Back to Journals » Clinical Ophthalmology » Volume 20
Physiological Responses During Phacoemulsification Cataract Surgery and Perceived Stress Among Ophthalmology Trainees: A Cross-Sectional Study
Authors Doostparast A, Kermani B, Semnani F, Ghandhari M, Zarei-Ghanavati S, Eslampoor A ![]()
Received 1 April 2026
Accepted for publication 30 May 2026
Published 6 June 2026 Volume 2026:20 552382
DOI https://doi.org/10.2147/OPTH.S552382
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Dr Bharat Gurnani
Armin Doostparast,1 Bahareh Kermani,1,2 Farbod Semnani,3 Maryam Ghandhari,1,4,5 Siamak Zarei-Ghanavati,1 Alireza Eslampoor1
1Eye Research Center, Mashhad University of Medical Sciences, Mashhad, Iran; 2Eye Research Center, The Five Senses Health Institute, Mohebkhah Hospital, Iran University of Medical Sciences, Tehran, Iran; 3School of Medicine, Tehran University of Medical Sciences, Tehran, Iran; 4Student Research Committee, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran; 5Department of Radiology, School of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran
Correspondence: Alireza Eslampoor, Email [email protected] Armin Doostparast, Email [email protected]
Background: Intraoperative stress can adversely affect surgical performance and trainee well-being, particularly in ophthalmic surgeries where micro-level precision plays a paramount role. This study aimed to evaluate both subjective measures of general perceived stress and objective physiological responses during phacoemulsification cataract surgery among ophthalmology trainees.
Materials and Methods: In this cross-sectional study, 59 ophthalmology residents and fellows were enrolled. Objective physiological responses, including systolic blood pressure (SBP), diastolic blood pressure (DBP), heart rate (HR), and arterial oxygen saturation (SpO2), were recorded before and during key steps of surgery (incision, capsulorhexis, and lens removal with intraocular lens (IOL) implantation) by an ambulatory electrocardiograph (ECG) device. General perceived stress was also assessed during the preoperative resting period using the 14-item perceived stress scale (PSS-14).
Results: SBP and HR increased significantly throughout the surgical steps, with the highest values observed during lens removal and IOL implantation (all P < 0.03). In contrast, changes in DBP and SpO2 were not statistically significant (P > 0.05). Less experienced trainees demonstrated higher overall DBP trends compared to more experienced counterparts (P = 0.01). Based on PSS-14 scores, female surgeons and those with lower levels of training reported significantly higher perceived stress (P = 0.04 and P < 0.001, respectively). Pre-operative propranolol use was associated with lower perceived stress (P = 0.02), although it did not significantly affect physiological parameters.
Conclusion: Physiological responses in ophthalmology trainees increase during phacoemulsification cataract surgery, which may be translated into higher intra-operative stress. This increase is particularly higher in later stages, and is influenced by experience level and individual factors. As a result, these findings underscore the importance of implementing targeted strategies to enhance ophthalmology trainee well-being and improve surgical training environments, especially for individuals more susceptible to elevated stress levels.
Keywords: stress, trainee, phacoemulsification, cataract, heart rate, PSS-14
Introduction
Psychological stress, or simply stress, is a widely known factor that significantly impacts the health and productivity of individuals globally.1,2 Experiencing stress for an extended period of time results in burnout, substance abuse, absenteeism from work, depression, and significant financial setbacks.2–5 In particular, surgery stands out that, considering they work in an environment filled with uncertainty and stress, surgeons in operating rooms face a multitude of challenges, such as unexpected complications, exposure to traumatizing events, noise, and interruptions, multitasking, technical difficulties, teamwork issues, long working hours and lack of sleep; all of which can impact their cognitive states and psychomotor performance.6–9
Within the realm of medicine, ophthalmology is distinguished due to its focus on precision microsurgeries and the use of cutting-edge devices for particularly accurate measurements, which, as a result, can cause a significant amount of stress for both ophthalmology consultants and trainees.6,10 This places extra emphasis on exploring this phenomenon among trainees, as burnout, depersonalization, and fatigue are most common among residents and fellows in training.11,12
Cataract surgery using the phacoemulsification technique is one of the most common and successful surgical procedures performed worldwide,13 which demands immediate and flawless results. Any errors or complications during the surgery are impossible to conceal from patients, putting immense pressure on ophthalmic surgeons.14
The current scholarly literature suggests that every ophthalmic surgeon is under stress during cataract surgeries, regardless of age.14 Yet, the level of intraoperative stress correlates inversely with experience and is particularly higher among trainees.14–16 Moreover, stress is shown to be highly associated with a number of physiologic parameters.6,17,18 On top of fluctuations of stress-related physiological parameters, it is essential to quantify general perceived stress, as it directly affects surgeons’ long-term mental well-being. A nationwide study by Ansari et al also demonstrated that 40% of respondents disclosed that they had cataract surgery-related high burnout in terms of decreased feelings of personal accomplishment.13 Taken together, these findings highlight the need to study ophthalmic trainees’ mental well-being and its relationship with the sociodemographic characteristics, as well as investigating the fluctuations of objective physiologic parameters. However, there is a lack of sufficient evidence regarding the concurrent assessment of both objective and subjective perceived stress among ophthalmology trainees. Therefore, the current study aimed to investigate both perceived stress and stress-related physiologic responses among ophthalmology trainees during phacoemulsification cataract surgery. The findings may bring a better understanding of how to reduce intraoperative stress and mental well-being of ophthalmology trainees in surgical-educational settings and provide viable insights for optimizing a better training curriculum.
