Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Physical and Cognitive Impairments at ICU Discharge are Associated with High Long-Term Mortality in ICU Survivors with Solid Malignancies: A Retrospective Cohort Study
Authors Lee SY, Huh JW, Hong SB, Lim CM, Ahn JH ![]()
Received 10 March 2025
Accepted for publication 13 July 2025
Published 21 July 2025 Volume 2025:21 Pages 1121—1133
DOI https://doi.org/10.2147/TCRM.S520206
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor De Yun Wang
Su Yeon Lee, Jin Won Huh, Sang-Bum Hong, Chae-Man Lim, Jee Hwan Ahn
Department of Pulmonary and Critical Care Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, South Korea
Correspondence: Jee Hwan Ahn, Department of Pulmonary and Critical Care Medicine, Asan Medical Center, University of Ulsan College of Medicine, 88, Olympic-Ro 43-Gil, Songpa-Gu, Seoul, 05505, South Korea, Email [email protected]
Background: Many ICU survivors experience post-ICU physical, cognitive, or mental impairments. In ICU survivors with solid malignancies, post-ICU impairments can impede further cancer treatments and negatively impact their outcomes. This study aimed to investigate post-ICU mortalities and their risk factors at ICU discharge in ICU survivors with solid malignancies.
Methods: In this retrospective cohort study, adult patients with solid malignancies who were unexpectedly admitted to the medical ICU of a tertiary hospital between 2016 and 2022 and survived to ICU discharge were included. Data at ICU discharge were collected from electronic medical records. In-hospital and 1-year mortality and their risk factors were analyzed.
Results: Of the 708 ICU survivors, 25.1% died in the hospital, and 61% died within one year. At ICU discharge, 20.9% had delirium, 3.8% had coma, and 80.6% had impaired mobility. Respiratory support, including bilevel positive airway pressure (BiPAP), high-flow nasal cannula (HFNC), or other oxygen therapies was used in 88.7% of patients. Delirium (adjusted OR 1.73; 95% CI 1.04– 2.87; p = 0.035), coma (adjusted OR 5.63; 95% CI 2.09– 16.17; p < 0.001), limited mobility (adjusted OR 2.41; 95% CI 1.22– 5.14; p = 0.015), and use of BiPAP (adjusted OR 21.63; 95% CI 5.36– 99.57; p < 0.001) or HFNC (adjusted OR 7.08; 95% CI 2.45– 23.99; p < 0.001) were independently associated with in-hospital mortality. One-year survival was significantly lower in patients with delirium (35%, p < 0.001), coma (26%, p < 0.001), limited mobility (37%, p = 0.003), or those receiving respiratory support at ICU discharge (35%, p < 0.001).
Conclusion: A considerable portion of ICU survivors with solid malignancies died in the hospital or within one year after ICU discharge in our study. Cognitive, mobility, and pulmonary impairments at ICU discharge were significant risk factors for both in-hospital and long-term mortality.
Keywords: solid cancer, solid malignant tumor, ICU survivors, in-hospital mortality
Background
Patients with solid malignancies account for 10% to 15% of all admissions to the intensive care unit (ICU) admissions.1 ICU mortality rates have decreased due to significant advances in critical care management.2,3 However, ICU mortality is not the only outcome of interest.4 The long-term impact of critical illness has become an increasingly important concern beyond ICU discharge.5,6 Despite recent advances, long-term outcomes in patients with cancer treated in the ICU are worse than those in patients without cancer.7,8 While 5% to 27% of ICU survivors die in the hospital after ICU discharge,9 those with solid malignancies have a higher risk of in-hospital death.10
ICU survivors may experience a period of impaired quality of life.11,12 Up to 80% of ICU survivors experience new or worsening post-ICU physical, cognitive, and/or mental impairments, specifically referred to as post-intensive care syndrome (PICS).6 Particularly for advanced cancer patients, post-ICU impairments can serve as barriers to receiving additional cancer treatment, as decisions regarding the resumption of treatment are based on a patient’s overall functional status and general condition.13–15 In individuals with limited life expectancy, treatment delays caused by post-ICU impairments may lead to poor outcomes, including disease progression or reduced survival.16,17 To date, there has been a lack of studies on short- and long-term outcomes and their risk factors in patients with solid malignancies who survive in the ICU.
The aim of this study was to identify risk factors at the time of ICU discharge associated with in-hospital mortality and to investigate long-term outcomes in ICU survivors with solid malignancies.
