")
Back to Journals » Journal of Blood Medicine » Volume 5
Physical and psychosocial challenges in adult hemophilia patients with inhibitors
Authors duTreil S
Received 28 February 2014
Accepted for publication 2 May 2014
Published 22 July 2014 Volume 2014:5 Pages 115—122
DOI https://doi.org/10.2147/JBM.S63265
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Sue duTreil
Louisiana Center for Bleeding and Clotting Disorders, Tulane University Health Sciences Center, New Orleans, LA, USA
Abstract: Numerous challenges confront adult hemophilia patients with inhibitors, including difficulty in controlling bleeding episodes, deterioration of joints, arthritic pain, physical disability, emotional turmoil, and social issues. High-intensity treatment regimens often used in the treatment of patients with inhibitors also impose significant scheduling, economic, and emotional demands on patients and their families or primary caregivers. A comprehensive multidisciplinary assessment of the physical, emotional, and social status of adult hemophilia patients with inhibitors is essential for the development of treatment strategies that can be individualized to address the complex needs of these patients.
Keywords: adult hemophilia patients with inhibitors, adherence, physical challenges, psychosocial challenges, health-related quality of life
Introduction
While bypassing agents can achieve an effective level of control for most bleeding episodes in hemophilia patients with inhibitors, their hemostatic efficacy is not equivalent to that of factor replacement in patients without inhibitors and bleeding is harder to control.1 Patients with inhibitors have worse treatment-related outcomes, including greater incidence of joint abnormalities, more rapid progression of arthropathy, more chronic joint pain,2–5 and an increased incidence of intracranial hemorrhage than patients without inhibitors.6 The assumption has been that these poor outcomes are the result of inadequately controlled intra-articular bleeding in patients with inhibitors. However, a prospective study of patients with hemophilia and inhibitors has reported joint and other types of bleeds at lower frequencies than those described in some studies of patients without inhibitors.7 Additional factors that might contribute to these outcomes include comorbidities and high-intensity treatment and are discussed later.
The purpose of this paper is to review the major psychosocial challenges faced by adult patients with inhibitors where such data exist, to describe the need for psychosocial data specific to patients with inhibitors, and to suggest psychosocial intervention strategies for patients dealing with the challenges of hemophilia with inhibitors. In order to identify articles describing these issues, literature searches were conducted through PubMed for the term “hemophilia OR haemophilia” in combination with “quality of life”, “social”, “family”, “psychosocial”, “work”, “self-esteem”, “stress”, and “psychological”. Searches were limited to the last 10 years, English language, and adult populations (≥18 years of age). Results from these searches were combined and duplicates, laboratory, and genetic studies removed. Studies involving patients with inhibitors were then hand-selected from a search for “inhibitor”.
Physical impact of inhibitors in patients with hemophilia
Hemophilic arthropathy in patients with inhibitors
Hemophilic arthropathy is an ongoing cumulative process that eventually results in damaging joint effects.8–11 The long-term effects on joints include limited range of motion (ROM), deformity, crippling disability, and chronic pain.3,4,12–14 Studies have confirmed that patients with inhibitors experience greater ROM limitations and joint pain at an earlier age than those without inhibitors.3,4,15 Patients with high-titer inhibitors clearly demonstrate worse clinical and radiological joint scores than patients without inhibitors, and a three-fold increased risk of disability,3,4,12 due to more rapidly progressive joint disease.2,11,16
Strategies for joint disease management in patients with inhibitors
Several strategies are important in the management of evolving joint disease in patients with inhibitors, including exercise, physical therapy, orthopedic interventions, and pain management.10 In addition, recent studies17–19 suggest that the prevention of joint bleeding may be possible with the regular use of secondary prophylaxis with bypassing agents, a therapeutic modality that could be helpful in interrupting the progression of joint disease if started early in patients who are experiencing repeated bleeding in a particular joint.
Physical inactivity, especially early in a patient’s clinical course (prior to the development of end-stage joint disease) can lead to weight gain and muscle weakening, both of which may increase the likelihood of joint bleeds.3,4,20,21 In patients with and without inhibitors, exercise is essential to strengthen muscles and maintain general fitness, which in turn can protect joints and improve patients’ physical, emotional, and social well-being.22 Low-impact activities such as swimming are highly recommended because they can improve overall fitness, build muscle strength, and reduce the risk of joint bleeds.22–24 Supervised physical training can reduce bleeding frequency, increase isometric muscular strength, and increase proprioceptive performance.25,26 Some other sports, such as golf, tai chi, and bicycling, are deemed to be of safe-to-moderate risk,27 and may be appropriate for patients with inhibitors, particularly with routine prophylactic coverage with bypassing agents when necessary to prevent joint bleeds.17,18 Even with some existing joint disability, adult patients with inhibitors should be encouraged to find an appropriate, individualized exercise plan that can help to protect joints that have not yet experienced significant damage.
