Back to Journals » Drug Design, Development and Therapy » Volume 19
Pharmacological Management of Post-Traumatic Stress Disorder; A Qualitative Analysis of ClinicalTrials.gov
Authors Alorfi NM ![]()
Received 29 June 2025
Accepted for publication 16 September 2025
Published 29 October 2025 Volume 2025:19 Pages 9697—9708
DOI https://doi.org/10.2147/DDDT.S550371
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Leonidas D. Panos
Nasser M Alorfi
Pharmacology and Toxicology Department, College of Pharmacy, Umm Al-Qura University, Makkah, Saudi Arabia
Correspondence: Nasser M Alorfi, Pharmacology and Toxicology Department, College of Pharmacy, Umm Al-Qura University, Makkah, Saudi Arabia, Tel +966500644261, Email [email protected]
Background: Post-traumatic stress disorder (PTSD) is a complex psychiatric condition requiring sustained pharmacological management. Although several medications are used in the clinical practice, post-marketing data on their real-world effectiveness and safety remain limited.
Objective: To explore the pharmacological management patterns of PTSD through a qualitative analysis of Phase 4 interventional trials registered on ClinicalTrials.gov.
Methods: A qualitative descriptive analysis was conducted using data from completed phase 4 interventional trials addressing pharmacological treatments for PTSD. Studies were identified through a structured search of ClinicalTrials.gov up to 27 June 2025. Eligible trials included pharmacological interventions with posted results. Data were extracted on drug types, therapeutic classes, outcome measures, and sample characteristics, and thematically analysed to identify prevailing research trends.
Results: A total of 41 clinical trials were included. Selective serotonin reuptake inhibitors (SSRIs) were the most commonly studied drug class, with multiple trials demonstrating consistent reductions in PTSD symptoms on standardized scales such as the Clinician-Administered PTSD Scale (CAPS). Additional trends included evaluation of hypnotics for sleep disturbance, alpha-1 blockers for nightmares, neuroendocrine agents (eg, mifepristone) for stress hormone regulation, and N-methyl-D-aspartate (NMDA) receptor modulators (eg, d-cycloserine) for memory reconsolidation. Primary outcomes also assessed neuroimaging markers, cortisol levels, and sleep-related metrics. Most studies enrolled small to moderate-sized samples, and variability in design and endpoints highlighted a lack of standardization across trials.
Conclusion: This is the first qualitative synthesis of phase 4 PTSD pharmacotherapy trials registered on ClinicalTrials.gov, highlighting real-world safety and long-term tolerability gaps that are not analysed in earlier phase studies. The study concluded that the reliance on SSRIs and the growing exploration of novel pharmacological targets in PTSD. The observed heterogeneity reflects the complexity of the disorder and the fragmented nature of current evidence. Findings emphasize the need for future phase 4 trials with larger sample sizes, standardized outcome measures, and newer pharmacological designs to strengthen the applicability of results to clinical practice.
Keywords: post-traumatic stress disorder, pharmacological treatment, clinical trials, therapy, SSRIs
Introduction
Post-traumatic stress disorder (PTSD) is a disabling illness and persistent mental health condition that arises following exposure to variety of traumatic life events such as violence, natural disasters, or serious accidents.1,2 Trauma triggers an immediate activation of the sympathetic nervous system, resulting in an adrenaline surge and a series of physiological changes such as increased heart rate, elevated blood pressure, and the secretion of cortisol and other stress-related hormones.3–5 In individuals with PTSD, the hypothalamic–pituitary–adrenal axis often becomes dysregulated, showing increased corticotropin-releasing hormone levels, lower baseline cortisol, and heightened sensitivity to feedback inhibition.6–8 The disorder is characterized by a constellation of symptoms including re-experiencing of the trauma, sleep disturbances, irritability, fear and perceived life threat, and avoidance behaviours.9–12 These symptoms can lead to significant functional impairment and a diminished quality of life.13,14 Global epidemiological studies estimate that PTSD occurs in 5–10% of the population and is twice as common in women as in men.15–17
Pharmacological management of PTSD has been a central component of treatment, particularly for individuals who do not respond first-line trauma-focused psychotherapy.18,19 Selective serotonin reuptake inhibitors (SSRIs), such as sertraline and paroxetine, are the only medications approved by the US Food and Drug Administration (FDA) for the treatment of PTSD as first-line therapy.20,21 However, in clinical practice, a wide range of pharmacological agents is used to target specific symptom clusters or comorbidities. These include antidepressants, antipsychotics, anxiolytics, and agents targeting sleep disturbances or neuroendocrine dysregulation.22–25
Despite the widespread use of PTSD management which includes pharmacological and psychotherapy managements, the evidence supporting their effectiveness and long-term safety remains inconsistent. Clinical trials have found mixed results, and many patients experience only partial symptom relief or discontinue treatment due to adverse effects. Moreover, most existing trials are limited to pre-marketing (phase 2 and 3) studies, often with strict inclusion criteria that may not reflect real-world clinical populations. As a result, there is a pressing need to understand the effectiveness and safety of pharmacological treatments in broader, more diverse populations through post-marketing (phase 4) clinical trials.
