SWD on individuals with certain medical conditions, particularly on tissues that are already compromised. For instance, individuals with cancer, hemorrhage, blood clots, ischemia, or other conditions may be at risk of further damage from exposure to electromagnetic field yielded by SWD. While there is a lack of scientific research to support all these contraindications, it is generally recommended to err on the side of caution and avoid using SWD in these cases. Ultimately, it is crucial for therapists to prioritize patient safety and individual needs when incorporating SWD into their treatment plans. This necessitate the establishment of national protection standards and guidelines for the use of SWD in medical practice which has been achieved in many developed countries.15,16
The professional guidelines for the use of therapeutic diathermy have been studied to the extent of their application. Shah and Farrow visited 46 physiotherapy departments in England and reported good practices and procedures regarding therapeutic diathermy devices.15 Furthermore, they found that most therapists preferred to use PSWD more than continuous shortwave diathermy (CSWD), which could be due to health and safety concerns or a lack of affirmative knowledge of the contraindications of SWD.15 And for the same reason, the SWD apparatus was widely available in Australian hospitals; however, few facilities used it daily with patients, according to researchers.16 In Jordan, therapeutic diathermy is commonly used in physiotherapy practice, but there are concerns about the lack of standardized protocols and guidelines in healthcare system. This has led to variations in the use of diathermy among different therapists and clinics. Therefore, it’s important to examine the therapist’s understanding of SWD contraindications and the evidence of good practices and procedures for using SWD.
A survey was conducted in Ireland to determine the agreement among physical therapists on the contraindications for continuous and pulsed SWD. The survey showed that CSWD had a higher level of agreement than PSWD.17 As with the Irish study, the purpose of this study is to assess the knowledge of pulsed and continuous SWD contraindications among Jordanian physiotherapists. And investigate the potential contraindications about which Jordanian physiotherapists may have limited knowledge. Furthermore, to compare the knowledge of SWD contraindications between Jordanian and Irish physiotherapists in a general sense. The same survey questionnaire was distributed to physiotherapists in both private and public hospitals in Jordan.
Materials and Methods
The authors of “Contraindications to Shortwave Diathermy: Survey of Irish Physiotherapists”, Shields et al authorized the use of the same questionnaires in this study via email. The questionnaire was written in English and was validated by the authors.17 The participants received the same questionnaire without modifications or Arabic translation. Since English is Jordan’s second language, all physical therapy programs are taught in English. In three hospitals, a pilot study was carried out to test the barrier language with nine physiotherapists who were not part of the study. Four were interviewed, and five were asked to complete the form attached to the questionnaire. All physical therapists agreed that the questionnaire was written in simple, easy-to-understand medical terminology. The study protocols and the consent form were approved by the Hashemite University’s Institutional Review Board.
Subjects
According to the Jordanian Ministry of Health, there are 116 public and private hospitals in Jordan.18 The Middle or Capital Region had the most hospitals in the country, accounting for 74 (63.8%) of all hospitals. The Northern and Southern regions followed with 29 (25.0%) and 13 (11.2%), respectively. After contacting the physical therapy departments of these hospitals, we found that 45 (28 public, 17 private) of them use SWD equipment that operates in continuous and pulsed modes. There are 28 physical therapy departments in the Middle Region, 12 in the North Region, and 5 in the South Region. The supervisors of these departments were then contacted to explain the purpose of the study and request their participation. Only 38 physical therapy departments agreed to participate in the study: 26 in the middle region, 10 in the northern part, and 2 in the southern part. Participants must have a Bachelor of Science (BSc), two years of post-graduation experience, and apply SWD in their therapy as a physiotherapist. A total of 270 physiotherapists were estimated to be eligible to participate in this study across all hospitals. At a confidence level of 95% (p<0.05) at a margin error 5% (0.05), a sample size of 159 was calculated to be representative. However, only 150 physiotherapists agreed to take part in this study, and each was given a copy of the questionnaire and consent form. Prior to participating in this study, a subject must sign a consent form.
Procedures
A hand-delivery envelope containing several questionnaires copies proportional to the number of physiotherapists in the department of interest was prepared. The department head distributed the copies to the therapists after receiving the envelope. In the northern region, the distance between the study site and the most distant hospitals of interest was roughly one hour by car, whereas in the southern region, it was two hours. We requested that the supervisor keep the envelope in a location accessible to all physiotherapists. After completing the questionnaires, the therapists were instructed to return them directly to the envelope without handing them over to anyone else. This was done to protect the confidentiality of the questionnaire from anyone other than researchers. After the therapists in each department had completed the questionnaire, the questionnaires were collected later that day, the following day, or a few days later, depending on the follow-up call with the physical therapy supervisor.
Participants were requested to provide their age, years of experience, seniority, preferred SWD mode, and frequency of use. In addition, each participant was asked to designate whether 32 medical conditions, such as “always”, “sometimes”, “never”, and “not knowing”, were contraindicated on two identical forms of the questionnaire. The first form is for CSWD contraindications, and the second form is for PSWD contraindications. The possible impact of each choice was explained to the participants. Always contraindicated means that SWD is never applicable. Sometimes contraindicated indicates that SWD can be applied, for example, to other parts of the body or under certain circumstances. A participant must provide more details when choosing this option. Never contraindicated indicates that SWD can be applied directly or indirectly to other parts of the body in the presence of the proposed condition. The answer “I do not know” indicated the uncertainty as to whether SWD is applicable to the proposed conditions or not. Along with the suggested conditions, each question has a short blank space for participants to add additional information.
Statistical Analysis
Data were analyzed using the Windows version of the Social Science Statistics Package (version 23.0, SPSS Inc., New York, USA). Each condition with an “always”, “sometimes”, “never”, or “do not know” contraindication was coded and analyzed. The frequency was calculated for all the “respondents” answers to each question. The descriptive statistics for each question were then calculated and expressed as percentages in the results section. Cochran’s formula was used to calculate the sample size.
Results
With 128 out of 150 questionnaires returned, the average response rate was 85.3% (Table 1). Very few questions on the CSWD or PSWD questionnaires were left unanswered by the participants. In our statistical analysis we coded these questions as “do not know”. Most respondents to the “sometimes” option clearly indicated that the SWD can be used on other body parts, but not directly on the proposed condition.
