Back to Journals » Neuropsychiatric Disease and Treatment » Volume 17
Physical Activity and Motor Performance: A Comparison Between Young Children With and Without Autism Spectrum Disorder
Authors Sung YS, Loh SC ![]() , Lin LY
, Lin LY ![]()
Received 9 October 2021
Accepted for publication 8 December 2021
Published 18 December 2021 Volume 2021:17 Pages 3743—3751
DOI https://doi.org/10.2147/NDT.S343552
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Yu-Ping Ning
Yi-Shan Sung,1,2 Sau Cheong Loh,3 Ling-Yi Lin1,4
1Institute of Allied Health Sciences, College of Medicine, National Cheng Kung University, Tainan, Taiwan; 2Department of Physical Medicine and Rehabilitation, National Taiwan University Hospital Hsin-Chu Branch, Hsin-Chu, Taiwan; 3Department of Educational Psychology and Counseling, Faculty of Education, University of Malaya, Kuala Lumpur, Malaysia; 4Departments of Occupational Therapy, College of Medicine, National Cheng Kung University, Tainan, Taiwan
Correspondence: Ling-Yi Lin
Department of Occupational Therapy, Institute of Allied Health Sciences, College of Medicine, National Cheng Kung University, No. 1 University Road, Tainan, 701, Taiwan
Tel +886-6-235-3535 ext. 5917
Fax +886-6-237-6604
Email [email protected]
Purpose: This study aims to examine the differences in physical activity and motor performance between young children with autism spectrum disorder (ASD) and children with typical development (TD) and to investigate the relationships between the levels of physical activity and motor performance.
Patients and Methods: Twenty-five children with ASD (mean age = 59.3 ± 8.1 months) and 28 children with TD (mean age = 63.1 ± 8.6 months) were recruited. The Actigraph accelerometer, Movement Assessment Battery for Children-second edition, and Assessment of Preschool Children’s Participation were used.
Results: Young children with ASD spent significantly less time in moderate and light physical activity and exhibited more sedentary behavior than did children with TD. Those children with ASD also had greater motor difficulties and engaged less frequently in physical recreation activities compared to their TD peers. Motor performance was significantly correlated with physical activity in all children.
Conclusion: This study highlighted the specificity of the levels of physical activity, motor difficulties, and participation diversity in children with ASD comparing performances on children with TD. Additional research is needed to provide valuable information for early interventions.
Keywords: autism spectrum disorder, physical activity, motor competence, early childhood, sedentary behavior
Introduction
In the past decade, the number of people diagnosed with autism spectrum disorder (ASD) in Taiwan has increased from 8151 to 14,533.1 Individuals with ASD have social interaction and communication challenges, along with restricted or repetitive behaviors, interests, and patterns that are associated with less participation in physical activity and social participation.2,3 Children with ASD have been found to be less physically active during recess compared to those without disabilities. They tend to spend less time engaging in physical activities compared to their peers with typical development (TD).4–6
Physical activity is associated with a better health-related quality of life in children, and the short-term and long-term health benefits last well beyond adolescence.7,8 While regular physical activity helps prevent chronic physical and mental illnesses and improves overall health in young children with TD, sedentary behaviors increase obesity rates.7,9 Physical activity guidelines recommend that young children should engage in at least 180 min per day of physical activity, including 60 min of moderate and vigorous physical activity per day (MVPA).10 A previous study found that 89% of children between 3 and 6 years of age failed to meet the recommended amount of physical activity in Taiwan.11 Physical activity in preschool children has received increasing attention because preschool children are at a critical period in the development of their motor skills and abilities; participating in physical activity might promote the development of these skills in children.12
The patterns of physical activity refer to the temporal distribution of the frequency and amount of body movement over the participating period, including vigorous physical activity (VPA), moderate physical activity (MPA), light physical activity (LPA), and sedentary physical activity (SPA).10,13–15 These patterns are categorized based on the time spent engaging in these different physical activities, which was expressed as total counts divided by measured time per day (counts per minute, CPM).16 Previous research has explored patterns of physical activity in preschool children with ASD.13–15 However, only three studies have used objective measurements to examine their levels of physical activity, and the results have been inconsistent.13–15 Using data logging accelerometers to track the movements of participants over a span of 1 week, two studies found that preschool children with ASD spent the same amount of time engaging in MPA and VPA as their peers with TD did.13,14 MPA levels were lower for preschool children with ASD than for their peers with TD.13 On the other hand, Ketcheson et al15 preschool children, with ASD engaging in higher MPA and VPA when compared to children with TD. While these studies were conducted in the United States and Australia,13,15 no research to date has been done involving young children with ASD in Taiwan. Thus, information regarding the variables that account for the physical activity patterns of Taiwanese young children with ASD is lacking.