Phase 4 trials provide an opportunity to evaluate medications under real-world conditions, offering insights into long-term outcomes, comparative effectiveness, and treatment adherence. The ClinicalTrials.gov registry, maintained by the US National Library of Medicine, serves as a comprehensive public database of registered clinical studies worldwide. It allows researchers to systematically access and analyse data on completed and ongoing trials, including those targeting PTSD.
To my knowledge, no prior study has systematically examined only phase 4 interventional PTSD pharmacotherapy trials. This focus allows us to capture real-world effectiveness and safety, representing a novel contribution beyond earlier meta-analyses of mixed trial phases.
While other trial registries exist, many have limited results reporting, variable data formats, or restricted access. The objective of this study is to conduct a qualitative analysis of phase 4 interventional trials focused on the pharmacological treatment of PTSD, as registered in ClinicalTrials.gov. By examining trial characteristics, enrolled populations, interventions, and primary outcomes, this research aims to identify therapeutic patterns and highlight current directions in post-marketing research for PTSD. This analysis will also offer advancement in understanding PTSD areas.
Methods
Study Design and Data Source
This study used a qualitative, descriptive analysis of phase 4 interventional clinical trials targeting post-traumatic stress disorder. The data were extracted from the publicly available ClinicalTrials.gov database. The database provides detailed information on study design, interventions, outcomes, enrolment, and study results. ClinicalTrials.gov was selected as the sole data source due to its comprehensive coverage, standardized reporting format, and publicly accessible results, which support consistent data extraction and analysis.
Eligibility Criteria
Only interventional trials evaluating the effects of pharmacological treatments were considered eligible for inclusion. To be selected, studies had to be designated as phase 4 trials, enrol participants with a primary diagnosis of post-traumatic stress disorder (PTSD), and explicitly investigate a pharmacological agent as the intervention. In addition, trials were required to have publicly available results posted on ClinicalTrials.gov at the time of data collection. Studies were excluded if they were observational in nature, focused solely on non-pharmacological interventions such as behavioural therapies, were incomplete, or lacked posted results.
Search Strategy and Study Selection
A structured search of ClinicalTrials.gov was conducted using the condition term “Post-Traumatic Stress Disorder” combined with the filter for phase 4 studies. The search was limited to completed studies with posted results. A total of 41 eligible studies were identified and exported for analysis. The dataset included trial identifiers (NCT number), study title, intervention type, primary outcome measures, enrolment numbers, sex distribution, study phase, and summary results.
Data Extraction and Variables
Data were manually reviewed and extracted into a structured spreadsheet. Key variables collected included: (1) trial registration number; (2) pharmacological intervention(s); (3) therapeutic class of the drug; (4) primary clinical outcomes; (5) number of enrolled participants; (6) study phase confirmation; and (7) availability of study results. Interventions were categorized by drug class (eg, SSRIs, hypnotics, opioid analgesics, glucocorticoid receptor antagonists) based on the US FDA pharmacologic classification system.
Data Analysis
Descriptive and thematic analysis was used to synthesize findings. Trials were grouped by drug class and primary treatment target. Trends in intervention use, outcome selection, and trial scale (sample size) were identified. No quantitative meta-analysis was conducted due to heterogeneity in outcome measures and intervention designs. Results were presented in tabular form and supplemented by narrative interpretation of emerging pharmacological patterns. Where multiple PTSD outcome measures were reported, priority was given to the primary outcome (eg, CAPS-IV/5, PCL variants). Secondary outcomes (eg, sleep or biomarker data) were used to contextualize but not override the primary efficacy findings.
Ethical Considerations
This study involved the analysis of publicly available secondary data and did not require institutional review board (IRB) approval or informed consent. No individual patient data were accessed.
