")
Back to Journals » Open Access Journal of Contraception » Volume 14
Phenomenology of Induced Abortion in Northern Uganda Among HIV-Positive Women Following an Unintended Pregnancy
Authors Kabunga A , Acanga A , Akello Abal J , Kambugu Nabasirye C , Namata H, Mwesigwa D, Grace Auma A, Kigongo E , Udho S
Received 11 February 2023
Accepted for publication 18 April 2023
Published 20 April 2023 Volume 2023:14 Pages 73—82
DOI https://doi.org/10.2147/OAJC.S407547
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Igal Wolman
Amir Kabunga,1 Alfred Acanga,2 Judith Akello Abal,3 Caroline Kambugu Nabasirye,4 Halimah Namata,5 David Mwesigwa,2 Anna Grace Auma,4 Eustes Kigongo,6 Samson Udho4
1Department of Psychiatry, Lira University, Lira, Uganda; 2Department of Public Administration and Management, Lira University, Lira, Uganda; 3Department of Commerce and Business Management, Lira University, Lira, Uganda; 4Department of Midwifery, Lira University, Lira, Uganda; 5Department of Mental Health, Makerere University, Lira, Uganda; 6Department of Infectious Diseases, Lira University, Lira, Uganda
Correspondence: Amir Kabunga, Department of Psychiatry, Lira University, Lira, Uganda, Tel +256777929576, Email [email protected]
Background: More than half of pregnancies in Uganda are unintended, and nearly a third of these end in abortion. However, little research has focused on women living with HIV’s subjective experiences following induced abortion. We explored how women living with HIV subjectively experience induced abortions in health facilities in Lira District, Uganda.
Materials and Methods: This was a descriptive-phenomenological study between October and November 2022. The study was conducted among women of reproductive age (15– 49 years) who were HIV positive and had undergone induced abortion following an unintended pregnancy. Purposive sampling was used to sample 30 participants who could speak to the research aims and have experience with the phenomenon under scrutiny. The principle of information power was used to estimate the sample size. We conducted face-to-face, in-depth interviews to collect data. Data were presented as direct quotes while providing a contextual understanding of the lived experiences of the study participants.
Results: The results showed that the major causes of induced abortion were financial constraints, concern for the unborn babies, unplanned pregnancy, and complex relationships. Regarding induced abortion-related experiences, three themes emerged: loss of family support, internalized and perceived stigma, and feelings of guilt and regret.
Conclusion: This study highlights the lived experiences of women living with HIV following an induced abortion. The study shows that women living with HIV had induced abortions due to numerous reasons, including financial concerns, complicated relationships, and a fear of infecting their unborn babies. However, after induced abortion, the women living with HIV faced several challenges like loss of family support, stigma, and feelings of guilt and regret. Based on HIV-infected women who underwent induced abortion and an unexpected pregnancy, they may need mental health services to reduce the stigma associated with induced abortion.
Keywords: abortion, lived experiences, unintended pregnancy
Background
Unintended pregnancy and abortion are intricately linked.1 In 2015–19, 61% of unintended pregnancies ended in abortion globally, while 37%, 72%, and 47% of unintended pregnancies in sub-Saharan Africa, Central, and South Asia, and Europe and Northern America, ended in abortion, respectively.1 This pattern underscores the restrictive abortion environment and the poor access to safe and quality comprehensive abortion care in sub-Saharan African countries like Uganda.2 More than half of pregnancies in Uganda are unintended, and nearly a third of these end in abortion.3
Women living with HIV are particularly at risk for unintended pregnancy and unsafe abortion.4 Studies show that women living with HIV have unwanted pregnancies due to domestic violence, being single, unstable relationships, multiple partners, and having low economic resources to take care of a child.5 Studies further reveal that there are higher chances of performing an abortion post-HIV diagnosis.2 In Uganda, abortion is permitted under some circumstances, but the relevant laws and policies are unclear and are often interpreted inconsistently, making it difficult for both women to access safe and quality abortion services, thus, unsafe abortion.3 According to statistics, there are 336 maternal fatalities for every 100,000 live births, and there are an estimated 16 to 18 maternal deaths every day, with 4–6 of those deaths being directly related to unsafe abortion.6 This highlights the need for interventions to reduce unintended pregnancies and unsafe abortions.3
Although abortion is illegal in Uganda, post-abortion care (PAC) was adopted as one of the intervention packages to reduce the risks of abortion complications.2 PAC consists of emergency treatment of incomplete abortion and its complications, contraceptive counselling and provision, and evaluation and treatment of sexually transmitted diseases.7 Most of the clients seeking post-abortion evacuation are often victims of incomplete and unsafe abortion performed by unqualified personnel. However, we do not know how these women experience PAC services offered in public healthcare facilities. Subsequently, there is a dearth of literature on how they cope with their experience of care.
