Back to Journals » Clinical Epidemiology » Volume 12
Physical Activity as an Effect Modifier of the Association Between Obesity and Venous Thromboembolism: A Danish Population-Based Cohort Study
Authors Solli H ![]() , Olsen M, Larsen FB, Pedersen L, Schmidt M
, Olsen M, Larsen FB, Pedersen L, Schmidt M ![]()
Received 1 August 2020
Accepted for publication 12 November 2020
Published 8 December 2020 Volume 2020:12 Pages 1361—1370
DOI https://doi.org/10.2147/CLEP.S275079
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Eyal Cohen
Henrik Solli,1 Morten Olsen,1 Finn Breinholt Larsen,2 Lars Pedersen,1 Morten Schmidt1,3
1Department of Clinical Epidemiology, Aarhus University Hospital, Aarhus, Denmark; 2DEFACTUM, Social & Health Services and Labour Market, Central Denmark Region, Aarhus, Denmark; 3Department of Cardiology, Aarhus University Hospital, Aarhus, Denmark
Correspondence: Henrik Solli
Department of Clinical Epidemiology, Aarhus University Hospital, Olof Palmes Allé 43-45, Aarhus 8200 Aarhus N, Denmark
Email [email protected]
Purpose: Obesity is an established risk factor for venous thromboembolism (VTE), while studies on physical inactivity and VTE risk show conflicting results. We examined whether physical activity modified the association between obesity and VTE.
Patients and Methods: We conducted a population-based cohort study by combining data on outcome diagnoses, comorbidities and medication from nationwide registries with self-reported lifestyle data from an extensive Danish lifestyle questionnaire (2001– 2015). We computed incidence rates (IRs) and hazard ratios (HRs) of VTE for categories of body mass index (BMI), among the total study population (n=57,523) and for physically active (n=25,387) and inactive individuals (n=30,902) separately.
Results: Obesity (BMI ≥ 30 kg/m2) was as expected associated with increased VTE risk compared with normal weight (HR 1.62, 95% confidence interval (CI): 1.26– 2.09). Independent of BMI category, the rate of VTE was higher for inactive than active individuals. Thus, among obese individuals, the IR per 1000 person-years was 2.03 (95% CI: 1.60– 2.57) for inactive and 1.44 (95% CI: 0.97– 2.15) for active individuals. In contrast, the HR for VTE comparing obese with normal weight individuals were higher for active (HR 2.19, 95% CI: 1.35– 3.58) than inactive individuals (HR 1.36, 95% CI: 1.00– 1.84).
Conclusion: Physical activity acts as an effect measure modifier of the association between obesity and VTE. Thus, physical activity reduced the absolute rate of VTE among obese individuals but increased the relative rate of VTE among obese compared with normal weight individuals.
Keywords: venous thromboembolism, obesity, exercise, epidemiology, surveys and questionnaires
Introduction
Venous thromboembolism (VTE) includes deep venous thrombosis and pulmonary embolism. VTE has a reported incidence rate (IR) per 1000 person-years (PY) of 1.5 in individuals aged 15 and older, rising sharply with age.1 VTE is a potentially lethal condition2 and is a leading cause of preventable in-hospital deaths.3 Conditions leading to a pro-thrombotic state, such as pregnancy, surgery, trauma, cancer, and immobilization, are all established as transient risk factors for VTE.1
A growing body of research has pointed to obesity as a risk factor for VTE.4–11 In 2008, a meta-analysis pooling studies of high quality in which body mass index (BMI) was adequately measured found an odds ratio of 1.84 (95% confidence interval (CI): 1.55–2.18) for VTE among obese individuals.12 Studies investigating the association between physical activity and VTE have reported conflicting results.6–11,13–17 Thus, some studies have found that physical activity either reduce10,11,15–17 or, under some conditions, increase6,13–15 the risk of VTE, while others found no association.7–9,13,14 While some studies have investigated whether BMI modifies the association between physical activity and VTE,13,15 to our knowledge, no previous study has assessed whether physical activity modifies the obesity-associated risk on VTE.
We hypothesized that physical activity reduced the rate for VTE among obese individuals, making physical activity an effect measure modifier of the association between obesity and VTE. We therefore identified responders to an extensive lifestyle questionnaire and conducted a cohort study to assess the association between BMI and VTE among physically active and inactive individuals.
Patients and Methods
Setting
We conducted this cohort study among residents in one of Denmark’s five regions, the Central Denmark Region, which has a population of approximately 1.3 million individuals.18 The Danish National Health Service provides universal tax-supported health care which guarantees free and unfettered access to general practitioners and hospitals, and partial reimbursement for prescribed medications.19
Accurate and unambiguous individual-level linkage of all Danish registries is possible using the unique Civil Personal Register (CPR) number assigned to all residents at birth or upon immigration.20 The CPR number is issued by the Danish Civil Registration System which is updated daily and contains vital statistics of members of the Danish population – including date of birth, change of address, date of emigration, and exact date of death – dating back to 1968.20
Study Cohort
The questionnaire-based public health survey “How Are You?” has been conducted five times since 2001 by The Population Health Surveys unit, Central Denmark Region.21 Our study population included all individuals who answered the questionnaire in 2001, 2006, and 2010. Questionnaires were distributed by mail to a random sample of inhabitants of the Central Denmark Region aged 25–79, and from 2010: aged 16 and older, with at least one parent born in Denmark. Study participation was voluntary, and participants provided self-reported answers to a detailed questionnaire regarding lifestyle factors containing approximately 400 questions. Response rates for the different questionnaires varied between 76% and 65%.22 A total of 57,523 individuals were eligible for inclusion in the study population.