Physical therapy may be helpful in restoring joint motion, muscle flexibility, and strength, particularly for patients with chronic synovitis that has not yet progressed to end-stage joint disease.28,29 For patients with inhibitors, isometric exercises are best for beginning physical therapy followed by cautious use of resistive exercises. A distinct set of exercises is utilized for each joint to help maintain or improve ROM, proprioception, and muscle strength.28,29 Physical therapy may also be helpful in restoring function after muscular bleeds.
Orthopedic procedures have become an increasingly important option to improve mobility and quality of life (QoL) in the inhibitor population;30–32 however, the benefits and risks should be determined on an individual basis. A comprehensive approach by the hemophilia care team to manage expectations for surgical improvement of orthopedic status in patients with inhibitors is imperative to optimize the outcome.
Pain
A serious consequence of progressive joint disease that cannot be surgically corrected in all patients with hemophilia is chronic pain; often, this pain persists despite the patient’s and medical team’s best efforts to control joint bleeding and disease progression.12,13,33,34 Intractable pain can lead to chronic narcotic use, and in some patients, dependence on alcohol and illicit drugs to augment attempts at pain relief.34
While the early administration of bypassing agents and appropriate use of pain medication are useful for managing pain associated with acute bleeds, pain management for patients with chronic arthropathies that are not amenable to medical, physical, or surgical interventions can be quite difficult. In addition to analgesic medications, therapies for arthropathy may include cryotherapy, hydrotherapy, electrotherapy, acupuncture, relaxation techniques, and gentle manual mobilization of arthropathic joints.11,13,23,28,29,35,36 Managing moderate to severe pain with the use of opioid analgesics is often necessary; however, opioid analgesics may have serious long-term side effects, including issues of drug dependence.13,34 For chronic pain that is difficult to manage, patient referral to a pain clinic is appropriate.
Comorbid conditions
In addition, comorbid conditions may further complicate the management of adult patients with or without inhibitors; the most serious include human immunodeficiency virus (HIV) and hepatitis C virus (HCV) infections,37 arthritis,8,12 osteoporosis,38,39 and obesity.20 HIV- and HCV-positive individuals may contend with significant clinical problems related to acquired immunodeficiency syndrome (AIDS) or liver disease, both of which are associated with increased bleeding symptoms and clotting factor consumption.37 Increased incidences of osteoporosis and arthritis may result from recurring hemarthroses and frequent limb immobilization.38,39 Higher body mass index, an increasing problem among all segments of the US population, can be particularly problematic for patients with arthropathy in weight-bearing joints because it is associated with greater limitations of ROM.4,20 As with any aging population, older patients with inhibitors may also experience other comorbid conditions such as diabetes, hypertension, renal disease, and cancer.21,40
Effect of high-intensity treatment approaches
Aggressive high-intensity treatment approaches, including immune tolerance induction (ITI) for inhibitor eradication and prophylactic use of bypassing agents, are often indicated to mitigate bleeding risk and improve patient QoL.1,17,41,42 Highly effective treatment options are more limited for individuals with inhibitors compared with those without inhibitors.1,2,11 Frequently used treatment options in patients with inhibitors include high-intensity factor concentrate regimens and require a major commitment of time and resources from patients and their families. These regimens include: 1) ITI therapy to eradicate recently developed inhibitors,41 2) administration of higher doses of factor VIII (>50 IU/kg) to control bleeding for patients with low-titer inhibitors (<5 BU),43 and 3) prophylactic regimens consisting of frequent administration of bypassing agents to prevent bleeding in an attempt to interrupt joint bleeding and further joint deterioration for patients with high-titer inhibitors (>5 BU).17,18 These therapeutic strategies pose significant challenges to patients and their families due to cost, time commitments, and the need to maintain rigorous adherence to the protocols being used.