Additionally, only a few studies have compared the motor performance (eg, postural control, bilateral coordination, manual dexterity, handwriting, object control, and visuo-motor integration skills) of children with ASD with that of children with TD, and most of them have focused on children between the ages of 5 to 12 years.17–19 These studies have reported that children with ASD have poorer motor performance compared to children with TD.17–19 Other studies20–22 have reported poor motor performance in preschoolers with ASD; however, there were too few practical comparisons has been made with TD children. Relatively little is known about the development gap between children with ASD and TD children. According to previous studies, children with TD are less likely to participate in physical activity if they have poor motor performance.23,24 However, no association was found between the level of physical activity and motor skills in preschool children with ASD.15 This relationship among young children with ASD in Taiwan has not been well investigated.
Activity levels in young children with ASD can be measured using accelerometers, which provide objective information about physical activity. However, information on the type of everyday activity being performed is not provided. Previous studies reported that children with ASD had lower levels of activity participation (eg, play, skill development, active physical recreation, and social activities) than children with TD.25,26 There is a lack of direct evidence correlating activity participation with levels of physical activity among young children with ASD. Thus, investigating the types and diversity of everyday activities in which children with ASD participate would increase our understanding of physical activity practices in this population. The research questions we aimed to answer for this study were as follows: (a) How much time do young children spend on sedentary, light, moderate, and vigorous physical activities? (b) Are there differences in sedentary, low, moderate, and vigorous physical activity levels, motor performance, and levels of activity participation between young children with ASD and with TD? (c) How does physical activity relate to motor performance and participation diversity of the two groups?
Method
Participants
A total of 53 children between 48 and 72 months of age were recruited. Out of the total, 25 children were diagnosed with ASD by a pediatric psychiatrist using the standard criteria for the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). The Childhood Autism Rating Scale, second edition (CARS-2) was used to support diagnosis and for ASD severity. The remaining 28 children with TD were recruited from preschools and kindergartens in Tainan City. The exclusion criteria for both groups were children with attention-deficit hyperactivity disorder or any condition or disease that could affect physical activity and motor performance (eg, cerebral palsy, genetic disorder, chronic disease, heart disease, cancer, severe visual impairment, and acute or chronic injuries). For children with ASD, the primary investigator reviewed their medical records to check whether they had comorbidities. For children with TD, parents reported whether their child had attention-deficit hyperactivity disorder or any developmental delay.
As shown in Table 1, there were no significant differences in age, body mass index (BMI), BMI percentiles, or BMI rankings between both groups. One child in each group was underweight. Five children in the ASD group and seven children in the TD group were overweight or obese. All of the children with ASD scored over 30 on the CARS-2, with a mean score of 35.7; 68.0% were categorized as mild-to-moderate autism and 32% were categorized as severe autism. Their intellectual quotient scores ranged from 49 to 117. There was a significant difference in gender between the two groups. We recruited four female children and 21 male children with ASD. The ratio of males to females was 5.25:1, which is similar to the reported ASD general population sex ratio. All participants did not take medications during the study.
 |
Table 1 Demographic Data of Children with ASD and TD |
Measurements
Childhood Autism Rating Scale, Second Edition (CARS-2)
CARS-2 is used to identify the severity of ASD symptoms.27 The scale contains 15 items relating to people, imitation, emotional response, body use, object use, adaptation to change, visual response, listening response, response and use of the senses (taste, smell, and touch), fear or nervousness, verbal communication, nonverbal communication, activity level, level and consistency of intellectual response, and general impression. The examiner assesses the items using a scale ranging from 1 (age appropriate) to 4 (severely abnormal), with the possibility of assigning half-point scores for each item. A total score below 30 indicates that the examinee is non-autistic, while a score of 30 or greater indicates the presence of autism. This measure is a valid and reliable measure, with a Cronbach’s alpha of 0.93.27 Its sensitivity and specificity values are 0.88 and 0.86, respectively.27
Actigraph Accelerometer
Physical activity levels were measured using an ActiGraph wGT3X-BT (ActiGraph, Pensacola, FL) worn on the participants’ wrist. The accelerometer is a three-dimensional sensor that captures the frequency and amount of body movement with well-established reliability and validity when used in children aged three to five years.16 Cut-off points for VPA, MPA, LPA, and SPA levels were above 4450 cpm, 2120–4449 cpm, 240–2119 cpm, and 0–239 cpm, respectively.16 For comparison purposes, the MPA and VPA levels were combined into MVPA to coincide with the WHO guidelines.10 Participants were asked to wear the accelerometer for 24 h on a weekday under a caregiver’s supervision to prevent the children from taking off the accelerometer on their own. For our study, an epoch length of 10 s was chosen. Non-wear time was defined as 60 min of consecutive zeros and a two-minute tolerance.28 We used the ActiLife software for calibration and data access. The data were then exported into Excel to obtain percentages of the amount of time spent for each physical activity level.