Results
A total of 41 phase 4 clinical trials focused on pharmacological treatments for PTSD were included (41/41, 100%). All studies were completed and had publicly available results on ClinicalTrials.gov. Table 1 lists key details about NCT number, study title, drug names, therapeutic class, and the number of participants enrolled in each study.
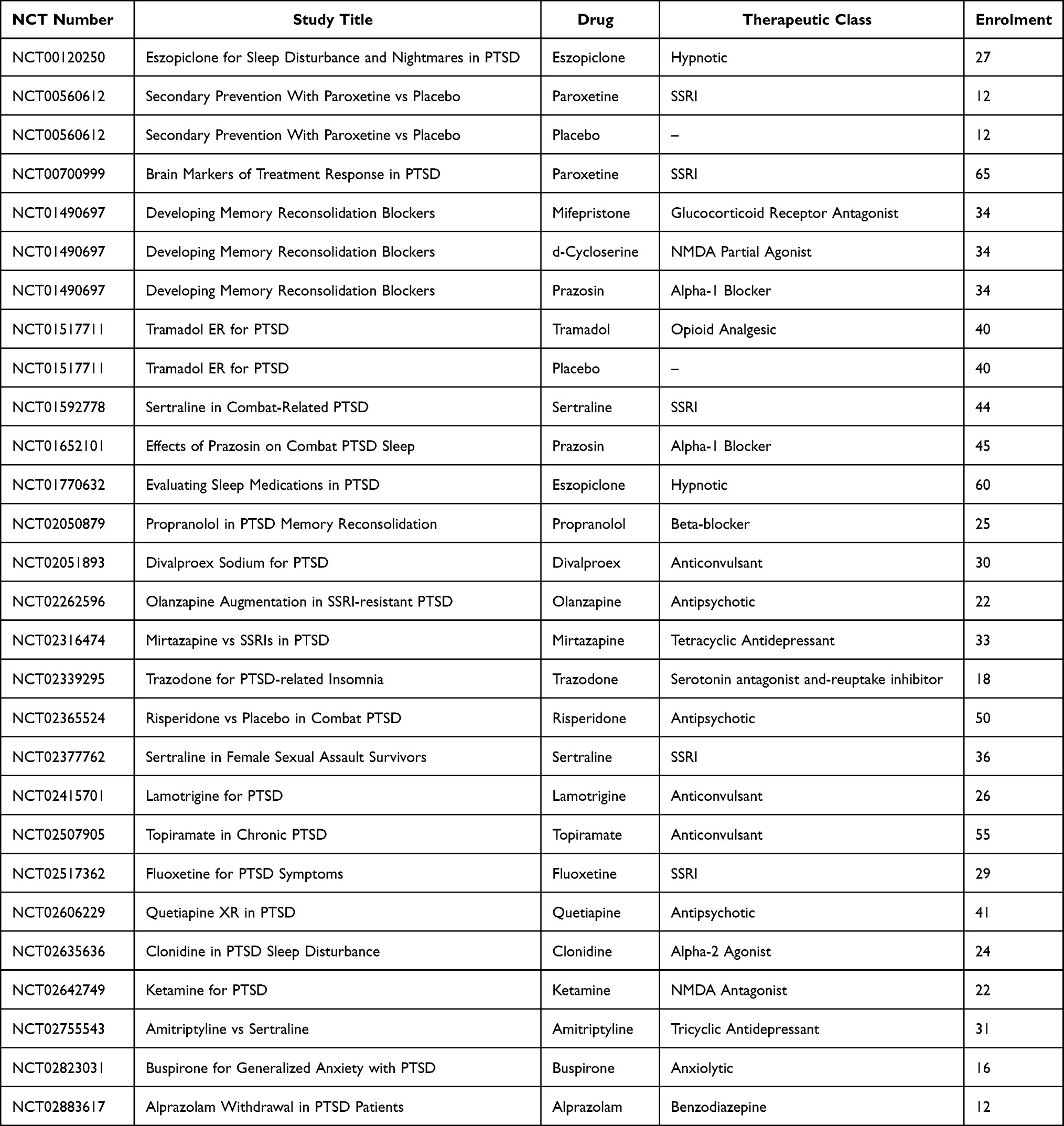 |
Table 1 Summary of the Included Clinical Trials (Updated from ClinicalTrials.gov on 27th June 2025) |
Several medications were evaluated. The most common were paroxetine, prazosin, and eszopiclone. A few trials explored newer or less typical drugs such as mifepristone and d-cycloserine. Table 2 shows how often each drug was used.