Exposure Variables
Information regarding our two exposure variables, BMI and physical activity, was extracted from the “How Are You?” survey. BMI was calculated as weight in kilograms divided by height in meters squared and grouped into four categories, as defined by the World Health Organization: underweight (BMI<18.5), normal weight (18.5≤BMI<25), overweight (25≤BMI<30), and obese (BMI≥30).23 Physical activity was dichotomized as “active” and “inactive”. Because of minor differences in the wording of the different questionnaires, some discrepancies occurred among the sub-cohorts. All physically active questionnaire responders stated that they conducted sport or other physical activity in their spare time on a regular basis. In addition to this, physically active individuals in the 2001 sub-cohort stated that their activities exceeded 2 hours per week, whereas physically active individuals in the 2006 and 2010 sub-cohort stated that they spent at least 2 days per week with more than 30 minutes of moderate to strenuous physical activity during work or spare time.
Outcome Variables
We used the Danish National Patient Registry (DNPR) to identify all individuals with a first-time primary or secondary diagnosis of VTE (defined as deep venous thrombosis or pulmonary embolism).24 The DNPR records information on patients discharged from all Danish non-psychiatric hospitals since 1 January 1977 and from all emergency room and outpatient specialty clinic visits since 1995.24 Each hospital discharge or outpatient visit is recorded in the registry with one primary diagnosis and one or more secondary diagnoses classified according to the International Classification of Diseases, 8th revision (ICD-8) until the end of 1993 and the 10th revision (ICD-10) thereafter.24
We further subdivided VTE diagnoses into provoked and unprovoked events.6 A VTE event was defined as provoked if the patient had a history of malignancy any time prior to or within 90 days after the diagnosis of VTE or a recorded discharge diagnosis of fracture, trauma, surgery, or pregnancy within 90 days before the VTE diagnosis. Conditions defining provoked VTE were recorded in the DNPR. Remaining cases were classified as unprovoked.
Covariates
The Danish National Health Service Prescription Database (DNHSPD) was used to identify the use of different classes of medications among study participants.25 This database encompasses the reimbursement records of all reimbursable drugs sold in community pharmacies and hospital-based outpatient pharmacies in Denmark since 2004. Stored in the database is information regarding the dispensed drug (name, form, strength, and pack size), patient, prescriber, and pharmacy.25 Drug use was defined as a registered redemption of a reimbursable drug within 90 days before start of follow-up. We collected data on statins, vitamin K antagonists, and low-dose aspirin. We did not record use of Non-vitamin K antagonist oral anticoagulants (NOACs), as these drugs were not available in Denmark at start of follow-up for the different sub-cohorts (2001–2010).
We used the Charlson comorbidity index (CCI) to assess each individual’s burden of comorbidity.26 The CCI assigns between one to six points to a range of diseases depending on their severity and anticipated 1-year mortality.26 Diagnoses included in the CCI were extracted from the DNPR.27 For all 19 comorbidities in the index, we computed the cumulative score for each individual study participant and defined three categories of comorbidity based on scores of 0 (low), 1–2 (moderate), and ≥3 (severe).28
Diagnoses of hypertension, atrial fibrillation/flutter, and diabetes were extracted from the DNPR, combined with prevalence of either hypertension or diabetes stated in the “How Are You?” questionnaire. We also used the redemption of anti-diabetic drugs through the DNHSPD to identify diabetic patients.25
Potential confounding lifestyle variables were extracted from the “How Are You?” questionnaire. Smoking status was categorized into three categories: never smokers, former smokers, and current smokers. Level of education was grouped into three categories: 1) ≤10 years of primary education, 2) high school, vocational training or equivalent, or short higher education, and finally 3) higher education of medium or long duration.
Statistical Analysis
All individuals were followed from the date of return of the questionnaire in 2001, 2006, or 2010, depending on the sub-cohort, and until the date of outcome, death, emigration, or 1 January 2015, whichever came first. We censored all analysis time at the date of the first VTE event, regardless of whether the event was provoked or unprovoked. We excluded all individuals with a recorded diagnosis of VTE before start of follow-up from the study population (n=534). For individuals with missing information regarding one or more lifestyle factors in the “How Are You?” survey, we imputed the missing values using the multiple imputation by chained equations (MICE) method.29 Among the individuals (n=1690) who was sent more than one questionnaire, we used the date and lifestyle factors reported in the first answered questionnaire as baseline, and all later questionnaire answers were disregarded. To assess physical activity as an effect measure modifier of the association between obesity and VTE, we made two sub-cohorts of physically active and inactive individuals. Individuals with missing information regarding physical activity (n=1234, including 26 with VTE events) were excluded from this sub-analysis.
We calculated IRs as numbers of outcomes per 1000 person-years for BMI and physical activity groups. We computed crude and adjusted hazard ratios (HRs) for all BMI groups using normal weight individuals as reference for all outcome events using Cox proportional-hazards regression. Carefully taking into consideration the relatively few number of outcomes, we chose to include only relevant confounding variables in our multivariate statistical model using the “change in estimate”-method.30 Although diabetes may be a risk factor for VTE, we chose not to adjust for this condition, as diabetes may be an intermediary step on the causal pathway between obesity and VTE, and thus not represent a confounding covariate. The proportional hazard assumption was assessed graphically for all analyses by plotting log(-log(survival function)) against time, and it was found to be valid. All statistical analyses were conducted using Stata software version 12.1.
Results
Descriptive Data
The demographical data for the total study population (n=57,523) according to BMI group (Table 1) showed that obese individuals had a higher proportion of physical inactivity compared with other BMI groups. Obese also had a higher burden of comorbidity, both Charlson Comorbidity Index score, individual comorbidities, and use of cardiovascular drugs.