This study was anchored on social constructionism theory. According to this theory, things like laws and practices that are typically taken for granted are actually only “perspectives” that can be questioned. They might be seen as institutionalized viewpoints tailored to specific social groups. This perspective contends that social issues should not be viewed as objective situations, but rather as a component of broader social processes.8 Discourses are described as various, intrinsically positioned representations of social existence in critical discourse analysis.8 Differently positioned actors have varied perspectives on and representations of social life. These discourses are sequential and engage in interaction. Dominance, or understanding that some ways of producing assertions are dominant and others are marginal, is one component of this arrangement.9 It is possible to understand current social climates and various power relations by examining the presence or absence of particular viewpoints, perspectives, and wordings in a book.9
This study starts with a social issue: the many unintended pregnancies among HIV-positive women and how they frequently result in unsafe abortions. In order to contribute to a deeper understanding of abortion related experience in the Ugandan setting, we aimed to explore the experiences of unintended pregnancy and induced abortion among HIV-positive clients in Lira District, northern Uganda. The results of this study will strengthen the debate to liberalize and improve comprehensive abortion care services in countries with restrictive abortion policies.
Materials and Methods
Study Setting
The study was conducted in Lira District, Lango Sub-region, northern Uganda. Lira District has two counties, six sub-counties, 49 parishes, and 510 villages. The 2020 population of the district stood at 235,37910 which is served by seven public health facilities with the capacity to offer post-abortion care services.11 Lira District was chosen because of the high burden of unintended pregnancy and induced abortion.12
Research Design
We conducted a descriptive phenomenological study between October and November 2022. In using descriptive phenomenology, we aimed to describe the universal essence of an experience as lived by HIV positive women who had an induced abortion following an unintended pregnancy which represents accurately the true nature of the phenomena.13
Study Participants and Sample Size Estimation
The study was conducted among women of reproductive age (15–49 years) who were HIV positive and had undergone induced abortion following an unintended pregnancy. Information redundancy was used to establish the sample size. To ensure saturation, data were examined for the presence of codes or categories and the need for more interviews in a preliminary manner at the conclusion of each interview day. Authors made sure that interviews were no longer producing fresh data, as new interviews frequently repeat previously gathered information.
Sampling Criteria
Purposive sampling was used to sample 30 participants who could speak to the research aims and have experience with the phenomenon under scrutiny.14
Data Collection Instruments
We conducted face-to-face, in-depth interviews using interview guides with open-ended questions. To ensure the suitability of the interview guide, it was designed based on a literature review and expert consultation. The interview guide was pilot-tested on five participants who were excluded from the study, and appropriate adjustments were made to the guide. The interviews were conducted in both English and the local dialect, by research assistants who are social scientists with training in qualitative study and interview methods. The interviews were conducted in the participants’ homes in a setting of their choice that would enhance privacy and confidentiality. All interviews were audio-recorded with the participants’ consent. Nonverbal cues, like participants’ facial expressions and emotional shifts, were noticed during the interview and noted in the field notes. The interviews lasted, on average, 45 minutes. Participants who, at the time of data collection, were emotionally unstable and had an unstable health status were excluded from the study.
Procedure
The study participants were identified from the postnatal clinics of Amach Health Center IV, Ober Health Center IV, and Ogur Health Center IV, Lira District. The files of clients who had sought post-abortion care services from these facilities were retrieved, and those who were HIV-positive were identified. The prospective participants were contacted by phone, and an appointment was made to meet with them in the community. Upon meeting the prospective participants, we screened for participants who met the inclusion criteria (induced abortion following an unintended pregnancy). We explained the purpose, risks, and benefits of participating in our study, and those who consented to participate in the study were recruited.
Data Analysis
The data were transcribed verbatim into Microsoft Word within 24 hours after the interview by the research assistants, who are trained in qualitative data transcription. The texts were annotated with field notes incorporating participant non-verbal cues to aid in data interpretation. We analyzed the data using inductive thematic analysis.15 Data coding was done by two independent authors. Themes were generated based on the frequency of codes and the sufficiency of data extracts to back up the codes. Discrepancies in codes and themes were resolved through group discussions involving the authors. Data were presented as direct quotes while providing a contextual understanding of the lived experiences of the study participants.
