Back to Journals » Journal of Healthcare Leadership » Volume 17
Physician Leadership and Its Effect on Physician Burnout and Satisfaction During the COVID-19 Pandemic
Authors Spilg EG ![]() , McNeill K, Dodd-Moher M
, McNeill K, Dodd-Moher M ![]() , Dobransky JS, Sabri E, Maniate JM, Gartke KA
, Dobransky JS, Sabri E, Maniate JM, Gartke KA
Received 30 August 2024
Accepted for publication 14 January 2025
Published 27 February 2025 Volume 2025:17 Pages 49—61
DOI https://doi.org/10.2147/JHL.S487849
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Zhanming Liang
Edward G Spilg,1– 3 Kylie McNeill,1 Melanie Dodd-Moher,2,4 Johanna Suzanne Dobransky,2,4 Elham Sabri,2 Jerry M Maniate,1– 3 Kathleen A Gartke2,4
1Department of Medicine, University of Ottawa, Ottawa, ON, Canada; 2Clinical Epidemiology Program, Ottawa Hospital Research Institute, Ottawa, ON, Canada; 3Bruyère Research Institute, Ottawa, ON, Canada; 4Division of Orthopaedic Surgery, the Ottawa Hospital, Ottawa, ON, Canada
Correspondence: Edward G Spilg, Department of Medicine, University of Ottawa, 1053 Carling Ave, Ottawa, ON, K1Y 4E9, Canada, Tel +1 613 798 5555, Email [email protected]
Purpose: Physician burnout is a global issue associated with low job satisfaction, decreased quality of patient care, reduced productivity, and early retirement from clinical practice. We sought to evaluate the impact of the leadership qualities of direct physician supervisors on the burnout and professional satisfaction of the physicians they supervise.
Methods: An online survey was distributed by Email to all staff physicians practicing at a large Canadian academic tertiary care hospital. The primary outcome was the prevalence of burnout and professional satisfaction, assessed using the 2-item Maslach Burnout Inventory and a single item 5-point Likert scale rating, respectively. The secondary outcome was the relationship between composite leadership score and burnout/satisfaction, with leadership assessed by the 12-item Mayo Clinic Participatory Management Leadership Index.
Results: Out of the 1176 physicians surveyed, 383 (32.6%) responded (51.2% male; 41.5% female). Overall, 41.7% of physicians reported at least one symptom of burnout (40.0% reported high emotional exhaustion; 15.3% reported high depersonalization). 40.1% of physicians reported being satisfied with the organization, 26.3% were neutral, and 33.6% were dissatisfied. On multivariate analysis adjusting for age, sex, duration of employment at the institution, and specialty, each one-point increase in composite leadership score was associated with a 3.1% decrease in the likelihood of burnout (p = 0.0017), and a 6.6% increase in the likelihood of satisfaction (p < 0.0001).
Conclusion: Physician burnout is prevalent and positive leadership qualities of direct supervisors decreases the likelihood of burnout in physicians and increases the likelihood of their satisfaction with the organization.
Trial Registration: ClinicalTrials.gov; Identifier: NCT04896307.
Keywords: physician wellness, burnout, satisfaction, leadership
Introduction
Physician burnout is a global issue characterized by emotional exhaustion, depersonalization, and low levels of personal accomplishment.1 Burnout symptoms as high as 50% have been documented worldwide2–6 and according to the 2021 National Physician Health Survey, it is experienced by 53% of Canadian physicians and resident physicians.7 This can have devastating consequences on physician health8–10 and is associated with low job satisfaction,11,12 decreased patient satisfaction13–16 and quality of care,17–21 reduced productivity, high job turnover, and early retirement from clinical practice.22–24 Healthcare expenditures are also indirectly affected by higher rates of medical errors,12,13,23,25 absenteeism, and lower job productivity,22,24 leading to an estimated cost burden ranging from $168.2 million to $252.4 million in Canada.23 Numerous factors drive physician burnout including heavy workloads, staff shortages, inefficiencies of Electronic Health Record (EHR) systems, administrative burden, and high patient volume.26,27
A number of studies have been published stating the high rates of stress and burnout of physicians within our Canadian tertiary care centre including during the implementation of a new EHR in the months preceding the COVID-19 pandemic.28 Furthermore, physicians within our healthcare facility have expressed difficulties with maintaining their wellness in the face of individual and organizational challenges.8,29 During the height of the pandemic in our Canadian tertiary care center, physicians faced added organizational stressors including the implementation of PPE requirements and new safety procedures, changes in clinical directives, visitor restrictions, reduced support staff and resources, and a rapid shift to virtual care, which could lead to moral distress if providers felt it compromised patient care. For those in surgical specialties, frequent operating room closures contributed to ever-increasing waitlists, and a potential decrease in income given the fee-for-service model in our organization. This was all in the backdrop of the province of Ontario, Canada, releasing the Adult Critical Care Clinical Emergency Standard of Care for Major Surge (Emergency Standard of Care [ESoC]) in 2021, a triage framework to guide the allocation of critical care resources in the expectation that intensive care units would be overwhelmed.30
Evidence suggests that burnout is reversible and even preventable.31 Both organization-directed and physician-directed interventions have been shown to result in meaningful reductions in burnout among physicians.32,33 Recently, the importance of organizational structures and environment,34–37 has been highlighted as having a significant effect on the health of the physician, the patient, and the organization.12,20,34,35 Leadership in particular has a profound impact on reducing burnout and promoting job satisfaction.36–39 A recent study by Shanafelt and colleagues performed at the Mayo Clinic in the United States, found that positive leadership qualities of direct physician supervisors decrease the likelihood of burnout and increases satisfaction in the physicians they supervise.12
The results of this study underscore the importance of leadership as a modifiable factor to address physician burnout, however, to our knowledge there are no studies that examine this relationship in a Canadian healthcare setting. Given significant differences between American and Canadian healthcare systems, including the publicly funded and a fee-for-service physician renumeration model of the Canadian system,40 it is important to assess the validity of these results in this setting. Moreover, the COVID-19 pandemic introduced many new organizational stressors,41–43 offering valuable insight into the impact of leadership during highly stressful periods. This context allows for the unique opportunity to investigate whether positive leadership qualities contribute similarly to physician well-being in spite of the larger socioeconomic and political factors that impacted healthcare delivery during this period.