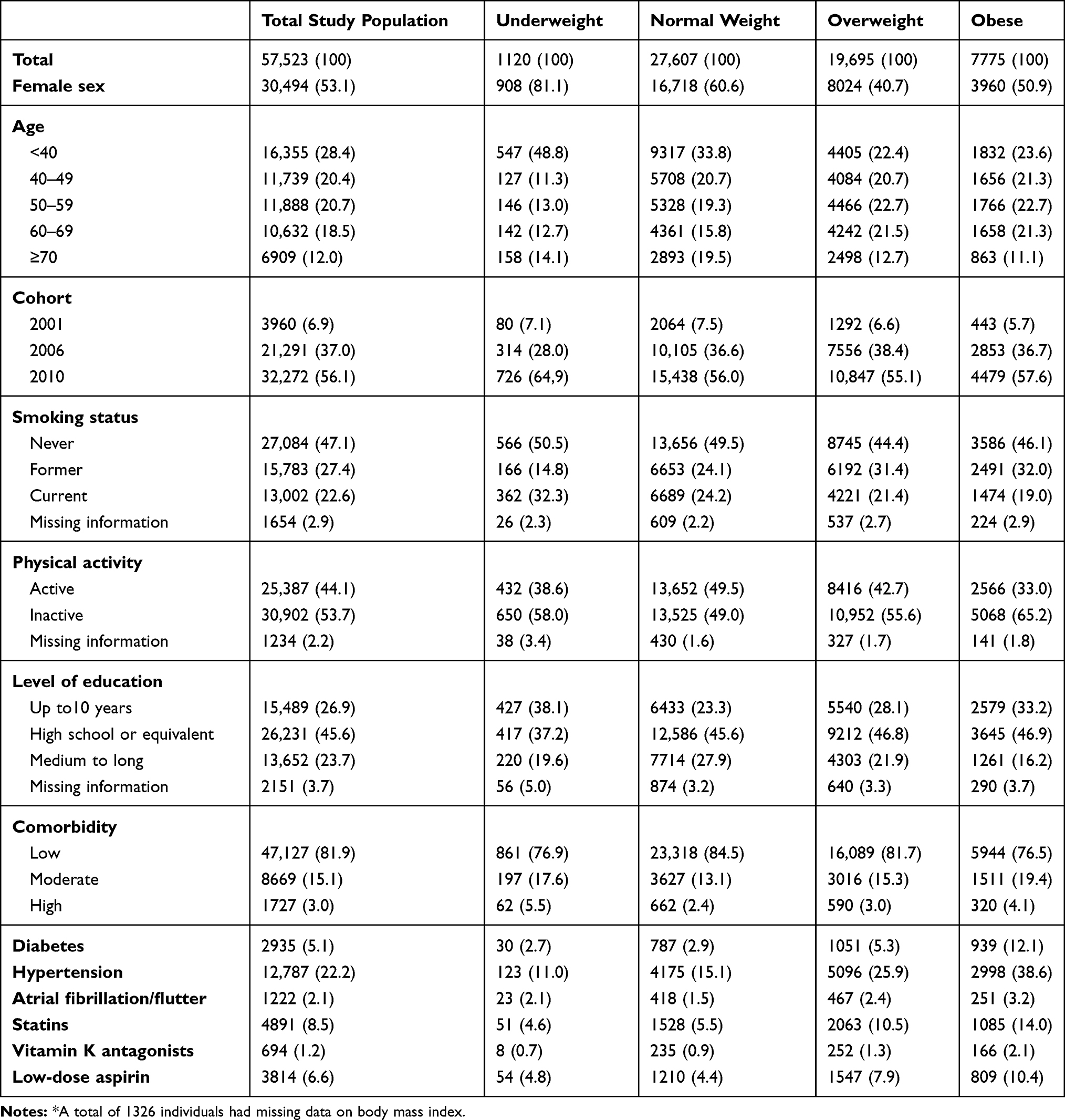 |
Table 1 Study Population Characteristics According to Body Mass Index Category* |
When stratifying the study population (n=57,523) on the physically active (n=25,387) and inactive (n=30,902) individuals (Table 2), we found that, independent of BMI category, inactive individuals had a higher proportion of current smokers, a lower level of education, and a higher burden of comorbidity and drug use than the physically active individuals.