Movement Assessment Battery for Children-Second Edition (MABC-2)
The MABC-2 is a standardized motor assessment used to evaluate and identify motor impairments in children and adolescents between 3 and 16 years of age.29 The performance scale is divided into three age bands. Each band includes eight tasks within three categories: manual dexterity, ball skills, and balance. For this study, a three- to six-year-old age band was employed. The standard and percentile scores were reported in accordance with the examiner’s manual.29 Comparison between groups was used for the standard scores. The interrater reliability for this tool is over 0.75, and the intrarater reliability is 0.70.29
Assessment of Preschool Children’s Participation-Chinese Version (APCP-C)
The ACPC is a parent-completed questionnaire about preschool children’s participation in everyday activities.30 The assessment classifies 45 activities into four categories: play, skill development, active physical recreation, and social activity. For each activity, parents are asked to indicate if their child has participated in the activity (yes/no) in the previous 4 months, and how often this has happened. The frequency questions use a 7-point Likert-type scale ranging from 1 (once over the last 4 months) to 7 (once daily or more). Diversity and intensity scores are calculated for each of the four categories. The diversity score is the percentage of time for which the child has engaged in one of the activities. The intensity score is calculated by dividing the sum of frequency scores across for all items by the total number of times for which the child participated in each of the four categories. APCP-C can be used for children aged two to five years and 11 months. The APCP-C has some modified activities to account for Taiwanese culture. For example, in the “popular community organization” item, a picture book reading group and Chinese literature reading group have been added.30 The internal consistency for the diversity and intensity of participation from children with disabilities is 0.85 and 0.86, respectively.30
Procedure
This study is an exploratory study and was approved by the Research Ethics Committee of NTUH Hisn-Chu branch Institutional interview board (107–062-F). Study procedures were conducted in accordance with the principles of the Declaration of Helsinki. Parents were briefed on the procedure of the study and provided informed consent prior to commencement. Participants were asked for verbal consent to wearing the wrist accelerometer before parent signed consent was solicited. In order to examine the severity of ASD, a CARS-2 score was determined by a trained occupational therapist or psychologist who is well known to participants through direct observation of the child playing with a researcher in the hospital. Participants were instructed to wear accelerometers on their non-dominant wrist for 1 week except when swimming, showering, and bathing. All participants were assessed by registered occupational therapists using the Movement Assessment Battery for Children and Assessment of preschool children’s Participation. The physical activity monitored day were separated by the assessment day. All procedures were completed within 3 weeks.
Statistical Analysis
The analysis was done using the Statistical Package for Social Sciences (SPSS) software (SPSS Inc., Chicago, IL, USA). The alpha level of this study was set as p < 0.05 to indicate statistical significance. Demographic data were reported using descriptive statistics, consisting of mean, standard deviation, percentage, frequency, and median. Test of normality was examined by the Shapiro–Wilk statistic. Differences in levels of physical activity, motor performance, and participation diversity between the two groups were evaluated using independent t tests. We also evaluated effect size with Cohen’s d based on mean and standard deviation for each comparison. The interpretation for size of effect indicating small, moderate, large were 0.2, 0.5, 0.8, respectively.31 Categorical variables, such as gender and BMI ranking, were calculated using Chi-square and Fisher’s exact test. The relationship between physical activity, motor performance, and participation diversity in all the participants and of both groups individually was calculated using a Spearman correlation coefficient. Physical activity in both groups was compared for four different levels (MVPA, MPA, LPA, and SPA) and recorded as a percentage. Due to the lack of vigorous physical activity data collected from children with ASD, we did not compare this level of physical activity between the groups.
