Back to Journals » Drug Design, Development and Therapy » Volume 13
Pharmacokinetic interactions between telmisartan/amlodipine and rosuvastatin after multiple oral administrations in healthy Korean male subjects
Authors Moon SJ, Jeon JY, Jang K, Yu KS ![]() , Lim Y
, Lim Y ![]() , Kim MG
, Kim MG ![]()
Received 28 March 2019
Accepted for publication 12 June 2019
Published 25 July 2019 Volume 2019:13 Pages 2533—2542
DOI https://doi.org/10.2147/DDDT.S210364
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Cristiana Tanase
Seol Ju Moon,1,2 Ji-Young Jeon,1 Kyungho Jang,1 Kyung-Sang Yu,2 Yeji Lim,3 Min-Gul Kim1,4–5
1Center for Clinical Pharmacology, Biomedical Research Institute, Chonbuk National University Hospital, Jeonju, Republic of Korea; 2Department of Clinical Pharmacology and Therapeutics, Seoul National University College of Medicine and Hospital, Seoul, Republic of Korea; 3Yuhan Research Institute, Yuhan Corporation, Seoul, Republic of Korea; 4Research Institute of Clinical Medicine of Chonbuk National University, Jeonju, Republic of Korea; 5Department of Pharmacology, School of Medicine, Chonbuk National University, Jeonju, Republic of Korea
Purpose: Hypertension and dyslipidemia are major risk factors for cardiovascular diseases, and reduction of cardiovascular risks can be achieved by combining antihypertensive therapy with statins. The objective of this study was to evaluate the pharmacokinetic interaction between telmisartan/amlodipine fixed dose combination and rosuvastatin in healthy Korean male volunteers.
Patients and methods: An open-label, two-cohort, multiple-dose, single-sequence crossover study was conducted in healthy male subjects. In Cohort 1, the subjects were administered one tablet of telmisartan/amlodipine 80 mg/5 mg once daily for 14 days with or without one tablet of rosuvastatin 20 mg once daily. In Cohort 2, the subjects were administered one tablet of rosuvastatin 20 mg once daily for 14 days with or without one tablet of telmisartan/amlodipine 80 mg/5 mg once daily. Serial blood samples were collected up to 24 hrs post-dose on the 9th and 14th days in Cohort 1 and on the 5th and 14th days in Cohort 2. Plasma drug concentrations were measured by liquid chromatography/tandem mass spectrometry. Pharmacokinetic parameters, including maximum plasma concentration at steady state (Cmax,ss) and area under the plasma concentration versus time curve over dosing interval (AUCτ,ss), were determined by non-compartmental analysis. The geometric least-square mean (GLSM) ratios and associated 90% confidence intervals (CIs) of log-transformed Cmax,ss and AUCτ,ss for separate or concurrent therapy were calculated to evaluate pharmacokinetic interactions.
Results: Thirty-eight subjects from Cohort 1 and nineteen subjects from Cohort 2 completed the study. The GLSM ratios and 90% CIs of Cmax,ss and AUCτ,ss, were 0.9829 (0.8334–1.1590) and 1.0003 (0.9342–1.0710) for telmisartan; 0.9908 (0.9602–1.0223) and 1.0081 (0.9758–1.0413) for amlodipine; and 2.2762 (2.0113–2.5758) and 1.3261 (1.2385–1.4198) for rosuvastatin, respectively.
Conclusion: The pharmacokinetic parameters of telmisartan/amlodipine, but not rosuvastatin, met the pharmacokinetic equivalent criteria. The increase in systemic exposure to rosuvastatin caused by telmisartan/amlodipine co-administration would not be clinically significant in practice. Nevertheless, an appropriately designed two-sequence crossover study is needed to confirm the results of this study.