Psychosocial impact of inhibitors on patients with hemophilia
Patients with inhibitors also have higher incidences of mobility-related problems,3,4,15,16 hospitalizations,3,4 school and work absenteeism,3 and difficulty maintaining a job,3 along with higher treatment costs, compared with patients without inhibitors3,44 (Table 1). As would be expected based on these factors, the QoL of patients with inhibitors is lower than for non-inhibitor hemophilia patients.4,12,13,33,45 A limited number of studies of psychosocial well-being have been performed in patients with hemophilia (reviewed by Cassis46), and data exploring the specific issues faced by patients with inhibitors are largely lacking and highlight the need for more studies in this area.
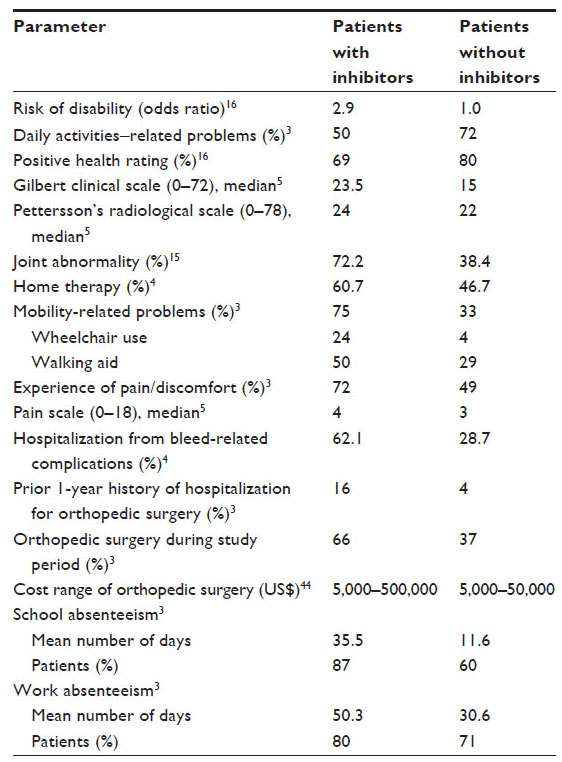 | Table 1 Outcomes for hemophilia patients with and without inhibitors |
Health-related QoL
Taken together, the challenges faced by patients with inhibitors (Table 1) combine to have a significant negative impact on well-being, as well as psychosocial functional status.3,14,33 Patients are affected in both their personal and professional lives. Studies of health-related QoL have shown that significantly more patients with inhibitors had difficulties managing daily life challenges compared with those without inhibitors.3,14,33 Work-related challenges include medical absenteeism, concerns about insurance coverage, and limitations for advancement and promotion.3 A greater proportion of patients with inhibitors may be unemployed or underemployed, or may receive disability income3 compared with patients without inhibitors and the general population.16,47
Social issues associated with employment, disability status, medical absenteeism, and insurance coverage also negatively impact patient perception of self and self-esteem. Low self-esteem has been correlated with depression, anxiety, and low social expectations; patients with hemophilia with or without inhibitors have been shown to have lower self-esteem than healthy subjects.48 In addition to these challenges, the inhibitor patient may struggle with:
- Self-autonomy because he needs assistance with self-care when joint damage does not allow him full ROM;
- fear that he may have a bleed that cannot be stopped;
- and embarrassment that he is unable to compete with other men in sports, personal relationships, and physical appearance.
Approaches to assist the patient with these psychosocial issues can include problem solving, self-care, anger management techniques, encouraging more social contacts, and open communications with family and medical professionals.49
Mental health
We speculate that loss of independence, the inability to achieve educational goals, and difficulty with employment suffered by many patients with inhibitors likely contribute to low self-esteem. In a study50 of 60 hemophilia patients (seven <20 years of age and 53 >20 years of age) who were compared to 78 healthy subjects, it was found that subjects with hemophilia had lower self-esteem than the control group and that self-esteem correlated with the potential to develop depressive or anxiety disorders.
Catastrophizing is a coping strategy used by hemophilia patients who lack a personal sense of psychosocial well-being, and strong positive correlations have been described between the use of this coping mechanism and pain and disability in these patients.34 Adult hemophilia patients utilize coping strategies similar to patients with other chronic disease or pain states, although the use of such a strategy has been shown to be independent of disease severity.34,48
Up to one-third of individuals with a serious medical condition have symptoms of depression;46,51 experience at our hemophilia treatment center suggests a similar rate exists in our hemophilia patient population. Men affected by depression often report experiencing fatigue, loss of interest, and irritability rather than the feelings of sadness or guilt that are more commonly reported by women, reflecting a significant gender difference.51 Moreover, depression worsens health scores when diagnosed in conjunction with other chronic illnesses.46,48,51 Social isolation and depression may also occur in patients with inhibitors as the result of having a long-term chronic condition accompanied by pain and limited mobility.46 Referrals for psychological and social support to combat depression and feelings of isolation are critical for the well-being of these patients.