Results
Accelerometers
According to the data collected by the accelerometers, children with ASD accumulated an average of 2.0 h/day of MPA, 3.3 h/day of LPA, and 18.7 h/day of SPA on weekdays, respectively. Physical activity level was calculated as a percentage. The Shapiro–Wilk test suggested that the physical activity level was normally distributed. On average, young children with ASD spent most of their daily time on SPA (78.1 ± 11.5%), followed by LPA (13.7 ± 6.3%), and the least amount of daily time on MVPA (8.2 ± 5.7%). None of the children with ASD engaged in VPA (0%). Therefore, for statistical purposes and to align participant comparisons to the WHO guidelines, percentages from MPA (8.2%) and VPA (0%) for the ASD group were combined to create MVPA (8.2%). On the other hand, children with TD accumulated an average of 14.8 h/day of SPA, 5.0 h/day of LPA, 3.8 h/day of MPA, and 0.4 h/day of VPA on weekdays. Children with TD spent a greater portion of time on LPA (21.0 ± 4.5%) and MPA (16.0 ± 5.9%) compared to children with ASD. Children with ASD had significantly lower percentages of MVPA (t(51) = −5.805, p < 0.001), MPA (t(51) = −4.906, p < 0.001), and LPA (t(51) = −4.871, p < 0.001) compared to children with TD (Table 2). Children with ASD also spent more time on SPA than their peers with TD. The effect sizes for the differences in MVPA, MPA, LPA, and SPA were large (Table 2). The effect sizes for VPA difference between two groups were moderate. Seven of the 25 (28%) children with ASD did not meet the WHO recommended time for daily MVPA. For children with TD, all children except one met the recommended guideline.
 |
Table 2 Comparison of Physical Activity Level and Motor Performance Between ASD and TD Groups |
Comparison of the Motor Performance of Both Groups
The Shapiro–Wilk test suggested that the aiming and catching was not normally distributed. Manual dexterity and balance scores were found to be normally distributed. Most children with ASD (76.0%) experienced overall motor difficulties. Participants showed motor difficulties in aiming and catching (72.0%), manual dexterity (60.0%), and balance (56.0%). The mean of the total score and subtest standard scores on the MABC-2 for children with ASD was 53.6, 5.8, 5.4, and 6.7, respectively. Contrary to the ASD group, only one child (3.6%) in the TD group had overall motor difficulties. Children with TD showed motor difficulties in manual dexterity (10.7%) and in aiming and catching (10.7%), but none had balance problems. The mean for the total score and subtest standard scores on the MABC-2 for children with TD was 85.0, 10.4, 10.1, and 13.6, respectively. Significant differences in manual dexterity (t(51) = −5.206, p < 0.001), aiming and catching (t(51) = −6.811, p < 0.001), and balance (t(51) = −9.77, p < 0.001) were observed between the two groups. Children with ASD showed greater motor difficulties than children with TD (t(51) = −8.104, p < 0.001). The effect sizes of all motor performance difference between children with ASD and children with TD were large.
Concerned about the sex distribution for the ASD group, we generated a linear model using sex as a controlled covariant, and the differences in physical activity and motor performance still remained significant between the two groups. Additionally, the significance of differences in physical activity and motor performance between groups persisted after controlling for age.
Comparing the Participation Between Both Groups Using the APCP-C
Scores on skill development activities, physical recreation activities, and social activities were found to be normally distributed. Children with ASD participated in an average of 29.4 (SD = 5.6) of the 45 APCP-C activities (65.3%), with individual children performing between 21 (46.7%) and 39 (86.7%) activities. On average, the children participated in these activities once a week. The children had an average participation diversity of 65.3 (SD = 12.5), with the highest score for the skill development activities (73.3 ± 15.5), followed by the play activities (71.1 ± 18.9), and the physical recreation activities (61.2 ± 13.6). The lowest score was in the social activities (53.4 ± 17.6). Children with ASD engaged frequently in play and skill development activities. However, they had significantly lower scores on participation diversity for all four APCP areas compared with those in TD children (Table 2). The effect sizes for participation diversity in all APCP area were ranged from moderate to large scale.
Correlation Analysis
A Spearman correlation coefficient was used to examine the relationship between physical activity, motor performance, and participation diversity among all participants. As shown in Table 3, motor performance was significantly correlated with a higher MVPA and LPA, and a lower SPA level in all children. This indicates that children with better motor performance participated more frequently in light to vigorous physical activities. However, no significant correlations between physical activity and motor performance were observed in either group. Regarding participation diversity, MVPA and SPA were correlated with all four areas of participation diversity, indicating that greater participation diversity was associated with higher MVPA and lower SPA levels when the correlation ran in TD group separately. However, there was no significant correlation between physical activity levels and participation diversity in children with ASD. For children with ASD, the ASD severity was significantly correlated with manual dexterity (ρ= −0.466, p = 0.025) and total scores (ρ= −0.408, p = 0.043) of the MABC-2 as well as the total activity participation (ρ= −0.402, p = 0.047); however, no significant correlation between the ASD severity and physical activity levels was observed.