Materials and Methods
Study Design and Subjects
This cross-sectional study included 59 ophthalmology residents and fellows of Khatam-al-anbia Eye Hospital affiliated with Mashhad University of Medical Sciences, Iran. The study protocol adhered to the guidelines outlined in the Declaration of Helsinki, and the institutional review board of Mashhad University of Medical Sciences approved the study (approval code: IR.MUMS.fm.REC.1395.192). Written informed consent was provided by all study participants after a clear explanation of the study goals and procedures. Included in the study were all ophthalmology residents and fellows who were trained to perform cataract surgery using the phacoemulsification technique. To ensure consistency in surgical complexity, only cases of uncomplicated cataracts with grade 2–3 nuclear opacities, according to the Lens Opacities Classification System III (LOCS III), and with sufficient pupillary dilation were included. Participants were excluded if they had a history of cardiovascular disease, arrhythmias, or any systemic condition known to affect heart rate or blood pressure. Individuals using medications that could influence cardiovascular parameters (eg, antihypertensive agents, antiarrhythmic drugs, or anxiolytics) were also excluded, with the exception of the prescription of propranolol (40 mg oral tablets used 30–60 minutes prior to surgery), which was recorded and analyzed separately. Additional exclusion criteria included any underlying respiratory disorders affecting oxygen saturation, inability to complete the perceived stress scale – 14-item version (PSS-14) questionnaire, or incomplete intraoperative physiological data. The trainees’ sociodemographic characteristics, such as age, sex, and level of education, were recorded at the beginning of the study. Any upcoming complications during surgery, as well as pre-operative use of propranolol and the anesthesia method, whether topical or general anesthesia, were also recorded.
Phacoemulsification Surgical Procedures
All cataract surgeries were performed electively by ophthalmology residents or fellows under the supervision of experienced consultant surgeons. A standardized phacoemulsification technique was applied in all cases, consistent with the routine surgical protocol of the institution.15
Depending on the patient’s condition and the surgeon’s preference, procedures were conducted under either topical anesthesia using tetracaine eye drops or general anesthesia, with the latter being more frequently utilized due to the educational nature of the center. Surgical access was achieved through temporal or supratemporal clear corneal incisions. Pharmacologic pupil dilation was maintained intraoperatively using diluted intracameral adrenaline when necessary. In selected cases with poor red reflex, trypan blue dye was applied to facilitate visualization of the anterior capsule. A viscoelastic substance (2% hydroxypropyl methylcellulose) was injected into the anterior chamber to maintain space and protect intraocular structures.
A continuous curvilinear capsulorhexis (CCC) was then created, followed by hydrodissection and hydrodelineation to mobilize the lens nucleus. Phacoemulsification of the nucleus was performed using standard techniques such as divide-and-conquer or chop methods, depending on the surgeon’s preference and case complexity. Residual cortical material was removed using irrigation and aspiration. Subsequently, a foldable acrylic intraocular lens (IOL) was implanted, typically within the capsular bag in uncomplicated cases or in the ciliary sulcus when capsular support was inadequate. At the end of the procedure, the anterior chamber was irrigated to remove remaining viscoelastic material. Corneal incisions were secured either by stromal hydration or, when indicated, by placement of nylon sutures. All surgeries were closely supervised, and in cases of intraoperative complications, immediate assistance was provided by attending surgeons.
Vital Signs Measurement
Ophthalmology trainees’ systolic blood pressure (SBP), diastolic blood pressure (DBP), heart rate (HR), and arterial oxygen saturation (SpO2) were measured and recorded thirty minutes prior to surgery, after a resting period in the preoperative setting, before surgical manipulation or intraoperative stress exposure to minimize any potential effects on the baseline measurements. These vital signs were measured by an ambulatory electrocardiograph (ECG) device and were recorded throughout the entire time of surgery, including at the time of making a clear corneal incision, capsulorhexis, and lens removal (nucleus removal, cortical removal, aspiration, and irrigation) with intraocular lens (IOL) implantation. The values for physiological responses were averaged during each step of the surgery. To avoid any interference during surgery, the monitoring cuff was positioned on the non-dominant arm of the surgeon, ensuring minimal disruption to the surgeon’s performance.14
Perceived Stress Measurement and Questionnaire
Trainees’ stress levels have been evaluated using the perceived stress scale (PSS). The PSS, developed by Cohen et al (1983), is one of the most widely used methods to determine people’s level of stress.19 The PSS has three versions with 4, 10, and 14 items each, and is used to gauge how much stress has been felt generally over the past month.20 The PSS contains 14 items in its original form (PSS-14), including 14 various questions with both negative (items 1, 2, 3, 8, 11, 12, and 14) and positive qualities (items 4, 5, 6, 7, 9, 10, and 13).21 Items evaluating negative traits include feeling unable to deal with life’s problems or feeling sad or anxious. Feeling confident or strong enough to overcome obstacles and challenges is among the items assessing positive qualities.
According to the 5-point Likert scale, the questionnaire is scored as follows: For the negative questions, 0 indicates never, 1 rarely, 2 occasionally, 3 frequently, and 4 most of the time; however, in the positivity subscale, the phrases never = 4, to most of the time = 0, are scored inversely. 0 is the lowest, and 56 is the highest possible score. The greater perceived stress is indicated by a higher score.21 The PSS assesses stress management and emotional response to stressful events through thoughts and feelings. This scale also identifies stressful interpersonal dynamics and assesses behavioral disorder risk factors.21,22 The PSS has been validated and is used in numerous countries due to its wide range of applications, and has been translated into various languages.20–22 The 14-item version of this questionnaire (PSS-14) has been used in this study. To avoid recall bias, this questionnaire was administered to each trainee during the preoperative resting period, prior to any surgical intervention, to capture their general perceived stress level independent of the outcome of the surgical procedure.
Statistical Analysis
Statistical analysis was performed using SPSS software (version 27.0; IBM Corp., Armonk, NY, USA). Continuous variables were expressed as mean ± standard deviation (SD), and categorical variables as frequencies and percentages. Each individual trainee contributed only one procedure, ensuring statistical independence. The normality of data distribution was assessed using the Shapiro–Wilk test and Q-Q plots. To evaluate changes in physiological parameters (SBP, DBP, HR, and SpO2) across different surgical steps, repeated-measures analysis of variance (RM-ANOVA) was applied to represent the time-by-group interaction. Sphericity assumptions were also assessed using Mauchly’s test, and Greenhouse–Geisser correction was applied when violations were detected. When a significant overall effect was detected, pairwise comparisons were performed using the post hoc test and Bonferroni correction. For analysis of trends in physiological parameters across surgical steps stratified by baseline characteristics, mixed-design (between–within) ANOVA was used. PSS-14 scores were analyzed using the independent t-test or one-way ANOVA. A two-tailed P-value < 0.05 was considered statistically significant.
