Back to Journals » Drug Design, Development and Therapy » Volume 12
Pharmacokinetics and tolerability of eletriptan hydrobromide in healthy Korean subjects
Authors Kim YK ![]() , Shin KH
, Shin KH ![]() , Alderman J, Yu KS
, Alderman J, Yu KS ![]() , Jang IJ
, Jang IJ ![]() , Lee S
, Lee S ![]()
Received 14 August 2017
Accepted for publication 27 December 2017
Published 19 February 2018 Volume 2018:12 Pages 331—337
DOI https://doi.org/10.2147/DDDT.S149119
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Yu Kyong Kim,1 Kwang-Hee Shin,2 Jeffrey Alderman,3 Kyung-Sang Yu,1 In-Jin Jang,1 SeungHwan Lee1
1Department of Clinical Pharmacology and Therapeutics, Seoul National University College of Medicine and Hospital, Seoul, Republic of Korea; 2College of Pharmacy, Kyungpook National University, Daegu, Republic of Korea; 3Pfizer, Inc., New York, NY, USA
Background: Migraine is one of the most common headache disorders that greatly affect the quality of life. Selective serotonin (5-HT) receptor agonists such as triptamine-based drugs called triptans are used for treatment of migraine.
Purpose: This study aimed to evaluate the pharmacokinetic (PK) and tolerability profiles of eletriptan hydrobromide (eletriptan HBr), a selective 5-hydroxytryptamine (also known as serotonin) 1B/1D receptor agonist, in Koreans and compare the results to those observed in non-Koreans in a previously published study.
Patients and methods: A randomized, open-label, single, and repeated-dose study was conducted in 16 healthy Korean male subjects using a four-treatment, four-period, and four-sequence crossover design (NCT01139515). The subjects received one of the following four treatments in each period: a single dose of 20, 40, 80 mg eletriptan HBr or a repeated oral dose of 40 mg 2 h apart. Blood samples were collected before and up to 26 h after dosing for quantification of plasma eletriptan concentration by high-performance liquid chromatography tandem–mass spectrometry. The PK parameters were estimated using noncompartmental methods. Ethnicity differences between Korean and non-Korean subjects were identified using geometric mean ratios and 90% confidence intervals (CIs) of dose-normalized maximum plasma concentration (Cmax) and dose-normalized area under the plasma concentration versus time curve from 0 h to the last measurable concentration (AUC0–t).
Results: After single-dose administration of eletriptan HBr to Korean subjects, the mean Cmax and AUC0–t increased linearly with dose. Comparable total systemic exposures were observed in the 2 h apart 40 mg repeated and single 80 mg dose. The geometric mean ratios (90% CIs) of the dose-normalized Cmax and AUC0–t of Korean subjects were similar to those of non-Korean subjects reported in the literature. The adverse events observed were transient and mild in severity.
Conclusion: Eletriptan HBr showed linear PK and was well tolerated in Korean subjects. The PK and tolerability of eletriptan HBr did not differ between Korean and non-Korean subjects.
Keywords: pharmacokinetics, migraine, eletriptan hydrobromide, Korean subjects
Introduction
Migraine is one of the most common headache disorders that greatly affect the quality of life. The prevalence of migraine is relatively high: about 15%–18% in women and 6% in men.1 For effective treatment of migraine, it is necessary to understand its pathophysiology. A proposed theory on migraine pathophysiology is the neurovascular theory, which is characterized by a cascade of events involving various combinations of neurologic, autonomic, and gastrointestinal changes.2 Selective serotonin (5-HT) receptor agonists can arrest the pathophysiological cascade; therefore, various agonists, which are collectively called triptans, have been developed for clinical use.
According to the neurovascular theory described above, triptamine-based drugs such as triptans elicit their effects on migraine patients through intracranial vasoconstriction, in addition to the inhibition of neuropeptide release,3 which ultimately relieves the acute migraine symptoms. The triptans currently available and widely used for the treatment of acute migraine attacks in Korea are naratriptan, sumatriptan, and zolmitriptan. As a potent and selective 5-HT1B/1D agonist, eletriptan hydrobromide (eletriptan HBr) acts selectively on the carotid region of 5-HT receptors4 instead of the coronary arteries.5 However, the pharmacokinetics (PK) and tolerability profiles of eletriptan HBr in Koreans were undetermined and not yet approved in Korea. By comparing with the results of a previous head-to-head comparative study with sumatriptan6 and double-blind single-attack studies with naratriptan7 and zolmitriptan,8 eletriptan HBr was found to show a more rapid onset of efficacy.
