")
Back to Journals » Drug Design, Development and Therapy » Volume 18
Pharmacokinetics, Pharmacodynamics, and Safety of Evocalcet (KHK7580), a Novel Calcimimetic Agent: An Open-Label, Single- and Multiple-Dose, Phase I Trial in Healthy Chinese Subjects
Authors He X , Narushima K, Kojima M, Nagai C, Li K
Received 7 September 2023
Accepted for publication 4 February 2024
Published 26 February 2024 Volume 2024:18 Pages 567—581
DOI https://doi.org/10.2147/DDDT.S437903
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Georgios Panos
Xuemei He,1 Kazuya Narushima,2 Masahiro Kojima,2 Chisato Nagai,2 Kexin Li1
1Clinical Trial Center, Beijing Hospital, National Center of Gerontology; Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, Beijing Key Laboratory of Assessment of Clinical Drugs Risk and Individual Application, Beijing, People’s Republic of China; 2Research & Development Division, Kyowa Kirin Co., Ltd, Tokyo, Japan
Correspondence: Kexin Li, Clinical Trial Center, Beijing Hospital, National Center of Gerontology; Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, Beijing Key Laboratory of Assessment of Clinical Drugs Risk and Individual Application, Beijing, People’s Republic of China, Email [email protected]
Purpose: This study explored the pharmacokinetics (PK), pharmacodynamics (PD), and safety of evocalcet (KHK7580), a new calcimimetic agent, in healthy Chinese subjects following single and multiple doses.
Methods: This was a single-center, open-label phase I trial conducted in China. The study started from the single-dose cohorts (1, 3, 6, 12 mg evocalcet, step-by-step administration) and proceeded to the multiple-dose cohort (6 mg evocalcet once daily for eight days). Blood and urine samples were collected at the designated time points for pharmacokinetic and pharmacodynamic analysis. Safety was evaluated by treatment-emergent adverse events (TEAEs), clinical laboratory tests, vital signs, electrocardiograms (ECGs), and ophthalmological examination.
Results: Among 42 enrolled subjects, eight in each single-dose cohort and 10 in multiple-dose cohort, 40 subjects completed the study. In single-dose cohorts, tmax was 1.00– 2.00 h and declined biphasically. The mean t1/2 was 15.99– 20.84 h. Evocalcet exposure in AUC0-inf, AUC0-t, and Cmax showed a dose-proportional increase. In the multiple-dose cohort, tmax was 2.00 h and declined biphasically after multiple administrations. The accumulation was negligible. Ctrough levels were similar across days and steady from 24 hours after the first administration. The mean t1/2 was 15.59 h. PD analysis showed that evocalcet decreased intact parathyroid hormone and corrected calcium levels in a dose-dependent manner. Seventeen (40.5%) subjects reported TEAEs. No serious or severe TEAE occurred.
Conclusion: In healthy Chinese subjects, evocalcet demonstrated dose-dependent PK and PD properties and was well-tolerated.
Keywords: evocalcet, calcimimetic agents, secondary hypoparathyroidism, pharmacokinetic, pharmacodynamic, safety
Introduction
Chronic kidney disease (CKD)-mineral and bone disorder (MBD) is a systemic disorder of mineral and bone metabolism due to CKD and is associated with common complications such as fragility fractures and vascular and valvular calcification.1,2 Secondary hyperparathyroidism (SHPT) is one of the most significant types of CKD-MBD, with a prevalence of 11.5%-54%.3,4 It is characterized by excessive secretion of parathyroid hormone (PTH), hyperphosphatemia, and hypocalcemia, leading to osteitis fibrosis and ectopic calcification, resulting in high morbidity and mortality.4–6 In China, the prevalence of severe hyperphosphatemia (>7 mg/dL) and SHPT (>600 pg/mL) were 27% and 21% in patients undergoing hemodialysis, respectively. Furthermore, the management of MBD in China requires improvement and standardization.7
The traditional interventions for SHPT include the modulation of phosphorus (P) and calcium (Ca) balance by dialysis and dietary restriction, calcitriol, other vitamin D analogs, and phosphate binders.5 Furthermore, serum PTH levels should be lowered to a target range.8 Calcimimetic agents mimic the action of Ca on calcium-sensing receptors (CaSR) in the parathyroid gland, thus suppressing PTH synthesis and secretion.9–11 Cinacalcet hydrochloride (the first calcimimetic agent approved for use) and etelcalcetide reduce intact PTH levels and affect P and Ca in CKD patients with SHPT.9,12,13 Nevertheless, the safety concerns of cinacalcet hydrochloride regarding the upper gastrointestinal tract burden the patients and limit the dosage increase to a thoroughly effective level.14 In addition, specific considerations for drug interactions are required when coadministered with other drugs because cinacalcet hydrochloride has a strong inhibitory effect on cytochrome P450 (CYP) 2D6 and is metabolized by CYP3A4.15–17 Unlike cinacalcet, etelcalcetide activates the CaSR by binding the extracellular domain. Etelcalcetide allows better compliance than cinacalcet due to fewer pills to be taken and it is administered when the hemodialysis session is completed.18 Etelcalcetide did not inhibit or induce CYP450 enzymes and was itself not a substrate for metabolism by CYP450 enzymes. However, the incidence of upper gastrointestinal symptoms (such as nausea and vomiting) was similar to cinacalcet.19,20 Furthermore, the demand of peritoneal dialysis patients was not met because of intravenous administration.
Evocalcet (KHK7580), a new calcimimetic agent, is developed to resolve the issues of the upper gastrointestinal adverse reactions,13,21 drug interactions,22 and low bioavailability observed with cinacalcet while retaining its efficacy on PTH reduction and improvement of SHPT.21 In peritoneal dialysis patients, oral administration is preferred. Evocalcet was subsequently approved in Japan in 2018 for the treatment of hemodialysis and peritoneal dialysis patients with SHPT.13 A phase IIb trial showed that evocalcet decreased the intact PTH levels by −8.40%, −10.56%, and −20.16% at doses of 0.5, 1, and 2 mg once daily for 3 weeks with adverse reaction profiles similar to cinacalcet.23 A large randomized controlled trial found that in East Asian patients on haemodialysis with SHPT, the mean percentage change in intact PTH from baseline at 52 weeks was −34.7% and −30.2% in the evocalcet and cinacalcet groups, respectively. Evocalcet was shown to be non-inferior to cinacalcet.24 In addition, no major safety concerns were observed in evocalcet group, and gastrointestinal adverse events (AEs) were significantly less frequent in the evocalcet group than in the cinacalcet group (33.5% vs 50.5%, P=0.001).24 This suggests that evocalcet has good efficacy and a manageable safety profile for patients with SHPT.
The pharmacokinetics (PK) and pharmacodynamics (PD) of evocalcet have only been investigated in healthy Japanese subjects. The maximum plasma concentrations (Cmax) of evocalcet were reached within 1.5–2 h. The elimination half-life (t1/2) was 12.98–19.77 h. Evocalcet decreased intact PTH and corrected Ca levels in a dose-proportional manner.25 The PK and PD of evocalcet have not been investigated in healthy Chinese individuals, and China has a huge dialysis population and a heavy burden of end-stage renal disease.26,27 Therefore, this was the first study to evaluate the PK, PD and safety of evocalcet in a healthy Chinese population, and to provide support for further research of evocalcet in China.