Results
Baseline Demographic and Clinical Characteristics
This study included a total of 59 ophthalmology trainees, with a mean age of 29.2 ± 4.6 years. Of these, 35 (59.3%) were male, and 24 (40.7%) were female. Regarding the level of training, 14 trainees (23.7%) were PGY-2 residents, 35 (59.3%) were PGY-3,4 residents, and 10 (17.0%) were fellows. The majority of surgeries were performed under general anesthesia (81.4%). Pre-operative propranolol was used by 15 trainees (Table 1).
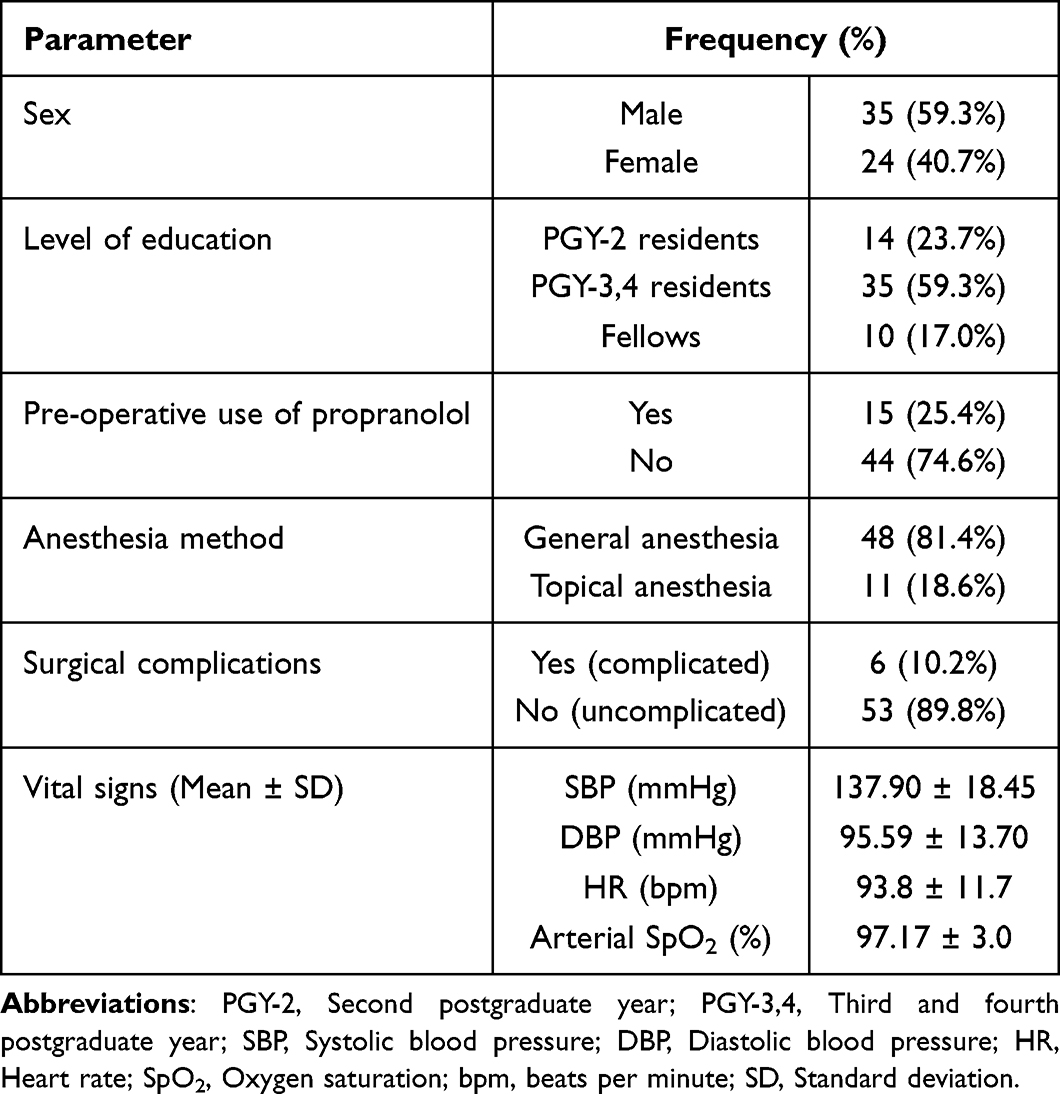 |
Table 1 Trainees’ Baseline Demographic and Clinical Factors and Their Vital Signs |
Physiological Responses Across the Surgical Steps
Table 2 exhibits and compares the trainees’ vital signs across the three steps of phacoemulsification cataract surgery. SBP consistently rose throughout the surgery, with an increase of 7.86 ± 14.13 mmHg during capsulorhexis compared to incision, 11.17 ± 14.74 mmHg during lens removal and IOL implantation compared to incision, and 3.30 ± 11.30 mmHg during lens removal and IOL implantation compared to capsulorhexis, with all of which were found to be statistically significant (P <0.001, <0.001 and 0.03, respectively).