Methods
Study Design and Patients
This is a retrospective cohort study conducted at a single tertiary hospital in South Korea. Among adult patients with solid malignancies actively treated by oncologists and admitted to the medical ICU between 2016 and 2022, those who survived in the ICU and were transferred to the general ward were included. This study included patients who met the following criteria: (1) patients aged over 18 years and (2) patients treated for more than 1 day in the ICU and transferred to the general ward. Exclusion criteria were as follows: (1) patients who died in the ICU, (2) patients who were transferred from the ICU to another hospital, and (3) patients admitted to the ICU for 1 day for monitoring or post-operative care. Only the first ICU admission per patient was included. ICU discharge decisions were made by board-certified intensivists based on institutional protocols and the patient’s clinical condition (Appendix 1).
Data Collection
Data from patients’ electronic medical records were gathered as follows: underlying cancer type, cancer stage, sex, age, weight, height, body mass index (BMI), and causes of ICU admission; dates of hospital admission and discharge, dates of ICU admission and discharge, date of last follow-up, date of death. During the ICU stay, information on the use of vasopressors, use of mechanical ventilation, initiation of renal replacement therapy and whether tracheostomy was performed were collected. At the time of ICU discharge, clinical status and treatment variables were collected based on the patient’s condition at the time of transfer from the ICU to the general ward. These included body weight and BMI change; respiratory support devices such as bilevel positive airway pressure (BiPAP), high-flow nasal cannula (HFNC), or other oxygen therapies, and FiO2; vasopressor use and dosages; whether hemodialysis was discontinued; Glasgow Coma Scale (GCS) score; results of the Confusion Assessment Method for the ICU (CAM-ICU); Richmond Agitation Sedation Scale (RASS); and laboratory data including arterial blood gas analysis. Whether patients had delirium at the time of ICU discharge was assessed using CAM-ICU in patients with a RASS score of ≥ −3.18 If patients had a RASS score of −4 or −5, they were recorded as “unable to assess delirium due to coma status”.
Patient’s mobility was assessed using the Braden Scale, which was developed to predict the risk of pressure ulcers.19,20 In the Braden scale, mobility is defined as the ability to change and control body position. There are 4 categories to assess mobility: no limitation (make major and frequent changes in position without assistance), slightly limited (make frequent though slight changes in body or extremity position independently), very limited (make occasional slight changes in body or extremity position but unable to make frequent or significant changes independently), completely immobile (does not make even slight changes in position without assistance). Based on the recorded scores, we classified patients into “no mobility limitation” or “limited mobility” (including slightly limited to completely immobile).
The primary outcome was the risk factor for in-hospital mortality, and the secondary outcomes were in-hospital mortality rates and 1-year mortality rate.
Statistical Analysis
The distribution of continuous variables was assessed using the Shapiro–Wilk test. Variables were summarized as mean ± standard deviation when normally distributed, or as median with interquartile range when not. The included patients were categorized as survivors and non-survivors according to in-hospital mortality. The characteristics at the time of ICU admission, discharge, and post-ICU outcomes were compared between the two groups. Continuous variables were compared using Student’s t-test when the assumption of normality was met; otherwise, the Mann–Whitney U-test was used. Categorical variables were compared using the chi-squared test or Fisher’s exact test. Multivariable logistic regression analysis was used to identify risk factors for in-hospital mortality. Variables with p-values < 0.1 in the univariable analysis were included in the multivariable model to ensure that potentially important predictors were not excluded prematurely. Backward elimination was applied for variable selection. Kaplan-Meier method and the Log rank test were used for survival analysis. All p-values were two-tailed, and the threshold for statistical significance was set at a p-value of less than 0.05. Missing data were not imputed. All statistical analyses were conducted using R software (version 4.2.1, R Core Team, Vienna, Austria).
Ethical Approval and Informed Consent
The study protocol was approved by the Institutional Review Board of Asan Medical Center (IRB number: 2023–0922) with a waiver of informed consent granted due to the observational design of the study. All research was performed in accordance with national guidelines and regulations. Patient data were anonymized prior to analysis, and the study was conducted in accordance with the principles of the Declaration of Helsinki.
Results
Of the 955 patients with solid malignancies admitted between 2016 and 2022, 224 patients who died in the ICU and 23 patients who were transferred to another hospital during their ICU stay were excluded (Figure 1). Among the 708 patients who survived in the ICU and were transferred to the general ward, 178 patients (25.1%) died in the hospital. Lung cancer (30.4%) was the most common type of cancer among the study patients, and 77.7% had metastatic cancer at the time of ICU admission (Table 1).