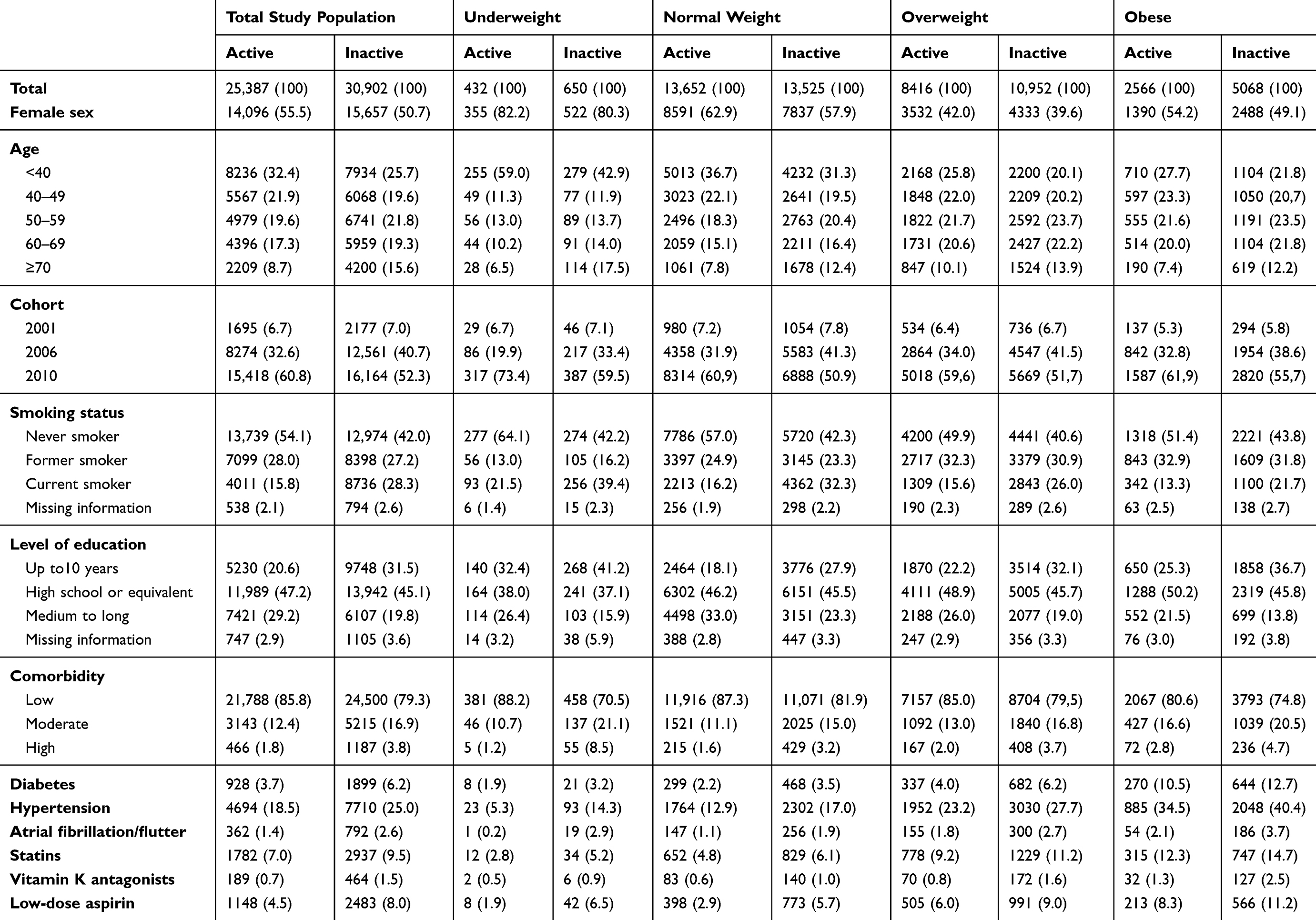 |
Table 2 Study Population Characteristics According to Body Mass Index Category and Physical Activity |
Effect Measures
A total of 534 VTE events were recorded during the follow-up time, 257 of which were provoked and 277 of which were unprovoked (Table 3). A total of 385,814 person-years of follow-up were recorded. The adjusted HR for VTE using normal weight individuals as reference were 0.96 (95% CI: 0.42–2.15) for underweight, 1.34 (95% CI: 1.09–1.64) for overweight, and 1.62 (95% CI: 1.26–2.09) for obese individuals. For overweight individuals, the HR did not differ between provoked and unprovoked VTE. For obese individuals, the risk of unprovoked VTE was 1.81 (95% CI: 1.27–2.58) and 1.43 (95% CI: 0.98–2.08) for provoked VTE.
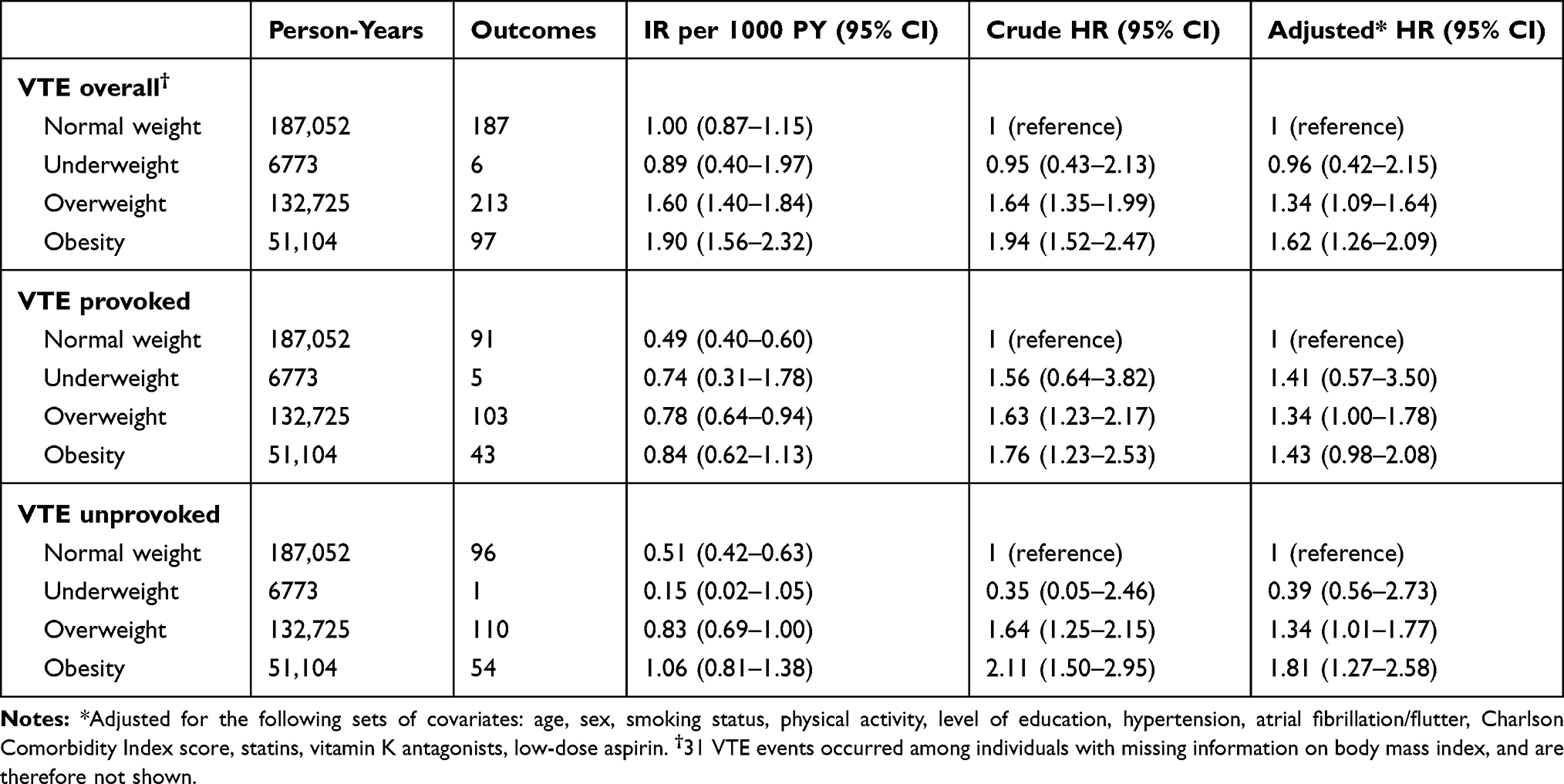 |
Table 3 Association Between Body Mass Index and Venous Thromboembolism |
When stratifying by physical activity, we observed that 168 VTE events occurred among active individuals and 340 events among inactive individuals. Inactive individuals had a consistent higher IR compared with active individuals overall (Supplementary eTable 1) and within the same BMI group (Table 4). Comparing active vs