Methods
Study Design and Population
This open-label phase I trial was conducted between December 2019 and June 2021 at Beijing Hospital, Beijing, People’s Republic of China. The study was approved by the Ethics Committee of Beijing Hospital. All subjects provided written informed consent. The trial was registered on Clinicaltrials.gov (NCT04206657) and Chinadrugtrials.org.cn (CTR20192259).
Chinese healthy volunteers between 20 and 40 years of age with a body mass index (BMI) between 18.5 and 25.0 kg/m2 were enrolled. Subjects with clinically significant abnormality in the crystalline lens, digestive system disorder, or electrocardiogram (ECG) waveform shape unfit for QT interval measurement were excluded. The complete inclusion and exclusion criteria are detailed in the Supplementary Material.
This study consisted of single- and multiple-dose administration cohorts. The number of subjects in this study complied with the principle of the National Medical Products Administration (NMPA) in China that issued the “Technical Guidelines for Clinical Pharmacokinetic Research of Chemical Drugs”, which generally requires 8–12 subjects per dose group. Hence, a total of 42 subjects, eight each in the four single-dose cohorts and 10 subjects in the multiple-dose cohort, were recruited. The study started with the single-dose administration cohorts (1, 3, 6, and 12 mg evocalcet in the fasting state for 10 h or more, step-by-step administration from the lowest dose) and proceeded to the multiple-dose administration cohort (6 mg evocalcet within 30 min after meal once daily for eight days). Subjects in the single-dose administration cohort were hospitalized on day −2 and discharged on day 4 (three days after administration), while subjects in the multiple-dose administration cohort were hospitalized on day −2 and discharged on day 12 (four days after the final administration). The use of nicotine-containing anti-smoking treatment was prohibited. During hospitalization, caffeine- and alcohol-containing beverages were also prohibited.
Endpoints and Assessments
The primary endpoint was the PK evaluation, including the plasma evocalcet concentration and PK parameters. PK parameters for evocalcet were estimated by noncompartmental methods using actual elapsed time from the start of the respective dose administration. In the single-dose administration cohorts, blood samples were collected before the administration of evocalcet (0 h) and at 0.25, 0.5, 1, 2, 3, 4, 6, 8, 12, 24, 36, 48, and 72 h after administration.
In the multiple-dose administration cohort, blood samples were collected before the administration of evocalcet (0 h) and at 0.25, 0.5, 1, 2, 3, 4, 8, and 12 h after administration on day 1; just before administration on days 2–7; and before the administration of evocalcet (0 h) and at 0.25, 0.5, 1, 2, 3, 4, 8, 12, 24 (day 9), 48 (day 10), 72 (day 11), and 96 (day 12) h after administration on day 8.
Plasma evocalcet concentrations were measured using a validated liquid chromatography-tandem mass spectrometry method.25 The PK parameters were estimated using Phoenix® WinNonlin Version 8.3. The reported PK parameters included area under the concentration-time curve from zero to time of 24 hours (AUC0-24), area under the concentration-time curve from zero to infinity (AUC0-inf), and area under the concentration-time curve from zero to time t (AUC0-t) for only the single-dose cohorts; area under the concentration-time curve from zero during a dosing interval (AUC0-tau), predose observed drug concentration (Ctrough), accumulation ratio for AUC0-24 (Robs, AUC0-24), accumulation ratio for maximum plasma concentration (Robs, Cmax), and accumulation ratio for Ctrough (Robs, Ctrough) for only the multiple-dose cohort, percentage of AUC0-inf obtained by extrapolation (AUCextra), apparent systemic clearance after extravascular dosing (CL/F), Cmax, apparent terminal rate constant (kel or λz), terminal elimination half-life (t1/2), time of maximum concentration (tmax), and apparent volume of distribution (Vz/F) for all cohorts.
PD parameters and safety profiles were assessed as the secondary endpoint. Peripheral PD, including intact PTH, serum corrected Ca, serum P, and calcitonin, were measured. When the serum albumin (Alb) level was <4.0 g/dL, the serum Ca level would be corrected according to the following formula. Corrected serum Ca level (mg/dL) = Observed serum Ca level (mg/dL) + 4 − serum Alb level (g/dL). Urine PD included Ca, P, magnesium (Mg), sodium (Na), potassium (K), chloride (Cl), uric acid (UA), and urine creatinine concentration (UCr). Urine was pooled from 24 h before the administration of evocalcet and at 0–4, 4–8, 8–12, 12–24, 24–48, and 48–72 h in single-dose administration cohorts. In the multiple-dose administration cohort, urine was pooled from 24 h before the first dosing of evocalcet and on day 1 (0–4, 4–8, 8–12, 12–24 hours after the first dosing), day 8, and thereafter (0–4, 4–8, 8–12, 12–24, 24–48, 48–72, 72–96 hours after the last dosing).
UCr correction was performed using the following formula for each examination period.
For Ca, P, Mg, and UA, the following formula was used.
Urine creatinine-corrected [mg/gCre] = 1000 × Laboratory [mg/dL]/Urine creatinine [mg/dL]
For Na, K, and Cl, the following formula was used.
Urine creatinine-corrected [mEq/gCre] = 1000 × Laboratory [mEq/L]/(10 × Urine creatinine [mg/dL])
Safety was evaluated according to AEs, laboratory tests, vital signs, ECG, and ophthalmologic examination. Treatment-emergent AEs (TEAEs), which were defined as any untoward medical occurrence in a subject that occurred after study drug administration, were monitored over the entire study period and classified using the Medical Dictionary for Regulatory Activities version 24.0 or higher.
Statistical Analysis
All statistical analyses were conducted using SAS 9.4 (SAS Institute, Inc., Cary, NC, USA). Categorical data were summarized using frequencies and percentages, and continuous data were summarized using descriptive statistics consisting of mean ± standard deviation (SD) and median (minimum, maximum).
For the PK parameters, coefficients of variation (CV%) and geometric mean values were calculated in addition to the number of subjects, mean ± SD, and median (minimum, maximum). The linearity of PK assessment for evocalcet single-dose administration cohorts was evaluated by plotting the PK exposure parameters (Cmax and AUC0-inf) on the y-axis against the dose on the x-axis. Linear regression lines were also presented in the same chart, based on the model: log (parameter) = a + b * log (dose), where “a” was the intercept and “b” was the slope. Descriptive statistics were used to summarize the results for PD and safety.
Results
Demographics and Baseline Characteristics
Eight subjects each in the single-dose cohorts and 10 subjects in the multiple-dose cohort (a total of 42 subjects) were enrolled. All enrolled subjects received at least one dose of the study drug. Two (4.8%) of the 42 subjects withdrew from the study, and both of them were in the multiple-dose cohort. One subject was withdrawn due to TEAE by the investigator’s decision on day 1, and the other subject withdrew due to personal reasons on day 1. Demographic parameters were generally balanced between each cohort, which are shown in Table 1. More male subjects than female subjects participated in this study. The subjects were 21–38 years of age, 92.9% were male, and the BMI was 18.6–25.3 kg/m2 (Table 1).