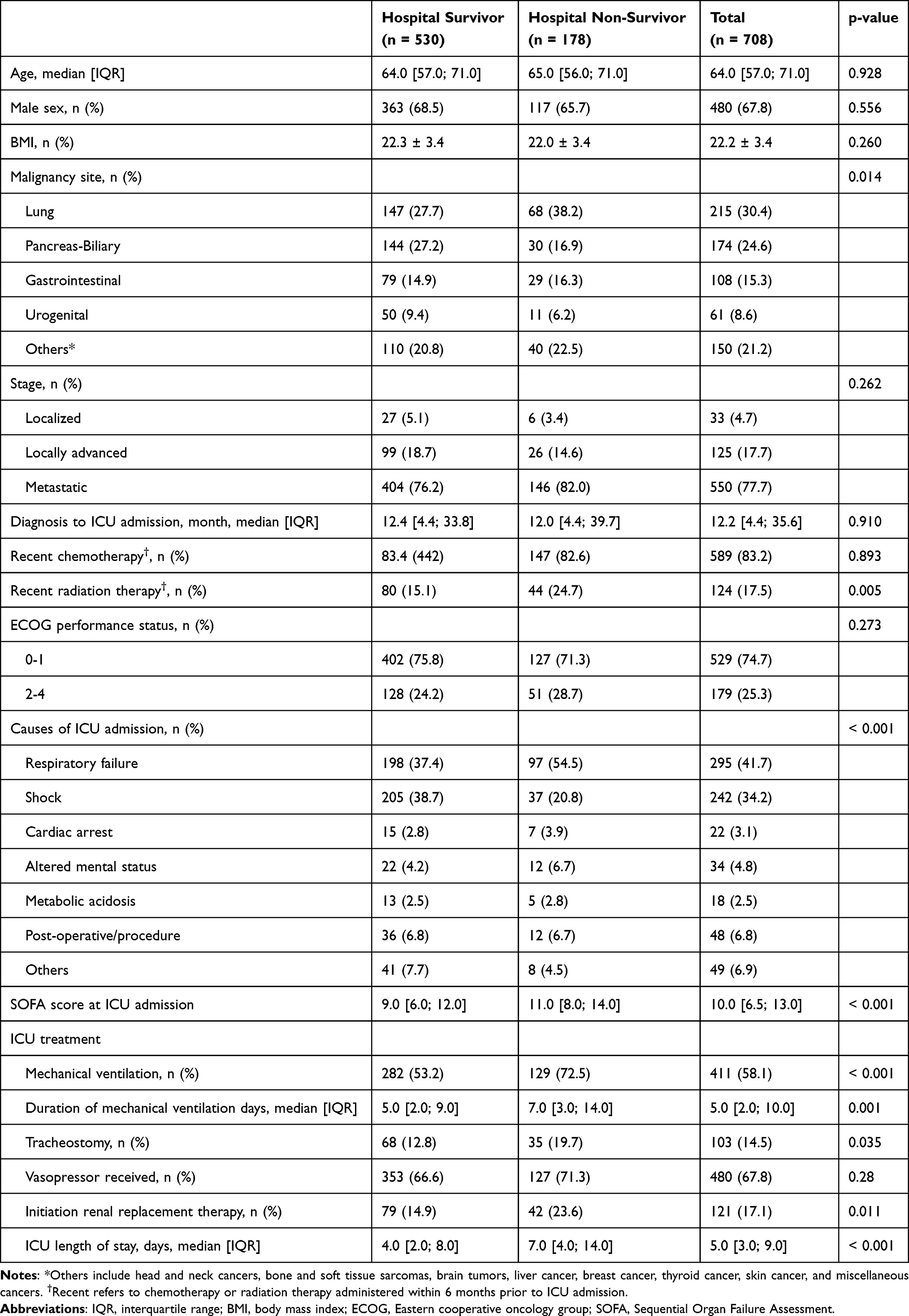 |
Table 1 Characteristics of the Patients at ICU Admission and ICU Treatment According to in-Hospital Mortality |
 |
Figure 1 Patient inclusion flow diagram. |
Mechanical ventilation was used in 58.1% of patients, and the median length of ICU stay was 5 (interquartile range [IQR], 3–9) days. At the time of ICU discharge, 88.7% of patients were using oxygen devices, including BiPAP (4.9%) and HFNC (15.5%; Table 2). The proportion of patients receiving vasopressors at the time of ICU discharge was 17.4%, and they were administered 0.01 ± 0.04 mcg/kg/min of norepinephrine. Delirium was observed in 20.9% of patients, and 3.8% of patients were in a comatose state. The proportion of patients with limited mobility was 80.6%. Among ICU survivors, those who died later during hospitalization had a longer ICU length of stay compared to hospital survivors (7.0 [4.0–14.0] vs 4.0 [2.0–8.0], p < 0.001). The proportion of patients receiving hemodialysis (18.5% vs 8.7%, p < 0.001), oxygen therapy (96.6% vs 86%, p < 0.001), and vasopressors (28.7% vs 13.6%, p < 0.001) was higher in hospital non-survivors than in hospital survivors. In addition, patients who died in the hospital had a lower mean GCS score (13.3 ± 3.2 vs 14.5 ± 1.3, p < 0.001) and a higher proportion of delirium (34.3% vs 16.4%, p < 0.001) and coma (10.7% vs 1.5%, p < 0.001). Patients who died in the hospital were more likely to have limited mobility (93.3% vs 76.4%, p < 0.001).