Our study objectives were first, to assess the prevalence of burnout and professional satisfaction of physicians working at a large Canadian academic tertiary care hospital during the COVID-19 pandemic and second, to evaluate the relationship between the leadership qualities of direct physician supervisors and the well-being and burnout of their physicians during this time.
Materials and Methods
Study Design
We conducted a cross-sectional online survey study targeting all staff physicians at a large Canadian academic tertiary care hospital between May 2021 and February 2022, during the COVID-19 pandemic. We sought to replicate the design of Shanafelt and colleagues’ study conducted at the Mayo Clinic.12 This large academic health sciences system consists of three campuses (1 ambulatory care and 2 tertiary care sites) and over 12,600 employees, physicians, and trainees.
Study recruitment involved a two-step process. First, one of the study authors attended a meeting for each division within the hospital (or department meeting, without separate divisions within a department) to give a 10-minute presentation on the study’s objectives. Second, on the day following the presentation, an Email with a link to the survey was sent to every physician member of that division/department by the administrator responsible for that mailing list. Follow-up reminder emails were sent at one and two weeks following the email, for a total of three emails. This was completed for 42 of the 44 divisions/departments. Our survey was hosted by LimeSurvey, with all appropriate licensing, and was piloted to ensure functionality before launch.
This study was approved by the Ottawa Health Science Network Research Ethics Board (REB#20200431-01H) and complies with the Declaration of Helsinki. Implied consent was obtained from participants by completing the survey following provision of information regarding the purpose of the study, time involved, risks/benefits, withdrawal, and confidentiality.
Survey
The survey consisted of 19 questions over 9 pages: 4 demographic questions, 12 questions rating the leadership qualities of their direct supervisor, 2 questions assessing burnout, and 1 question regarding overall satisfaction with the hospital. The survey was voluntary and anonymous. We enabled backwards navigation so respondents could review their responses and used cookies to prevent repeat participation. This study is reported as per the Checklist for Reporting Results of Internet E-Surveys (CHERRIES).44
Demographics
Respondents were asked for their sex, age, duration of employment, and to select the name of their immediate supervisor (ie, Division Head, Department Head, or Chief of Staff) from a drop-down menu. To account for potential recent changes in physician leader, instructions were given to evaluate the leader who was in position in December 2020.
Leadership
We employed the 12-item Mayo Clinic Participatory Management Leadership Index12,34,35,45,46 to assess the leadership qualities of respondents’ immediate supervisor. This instrument was designed and validated by Shanafelt and colleagues to evaluate dimensions of leadership that drive engagement among team members.34 For respondents who completed at least 9 out of 12 items, a total composite score was calculated by summing the items, with higher scores indicative of more effective leadership.
Burnout
To assess burnout, we used the 2-item Maslach Burnout Inventory (MBI)47–49 adapted from the original 22-item MBI.1,50 This inventory uses single-item measures to assess the emotional exhaustion and depersonalization dimensions of burnout. Respondents indicated how often they experience these symptoms on a 7-point Likert scale (0=Never, 1=A few times a year or less, 2=Once a month or less, 3=A few times a month, 4=Once a week, 5=A few times a week, 6=Every day). A dichotomous burnout variable was determined by respondents with scores ≥4 on at least one of the two items.12,34,35,45–48
Satisfaction
Overall satisfaction with the organization was assessed using a single item: “Considering everything, how would you rate your overall satisfaction with [name of the hospital] as a whole at the present time?”. Responses were provided on 5-point Likert scale and were dichotomized into either dissatisfied or satisfied (respondents who answered “very satisfied” or “satisfied” with a organization).12,35,45,46
Statistical Analysis
We calculated basic summary statistics with continuous variables and categorical variables summarized using means ± standard deviations and frequencies and percentages, respectively. Chi-squared tests of independence (χ2) and independent samples t-tests were used to compare categorical variables and continuous variables, respectively. Pearson correlation coefficients were calculated to assess relationships between leadership ratings and emotional exhaustion, depersonalization, and satisfaction. Two-sided tests were performed to assess if the linear relationship was statistically significant. We then performed two separate multivariate logistic regressions to evaluate the relationship between composite leadership score and the outcomes of burnout and satisfaction, respectively. In both models, we adjusted for age, sex, specialty, and duration of employment. Adjusted odds ratios (aOR) with 95% confidence intervals (95% CI) as well as p values are reported. To explore burnout and satisfaction at the division/department level, we first calculated the mean composite leadership score for each of the 34 division/department leaders with at least four evaluations (mean = 46.6 ± 7.0; range = 33.8–57.4) based on the collective rating of all responding physicians they supervised. Then we evaluated the Pearson correlation coefficient between the mean composite leadership score and the prevalence of burnout and satisfaction for the division/department. All statistical analyses were conducted using SAS version 9.4 (SAS Institute, Cary, NC) and statistical significance was set at p < 0.05.
Results
Of the 1176 physicians surveyed, 383 (32.6%) responded (51.2% male; 41.5% female). The participation rate was 383/398 (96.2%), and the completion rate was 358/383 (93.5%) (see Figure 1). Demographic characteristics and rates of burnout and satisfaction of respondents are presented in Table 1. Overall, 41.7% reported at least one symptom of burnout; 40.0% reporting high emotional exhaustion and 15.3% reporting high depersonalization. Collectively, 40.1% of physicians reported being either very satisfied or satisfied with the organization, 26.3% were neutral, and 33.6% were either dissatisfied or very dissatisfied.