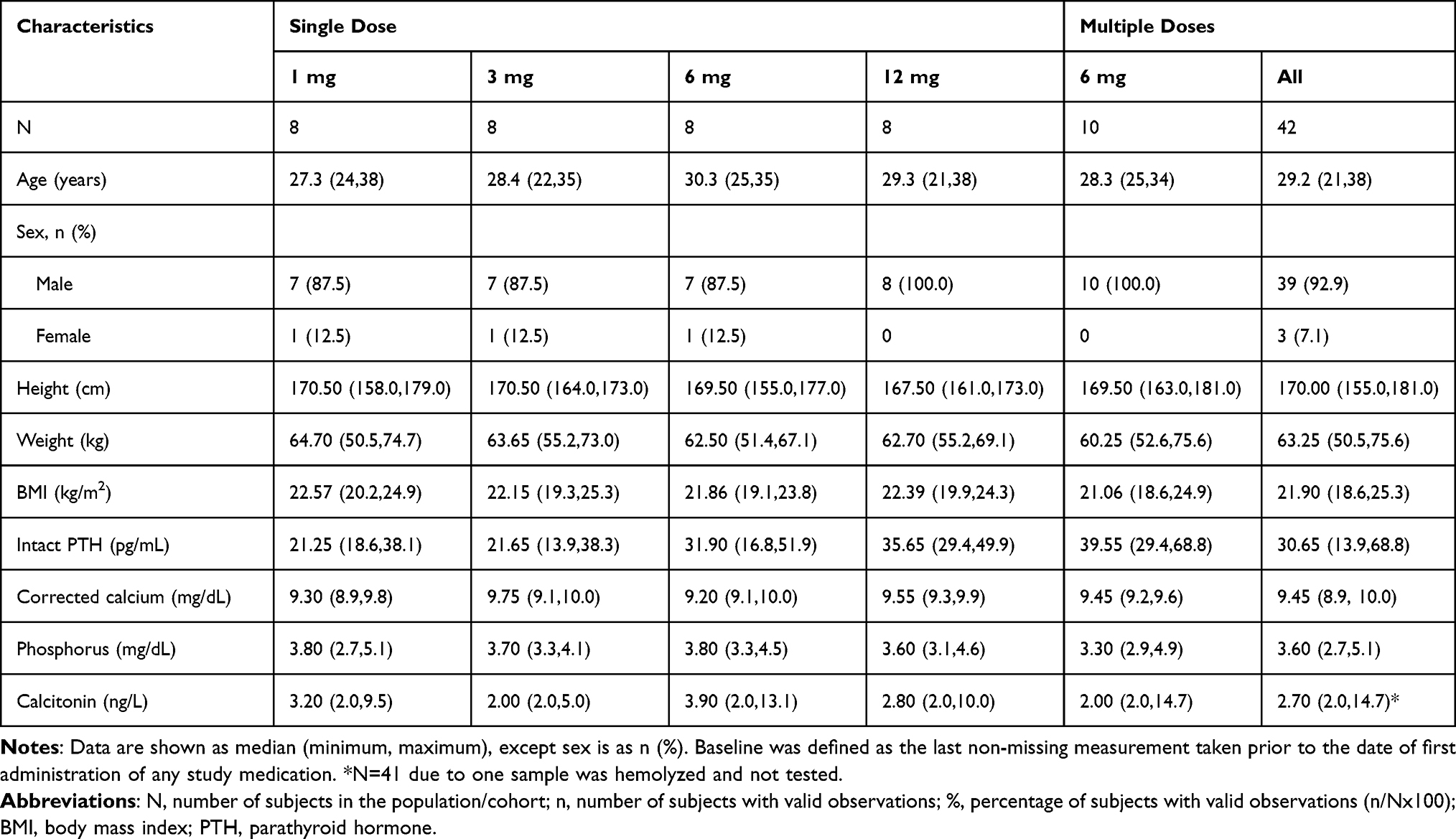 |
Table 1 Demographic and Baseline Characteristics of the Study Subjects |
Pharmacokinetics
In the single-dose study, plasma evocalcet concentrations reached tmax at 1.00–2.00 h (median) and declined biphasically. The geometric mean t1/2 was 15.99–20.84 h (Figure 1A and Table 2). In the multiple-dose study, the median tmax on days 1 and 8 were both 2.00 h. On day 8, the geometric mean t1/2, geometric mean Robs for Cmax, AUC0-24, and Ctrough were 15.59 h, 1.075, 1.102, and 1.126, respectively (Figure 1B and Table 2). In addition, Table 2, Figure 1C and D indicate a dose-proportional increase in evocalcet exposure over the dose range of 1 mg to 12 mg following single oral administration.
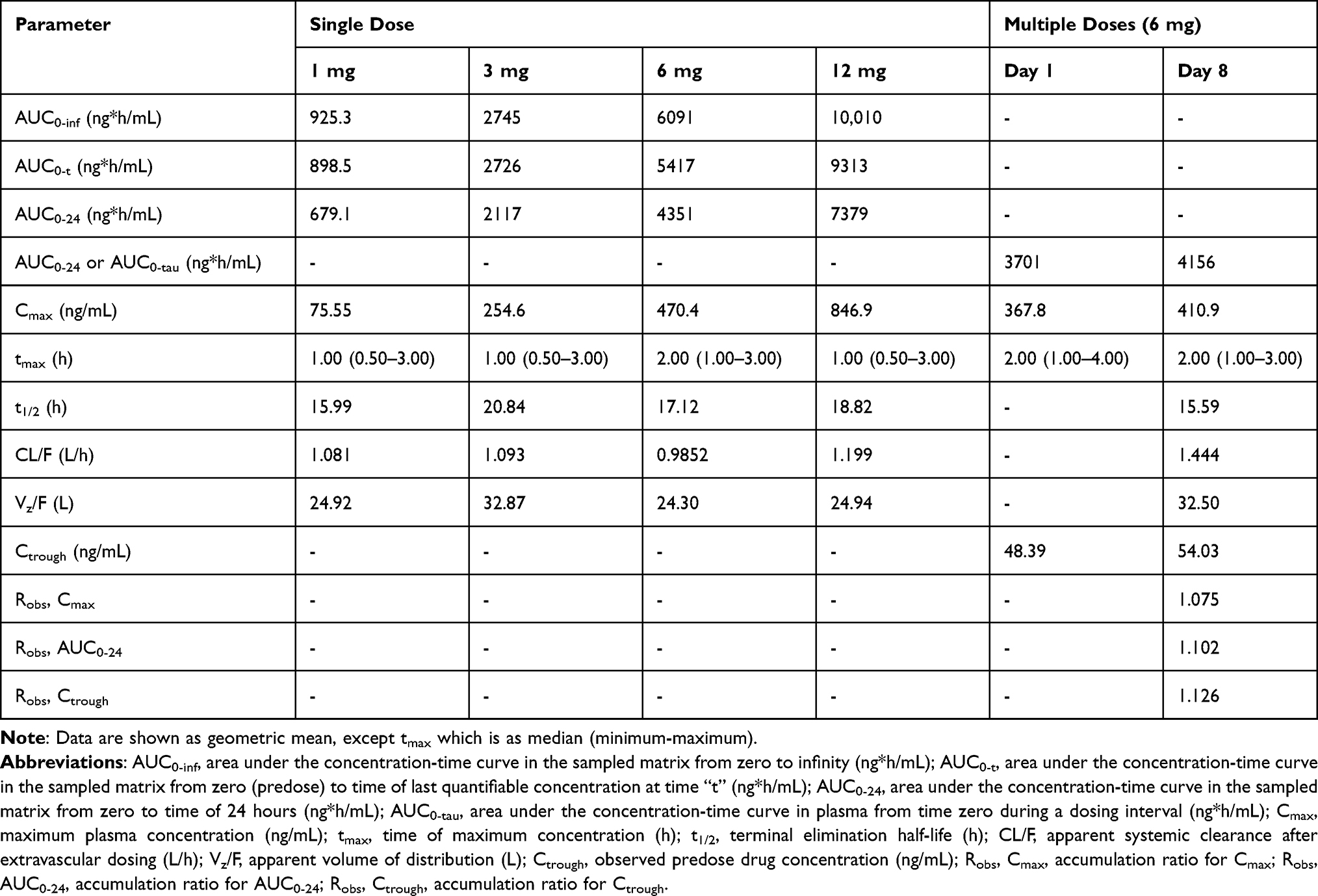 |
Table 2 Summary of Primary Pharmacokinetic Parameters for Plasma Evocalcet by Treatment in Chinese Healthy Volunteers (Pharmacokinetic Set) |
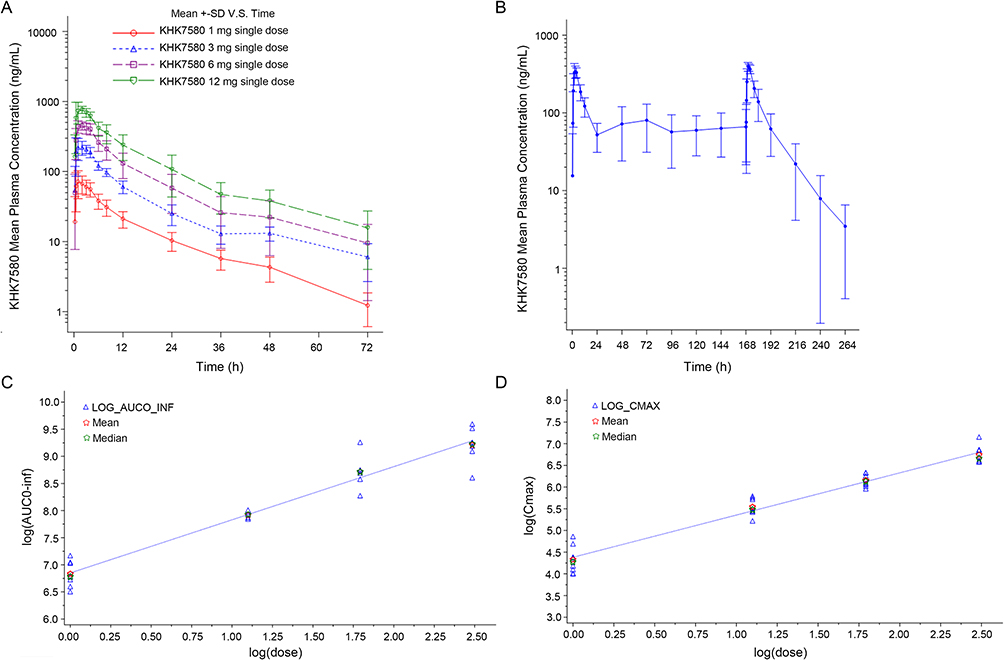 |
Figure 1 (A) Single Dose KHK7580 Plasma Concentration-Time Profiles (PKS); (B) Multiple Dose KHK7580 Plasma Concentration-Time Profiles (PKS); (C) Dose-proportional increase in evocalcet exposure (AUC0-inf) over the dose range of 1 mg to 12 mg following single oral administration; (D) Dose-proportional increase in evocalcet exposure (Cmax) over the dose range of 1 mg to 12 mg following single oral administration. Data in (A and B) are presented as mean ± standard deviation. Data in (C and D) are presented as individual, mean, and median. |
Pharmacodynamic
Intact PTH