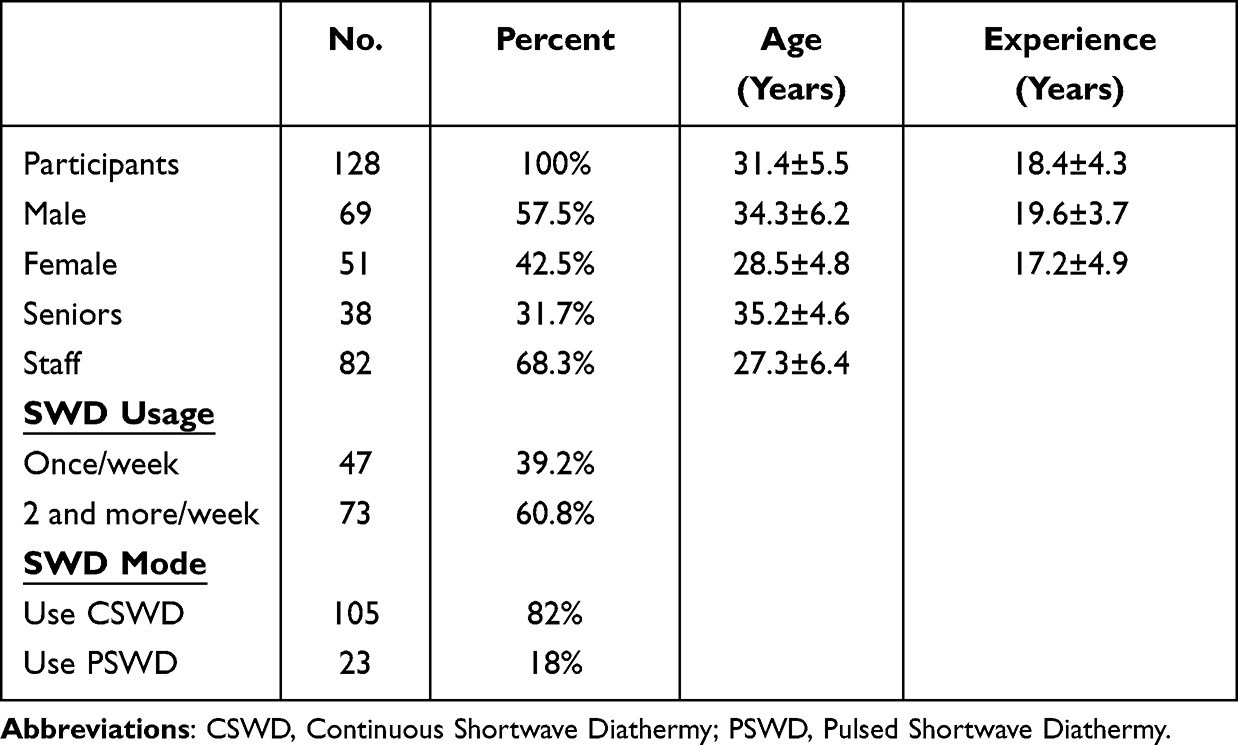 |
Table 1 Demographical Data of Participants and Shortwave Diathermy Usage |
Artificial Implants
Most participants agreed that CSWD was always contraindicated on metal implant, pacemaker and intrauterine device. Only a small percentage of therapists believed otherwise. However, they were less confident about using PSWD. Approximately 60(47%) and 55(43%) of the respondents believed that PSWD was always contraindicated for patients with metal implants or intrauterine devices, respectively. It is concerning that 46(36%) respondents believed PSWD could be used in the presence of a pacemaker or could be applied to other body parts (Figure 1).
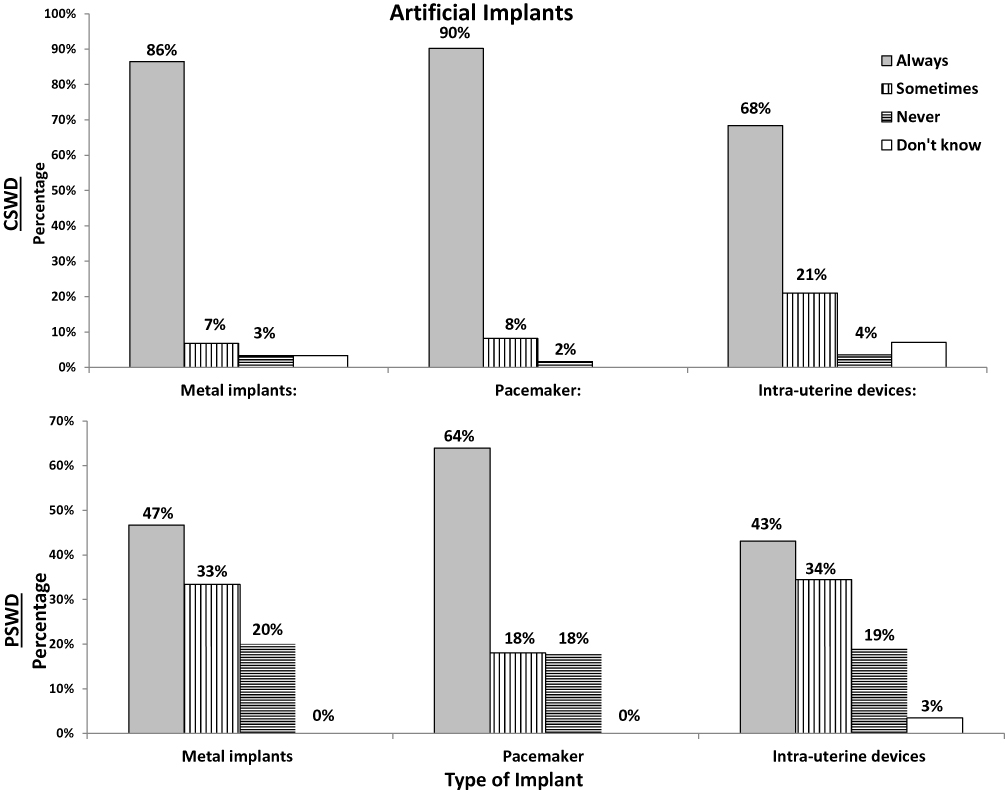 |
Figure 1 The responses of 128 Jordanian physiotherapists to the use of continuous shortwave diathermy (CSWD) and pulse shortwave diathermy (PSWD) under various artificial implant conditions. |
Cardiovascular Conditions
The majority of respondents believed that CSWD was always contraindicated for patients with ischemic tissues 87(68%), hemorrhage 115(90%), and venous thrombosis 113(88%), as well as about 64(50%) for those with heart and blood pressure issues. Their answers revealed strong agreement, especially when we take into account the sometimes-choice percentage. As applying CSWD in other body parts, the agreement will be significantly more favorable. More than half of respondents believed PSWD was always contraindicated in cases of hemorrhage 79(62%) and vein thrombosis 70(55%). The majority believed PSWD was sometimes contraindicated for ischemic tissues 61(48%), heart disease 56(44%), and abnormal blood pressure 61(48%). Obviously, the responses were almost equally divided as always or sometimes contraindicated using continuous or pulsed SWD to abnormalities in heart and blood pressure. Also, it is alarming that 24(9%) of respondents thought PSWD could be used in people with venous thrombosis without being contraindicated (Figure 2).