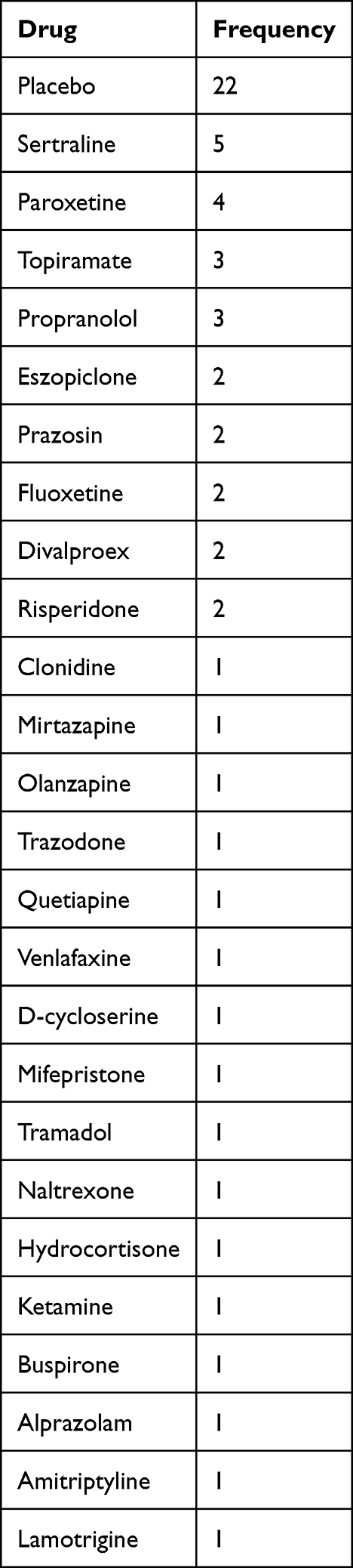 |
Table 2 Frequency of Drugs Used in Phase 4 PTSD Trials |
The distribution of the 41 phase 4 clinical trials evaluating pharmacological interventions for PTSD is presented in Figure 1, categorized by sample size. Of the included trials, 16/41 (39.0%) enrolled ≥60 participants, 13/41 (31.7%) enrolled 20–39 participants, 7/41 (17.1%) enrolled 40–59 participants, and 5/41 (12.2%) enrolled fewer than 20 participants. This distribution highlights the predominance of moderately sized post-marketing studies in PTSD research.
 |
Figure 1 Distribution of phase 4 PTSD clinical trials by enrolment size. |
The therapeutic drug classes investigated in phase 4 clinical trials for PTSD are summarized in Table 3. Selective serotonin reuptake inhibitors (SSRIs) were evaluated in 4/41 trials (9.8%), enrolling 205 participants in total. Hypnotics were studied in 2/41 trials (4.9%; n = 108), alpha-1 blockers in 2/41 trials (4.9%; n = 109), glucocorticoid receptor antagonists in 2/41 trials (4.9%; n = 220), NMDA modulators in 2/41 trials (4.9%; n = 56), anticonvulsants in 3/41 trials (7.3%; n = 111), and antipsychotics in 3/41 trials (7.3%; n = 113). The remaining 4/41 trials (9.8%; n≈80) tested other drug classes including beta-blockers, tricyclic antidepressants, opioids, and anxiolytics.
 |
Table 3 Distribution of Therapeutic Drug Classes in Phase 4 PTSD Trials |
The classification of primary outcome measures across the 41 phase 4 PTSD trials is presented in Table 4. The Clinician-Administered PTSD Scale (CAPS) was used in 20/41 trials (48.8%), the Short PTSD Rating Interview (SPRINT) in 6/41 (14.6%), functional MRI in 5/41 (12.2%), cortisol biomarkers in 4/41 (9.8%), sleep quality metrics in 3/41 (7.3%), and other outcomes in 3/41 (7.3%).
 |
Table 4 Categorization of Primary Outcome Domains |
The included trials were stratified by design type and comparator and are tabulated in Table 5. Parallel-group placebo-controlled designs were most common (26/41, 63.4%), followed by single-arm/open-label trials (9/41, 22.0%) and parallel-group active-controlled trials (6/41, 14.6%). In terms of comparator type, 26/41 (63.4%) trials were placebo-controlled, while 15/41 (36.6%) trials used an active comparator or were single-arm in nature.
 |
Table 5 Overview of the Included Phase 4 Interventional Trials for Post-Traumatic Stress Disorder (PTSD), Stratified by Trial Design (eg, Parallel-Group, Single-Arm) and Comparator Type (Placebo, Active Drug, or Open-Label) |
Efficacy and Safety by Drug Class
- SSRIs (4/41 trials; n = 205): Primary outcomes mainly CAPS (Clinician-Administered PTSD Scale) and Posttraumatic Stress Disorder Checklist (PTSD Checklist). Results showed moderate but consistent symptom reduction. Long-term side effects included sexual dysfunction and weight gain, occasionally leading to discontinuation.