 |
Table 2 Characteristics of the Patients at the Time of ICU Discharge According to in-Hospital Mortality |
The 1-year mortality rate of the study patients was 61% (Table 3). Patients in the hospital non-survivor group died after a median of 10 (3–22) days from ICU discharge. For patients who survived and were discharged from the hospital, the 1-year mortality rate was 47.9%. Among patients with metastatic cancer (n = 550), 44.5% of patients received further chemotherapy after ICU discharge (Supplementary Table 1).
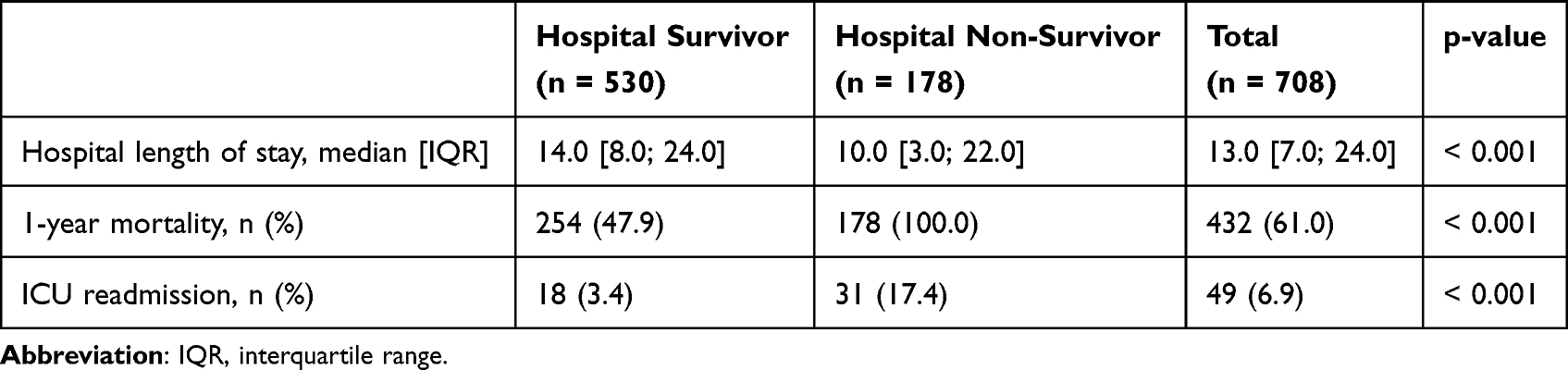 |
Table 3 Post-ICU Outcomes |
In the multivariable logistic regression analysis (Table 4), the administration of vasopressors (Odds Ratio [OR] 2.08; 95% Confidence Interval [CI] 1.20–3.61; p = 0.009), delirium (OR 1.73; 95% CI 1.04–2.87; p = 0.035), coma (OR 5.63; 95% CI 2.09–16.17; p < 0.001), limited mobility (OR 2.41; 95% CI 1.22–5.14; p = 0.015), and oxygen therapy with BiPAP (OR 21.63; 95% CI 5.36–99.57; p < 0.001), HFNC (OR 7.08; 95% CI 2.45–23.99; p < 0.001), and other oxygen devices (OR 3.16; 95% CI 1.20–9.92; p = 0.031) used at the time of ICU discharge were identified as independent risk factors for in-hospital mortality. Hyperbilirubinemia (OR 1.12; 95% CI 1.06–1.19; p < 0.001), and hyperlactatemia (OR 1.57; 95% CI 1.18–2.09; p = 0.002) were also significant risk factors for hospital mortality. In our cohort, ICU survivors with pancreas-biliary cancer was associated with a lower risk of hospital mortality (OR 0.48; 95% CI 0.23–0.99; p = 0.048). ICU admission due to shock was associated with lower hospital mortality compared to admission due to respiratory failure (OR 0.36; 95% CI 0.19–0.67; p = 0.001). Figure 2 depicts 1-year survival curves of study patients according to their mental status (A), mobility status (B), and oxygen devices (C) at the time of ICU discharge. The one-year survival rates were significantly lower in patients with delirium (35%), coma (26%, p < 0.001), limited mobility (37%, p = 0.003), or on oxygen therapies (35%, p < 0.001).