Owing to the presence of greater lipophilic characteristics than other triptans, eletriptan HBr has relatively higher bioavailability (~50%) and volume of distribution. The peak plasma concentrations in non-Korean healthy subjects occurred between 1 and 1.5 h after dosing (time required to reach maximum plasma concentration [Tmax]), and in migraine patients with an acute migraine attack, the median Tmax occurred at 2 h.9 Approximately 85% of eletriptan HBr was protein bound with an elimination half-life (t1/2) ranging from 4.8 to 7 h in healthy subjects, and the half-life was unaffected by sex, race, age, or menstrual cycle phases in female subjects.10 Only 10% of eletriptan is cleared through the renal pathway, about 80% is eliminated via hepatic demethylation by CYP3A4 isoenzyme, and 10% by CYP2D6.10
Eletriptan HBr is approved in the United States and Japan at recommended single doses of 20, 40, 80 mg or repeated doses of 40 mg if required, with a maximum daily dose of 80 mg. However, the PK and tolerability profiles of eletriptan HBr in Koreans were undetermined, and the medication is not yet approved in Korea.
We performed a clinical study with the objective of evaluating the PK and tolerability profiles of eletriptan HBr in healthy Korean subjects and compared it with those reported previously in non-Koreans.9
Methods
Study drug, ethics approval, and consent to participate
Eletriptan HBr 20 mg as a 20 mg tablet, 40 mg as a 40 mg tablet, and 80 mg as two 40 mg tablets were administered for the assessment of PK and tolerability to healthy Korean subjects who met the inclusion and exclusion criteria of the study. Candidates were considered to be healthy based on clinical laboratory test results and clinical assessments such as physical examination performed at the time of screening. Written informed consent was obtained from all individual participants included in the study prior to screening tests.
The study protocol was reviewed and approved by the Institutional Review Board at Seoul National University Hospital (ClinicalTrials.gov registry no: NCT01139515). This study was conducted at the Clinical Trials Center, Seoul National University Hospital, Seoul, Korea. The study was conducted in accordance with the principles stipulated in the Declaration of Helsinki as amended in 2013 (Fortaleza, Brazil)11 and the International Conference on Harmonization Good Clinical Practice Guideline.12
Study design
This study was designed as a randomized, open-label, single and repeated-dose, 4-period, and 4-sequence crossover study. Sixteen subjects between the ages of 18 and 55 years were randomized into four treatment groups; a single oral dose of 20, 40, or 80 mg, and a 2 h apart repeated oral dose of 40 mg of eletriptan HBr (Figure 1). The subjects had at least a 46-h washout period between the doses in each period. The study drugs were orally administered under fasting conditions, with 240 mL of water.
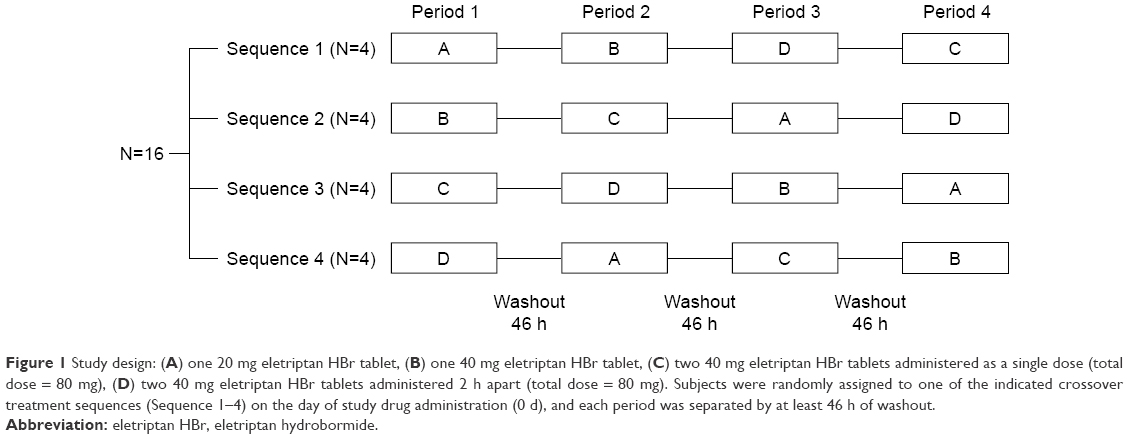 | Figure 1 Study design: (A) one 20 mg eletriptan HBr tablet, (B) one 40 mg eletriptan HBr tablet, (C) two 40 mg eletriptan HBr tablets administered as a single dose (total dose = 80 mg), (D) two 40 mg eletriptan HBr tablets administered 2 h apart (total dose = 80 mg). Subjects were randomly assigned to one of the indicated crossover treatment sequences (Sequence 1–4) on the day of study drug administration (0 d), and each period was separated by at least 46 h of washout. |
All subjects were admitted to the Clinical Trials Center a day before dosing, and they were required to fast for at least 8 h prior to dosing. During the entire study period, the subjects were restricted from taking any concomitant medication or beverages containing xanthine or alcohol.