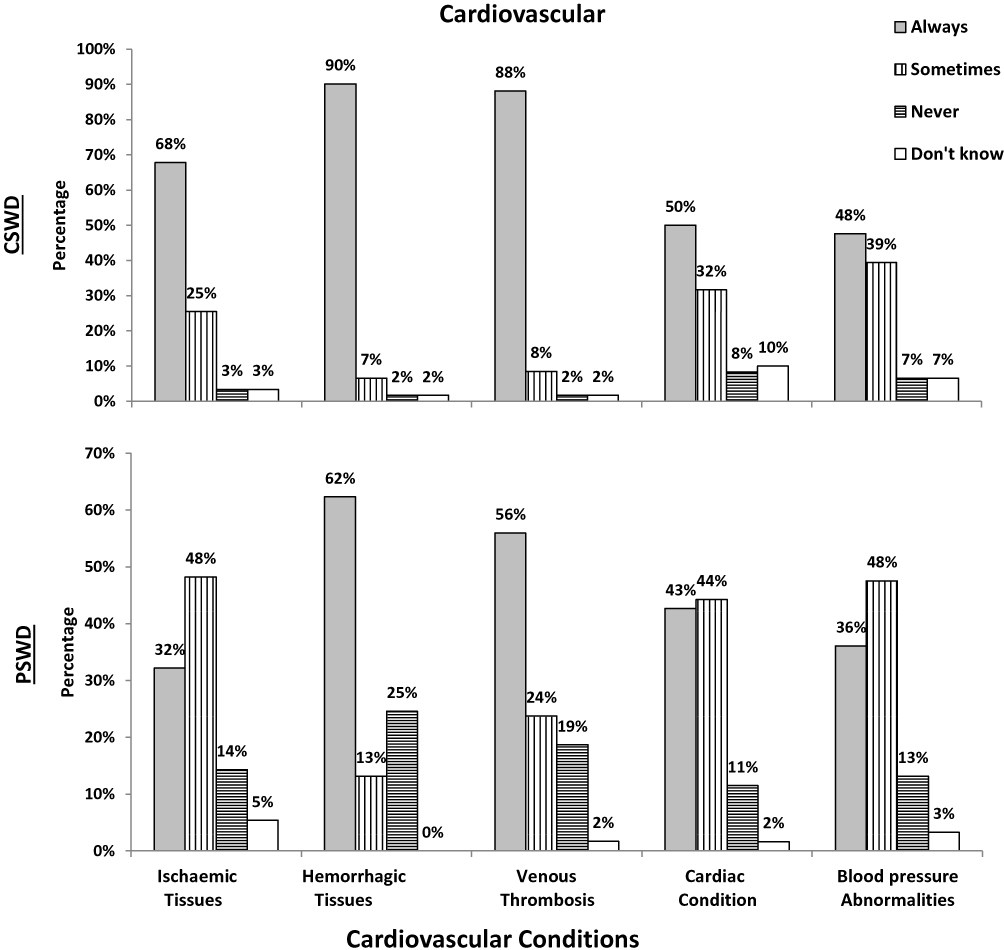 |
Figure 2 The responses of 128 Jordanian physiotherapists to the use of continuous shortwave diathermy (CSWD) and pulse shortwave diathermy (PSWD) under various cardiovascular conditions. |
Musculoskeletal Conditions
The majority of respondents felt confident that CSWD is always or sometimes contraindicated for synovitis, acute injury, osteomyelitis, and tuberculosis. They were unsure, however, about the use of CSWD to treat osteoporosis and rheumatoid arthritis. Their responses were nearly evenly divided among always, sometimes, and never being contraindicated (Figure 3). Also, therapists’ reactions to the use of PSWD for musculoskeletal conditions, especially acute injury and synovitis, have been observed to be uncertain (Figure 3). It is concerning that 18(14%) and 41(32%) of respondents, respectively, thought that using CSWD and PSWD was never contraindicated for tuberculosis. Similarly, 27(21%) and 32(25%), respectively, shared opinions regarding the use of CSWD and PSWD in osteomyelitis cases.
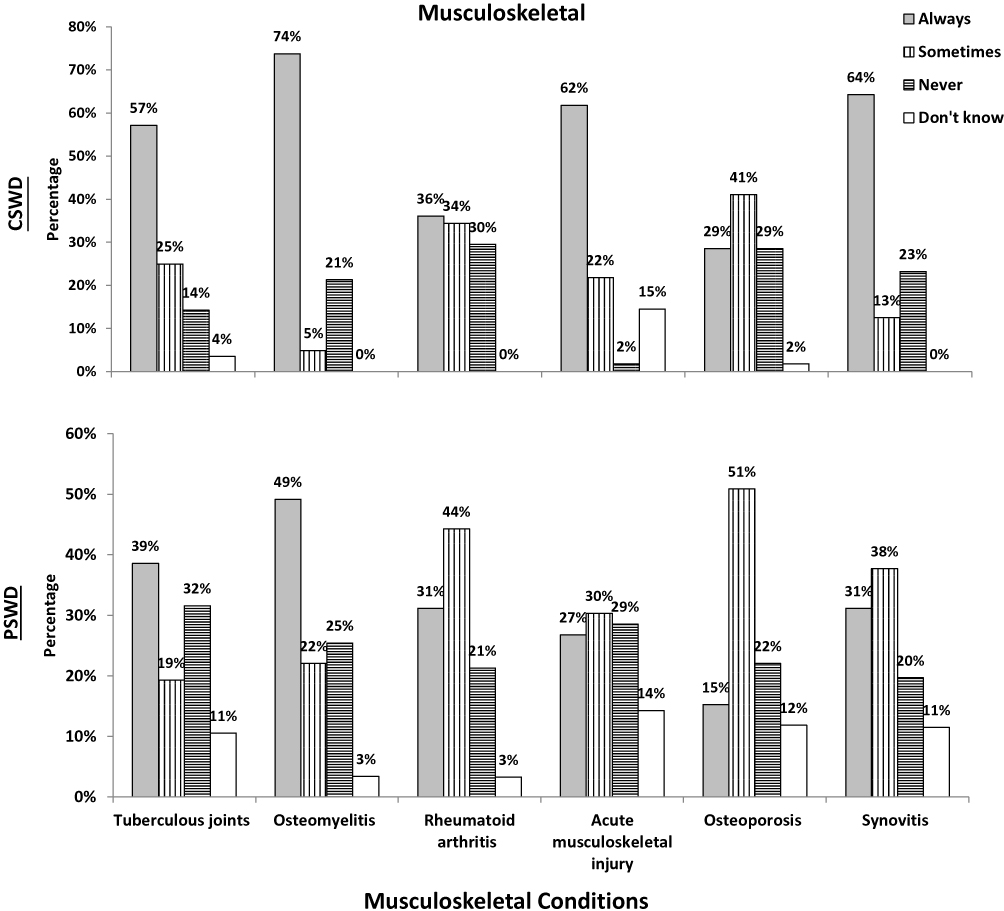 |
Figure 3 The responses of 128 Jordanian physiotherapists to the use of continuous shortwave diathermy (CSWD) and pulse shortwave diathermy (PSWD) in various musculoskeletal conditions. |
Dermatological Conditions
Locations with decreased feeling, moist or adhesive dressings, and an open wound, utilizing CSWD is always contraindicated, according to the vast majority of respondents. Yet, there was considerable uncertainty regarding the use of PSWD under the same circumstances. Almost 50% of respondents believed that PSWD was always contraindicated around wet or adhesive dressings and open wounds, whereas 72(56%) thought that PSWD was sometimes contraindicated over area with decreased feeling (Figure 4).
