Back to Journals » Advances in Medical Education and Practice » Volume 17
Pharmacy Practice in Somalia: Addressing Educational and Regulatory Gaps: A Commentary
Authors Sabrie Z ![]()
Received 8 May 2026
Accepted for publication 12 July 2026
Published 16 July 2026 Volume 2026:17 621531
DOI https://doi.org/10.2147/AMEP.S621531
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Zainab Sabrie1,2
1Faculty of Medicine and Health Sciences, SIMAD University, Mogadishu, Somalia; 2Department of Pharmacy, Dr. Sumait Hospital, SIMAD University, Mogadishu, Somalia
Correspondence: Zainab Sabrie, Faculty of Medicine and Health Sciences, SIMAD University, 389H+29G, Jidka Warshadaha, Mogadishu, 2526, Somalia, Email [email protected]
Abstract: Pharmacists play a key role in ensuring optimal patient care. Despite the expansion of health training institutions in Somalia in recent years, pharmacy programs remain underrepresented. In addition, although pharmaceutical regulatory frameworks have recently been developed in Somalia, implementation and enforcement remain limited. These gaps are evident in pharmacy practice, marked by workforce shortages, inconsistent dispensing practices, and variability in pharmaceutical care standards. This commentary highlights the influence of educational and regulatory barriers on pharmacy practice in Somalia, as well as recent developments, including the approval of the Somalia Medicines Bill, a significant milestone in pharmaceutical governance. Ongoing improvement of pharmacy practice will depend on coordinated reforms in pharmacy education, workforce development, and regulatory oversight. Future policy initiatives should emphasize standardizing pharmacy curricula, strengthening professional regulation and practice oversight, and promoting collaboration among government, academia, and professional stakeholders.
Keywords: pharmacy practice, regulatory gaps, pharmacy education, Somalia
Introduction
The pharmacy profession has evolved from a traditional focus on compounding and dispensing medicines to a patient-centered one.1 Pharmacists are recognized as medication experts within multidisciplinary healthcare teams, especially in low-resource settings, where they are the most accessible healthcare professionals.2,3 To ensure appropriate medication use and good pharmacy practice, qualified, well-regulated pharmacists are needed.4 However, the quality of the pharmacy profession depends on the availability of a regulatory framework, structured educational systems, and established practice standards.5,6 Unfortunately, these critical components remain underdeveloped in many low-resource settings, resulting in inconsistent pharmacy practice and a lack of alignment with global standards.7,8
Somalia warrants special consideration because the negative impacts of long-term conflict and political instability on pharmacy education, training, and regulation, which are required to sustain professional practice, are severe. Decades of civil war led to the collapse of Somalia’s health system, leaving it fragmented and weakly regulated.9 Although health professions education has expanded considerably in recent years in Somalia, concerns remain regarding accreditation, quality assurance, workforce distribution, and regulatory oversight.10 As the World Health Organization reported, based on IFTIN Foundation data, only 13 students graduated from pharmacy out of 5,822 total graduates from health programs.11 This underscores the limited availability of pharmacy training programs, as prior evaluations have indicated. These evaluations documented a lack of pharmacy education/training options, insufficient numbers of trained professionals in the field of pharmacy, and limited institutional capacity for pharmaceutical regulation in Somalia, Somaliland, and Puntland.12,13 While those evaluations occurred before the most recent health care reform measures were implemented, the information they contain provides important historical context for ongoing problems in the pharmaceutical sector. There remains very little recent research evaluating the distribution of the pharmacy workforce, standards of pharmacy education, the content of pharmacy curricula, and the professional competency of pharmacists working in Somalia. A recent scoping review of pharmacy education in sub-Saharan Africa identified a scarcity of literature describing the development of pharmacy education processes, accreditation schemes, competency standards, and educational evaluation in numerous countries across the region.14 The lack of up- to- date information on this topic constitutes a significant knowledge gap for analyzing the current state and future needs of the pharmaceutical profession in Somalia. Since pharmacists play a key role in ensuring that drugs are used safely and properly, this commentary explains why it is important to address gaps in pharmacy education and regulation to enhance the provision of pharmaceutical services in Somalia.