 |
Table 4 Risk Factors Associated with in-Hospital Mortality in ICU Survivors (n = 704) |
 |
Figure 2 One-year survival curve (A) according to delirium and coma status (B) according to mobility status (C) according to oxygen device at the time of ICU discharge. Delirium was assessed using CAM-ICU assessment tools. Mobility was assessed using the Braden scale. Abbreviations: BiPAP, Bilevel positive airway pressure; HFNC, high-flow nasal cannula. |
Patients with mobility limitation had a significantly longer median duration of mechanical ventilation (5.0 [3.0–10.0] vs 2.0 [1.0–5.0] days, p < 0.001), and respiratory failure was more commonly identified as the cause of ICU admission among patients with mobility limitation (44.8% vs 28.5%, p < 0.001). (Supplementary Table 2). Missing data across the overall analysis are summarized in Appendix 2.
Discussion
This retrospective cohort study of ICU survivors with solid malignancies analyzed seven years of data from a single center in Korea. We previously published research on risk factors for ICU mortality at ICU admission among the entire cohort of ICU patients with solid malignancies.21 This current study extends that research by focusing on a different patient population, namely ICU survivors at the time of ICU discharge, and emphasizes the role of post-ICU impairments in these patients, with a particular focus on patient characteristics at the time of ICU discharge. Patients who had delirium or coma, mobility limitations, or were receiving oxygen therapy at the time of ICU discharge had a significantly higher risk of both in-hospital and long-term mortalities. The in-hospital mortality rate for study patients was 25.1%, and they died a median of 10 days after ICU discharge. The 1-year mortality rate was as high as two-thirds. To our knowledge, this is the first study to report risk factors at the time of ICU discharge for short- and long-term mortality in ICU survivors with solid malignancies.
Our study examined the influence of cognitive and physical impairments present at the time of ICU discharge on post-ICU hospital mortality and 1-year mortality in patients with solid malignancies. After discharge from acute critical illness, patients may still suffer from persistent hypoxia, ICU-acquired weakness (ICU-AW), reduced physical function, and psychiatric and cognitive problems.4 In our cohort, a quarter of the patients had altered mental status, including delirium or coma, at the time of ICU discharge. Previous studies have shown that delirium in critically ill adults is strongly associated with cognitive impairment 3 to 12 months after ICU discharge and longer hospital stays, while no consistent association with mortality has been reported.22,23 Our findings showed that delirium at ICU discharge was associated with increased in-hospital mortality in patients with solid malignancies. As many as 80% of patients at the time of ICU discharge reported new physical impairments, including ICU-AW and pulmonary dysfunction.24 ICU-AW specifically manifests as poor mobility, weakness, and reduced exercise tolerance. According to a previous report, this condition commonly occurs in patients with sepsis or in those receiving mechanical ventilation for more than 4 days.25 Consistent with this, ICU survivors with mobility limitation in our cohort had a median of 5 days of mechanical ventilation, compared to 2 days in those without mobility limitation. In our cohort, 80% of patients had mobility limitations, and 89% of patients received oxygen therapy due to persistent pulmonary dysfunction at the time of ICU discharge. Our findings indicate that physical impairments in solid malignancies impact both hospital mortality and 1-year mortality. As ICU-acquired weakness and pulmonary dysfunction can persist for years,4 and a previous study reported that more than half of patients experienced PICS at 1 year after hospital discharge,26 these post-ICU impairments may substantially limit functional performance. In patients with cancer, especially those with limited life expectancy, impaired physical function may delay or prevent the resumption of cancer treatment, which in turn can contribute to disease progression or reduced survival.27 Decline in performance caused by physical impairment could act as barriers to chemotherapy and other oncologic treatments. Although cognitive impairment alone may not necessarily preclude further treatment, significant changes in cognitive function could influence oncologists’ decisions regarding chemotherapy. In our cohort, 96.5% of patients had physical or cognitive impairments at the time of ICU discharge, which is a higher proportion than the reported prevalence of PICS in the general population.6 Due to the existing burden of chronic illness from underlying solid malignancies,28 patients may be vulnerable to developing post-ICU impairments. Further research is needed on the impact of PICS on the quality of life in patients with solid malignancies, especially because quality of life is a major treatment consideration in patients with limited life expectancy.29
The present study showed a higher in-hospital mortality rate (24% vs 12%) compared to the previous study by Lee et al,10 which involved all medical ICU survivors in a single Korean center. In Lee’s study, a solid malignancy was identified as a risk factor for in-hospital mortality, with an odds ratio of 4.1. In our ICU survivors with solid malignancies, the stage of the underlying solid malignancy was not related to in-hospital mortality after ICU discharge. However, the presence of remaining organ dysfunction at the time of ICU discharge, including hepatic, cardiovascular, pulmonary, and central nervous system dysfunction, was independently associated with in-hospital mortality. Among the different types of cancer, pancreatic-biliary cancer was associated with lower hospital mortality in our cohort of ICU survivors. This may be partly explained by previous reports suggesting that biliary septic shock, a potentially reversible condition when treated with prompt intervention, is a common cause of ICU admission in this population.30 In our prior study, pancreatic-biliary cancer was also associated with lower ICU mortality compared to other cancer types, showing a similar pattern to what was observed in this study.21 Rapid shock reversal through biliary interventions in these cases could lead to minimal residual organ dysfunction and improved short-term outcomes, including lower ICU or hospital mortality.