In the single-dose cohorts, the intact PTH levels started to decrease at 0.5 h after evocalcet administration and reached a nadir within 0.5–2 h after administration in different dose cohorts. The intact PTH levels remained decreased longer with an increasing dose of evocalcet. The intact PTH levels were restored 24 h after evocalcet administration (Figure 2A). For the multiple-dose cohort, the intact PTH levels temporarily decreased after administration of evocalcet on days 1 and 8 and returned to similar levels to but slightly lower than the baseline levels on days 2 (before dosing) and 9 (24 h after the last dosing). The maximum decrease after administration of evocalcet on day 1 was similar to that on day 8 (Figure 2B).
 |
Figure 2 (A) Percentage change from baseline in intact parathyroid hormone (PTH) levels in single-dose cohorts; (B) Percentage change from baseline in intact PTH levels in multiple-dose cohort. |
Corrected Ca
In the single-dose cohorts, the corrected serum Ca levels decreased after administration of evocalcet and reached a nadir at 12–24 h after administration, and the decrement was dose-dependent with the increasing dose of evocalcet. The corrected serum Ca levels returned to baseline on day 3 (Figure 3A). In the multiple-dose cohort, corrected serum Ca levels decreased throughout the dosing period after initiation of evocalcet administration and returned to the baseline levels on three to four days (day 11 and day 12) after the last dosing on day 8. The maximum decrease observed between day 1 (two hours after the first dosing) and day 2 (before dosing) and that between day 8 (two hours after the last dosing) and day 9 (24 hours after the last dosing) was −7.33% (at 12 hours after day 1 dosing) and −15.27% (at eight hours after day 8 dosing), respectively, indicating a higher maximum decrease between days 8 and 9 than between days 1 and 2 (Figure 3B).