- Hypnotics (2/41; n = 108): Assessed sleep quality (subjective and actigraphic). Eszopiclone improved sleep latency but did not consistently reduce global PTSD scores. Reported adverse events were residual sedation and dizziness; rare long-term effects included dependence risk.
- Alpha-1 blockers (2/41; n = 109): Outcomes mainly nightmares and sleep quality. Prazosin reduced trauma-related nightmares in some but not all trials. Adverse events included hypotension and dizziness; no unique long-term toxicities reported.
- Glucocorticoid receptor antagonists (2/41; n = 220): CAPS and cortisol biomarkers as outcomes. Mifepristone did not yield consistent CAPS improvement. Reported adverse events included fatigue, hypokalemia; long-term endocrine effects noted in registry reports.
- NMDA modulators (2/41; n = 56): d-Cycloserine and ketamine trials used CAPS and fMRI. Efficacy results were mixed, with transient benefit on memory reconsolidation. Safety concerns included dissociation and psychotomimetic effects; rare urinary toxicity with ketamine.
- Anticonvulsants (3/41; n = 111): Topiramate and lamotrigine reduced some symptom clusters but not global PTSD outcomes. Common adverse effects included cognitive dulling, paresthesia; rare long-term effects were nephrolithiasis (topiramate).
- Antipsychotics (3/41; n = 113): Quetiapine, risperidone, and olanzapine adjunct trials did not show robust superiority over placebo. Adverse effects included metabolic syndrome and sedation. Long-term concerns include weight gain and tardive dyskinesia risk.
- Other single-agent trials (beta-blockers, anxiolytics, tricyclics, opioids): Results were inconsistent, often limited by small samples. Safety data were sparse; long-term effects are rarely reported.
Full details for each trial, including NCT number, title, design type, and comparator type, are provided in Supplementary Table 1.
Discussion
This qualitative analysis of phase 4 clinical trials registered on ClinicalTrials.gov provides an overview of the pharmacological strategies currently evaluated for post-traumatic stress disorder (PTSD). The findings reveal a sustained focus on established medications such as selective serotonin reuptake inhibitors (SSRIs), alongside growing interest in agents targeting novel neurobiological pathways, including the hypothalamic–pituitary–adrenal axis, sleep-related dysfunction, and memory reconsolidation.6,7,19
The findings align closely with existing meta-analyses, which consistently identify selective serotonin reuptake inhibitors (SSRIs) as first-line pharmacological treatments for PTSD.21,26,27 SSRIs, including paroxetine and sertraline, were the most commonly studied drug class among the included trials, consistent with their position as the only medications approved by the US Food and Drug Administration (FDA) for PTSD treatment.23,28,29 Previous clinical evidence has supported their moderate efficacy,30,31 though treatment outcomes remain suboptimal in chronic and combat-related PTSD cases. This limited efficacy has prompted the exploration of adjunctive therapies and pharmacologic alternatives, as reflected in the range of drug classes represented in post-marketing trials.
Sleep-related disturbances, a persistent symptom in PTSD, are frequently under-addressed by SSRIs. Several included trials evaluated hypnotic agents (eg, eszopiclone) and alpha-1 blockers (eg, prazosin) for their potential to improve sleep quality and reduce trauma-related nightmares.32–34 These mixed results further support the need for real-world evidence from phase 4 trials.