Keywords: drug–drug interactions, pharmacokinetics, phase I, antihypertensive, statins
Introduction
Cardiovascular diseases (CVDs) are one of the most prevalent causes of fatality worldwide, contributing to 17.9 million deaths each year (approximately 31% of all global deaths).1 CVDs are multifactorial disorders caused by multiple risk factors, including hypertension, dyslipidemia, and obesity. Various epidemiological studies have shown that hypertension and dyslipidemia are often observed as co-existing in patients.2 This co-existence of hypertension and dyslipidemia leads to a greater impact on the vascular endothelium, which results in atherosclerosis and further CVDs.3 As two or more risk factors interact with each other, moderate reductions in several risk factors could be more effective in lowering CVD risks.4
The American College of Cardiology (ACC) and the American Heart Association (AHA) published a new guideline in 2017 that includes a stricter definition of hypertension to account for complications that can occur at lower numbers. According to the ACC/AHA 2017 Guideline, Stage 1 hypertension is now defined as systolic blood pressure (SBP) between 130 and 139 mmHg or diastolic blood pressure (DBP) between 80 and 89 mmHg.5 In line with this new definition, a blood pressure of less than 130/80 mmHg (SBP/DBP) is considered ideal in most patients. The guideline also recommends assessment of CVD risks, such that if the risks are high, antihypertensive medication can be started at earlier stages.
The assessment of CVD risks can be performed based on guidelines such as the ACC/AHA Guideline on the Assessment of Cardiovascular Risk and the NICE Clinical Guideline CG181.6,7 According to the result of the risk assessment, further guidelines such as the 2018 ACC/AHA Guideline for the Management of Blood Cholesterol can be used to manage blood cholesterol,8 and guidelines such as the 2014 Eighth Joint National Committee (JNC 8) panel recommendations can be used to manage hypertension.9
According to these guidelines, the initial therapy for hypertension generally includes primary agents such as thiazide diuretics, angiotensin-converting enzyme inhibitors (ACEI), angiotensin receptor blockers (ARB), and calcium channel blockers (CCB) alone or in combination.9 Evidence supports the idea that combination therapy of two or more antihypertensive drugs is much more effective in lowering blood pressure,10 and some antihypertensive medications are now marketed as a fixed dose combination of two or three drug products that include ARB, CCB, and thiazide diuretics. On the other hand, management of blood cholesterol usually involves initiating statin therapy and adding ezetimibe as an add-on. Especially high- to moderate-intensity statin therapies are recommended to be used extensively, and some examples of first-line statins include atorvastatin, simvastatin, and rosuvastatin.
Telmisartan is an ARB that is highly selective to the angiotensin II type 1 (AT1) receptor, which is known to mediate most of the physiological actions related to blood pressure regulation.11 By blocking the vasoconstrictor and aldosterone-secreting effects of angiotensin II, it reduces blood pressure independently from the angiotensin II synthesis pathway. Telmisartan reaches peak concentrations about 0.5 to 1 hr after oral administration and is mainly eliminated in the feces via biliary excretion with an elimination half-life of about 24 hrs.
Amlodipine is one of the most widely marketed CCBs; these work by disrupting calcium movement, thereby relaxing smooth muscles located in heart and blood vessels. This leads to a lowering of the afterload, increasing glomerular filtration and thus having a subsequent diuretic effect, leading to lowered blood pressure. Amlodipine is slowly absorbed after administration, with a half-life of 35 to 40 hrs, and its antihypertensive effect is gradual with a low possibility of adverse events (AEs) such as orthostatic hypotension.11,12
Rosuvastatin is a selective and competitive inhibitor of hydroxymethylglutaryl-coenzyme A (HMG-CoA) reductase, which is involved in cholesterol synthesis.13 It also increases the number of hepatic low-density lipoprotein (LDL) receptors such that LDL uptake and catabolism are increased. Rosuvastatin reaches peak concentrations 3 to 5 hrs after dosing, and mainly excreted in the feces with an elimination half-life of about 19 hrs.
Hence, a fixed dose combination of these three drugs – telmisartan, amlodipine, and rosuvastatin – may improve patient compliance by reducing pill burden, while reducing the cardiovascular risks that are posed by hypertension and dyslipidemia. The objective of this study was to evaluate the pharmacokinetic interaction between telmisartan/amlodipine and rosuvastatin, after multiple oral administration in healthy male volunteers.