Self-esteem and effects on adherence
A major key to success is patient adherence to the complex medical treatment regimens required for patients with inhibitors, because even brief periods of nonadherence can lead to a major loss in efficacy of the treatment regimen in general. For example, interruption of daily factor VIII infusion given for ITI may lead to reemergence of an inhibitor that had been responding to the tolerance program and may result in the loss of gains previously made at a high cost. Similarly, a patient on prophylaxis with daily bypassing therapy who has experienced benefit in the prevention of joint bleeding may experience recurrent joint bleeding and joint deterioration with an interruption of therapy.
The demanding nature of high-intensity treatment regimens, such as ITI and prophylaxis, used in many patients with inhibitors can significantly affect adherence rates of adult patients with inhibitors.41,45,52,53 One study of 47 hemophilia patients (including 28 adults) noted that adherence to high-intensity regimens was significantly worse than adherence to on-demand treatment regimens.52 High-demand regimens, such as ITI and prophylaxis, require regular infusion therapy in the absence of symptoms, often skewing patient perception that prophylactic treatment is unnecessary.45,53 A global survey found that overall compliance rates declined in an age-related manner, with the lowest rate at 36% in those aged 19–58 years.54 Other major barriers to adherence include patient failure to understand treatment benefits, patient denial, poor venous access, lack of family support, lifestyle interference, teenage rebellion, time constraints, relief or disappearance of symptoms, and forgetfulness.54,55
In order to adhere to complex therapy that is not based on present symptoms but on a longer view of achieving and maintaining health in the future, patients have to be forward-looking and optimistic, and should appreciate that their future health is worth the present investment. There is evidence in individuals with diabetes mellitus that self-esteem impacts treatment adherence,56 and that low self-esteem results in patients placing a low-priority value on the effort required to adhere to a complex treatment process that may serve as a negative reminder of health impairment. Since the study associating low self-esteem with poor adherence was in patients with diabetes, further studies evaluating this causal pathway in patients with hemophilia should be done prior to developing and implementing interventions to raise self-esteem. It is important that efforts are made to help patients address negative attitudes, expressions, and beliefs that are suggestive of self-esteem problems.
Psychosocial intervention strategies
Psychosocial professionals often use the “strengths perspective”57 when working with patients. This approach assumes that all individuals have strengths, access to resources, and the capacity to grow. It also assumes that people learn from difficulties they encounter in life as well as from their successes. The primary intervention strategy used in the strengths perspective is based on developing these capacities in order to overcome adversity and achieve goals. The strategy encourages positive coping skills, including motivation, resilience, willpower, and the ability to see illness as an opportunity that will help the patient to more readily accept his disease and adhere to the treatment plan. Psychosocial professionals are trained to listen to the patient’s life story, which often includes the patient’s cognitive, emotional, and behavioral reactions to situational events in his life. By learning to listen beyond the failed and pathological reactions, the psychosocial professional hears the coping mechanisms or strengths the person uses to live in the present and to find a path to the future.
Psychosocial professionals often engage the patient by using cognitive behavioral therapy (CBT) techniques to help relieve the patient’s negative feelings.58 The National Alliance on Mental Illness describes CBT as a technique based on the theoretical concept that behaviors and feelings are formed by our thoughts and that we can learn new ways of thinking.59 CBT is a proven theory that has shown to be a somewhat more superior treatment than antidepressants in adults with depression.60 Consequently the psychosocial professional will help patients and their families recognize, challenge, test, and change negative thoughts and unrealistic beliefs into positive, realistic ones. This is done by having the patient or family member reframe the negative thought or unrealistic belief. Reframing begins with establishing that the negative thought is only one way of describing the problem situation, and then visualizing and verbalizing other versions of the problem that are more positive. An example would be a college student with an inhibitor who believes he is not an intelligent person because he failed a test. His psychosocial professional would help him reframe this conception by helping him to see that it was just one test and to think about what might have caused that one test to be a problem. Did he do all the homework assignments in that subject? Does he know how to study for a test? What does he think he needs to pass the next test? This introduction to a more realistic concept of the problem gives the patient a new way to think about it; one that is more positive and gives hope that the problem can be fixed.