In those without cancer, the 1-year mortality rate of ICU survivors has been reported to be 10% to 20%.31,32 However, in our study, 61% of ICU survivors with solid malignancies died within 1 year, and even among patients discharged alive from the hospital, 48% of them died within 1 year. Our significantly higher 1-year mortality rate compared to that of the general ICU population highlights that, despite the decreased ICU mortality in cancer patients due to improved critical care, their long-term outcomes still remain poor. This may be due to the nature of the advanced cancer itself or the discontinuation of oncologic treatment caused by the patient’s post-ICU impairment. According to the study by Borcoman et al,8 the inability to receive oncologic treatment after ICU discharge was a significant risk factor for 1-year mortality after ICU discharge, with a hazard ratio of 5.34.
Our findings show that the prognosis of patients with solid malignancies who survived from the ICU is particularly poor. Therefore, considering the shortage of ICU beds and the poor prognosis of these patients, it is crucial that initial decisions regarding life-sustaining treatment be informed by an understanding of the anticipated long-term prognosis after ICU care and through a well-informed discussion involving the patient, family, and attending oncologist. In our cohort, 83% of the hospital non-survivor group made an informed decision not to receive further life-sustaining treatment after being discharged alive from the ICU. These results suggest that there was a discrepancy between the recovery expected by patients, their families, and oncologists, and the actual state of recovery after the initial ICU treatment in many patients. Because mechanical ventilation for more than 4 days and sepsis have been reported as risk factors for the development of ICU-acquired weakness, many patients who are treated in the ICU may continue to suffer from weakness after discharge from the ICU.25 The patients and their families need to be aware of the possibility that patients may have remaining organ dysfunctions or mental or physical impairments, which can prevent them from undergoing further cancer treatment after discharge from the ICU.
This study has several limitations. First, due to its single-center design, the generalizability of our findings may be limited. Nevertheless, our study includes a substantial cohort of patients from one of the largest referral hospitals in Korea over a 7-year period. Second, most of the patients in this study were in the locally advanced or metastatic stage, and therefore, they are not representative of patients with all types of solid malignancies. This reflects the real-world composition of patients with solid malignancies who were unexpectedly admitted to the ICU in a tertiary hospital in Korea. Patients in locally advanced or metastatic stages may be more susceptible to life-threatening conditions, such as sepsis or acute respiratory failure, than patients in early stages because cancer treatments can weaken the immune system.33 Third, our study lacks detailed information on responses to chemotherapy, which may influence long-term mortality. Fourth, our assessment of physical impairment was limited by the retrospective nature of the study. In the context of PICS, physical impairments encompass a broad spectrum of conditions including ICU-acquired weakness, impaired pulmonary function, cachexia, and fatigue.6,34 These can be evaluated using structured questionnaires, pulmonary function tests, the 6-minute walk test, or objective assessments such as the Medical Research Council muscle strength score, nerve conduction studies, or electromyography.35,36 However, such evaluations could not be performed in our study. Instead, we used the Braden mobility subscale to assess reduced physical function, and interpreted the persistent need for respiratory support at ICU discharge as indicative of pulmonary dysfunction. While these measures do not fully capture the diagnostic criteria of physical impairments in PICS, they represent clinically meaningful proxies for physical limitations in this patient population.37 Lastly, since our study did not include a comparison group of patients with solid malignancies who were not admitted to the ICU, it limits our ability to compare post-discharge outcomes that are specific to ICU survivors.
Conclusions
In our study, a considerable portion of ICU survivors with solid malignancies died in the hospital and within one year after ICU discharge. Cognitive impairment, mobility impairment, and persistent pulmonary dysfunction at ICU discharge were significant risk factors for both in-hospital and long-term mortality.