Education and Regulatory Gaps
Pharmacy education is essential for equipping the pharmacy workforce with adequate numbers and appropriate competencies to deliver relevant pharmaceutical care.15 Modern technology, including artificial intelligence, is gaining popularity in pharmacy training as a learning aid; nonetheless, research shows that such technologies should only complement traditional methods of learning due to concerns about credibility and usability.16
Enhancing pharmacy education and strengthening regulatory oversight are fundamental to improving pharmacy practice. Pharmacy practice in Somalia has significant gaps. - From past analyses of the pharmaceutical industry in Somalia, it is evident that there has always been a gap in pharmacy education and workforce capacity in Somalia, including limited training opportunities and shortages of qualified pharmaceutical personnel.12 This is evidenced by the very low ratio of pharmacists to population in Somalia; it has been reported that Somalia has a ratio of 0.02 pharmacists per 10,000 people.17 Although these data are now dated, they highlight longstanding workforce constraints that have affected the development of pharmacy practice in the country. Evidence from the literature further illustrates the severity of these gaps. A 2020 study in Mogadishu found that only 12% of surveyed pharmacy staff were qualified pharmacists; moreover, 86% of employees admitted to dispensing prescription medications without a prescription, a significant deviation from standard pharmaceutical practice.18 Moreover, a nationwide study of the private health sector indicated that only 46% of pharmacies and dispensaries had licensed pharmacists, implying that properly trained pharmacy professionals did not staff many pharmacies.19
Together, these findings suggest that shortages of qualified pharmacy personnel remain a persistent challenge affecting the pharmaceutical sector’s capacity in Somalia. Similar workforce challenges have been reported across low- and middle-income countries, where insufficient investment in pharmacy workforce development contributes to shortages of pharmacists and inequities in access to pharmaceutical services and expertise in medicines.8,17
The consequences of these workforce and educational limitations are particularly significant because pharmacies are among the most accessible forms of healthcare delivery in Somalia. Multiple assessments have found that pharmacies frequently serve as the first point of contact for individuals seeking medication and healthcare advice. However, evidence suggests that medicines are often dispensed without consultation with appropriately qualified healthcare professionals, reflecting the combined effects of workforce shortages, educational constraints, and limited professional oversight.12,19–21
Educational limitations are further compounded by regulatory challenges. The proper implementation of pharmaceutical regulations can enhance the quality of pharmacy practice.22 The regulation of medical products is the responsibility of national regulatory authorities whose role is to enhance the quality of medicines, effectiveness, and safety within the country.23,24 In Somalia, the private health sector is largely unregulated, and implementation of licensing requirements for pharmacies and medicine importers has historically been limited.11 Similar concerns regarding weak enforcement capacity, limited institutional resources, and poor dissemination of regulations have been reported in earlier assessments.12 In addition, it was noted that professional associations historically had limited authority over registration, licensing, accreditation, continuing professional development, and enforcement of professional standards, constraining their ability to support workforce regulation and quality assurance.25
Taken together, the available evidence suggests that pharmacy workforce shortages, limited educational capacity, and weak professional regulatory oversight are not isolated challenges but interconnected factors that collectively shape pharmacy practice in Somalia. Recent reforms, including the National Health Professionals Council Act, the establishment of the interim National Medicines Regulatory Authority, and approval of the Somalia Medicines Bill, provide an important foundation for strengthening governance.26–28 However, their long-term impact will depend on effective implementation and continued investment in pharmacy education, workforce development, and professional regulation.
Implications and Future Directions
Addressing pharmacy practice shortages will require a multifaceted approach, including pharmacy education, workforce development, and regulatory systems. While education develops the knowledge and competencies of future pharmacists, regulatory systems are essential for defining professional standards and ensuring safe and appropriate practice. Enhancing regulatory oversight is crucial to ensure consistent standards in pharmacy practice. Well-regulated systems, supported by efficient national regulatory authorities, are essential to guarantee the quality, safety, and appropriate use of drugs.29 According to the FIP Nanjing Statements, pharmacy education needs to be competency-based and tailored to the needs of local health care systems. It also calls for the establishment of efficient quality assurance systems to keep pace with constantly changing educational standards. The recommendations provided herein apply to the situation in Somalia, where pharmacy education systems are varied and regulation is limited, and they imply the need to improve competency-based curricula and to establish quality assurance programs for all concerned parties, including academia and professional bodies.30
Developing a strong pharmacy practice in Somalia requires clear actions by relevant stakeholders. The health professional regulatory function responsible for licensing and registration should strengthen systems for pharmacist registration and licensing. The national regulatory agency for medicines should ensure proper regulation of medicines, including quality control, safe dispensing, and adherence to distribution standards. These functions are part of the regulatory system that facilitates safe and effective pharmacy practice. Universities should ensure the development of competency-based curricula and experiential learning. There may also be a need to cooperate with international organizations, such as the World Health Organization and the International Pharmaceutical Federation, to strengthen technical capacity, regulation, and workforce development.