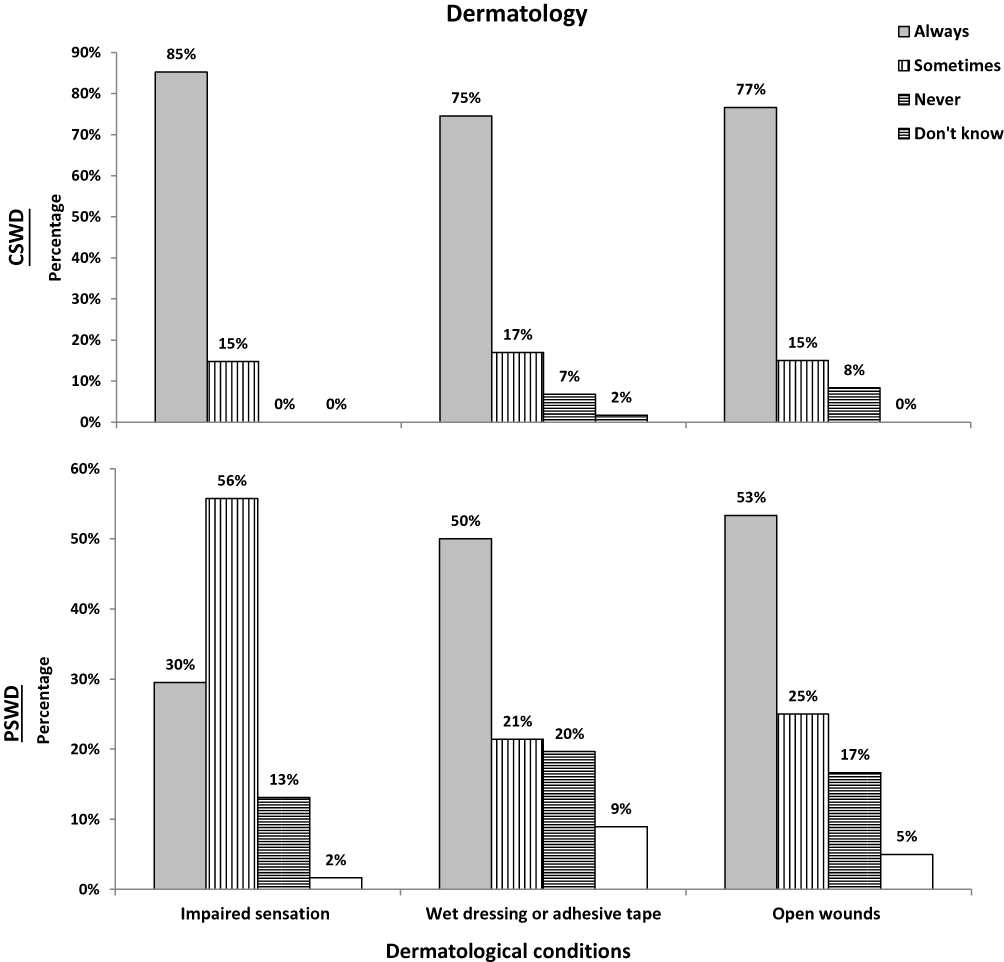 |
Figure 4 The responses of 128 Jordanian physiotherapists to the use of continuous shortwave diathermy (CSWD) and pulse shortwave diathermy (PSWD) for the treatment of different dermatological conditions. |
Patients with Medical Conditions
The majority of respondents believed that SWD was always contraindicated for the treatment of patients who had recently received radiation with both modes of the SWD. While 26(20%) believed that it was sometimes contraindicated and that it could be used on other body parts. Seventy-six (59%) respondents felt that anticoagulants were always contraindicated for CSWD and 89(46%) for PSWD. About 73(29%) agreed that both forms of SWD sometimes contraindicated for patients on anticoagulants. The respondents reported CSWD could be applied with small dosages of anticoagulants. Regarding recent analgesic use, respondents conceded that CSWD 72(65%) and PSWD 41(32%), respectively, are always contraindicated. Nevertheless, 29(23%) and 55(43%) of respondents, respectively, agreed that CSWD and PSWD are sometimes contraindications and that SWD may be used on an area of the body that has not received analgesia (Figure 5).
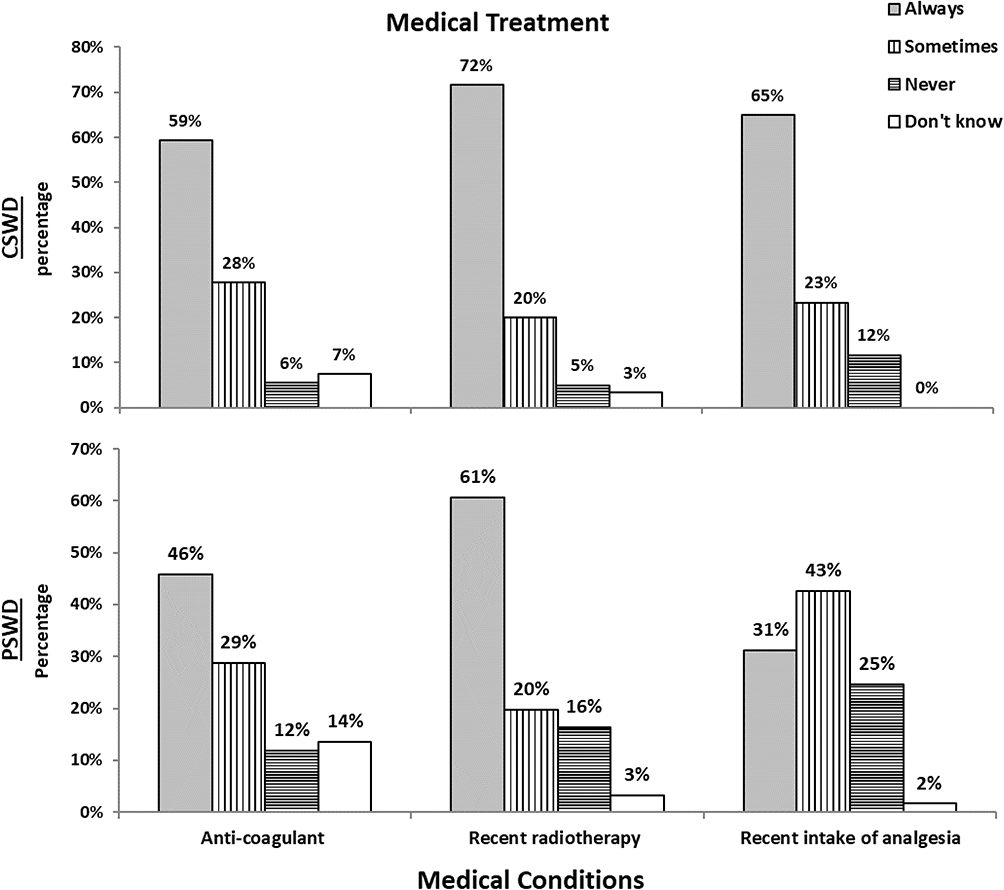 |
Figure 5 The responses of 128 Jordanian physiotherapists to the use of continuous shortwave diathermy (CSWD) and pulse shortwave diathermy (PSWD) on various medical conditions. |
Specialized Tissues
Most of the respondents agree well on the use of CSWD in specialized body tissues. They believed that it should not be applied to malignant tissues, during pregnancy or menstruation, to the eyes, gonads and epiphyseal region (Figure 6). Similarly, most respondents believe that PSWD should not be used in these tissues. However, 27(21%) to 36(28%) of respondents believed that PSWD was never contraindicated in these tissues (Figure 6).