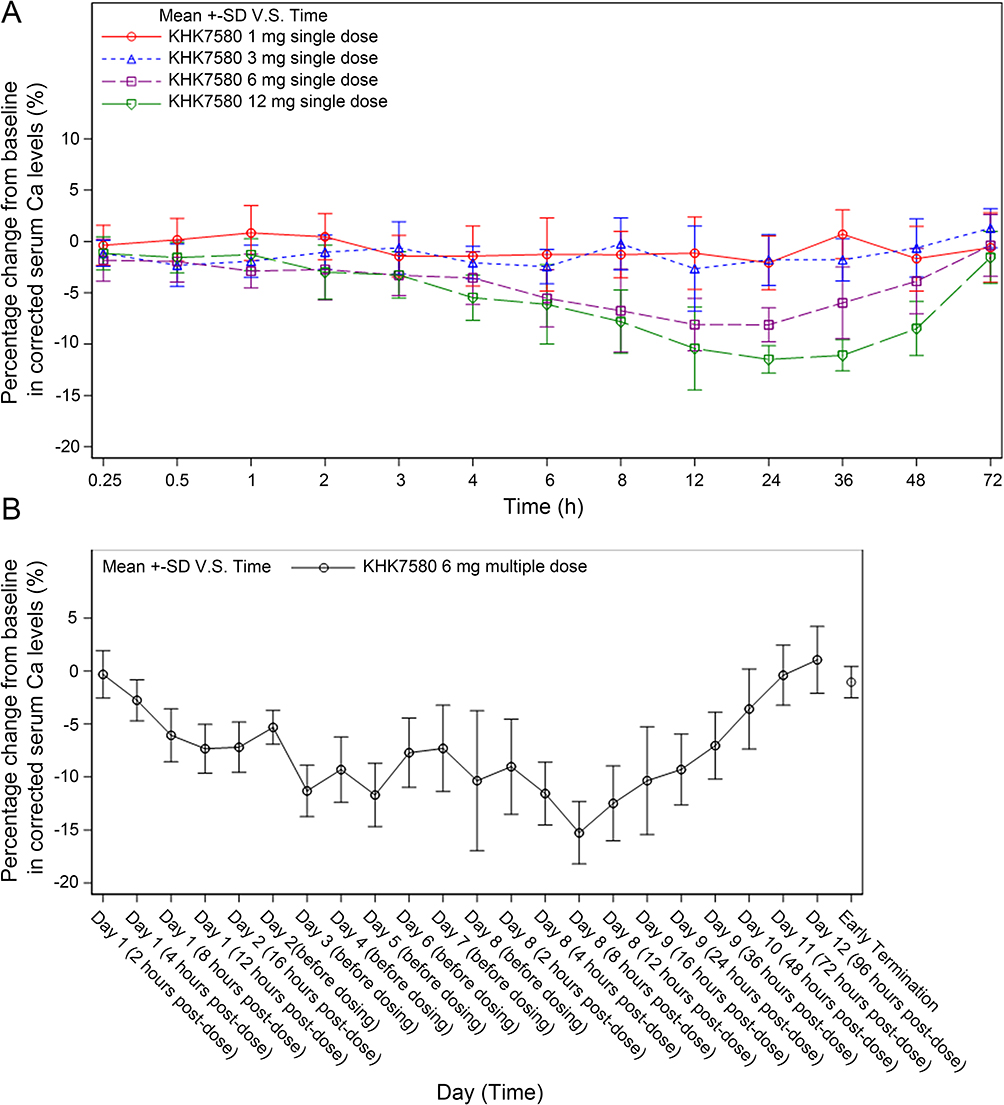 |
Figure 3 (A) Percentage change from baseline in corrected calcium (Ca) levels in the single-dose cohorts; (B) Percentage change from baseline in corrected Ca levels in the multiple-dose cohort. |
P
In the single-dose cohorts, serum P levels decreased during the first 6 h after study drug administration, started to increase at 8 h, and peaked at 12 h. The percentage changes from baseline at 12 and 24 h showed a dose-dependent manner, except in the 3- and 6-mg single-dose cohorts, where P levels were similar (Figure 4A). In the multiple-dose cohort, on days 1 (2 h after the first dosing) and 8 (2 h after the last dosing), serum P levels temporarily decreased after administration of the study drug. At 4 h after evocalcet administration on days 1 and 8, the values returned to the levels before dosing (Figure 4B).
 |
Figure 4 (A) Percentage change from baseline in serum phosphorus (P) levels in the single-dose cohorts; (B) Percentage change from baseline in serum P levels in the multiple-dose cohort. |
Calcitonin
In the single-dose cohorts, calcitonin levels increased dose-dependently from 0.5 h after administration of evocalcet. The increments were transient as the calcitonin levels reversed back to baseline at 8 h after evocalcet administration (Figure 5A). In the multiple-dose cohort, calcitonin levels transiently increased after administration of the study drug on days 1 and 8 and returned to the baseline levels on days 1 and 8 (8 h post administration). When the calcitonin levels were measured before administration between days 2 and 7, no marked changes in calcitonin levels were observed (Figure 5B).
 |
Figure 5 (A) Percentage change from baseline in calcitonin levels in the single-dose cohorts; (B) Percentage change from baseline in calcitonin levels in the multiple-dose cohort. |
Urine PD
In the single-dose cohorts, creatinine-corrected urinary Ca excretion increased dose-dependently from 0–4 h to 8–12 h after evocalcet administration and returned to baseline levels at 12–24 h (Figure S1A). The creatinine-corrected urinary P excretion decreased dose-dependently at 4–8 h after evocalcet administration and returned to near baseline levels at 12–24 h for most cohorts (Figure S1B). The creatinine-corrected urinary excretions of Mg, Na, K, and Cl transiently increased at different periods after evocalcet administration (Figure S1C-F). For all dose cohorts, urine UA (creatinine-corrected) decreased at 0 to 4 hours and met nadir at 12 to 24 hours after evocalcet administration. However, urine UA level was increased at 24 to 48 hours after administration, and the changes showed the same trend in different evocalcet cohorts (Figure S1G). The changes were dose-dependent for urine Mg excretion.
In the multiple-dose cohort, creatinine-corrected urinary Ca excretion transiently increased after administration of evocalcet both on days 1 and 8; it reached a maximum at 4–8 h after evocalcet administration and then decreased to levels below the baseline. The maximum percentage increase was higher on day 1 after the evocalcet administration than on day 8 (Figure S2A). The creatinine-corrected urinary P excretion decreased by over 50% from baseline after administration of evocalcet on day 1 up to 8–12 h after administration. Urinary P excretion also decreased after administration of evocalcet on day 8, but the decrease on day 8 was smaller than on day 1. After the last dosing on day 8, the urine P levels returned to baseline at 24–48 h after administration (Figure S2B). The creatinine-corrected urinary excretions of Mg, Na, K, and Cl transiently increased after the administration of evocalcet on day 1 (Figure S2C-F). Urine UA (creatinine-corrected) decreased after the study drug administration (Figure S2G).
Safety
Seventeen (40.5%) subjects reported TEAEs during the study period, with two (25.0%) subjects each in the 1- and 6-mg single-dose cohorts, three (37.5%) subjects in the 3-mg single-dose cohort, and all 10 (100.0%) subjects in the multiple-dose cohort (Table 3). Study drug-related TEAEs were reported by two (25.0%) subjects each in the 1-, 3-, and 6-mg single-dose cohorts and all 10 (100.0%) subjects in the multiple-dose cohort. No serious or severe TEAE was reported in the study. No subjects in this study suffered from tetany.