Adult hemophilia patients with inhibitors are usually patients with joint disease, and consequently, are experiencing much pain. In a recent article,61 a list of interventions that are non-pharmacologic are given for pain management in patients with hemophilic arthropathy, including acupuncture, biofeedback, CBT, distraction, exercise, guided imagery, herbal therapy, hydrotherapy, hypnosis, integrative therapy, physical therapy, therapeutic massage, and transcutaneous electrical neurostimulation (TENS). Of these interventions, acupuncture, physical therapy, and TENS address the physical pain directly. The other interventions could be and are used by psychosocial and medical professionals to intervene with emotional and behavioral reactions to difficult life situations, including pain.
An article in the National Hemophilia Foundation’s publication, HemAware,62 gives descriptions by patients with inhibitors of their use of self-hypnosis to control joint pain. There is no way to measure pain objectively, so it is the patient’s perception of pain that determines their level of pain. These patients report that having a method to calm the mind while internally visualizing the pain decreasing does impact the level of pain experienced.
Meditation is another intervention that is similar to hypnosis, in that it can be used as a self-induced form of relaxation.63 It takes less time than hypnosis and its purpose is simply to induce a relaxed state, but not so relaxed that that the brain is open to suggestion, as is the case with self-hypnosis. One achieves this state of relaxation by quieting oneself, usually with deep breathing and becoming mindful of that breathing. Visualizations (for example, thinking of being on a beach or in the forest) can also be used to bring the patient to this state. By practicing meditation periodically during the day, patients with inhibitors have found their overall pain has been reduced and that they cope better emotionally.
Recommendations for an integrated approach to challenges faced by the inhibitor patient
Interventions to improve the QoL of patients with inhibitors are best handled by a multidisciplinary team approach that includes physicians, nurses, social workers, physical and occupational therapists, and psychologists. Clinical care includes the prevention and management of bleeding events and complications of bleeding, and regular exercise and visits to a physical therapist to maintain good joint health, slow or prevent the development of musculoskeletal complications, and mitigate chronic arthropathies and chronic pain.
The psychosocial component of the comprehensive care model is highly important for patients with inhibitors. Screening for symptoms of low self-esteem, low coping skills, depression, anxiety, and substance abuse should begin early in life and continue throughout adulthood. The psychosocial team member helps the inhibitor patient to improve or enhance his QoL by counseling and assisting him in obtaining a wide range of services and resources regarding his adjustment to having hemophilia with an inhibitor. These resources may be needed to address educational needs, career choices, employment, finances, transitioning to adulthood, interpersonal relationships, parenting skills, self-esteem, coping skills, mental health, substance abuse, aging, and end of life issues. Additionally, assessing patients’ commitment to treatment and adherence to complex therapies may be best accomplished by psychosocial team members so that intervention strategies can be instituted early to provide these vulnerable patients with the best chance at achieving and maintaining a good QoL.
Adjunctive therapeutic strategies for adult patients should ideally include vocational contingency planning for possible work-related disruptions caused by bleeding and disability. Finally, familial and caregiver support, combined with effective intervention strategies by the multidisciplinary team, will assist in building good self-esteem and positive coping strategies such as problem solving and increased socialization skills in patients, leading to improved physical and emotional well-being.
Treatment plans should involve the entire comprehensive team and encompass both physical and psychosocial evaluations and intervention strategies. The goals of intervention are to maintain good physical function, prevent joint disease and chronic pain (when possible), and screen patients for early signs of mental health problems that can negatively impact QoL and adherence to treatment.1,34,46
Acknowledgments
Editorial assistance was provided by Jim Loss, PhD, CMPP, ETHOS Health Communications, Newtown, PA, USA, with financial assistance from Novo Nordisk, in compliance with international guidelines for Good Publication Practice. I would like to thank Cindy Leissinger, MD, for her review and contribution to the manuscript.
Disclosure
The author reports no conflict of interest in this work.