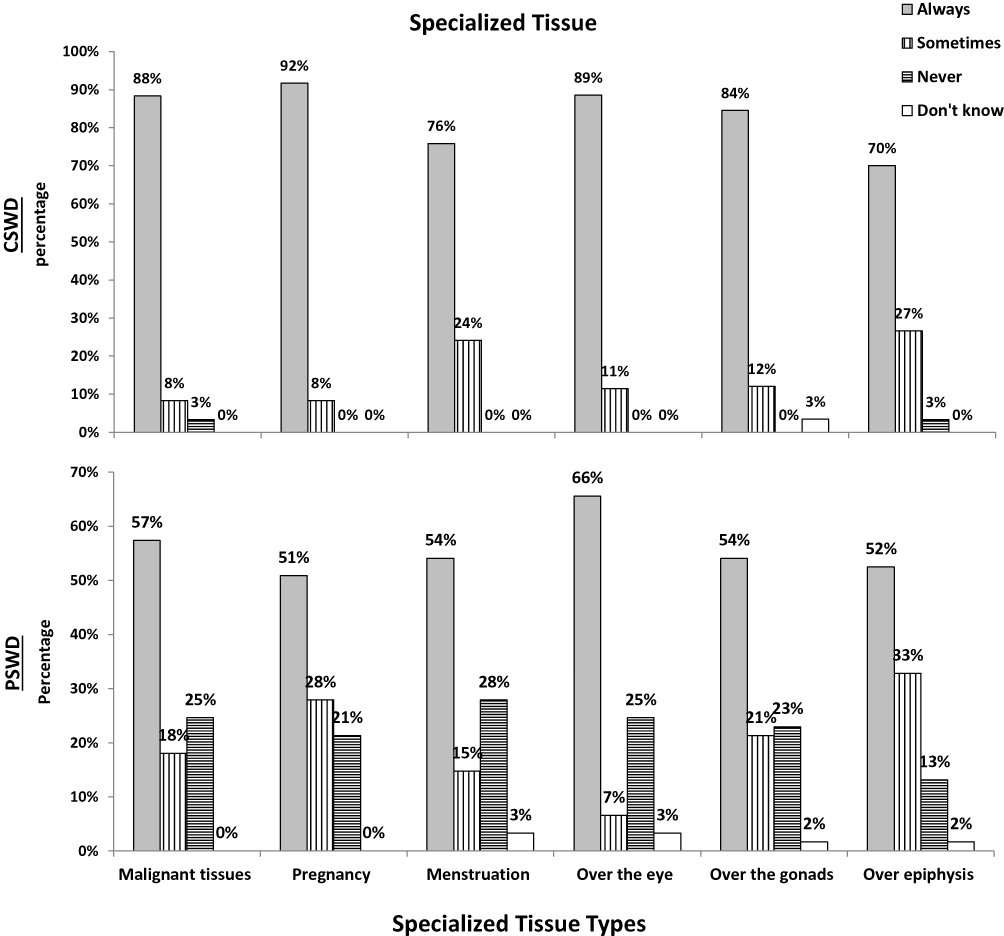 |
Figure 6 The responses of 128 Jordanian physiotherapists to the use of continuous shortwave diathermy (CSWD) and pulse shortwave diathermy (PSWD) on a variety of specialized tissues. |
Other Conditions
With the exception of obesity, between 65% and 93% of participants believed that CSWD was always contraindicated for unreliable patients (such as those with mental health problems), excessive edema, acute inflammation, pyrexia and neurological diseases. In the case of obesity, 49(38%) of the therapists considered CSWD to be contraindicated, while 60(47%) considered it to be sometimes contraindicated. Some reports could be applied with high precautions to slightly obese patients. Similarly, the majority of therapists believed that PSWD was always contraindicated for the same conditions, with the exception of those with obesity, 67(52%) believed that it could sometimes be contraindicated and 23(18%) that it was never contraindicated (Figure 7).
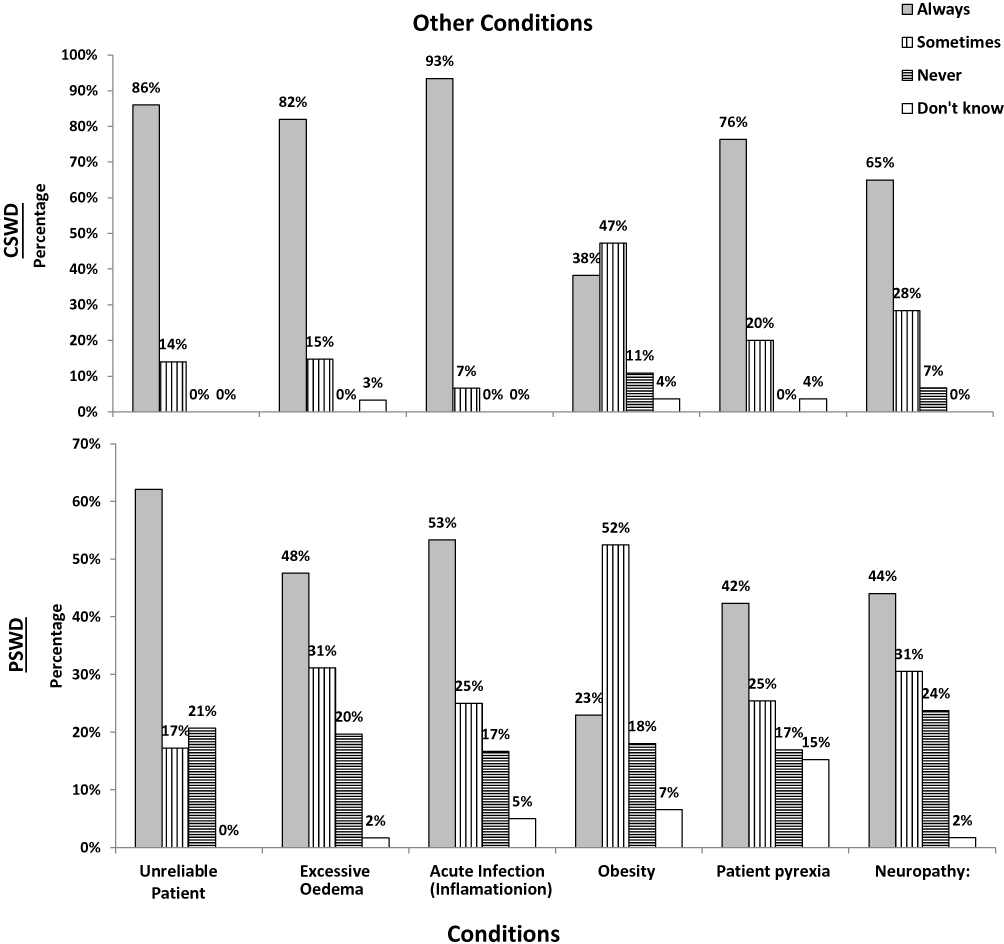 |
Figure 7 The responses of 128 Jordanian physiotherapists to the use of continuous shortwave diathermy (CSWD) and pulse shortwave diathermy (PSWD) under various other conditions. |
Discussion
This study was conducted to evaluate the knowledge and consensus of Jordanian physical therapists regarding shortwave contraindications. The response rate was 85.3% (128/150), and the sample was comprehensive and representative (at confidence level 95% and margin error 6%) of the Jordanian physiotherapist that utilized SWD at least once a week for their patients.