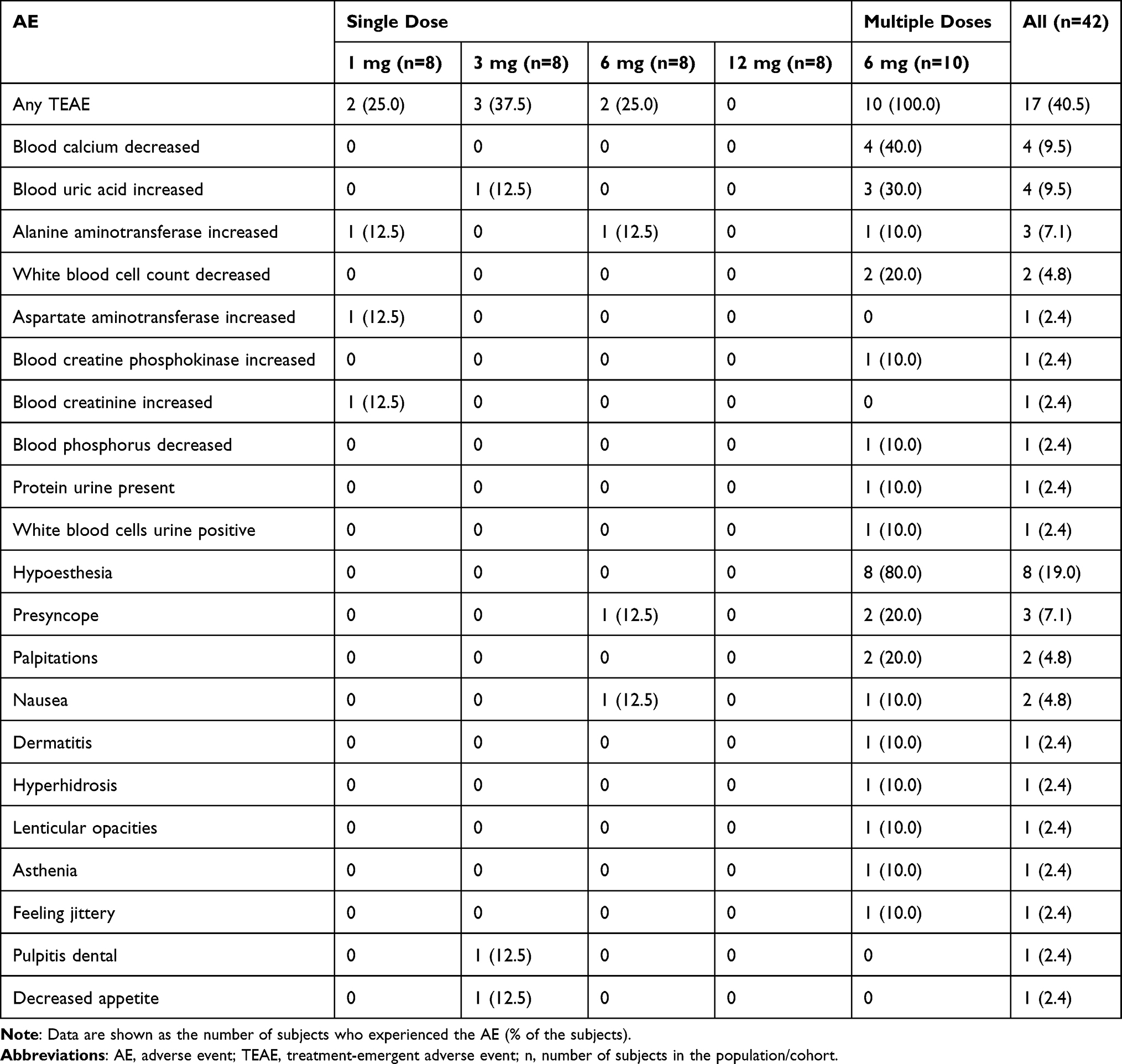 |
Table 3 Number (Percentage) of Treatment-Emergent Adverse Events in Chinese Healthy Subjects (Safety Set) |
In the multiple-dose cohort, one subject reported study drug-related TEAEs leading to study drug withdrawal. Hypoesthesia (reported by eight subjects, 19.0%), blood Ca decreased, and blood UA increased (each reported by four subjects, 9.5%) were the common TEAEs, which were considered related to the study drug. Lenticular opacity was reported in one (2.4%) subject and was considered possibly related to evocalcet, but the TEAE was mild and recovered with no action taken. All study drug-related TEAEs were mild to moderate.
Nausea was reported in two (4.8%) subjects each in the 6-mg single-dose cohort and in the multiple-dose cohort, which was considered possibly related to evocalcet. One subject (No. 05–49) in the multiple-dose cohort experienced TEAEs of nausea, asthenia, and hypoesthesia, leading to discontinuation of the study drug, but all these TEAEs were moderate in severity. Nausea was reported on day 2 of the study and resolved on the same day without corrective treatment. A low incidence of gastrointestinal adverse events was observed.
There were hematology and blood chemistry parameters found to show abnormalities at post-baseline assessments. However, no particular relationship between these laboratory abnormalities (except the PD parameters) and the treatment dose of evocalcet was reported. No clinically meaningful changes in mean value were observed in other laboratory parameters. There were no clinically significant changes noted in vital signs, physical examinations, or ECG after administration of the study drug.
Discussion
Evocalcet is a new calcimimetic agent with comparable efficacy in reducing intact PTH levels and fewer gastrointestinal adverse reactions than cinacalcet hydrochloride.21 With the above advantages, evocalcet was approved in Japan in 2018 for the treatment of SHPT in patients with CKD on maintenance dialysis.28 However, it remains unknown whether the evocalcet is applicable to people outside Japan. The present study was the first to evaluate the PK, PD, and safety of evocalcet in healthy Chinese subjects. We found that evocalcet exhibited dose-dependent PK properties in healthy Chinese volunteers at a single dose of 1–12 mg and multiple doses of 6 mg once daily for eight days. The PD analysis suggested that evocalcet reduced intact PTH and corrected serum calcium levels in a dose-dependent manner. In addition, all TEAEs or study drug-related TEAEs were mild to moderate, and evocalcet has a manageable safety profile.
After a single dose of 1–12 mg evocalcet in healthy Chinese subjects under fasting conditions, the drug concentrations and PK parameters such as Cmax and AUC increased proportionally with the dose escalation. Following the once-daily oral administration of 6 mg evocalcet for eight days, the mean plasma evocalcet concentration-time profiles on day 8 were similar to those on day 1. The Robs for Cmax, AUC0-24, and Ctrough were 1.075, 1.102, and 1.126, respectively, indicating negligible evocalcet accumulation upon multiple dosing. Ctrough levels were similar across days, which suggested that a steady state was achieved as early as day 2. In addition, the PK parameters in the present study were almost consistent with previous results from a similar study conducted in healthy Japanese subjects administered evocalcet.25 Indeed, using a single dose (1–20 mg), the previous Japanese study reported a tmax attained in 1.5–2h, a t1/2 of 12.98–19.77 h, and dose-dependent Cmax and AUC. Using multiple doses of 6 mg, the tmax was 4.0 h, the Cmax was 394 ng/mL, the AUC0-24 was 3860 ng•h/mL, and the Ctrough on day 8 was 51.1 ng/mL.25 Those results are generally consistent with those of the present study.
The general PD data in the present study also appeared to be similar to those of the Japanese study.25 The effect of evocalcet on plasma intact PTH and Ca levels was dose- and exposure-dependent, with the maximum effect observed around the time of peak exposure, as observed with evocalcet in Japanese subjects25 and with cinacalcet hydrochloride.29 The rapid effect of increased calcitonin resulted in the transient decrement of serum P. However, following the decreased PTH, urine P kept decreasing, which resulted in a relatively sustained increment of serum P during the dose administration in healthy volunteers.