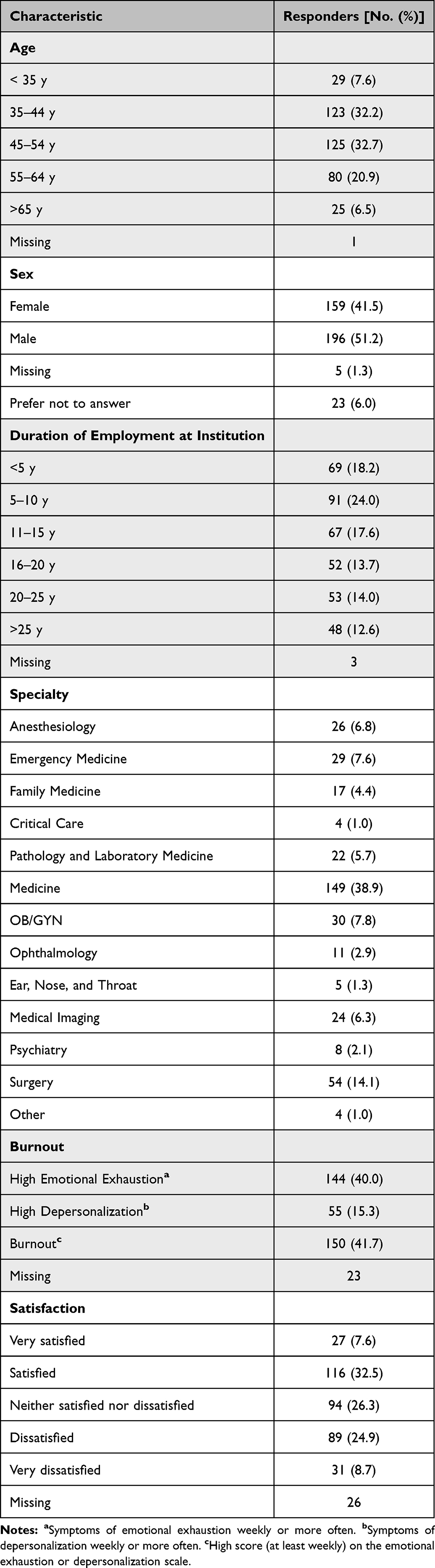 |
Table 1 Demographic Characteristics, Burnout, and Satisfaction of the 383 Responders |
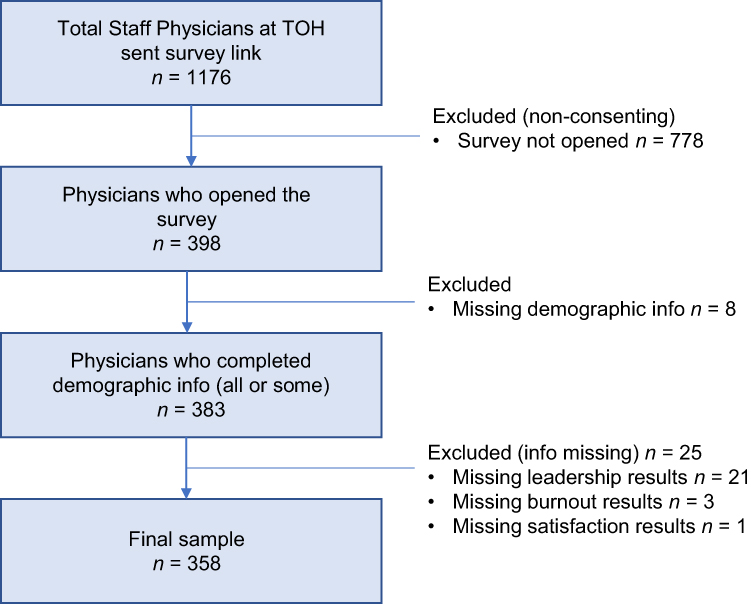 |
Figure 1 Flow chart of study sample. |
Physicians’ ratings of their leader in the 12 leadership dimensions assessed, and the mean scores in each dimension by burnout and satisfaction are shown in Supplemental Tables 1 and 2, respectively. All of the 12 dimensions demonstrated a statistically significant association with burnout and satisfaction. The prevalence of burnout and satisfaction in respondents rating their leader favourably (agree or strongly agree) and unfavourably (disagree or strongly disagree) in each of the leadership dimensions is shown in Table 2. Certain leadership dimensions were more strongly associated with burnout, including “My leader is interested in my opinion” (p = 0.0006), “empowers me to do my job” (p = 0.0017), and “recognizes me for a job well done” (p = 0.0021). There was a weak negative correlation between composite leadership score and both emotional exhaustion (r = −0.206, p = <0.0001) and depersonalization (r = −0.176, p = 0.0009) and a moderate positive correlation between composite leadership score and satisfaction (r = 0.302, p = <0.0001). This indicates that the higher the leadership score participants gave, the lower their emotional exhaustion and depersonalization, and the higher their level of satisfaction.