A phased implementation strategy could work for Somalia. In phase one, activities would include workforce mapping, enhancements to licensing and inspections, and strengthening of regulatory bodies. Other phases could include curriculum harmonization, additional training, professional development, and the provision of clinical pharmacy services in healthcare facilities. Indicators that could be used to monitor implementation success include the ratio of pharmacists to patients, the number of licensed pharmacists and licensed pharmacies, compliance with the prescription-only medicine law, participation in professional development, and the provision of clinical pharmacy services in hospitals. Further research is needed to provide up-to-date information on the capacity of the pharmacy workforce, educational outcomes, and the effects of regulatory reforms in the country.
To synthesize the key challenges discussed above and highlight potential system-level responses, Table 1 summarises the main gaps in pharmacy education and regulatory systems, along with corresponding recommendations.
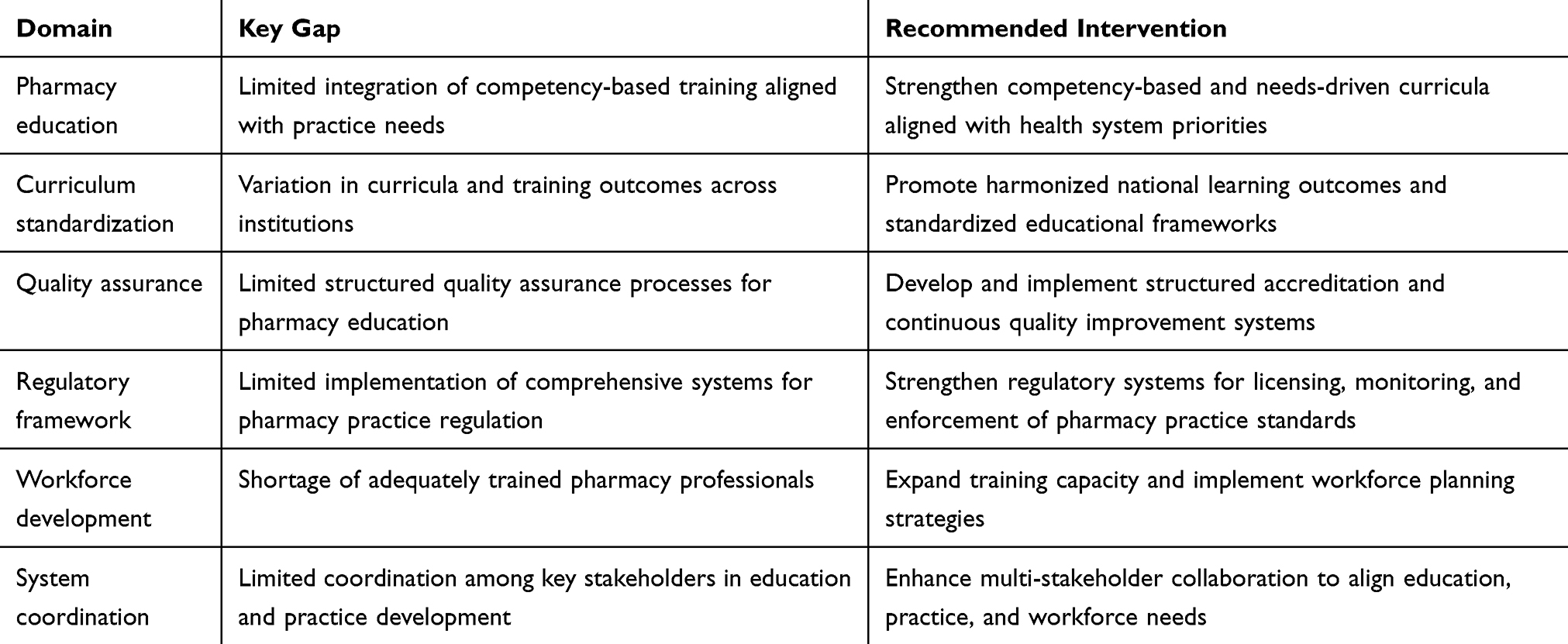 |
Table 1 Key Pharmacy Education and Regulatory Gaps and Proposed Interventions in Somalia |
The summarized interventions highlight the need for coordinated, system-wide approaches integrating pharmacy education, workforce development, and regulatory strengthening to improve pharmacy practice outcomes in Somalia.