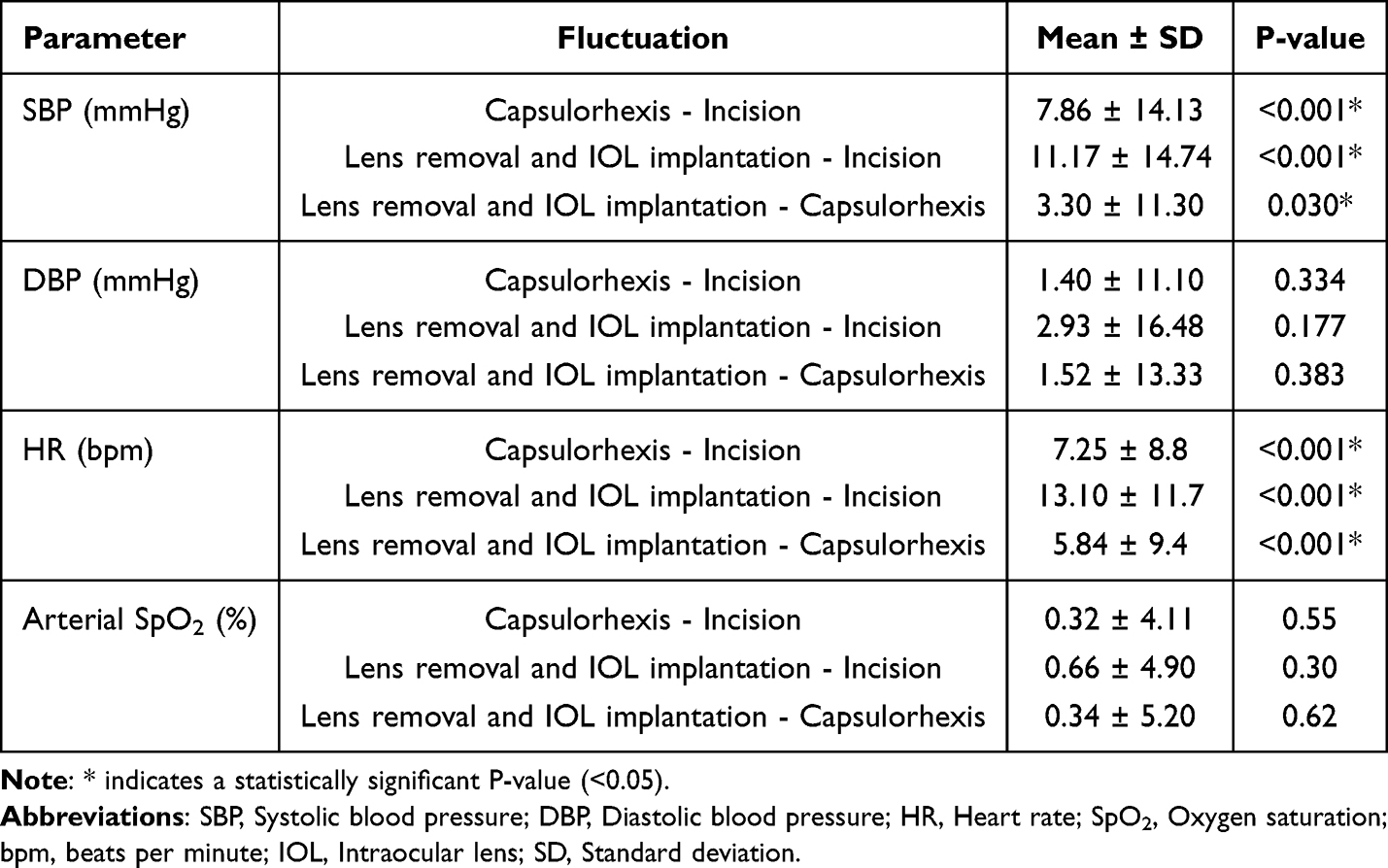 |
Table 2 Vital Signs Variations Across Different Steps of Phacoemulsification Cataract Surgery |
HR also rose throughout the various steps of cataract surgery, with an increase of 7.25 ± 8.8 bpm in capsulorhexis compared to incision, 13.10 ± 11.7 bpm in lens removal and IOL implantation compared to incision, and 5.84 ± 9.4 bpm in lens removal and IOL implantation compared to capsulorhexis; all of which were similarly found to be statistically significant (all P <0.001).
However, the changes in DBP and SpO2 during these surgical steps were statistically insignificant across all pairwise comparisons (P > 0.05). Figure 1 illustrates the trend of each of the vital signs during the different steps of phacoemulsification cataract surgery using a line graph.
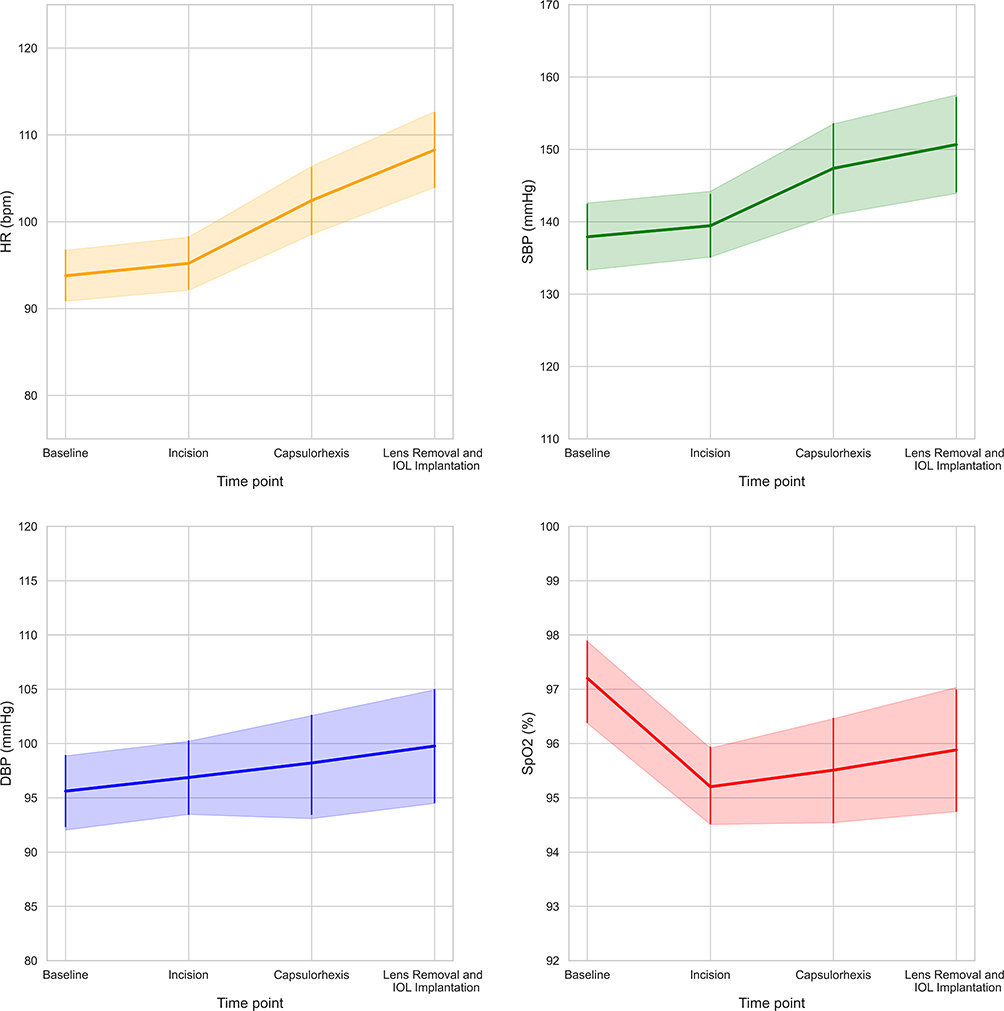 |
Figure 1 Changes in trainees’ vital signs at baseline and across different steps of phacoemulsification cataract surgery. The error bars show the 95% confidence intervals. Abbreviations: SBP, Systolic blood pressure; DBP, Diastolic blood pressure; HR, Heart rate; SpO2, Oxygen saturation; bpm, beats per minute; IOL, Intraocular lens. |
Physiological Responses Trends Stratified by Trainee Characteristics
Supplementary Tables S1–S4 summarize the assessments of trends of SBP, DBP, HR, and arterial SpO2 in the study population according to baseline demographic and clinical factors. The findings indicated that SBP, HR, and arterial SpO2 trend did not significantly differ when stratified by any of these factors (all P > 0.05) (Supplementary Tables S1, S3 and S4). DBP, on the other hand, showed a significant difference when being stratified by the trainee’s level of education (P-value = 0.01). PGY-2 ophthalmology residents had the highest DBP trend compared to both PGY-3,4 and fellows. Moreover, PGY-3,4 ophthalmology residents were also found to have a higher DBP compared to fellows. DBP trend, however, was not significantly associated with any of the remaining factors (Supplementary Table S2).
Perceived Mental Stress
Alternatively, the PSS-14 findings, summarized in Table 3, showed that female surgeons experienced higher levels of stress than males, which was statistically significant (P = 0.04). This general perceived stress was also found to be significantly associated with pre-operative use of propranolol (P = 0.02) and the level of education (P < 0.001), as PGY-2 residents experienced the highest and fellows experienced the lowest intraoperative stress. The level of stress was not significantly associated with the anesthesia method or the presence of surgical complications (P = 0.31 and 0.67, respectively).
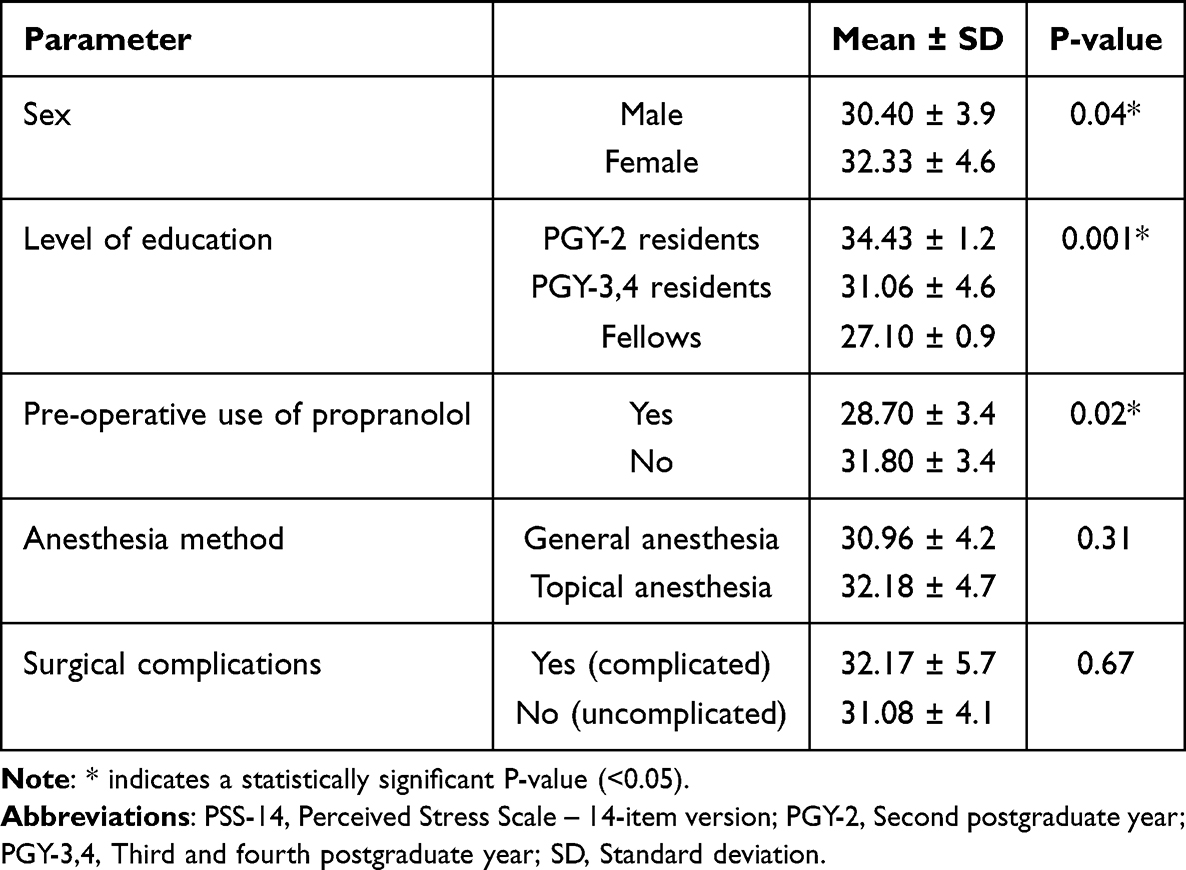 |