To ensure the trustworthiness of our research, we used research assistants who are social scientists with training in qualitative study and interview methods. Two researchers conducted independent analyses of data from various sources, including field notes and audio recordings. To ensure that the subjects were at the center of the data analysis and interpretation, the newly emerging themes were constantly compared to the original transcribed text, and the authors regularly met for debriefings. To improve the dependability and accuracy of the outcomes, the data analysis results were reviewed and debated until an agreement was reached. In order to prove conformability, the investigators used previous bias-reducing personal expectations and experiences as well as the words of participants as recorded in the interview transcripts. Finally, we have kept all audit trails from data collection to analysis to ensure that the processes of data collection and analysis could be linked back to the initial interviews.
Ethical Approval
The study followed the procedures recommended by the Helsinki Declaration. The present study was approved for publication by the Gulu University Research and Ethics Committee (GUREC-2022-305). Written informed consent was required for the recruitment of study participants, and confidentiality was upheld throughout the entirety of the research procedure process. Participants had the option to leave the study at any moment without incurring any penalties; the study was anonymous. Distressed participants during data collection were referred to a standby counselor for counseling services during the time of data collection. The participants’ informed consent included the publication of anonymized responses.
Results
Characteristics of the Participants
A total of 30 participants took part in the study, with a mean age of 25.93 (6.85) years. Half (15/30) of the study participants were married, while the majority (18/30) had no formal education. The summary statistics of the characteristics of the study participants are described in Table 1.
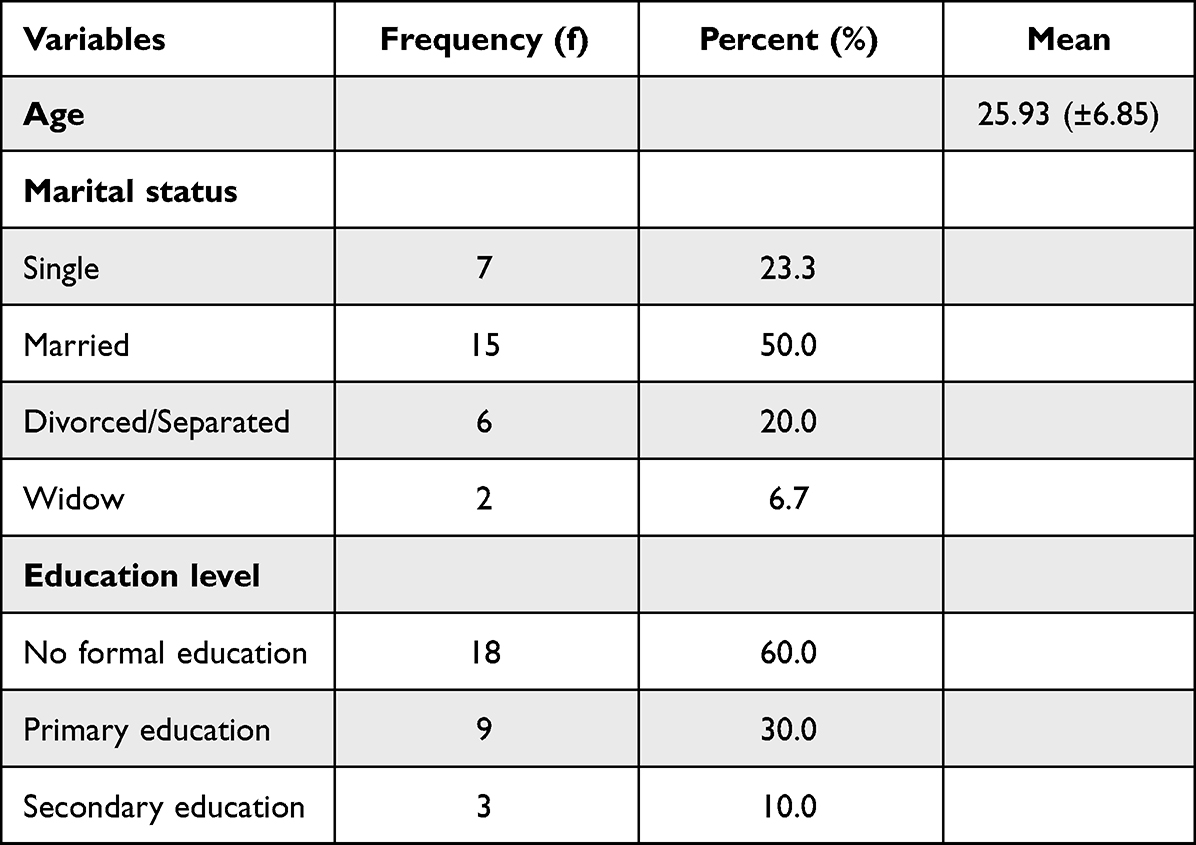 |
Table 1 Characteristics of the Study Participants |
Lived Experiences of Induced Abortion Following Unintended Pregnancy Among HIV-Positive Clients
We explored the experiences of women living with HIV who had induced abortions following unintended pregnancies. We identified 21 unique codes, 15 categories, and 3 themes. The coding of key themes is presented in Table 2.