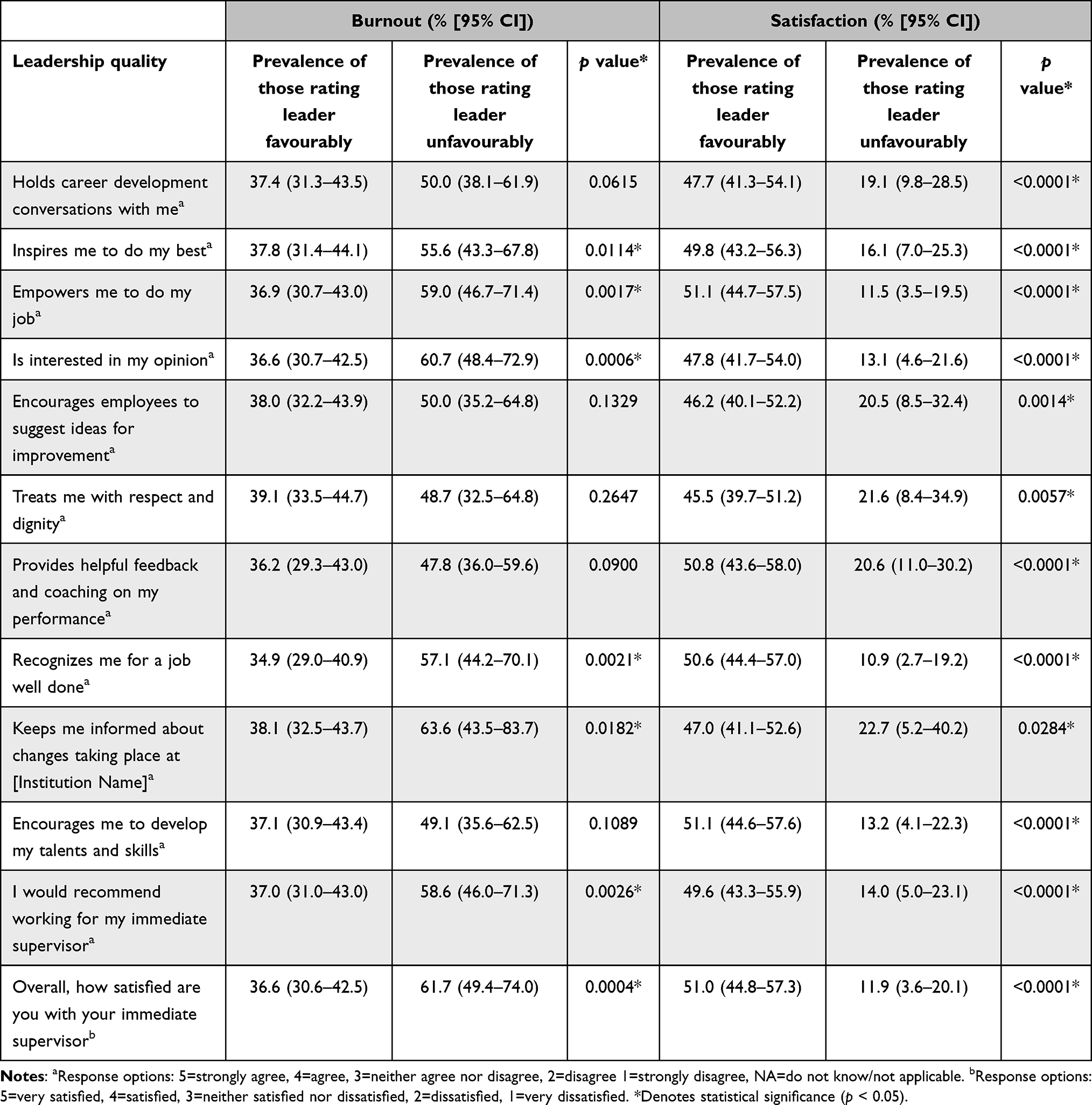 |
Table 2 Leadership Qualities of Immediate Physician Supervisors and the Prevalence of Burnout and Satisfaction in Physicians They Supervise |
After adjusting for age, sex, specialty, and duration of employment, we found that each one-point increase in composite leadership score was associated with a 3.1% decrease in the likelihood of burnout (aOR: 0.969; 95% CI, 1.2–5.0, p = 0.0017), and a 6.6% increase in the likelihood of satisfaction (aOR: 1.066; 95% CI, 4.1–9.2, p < 0.0001) (Figure 2). At the department level (see Figure 3), a weak negative correlation (r = −0.371, p = 0.0474) was found between the mean composite leader rating and the rate of burnout. No relationship was observed between mean leadership score and the rate of satisfaction (r = 0.199, p = 0.300).
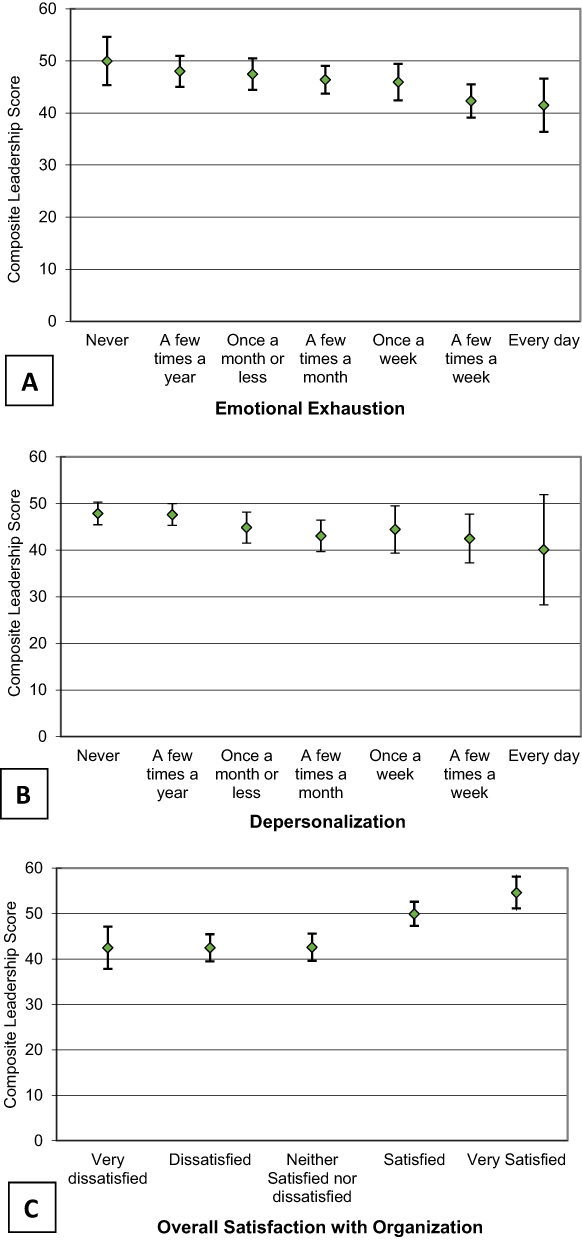 |
Figure 2 Relationship between mean composite leadership score and burnout and satisfaction. (A) Relationship between mean composite leadership score of the immediate supervisor and physician emotional exhaustion (correlation coefficient = −0.206, p < 0.0001). (B) Relationship between mean composite leadership score of the immediate supervisor and physician depersonalization (correlation coefficient = −0.176, p < 0.001). (C) Relationship between mean composite leadership score of the immediate supervisor and physician and satisfaction (correlation coefficient = 0.302, p < 0.0001). Error bars indicate 95% CI. |
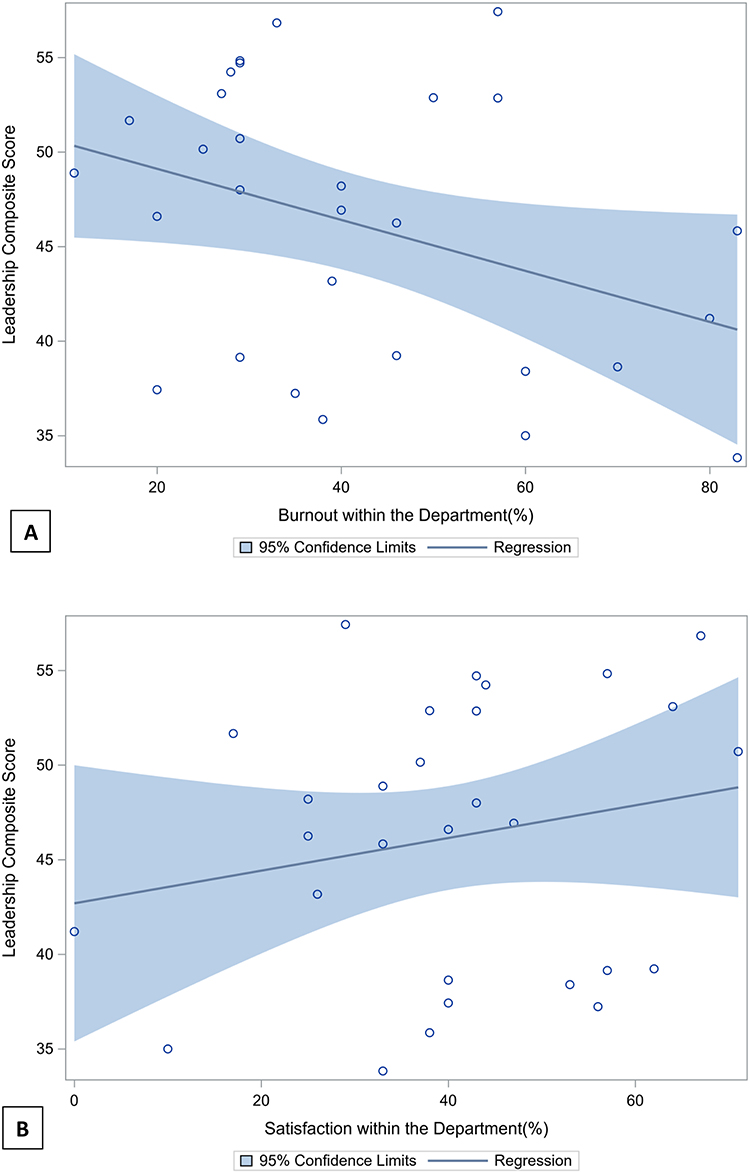 |
Figure 3 Composite leadership score and rate of burnout and satisfaction at the division/department level. (A) Mean composite leadership score and rate of burnout at the division/department level (correlation coefficient = −0.371, p = 0.0474). (B) Mean composite leadership score and rate of satisfaction at the division/department level (correlation coefficient = 0.199, p = 0.300). |
Discussion