Table 3 Stress Level of Trainees Performing Phacoemulsification Cataract Surgery According to the Baseline Demographic and Clinical Factors Measured by the PSS-14 Questionnaire |
Discussion
This study investigated the demographic and clinical factors potentially affecting intraoperative stress experienced by ophthalmology trainees during phacoemulsification cataract surgery. It was found that SBP and HR were consistently increased throughout the three steps of surgery. In contrast, DBP and SpO2 remained largely unaffected during these surgical stages. Compared based on demographic and clinical factors, the DBP trend was found to be significantly associated with the level of education, in the way that PGY-2 residents had the highest and fellows had the lowest DBP. No other statistically significant association was found between these factors and other vital signs. The magnitude of the observed SBP and HR increases warrants consideration of their clinical significance. The peak SBP rise of approximately 11 mmHg and peak HR rise of approximately 13 bpm from incision to lens removal and IOL implantation are consistent with the hemodynamic responses reported in other surgical stress studies and align with expected sympathetic activation under procedural demand.14,18 Although these changes are statistically significant, they remain within a physiologically moderate range and are unlikely to represent a clinically hazardous cardiovascular burden in otherwise healthy young trainees. Nonetheless, the sustained and progressive nature of these elevations across surgical steps, rather than a transient spike, suggests genuine sympathoadrenal engagement and reflects meaningful intraoperative stress rather than mere baseline variability. These findings reinforce the importance of addressing psychological preparedness and stress management strategies in surgical training curricula. In addition, the stratified analyses based on baseline demographic and clinical factors suggested that physiological stress responses are broadly consistent across trainee subgroups, with the exception of DBP, which was significantly higher in less experienced trainees, highlighting their potentially greater physiological burden. Additionally, according to the PSS-14 results, trainees’ perceived stress level was significantly affected by three items: sex, level of education, and pre-operative use of propranolol. Being a female, having less experience as a surgeon, and not taking propranolol prior to surgery made trainees perceive higher levels of stress.