Overall, the results from this study demonstrated the safety and tolerability of oral doses of evocalcet, from 1 mg to 12 mg as a single dose and 6 mg multiple doses once daily for eight days, and evocalcet did not trigger new safety issues in healthy Chinese subjects. Although TEAEs occurred in 40.5% of the subjects in this study, no serious or severe TEAEs were reported, and most TEAEs were manageable and recovered without any action taken. In addition, although all 10 subjects in the multi-dose dosing cohort developed TEAEs, all TEAEs were mild to moderate. No subjects suffered from tetany. The phase I trial in Japan reported three AEs in a higher dose range, including one moderate tetany in a subject (17%) of the 12 mg multiple dose evocalcet group,25 and gastrointestinal disorder in two subjects (33%) in the 20 mg group.25 In the present study, decreased blood Ca was observed in four subjects (9.5%). In addition, hypoesthesia, reported by eight subjects (19.0%), was also considered as Ca decrease-related. However, the changes in serum Ca are similar to the Japanese single- and multiple-dose cohorts, and ECG abnormalities, which can be caused by low Ca levels, have not been observed in the present study. Lenticular opacity was reported in one subject in the 6 mg multiple-dose cohort. This mild TEAE was observed on day 12 and later recovered on day 42 without action taken, and this subject experienced mild decreased blood Ca during the study. Hypocalcemia can cause or worsen cataracts.30–33 Therefore, there is a theoretical risk that calcimimetic agents could cause cataracts.34,35 Even though lenticular opacity is known as a class effect, it is known to occur due to long-lasting hypocalcemic conditions for about 6–12 months.30 In the present study, the patient with incident lens opacity had mild and short term hypocalcemia, and lens opacity resolved by itself after discontinuing the evocalcet. Therefore, the correlation between lens opacity and evocalcet could not be completely excluded, and the occurrence of lens opacity should be monitored in future clinical practice.
Of note, the present Phase 1 study was conducted in healthy Chinese subjects with normal serum calcium and intact PTH levels, which were very different from maintenance dialysis patients with hypercalcaemia and SHPT. A recent randomized, double-blind, international multi-center study compared the safety of evocalcet (n=203) versus cinacalcet (n=200) for 52 weeks in East Asian patients on hemodialysis with SHPT.24 The above study found that no major safety concerns were observed in patients using evocalcet, and the incidence of gastrointestinal AEs was significantly lower with evocalcet than with cinacalcet (33.5% vs 50.5%, P=0.001). Our study showed that only 4.8% of subjects experienced nausea. A study of evocalcet in 66 healthy Japanese subjects also showed that there was no clear difference in the incidence of nausea between single-dose fasting groups and multiple-dose post-meal groups. No nausea occurred in the 6 mg and 12 mg multiple-dose groups, and no nausea occurred at the same doses in the single-dose groups.25 In addition, the incidence of nausea in this study was lower than that of cinacalcet (7.1%) observed in PK study in Chinese healthy volunteers.29 This indicates that evocalcet has good efficacy and a manageable safety profile in healthy subjects or patients with SHPT, especially in terms of reducing gastrointestinal AEs.
The mechanism underlying how calcimimetic agents induce gastrointestinal side effects remains unclear. It was reported that cinacalcet directly stimulated the afferent vagus nerve of the gastrointestinal tract. It was suspected that cinacalcet activated the Ca receptor expressed in the gastrointestinal tract without an elevation in its serum concentration, as the increase in afferent action potentials occurred early after the administration.36 The pharmacological effects of evocalcet were observed at lower doses because of its higher bioavailability (62.7%) compared with cinacalcet (5–30%),13 which might have contributed to the reduced gastrointestinal tract symptoms, since only a small amount of evocalcet is exposed in the stomach with the dose administered. Additionally, it has been reported that evocalcet has less effect on gastric emptying compared to cinacalcet. The rapid disappearance of evocalcet from the digestive tract also might lead to limited stimulation of vagal nerves.22
This study had several limitations that should be considered. Even though a small number of subjects per treatment group are generally acceptable for phase I trials, the sample size of the present study was relatively small. Furthermore, the present study was limited by only one dose level in the multiple-dose study. Finally, no placebo arm was included in the study.
Conclusion
In conclusion, this was the first study to assess the PK, PD, and safety of evocalcet following single ascending doses and multiple doses in healthy Chinese subjects. Evocalcet demonstrated dose-dependent PK and PD properties and was well-tolerated after administration of a single oral dose of up to 12 mg and multiple doses of 6 mg once daily for eight days. These results suggest that evocalcet may have good efficacy and a manageable safety profile, and future studies with larger sample sizes and longer follow-up are needed to confirm these findings in patients with SHPT.
Data Sharing Statement
The original contributions presented in the study are included in the article and Supplementary Material, and further inquiries can be directed to the corresponding author. All data will be de-identified before sharing with a third party.
Ethics Approval
The study was approved by the Ethics Committee of Beijing Hospital. All subjects provided written informed consent. This study was conducted in accordance with consensus ethics principles derived from international ethics guidelines, including the Declaration of Helsinki and the International Council for Harmonisation guidelines for Good Clinical Practice, as well as all applicable laws, rules, and regulations.
Acknowledgments
The authors thank all the study investigators, study staff, and healthy subjects for their efforts and contributions. We thank Kyowa Kirin Co., Ltd for providing medical writing support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was initiated and funded by Kyowa Kirin Co., Ltd. Medical writing support was funded by Kyowa Kirin Co., Ltd.
Disclosure
Kazuya Narushima, Masahiro Kojima, and Chisato Nagai are employees of Kyowa Kirin Co., Ltd. Kexin Li and Xuemei He declared that they had no conflicts of interest in this work.
References
1. Cannata-Andia JB, Martin-Carro B, Martin-Virgala J, et al. Chronic Kidney Disease-Mineral and Bone Disorders: pathogenesis and Management. Calcif Tissue Int. 2021;108(4):410–422. doi:10.1007/s00223-020-00777-1
2. Moe S, Drueke T, Cunningham J, et al. Definition, evaluation, and classification of renal osteodystrophy: a position statement from Kidney Disease: improving Global Outcomes (KDIGO). Kidney Int. 2006;69(11):1945–1953. doi:10.1038/sj.ki.5000414
3. Cozzolino M, Shilov E, Li Z, et al. Pattern of Laboratory Parameters and Management of Secondary Hyperparathyroidism in Countries of Europe, Asia, the Middle East, and North America. Adv Ther. 2020;37(6):2748–2762. doi:10.1007/s12325-020-01359-1
4. Hedgeman E, Lipworth L, Lowe K, et al. International burden of chronic kidney disease and secondary hyperparathyroidism: a systematic review of the literature and available data. Int J Nephrol. 2015;2015:184321. doi:10.1155/2015/184321
5. Cunningham J, Locatelli F, Rodriguez M. Secondary hyperparathyroidism: pathogenesis, disease progression, and therapeutic options. Clin J Am Soc Nephrol. 2011;6(4):913–921. doi:10.2215/CJN.06040710
6. Cianciolo G, Capelli I, Cappuccilli M, et al. Calcifying circulating cells: an uncharted area in the setting of vascular calcification in CKD patients. Clin Kidney J. 2016;9(2):280–286. doi:10.1093/ckj/sfv145
7. Wang J, Bieber BA, Hou FF, Port FK, Anand S. Mineral and bone disorder and management in the China Dialysis Outcomes and Practice Patterns Study. Chin Med J (Engl). 2019;132(23):2775–2782. doi:10.1097/CM9.0000000000000533
8. Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Update Work Group. KDIGO 2017 Clinical Practice Guideline Update for the Diagnosis, Evaluation, Prevention, and Treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). Kidney Int Suppl. 2017;7:1–59. doi:10.1016/j.kisu.2017.04.001
9. Evenepoel P. Calcimimetics in chronic kidney disease: evidence, opportunities and challenges. Kidney Int. 2008;74(3):265–275. doi:10.1038/ki.2008.166
10. Drueke TB. Calcimimetics and outcomes in CKD. Kidney Int Suppl. 2013;3(5):431–435. doi:10.1038/kisup.2013.90
11. Pereira L, Meng C, Marques D, Frazao JM. Old and new calcimimetics for treatment of secondary hyperparathyroidism: impact on biochemical and relevant clinical outcomes. Clin Kidney J. 2018;11(1):80–88. doi:10.1093/ckj/sfx125
12. Martin KJ, Pickthorn K, Huang S, et al. AMG 416 (velcalcetide) is a novel peptide for the treatment of secondary hyperparathyroidism in a single-dose study in hemodialysis patients. Kidney Int. 2014;85(1):191–197. doi:10.1038/ki.2013.289
13. Akizawa T, Ikejiri K, Kondo Y, Endo Y, Fukagawa M. Evocalcet: a New Oral Calcimimetic for Dialysis Patients With Secondary Hyperparathyroidism. Ther Apher Dial. 2020;24(3):248–257. doi:10.1111/1744-9987.13434
14. Investigators ET, Chertow GM, Block GA, et al. Effect of cinacalcet on cardiovascular disease in patients undergoing dialysis. N Engl J Med. 2012;367(26):2482–2494. doi:10.1056/NEJMoa1205624.