References
DiMichele D. Inhibitors in Hemophilia: A Primer. Montreal, Canada: World Federation of Hemophilia; 2008. Available from: http://www1.wfh.org/publication/files/pdf-1122.pdf. Accessed June 3, 2014. | |
Berntorp E, Shapiro A, Astermark J, et al. Inhibitor treatment in haemophilias A and B: summary statement for the 2006 international consensus conference. Haemophilia. 2006;12 Suppl 6:1–7. | |
Morfini M, Haya S, Tagariello G, et al. European study on orthopaedic status of haemophilia patients with inhibitors. Haemophilia. 2007;13(5):606–612. | |
Soucie JM, Cianfrini C, Janco RL, et al. Joint range-of-motion limitations among young males with hemophilia: prevalence and risk factors. Blood. 2004;103(7):2467–2473. | |
Windyga J, Lopaciuk S, Stefanska E, et al. Haemophilia in Poland. Haemophilia. 2006;12(1):52–57. | |
Nuss R, Soucie JM, Evatt B; Hemophilia Surveillance System Project Investigators. Changes in the occurrence of and risk factors for hemophilia-associated intracranial hemorrhage. Am J Hematol. 2001;68(1):37–42. | |
Kasper CK. Diagnosis and Management of Inhibitors to Factors VIII and IX. An Introductory Discussion for Physicians. Montreal, Canada: World Federation of Hemophilia; 2004. Available from: http://www1.wfh.org/publication/files/pdf-1178.pdf. Accessed June 3, 2014. | |
Jacobson JA, Girish G, Jiang Y, Sabb BJ. Radiographic evaluation of arthritis: degenerative joint disease and variations. Radiology. 2008;248(3):737–747. | |
Jansen NW, Roosendaal G, Lafeber FP. Understanding haemophilic arthropathy: an exploration of current open issues. Br J Haematol. 2008; 143(5):632–640. | |
Roosendaal G, Lafeber FP. Pathogenesis of haemophilic arthropathy. Haemophilia. 2006;12 Suppl 3:117–121. | |
Wallny T, Lahaye L, Brackmann HH, Hess L, Seuser A, Kraft CN. Clinical and radiographic scores in haemophilic arthropathies: how well do these correlate to subjective pain status and daily activities? Haemophilia. 2002;8(6):802–808. | |
Bossard D, Carrillon Y, Stieltjes N, et al. Management of haemophilic arthropathy. Haemophilia. 2008;14 Suppl 4:11–19. | |
Wallny TA, Brackmann HH, Gunia G, Wilbertz P, Oldenburg J, Kraft CN. Successful pain treatment in arthropathic lower extremities by acupuncture in haemophilia patients. Haemophilia. 2006;12(5):500–502. | |
Scalone L, Mantovani LG, Mannucci PM, Gringeri A; COCIS Study Investigators. Quality of life is associated to the orthopaedic status in haemophilic patients with inhibitors. Haemophilia. 2006;12(2):154–162. | |
Su Y, Wong WY, Lail A, Donfield SM, Konzal S, Gomperts E. Long-term major joint outcomes in young adults with haemophilia: interim data from the HGDS. Haemophilia. 2007;13(4):387–390. | |
Rosendaal FR, Smit C, Varekamp I, et al. Modern haemophilia treatment: medical improvements and quality of life. J Intern Med. 1990;228(6):633–640. | |
Ettingshausen CE, Kreuz W. Early long-term FEIBA prophylaxis in haemophilia A patients with inhibitor after failing immune tolerance induction: a prospective clinical case series. Haemophilia. 2010;16(1):90–100. | |
Konkle BA, Ebbesen LS, Erhardtsen E, et al. Randomized, prospective clinical trial of recombinant factor VIIa for secondary prophylaxis in hemophilia patients with inhibitors. J Thromb Haemost. 2007;5(9):1904–1913. | |
Leissinger C, Berntorp E, Biasioli C, Carpenter S, Jo H, Kavakli K. Prophylactic dosing of anti-inhibitor coagulant complex (FEIBA) reduces bleeding frequency in hemophilia A patients with inhibitors: results of the Pro-FEIBA study. Blood (ASH Annual Meeting Abstracts). 2010;116:720. | |
Hofstede FG, Fijnvandraat K, Plug I, Kamphuisen PW, Rosendaal FR, Peters M. Obesity: a new disaster for haemophilic patients? A nationwide survey. Haemophilia. 2008;14(5):1035–1038. | |
Mauser-Bunschoten EP, Fransen Van De Putte DE, Schutgens RE. Co-morbidity in the ageing haemophilia patient: the down side of increased life expectancy. Haemophilia. 2009;15(4):853–863. | |