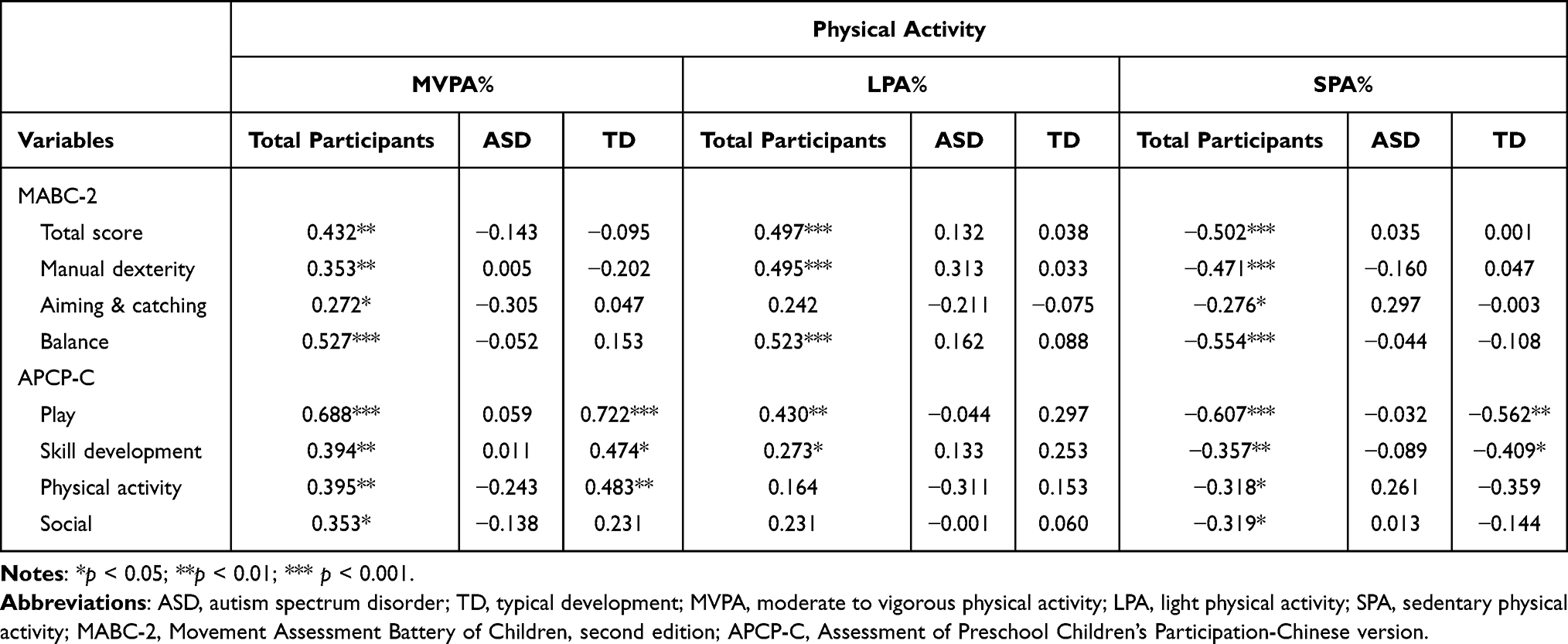 |
Table 3 Correlations Between Physical Activity, Motor Performance, and Activity Diversity |
Discussion
This study was the first to explore physical activity in young children with ASD in Taiwan using an objective measurement. Our study yielded four main findings: (1) young children with ASD spent less time in moderate and vigorous physical activity and light physical activity, and sedentary physical activity than did children with TD, (2) children with ASD had greater motor difficulties compared to their peers with TD, (3) children with ASD engaged less frequently in activities than did children with TD, and (4) all young children who engaged more frequently in moderate and vigorous physical activity had better motor performance and greater participation diversity.