inactive individuals’ incidence rates per 1000 person-years for VTE yielded the following results: 0.63 (95% CI: 0.48–0.81) vs 1.32 (95% CI: 1.11–1.57) for normal weight, 1.49 (95% CI: 1.20–1.84) vs 1.70 (95% CI: 1.43–2.02) for overweight, and 1.44 (95% CI: 0.97–2.15) vs 2.03 (95% CI: 1.60–2.57) for obesity.
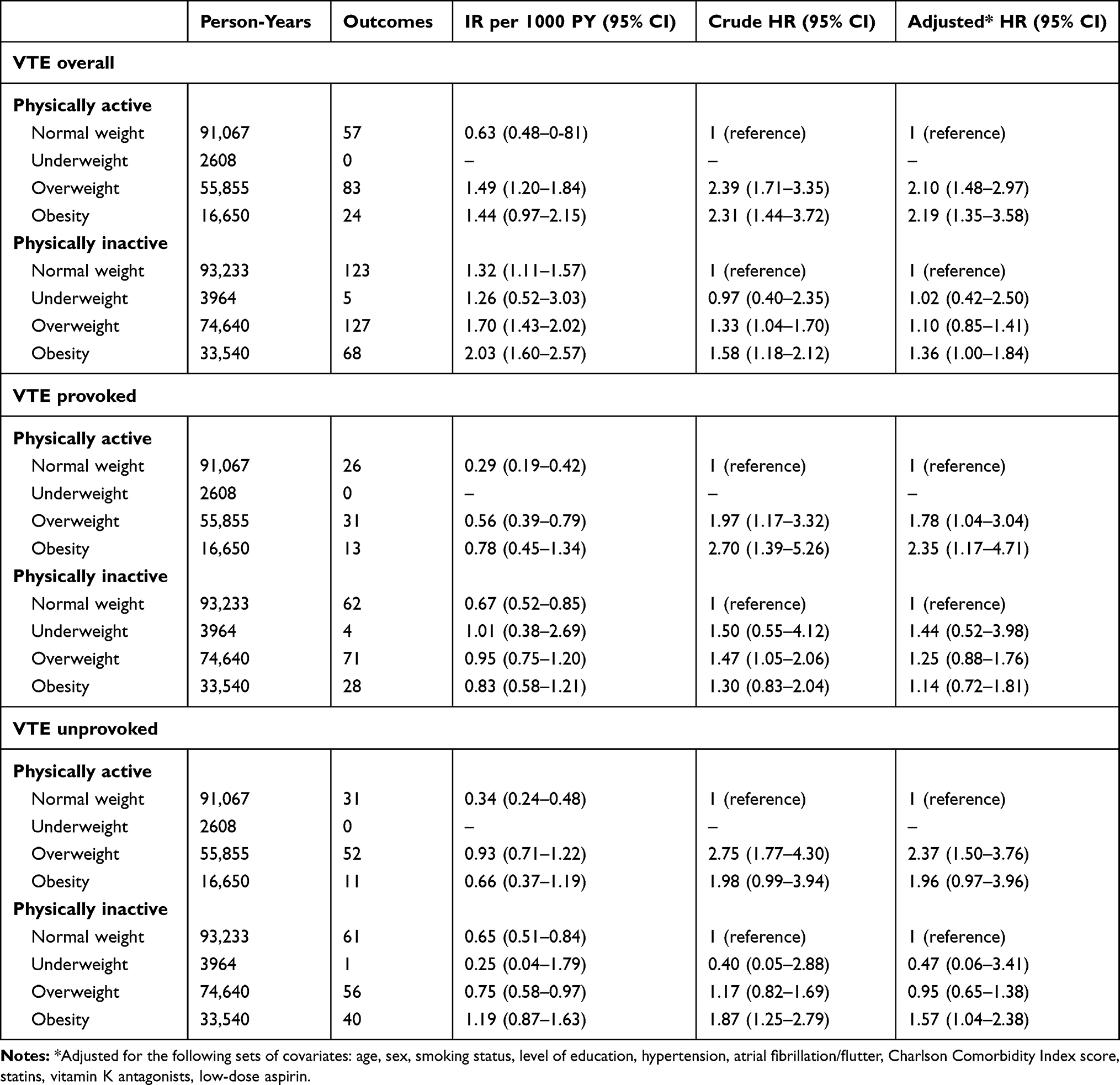 |
Table 4 Association Between Body Mass Index and Venous Thromboembolism Among Physically Active and Inactive Individuals |
The adjusted HR for VTE among overweight individuals compared with normal weight individuals were 2.10 (95% CI: 1.48–2.97) for active individuals and 1.10 (95% CI: 0.85–1.41) for inactive individuals. Among overweight individuals, active individuals had higher HRs of both provoked and unprovoked VTE compared with inactive individuals, the most pronounced difference being for unprovoked VTE. Obese individuals had an adjusted HR compared with normal weight individuals of 2.19 (95% CI: 1.35–3.58) for active and 1.36 (95% CI: 1.00–1.84) for inactive individuals. Among obese individuals, active individuals also had higher HRs of both provoked and unprovoked VTE, but here, the highest HR and broadest difference were found for provoked VTE.