The results of this survey indicate that Jordanian physiotherapists are more likely to contemplate CSWD (82%) than PSWD (18%) (Table 1). Most likely because the CSWD can generate heat that satisfies the patient’s preferences and desires. This is consistent with literature reports indicating that the majority of patients undergoing physical therapy prefer heat production modalities over other modalities.19,20 The increased use of PSWD by physiotherapists in England, Australia, and Ireland, however, demonstrates that the preference for SWD modalities varies across countries.15–17 This could be because PSWD is safer and has undergone more clinical trials than CSWD.21,22
Good agreement was found on the contraindication of artificial implants, especially for intrauterine devices and orthopedic metal implants. This is because the metal will concentrate the radio-frequency field through a metal implant, which may increase the temperature around the implant and cause burns to surround tissues.23 In addition, most respondents believe that PSWD can be applied to patients with metal implants. It was reported that PSWD does not produce heat or heat the meta-implant. However, it is not approved for certain implants, such as loop-shaped wire implants.24,25 When applying CSWD or PSWD to artificial devices, Irish and Jordanian physiotherapists reached a comparable agreement except for applying PSWD to pacemakers. The fact that about 36% agreed to operate PSWD on patients with a pacemaker is worrying. Nevertheless, whether the application of SWD was directly or indirectly to other parts of the body is not safe for the patient. The literature not only prohibits the use of SWD in pacemakers but also warns patients not to be near operating SWD machines. Because electromagnetic waves propagate around the machine, which can interfere with the setting of the pacemaker.26 Applying SWD to pacemakers, neurostimulators, or defibrillators can damage the device, threaten life, or at least cause the destruction of surrounding tissues.10,22–26 This lack of knowledge of the respondents with PSWD is worrying and need further investigation and may be refreshment education.
The respondents were uncertain about using continuous and pulsed SWD for cardiac and blood pressure abnormalities. About 50% who chose sometime contraindication reported that both modes of SWD cannot apply directly to the heart, but it can be applied to other body parts. SWD is typically avoided in cardiovascular conditions for theoretical reasons, especially in case of heart and blood pressure abnormality.26,27 The main concern is that the body may be uncapable to adapt to the systemic change in temperature in response to SWD exposure.17 However, no scientific research support this proposition. If this is the case, a controlled room temperature would resolve any systematic increase in the body temperature. Only animals’ studies have shown that direct CSWD application can affect the heart’s enzymes and structures of rats.28 And considering the ratio of the rats’ size and the amount of electromagnetic energy exposed to, it is not comparable for a real patient receiving SWD. Despite the low research evidence, it seems the respondents prioritize patient’s safety by accepting to apply SWD not directly to the heart or not applying it at all. The Jordanian and Irish physiotherapist have comparable agreement about these conditions.
Physiotherapists in Jordan were aware that the risk of burns increases when CSWD is applied to an area with impaired circulation. Due to the skin’s inability to dissipate heat, burn occurs.23,29 Nonetheless, ischemic tissues can be treated with a non-thermal (PSWD) method. The research revealed that using PSWD with an average power of between 6 and 36 watts in an area with poor circulation has no negative effects.30,31 In addition, studies have banned the use of all types of SWD in hemorrhagic or thrombotic regions, despite the fact that PSWD has not been linked to any adverse effects.32 Utilizing SWD in a hemorrhagic region can increase bleeding. Moreover, patients with deep vein thrombosis should carefully consider the possibility of fatal side effects associated with detaching the thrombotic clot from its location to vital organs.29,33 In cases of hemorrhage or deep vein thrombosis, the respondents have a better agreement in favor of using CSWD rather than PSWD. A small percentage of the respondents would utilize PSWD in hemorrhage (25%) and in deep vein thrombosis (19%) conditions. The effects of PSWD on hemorrhagic and thrombotic tissues require additional investigation. In the meantime, it is recommended to avoid PSWD on these tissues. Jordanian and Irish physiotherapists have also come to a similar agreement.
CSWD should not be used for acute musculoskeletal injuries and inflammations such as synovitis, osteomyelitis, rheumatoid arthritis, tuberculosis, and osteoporosis, according to the scientific literature. Because heat can exacerbate already inflamed cells and accelerate the inflammatory response.34,35 About 14 to 21% of participants would use CSWD to treat osteomyelitis and tuberculosis, respectively. Even though it is a small percentage, it is concerning as these conditions are considered contraindications for SWD and it is crucial to avoid potential harm to their patients.
The primary advantage of CSWD in the treatment of chronic musculoskeletal disorders is its thermal effect.19,20 However, the literature focuses more on the nonthermal effects of PSWD in the treatment of musculoskeletal disorders, particularly knee arthritis.35–37 In addition, textbooks did not recommend the use of PSWD in cases of tuberculosis and osteomyelitis to prevent a possible increase in bacterial activity, despite the lack of scientific evidence.38,39 It is concerning, the fact that 32% and 25% of respondents would use PSWD for osteomyelitis and tuberculosis, respectively. We believed that Jordanian physiotherapists should refrain from using PSWD in these situations until contrary evidence is presented. The paucity of literature on wide range of musculoskeletal diseases may explain the respondents’ ambiguity regarding the use of PSWD in the majority of musculoskeletal conditions.
Heat can cause serious damage to the eye’s structure if it accumulates in the fluid-filled chamber of the eye due to poor circulation. Therefore, neither form of SWD should be applied to the eyes.23,39 Similarly, SWD is not recommended for dividing malignant tissues, gonads, or epiphyses. Thermal or non-thermal SWD can speed up cell division in these tissues.23,39,40 Due to a lack of evidence in the scientific literature, textbooks discourage the use of SWD on these tissues and prioritize patient safety over the possibility of unidentified adverse effects.23,39 Unfortunately, approximately 25% of respondents were unaware of these facts and agreed to use PSWD on these tissues. We believed that Jordanian physiotherapists should adhere to the textbook’s recommendations. Prioritizing patient safety is essential over the potential risks associated with using PSWD on any of aforementioned tissues.
Most alarming is the fact that approximately 8% and 49% of respondents would use CSWD and PSWD on pregnant women, respectively. Research and textbooks explicitly forbid the use of SWD on pregnant women, whether on the abdomen or any other body part. In addition, for occupational safety, a pregnant therapist should maintain a distance of 1 to 1.5 meters from an operating SWD machine.40 Clearly, the Jordanian physiotherapists lacked agreement and knowledge regarding the specialized tissues section of the questionnaire. The Irish physiotherapists were more knowledgeable than their Jordanian counterparts regarding the use of SWD in these conditions.