Abbreviations
BiPAP, bilevel positive airway pressure; BMI, body mass index; CAM-ICU, Confusion Assessment Method for the ICU; GCS, Glasgow Coma Scale; HFNC, high-flow nasal cannula; ICU, intensive care unit; ICU-AW, ICU-acquired weakness; IQR, interquartile range; OR, Odds Ratio; PICS, post-intensive care syndrome; RASS, Richmond Agitation Sedation Scale.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Martos-Benitez FD, Soler-Morejon CD, Lara-Ponce KX, et al. Critically ill patients with cancer: a clinical perspective. World J Clin Oncol. 2020;11(10):809–835. doi:10.5306/wjco.v11.i10.809
2. Vigneron C, Charpentier J, Valade S, et al. Patterns of ICU admissions and outcomes in patients with solid malignancies over the revolution of cancer treatment. Ann Intensive Care. 2021;11(1):182. doi:10.1186/s13613-021-00968-5
3. Zampieri FG, Romano TG, Salluh JIF, et al. Trends in clinical profiles, organ support use and outcomes of patients with cancer requiring unplanned ICU admission: a multicenter cohort study. Int Care Med. 2021;47(2):170–179. doi:10.1007/s00134-020-06184-2
4. Needham DM, Davidson J, Cohen H, et al. Improving long-term outcomes after discharge from intensive care unit. Crit Care Med. 2012;40(2):502–509. doi:10.1097/CCM.0b013e318232da75
5. Geense WW, Zegers M, Peters MAA, et al. New physical, mental, and cognitive problems 1 year after ICU admission: a prospective multicenter study. Am J Respir Crit Care Med. 2021;203(12):1512–1521. doi:10.1164/rccm.202009-3381OC
6. Hiser SL, Fatima A, Ali M, Needham DM. Post-intensive care syndrome (PICS): recent updates. J Intensive Care. 2023;11(1):23. doi:10.1186/s40560-023-00670-7
7. van der Zee EN, Termorshuizen F, Benoit DD, et al. One-year mortality of cancer patients with an unplanned ICU admission: a cohort analysis between 2008 and 2017 in the Netherlands. J Intensive Care Med. 2022;37(9):1165–1173. doi:10.1177/08850666211054369
8. Borcoman E, Dupont A, Mariotte E, et al. One-year survival in patients with solid tumours discharged alive from the intensive care unit after unplanned admission: a retrospective study. J Crit Care. 2020;57:36–41. doi:10.1016/j.jcrc.2020.01.027
9. Es LGA, de Maio Carrilho CMD, Talizin TB, Cardoso LTQ, Lavado EL, Grion CMC. Risk factors for hospital mortality in intensive care unit survivors: a retrospective cohort study. Acute Crit Care. 2023;38(1):68–75. doi:10.4266/acc.2022.01375
10. Lee J, Cho Y-J, Kim SJ, et al. Who dies after ICU discharge? Retrospective analysis of prognostic factors for in-hospital mortality of ICU survivors. J Korean Med Sci. 2017;32(3):528–33.
11. Zhou M, Zhang J, Xu Z, Gu H, Chen Z, Ding Y. Incidence of and risk factors for post–intensive care syndrome among Chinese respiratory intensive care unit patients: a cross-sectional, prospective study. Austr Crit Care. 2023;36(4):464–469. doi:10.1016/j.aucc.2022.07.005
12. Gayat E, Cariou A, Deye N, et al. Determinants of long-term outcome in ICU survivors: results from the FROG-ICU study. Critical Care. 2018;22(1). doi:10.1186/s13054-017-1922-8.
13. Meyers DE, Pasternak M, Dolter S, et al. Impact of performance status on survival outcomes and health care utilization in patients with advanced NSCLC treated with immune checkpoint inhibitors. JTO Clin Res Rep. 2023;4(4):100482. doi:10.1016/j.jtocrr.2023.100482
14. West HJ, Jin JO. JAMA oncology patient page. performance status in patients with cancer. JAMA Oncol. 2015;1(7):998. doi:10.1001/jamaoncol.2015.3113
15. Dall’Olio FG, Maggio I, Massucci M, Mollica V, Fragomeno B, Ardizzoni A. ECOG performance status ≥2 as a prognostic factor in patients with advanced non small cell lung cancer treated with immune checkpoint inhibitors-A systematic review and meta-analysis of real world data. Lung Cancer. 2020;145:95–104. doi:10.1016/j.lungcan.2020.04.027
16. Hanna TP, King WD, Thibodeau S, et al. Mortality due to cancer treatment delay: systematic review and meta-analysis. BMJ. 2020;371:m4087. doi:10.1136/bmj.m4087
17. Lafferty M, Fauer A, Wright N, Manojlovich M, Friese CR. Causes and consequences of chemotherapy delays in ambulatory oncology practices: a multisite qualitative study. Oncol Nurs Forum. 2020;47(4):417–427. doi:10.1188/20.ONF.417-427