When compared to the results of previous studies involving young children with ASD, our results are consistent with those of Bandini et al,13 who reported that children with ASD engaged in less MPA on weekdays compared with children with TD, after adjusting for sex and age. However, our findings differ from those of Ketcheson et al,15 who reported that young children with ASD spent more time on MVPA and LPA and less time on SPA behaviors when compared to their peers with TD. It may be attributed to the age difference of the participants. Participants in the study of Ketcheson et al15 were between 2 and 5 years of age, significantly younger than the participants in our study (4–6 years). Ketcheson et al15 inferred that this finding attributed to the contribution of comorbidities such as ADHD and anxiety. However, little research has established a link between comorbidities and levels of physical activity in this population. The impact of comorbidities on levels of physical activity in children with ASD should be studied further in future research. Moreover, Thomas et al14 and Bandini et al13 reported similar time spent on MVPA with no significant differences between children with ASD and those with TD, even after adjusting for age and sex. It appears that there were contrary results in our study, indicating that young children with ASD spent less time on MVPA when compared to children with TD after controlling for age and sex. According to the WHO guidelines,10 young children should spend at least three hours daily engaging in physical activity, with at least 60 min of MVPA per day. However, young children with ASD in our study did not engage in VPA. Although some of the children with ASD engaged in sufficient physical activity according to WHO guidelines, they were not sufficiently active based on APAC-C. On the contrary, children with TD in our study engaged in sufficient physical activity, only one participant in this group did not meet the recommended amount. Regarding the ASD severity, our study was in line with the study of Bandini et al13 that there was no significant relationship between autism status and reported time spent on physical activities. This highlights those other potential variables which might be related to levels of physical activity that can be investigated in the future. Notably, in this study, we found significant group differences for all types of physical activities, indicating that young children with ASD spent less time engaging in physical activities than did children with TD. The findings of this study extend the results of earlier studies which showed lower levels of physical activity from school-aged children and adolescents to young children with ASD.4,6,32
The results are consistent with those of other studies in which young children with ASD exhibited significantly greater motor difficulties in comparison to their peers with TD.17,18,20,33–35 Further, the motor performance of children between 3 and 16 years of age differed significantly between both groups, which is consistent with the findings in previous studies that used the MABC‐2.17,18,35 Our study showed that children with ASD had a significant lower score not only in total performance, but also in manual dexterity, aiming and catching, and balance subscales. A possible explanation for this might be that these motor tasks, especially aiming and catching, involve the child’s ability to coordinate visual information and imitate others’ actions.17,36 Deficits in visual motor integration and imitation in children with ASD are a common occurrence.36,37 Both Forti et al33 and Roley et al38 reported that a limited motor planning capacity could impact the performance of motor integration in children with ASD.
Consistent with Bandini et al,13 children with ASD participated in fewer types of activities than children with TD did. Must et al39 observed that children with ASD between 3 and 11 years old spent more time on sedentary activities (such as screen-based activities) than children with TD did. Specifically, children with ASD engaged more frequently in play and skill development activities categorized as LPA or SPA. Such activities include playing with toys, watching TV or videos, creating a craft project, drawing or coloring, listening to stories, doing puzzles, and taking music lessons. Furthermore, the study indicated that children with ASD who spent more hours per day on screen-based activities excluded other recreational activities, such as physical activities or exercise.39 In our study, children with ASD participated in fewer physical recreation activities and had poor motor performance. Poor motor performance deters children with ASD from participating in MVPA. Thus, designing motor skills interventions to increase MVPA levels may be beneficial for young children with ASD.
No significant correlations between physical activity and motor performance were observed in either children with ASD or children with TD. This finding supports the results from a previous study where no association was observed because the participants with ASD were very young and at a transitional stage in their physical development.15 Another possible explanation for the lack of association may be attributed to highly skewed data in each group. If all participants are considered, the results reinforce the theory that motor performance in young children is related to higher levels of physical activity. Williams et al23 and Wrotniak et al24 found an association between motor proficiency and MVPA in young children, and the results of the current study lend support for this association. However, because of its potential to provide valuable information for early interventions, future research is warranted to confirm this relationship in young children with ASD.
Limitations of this study included only using accelerometers for a weekday. Future study should measure physical activity for longer time span. Other limitations of this study included a small sample size and a skewed sex ratio in the ASD group, which could limit the generalizability of these results. Future research should aim to recruit participants with a balanced sex ratio from a wider community sample. In addition, since no accelerometer cut-offs have been established for children with ASD, we used the cut-offs based on young children with TD to analyze the physical activity levels. Furthermore, we did not consider the effects of cognitive ability or other developmental concerns on motor performance and participation diversity. A description of ASD functioning profile was lacking as well. Cognitive and language abilities were estimated for all participants. Future research will be warranted to obtain related characteristics for both children with ASD and TD. Nevertheless, despite these limitations, the use of accelerometers to measure young children’s physical activity levels was a strength of this study.
Conclusion
This study is, to our knowledge, the first to use objective measurements to examine physical activity among young children with ASD in Taiwan. Findings showed that young children with ASD spent less time engaging in all levels of physical activity when compared to children with TD. This study highlights the specificity of motor difficulty and activity participation diversity in children with ASD by comparing their performance with that of children with TD. This suggests the need for occupational therapy interventions that target the motor skills of young children with ASD. To link the findings to training and interventions on motor difficulties among young children with ASD, further evidence-based research will be necessary. Future studies should examine the associated factors of physical activity, such as sex, age, developmental abilities, and activity participation patterns in young children with ASD.