We employed an online survey to assess the prevalence of burnout and satisfaction of physicians at a large Canadian academic tertiary care hospital, and to evaluate the relationship between the leadership qualities of direct physician supervisors and the well-being of their staff. Overall, 41.7% of respondents reported at least one symptom of burnout and 33.6% were either dissatisfied or very dissatisfied with the organization. After adjustment, each one-point increase in the composite leadership score of supervisors was associated with a 3.1% decrease in the likelihood of burnout, and a 6.6% increase in the likelihood of satisfaction in the physicians they supervised. Our study further substantiates the prevalence of burnout among physicians and is the first example of research supporting the relationship between leadership quality and physician burnout and satisfaction in a Canadian healthcare setting.
Overall, the prevalence of burnout in our study was similar to a recent report on Canadian physicians (52%)7 and a study on academic physicians in a Canadian hospital (49%).8 Our findings related to leadership and burnout and satisfaction paralleled those of Shanafelt et al’s Mayo Clinic study12 closely, with each one-point increase in leadership score reducing the likelihood of burnout by 3.1% (vs 3.3% in Shanafelt’s work) and increasing satisfaction by 6.6% (compared to their 9.0%). Although our study’s lower response rate necessitates cautious interpretation, these results offer preliminary support for the generalizability of the leadership-burnout and leadership-satisfaction relationships to the Canadian healthcare landscape. This is true despite important contextual differences between Canadian and American systems, including workload, scheduling, compensation, and insurance coverage.40,41 Further, our study occurred during the COVID-19 pandemic, whereas Shanafelt’s took place pre-pandemic. The amount of variance accounted for by leadership in burnout and satisfaction remained consistent, suggesting that leadership may contribute similarly to well-being despite other external factors.