18. Gusmao-Flores D, Salluh JI, Chalhub R, Quarantini LC. The confusion assessment method for the intensive care unit (CAM-ICU) and intensive care delirium screening checklist (ICDSC) for the diagnosis of delirium: a systematic review and meta-analysis of clinical studies. Crit Care. 2012;16(4):R115. doi:10.1186/cc11407
19. Braden BJ. The Braden scale for predicting pressure sore risk: reflections after 25 years. Adv Skin Wound Care. 2012;25(2):61. doi:10.1097/01.ASW.0000411403.11392.10
20. Lee SY, Oh DK, Hong SB, Lim CM, Huh JW. Neuromuscular blocking agents and opioids are major risk factors for developing pressure injuries in patients in the intensive care unit. Korean J Intern Med. 2022;37(6):1186–1194. doi:10.3904/kjim.2021.546
21. Lee SY, Huh JW, Hong SB, Lim CM, Ahn JH. Short-term and long-term outcomes of critically ill patients with solid malignancy: a retrospective cohort study. Korean J Intern Med. 2024;39(6):957–966. doi:10.3904/kjim.2024.054
22. Devlin JW, Skrobik Y, Gelinas C, et al. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. 2018;46(9):e825–e873. doi:10.1097/CCM.0000000000003299
23. Cavallazzi R, Saad M, Marik PE. Delirium in the ICU: an overview. Ann Intensive Care. 2012;2(1):49. doi:10.1186/2110-5820-2-49
24. Schwitzer E, Jensen KS, Brinkman L, et al. Survival ≠ Recovery. CHEST Critical Care. 2023;1(1):100003. doi:10.1016/j.chstcc.2023.100003
25. Harvey MA, Davidson JE. Postintensive care syndrome: right care, right now and later. Crit Care Med. 2016;44(2):381–385. doi:10.1097/CCM.0000000000001531
26. Marra A, Pandharipande PP, Girard TD, et al. Co-occurrence of post-intensive care syndrome problems among 406 survivors of critical illness. Crit Care Med. 2018;46(9):1393–1401. doi:10.1097/CCM.0000000000003218
27. Benguerfi S, Messéant O, Painvin B, et al. Factors associated with cancer treatment resumption after ICU stay in patients with solid tumors. Ann Intensive Care. 2024;14(1):135. doi:10.1186/s13613-024-01366-3
28. Mishra S, Gulia A, Satapathy S, Gogia A, Sharma A, Bhatnagar S. Caregiver burden and quality of life among family caregivers of cancer patients on chemotherapy: a prospective observational study. Indian J Palliat Care. 2021;27(1):109–112. doi:10.4103/IJPC.IJPC_180_20
29. Akhlaghi E, Lehto RH, Torabikhah M, et al. Chemotherapy use and quality of life in cancer patients at the end of life: an integrative review. Health Qual Life Outcomes. 2020;18(1):332. doi:10.1186/s12955-020-01580-0
30. Kemoun G, Weiss E, El Houari L, et al. Clinical features and outcomes of patients with pancreatic cancer requiring unplanned medical ICU admission: a retrospective multicenter study. Dig Liver Dis;2023. 514–521. doi:10.1016/j.dld.2023.08.049
31. Bastian K, Hollinger A, Mebazaa A, et al. Association of social deprivation with 1-year outcome of ICU survivors: results from the FROG-ICU study. Int Care Med. 2018;44(12):2025–2037. doi:10.1007/s00134-018-5412-5
32. Nakazone MA, Doherty Z, Kippen R, et al. Long-term outcomes of hospital survivors following an ICU stay: a multi-centre retrospective cohort study. PLoS One. 2022;17(3):e0266038.
33. Sharma A, Jasrotia S, Kumar A. Effects of chemotherapy on the immune system: implications for cancer treatment and patient outcomes. Naunyn Schmiedebergs Arch Pharmacol. 2023;397(5):2551–66.
34. Mikkelsen ME, Still M, Anderson BJ, et al. Society of critical care medicine’s international consensus conference on prediction and identification of long-term impairments after critical illness. Crit Care Med. 2020;48(11):1670–1679. doi:10.1097/CCM.0000000000004586
35. Stevens RD, Marshall SA, Cornblath DR, et al. A framework for diagnosing and classifying intensive care unit-acquired weakness. Crit Care Med. 2009;37(10 Suppl):S299–308. doi:10.1097/CCM.0b013e3181b6ef67
36. Na A, O’Brien JM Jr, Hoffmann SP, et al. Acquired weakness, handgrip strength, and mortality in critically ill patients. Am J Respir Crit Care Med. 2008;178(3):261–268. doi:10.1164/rccm.200712-1829OC
37. Valiani V, Chen Z, Lipori G, Pahor M, Sabbá C, Manini TM. Prognostic value of Braden activity subscale for mobility status in hospitalized older adults. J Hosp Med. 2017;12(6):396–401. doi:10.12788/jhm.2748
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.