Conclusion
This commentary highlights the interconnected weaknesses across pharmacy education, workforce capacity, and regulatory structures that affect pharmacy practice in Somalia. Interventions should focus on pharmacy education, workforce development, and regulation to ensure that pharmacists receive adequate training and are properly positioned within a robust regulatory framework. Developing these interdependent pillars needs to become a top priority for policymakers and institutions across sectors, from education to licensing authorities, concerned with improving the delivery of pharmaceutical services in Somalia.
Acknowledgments
I appreciate the Center for Research and Development at SIMAD University for their invaluable guidance and recommendations.
Funding
This article was supported by SIMAD University.
Disclosure
The author declares no competing interests in this work.
References
1. Toklu HZ, Hussain A. The changing face of pharmacy practice and the need for a new model of pharmacy education. J Young Pharm. 2013;5(2):38–5. doi:10.1016/j.jyp.2012.09.001
2. Valliant SN, Burbage SC, Pathak S, Urick BY. Pharmacists as accessible health care providers: quantifying the opportunity. J Manag Care Spec Pharm. 2022;28(1):85–90. doi:10.18553/jmcp.2022.28.1.85
3. Akachukwu OM, Eigbokhan GO, Nelly TN. Pharmacists in global primary healthcare systems: a comprehensive model for community health empowerment. Int J Front Med Surg Res. 2024;6(2):19–28. doi:10.53294/ijfmsr.2024.6.2.0051
4. Jawaid SA. Quality of pharmacy services and regulatory compliance. Pak J Med Sci. 2016;32(5):1063–1064. doi:10.12669/pjms.325.11111
5. Anderson C, Bates I, Beck D, et al. The WHO UNESCO FIP pharmacy education taskforce. Hum Resour Health. 2009;7(1):45. doi:10.1186/1478-4491-7-45
6. World Health Organization. Joint FIP/WHO guidelines on good pharmacy practice: standards for quality of pharmacy services. WHO Technical Report Series. 2011;961.
7. Kheir N. The paradox of community pharmacy practice in low- and middle-income countries (LMICs). J Pharm Policy Pract. 2025;18(1):2475082. doi:10.1080/20523211.2025.2475082
8. Babar ZU, Scahill S. Barriers to effective pharmacy practice in low- and middle-income countries. Integr Pharm Res Pract. 2014;3:25–27. doi:10.2147/IPRP.S35379
9. Nur FA. Rebuilding a Health System – Experiences From Somalia. Stockholm: Expert Group for Aid Studies (EBA); 2024. EBA Somalia Report.
10. Hassan MM, Ali AN, Ali I, et al. Regulation of health professions education and the growth of schools in Somalia. BMC Med Educ. 2024;24(1):1178. doi:10.1186/s12909-024-06122-5
11. World Health Organization Regional Office for the Eastern Mediterranean. Understanding the private health sector in Somalia. Cairo: WHO Regional Office for the Eastern Mediterranean; 2024. Available from: https://applications.emro.who.int/docs/9789292742041-eng.pdf.
12. Buckley J, O’Neill L, Aden AM. Assessment of the private health sector in Somaliland, Puntland and south central Somalia. Oxford: Health & Education Advice & Resource Team (HEART); 2015. Available from: https://assets.publishing.service.gov.uk/media/57a0899bed915d622c0002e3/Assessment-of-the-Private-Health-Sector-in-Somaliland-Puntland-and-South-Central.pdf.