Acknowledgment
The authors wish to thank the case manager, the occupational therapists, the psychologists in early intervention center of National Taiwan University Hospital Hsin-Chu Branch, pediatric rehabilitation clinicians, and all the parents who participated in this study. This research was supported in part by Higher Education Sprout Project, Ministry of Education to the Headquarters of University Advancement at National Cheng Kung University (NCKU). This work was supported by the SATU Joint Research Grant Scheme between the National Cheng Kung University and the Universiti Malaya, Malaysia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ministry of Health and Welfare. Statistics of general health and welfare; 2018. Available from: https://www.mohw.gov.tw/lp-4614-2.html.
2. Lawson LM, Foster L. Sensory patterns, obesity, and physical activity participation of children with autism spectrum disorder. Am J Occup Ther. 2016;70(5):7005180070p1–7005180070p8. doi:10.5014/ajot.2016.021535
3. Pan CY, Frey GC. Physical activity patterns in youth with autism spectrum disorders. J Autism Dev Disord. 2006;36(5):597–606. doi:10.1007/s10803-006-0101-6
4. Pan CY. Objectively measured physical activity between children with autism spectrum disorders and children without disabilities during inclusive recess settings in Taiwan. J Autism Dev Disord. 2008;38(7):1292–1301. doi:10.1007/s10803-007-0518-6
5. Stanish HI, Curtin C, Must A, Phillips S, Maslin M, Bandini LG. Physical activity levels, frequency, and type among adolescents with and without autism spectrum disorder. J Autism Dev Disord. 2017;47(3):785–794. doi:10.1007/s10803-016-3001-4
6. Tyler K, MacDonald M, Menear K. Physical activity and physical fitness of school-aged children and youth with autism spectrum disorders. Autism Res Treat. 2014;2014:312163. doi:10.1155/2014/312163
7. Timmons BW, Leblanc AG, Carson V, et al. Systematic review of physical activity and health in the early years (aged 0–4 years). Appl Physiol Nutr Metab. 2012;37(4):773–792. doi:10.1139/h2012-070
8. Wu XY, Han LH, Zhang JH, Luo S, Hu JW, Sun K. The influence of physical activity, sedentary behavior on health-related quality of life among the general population of children and adolescents: a systematic review. PLoS One. 2017;12(11):e0187668. doi:10.1371/journal.pone.0187668
9. Ziviani J, Macdonald D, Jenkins D, Rodger S, Batch J, Cerin E. Physical activity of young children. OTJR. 2006;26(1):4–14. doi:10.1177/153944920602600102
10. World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World. World Health Organization; 2019.
11. Lin LY, Cherng RJ, Chen YJ. Relationship between time use in physical activity and gross motor performance of preschool children. Aust Occup Ther J. 2017;64(1):49–57. doi:10.1111/1440-1630.12318
12. Figueroa R, An R. Motor skill competence and physical activity in preschoolers: a review. Matern Child Health J. 2017;21(1):136–146. doi:10.1007/s10995-016-2102-1
13. Bandini LG, Gleason J, Curtin C, et al. Comparison of physical activity between children with autism spectrum disorders and typically developing children. Autism. 2013;17(1):44–54. doi:10.1177/1362361312437416
14. Thomas S, Hinkley T, Barnett LM, May T, Rinehart N. Young children with ASD participate in the same level of physical activity as children without ASD: implications for early intervention to maintain good health. J Autism Dev Disord. 2019;49(8):3278–3289. doi:10.1007/s10803-019-04026-9
15. Ketcheson L, Hauck JL, Ulrich D. The levels of physical activity and motor skills in young children with and without autism spectrum disorder, aged 2–5 years. Autism. 2018;22(4):414–423. doi:10.1177/1362361316683889
16. Butte NF, Wong WW, Lee JS, Adolph AL, Puyau MR, Zakeri IF. Prediction of energy expenditure and physical activity in preschoolers. Med Sci Sports Exerc. 2014;46(6):1216–1226. doi:10.1249/MSS.0000000000000209
17. Craig F, Lorenzo A, Lucarelli E, Russo L, Fanizza I, Trabacca A. Motor competency and social communication skills in preschool children with autism spectrum disorder. Autism Res. 2018;11(6):893–902. doi:10.1002/aur.1939