While Shanafelt et al reported a significant link between composite leadership score and burnout and satisfaction at the division/department level12, our findings did not reveal such a relationship. This is possibly due to our smaller sample size, higher dilution of votes per leader and resultant lower statistical power per leader. Further research with larger sample sizes would be instrumental in validating these findings. Additionally, a recent study showed differences in perceived organizational support among different specialties,41 so future studies might explore the differential impact of leadership across specialties. For instance, it is possible that surgical specialties may benefit from different leadership traits, than specialties with more intensive patient-physician interaction, such as family medicine or psychiatry.
Practical Implications
The association between physician leadership, burnout, and satisfaction has significant implications for healthcare systems. Interventions aimed at improving physician leadership, such as training programs that emphasize emotional intelligence, team building, and conflict resolution, may be effective in reducing burnout rates. While frontline hospitals in the US have pioneered programs to identify, develop, and equip physician leaders32,33,37,51,52, such programs are not widespread in Canada. Applying the principles outlined in the Mayo Leadership Index, there is an imperative to establish and expand leadership development programs across Canada.
For senior hiring personnel, our study suggests that it may be important to prioritize the recruitment of physician leaders based not only on clinical expertise but on their leadership capabilities. Leaders who effectively support their staff may foster a more resilient workforce, ultimately enhancing physician well-being and patient care. Finally, for those physicians currently in leadership positions, the Mayo Leadership Index offers a number of actionable items that can be implemented immediately to positively influence their teams. Practical actions such as keeping staff informed about institutional changes, conducting career development discussions, soliciting feedback, and encouraging team members to contribute ideas, offer straightforward yet impactful approaches to fostering a supportive work environment.
Future Directions in the Area of Study
Longitudinal studies examining physician burnout and satisfaction before and after a leadership training intervention45, would allow for evaluation of causality, strengthening the relationship between leadership and burnout. This could also involve further examination of whether certain dimensions in the Leadership Index have a greater effect on well-being, thereby providing focus for both leadership training programs and immediate action items for current physician leaders. In our study, satisfaction with the organization was measured using a single item; a method that can have low sensitivity and reliability. While this approach was chosen for consistency with previous studies,12 a validated scale to assess satisfaction (eg, the Job Descriptive Index (JDI)53) would improve reliability and provide more detail on specific factors contributing to satisfaction or dissatisfaction. Similarly, the Professional Fulfillment Index (PFI)54 includes items assessing exhaustion, interpersonal engagement, and medical errors, and has been used recently to assess the relationship between professional fulfillment and leadership behaviours.55 The benefits of these more detailed measures would need to be balanced with the potential effect on survey completion rate, given the length of the JDI (78 items), PFI (16 items), and other similar scales.56
Limitations
This study has several limitations. First, despite efforts to encourage participation through a two-step recruitment strategy, our response rate of 32.6% was much lower than the 72.2% rate achieved by Shanafelt et al,12 although we did get representation from all 44 divisions/departments within the hospital. This possibly introduced selection bias, as it is conceivable that those dissatisfied with their leaders or organization are more likely to respond, or alternatively, those who are burned out may be less likely to take the time to respond. Further, data was not collected on non-responders, so we were unable to assess any differences in characteristics between responders and non-responders. Some changes in leadership may have diluted results for those divisions/departments where the leader changed during the study period. We attempted to mitigate this effect by instructing respondents to rate their leader that was in post for at least six months. As a cross-sectional study we cannot determine causality or the directionality of observed relationships. However, this study was a necessary first step, providing preliminary data and justification for a larger scale, longitudinal trial with a leadership training intervention. Finally, as a single-center study at a large academic health sciences system these results may not be generalizable to other settings. Future studies should include multiple centers across different countries and different practice settings, including community and urgent care clinics, secondary care, and community hospitals. It is notable, however, that our results are consistent with those of Shanafelt et al,12 which was performed at 3 large academic campuses and a group of community-based hospitals in the United States. Given the limited knowledge available on this topic in Canada, this study adds a valuable starting point for expanding knowledge and training opportunities in this field.
Conclusion
Overall, 41.7% of physicians in our study reported burnout. Positive leadership qualities of direct supervisors decrease the likelihood of burnout in physicians and increase the likelihood of their satisfaction with the organization. This could inform future organizational directives for leader recruitment and development that in turn will positively affect physicians’ well-being.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ottawa Health Science Network Research Ethics Board (REB#20200431-01H) and complies with the Declaration of Helsinki. Implied consent was obtained from participants by completing the survey following provision of information regarding the purpose of the study, time involved, risks/benefits, withdrawal, and confidentiality.
Consent for Publication
All authors accepted the publication of the manuscript.
Funding
A one-time grant through The Ottawa Hospital Academic Medical Association (TOHAMO) funded this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Maslach C, Jackson S, Leiter M. Maslach Burnout Inventory Manual.; 1996. Available from: www.mindgarden.com.
2. Linzer M, Visser M, Oort F, Smets E, McMurray J, de Haes H. Predicting and preventing physician burnout: results from the United States and the Netherlands. Am J Med. 2001;111(2):170–175. doi:10.1016/S0002-9343(01)00814-2
3. Schaufeli W, Leiter M, Maslach C. Burnout: 35 years of research and practice. Career Dev Int. 2009;14(3):204–220. doi:10.1108/13620430910966406
4. Klein J, Grosse Frie K, Blum K, von Dem Knesebeck O. Burnout and perceived quality of care among German clinicians in surgery. Int J Qual Health Care. 2010;22(6):525–530. doi:10.1093/intqhc/mzq056
5. Panagopoulou E, Montgomery A, Benos A. Burnout in internal medicine physicians: differences between residents and specialists. Eur J Intern Med. 2006;17(3):195–200. doi:10.1016/j.ejim.2005.11.013
6. Arigoni F, Bovier P, Sappino AP. Trend in burnout among Swiss doctors. Swiss Med Wkly. 2010;140(AUGUST). doi:10.4414/smw.2010.13070