For the determination of plasma eletriptan concentrations, blood samples (6 mL) were serially collected in tubes containing lithium heparin prior to dosing and at 0.5, 0.75, 1, 1.5, 2, 3, 4, 6, 8, 10, 12, 16, and 24 h after dosing for the single-dose treatment groups. For the repeated-dose group of 40 mg, the blood samples were collected prior to dosing and at 0.5, 0.75, 1, 1.5, 2, 2.5, 2.75, 3, 3.5, 4, 5, 6, 8, 10, 12, 14, 18, and 26 h after dosing. Samples were centrifuged at 1,700 × g for 10 min at 4°C. The plasma was separated and stored at −20°C until concentration analysis.
Determination of eletriptan plasma concentration
Plasma concentrations of eletriptan were assayed by a validated method using high-performance liquid chromatography with mass spectrometry detection. The lower and upper limits of quantification were 0.5 and 250 ng/mL, respectively, and the calibration curve of the method was linear over this range. Where necessary, samples were diluted with normal human plasma to bring the concentration within the calibration range. Calibration standards were prepared by spiking blank plasma samples with known amounts of eletriptan ranging from 0.5 to 250 ng/mL. The accuracy (expressed as the percentage difference from the theoretical concentration) of the quality control samples used during the sample analysis ranged from −2.0% to 4.7% with a precision (expressed as the coefficient of variation) of ≤ 9.7%.
PK evaluation and ethnic comparison
The plasma concentrations of eletriptan with time after the dose were analyzed. The following PK parameters for each treatment group (20, 40, 80 mg, and two 40 mg repeated dose, 2 h apart) were analyzed: maximum plasma concentration (Cmax), Tmax, area under the plasma concentration versus time curve from 0 h to the last measurable concentration (AUC0–t, where t is the last time point with a measurable concentration), area under the plasma concentration versus time curve from 0 h to infinity (AUC0–inf), and the elimination half-life (t1/2). The AUC0–t was calculated using the linear trapezoidal method. The observed concentrations and times were used to estimate the Cmax and Tmax of eletriptan. AUC0–inf was calculated as AUC0–t + Ct/λz, where Ct is the last measured concentration and λz is the elimination rate constant calculated using linear regression of the log-linear portion of the plasma concentration–time curve. The t1/2 was calculated as ln (2)/λz. All the PK parameters were estimated using Phoenix® WinNonlin® (version 6.3; Certara USA Inc., Princeton, NJ, USA). For evaluating the dose linearity of eletriptan HBr in Korean subjects, the dose-normalized mean differences of Cmax, AUC0–t, and AUC0–inf and the corresponding 90% confidence intervals (CIs) for the differences were exponentiated to provide estimates of the ratio of dose-normalized geometric means and 90% CIs.
The current PK of eletriptan HBr in Koreans were compared with the data of non-Koreans published in 20029 for an ethnic comparison between the two populations. The PK of eletriptan HBr for the two populations were compared by calculating the point estimate and 90% CI of the dose-normalized Cmax, AUC0–t, and AUC0–inf by weighted average pooling method. All statistical analyses were performed using SAS version 9.4 software (SAS Institute Inc., Cary, NC, USA).