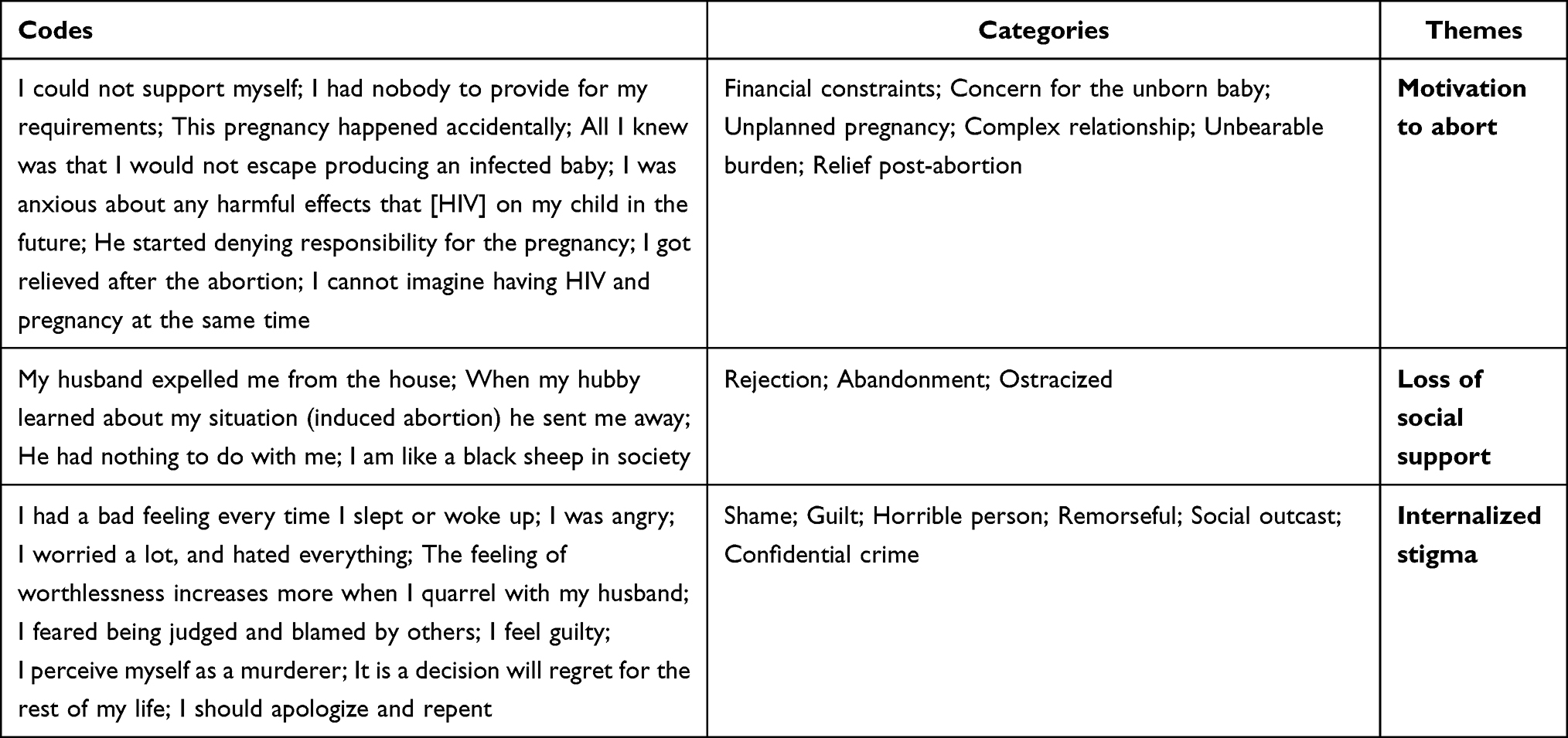 |
Table 2 Codes, Categories, and Themes of Lived Experiences of Induced Abortion |
Themes
Three major themes emerged: perspectives on the causes of induced abortion, loss of family support, and internalized and perceived stigma.