7. Canadian Medical Association. National Physician Health Survey 2021.; 2022.
8. Spilg E, McNeill K, Sabri E, et al. A cross-sectional study of the interrelationship between burnout, empathy and resilience in academic physicians. Psychol Health Med. 2022;27(8):1813–1820. doi:10.1080/13548506.2021.1954670
9. Oreskovich M, Kaups K, Balch CM, et al. Prevalence of Alcohol Use Disorders Among American Surgeons. Arch Surg. 2012;147(2):168–174. doi:10.1001/archsurg.2011.1481
10. Shanafelt T, Balch C, Dyrbye L, et al. Special report - suicidal ideation among American surgeons. Arch Surg. 2011;146(1):54–62. doi:10.1001/archsurg.2010.292
11. Weng HC, Hung CM, Liu YT, et al. Associations between emotional intelligence and doctor burnout, job satisfaction and patient satisfaction. Med Educ. 2011;45(8):835–842. doi:10.1111/j.1365-2923.2011.03985.x
12. Shanafelt T, Gorringe G, Menaker R, et al. Impact of organizational leadership on physician burnout and satisfaction. Mayo Clin Proc. 2015;90(4):432–440. doi:10.1016/j.mayocp.2015.01.012
13. Shanafelt T, Balch C, Bechamps G, et al. Burnout and medical errors among American surgeons. Ann Surg. 2010;251(6):995–1000. doi:10.1097/SLA.0b013e3181bfdab3
14. Wallace J, Lemaire J, Ghali W. Physician wellness: a missing quality indicator. Lancet. 2009;374(9702):1714–1721. doi:10.1016/S0140-6736(09)61424-0
15. Firth-Cozens J, Greenhalgh J. Doctors’ perceptions of the links between stress and lowered clinical care. Soc Sci Med. 1997;44(7):1017–1022. doi:10.1016/S0277-9536(96)00227-4
16. Grol R, Mokkink H, Smits A, et al. Work satisfaction of general practitioners and the quality of patient care. Fam Pract. 1985;2(3):128–135.
17. Bianchi R, Schonfeld IS, Laurent E. Burnout-depression overlap: a review. Clin Psychol Rev. 2015;36:28–41. doi:10.1016/j.cpr.2015.01.004
18. Williams E, Manwell L, Konrad T, Linzer M. The relationship of organizational culture, stress, satisfaction, and burnout with physician-reported error and suboptimal patient care: results from the MEMO study. Health Care Management. 2007;32(3):203–212.
19. Welp A, Meier L, Manser T. Emotional exhaustion and workload predict clinician-rated and objective patient safety. Front Psychol. 2015;6:5. doi:10.3389/fpsyg.2014.01573
20. West C, Dyrbye L, Shanafelt T. Physician burnout: contributors, consequences and solutions. J Intern Med. 2018;283(6):516–529. doi:10.1111/joim.12752
21. Halbesleben J, Rathert C. Linking physician burnout and patient outcomes: exploring the dyadic relationship between physicians and patients. Healthcare Management Rev. 2008;33(1):29–39. doi:10.1097/01.HMR.0000304493.87898.72
22. Dewa C, Loong D, Bonato S, Thanh NX, Jacobs P. How does burnout affect physician productivity? A systematic literature review. BMC Health Serv Res. 2014;14(1). doi:10.1186/1472-6963-14-325
23. Dewa C, Jacobs P, Thanh NX, Loong D. An estimate of the cost of burnout on early retirement and reduction in clinical hours of practicing physicians in Canada. BMC Health Serv Res. 2014;14(1). doi:10.1186/1472-6963-14-254
24. Shanafelt T, Mungo M, Schmitgen J, et al. Longitudinal study evaluating the association between physician burnout and changes in professional work effort. Mayo Clin Proc. 2016;91(4):422–431. doi:10.1016/j.mayocp.2016.02.001
25. Dyrbye L, Shanafelt T, Physician burnout a potential threat to successful health care reform. J Am Med Assoc. 2011;305(19):2009–2010. doi:10.1001/jama.2011.652
26. Goldberg DG, Soylu T, Hoffman CF, Kishton RE, Cronholm PF. Anxiety, COVID, burnout and now depression”: a qualitative study of primary care clinicians perceptions of burnout. J Gen Intern Med. 2024;39(8):1317–1323. doi:10.1007/s11606-023-08536-2
27. Sipos D, Goyal R, Zapata T. Addressing burnout in the healthcare workforce: current realities and mitigation strategies. Lancet Reg Health - Europe. 2024;42:100961. doi:10.1016/j.jpsychires
28. Spilg EG, Kuk H, Ananny L, et al. The impact of Stress Management and Resilience Training (SMART) on academic physicians during the implementation of a new health information system: an exploratory randomized controlled trial. PLoS One. 2022;17(4 April):e0267240. doi:10.1371/journal.pone.0267240
29. Ladonna KA, Cowley L, Touchie C, Leblanc VR, Spilg EG. Wrestling with the invincibility myth: exploring physicians’ resistance to wellness and resilience-building interventions. Acad Med. 2022;97(3):436–443. doi:10.1097/ACM.0000000000004354
30. Heidinger BA, Downar A, Frolic A, Downar J, Isenberg SR. Physician and administrator experience of preparing to implement Ontario’s intensive care unit triage emergency standard of care during the COVID-19 pandemic: a qualitative study. CMAJ Open. 2023;11(5):E838–E846. doi:10.9778/cmajo.20220168
31. Collier R. Physician burnout a major concern. Can Med Assoc J. 2017;189(39):E1236–E1237. doi:10.1503/cmaj.1095496
32. Panagioti M, Panagopoulou E, Bower P, et al. Controlled interventions to reduce burnout in physicians a systematic review and meta-analysis. JAMA Intern Med. 2017;177(2):195–205. doi:10.1001/jamainternmed.2016.7674
33. West C, Dyrbye L, Erwin P, Shanafelt T. Interventions to prevent and reduce physician burnout: a systematic review and meta-analysis. Lancet. 2016;388(10057):2272–2281. doi:10.1016/S0140-6736(16)31279-X
34. Shanafelt T, Wang H, Leonard M, et al. Assessment of the association of leadership behaviors of supervising physicians with personal-organizational values alignment among staff physicians. JAMA Network Open. 2021;4(2):e2035622. doi:10.1001/jamanetworkopen.2020.35622
35. Dyrbye L, Leep Hunderfund A, Winters R, et al. The relationship between residents’ perceptions of residency program leadership team behaviors and resident burnout and satisfaction. Acad Med. 2020;95(9):1428–1434. doi:10.1097/ACM.0000000000003538
36. Shanafelt T, Noseworthy J. Executive Leadership and Physician Well-being: nine Organizational Strategies to Promote Engagement and Reduce Burnout. Mayo Clin Proc. 2017;92(1):129–146. doi:10.1016/j.mayocp.2016.10.004
37. Montgomery A. The inevitability of physician burnout: implications for interventions. Burn Res. 2014;1(1):50–56. doi:10.1016/j.burn.2014.04.002
38. Hu JS, Pangaro LN, Andrada BMG, Ceasar RC, Phillips JL. Physician leadership and burnout: the need for agency; a qualitative study of an academic institution. J Healthc Leadersh. 2024;16:121–130. doi:10.2147/JHL.S419203
39. Montgomery AJ. The relationship between leadership and physician well-being: a scoping review. J Healthc Leadersh. 2016;8:71–80. doi:10.2147/JHL.S93896
40. Gumas ED, Shah A, Gunja MZ, Williams RD. Mirror, Mirror 2024: a Portrait of the Failing U.S. Health System – Comparing Performance in 10 Nations.; 2024.