These findings are supported by those of the previous studies. In a study by Chandra et al, ophthalmic surgeons performing uncomplicated cataract surgery were divided into the consultant and trainee groups In both groups, post-operative values of SBP, DBP, pulse rate (PR), blood cortisol, and urine catecholamines were significantly higher than their pre-operative values. Alternatively, trainee surgeons had a higher SBP, DBP, PR, blood cortisol, urine adrenaline, and urine dopamine when compared to consultants.14 In another study, Yamamoto et al found that HR and urine adrenaline levels of surgeons and nurses during cataract surgery varied based on their level of experience and all stress-related parameters’ values were higher in inexperienced individuals compared to their more experienced peers23 This observation is consistent with other studies, which concluded that stress level was higher in residents and inexperienced surgeons compared to consultants and more experienced ones, whether measured by objective parameters such as heart rate variability (HRV) or blood pressure or reported based on various questionnaires like STAI or the PSS.14,17,18,23–25 Yet, one study found no association between stress level and level of experience.26 Yamamoto et al also found that stress was the highest at the beginning of the surgery, which is in contrast with our findings In our study, stress-related parameters, namely HR and SBP, have increased towards the end of the surgery.23 Similar to our findings, a recent study by Tekin et al found that HR in ophthalmology residents was consistently elevated throughout all phacoemulsification surgery steps compared with baseline, and it was highest during the capsulorhexis step Measuring HR and HRV using Holter monitoring during the surgery, they suggested that this higher stress is probably a result of sustained autonomic stress and sympathetic activation during phacoemulsification surgery.18
Another study by Kaushik et al investigated the effect of complicated cataract surgery on SBP, DBP, MAP (mean arterial pressure), HR, and arterial SpO2 of an experienced ophthalmic surgeon It was discovered that the SBP, DBP, MAP, and HR of the surgeon were significantly higher in the complicated group compared to the uncomplicated group. However, arterial SpO2 was not significantly affected.6 In our study, we found that SBP, DBP, HR, and arterial SpO2 were not related to surgical complications. The explanation for this difference may be that Kaushik et al defined complicated cataract as advanced or severe cataract disease and recorded the subsequent surgeon’s physiologic response triggered when operating on these advanced cataract eyes While in our study, we defined complications differently as intraoperative surgical complications, and the complexity of cataract surgeries was standardized by only including the cataract eyes with grade 2–3 nuclear opacities according to LOCS III.