Perspectives That Led to Induced Abortion
We further probed the perspective that led the participants to have an induced abortion, and the findings yielded three sub-themes. These were financial constraints, concern for the unborn babies, unplanned pregnancy, and complex relationships.
Financial Constraints
The participants gave economic issues a great deal of thought. The majority of them acknowledged considering the financial ramifications of their unplanned pregnancies before deciding to have them terminated. This was made worse by the husband’s or boyfriend’s lack of assistance.
I can’t imagine having HIV and pregnancy at the same time, the situation can be dire and stressful as both present with crazy demands that cannot be easily met; demand for a certain type of food, once on ART, one needs a lot of rest just like the situation with pregnancy amidst the demand to work hard in meeting the ever-increasing cost of living. I had no way of surviving because the man denied having any ownership of my pregnancy. (P021)
I lacked financial assistance, ………. But my efforts to find a job were fruitless. Thus, I decided to get an abortion. Moreover, the man who caused my pregnancy did not have a job, and I did not even bother to inform him of it. I decided to get an abortion. (P013)
I considered what I would do if I gave birth. I was challenged by the man, who repeatedly denied the pregnancy, so I decided to induce the abortion. (P025)
Our socioeconomic situation was not good, which had a significant impact on my decision to induce that abortion. However, I had never intended to have an abortion in my life, but I had no other choice. (P004)
Concern About Their Babies
The participants were also concerned about their own welfare as well as the welfare of their infants. They indicated in their narratives a fear of transmitting HIV to their unborn children.
All I knew was that I would not escape producing an infected baby, my adherence was poor, the infection would have been either during pregnancy or breastfeeding since I would not afford early weaning of the baby, and these stressed me up. (P005)
My moments were full of worries about the likeliness of being weaker as the processes of giving birth weaken HIV-infected mothers, the likeliness of dying as a result of childbirth given my already compromised immunity. I also fear being nonproductive when pregnancy reduces further my body’s immunity. I was unhappy and anxious because I worried about any harmful effects that [HIV] would have on my child in the future. My child did not deserve this; thus, I could not make the error of transmitting HIV to them. I chose to end the pregnancy. (P010)
I felt mixed emotions about my pregnancy. I learn about the pregnancy and am very happy because of the news. But immediately I remembered that I had the disease and that there is a chance that I would pass it on to my unborn kid. I could take it and I aborted. (P020)
I was aware that there was a little chance, but because of all the rhetoric about HIV not being contagious and other things, I don’t consider it for myself. All I knew was that I wanted a healthy birth for my child. Nevertheless, I was concerned that I might become ill and that my child would not live. Who would take care of my baby? Termination of the pregnancy remained the only option. (P008)
Complex Relationship
We looked into the causes of induced abortion. According to the study findings, complicated relationships were among the major causes leading to induced abortions. The following excerpts can explain this phenomenon;
When I conceived my husband was loving, providing for me. But later he started denying responsibility for the pregnancy. Got another girlfriend. This angered me and accordingly, I decided to abort. I was pregnant by this man, but I wasn’t even somewhat in love with him. (P025)
Back then, the man who inherited me and was responsible for the pregnancy was my best friend, we loved each other so much but after impregnating me (sigh), refused to support me socially, physically, and economically and to make matters worse, he denied being responsible for the pregnancy yet I also have my other orphaned children to look after. I was left with no option but to abort. (P006)
When I conceived, domestic violence became the order of the day. Blame game as to who wanted and who didn’t want the unintended pregnancy ensured thereafter. He was particularly annoying, constantly reminding me of who married the other. I had no interest in carrying that pregnancy. (P017)
I told my husband that I was pregnant. His response was very clear that he did not desire a child at that time. My boyfriend’s behaviour angered me, so I chose to have an abortion. (P011)
He (my boyfriend) berated me and made fun of me almost every day and with great penitence, I chose abortion. I believe that a child deserves the affection of both parents. I did not anticipate my unborn child living such a life. (P005)
The aforementioned information suggests that the choice to terminate the pregnancy was motivated by rage and a desire to exact revenge on the cheating husband or boyfriend.