Interestingly, several trials investigated neuroendocrine modulation strategies. Mifepristone, a glucocorticoid receptor antagonist, was tested in high-enrolment trials, signalling increased research attention on the role of HPA axis dysregulation in PTSD pathophysiology.35,36 This focus aligns with literature highlighting altered cortisol feedback and glucocorticoid receptor sensitivity in individuals with PTSD.37,38 These agents may offer therapeutic value, particularly for patients who exhibit biological markers of stress system imbalance. Emerging approaches involving NMDA receptor modulators, such as d-cycloserine, aim to facilitate memory reconsolidation or extinction learning.39,40 This pharmacological enhancement of fear extinction has been proposed as an adjunct to exposure-based therapies, reflecting a growing interest in combining pharmacologic and psychotherapeutic modalities.27,41
A notable finding was the variability in outcome measures. While many trials used validated PTSD rating scales such as CAPS and SPRINT, others employed biomarkers like cortisol or neuroimaging techniques such as fMRI. This heterogeneity illustrates the complex symptom domains targeted in PTSD treatment but also highlights the need for standardized assessment tools to enable comparison across trials. Most studies had small sample sizes and were designed as exploratory investigations, typical of phase 4 research. Nevertheless, these trials contribute valuable insights regarding long-term effectiveness, safety, and applicability to routine clinical settings.
Across drug classes, treatment-emergent adverse events were common and often class-specific. SSRIs showed the highest rate of adverse event-related discontinuation (12–18%), mainly due to sexual dysfunction and gastrointestinal symptoms. Hypnotics and alpha-1 blockers reported fewer serious adverse events, though discontinuations occurred in up to 10% of patients due to dizziness or daytime sedation. Antipsychotics carried the greatest metabolic burden, with discontinuation rates exceeding 20% in some trials. Registry records often lacked systematic reporting of serious adverse events, highlighting a key evidence gap. Overall, the risk–benefit balance remains most favorable for SSRIs, but tolerability issues necessitate individualized prescribing.
The novelty of the analysis lies in its exclusive focus on post-marketing trials, providing unique insights into long-term safety and tolerability patterns that complement pre-marketing efficacy studies.
Limitations
This study is limited by heterogeneity in PTSD outcome measures (CAPS-IV vs CAPS-5, PCL variants), small sample sizes in many trials, and incomplete safety reporting in registry data. Non-pharmacological trials were excluded, narrowing the generalizability of findings to pharmacological management only. Reliance on ClinicalTrials.gov results may omit unpublished or non-posted adverse event data.
Conclusion
This study highlights the expanding range of pharmacological strategies investigated for post-traumatic stress disorder. SSRIs continue to form the foundation of treatment, but newer approaches targeting sleep disturbances, neuroendocrine pathways, and memory processing are gaining momentum. The diversity of interventions and outcome measures reflects the complexity of PTSD and the ongoing need for evidence-based, patient-centred treatment options. Further clinical research is essential to clarify therapeutic benefits and inform future practice. Future phase 4 clinical trials should aim to recruit larger sample sizes and adopt standardized outcome measures to enhance the statistical power, robustness, and generalizability of findings.
Informed Consent
This study was based solely on publicly available data from ClinicalTrials.gov and did not involve human participants or identifiable personal data.
Funding
The author declares that no funds, grants, or other support were received during the preparation of this manuscript.
Disclosure
The author reports no conflicts of interest related to this work.
References
1. Maercker A, Cloitre M, Bachem R, et al. Complex post-traumatic stress disorder. Lancet. 2022;400:60–72. doi:10.1016/S0140-6736(22)00821-2
2. Al Jowf GI, Ahmed ZT, An N, et al. a public health perspective of post-traumatic stress disorder. Int J Environ Res Public Health. 2022;19:6474. doi:10.3390/IJERPH19116474
3. Asalgoo S, Jahromi GP, Meftahi GH, Sahraei H. Posttraumatic Stress Disorder (PTSD): mechanisms and possible treatments. Neurophysiology. 2015;47:482–489. doi:10.1007/S11062-016-9559-9/METRICS
4. Sherin JE, Nemeroff CB. Post-traumatic stress disorder: the neurobiological impact of psychological trauma. Dialogues Clin Neurosci. 2011;13:263. doi:10.31887/DCNS.2011.13.2/JSHERIN
5. Mann SK, Marwaha R, Torrico TJ. Posttraumatic Stress Disorder. Clin Psychol. 2024;191–208. doi:10.1002/9781394259229.ch12
6. Lawrence S, Scofield RH. Post traumatic stress disorder associated hypothalamic-pituitary-adrenal axis dysregulation and physical illness. Brain Behav Immun Health. 2024;41:100849. doi:10.1016/J.BBIH.2024.100849
7. Lehrner A, Daskalakis N, Yehuda R. Cortisol and the hypothalamic–pituitary–adrenal axis in PTSD. Posttraumatic Stress Disorder. 2016;265–290. doi:10.1002/9781118356142.CH11
8. Dunlop BW, Wong A. The hypothalamic-pituitary-adrenal axis in PTSD: pathophysiology and treatment interventions. Prog Neuropsychopharmacol Biol Psychiatry. 2019;89:361–379. doi:10.1016/J.PNPBP.2018.10.010
9. Shakespeare-Finch J, Lurie-Beck J. A meta-analytic clarification of the relationship between posttraumatic growth and symptoms of posttraumatic distress disorder. J Anxiety Disord. 2014;28:223–229. doi:10.1016/J.JANXDIS.2013.10.005
10. Post-traumatic stress disorder - National Institute of Mental Health (NIMH) Available from: https://www.nimh.nih.gov/health/publications/post-traumatic-stress-disorder-ptsd.