The sex of surgeons may also affect stress level and associated physiologic parameters. Several studies reported that female surgeons and students are more likely to experience and report higher levels of stress.7,27,28 These findings are consistent with our findings based on the PSS-14, as female residents and fellows reported a higher perceived stress level. However, we did not find a connection between sex and fluctuations in trainees’ HR, SBP, DBP, and arterial SpO2 during cataract surgery. This may be because females define and perceive stress differently, leading to higher reports of stress despite no significant difference in the fluctuations of the mentioned physiological parameters between males and females.29,30
Another strategy for reducing intraoperative stress is to take medication. Propranolol is one of the safest and most widely used medications by residents and surgeons prior to the surgeries to reduce tremors and anxiety, and hence increase efficacy during the surgeries. In our study, no association was found between pre-operative use of propranolol and fluctuations in physiologic parameters during cataract surgery; however, residents who used propranolol significantly scored lower on stress levels based on the PSS-14. Moreover, no complication related to propranolol use was recorded in this study. This finding may partly be explained by the known physiological effects of propranolol, which has been shown to reduce baseline HR and SBP and attenuate their elevation during stress or exercise conditions, while having relatively limited effects on DBP.31 A study by Roizenblatt et al showed that pre-operative use of low-dose beta-blockers can enhance the performance of ophthalmology residents in microsurgeries by reducing hand tremors and their anxiety32 A randomized controlled trial by Elman et al conducted also found that the use of propranolol prior to surgery resulted in a reduction of hand tremors and anxiety levels amongst ophthalmology residents; however, it remained unclear whether these reductions would lead to better surgical performance.33
The present study simultaneously assessed both objective physiological parameters and subjective perceived stress among ophthalmology trainees during phacoemulsification cataract surgery, providing a comprehensive evaluation of cataract surgery-related stress among these trainees. Additionally, the stepwise analysis across different stages of phacoemulsification surgery offers detailed insight into how stress evolves during the procedure. Nonetheless, this study has several limitations. First, the sample size was relatively small, particularly within some subgroups, which may limit the statistical power, generalizability of the findings, and adjustment for confounder variables. Second, the cross-sectional design precludes establishing causal relationships between stress and the evaluated factors. Third, Several factors that may potentially influence intraoperative physiologic responses were not fully controlled in the present study, including surgical duration, the number of prior surgeries performed by each trainee, intraoperative difficulty beyond basic LOCS III grading, fatigue, workload, baseline anxiety, caffeine intake, and the extent of supervisor intervention. Therefore, although increases in SBP and HR observed during surgery may reflect sympathetic activation associated with intraoperative stress, these parameters should be interpreted as indirect physiologic markers rather than definitive measures of stress alone. Consequently, the observed physiologic changes may have been partially affected by additional procedural, environmental, and individual-related factors. The surgical performance parameters, including surgical duration and final outcomes, were also not recorded. It is also noteworthy that the potential differences in trainee stress levels attributable to individual supervising surgeons, as well as the Hawthorne effect, where individuals alter their behavior when aware of being observed,34 were other inherent limitations that could not be fully adjusted. Lastly, the study relied on intra-operative physiological responses and a single self-reported questionnaire (PSS-14), which measures the long-term general perceived stress and may not fully capture the multidimensional nature of stress, particularly during the surgery.
Future studies with larger, multicenter cohorts are recommended to validate these findings and improve generalizability. Incorporating comprehensive psychological assessments and advanced stress biomarkers may provide a more detailed understanding of intraoperative stress and its determinants. Additionally, further studies can investigate the pre-operative use of beta-blockers like propranolol by ophthalmologists as a possible strategy to reduce anxiety and stress during these procedures. Beyond pharmacological approaches, future research should introduce and evaluate targeted interventions such as simulation-based training, mindfulness programs, and structured mentorship to actively alleviate intraoperative stress among ophthalmology trainees, which would significantly enhance the translational value of this line of research.
Conclusion
In conclusion, the physiological responses among ophthalmology trainees increase progressively during phacoemulsification cataract surgery, which may be translated into higher intra-operative stress. This physiologic arousal is reflected by significant rises in SBP and HR, while DBP and arterial SpO2 remain largely unchanged. Less experienced trainees exhibited higher general perceived stress, and this perceived stress was also associated with factors such as sex, level of training, and pre-operative propranolol use, highlighting the need for targeted strategies to optimize trainee well-being and surgical training environments, particularly for those who are more prone to experience higher levels of stress. However, given the observational study design and the role of confounding variables, future studies are warranted to introduce effective stress-reducing interventions.
Data Sharing Statement
The data supporting the findings of this study are not publicly accessible due to participant privacy concerns, but can be obtained from the corresponding author (Alireza Eslampoor) upon reasonable request.
Funding
No funding or financial support was provided for this study.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Jackson M. The stress of life: a modern complaint? Lancet. 2014;383(9914):300–10. doi:10.1016/S0140-6736(14)60093-3
2. Sadeghpour S, Doostparast A, Sadeghpour S, et al. The spectrum of somatic and psychological distress: a novel cross-disciplinary analysis of medical and non-medical students in the academic landscape. BMC Med Educ. 2026;26(1). doi:10.1186/s12909-026-09150-6