Discussion
We found that obesity and physical inactivity were both risk factors of VTE. Importantly, physical inactivity increased the BMI-associated risk of VTE. Physical inactivity thus acted as an effect measure modifier. Obesity increased the rate of VTE compared with normal weight individuals relatively more in physical active individuals, likely due to the lower baseline risk of VTE among physical active individuals.
Comparison with Other Studies
Our results are in accordance with previous studies which have identified obesity as a risk factor for VTE.4–11 Studies investigating the association between physical activity and risk of VTE have reached different conclusions.6–11,13–17 Some studies have reported no association between physical activity as a whole and overall VTE,7–9,13,14 while others have found a reduction in VTE risk among physically active individuals.10,11,15–17 Furthermore, some studies have found an increased risk for VTE, especially provoked VTE among practitioners of strenuous exercise.6,13–15 This last finding is interesting, as it points to exercise having an opposite effect on arterial and venous thrombotic diseases.6
Two studies should be emphasized for their interesting conclusions in assessing the interplay between obesity and physical activity on VTE-risk. Borch et al13 conducted a cohort study among the general population of one region of Norway. Regular physical activity of both moderate and high intensity had no statistically significant effect on risk of overall VTE. High-intensity exercise was associated with an elevated risk of provoked VTE compared with inactive individuals, and moderate physical activity was associated with a decreased risk of VTE among subjects under 60 years of age. Borch et al found similar risk estimates for each BMI group; however, normal weight individuals who conducted moderate physical activity had a lower risk of VTE compared with inactive normal weight individuals, and obese individuals who conducted strenuous activity had a higher risk of VTE compared with obese inactive individuals.13 Armstrong et al15 conducted a cohort study as part of the Million Women Study, containing 1.1 million British women without previous vascular disease. Individuals who conducted moderate physical activity had a significant lower risk of VTE, as well as coronary heart disease and cerebrovascular events, compared with inactive individuals. Strenuous activity increased the risk of all three conditions. Armstrong et al found no strong evidence of heterogeneity between categories of BMI.15
Pathophysiological Explanations
Virchow’s triad states that the three main causes of thrombosis are venous stasis, endothelial injury, and hypercoagulability. Obesity has been linked with all these causes. Body fat may raise the intra-abdominal pressure and in turn limit venous return from the lower extremities.31 Perivascular adipose tissue in obese individuals is known to promote endothelial oxidative stress and a reduced bioavailability of nitric oxide.32 Furthermore, obesity has been showed to be correlated with elevated levels of several coagulation factors.31,33
Through several mechanisms, physical activity may counteract the adverse effects of obesity on thrombosis. Body movement activates the skeletal muscle pump, which in turn promotes venous return.34,35 Physical activity has been shown to reduce levels of C-reactive protein, which is a general marker of inflammation,36 as well as having beneficial effects on endothelial function, plasma viscosity, and platelet aggregation.37 However, all of the vascular beneficial effects of physical activity may be reverted due to the risk of exercise-induced injury, which may lead to both prolonged immobilization as well as tissue damage.38,39 The pathophysiological relationship between obesity, physical activity, and thrombosis is therefore complex to assess.
Strengths and Limitations
Some issues should be considered when interpreting our results. The free access to health care provided by the Danish Health System and the computerized manner in which discharge diagnoses are recorded minimized referral and diagnostic biases of the diagnosis of VTE. The positive predictive value of a VTE diagnosis in the DNPR has been reported as 88% for first-time events.40 Prevalence of diabetes and hypertension was not only determined by discharge diagnoses but also by reported comorbidity in the lifestyle questionnaire and, with regards to diabetes, redemption of antidiabetic drugs.
We cannot exclude unmeasured confounding. In general, responders to health questionnaires tend to be healthier than individuals who decline to participate. However, our study population had comparable proportions of both diabetic41 and hypertensive42 patients as well as BMI groups43 to that of the general Danish population. Although lifestyle factors such as obesity and smoking status tend to be underreported in questionnaires,44,45 because the information in the questionnaire was collected at the start of follow-up, we find it unlikely that the manner in which the questionnaire was answered should be associated with whether or not the individual experienced a VTE event. Still, the fact that lifestyle factors, among these our exposure variables BMI and physical activity, were based on self-reported data rather than direct measurements, is a limitation.
We were unable to record individual changes in categories of BMI, physical activity or confounding variables after start of follow-up. A recent study on lifestyle factors and risk of myocardial infarction and VTE found similar risk estimates when recoding lifestyle data once versus adjusting risk estimates for changes in lifestyle through several re-assessments of lifestyle factors.46
There is a potential risk of residual confounding, as physical activity was only dichotomized as active/inactive, in contrast to previous studies, which have been able to further quantify the amount of physical activity. Finally, the low number of outcomes was a major limitation in our study.