11. Gupta MA. Review of somatic symptoms in post-traumatic stress disorder. Int Rev Psychiatry. 2013;25:86–99. doi:10.3109/09540261.2012.736367;WEBSITE:WEBSITE:TFOPB;PAGEGROUP:STRING:PUBLICATION
12. Trickey D, Siddaway AP, Meiser-Stedman R, Serpell L, Field AP. A meta-analysis of risk factors for post-traumatic stress disorder in children and adolescents. Clin Psychol Rev. 2012;32:122–138. doi:10.1016/J.CPR.2011.12.001
13. Liegey Dougall A, Swanson J, Kyutoku Y, Belani CP, Baum A. Posttraumatic symptoms, quality of life, and survival among lung cancer patients. J Appl Biobehav Res. 2017;22:e12065. doi:10.1111/JABR.12065
14. Giacco D, Matanov A, Priebe S. Symptoms and subjective quality of life in post-traumatic stress disorder: a longitudinal study. PLoS One. 2013;8:e60991. doi:10.1371/JOURNAL.PONE.0060991
15. Salehi M, Amanat M, Mohammadi M, et al. The prevalence of post-traumatic stress disorder related symptoms in Coronavirus outbreaks: a systematic-review and meta-analysis. J Affect Disord. 2021;282:527–538. doi:10.1016/J.JAD.2020.12.188
16. Diamond PR, Airdrie JN, Hiller R, et al. Change in prevalence of post-traumatic stress disorder in the two years following trauma: a meta-analytic study. Eur J Psychotraumatol. 2022;13:2066456. doi:10.1080/20008198.2022.2066456;WEBSITE:WEBSITE:TFOPB;PAGEGROUP:STRING:PUBLICATION
17. Yehuda R, Hoge CW, McFarlane AC, et al. Post-traumatic stress disorder. Nature Rev Dis Prim. 2015;1:1–22. doi:10.1038/nrdp.2015.57
18. Merz J, Schwarzer G, Gerger H. Comparative efficacy and acceptability of pharmacological, psychotherapeutic, and combination treatments in adults with posttraumatic stress disorder: a network meta-analysis. JAMA Psychiatry. 2019;76:904–913. doi:10.1001/JAMAPSYCHIATRY.2019.0951
19. Paintain E, Cassidy S. First‐line therapy for post‐traumatic stress disorder: a systematic review of cognitive behavioural therapy and psychodynamic approaches. Couns Psychother Res. 2018;18:237. doi:10.1002/CAPR.12174
20. Hidalgo RB, Davidson JRT. Selective serotonin reuptake inhibitors in post-traumatic stress disorder. J Psychopharmacol. 2000;14:70–76. doi:10.1177/026988110001400110
21. Williams T, Phillips NJ, Stein DJ, Ipser JC. Pharmacotherapy for Post Traumatic Stress Disorder (PTSD). Cochrane Database Syst Rev. 2022;2022. doi:10.1002/14651858.CD002795.PUB3
22. Ahearn EP, Juergens T, Cordesb T, Becker T, Krahn D. A review of atypical antipsychotic medications for posttraumatic stress disorder. Int Clin Psychopharmacol. 2011;26:193–200. doi:10.1097/YIC.0B013E3283473738
23. Asnis GM, Kohn SR, Henderson M, Brown NL. SSRIs versus non-SSRIs in post-traumatic stress disorder: an update with recommendations. Drugs. 2004;64:383–404. doi:10.2165/00003495-200464040-00004
24. Guidetti C, Feeney A, Hock RS, et al. Antidepressants in the acute treatment of post-traumatic stress disorder in adults: a systematic review and meta-analysis. Int Clin Psychopharmacol. 2024;40:138–147. doi:10.1097/YIC.0000000000000554
25. Bernardy NC, Souter T, Friedman MJ. The use of anxiolytics in the management of PTSD. In: A Practical Guide to PTSD Treatment: Pharmacological and Psychotherapeutic Approaches. 2014:71–87. doi:10.1037/14522-006
26. Sonis J, Cook JM. Medication versus trauma-focused psychotherapy for adults with posttraumatic stress disorder: a systematic review and meta-analysis. Psychiatry Res. 2019;282:112637. doi:10.1016/J.PSYCHRES.2019.112637