15. Padhi D, Harris R. Clinical pharmacokinetic and pharmacodynamic profile of cinacalcet hydrochloride. Clin Pharmacokinet. 2009;48(5):303–311. doi:10.2165/00003088-200948050-00002
16. Harris RZ, Salfi M, Sullivan JT, Padhi D. Pharmacokinetics of cinacalcet hydrochloride when administered with ketoconazole. Clin Pharmacokinet. 2007;46(6):495–501. doi:10.2165/00003088-200746060-00003
17. Kumar GN, Sproul C, Poppe L, et al. Metabolism and disposition of calcimimetic agent cinacalcet HCl in humans and animal models. Drug Metab Dispos. 2004;32(12):1491–1500. doi:10.1124/dmd.104.000604
18. Rodriguez-Ortiz ME, Rodriguez M. Recent advances in understanding and managing secondary hyperparathyroidism in chronic kidney disease. F1000Res. 2020;9:1077. doi:10.12688/f1000research.22636.1
19. Block GA, Bushinsky DA, Cheng S, et al. Effect of Etelcalcetide vs Cinacalcet on Serum Parathyroid Hormone in Patients Receiving Hemodialysis With Secondary Hyperparathyroidism: a Randomized Clinical Trial. JAMA. 2017;317(2):156–164. doi:10.1001/jama.2016.19468
20. Nemeth EF, Van Wagenen BC, Balandrin MF. Discovery and Development of Calcimimetic and Calcilytic Compounds. Prog Med Chem. 2018;57(1):1–86. doi:10.1016/bs.pmch.2017.12.001.
21. Fukagawa M, Shimazaki R, Akizawa T. Evocalcet study g. Head-to-head comparison of the new calcimimetic agent evocalcet with cinacalcet in Japanese hemodialysis patients with secondary hyperparathyroidism. Kidney Int. 2018;94(4):818–825. doi:10.1016/j.kint.2018.05.013
22. Kawata T, Tokunaga S, Murai M, et al. A novel calcimimetic agent, evocalcet (MT-4580/KHK7580), suppresses the parathyroid cell function with little effect on the gastrointestinal tract or CYP isozymes in vivo and in vitro. PLoS One. 2018;13(4):e0195316. doi:10.1371/journal.pone.0195316
23. Akizawa T, Shimazaki R, Fukagawa M, Evocalcet Study G. Phase 2b study of evocalcet (KHK7580), a novel calcimimetic, in Japanese patients with secondary hyperparathyroidism undergoing hemodialysis: a randomized, double-blind, placebo-controlled, dose-finding study. PLoS One. 2018;13(10):e0204896. doi:10.1371/journal.pone.0204896
24. Ni Z, Liang X, Wu CC, et al. Comparison of the Oral Calcimimetics Evocalcet and Cinacalcet in East Asian Patients on Hemodialysis with Secondary Hyperparathyroidism. Kidney Int Rep. 2023;8(11):2294–2306. doi:10.1016/j.ekir.2023.08.034
25. Akizawa T, Shimazaki R, Shiramoto M, Fukagawa M. Pharmacokinetics, Pharmacodynamics, and Safety of the Novel Calcimimetic Agent Evocalcet in Healthy Japanese Subjects: first-in-Human Phase I Study. Clin Drug Investig. 2018;38(10):945–954. doi:10.1007/s40261-018-0687-4
26. Zuo L, Wang M. Chinese Association of Blood Purification Management of Chinese Hospital A. Current burden and probable increasing incidence of ESRD in China. Clin Nephrol. 2010;74(Suppl 1):S20–22.
27. Zhang L, Zuo L. Current burden of end-stage kidney disease and its future trend in China. Clin Nephrol. 2016;86(13):27–28. doi:10.5414/CNP86S104
28. Hamano N, Endo Y, Kawata T, Fukagawa M. Development of evocalcet for unmet needs among calcimimetic agents. Expert Rev Endocrinol Metab. 2020;15(5):299–310. doi:10.1080/17446651.2020.1780911
29. Liu H, Wang H, Liu T, et al. Pharmacokinetic and Pharmacodynamic Properties of Cinacalcet (KRN1493) in Chinese Healthy Volunteers: a Randomized, Open-label, Single Ascending-dose and Multiple-dose, Parallel-group Study. Clin Ther. 2016;38(2):348–357. doi:10.1016/j.clinthera.2015.12.015
30. Berlyne GM, Ari JB, Danovitch GM, Blumenthal M. Cataracts of chronic renal failure. Lancet. 1972;1(7749):509–511. doi:10.1016/S0140-6736(72)90175-4
31. Zhang H, Yang L, Xie J, Zhao M, Liu X. Hypocalcemic cataract secondary to idiopathic hypoparathyroidism in an adolescent. J Int Med Res. 2023;51(8):3000605231193820. doi:10.1177/03000605231193820
32. Daba KT, Weldemichael DK, Mulugeta GA. Bilateral hypocalcemic cataract after total thyroidectomy in a young woman: case report. BMC Ophthalmol. 2019;19(1):233. doi:10.1186/s12886-019-1224-9
33. Jafari R, Kamali M, Rad MM. A new pattern of bilateral cataracts associated with hypocalcemia secondary to uncontrolled hypoparathyroidism. Oman J Ophthalmol. 2022;15(3):389–392. doi:10.4103/ojo.ojo_238_21
34. Hannan FM, Olesen MK, Thakker RV. Calcimimetic and calcilytic therapies for inherited disorders of the calcium-sensing receptor signalling pathway. Br J Pharmacol. 2018;175(21):4083–4094. doi:10.1111/bph.14086
35. Ward DT, Riccardi D. New concepts in calcium-sensing receptor pharmacology and signalling. Br J Pharmacol. 2012;165(1):35–48. doi:10.1111/j.1476-5381.2011.01511.x
36. Tokunaga S, Kawata T. The effect of evocalcet on vagus nerve activity of the gastrointestinal tract in miniature pigs. PLoS One. 2021;16(1):e0245785. doi:10.1371/journal.pone.0245785
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.