Loss of Family Support
The participants claimed that sharing their status with family members had a detrimental impact on their family relationships. Eight participants reported that their families cut off their relationship with them after an induced abortion. Women who had induced abortions immediately felt abandoned by their families and as though they did not belong anywhere, as exemplified by the following excerpts:
My husband expelled me from the house after learning about my induced abortion and many thought I was a spoiled woman. (P021)
When my hubby learned about my situation (induced abortion), he sent me away………. No one wants to associate with me like they used to. My father frequently consumes alcohol and criticizes me in all of those establishments. (P007)
I returned home and I did not want anyone to know. Sadly, they were later informed. They told me you have been lying to us all the time; you are on your own, you are a shame to this family. I won’t soon forget that. (P016)
When I told my husband about the abortion, he claimed he want nothing to do with me. I considered telling my parents, but I knew they wouldn’t be happy due to their religious and cultural beliefs, so I made the decision to leave the house …………. (P005)
Internalized and Perceived Stigma
Participants reported feeling both internalized and perceived stigma after having an induced abortion, which was a recurring theme. Participants weighed the emotional relief from an undesired pregnancy vs the sentiments of guilt and sin associated with induced abortion because of internalized stigma and shame. Even among participants who had an abortion, some continued to have a negative opinion of the procedure or refused to take responsibility for their choice, showing internalized stigma.
………………… They talk about it so much in church the few times I’ve been there following the abortion! I no longer desire to attend church. Just from here, I’m praying. (P017)
Yes, I had an induced abortion and at first it was a relief. But currently, am like a black sheep in society, am a bad example to the rest of the women in my community. (P013)
I feel discriminated against and hear that men are warned against marrying me because I had an abortion…………. that I may continue with abortion even in marriage. They speak evil things about me. Even men living with HIV hesitate to marry me because they think I might abort their babies since I have done it before. (P003)
Many women spoke of wanting to keep their abortion experience a secret to escape stigma and shame. They also acknowledged how secrecy increased social isolation and the risk of health problems both during and after an abortion. Stigma and secrecy occasionally encouraged unsafe or self-inflicted abortions. Additionally, concealing an abortion raised health risks associated with receiving care from inexperienced professionals who frequently worked in clandestine settings at subpar facilities or withheld information from medical professionals.
One of my main concerns was whether to disclose, to whom and when. I feared being judged and blamed by others if I disclosed my condition. I don’t want anyone to be aware of my abortion situation…………. I don’t want anyone, not even a doctor, ……… tell me, to know what? What people will do for me? (P009)
If people learn that I had an abortion, they will judge me. I initially didn’t want to inform my husband, but I had to because perhaps he would eventually get to know it. Nobody else is aware of my condition but him, and he has agreed not to let anyone else know. (P027)
I do not want anyone to know that I had an abortion since they might not be able to help me and might blame me instead. Even when I was over-bleeding, I feared to visit the nearby clinic for help as I knew the nurses would tell people about my condition. (P024)
I made the decision right away that no one in my community should be aware that I had an abortion, and that the information should not be publicized. As a result, I removed my phone number from through which nurses contacted me. (P019)
The Feeling of Guilt and Regret
Other experiences of abortion participants indicate that they develop a guilty conscience.This feeling appears in patients as a feeling of guilt and remorse. The experience of the participants has shown that after abortion, they consider themselves guilty and complain about themselves.
I considered what I had done to my family to be abhorrent. I feel guilty and, in my family, I’m a horrible woman. (P014)
Some mothers in this situation thought of themselves as murderers. A young woman believed that God had punished her for being a murderer because she had not been pregnant for more than two years following an abortion that she had forced.
I perceive myself as a murderer, and I might actually be one. (P021)
………… I have been feeling guilty ever since I had an abortion. I believe I should apologize and repent daily for what I did. I was probably even cursed. (P006)
Some participants stated that they felt remorse for their actions as soon as they had an abortion. Women who had undergone an induced abortion felt terrible about it, were in pain and had many regrets. Many of them hoped they could go back on their decision; however, it was too late.
After having an abortion, I felt terrible about my history because I didn’t lead a healthy lifestyle………. I simply regretted having this abortion at that time. (P001)
It is a decision I will regret for the rest of my life. I’m in excruciating pain and worry constantly, wondering what I was doing when I forced an abortion. (P003)
However, the decision to undergo an induced abortion was viewed by some participants as means of resolving the painful experience and stress associated with an unwanted pregnancy. It led to relief rather than negative psychological experiences.