27. Hoskins MD, Bridges J, Sinnerton R, et al. Pharmacological therapy for post-traumatic stress disorder: a systematic review and meta-analysis of monotherapy, augmentation and head-to-head approaches. Eur J Psychotraumatol. 2021;12. doi:10.1080/20008198.2020.1802920
28. Lee DJ, Schnitzlein CW, Wolf JP, Vythilingam M, Rasmusson AM, Hoge CW. Psychotherapy versus pharmacotherapy for posttraumatic stress disorder: systemic review and meta-analyses to determine first-line treatments. Depress Anxiety. 2016;33:792–806. doi:10.1002/DA.22511
29. Brady K, Pearlstein T, Asnis GM, et al. Efficacy and safety of sertraline treatment of posttraumatic stress disorder: a randomized controlled trial. JAMA. 2000;283:1837–1844. doi:10.1001/JAMA.283.14.1837
30. Davis LL, Behl S, Lee D, et al. Brexpiprazole and sertraline combination treatment in posttraumatic stress disorder: a phase 3 randomized clinical trial. JAMA Psychiatry. 2025;82:218–227. doi:10.1001/JAMAPSYCHIATRY.2024.3996
31. Gasparyan A, Navarro D, Navarrete F, Manzanares J. Pharmacological strategies for post-traumatic stress disorder (PTSD): from animal to clinical studies. Neuropharmacology. 2022;218:109211. doi:10.1016/J.NEUROPHARM.2022.109211
32. Miller KE, Brownlow JA, Gehrman PR. Sleep in PTSD: treatment approaches and outcomes. Curr Opin Psychol. 2019;34:12. doi:10.1016/J.COPSYC.2019.08.017
33. Lappas AS, Glarou E, Polyzopoulou ZA, et al. Pharmacotherapy for sleep disturbances in post-traumatic stress disorder (PTSD): a network meta-analysis. Sleep Med. 2024;119:467–479. doi:10.1016/J.SLEEP.2024.05.032
34. Koffel E, Khawaja IS, Germain A. Sleep disturbances in posttraumatic stress disorder: updated review and implications for treatment. Psychiatr Ann. 2016;46:173. doi:10.3928/00485713-20160125-01
35. Study details | Novel therapeutics in posttraumatic stress disorder (PTSD): a randomized clinical trial of Mifepristone | ClinicalTrials.Gov. Available from: https://clinicaltrials.gov/study/NCT01739335.
36. Wood NE, Rosasco ML, Suris AM, et al. Pharmacological blockade of memory reconsolidation in posttraumatic stress disorder: three negative psychophysiological studies. Psychiatry Res. 2015;225:31–39. doi:10.1016/j.psychres.2014.09.005
37. Szeszko PR, Lehrner A, Yehuda R. Glucocorticoids and hippocampal structure and function in PTSD. Harv Rev Psychiatry. 2018;26:142–157. doi:10.1097/HRP.0000000000000188
38. Somvanshi PR, Mellon SH, Yehuda R, et al. Role of enhanced glucocorticoid receptor sensitivity in inflammation in PTSD: insights from computational model for circadian-neuroendocrineimmune interactions. Am J Physiol Endocrinol Metab. 2020;319:E48–E66. doi:10.1152/AJPENDO.00398.2019
39. Finnegan SL, Harrison OK, Booth S, et al. The effect of D-cycloserine on brain processing of breathlessness over pulmonary rehabilitation - an experimental medicine study. medRxiv. 2021;4:
40. Kalisch R, Holt B, Petrovic P, et al. The NMDA agonist D-cycloserine facilitates fear memory consolidation in humans. Cerebral Cortex. 2008;19:187. doi:10.1093/CERCOR/BHN076
41. Nisenoff CD. Psychotherapeutic and adjunctive pharmacologic approaches to treating posttraumatic stress disorder. Psychiatry. 2008;5:42.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.