Tolerability assessment
Tolerability assessment, including vital signs (systolic and diastolic blood pressures, pulse rate), physical examination, and adverse events (AEs) were conducted prior to the study drug administration until the completion of the study. The subjects were interviewed during the course of the study for collecting information regarding AE, which were monitored throughout the study by nonleading questioning.
For ethnic comparison, the types, frequency and severity of AEs, and other tolerability parameters including the changes in vital signs were compared between the Korean and non-Korean subjects.
Results
Subjects
Sixteen subjects completed the study and were included in the assessment of PK characteristics and tolerability. The mean ± standard deviation of age, height, weight, and body mass index were 24.8 ± 2.9 years, 172.2 ± 5.3 cm, 65.8 ± 5.7 kg, and 22.2 ± 1.8 kg/m2, respectively.
PK profiles
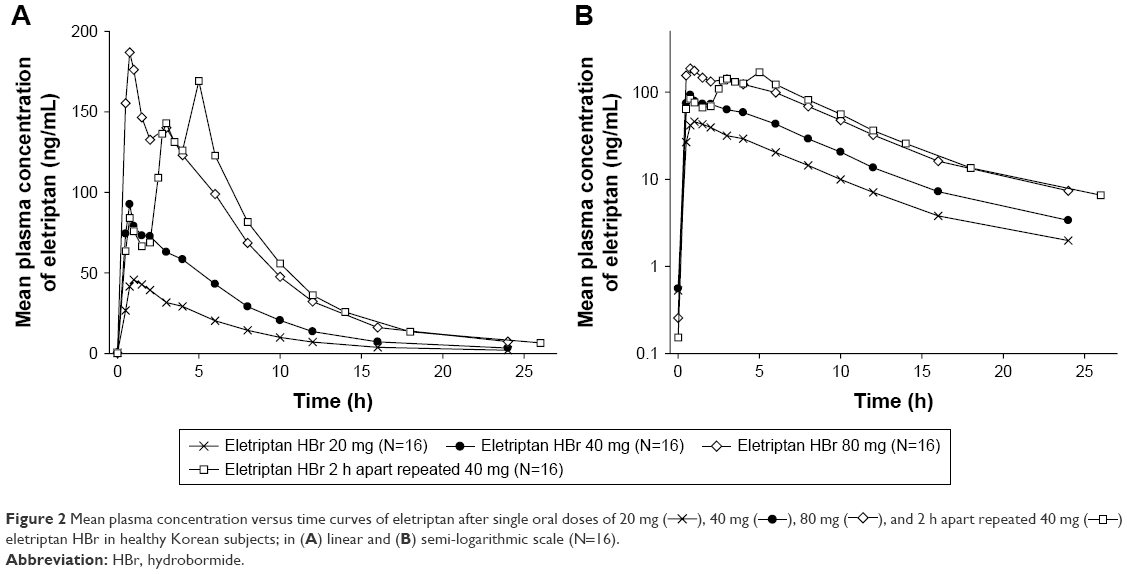
The mean plasma eletriptan concentration versus time curves after single oral doses of 20, 40, 80 mg, and 2 h apart repeated 40 mg dose of eletriptan HBr in healthy Korean subjects are presented in Figure 2. The median Tmax values were similar among the single oral doses of eletriptan HBr (0.75 h), while the median Tmax for the 2 h apart repeated 40 mg dose ranged from 0.75 to 5 h with a median value of 5 h (Figure 2; Table 1). The t1/2 was similar for all the four treatment groups, with the mean t1/2 values ranging from 4.6 to 4.9 h (Table 1).
 | Figure 2 Mean plasma concentration versus time curves of eletriptan after single oral doses of 20 mg ( |
 ), 40 mg (
), 40 mg ( ), 80 mg (
), 80 mg ( ), and 2 h apart repeated 40 mg (
), and 2 h apart repeated 40 mg ( ) eletriptan HBr in healthy Korean subjects; in (A) linear and (B) semi-logarithmic scale (N=16).
) eletriptan HBr in healthy Korean subjects; in (A) linear and (B) semi-logarithmic scale (N=16).