Von Mackensen S. Quality of life and sports activities in patients with haemophilia. Haemophilia. 2007;13 Suppl 2:38–43. | |
World Federation of Hemophilia. Guidelines for the Management of Hemophilia. Montreal, Canada: World Federation of Hemophilia; 2005. Available from: http://www1.wfh.org/publications/files/pdf-1472.pdf. Accessed June 3, 2014. | |
Seuser A, Boehm P, Kurme A, Schumpe G, Kurnik K. Orthopaedic issues in sports for persons with haemophilia. Haemophilia. 2007;13 Suppl 2:47–52. | |
Hilberg T, Herbsleb M, Puta C, Gabriel HH, Schramm W. Physical training increases isometric muscular strength and proprioceptive performance in haemophilic subjects. Haemophilia. 2003;9(1):86–93. | |
Tiktinsky R, Falk B, Heim M, Martinovitz U. The effect of resistance training on the frequency of bleeding in haemophilia patients: a pilot study. Haemophilia. 2002;8(1):22–27. | |
Anderson A, Forsyth A, National Hemophilia Foundation. Playing It Safe: Bleeding Disorders, Sports and Exercise. New York, NY: National Hemophilia Foundation; 2005. Available from: http://www.hemophilia.org/NHFWeb/Resource/StaticPages/menu0/menu2/menu35/menu204/PlayingItSafe.pdf. Accessed June 3, 2014. | |
Heijnen L. The role of rehabilitation and sports in haemophilia patients with inhibitors. Haemophilia. 2008;14 Suppl 6:45–51. | |
Seuser A, Berdel P, Oldenburg J. Rehabilitation of synovitis in patients with haemophilia. Haemophilia. 2007;13 Suppl 3:26–31. | |
Rodriguez-Merchan EC, Rocino A. Literature review of surgery management in inhibitor patients. Haemophilia. 2004;10 Suppl 2:22–29. | |
Rodriguez-Merchan EC, Wiedel JD, Wallny T, et al. Elective orthopaedic surgery for inhibitor patients. Haemophilia. 2003;9(5):625–631. | |
Solimeno LP, Mancuso ME, Pasta G, Santagostino E, Perfetto S, Mannucci PM. Factors influencing the long-term outcome of primary total knee replacement in haemophiliacs: a review of 116 procedures at a single institution. Br J Haematol. 2009;145(2):227–234. | |
Gringeri A, Mantovani LG, Scalone L, Mannucci PM. Cost of care and quality of life for patients with hemophilia complicated by inhibitors: the COCIS Study Group. Blood. 2003;102(7):2358–2363. | |
Santavirta N, Bjorvell H, Solovieva S, Alaranta H, Hurskainen K, Konttinen YT. Coping strategies, pain, and disability in patients with hemophilia and related disorders. Arthritis Rheum. 2001;45(1):48–55. | |
d’Young AI. Domiciliary application of CryoCuff in severe haemophilia: qualitative questionnaire and clinical audit. Haemophilia. 2008;14(4):823–827. | |
Gomis M, González LM, Querol F, Gallach JE, Toca-Herrera JL. Effects of electrical stimulation on muscle trophism in patients with hemophilic arthropathy. Arch Phys Med Rehabil. 2009;90(11):1924–1930. | |
Tencer T, Friedman HS, Li-McLeod J, Johnson K. Medical costs and resource utilization for hemophilia patients with and without HIV or HCV infection. J Manag Care Pharm. 2007;13(9):790–798. | |
Gallacher SJ, Deighan C, Wallace AM, et al. Association of severe haemophilia A with osteoporosis: a densitometric and biochemical study. Q J Med. 1994;87(3):181–186. | |
Wallny TA, Scholz DT, Oldenburg J, et al. Osteoporosis in haemophilia – an underestimated comorbidity? Haemophilia. 2007; 13(1):79–84. | |
Miesbach W, Alesci S, Krekeler S, Seifried E. Comorbidities and bleeding pattern in elderly haemophilia A patients. Haemophilia. 2009;15(4):894–899. | |
DiMichele DM, Hoots WK, Pipe SW, Rivard GE, Santagostino E. International workshop on immune tolerance induction: consensus recommendations. Haemophilia. 2007;13 Suppl 1:1–22. | |
Hoots WK, Ebbesen LS, Konkle BA, et al; Novoseven (F7HAEM-1505) Investigators. Secondary prophylaxis with recombinant activated factor VII improves health-related quality of life of haemophilia patients with inhibitors. Haemophilia. 2008;14(3):466–475. | |