Conclusion
Obesity and physical inactivity are both associated with risk of VTE. Physical activity act as an effect measure modifier of the association between obesity and VTE. Thus, physical activity reduced the absolute rate of VTE among obese individuals, but increased the relative rate of VTE among obese compared with normal weight individuals due to the lower baseline risk of VTE among physically active individuals.
Abbreviations
BMI, body mass index; CCI, Charlson comorbidity index; CI, confidence interval; CPR, civil personal register; DNHSPD, Danish National Health Service Prescription Database; DNPR, Danish National Patient Registry; HR, hazard ratio; ICD-8, International Classification of Diseases, 8th revision; ICD-10, International Classification of Diseases, 10th revision; IR, incidence rate; kg, kilogram; m, metre; MICE, multiple imputation by chained equations; n, sample size; NOAC, non-vitamin K antagonist oral anticoagulants; PY, person-years; VTE, venous thromboembolism.
Ethics Statement
Approval from an ethics committee is not required for registry-based studies.
Data permissions: The study has been reported to the Danish Data Protection Board by Aarhus University.
Patient and Public Involvement: No patient involvement.
Disclosure
The authors report no conflicts of interest in this work. This work was supported by the Department of Clinical Epidemiology, the Danish Heart Foundation (grant number 13-04-R95-A4570-22752), the Department of Clinical Medicine’s travel grant (Aarhus University), and the Foundation of 17-12-1981. MS is supported by the Novo Nordisk Foundation (grant NNF19OC0054908). None of the sponsors had any involvement in the execution of this research project.
References
1. Heit JA, Silverstein MD, Mohr DN, et al. The epidemiology of venous thromboembolism in the community. Thromb Haemost. 2001;86(1):452–463. doi:10.1055/s-0037-1616243
2. Cohen AT, Agnelli G, Anderson FA, et al. Venous thromboembolism (VTE) in europe. the number of VTE events and associated morbidity and mortality. Thromb Haemost. 2007;98(4):756–764. doi:10.1160/TH07-03-0212
3. Beckman MG, Hooper WC, Critchley SE, Ortel TL. Venous thromboembolism: a public health concern. Am J Prev Med. 2010;38(4 Suppl):S495–501. doi:10.1016/j.amepre.2009.12.017
4. Severinsen MT, Overvad K, Johnsen SP, et al. Genetic susceptibility, smoking, obesity and risk of venous thromboembolism. Br J Haematol. 2010;149(2):273–279. doi:10.1111/j.1365-2141.2010.08086.x
5. Braekkan SK, Hald EM, Mathiesen EB, et al. Competing risk of atherosclerotic risk factors for arterial and venous thrombosis in a general population: the tromso study. Arterioscler Thromb Vasc Biol. 2012;32(2):487–491. doi:10.1161/ATVBAHA.111.237545
6. Glynn RJ, Rosner B. Comparison of risk factors for the competing risks of coronary heart disease, stroke, and venous thromboembolism. Am J Epidemiol. 2005;162(10):975–982. doi:10.1093/aje/kwi309
7. Wattanakit K, Lutsey PL, Bell EJ, et al. Association between cardiovascular disease risk factors and occurrence of venous thromboembolism. A time-dependent analysis. Thromb Haemost. 2012;108(3):508–515. doi:10.1160/TH11-10-0726
8. Holst AG, Jensen G, Prescott E. Risk factors for venous thromboembolism: results from the copenhagen city heart study. Circulation. 2010;121(17):1896–1903. doi:10.1161/CIRCULATIONAHA.109.921460
9. Tsai AW, Cushman M, Rosamond WD, Heckbert SR, Polak JF, Folsom AR. Cardiovascular risk factors and venous thromboembolism incidence: the longitudinal investigation of thromboembolism etiology. Arch Intern Med. 2002;162(10):1182–1189. doi:10.1001/archinte.162.10.1182
10. Lutsey PL, Virnig BA, Durham SB, et al. Correlates and consequences of venous thromboembolism: the iowa women’s health study. Am J Public Health. 2010;100(8):1506–1513.
11. Kim J, Kraft P, Hagan KA, Harrington LB, Lindstroem S, Kabrhel C. Interaction of a genetic risk score with physical activity, physical inactivity, and body mass index in relation to venous thromboembolism risk. Genet Epidemiol. 2018;42(4):354–365. doi:10.1002/gepi.22118
12. Ageno W, Becattini C, Brighton T, Selby R, Kamphuisen PW. Cardiovascular risk factors and venous thromboembolism: a meta-analysis. Circulation. 2008;117(1):93–102. doi:10.1161/CIRCULATIONAHA.107.709204
13. Borch KH, Hansen-Krone I, Braekkan SK, et al. Physical activity and risk of venous thromboembolism. the tromso study. Haematologica. 2010;95(12):2088–2094. doi:10.3324/haematol.2009.020305
14. van Stralen KJ, Doggen CJ, Lumley T, et al. The relationship between exercise and risk of venous thrombosis in elderly people. J Am Geriatr Soc. 2008;56(3):517–522. doi:10.1111/j.1532-5415.2007.01588.x
15. Armstrong ME, Green J, Reeves GK, Beral V, Cairns BJ. Million women study collaborators. Frequent physical activity may not reduce vascular disease risk as much as moderate activity: large prospective study of women in the united kingdom. Circulation. 2015;131(8):721–729. doi:10.1161/CIRCULATIONAHA.114.010296
16. van Stralen KJ, Le Cessie S, Rosendaal FR, Doggen CJ. Regular sports activities decrease the risk of venous thrombosis. J Thromb Haemost. 2007;5(11):2186–2192. doi:10.1111/j.1538-7836.2007.02732.x
17. Lindqvist PG, Epstein E, Olsson H. The relationship between lifestyle factors and venous thromboembolism among women: a report from the MISS study. Br J Haematol. 2009;144(2):234–240. doi:10.1111/j.1365-2141.2008.07460.x
18. Web page. Central Denmark region - region Midtjylland web site. Available from: https://www.rm.dk/om-os/english/.
19. Schmidt M, Schmidt SAJ, Adelborg K, et al. The danish health care system and epidemiological research: from health care contacts to database records. Clin Epidemiol. 2019;11:563–591. doi:10.2147/CLEP.S179083
20. Schmidt M, Pedersen L, Sorensen HT. The danish civil registration system as a tool in epidemiology. Eur J Epidemiol. 2014;29(8):541–549. doi:10.1007/s10654-014-9930-3
21. Web page. Population health surveys - DEFACTUM (en) web site. Available from: http://www.defactum.net/research-areas/bif/.