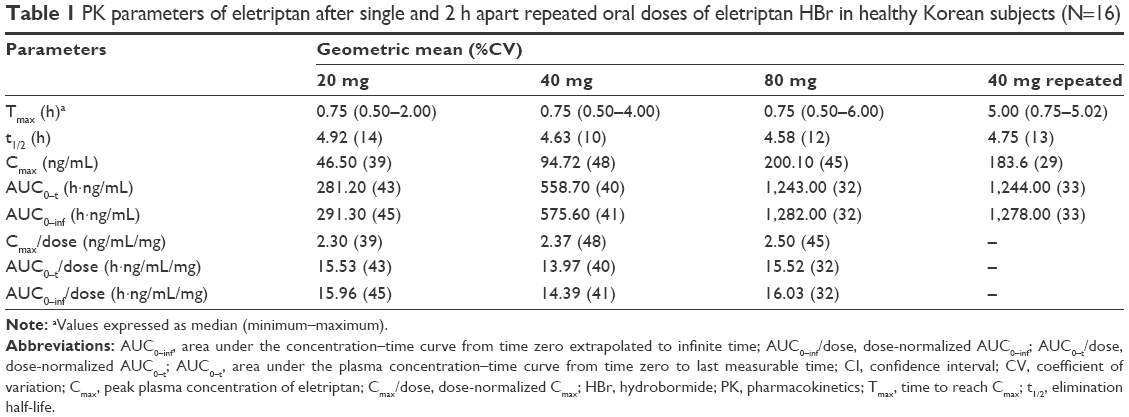 | Table 1 PK parameters of eletriptan after single and 2 h apart repeated oral doses of eletriptan HBr in healthy Korean subjects (N=16) |
Following the single oral doses of eletriptan HBr, the systemic exposure of eletriptan increased in a dose-proportional manner across the dose range of 20–80 mg in healthy Korean subjects (Table 1; Figure 3). This is further supported by the narrow ranges of dose-normalized Cmax, AUC0–t, and AUC0–inf values: 2.33–2.50 ng/mL/mg, 13.97–15.54 h·ng/mL/mg, and 14.39–16.03 h·ng/mL/mg, respectively.
 | Figure 3 Dose-normalized pharmacokinetic parameters of eletriptan after single oral doses of eletriptan hydrobromide in healthy Korean subjects; (A) Cmax and (B) AUC0–t. |
The point estimates and the 90% CI of the dose-normalized Cmax, AUC0–t, and AUC0–inf between Korean and non-Korean subjects were similar (Table 2). This indicates a similar bioavailability of eletriptan HBr between the two ethnic groups.
 | Table 2 The dose-normalized PK parameters of eletriptan following single oral doses of eletriptan HBr in Korean (N=48) and non-Korean (N=47) subjects |
Tolerability
Among the nine cases of AEs reported in the 16 Korean subjects who received the study drug, loose stool, abdominal pain, and headache were considered to be possibly related to the administration of eletriptan HBr. All reported study drug-related AEs were mild in intensity, and none of these led to the discontinuation of the study (Table 3). Throughout the study period, single oral doses of eletriptan HBr 20, 40, 80 mg, and two repeated doses of 40 mg 2 h apart were well tolerated in all Korean subjects. There were no discrepancies between the dose groups in frequencies and severity of AEs.
 | Table 3 Summary of treatment-emergent AEs that occurred after single and 2 h apart repeated oral doses of eletriptan HBr in healthy Korean subjects (N=16) |
When compared to the non-Korean subjects, Korean subjects did not exhibit any new adverse effects. Taking the AEs and other tolerability parameters such as vital signs and physical examination into consideration,9 tolerability in the Korean study appeared to be similar to that observed in the non-Korean study.
Discussion
This study was designed for the assessment of PK characteristics and tolerability of eletriptan HBr in Korean subjects after the administration of the US-approved doses of 20, 40, and 80 mg. In addition, the PK characteristics of the repeated dose of 40 mg 2 h apart were assessed. This is clinically important as only 70% of the migraine patients achieved headache relief 2 h after the single-dose administration of eletriptan HBr.13,14 The effectiveness of eletriptan HBr in the treatment of headache recurrence for the 40 mg dose has already been observed in migraine patients.15 For the achievement of balance and maximization of comparisons with the smallest number of subjects, Williams Design with four treatments, four sequences, and four periods was selected to assess the PK characteristics and tolerability of eletriptan HBr in Korean subjects.