Applying CSWD requires an intact sensation to avoid danger of burning the skin. It is not recommended in cases of impaired sensation or in a condition associated with sensational disturbances, such as recent radiation therapy, use of analgesia, or neuropathy.23,39 In addition, other cases such as excessive edema, obesity and wet clothing, CSWD is contraindicated in order to avoid the risk of tissues overheating due to a high liquid content.39 Respondents demonstrated a satisfactory understanding of these contraindications, in addition to contraindications in other conditions such as acute inflammation, pyrexia, unreliable patients, open wounds or taking anticoagulants. The thermal effect of electromagnetic waves causes the main side effects of these conditions. The responses of the Jordanian physiotherapist to these conditions were consistent with those of the Irish physiotherapist.
SWD is still used in many physical therapy clinics around the world.15–17,41 The third most available and used physical therapy modality in the England is PSWD after ultrasound and interferential.15 And according to our sample, about 34% of physical therapy departments in Jordan use SWD. In particular, those in large public hospitals; however, it is more likely that private hospitals in Jordan tend to use less SWD because of their costs, as reported in Ireland.21 In other countries, such as Australia, the use of SWD has decreased despite equipment availability in most physical therapy departments. Due to the lack of empirical evidence and data sources supporting its efficacy, many physical therapy professionals were reluctant to implement SWD in their clinics.16 Yet, it has been suggested that SWD should be removed from the PT curriculum for undergraduate students.16 Nonetheless, the use of SWD has once again emerged in the Chinese literature during the COVID-19 pandemic, as it is effective in treating respiratory symptoms of COVID-19.41,42 Studies conducted in China have shown that the use of SWD was effective as an antiseptic and reduced the severity of respiratory symptoms associated with pulmonary infections.42 Additionally, a new portable and wearable PSWD device has been investigated to alleviate post-amputation phantom pain.43 The device was worn continuously for 30 days and significantly alleviated pain for approximately 70% of the participants.43 These studies demonstrate the immense potential of SWD in treating various physical ailments and suggest that its use should be further explored.41–43
Conclusion
Physical therapists using short-wave electromagnetic therapy on their patients must be aware of the risks involved. In the present study, we noticed that Jordanian physiotherapists concurred with the widely accepted contraindications of CSWD. In a manner similar to the Irish physiotherapist’s understanding. Although Jordanian physical therapists were uncertain of several PSWD contraindications, their responses were satisfactory in some conditions and alarming in others.
We are particularly concerned about the considerable number of participants who would use PSWD for a condition that has been deemed an absolute contraindication based on research results or theoretical perspectives. Patients with pacemakers, malignant tissues, expectant women, and eyes should therefore avoid all forms of SWD.12,23–29,44 In addition, we are concerned about the use of PSWD for conditions with debatable contraindications, such as tuberculosis, osteomyelitis, and venous thrombosis. The Jordanian physiotherapist demonstrated a lack of awareness of their contraindications. They did not provide justifications for their responses on the questionnaire, and the reason for this was unknown. Since CSWD is utilized more frequently than PSWD, it appears that the Jordanian physiotherapist correlated the contraindications with the thermal cause of SWD. The other reason may be the paucity of scientific research on SWD for the majority of conditions included in this questionnaire. Lastly, the physical therapy profession in Jordan is still in its early stages of development compared to other developed nations. The first bachelor’s degree program was established in 1999, and no safety and application guidelines for physical therapy modalities have been officially proposed or adopted.45
Therefore, additional research is necessary to determine why Jordanian physical therapists are unfamiliar with some contraindications of SWD and to develop practical solutions to improve their knowledge. In the meantime, Jordanian physiotherapists must adhere to the guidelines outlined in the textbook and avoid using SWD on the above-mentioned conditions. By doing so, they can ensure that their patients receive a safe and effective treatment devoid of side effects.
Abbreviations
SWD, Short Wave Diathermy; CSWD, Continuous Short Wave Diathermy; PSWD, Pulsed Short Wave Diathermy.
Summary
This survey study evaluated how physical therapists in Jordan adhere to and understand SWD contraindications. Results showed that Jordanian physiotherapists were aware of shortwave contraindications, despite some lack of awareness in some conditions. However, there was considerable uncertainty about PSWD. This discrepancy highlights the need for more fact-based research and improved education so physical therapists can understand the issues with SWD modalities.
Acknowledgments
We appreciate Nora Shields for letting us use this questionnaire and for allowing us to compare our physiotherapist’s knowledge with the results of her research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Robertson V, Ward A, Low J, Reed A. Textbook on Electrotherapy Explained Principles and Practice.
2. Birkett J. Soft tissue healing and the physiotherapy management of lower limb soft-tissue injuries. Physical Ther Rev. 1999;4(4):251–263. doi:10.1179/ptr.1999.4.4.251
3. Benincá IL, de Estéfani D, Pereira de Souza S, Weisshahn NK, Haupenthal A. Tissue heating in different short wave diathermy methods A systematic review and narrative synthesis. J Bodyw Mov Ther. 2021;28:298–310. doi:10.1016/j.jbmt.2021.07.031
4. Balogun O. Management of chronic pelvic inflammatory disease with shortwave diathermy: a case report. Phys Ther. 2016;68(10):1541–1545.
5. Babaei-Ghazani A, Shahrami B, Fallah E, Ahadi T, Forough B, Ebadi S. Continuous shortwave diathermy with exercise reduces pain and improves function in Lateral Epicondylitis more than sham diathermy: a randomized controlled trial. J Bodyw Mov Ther. 2020;24(1):69–76. doi:10.1016/j.jbmt.2019.05.025
6. Picelli A, Munari D, Serina A, et al. Short-wave diathermy for spastic equinus foot in chronic stroke patients: a proof-of-concept pilot study. Minerva Med. 2021. doi:10.23736/S0026-4806.21.07581-9
7. Munari D, Serina A, Leonardelli A, et al. Effects of deep heating modalities on the morphological and elastic properties of the non-insertional region of Achilles tendon: a pilot study. Int J Hyperthermia. 2022;39(1):222–228. doi:10.1080/02656736.2022.2026497
8. Goats GC. Pulsed electromagnetic (short-wave) energy therapy. Br J Sports Med. 1989;23(4):213–216. doi:10.1136/bjsm.23.4.213
9. Murray CC, Kitchen S. Effect of pulse repetition rate on the perception of thermal sensation with pulsed shortwave diathermy. Physiother Res Int. 2000;5(2):73–84. doi:10.1002/pri.187