22. Web page. Oversigt over rapporter - DEFACTUM web site. Available from: http://www.defactum.dk/om-DEFACTUM/projektsite/hvordan-har-du-det/rapporter-og-analyser/oversigt-over-rapporter/.
23. Web page. WHO/Europe | nutrition - body mass index - BMI web site. Available from: http://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi.
24. Schmidt M, Schmidt SA, Sandegaard JL, Ehrenstein V, Pedersen L, Sorensen HT. The danish national patient registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449–490. doi:10.2147/CLEP.S91125
25. Johannesdottir SA, Horvath-Puho E, Ehrenstein V, Schmidt M, Pedersen L, Sorensen HT. Existing data sources for clinical epidemiology: the danish national database of reimbursed prescriptions. Clin Epidemiol. 2012;4:303–313. doi:10.2147/CLEP.S37587
26. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
27. Thygesen SK, Christiansen CF, Christensen S, Lash TL, Sorensen HT. The predictive value of ICD-10 diagnostic coding used to assess Charlson comorbidity index conditions in the population-based danish national registry of patients. BMC Med Res Methodol. 2011;11(1):
28. Jacobs DR
29. Sterne JA, White IR, Carlin JB, et al. Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. BMJ. 2009;338(jun29 1):b2393. doi:10.1136/bmj.b2393
30. Greenland S. Modeling and variable selection in epidemiologic analysis. Am J Public Health. 1989;79(3):340–349. doi:10.2105/AJPH.79.3.340
31. Allman-Farinelli MA. Obesity and venous thrombosis: a review. Semin Thromb Hemost. 2011;37(8):903–907. doi:10.1055/s-0031-1297369
32. Engin A. Endothelial dysfunction in obesity. Adv Exp Med Biol. 2017;960:345–379.
33. Singh P, Peterson TE, Barber KR, et al. Leptin upregulates the expression of plasminogen activator inhibitor-1 in human vascular endothelial cells. Biochem Biophys Res Commun. 2010;392(1):47–52. doi:10.1016/j.bbrc.2009.12.158
34. Sochart DH, Hardinge K. The relationship of foot and ankle movements to venous return in the lower limb. J Bone Joint Surg Br. 1999;81(4):700–704. doi:10.1302/0301-620X.81B4.0810700
35. McNally MA, Cooke EA, Mollan RA. The effect of active movement of the foot on venous blood flow after total hip replacement. J Bone Joint Surg Am. 1997;79(8):1198–1201. doi:10.2106/00004623-199708000-00012
36. Ford ES. Does exercise reduce inflammation? Physical activity and C-reactive protein among U.S. adults. Epidemiology. 2002;13(5):561–568. doi:10.1097/00001648-200209000-00012
37. Sherman DL. Exercise and endothelial function. Coron Artery Dis. 2000;11(2):117–122. doi:10.1097/00019501-200003000-00005
38. Jones BH, Cowan DN, Knapik JJ. Exercise, training and injuries. Sports Med. 1994;18(3):202–214. doi:10.2165/00007256-199418030-00005
39. Engelman DT, Gabram SG, Allen L, Ens GE, Jacobs LM. Hypercoagulability following multiple trauma. World J Surg. 1996;20(1):5–10. doi:10.1007/s002689900001
40. Sundboll J, Adelborg K, Munch T, et al. Positive predictive value of cardiovascular diagnoses in the danish national patient registry: a validation study. BMJ Open. 2016;6(11):
41. Web page. Sygdomsforekomst web site. Available from: http://esundhed.dk/sundhedsregistre/uks/uks01/Sider/Tabel.aspx.
42. Kronborg CN, Hallas J, Jacobsen IA. Prevalence, awareness, and control of arterial hypertension in denmark. J Am Soc Hypertens. 2009;3(1):19–24.e2. doi:10.1016/j.jash.2008.08.001
43. Bendixen H, Holst C, Sorensen TI, Raben A, Bartels EM, Astrup A. Major increase in prevalence of overweight and obesity between 1987 and 2001 among danish adults. Obes Res. 2004;12(9):1464–1472. doi:10.1038/oby.2004.183
44. Visscher TL, Viet AL, Kroesbergen IH, Seidell JC. Underreporting of BMI in adults and its effect on obesity prevalence estimations in the period 1998 to 2001. Obesity (Silver Spring). 2006;14(11):2054–2063. doi:10.1038/oby.2006.240
45. Fendrich M, Mackesy-Amiti ME, Johnson TP, Hubbell A, Wislar JS. Tobacco-reporting validity in an epidemiological drug-use survey. Addict Behav. 2005;30(1):175–181. doi:10.1016/j.addbeh.2004.04.009
46. Smabrekke B, Rinde LB, Hindberg K, et al. Atherosclerotic risk factors and risk of myocardial infarction and venous thromboembolism; time-fixed versus time-varying analyses. the tromso study. PLoS One. 2016;11(9):e0163242. doi:10.1371/journal.pone.0163242
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.