The PK profiles of eletriptan HBr showed peaks with shoulders in 20 and 40 mg treatment groups and double peaks in 80 mg treatment group around 4 h after the oral dose (Figure 2). This phenomenon may have occurred owing to the enterohepatic recirculation of eletriptan, which is mainly eliminated via metabolism by the liver CYP enzymes10 and through bile acid secretion after food intake, which was done 4 h after dosing; eletriptan HBr undergoes extensive biliary excretion.16 The already absorbed eletriptan is reintroduced into the gastrointestinal tract via the bile. As a result, the systemic exposure of eletriptan rises. This reabsorption from the bile contributes toward the formation of shoulders and double-peaked characteristics of the PK profiles.17 Such PK characteristics were often observed in previous studies.9,18
The point estimates of dose-normalized Cmax, AUC0–t, and AUC0–inf were also similar in Korean and non-Korean subjects after single oral doses of eletriptan HBr (Table 2). Sensitivity to ethnic differences evaluated in accordance with the International Conference on Harmonization E5 guideline, Appendix D, would be expected to be low.19 Low sensitivity to ethnic factors of eletriptan HBr was estimated using the known characteristics such as relatively high bioavailability,9 metabolism distributed among multiple pathways,10,20 and linear PK in previous non-Korean studies and the present Korean study.9,10,15 Currently, there is no evidence that the onset of migraine pattern differs in Korean and the non-Korean patients. In addition, no differences in dosage and corresponding effects have been reported in Korean and non-Korean subjects for other triptan drugs so far.21 The quantitative relationships between the exposure of eletriptan (PK) and the drug-driven effects (pharmacodynamics) observed in migraine patients have been well established in previous studies.6 Thus, we deduce that the clinical efficacy in Korean migraine patients will be similar to that in non-Korean patients at same dosage.
The most frequently reported AEs were nausea and headache, in the 20 mg and 40 mg single dose-groups, respectively, and chest discomfort from a single subject was the only moderate AE reported in 80 mg single-dose and 40 mg repeated-dose groups (Table 3). Based upon the absence of serious AEs, dose reductions or discontinuations due to reported AEs, eletriptan HBr was considered both safe and well tolerated after single administration within the dose range of 20–80 mg, as well as after repeated administration of 40 mg 2 h apart in healthy male subjects.
In summary, PK and tolerability in Korean subjects were comparable to those in the non-Korean subjects after single and repeated doses of eletriptan HBr. Although the present study has been performed in healthy male volunteers, the similar PK and tolerability profiles shown between the healthy and migraine patients in the previous non-Korean subject studies22 and known evidence of eletriptan PK being unaffected by sex22 suggests that different sex and patient status are factors unlikely to alter the conclusions reached from the healthy subjects in this study. From this evidence for low sensitivity to ethnic factors, dosage regimens identical to those for non-Korean patients may be suggested for Korean patients without further confirmatory study in Korean migraine patients.
Conclusion
Eletriptan HBr showed linear PK and was well tolerated in Korean subjects. The observed PK and tolerability were similar to those of non-Korean subjects. Therefore, we suggest that the same dosage regimen of eletriptan HBr may be recommended for Korean as well as non-Korean patients with migraine.
Acknowledgments
The first author (Yu Kyong Kim) received a scholarship from the BK21-plus education program provided by the National Research Foundation of Korea. This study was sponsored by Pfizer, Inc. The authors gratefully acknowledge the support of Ji-Young Lee, Pfizer, Inc., in manuscript coordination, and Hyungmi An, Seoul National University College of Medicine and Hospital, for statistical analyses.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
Jeffrey Alderman is employed by Pfizer, Inc. The authors report no other conflicts of interest in this work.