Much as it was a very painful and stressful experience, I got relieved after the abortion for the burden of both pregnancy and HIV is greater than carrying the pregnancy to its full term; now I’m left to battle with one issue that is HIV. (P006)
I was happy and relieved of the stress of unwanted pregnancy. This resolved the crisis of unwanted pregnancy and I continued to live a normal life after abortion. (P023)
I think I took the best decision to abort. I was relieved because I did not experience the physical symptoms of pregnancy anymore. (P027)
Discussion
This study explored the in-depth, unique experiences of induced abortion following unintended pregnancy among HIV-positive clients in Lira District, Uganda. In this phenomenological study, HIV-infected women recounted their lived experiences with induced abortion. The major causes of induced abortion were financial constraints, concern for the unborn babies, unplanned pregnancy, and complex relationships. Regarding induced abortion-related experiences, three themes emerged: loss of family support, internalized stigma, and perceived stigma. There is a need to note that, the law in Uganda expressly permits women to access safe and legal abortions only if doing so would save their lives.3 However, statistics indicate that there are numerous unsafe abortions in restricted environment like Uganda.16
Our study showed that numerous factors played a role in the choice to seek an induced abortion for many women living with HIV. In these circumstances, it might be challenging to single out one factor as being the most crucial. Even if a woman names one overriding reason for her decision, important information would still be lost because the full spectrum of factors influencing her choice would not be quantified. Thus, this study adds another dimension to understanding some of the underlying factors for induced abortion among HIV-infected women. This set of factors is particularly prevalent in Sub-Saharan Africa, where the majority of abortions are more likely to occur in unstable situations.17 Similarly, in Latin American countries, complex relationships and poverty are among the most important factors why women seek abortion.18
The trickle-down of cultural norms that led to HIV-infected women who have had an induced abortion enduring internalized and perceived stigma after abortion was a recurrent issue in our results. Stigma permeates the social and cultural conventions that influence the decision to abort.19 Our results mirror the findings of other previous studies. For instance, in one study of 87 adolescent girls and young women in Zambia, internalized stigma and shame caused adolescent girls and young women to consider the pros and cons of abortion in comparison to carrying on with an unplanned pregnancy as well as the emotional relief of abortion in comparison to the guilt and sin connected with it.20 A similar study with adolescent girls and young women in Ghana found that the illegality of abortion, religious sermons, media, and other social platforms reinforced the stigma and idea that abortion was a sin.21 Thus, psychological support professionals should be aware that internalized stigma affects HIV-infected women who get pregnant unintentionally and may need to be addressed.
Our results also show that the experiences of HIV-positive women who had induced abortions ranged from guilt, and regrets to a variety of other undesirable feelings. The majority of mental health distress could be attributed to high sensitivity to the comments of people around them which relate to abortion. While some studies show that having an abortion brings about relief.22 South African studies indicate that there are many difficulties, including moral conflict, negative feelings, regret, guilt, self-blame, judgment, and physical agony following abortion.23 However, our findings imply that a knowledge of the risk factors should result in the encouragement of more effective counselling and support for those women who require it.
Our results, however, showed that the decision to undergo an induced abortion was viewed by some participants as means of resolving the painful experience and stress associated with an unwanted pregnancy. It led to relief rather than negative psychological experiences. Induced abortion seemed to resolve the crisis of unwanted pregnancy and lessened the experiencing the physical symptoms of pregnancy. In line with our findings, studies showed that women who chose to have an abortion felt good about their decision.24 According to a 2009 study by Halldén et al, women felt relieved after having an abortion because it ended their dilemma over unintended pregnancy.25
Strength and Limitations
Our study is limited in scope and focused on pregnant HIV-infected women identified from the postnatal clinics in Lira District. Therefore, the experiences of HIV-infected women who did not seek post-natal were not captured. Also, the qualitative method of this study restricts the generalizability of our findings. However, the findings of this study may influence more extensive qualitative research and the creation of interventions to guarantee safe abortion and enhance the well-being of women with HIV.
Conclusion
This study highlights the lived experiences of women living with HIV following an induced abortion. The study shows that women living with HIV had induced abortions due to numerous reasons, including financial concerns, complicated relationships, and a fear of infecting their unborn babies. However, after induced abortion, the women living with HIV faced several challenges like loss of family support, stigma, and feelings of guilt and regret. Based on HIV-infected women who underwent induced abortion and unexpected pregnancy, they may need mental health services to reduce the stigma associated with induced abortion.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgment
The authors wish to acknowledge every participant who took part in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research work was supported by a seed grant from the Center for International Reproductive Health Training at the University of Michigan (CIRHT-UM). The content is solely the responsibility of the authors and does not necessarily represent the official views of CIRHT-UM. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bearak J, Popinchalk A, Ganatra B, et al. Unintended pregnancy and abortion by income, region, and the legal status of abortion: estimates from a comprehensive model for 1990–2019. Lancet Glob Heal. 2020;8:e1152–e1161.