10. Chartered Society of Physiotherapy (CSP). Physios warned of diathermy danger. Frontline. 2001;7:9.
11. Ouellet-Hellstrom R, Stewart WF. Miscarriages among female physical therapists who report using radio- and microwave-frequency electromagnetic radiation. Am J Epidemiol. 1993;138(10):775–786. doi:10.1093/oxfordjournals.aje.a116781
12. Lerman Y, Jacubovich R, Green MS. Pregnancy outcome following exposure to shortwaves among female physiotherapists in Israel. Am J Ind Med. 2001;39(5):499–504. doi:10.1002/ajim.1043
13. Gubéran E, Campana A, Faval P, et al. Gender ratio of offspring and exposure to shortwave radiation among female physiotherapists. Scand J Work Environ Health. 1994;20(5):345–348. doi:10.5271/sjweh.1387
14. Seiger C, Draper DO. Use of pulsed shortwave diathermy and joint mobilization to increase ankle range of motion in the presence of surgically implanted metal: a case series. J Orthop Sports Phys Ther. 2006;36(9):669–677. doi:10.2519/jospt.2006.2198
15. Shah S, Farrow A. Investigation of practices and procedures in therapeutic diathermy: a study from the physiotherapists’ health and safety perspective. Physiother Res Int. 2007;12(4):228–241. doi:10.1002/pri.382
16. Chipchase LS, Williams MT, Robertson VJ. A national study of the availability and use of electrophysical agents by Australian physiotherapists. Physiother Theory Pract. 2009;25(4):279–296. doi:10.1080/09593980902782611
17. Shields N, O’Hare N, Gormley J. Contra-indications to shortwave diathermy: a survey of Irish physiotherapists. Physiotherapy. 2004;90(1):42–53. doi:10.1016/S0031-9406(03)00005-1
18. Minister of Health. Hospitals - Minister of Health. Available from: https://moh.gov.jo/EN/List/Hospitals.
19. Jette AM, Delitto A. Physical therapy treatment choices for musculoskeletal impairments. Phys Ther. 1997;77(2):145–154. doi:10.1093/ptj/77.2.145
20. Denegar CR, Dougherty DR, Friedman JE, et al.Preferences for heat, cold, or contrast in patients with knee osteoarthritis affect treatment response. Clin Interv Aging. 2010;(5):199–206. doi:10.2147/CIA.S11431
21. Shields N, Gormley J, O’Hare N. Shortwave diathermy: a review of existing clinical trials. Phys Ther Rev. 2001;6:101–118. doi:10.1179/ptr.2001.6.2.101
22. Tzima E, Martin CJ. An evaluation of safe practices to restrict exposure to electric and magnetic fields from therapeutic and surgical diathermy equipment. Physiol Meas. 1994;15:201–216. doi:10.1088/0967-3334/15/2/008
23. Cameron F. Physical Agents in Rehabilitation: An Evidence-Based Approach to Practice.
24. Draper DO, Castel JC, Castel D. Low-watt pulsed shortwave diathermy and metal-plate fixation of the elbow. Athletic Ther Today. 2004;9(5):28–32.
25. Draper DO. Can pulsed shortwave diathermy be used over surgically-implanted metal? Int J Athletic Ther Train. 2022;22(6):23–27. doi:10.1123/ijatt.2016-0091
26. Jones SL. Electromagnetic field interference and cardiac pacemakers. Phys Ther. 1976;56(9):1013–1018. doi:10.1093/ptj/56.9.1013
27. Hamburger S, Logue JN, Silverman PM. Occupational exposure to non-ionizing radiation and an association with heart disease: an exploratory study. J Chronic Dis. 1983;36(11):791–802. doi:10.1016/0021-9681(83)90071-1
28. Zhang J, Yu C, Yao BW, et al. Dose-dependent cardiac dysfunction and structural damage in rats after shortwave radiation. Biomed Environ Sci. 2020;33(8):603–613. doi:10.3967/bes2020.079
29. Sousa NT, Guirro EC, Calió JG, Queluz MC, Guirro RRJ. Application of shortwave diathermy to lower limb increases arterial blood flow velocity and skin temperature in women: a randomized controlled trial. Braz J Phys Ther. 2017;21(2):127–137. doi:10.1016/j.bjpt.2017.03.008
30. Seaborne D, Quirion-De Girardi C, Rousseau M, Rivest M, Lambert J. The treatment of pressure sores using pulsed electromagnetic energy (PEME). Physiother Can. 1996;48:131–137.
31. Itoh M, Montemayor JS, Matsumoto E, Eason A, Lee MH, Folk FS. Accelerated wound healing of pressure ulcers by pulsed high peak power electromagnetic energy (Diapulse). Decubitus. 1991;4:24–34.
32. Fiscus KA, Kaminski TW, Powers ME. Changes in lower-leg blood flow during warm-, cold- and contrast-water therapy. Arch Phys Med Rehabil. 2005;86:1404–1410. doi:10.1016/j.apmr.2004.11.046
33. Rennie S. Electrophysical agents - contraindications and precautions: an evidence-based approach to clinical decision making in physical therapy. Physiother Can. 2010;62(5):1–80.
34. Laufer Y, Dar G. Effectiveness of thermal and thermal short-wave diathermy for the management of knee osteoarthritis: a systematic review and meta-analysis. Osteoarthritis Cartilage. 2012;20(9):957–966. doi:10.1016/j.joca.2012.05.005
35. Masiero S, Pignataro A, Piran G, et al. Short-wave diathermy in the clinical management of musculoskeletal disorders: a pilot observational study. Int J Biometeorol. 2020;64(6):981–988. doi:10.1007/s00484-019-01806-x
36. El Mohammad AR, Koneru S, Staelin R, McLeod K, Tabbouche O, Rawe IM. Pulsed shortwave therapy in cervical osteoarthritis: an NSAID- controlled, randomized clinical trial. Comprehensive Clin Med. 2021;3(1):166–175. doi:10.1007/s42399-020-00652-y
37. Bjordal JM, Johnson MI, Lopes-Martins RA, Bogen B, Chow R, Ljunggren AE. Short-term efficacy of physical interventions in osteoarthritic knee pain. A systematic review and meta-analysis of randomised placebo-controlled trials. BMC Musculoskelet Disord. 2007;8(1):51. doi:10.1186/1471-2474-8-51
38. Goodman CC, Fuller KS. Goodman and Fuller’s Pathology: Implications for the Physical Therapist.
39. Watson T, Nussbaum E. Electrophysical Agents: Evidence-Based Practice (Physiotherapy Essentials).
40. Karpowicz J, Gryz K. An assessment of hazards caused by electromagnetic interaction on humans present near short-wave physiotherapeutic devices of various types including hazards for users of electronic active implantable medical devices (AIMD). Biomed Res Int. 2013;150143. doi:10.1155/2013/150143
41. Yu HP, Jones AY, Dean E, Liisa LE. Ultra-shortwave diathermy - a new purported treatment for management of patients with COVID-19. Physiother Theory Pract. 2020;36(5):559–563. doi:10.1080/09593985.2020.1757264
42. Shah SZ, Nasb M, Lu M, Huang L, Wang Y, Chen H. Scaling the need, benefits, and risks associated with COVID-19 acute and postacute care rehabilitation: a review. Rehabil Res Pract. 2020;2020:3642143. doi:10.1155/2020/3642143
43. Ilfeld BM, Said ET, Abdullah B, Finneran IJ. Treating intractable postamputation pain with noninvasive, wearable, nonthermal, pulsed shortwave (radiofrequency) therapy: a 12-patient case series. Am J Case Rep. 2022;17(23):e937549.
44. Frontera C. Cancer pain and physical modalities. In: Gulati A, Puttanniah V, Bruel B, Rosenberg W, Hung J, editors. Essentials of Interventional Cancer Pain Management. NY: Springer International Publishing; 2019.
45. Maayah MF, Al-Jarrah M, Mysore S, et al. The perception of physical therapy students towards their profession in Jordan. Healthcare. 2022;10:849. doi:10.3390/healthcare10050849
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.