References
Lipton RB, Stewart WF, von Korff M. Burden of migraine: societal costs and therapeutic opportunities. Neurology. 1997;48(3 Suppl 3):S4–S9. | ||
Goodell H, Ostfeld AM, Pichler E, Wolff HG. Studies on headache; central versus peripheral action of ergotamine tartrate and its relevance to the therapy of migraine headache. AMA Arch Neurol Psychiatry. 1956;76(6):571–577. | ||
Napier C, Stewart M, Melrose H, Hopkins B, McHarg A, Wallis R. Characterisation of the 5-HT receptor binding profile of eletriptan and kinetics of [3H] eletriptan binding at human 5-HT1B and 5-HT1D receptors. Eur J Pharmacol. 1999;368(2–3):259–268. | ||
Willems E, De Vries P, Heiligers JP, Saxena PR. Porcine carotid vascular effects of eletriptan (UK-116,044): a new 5-HT1B/1D receptor agonist with anti-migraine activity. Naunyn Schmiedebergs Arch Pharmacol. 1998;358(2):212–219. | ||
Jhee SS, Shiovitz T, Crawford AW, Cutler NR. Pharmacokinetics and pharmacodynamics of the triptan antimigraine agents: a comparative review. Clin Pharmacokinet. 2001;40(3):189–205. | ||
Diener HC. Eletriptan in migraine. Expert Rev Neurother. 2005;5(1):43–53. | ||
Garcia-Ramos G, MacGregor EA, Hilliard B, Bordini CA, Leston J, Hettiarachchi J. Comparative efficacy of eletriptan vs naratriptan in the acute treatment of migraine. Cephalalgia. 2003;23(9):869–876. | ||
Steiner TJ, Diener HC, MacGregor EA, Schoenen J, Muirheads N, Sikes CR. Comparative efficacy of eletriptan and zolmitriptan in the acute treatment of migraine. Cephalalgia. 2003;23(10):942–952. | ||
Shah AK, Harris SC, Greenhalgh C, Morganroth J. The pharmacokinetics and safety of single escalating oral doses of eletriptan. J Clin Pharmacol. 2002;42(5):520–527. | ||
Milton KA, Scott NR, Allen MJ, et al. Pharmacokinetics, pharmacodynamics, and safety of the 5-HT(1B/1D) agonist eletriptan following intravenous and oral administration. J Clin Pharmacol. 2002;42(5):528–539. | ||
World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. | ||
Food and Drug Administration. Guidance for industry, E6 good clinical practice: consolidated guidance. Presented at International Conference on Harmonisation Good Clinical Practice. Federal Register. Vol 62, 1997:25691–25709. | ||
Dodick DW. Triptan nonresponder studies: implications for clinical practice. Headache. 2005;45(2):156–162. | ||
Tfelt-Hansen P, Edvinsson L. Pharmacokinetic and pharmacodynamic variability as possible causes for different drug responses in migraine. A comment. Cephalalgia. 2007;27(10):1091–1093. | ||
Food and Drug Administration Center for Drug Evaluation and Research. Clinical Review of NDA Number 21-016, Relpax. In: US Food and Drug Administration Division of Neuropharmacological Drug Products. Maryland: Food and Drug Administration; 2002. | ||
Food and Drug Administration Center for Drug Evaluation and Research. Pharmacology Review of NDA Number 21-016, Relpax. In: US Food and Drug Administration Division of Neuropharmacological Drug Products. Maryland: Food and Drug Administration; 1999. | ||
Davies NM, Takemoto JK, Brocks DR, Yanez JA. Multiple peaking phenomena in pharmacokinetic disposition. Clin Pharmacokinet. 2010;49(6):351–377. | ||
Shah AK, Laboy-Goral L, Scott N, Morse T, Apseloff G. Pharmacokinetics and safety of oral eletriptan during different phases of the menstrual cycle in healthy volunteers. J Clin Pharmacol. 2001;41(12):1339–1344. | ||
ICH Harmonised Tripartite Guideline. Ethinic Factors in the Acceptability of Foreign Clinical Data E5 (R1). Poster presented at: International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use. ICH Expert Working Group; 1998:1–13. | ||
Evans DC, O’Connor D, Lake BG, Evers R, Allen C, Hargreaves R. Eletriptan metabolism by human hepatic CYP450 enzymes and transport by human P-glycoprotein. Drug Metab Dispos. 2003;31(7):861–869. | ||
Morillo LE. Migraine headache in adults. Clin Evid. 2004;65(11):1696–1719. | ||
Relpax(R) [drug label]. New York: Pfizer Inc; 2013. Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2013/021016s021s023s024s027lbl.pdf. Accessed July 13, 2016. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.