Rodriguez-Merchan EC. Some recent developments regarding arthropathy and inhibitors in haemophilia. Haemophilia. 2008;14(2):242–247. | |
Rodriguez-Merchan EC, Rocino A, Ewenstein B, et al. Consensus perspectives on surgery in haemophilia patients with inhibitors: summary statement. Haemophilia. 2004;10 Suppl 2:50–52. | |
De Moerloose P, Urbancik W, Van Den Berg HM, Richards M. A survey of adherence to haemophilia therapy in six European countries: results and recommendations. Haemophilia. 2008;14(5):931–938. | |
Cassis FR. Psychosocial Care for People with Hemophilia. Montreal, Canada: World Federation of Hemophilia; 2007. Available from: http://www1.wfh.org/publications/files/pdf-1198.pdf. Accessed June 3, 2014. | |
Brown TM, Lee WC, Joshi AV, Pashos CL. Health-related quality of life and productivity impact in haemophilia patients with inhibitors. Haemophilia. 2009;15(4):911–917. | |
Steinhausen HC. A psycho-clinical investigation in adult hemophiliacs. J Psychosom Res. 1975;19(4):295–302. | |
Remor E, Arranz P, Miller R. Psychosocial impact of inhibitors on haemophilia patients’ quality of life. In: Rodriguez-Merchan EC, Lee C, editors. Inhibitors in Patients with Haemophilia. Oxford, UK: Blackwell Science; 2002:187–192. | |
Canclini M, Saviolo-Negrin N, Zanon E, Bertoletti R, Girolami A, Pagnan A. Psychological aspects and coping in haemophilic patients: a case-control study. Haemophilia. 2003;9(5):619–624. | |
National Institute of Mental Health. Men and Depression. Bethesda, MD: National Institutes of Health; 2009. http://www.nimh.nih.gov/health/publications/men-and-depression/complete-index.shtml#pub6. Accessed January 6, 2014. | |
du Treil S, Rice J, Leissinger CA. Quantifying adherence to treatment and its relationship to quality of life in a well-characterized haemophilia population. Haemophilia. 2007;13(5):493–501. | |
Lindvall K, Colstrup L, Wollter IM, et al. Compliance with treatment and understanding of own disease in patients with severe and moderate haemophilia. Haemophilia. 2006;12(1):47–51. | |
Geraghty S, Dunkley T, Harrington C, Lindvall K, Maahs J, Sek J. Practice patterns in haemophilia A therapy – global progress towards optimal care. Haemophilia. 2006;12(1):75–81. | |
Coppola A, Cerbone AM, Mancuso G, Mansueto MF, Mazzini C, Zanon E. Confronting the psychological burden of haemophilia. Haemophilia. 2011;17(1):21–27. | |
Kneckt MC, Keinanen-Kiukaanniemi SM, Knuuttila ML, Syrjala AM. Self-esteem as a characteristic of adherence to diabetes and dental self-care regimens. J Clin Periodontol. 2001;28(2):175–180. | |
Saleebey D. Introduction: Power in the People. In: Saleebey D, editor. The Strengths Perspective in Social Work Practice. 5th ed. New York, NY: Longman; 2009:15–19. | |
Greenberger D, Padesky CA. Mind Over Mood: Changing How You Feel by Changing the Way You Think. New York, NY: The Guilford Press; 1995. | |
National Alliance on Mental Illness. Cognitive Behavioral Therapy FACT SHEET. Arlington, VA: National Alliance on Mental Illness; 2012. Available from: http://www.nami.org/factsheets/CBT_factsheet.pdf. Accessed January 6, 2014. | |
Butler AC, Chapman JE, Forman EM, Beck AT. The empirical status of cognitive-behavioral therapy: a review of meta-analyses. Clin Psychol Rev. 2006;26(1):17–31. | |
Riley RR, Witkop M, Hellman E, Akins S. Assessment and management of pain in haemophilia patients. Haemophilia. 2011;17(6):839–845. | |
Powers MP. Hypnosis for Pain Management. New York, NY: National Hemophilia Foundation; 2010. Available from: http://www.hemaware.org/story/hypnosis-pain-management. Accessed January 6, 2014. | |
Boerner H. Think Again. New York, NY: National Hemophilia Foundation; 2012. Available from: http://www.hemaware.org/story/think-again. Accessed January 6, 2014. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.