41. Carlasare LE, Wang H, West CP, et al. Associations between organizational support, burnout, and professional fulfillment among US physicians during the first year of the COVID-19 Pandemic. J Healthc Manag. 2024;69(5):368–386. doi:10.1097/JHM-D-23-00124
42. Frenkel MO, Pollak KM, Schilling O, et al. Stressors faced by healthcare professionals and coping strategies during the early stage of the COVID-19 pandemic in Germany. PLoS One. 2022;17(1):e0261502. doi:10.1371/journal.pone.0261502
43. Norful AA, Rosenfeld A, Schroeder K, Travers JL, Aliyu S. Primary drivers and psychological manifestations of stress in frontline healthcare workforce during the initial COVID-19 outbreak in the United States. Gen Hosp Psychiatry. 2021;69:20–26. doi:10.1016/j.genhosppsych.2021.01.001
44. Eysenbach G. Improving the quality of web surveys: the Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J Med Internet Res. 2004;6(3):e34. doi:10.2196/jmir.6.3.e34
45. Dyrbye L, Major-Elechi B, Hays T, Fraser C, Buskirk S, West C. Physicians’ ratings of their supervisor’s leadership behaviors and their subsequent burnout and satisfaction: a longitudinal study. Mayo Clin Proc. 2021;96(10):2598–2605. doi:10.1016/j.mayocp.2021.01.035
46. Dyrbye L, Major-Elechi B, Hays T, Fraser C, Buskirk S, West C. Relationship between organizational leadership and health care employee burnout and satisfaction. Mayo Clin Proc. 2020;95(4):698–708. doi:10.1016/j.mayocp.2019.10.041
47. West C, Dyrbye L, Satele D, Sloan J, Shanafelt T. Concurrent validity of single-item measures of emotional exhaustion and depersonalization in burnout assessment. J Gen Intern Med. 2012;27(11):1445–1452. doi:10.1007/s11606-012-2015-7
48. West C, Dyrbye L, Sloan J, Shanafelt T. Single item measures of emotional exhaustion and depersonalization are useful for assessing burnout in medical professionals. J Gen Intern Med. 2009;24(12):1318–1321. doi:10.1007/s11606-009-1129-z
49. Schaufeli W, Taris T. The conceptualization and measurement of burnout: common ground and worlds apart. Work Stress. 2005;19(3):256–262. doi:10.1080/02678370500385913
50. Waddimba A, Scribani M, Nieves M, Krupa N, May J, Jenkins P. Validation of single-item screening measures for provider burnout in a rural health care network. Eval Health Prof. 2016;39(2):215–225. doi:10.1177/0163278715573866
51. Stoller JK. Commentary: recommendations and remaining questions for health care leadership training programs. Acad Med. 2013;88(1):12–15. doi:10.1097/ACM.0b013e318276bff1
52. Schwartz R, Pogge C, Gillis S, Holsinger J, Programs for the development of physician leaders: a curricular process in its infancy. Acad Med. 2000;75(2):133–140. doi:10.1097/00001888-200002000-00008
53. Smith P, Kendall L, Hulin C. The measurement of satisfaction in work and retirement: a strategy for the study of attitudes. RandMcNally. 1969.
54. Trockel M, Bohman B, Lesure E, et al. A brief instrument to assess both burnout and professional fulfillment in physicians: reliability and validity, including correlation with self-reported medical errors, in a sample of resident and practicing physicians. Acad Psychiatry. 2018;42(1):11–24. doi:10.1007/s40596-017-0849-3
55. Shanafelt TD, Makowski MS, Wang H, et al. Association of burnout, professional fulfillment, and self-care practices of physician leaders with their independently rated leadership effectiveness. JAMA Network Open. 2020;3(6):E207961. doi:10.1001/jamanetworkopen.2020.7961
56. Bowling NA, Hammond GD. A meta-analytic examination of the construct validity of the Michigan organizational assessment questionnaire job satisfaction subscale. J Vocat Behav. 2008;73(1):63–77. doi:10.1016/j.jvb.2008.01.004
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Influence of Competent Managers on Employee Retention, Job Satisfaction and Well-Being in the Healthcare Industry - A Scoping Review
Kumar S, Fong BYF, Liang Z
Journal of Healthcare Leadership 2026, 18:557143
Published Date: 8 January 2026