3. De Hert S. Burnout in healthcare workers: prevalence, impact and preventative strategies. Local Reg Anesth. 2020;13:171–183. doi:10.2147/lra.S240564
4. Ray A, Gulati K, Rai N. Stress, anxiety, and immunomodulation: a pharmacological analysis. Vitam Horm. 2017;103:1–25. doi:10.1016/bs.vh.2016.09.007
5. Benítez-Agudelo JC, Restrepo D, Navarro-Jimenez E, Clemente-Suárez VJ. Longitudinal effects of stress in an academic context on psychological well-being, physiological markers, health behaviors, and academic performance in university students. BMC Psychol. 2025;13(1):753. doi:10.1186/s40359-025-03041-z
6. Kaushik J, Pannu A, Chaitanya YVK, et al. Effect of complicated ocular surgery in stress-related parameters: a novel outlook into surgeon’s health. Indian J Ophthalmol. 2021;69(9):2282–2286. doi:10.4103/ijo.IJO_3517_20
7. Guglielmetti LC, Gingert C, Holtz A, Westkämper R, Lange J, Adamina M. Nationwide study on stress perception among surgical residents. World J Surg. 2022;46(7):1609–1622. doi:10.1007/s00268-022-06521-0
8. Torkamani-Azar M, Lee A, Bednarik R. Methods and measures for mental stress assessment in surgery: a systematic review of 20 years of literature. IEEE J Biomed Health Inform. 2022;26(9):4436–4449. doi:10.1109/jbhi.2022.3182869
9. Otukoya EZ, Amiri A, Alimohammadi E. Surgeon well-being: a systematic review of stressors, mental health, and resilience. BMC Surg. 2025;25(1):430. doi:10.1186/s12893-025-03180-5
10. Doostparast A, Semnani F, Ghandhari M, et al. Agreement and potential for arithmetic adjustment of anterior segment measurements across IOLMaster 700, Pentacam HR, and sirius. Sci Rep. 2026;16(1). doi:10.1038/s41598-026-42204-9
11. Dimou FM, Eckelbarger D, Riall TS. Surgeon burnout: a systematic review. J Am Coll Surg. 2016;222(6):1230–1239. doi:10.1016/j.jamcollsurg.2016.03.022
12. Dyrbye LN, West CP, Satele D, et al. Burnout among US medical students, residents, and early career physicians relative to the general US population. Acad Med. 2014;89(3):443–451. doi:10.1097/ACM.0000000000000134
13. Ansari AS, Tung ASW, Wright DM, Watts P, Williams GS. Stress and cataract surgery: a nationwide study evaluating surgeon burnout. Eur J Ophthalmol. 2023;33(4):1640–1649. doi:10.1177/11206721231154611
14. Chandra T, Khan P, Khan L. Study to evaluate stress among ophthalmic surgeons with different levels of surgical experience. Clin Ophthalmol. 2020;14:3535–3540. doi:10.2147/opth.S266501
15. Gharaee H, Jahani M, Banan S. A comparative assessment of intraoperative complication rates in resident-performed phacoemulsification surgeries according to Najjar-Awwad preoperative risk stratification. Clin Ophthalmol. 2020;14(null):1329–1336. doi:10.2147/OPTH.S252418
16. Melega MV, Pessoa Cavalcanti Lira R, da Silva IC, et al. Comparing resident outcomes in cataract surgery at different levels of experience. Clin Ophthalmol. 2020;14(null):4523–4531. doi:10.2147/OPTH.S285967
17. Cap V, Palkovits S, Bijak M, Ruiss M, Schmoll M, Findl O. New approach to quantifying acute stress in cataract surgeons to investigate the relationship between surgeon experience and intraoperative stress. J Cataract Refract Surg. 2022;48(5):549–554. doi:10.1097/j.jcrs.0000000000000798
18. Tekin K, Yalcinsoy KO, Tutan EO, Bilir A, Uzel MM, Tekin MI. From incision to implantation: holter-based stress profiling in ophthalmology residents during cataract surgery. Graefes Arch Clin Exp Ophthalmol. 2026. doi:10.1007/s00417-026-07189-1
19. Cohen S, Kamarck T, Mermelstein R. Perceived stress scale. Measuring Stress. 1994;10(2):1–2.
20. Lee EH, Chung BY, Suh CH, Jung JY. K orean versions of the P erceived S tress S cale (PSS‐14, 10 and 4): psychometric evaluation in patients with chronic disease. Scand J Caring Sci. 2015;29(1):183–192. doi:10.1111/scs.12131
21. She Z, Li D, Zhang W, Zhou N, Xi J, Ju K. Three versions of the perceived stress scale: psychometric evaluation in a nationally representative sample of Chinese adults during the COVID-19 pandemic. Int J Environ Res Public Health. 2021;18(16):8312. doi:10.3390/ijerph18168312
22. Chaaya M, Osman H, Naassan G, Mahfoud Z. Validation of the Arabic version of the Cohen perceived stress scale (PSS-10) among pregnant and postpartum women. BMC Psychiatry. 2010;10(1):1–7. doi:10.1186/1471-244X-10-111
23. Yamamoto A, Hara T, Kikuchi K, Hara T, Fujiwara T. Intraoperative stress experienced by surgeons and assistants. SLACK Incorporated Thorofare, NJ; 1999:27–30.
24. Weenk M, Alken APB, Engelen L, Bredie SJH, van de Belt TH, van Goor H. Stress measurement in surgeons and residents using a smart patch. Am J Surg. 2018;216(2):361–368. doi:10.1016/j.amjsurg.2017.05.015
25. Kikuchi K, Okuyama K, Yamamoto A, Hara T, Hara T. Intraoperative stress for surgeons and assistants. J Ophthalmic Nurs Technol. 1995;14(2):
26. Kuhn EW, Choi YH, Schönherr M, et al. Intraoperative stress in cardiac surgery: attendings versus residents. J Surg Res. 2013;182(2):e43–9. doi:10.1016/j.jss.2012.11.011
27. Ribeiro F, Mussi FC, Pires C, Silva RMD, Macedo TTS, Santos C. Stress level among undergraduate nursing students related to the training phase and sociodemographic factors. Rev Lat Am Enfermagem. 2020;28:e3209. doi:10.1590/1518-8345.3036.3209
28. Mavroudis CL, Landau S, Brooks E, et al. The relationship between surgeon gender and stress during the Covid-19 pandemic. Ann Surg. 2021;273(4):625–629. doi:10.1097/sla.0000000000004762
29. Weekes NY, MacLean J, Berger DE. Sex, stress, and health: does stress predict health symptoms differently for the two sexes? Stress Health. 2005;21(3):147–156. doi:10.1002/smi.1046
30. Brivio E, Lopez JP, Chen A. Sex differences: transcriptional signatures of stress exposure in male and female brains. Genes Brain Behav. 2020;19(3):e12643. doi:10.1111/gbb.12643
31. Matsuura H, Masaoka S, Kanazawa I, Murano S, Tsuchioka Y, Kajiyama G. Comparison of the acute effects of acebutolol and propranolol on blood pressure, heart rate and hormonal changes during graded treadmill exercise in patients with essential hypertension. Jpn J Med. 1989;28(1):8–15. doi:10.2169/internalmedicine1962.28.8
32. Roizenblatt M, Dias Gomes Barrios Marin V, Grupenmacher AT, et al. Association of weight-adjusted caffeine and β-blocker use with ophthalmology fellow performance during simulated vitreoretinal microsurgery. JAMA Ophthalmol. 2020;138(8):819–825. doi:10.1001/jamaophthalmol.2020.1971
33. Elman MJ, Sugar J, Fiscella R, et al. The effect of propranolol versus placebo on resident surgical performance. Trans Am Ophthalmol Soc. 1998;96:283–291. discussion 291-4.
34. Kaiser KP, Turgut F, Ernst S-CK, et al. Implementation of a modified risk stratification score in cataract surgery at a Swiss public hospital. Clin Ophthalmol. 2025;19(null):3307–3316. doi:10.2147/OPTH.S544354
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.