18. Liu T, Breslin CM. Fine and gross motor performance of the MABC-2 by children with autism spectrum disorder and typically developing children. Res Autism Spectr Disord. 2013;7(10):1244–1249. doi:10.1016/j.rasd.2013.07.002
19. Kaur M, Srinivasan SM, Anjana NB. Comparing motor performance, praxis, coordination, and interpersonal synchrony between children with and without Autism Spectrum Disorder (ASD). Res Dev Disabil. 2018;72:79–95. doi:10.1016/j.ridd.2017.10.025
20. Jasmin E, Couture M, McKinley P, Reid G, Fombonne E, Gisel E. Sensori-motor and daily living skills of preschool children with autism spectrum disorders. J Autism Dev Disord. 2009;39(2):231–241. doi:10.1007/s10803-008-0617-z
21. Landa R, Garrett-Mayer E. Development in infants with autism spectrum disorders: a prospective study. J Child Psychol Psychiatry. 2006;47(6):629–638. doi:10.1111/j.1469-7610.2006.01531.x
22. Lloyd M, MacDonald M, Lord C. Motor skills of toddlers with autism spectrum disorders. Autism. 2013;17(2):133–146. doi:10.1177/1362361311402230
23. Williams HG, Pfeiffer KA, O’Neill JR, et al. Motor skill performance and physical activity in preschool children. Obesity. 2008;16(6):1421–1426. doi:10.1038/oby.2008.214
24. Wrotniak BH, Epstein LH, Dorn JM, Jones KE, Kondilis VA. The relationship between motor proficiency and physical activity in children. Pediatrics. 2006;118(6):e1758–e1765. doi:10.1542/peds.2006-0742
25. Lin LY. Activity participation and sensory processing patterns of preschool-age children with autism spectrum disorder. Am J Occup Ther. 2020;74(6):7406345010p1–7406345010p7. doi:10.5014/ajot.2020.039297
26. LaVesser P, Berg C. Participation patterns in preschool children with an autism spectrum disorder. OTJR. 2011;31(1):33–39. doi:10.3928/15394492-20100823-01
27. Schopler E, Van Bourgondien ME, Wellman GJ, Love SR. Childhood Autism Rating Scale.
28. Troiano RP, Berrigan D, Dodd KW, Mâsse LC, Tilert T, McDowell M. Physical activity in the United States measured by accelerometer. Med Sci Sports Exerc. 2008;40(1):181–188. doi:10.1249/mss.0b013e31815a51b3
29. Henderson SE, Sugden DA, Barnett AL. Movement Assessment Battery for Children.
30. Kang LJ, Hwang AW, Palisano RJ, King GA, Chiarello LA, Chen CL. Validation of the Chinese version of the assessment of preschool children’s participation for children with physical disabilities. Develop Neurorehab. 2017;20(5):266–273. doi:10.3109/17518423.2016.1158746
31. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
32. Memari AH, Ghaheri B, Ziaee V, Kordi R, Hafizi S, Moshayedi P. Physical activity in children and adolescents with autism assessed by triaxial accelerometry. Pediatr Obes. 2013;8(2):150–158. doi:10.1111/j.2047-6310.2012.00101.x
33. Forti S, Valli A, Perego P, Nobile M, Crippa A, Molteni M. Motor planning and control in autism. A kinematic analysis of preschool children. Res Autism Spectr Disord. 2011;5(2):834–842. doi:10.1016/j.rasd.2010.09.013
34. Fournier KA, Hass CJ, Naik SK, Lodha N, Cauraugh JH. Motor coordination in autism spectrum disorders: a synthesis and meta-analysis. J Autism Dev Disord. 2010;40(10):1227–1240. doi:10.1007/s10803-010-0981-3
35. Siaperas P, Ring HA, McAllister CJ, et al. Atypical movement performance and sensory integration in Asperger’s syndrome. J Autism Dev Disord. 2012;42(5):718–725. doi:10.1007/s10803-011-1301-2
36. Ament K, Mejia A, Buhlman R, et al. Evidence for specificity of motor impairments in catching and balance in children with autism. J Autism Dev Disord. 2015;45(3):742–751. doi:10.1007/s10803-014-2229-0
37. Fuentes CT, Bastian AJ. ‘Motor cognition’ - what is it and is the cerebellum involved? Cerebellum. 2007;6(3):232–236. doi:10.1080/14734220701329268
38. Roley SS, Mailloux Z, Parham LD, Schaaf RC, Lane CJ, Cermak S. Sensory integration and praxis patterns in children with autism. Am J Occup Ther. 2015;69(1):6901220010. doi:10.5014/ajot.2015.012476
39. Must A, Phillips SM, Curtin C, et al. Comparison of sedentary behaviors between children with autism spectrum disorders and typically developing children. Autism. 2014;18(4):376–384. doi:10.1177/1362361313479039
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.