13. Rydell U, Elmi R. Assessment study of the pharmaceutical sector in Somaliland: report from a visit to Somaliland, 12–22 April 2012. Stockholm: Pharmacists without Borders (Farmaceuter utan Gränser); 2012. Available from: https://fug.se/wp-content/uploads/2016/05/Nippe-2011-Projekt-f%C3%B6r-f%C3%B6rb%C3%A4ttrad-l%C3%A4kemedelsf%C3%B6rs%C3%B6rjning-i-Somalia-Rhoda-Elmi-Report-Pharmaceutical-Sector-Assessment-Somaliland-April-2012_20120624.pdf.
14. Sheehy A, Cannon F, Hegarty G, et al. Development of pharmacy education programmes in sub-Saharan Africa: a scoping review. Int J Pharm Pract. 2026:riaf133. doi:10.1093/ijpp/riaf133
15. Anderson C, Arakawa N. Pharmacy education development. Pharmacy. 2021;9(4):168. doi:10.3390/pharmacy9040168
16. Pellesi L. Trust in AI feedback: challenges in pharmacy education. Med Sci Educ. 2025;35(5):2615–2619. doi:10.1007/s40670-025-02440-6
17. Bates I, John C, Bruno A, Fu P, Aliabadi S. An analysis of the global pharmacy workforce capacity. Hum Resour Health. 2016;14(1):61. doi:10.1186/s12960-016-0158-z
18. Sabrie Z. Assessment of practice details and resource availability of community and hospital pharmacies in Mogadishu, Somalia. J Pharm Pharmacol. 2020;8:320–325.
19. Zaman R, Morris R, Law B, Brouwer L, Thayil S, Lipcan A. Assessing the capacity of the private health system in Somalia. Final Report. 2018.
20. Gele AA, Ahmed MY, Kour P, Moallim SA, Salad AM, Kumar B. Beneficiaries of conflict: a qualitative study of people’s trust in the private health care system in Mogadishu, Somalia. Risk Manag Healthc Policy. 2017;10:127–135. doi:10.2147/RMHP.S137436
21. Ministry of Health and Human Services. Federal government of Somalia. Somalia health sector strategic plan 2022–2026 (HSSP III). Mogadishu; 2021. Available from: https://moh.gov.so/so/wp-content/uploads/2022/11/Health-Sector-Strategy-Plan-III.pdf.
22. Stenson B, Syhakhang L, Lundborg CS, Eriksson B. Private pharmacy practice and regulation: a randomized trial in Lao PDR. Int J Technol Assess Health Care. 2001;17(4):579–589. doi:10.1017/S026646230110709X
23. World Health Organization. WHO Global Benchmarking Tool (GBT) for Evaluation of National Regulatory Systems of Medical Products. Geneva: WHO; 2021.
24. Newton PN, Bond KC, Adeyeye M, et al. COVID-19 and risks to the supply and quality of tests, drugs, and vaccines. Lancet Glob Health. 2020;8(6):e754–e755. doi:10.1016/S2214-109X(20)30136-4
25. Tulenko K, Bile K, D’Lima N, Mohamed IN. Somalia health regulatory landscape: human resource for health (HRH) landscape report. Washington DC: World Bank; 2021. Available from: https://moh.gov.so/so/wp-content/uploads/2024/08/HRH-Regulatory-Landscape-Mission-Report_September-30-2021.pdf.
26. National Health Professions Council (NHPC). About us. Available from: https://nhpc.gov.so/about-us/.
27. National Medicines Regulatory Authority (NMRA). About us. Ministry of health, federal government of Somalia. NMRA About Us. 2023.
28. National Medicines Regulatory Autghority (NMRA). Somalia’s House of the People Approves the Somalia Medicines Bill in a Major Legislative Milestone. NMRA Medicines Bill Announcement; 2026.
29. World Health Organization. Regulatory Systems Strengthening (RSS) Programme. Geneva: WHO RSS Programme; 2026.
30. Law M, Bader L, Uzman N, Williams A, Bates I. The FIP Nanjing statements: shaping global pharmacy and pharmaceutical sciences education. Res Social Adm Pharm. 2019;15(12):1472–1475. doi:10.1016/j.sapharm.2019.03.013
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.