2. Bankole A, Hussain R, Sedgh G, et al. Unintended pregnancy and induced abortion in Burkina Faso: causes and consequences. NY Guttmacher Inst. 2014;1:75.
3. Hussain R. Unintended pregnancy and abortion in Uganda; 2013.
4. Narasimhan M, Orza L, Welbourn A, et al. Sexual and reproductive health and human rights of women living with HIV: a global community survey. Bull World Health Organ. 2016;94:243–249. doi:10.2471/BLT.14.150912
5. Pilecco FB, Teixeira LB, Vigo A, Dewey ME, Knauth DR. Lifetime induced abortion: a comparison between women living and not living with HIV. PLoS One. 2014;9(e95570):e95570. doi:10.1371/journal.pone.0095570
6. FIGO. End preventable deaths and disability from unsafe abortion; 2020. Available from: https://www.figo.org/news/end-preventable-deaths-and-disability-unsafe-abortion.
7. World Health Organization. Health Worker Role in Providing Safe Abortion Care and Post Abortion Contraception. World Health Organization; 2015.
8. Bacchi CL. Women, Policy and Politics: The Construction of Policy Problems. Sage; 1999.
9. Fairclough N. The discourse of new labour: critical discourse analysis; 2001.
10. Uganda Bureau of Statistics. Statistics, U. B. of. population projections by District, 2015 to 2021; 2020. Available from: https://www.ubos.org/population-projections-by-district-2015-to-2021/.
11. Lukwago D. Health spending in Uganda implications on the National minimum health care package; 2016.
12. Napyo A, Nankabirwa V, Mukunya D, et al. Prevalence and predictors for unintended pregnancy among HIV-infected pregnant women in Lira, Northern Uganda: a cross-sectional study. Sci Rep. 2020;10:1–8. doi:10.1038/s41598-020-73490-6
13. Willis DG, Sullivan-Bolyai S, Knafl K, Cohen MZ. Distinguishing features and similarities between descriptive phenomenological and qualitative description research. West J Nurs Res. 2016;38:1185–1204. doi:10.1177/0193945916645499
14. Ritchie J, Lewis J, Nicholls CM, Ormston R. Qualitative Research Practice: A Guide for Social Science Students and Researchers. Sage; 2013.
15. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3:77–101. doi:10.1191/1478088706qp063oa
16. Inzama W, Kaye DK, Kayondo SP, Nsanja JP. Gaps in available published data on abortion in Uganda and the missed opportunity to inform policy and practice. Int J Gynecol Obstet. 2023;161:1–7.
17. Renne EP. The pregnancy that doesn’t stay: the practice and perception of abortion by Ekiti Yoruba women. Soc Sci Med. 1996;42:483–494. doi:10.1016/0277-9536(95)00171-9
18. Mora M, Villarreal J. Unwanted pregnancy and abortion: bogotá, Colombia. Reprod Health Matters. 1993;1:11–20. doi:10.1016/0968-8080(93)90003-C
19. Zia Y, Mugo N, Ngure K, et al. Psychosocial experiences of adolescent girls and young women subsequent to an abortion in sub-Saharan Africa and globally: a systematic review. Front Reprod Heal. 2021;3:638013.
20. Dahlbäck E, Maimbolwa M, Yamba CB, et al. Pregnancy loss: spontaneous and induced abortions among young women in Lusaka, Zambia. Cult Health Sex. 2010;12:247–262. doi:10.1080/13691050903353383
21. Esia-Donkoh K, Darteh EKM, Blemano H, Asare H. Who cares? Pre and post abortion experiences among young females in Cape Coast metropolis, Ghana. Afr J Reprod Health. 2015;19:43–51.
22. Major B, Appelbaum M, Beckman L, et al. Abortion and mental health: evaluating the evidence. Am Psychol. 2009;64:863. doi:10.1037/a0017497
23. Mookamedi RE, Mogotlane SM, Roos JH. The experiences of women who undergo termination of pregnancy in Mpumalanga province, South Africa. Afr J Nurs Midwifery. 2015;17:161–417.
24. Lyon R, Botha K. The experience of and coping with an induced abortion: a rapid review. Heal SA Gesondheid. 2021;26:1–10.
25. Halldén B, Christensson K, Olsson P. Early abortion as narrated by young Swedish women. Scand J Caring Sci. 2009;23:243–250. doi:10.1111/j.1471-6712.2008.00612.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.