Materials and methods
Study population
Healthy male volunteers, defined as individuals with no clinically significant abnormalities in medical history, physical examination, 12-lead electrocardiogram (ECG), and clinical laboratory tests, were recruited after obtaining written informed consent. The eligible subjects were aged between 19 and 50 years, weighed at least 55 kg and over, with a body mass index (BMI) of at least 18.5 and no greater than 28 kg/m2. Specific exclusion criteria included a history or current evidence of acute or chronic illness, including hypersensitivity to any of the investigational products or any other clinically relevant hypersensitivity. Individuals with clinically significant abnormalities in blood chemistry, hematology, serology, and urinalysis were excluded. Individuals whose SBP was lower than or equal to 100 mmHg, or was greater or equal to 160 mmHg, or whose DBP was lower than or equal to 60 mmHg, or was greater than or equal to 95 mmHg, were also excluded. Subjects who participated in other clinical trials within 3 months, who donated whole blood within 2 months, and who received a blood transfusion or donated blood components within 1 month of the first day of the study were excluded. Subjects who could not refrain from consuming alcohol during hospitalization or who smoked more than 20 cigarettes a day were also excluded.
Study design
This study was an open-label, two-cohort, multiple-dose, single-sequence crossover study. In Cohort 1, the effects of rosuvastatin 20 mg on the pharmacokinetics of a telmisartan/amlodipine 80 mg/5 mg fixed dose combination were evaluated. In Cohort 2, the effects of a telmisartan/amlodipine 80 mg/5 mg fixed dose combination on the pharmacokinetics of rosuvastatin 20 mg were evaluated.
Eligible subjects participated in one of the two cohorts and visited the outpatient clinic or were admitted to the ward of Chonbuk National University Hospital according to the study protocol. In Cohort 1, the subjects were administered one tablet of telmisartan/amlodipine 80 mg/5 mg once daily from the first day to the 14th day, where one tablet of rosuvastatin 20 mg was co-administered once daily from the 10th to the 14th day. In Cohort 2, the subjects were administered one tablet of rosuvastatin 20 mg once daily from the first day to the 14th day, where one tablet of telmisartan/amlodipine 80 mg/5 mg was co-administered once daily from the 6th day to the 14th day. All investigational products were administered with 150 mL of water. Serial blood samples were collected up to 24 hrs post-dose on the 9th day and 14th day in Cohort 1, and up to 24 hrs post-dose on the 5th day and 14th day in Cohort 2, where the 14th-day blood sampling was performed to assess the pharmacokinetics of co-administration. Pharmacokinetic blood samples were collected in EDTA tubes and were centrifuged within 1 hr of collection at 2,000 g for 10 mins at 4 °C. Aliquots of plasma samples were collected and were stored at −70 °C until further analysis.
The study protocol was approved by the Institutional Review Board of Chonbuk National University Hospital and conducted in accordance with the principles of the Declaration of Helsinki and Korean Good Clinical Practice (ClinicalTrials.gov Identifier: NCT02951962).
Plasma drug concentration analysis
Plasma telmisartan concentrations were determined by a validated liquid chromatography/tandem mass spectrometry (LC-MS/MS, Waters Alliance HT LC System and Waters Quattro MICRO MS; Milford, MA, USA) using telmisartan-d7 as the internal standard. Chromatographic separation was performed using a C18 column (2.1 mm ID ×100 mm L, 3 μm) at a flow rate of 0.2 mL/min. The mobile phase was 10 mM ammonium formate/acetonitrile/formic acid (30:70:0.1, v/v/v). Electrospray ionization in positive ion mode was used for detection and quantification. The multiple reaction monitoring (MRM) transitions were m/z 515.05 → 276.10 for telmisartan and 522.10 → 280.10 for the internal standard. A calibration curve covering the range of 10 – 5000 ng/mL was constructed. The intra-day accuracy was 94.5 – 103.3% (with a precision of 1.2 – 7.2%), and the inter-day accuracy was 95.1 – 103.0% (with a precision of 1.1 – 3.3%).
For amlodipine, LC-MS/MS (Shiseido Nanospace SI-2, Shimadzu, Kyoto, Japan; 4000 QTRAP, AB Sciex, Foster City, CA, USA) was used to determine plasma concentrations using amlodipine-d4 as the internal standard. Chromatographic conditions were identical to those used for telmisartan, except that the mobile phase consisted of acetonitrile/deionized water/formic acid (50:50:0.01, v/v/v). The MRM transitions were m/z 409.5 → 238.3 for amlodipine and 413.5 → 238.3 for the internal standard. A calibration curve covering the range of 0.5 – 100 ng/mL was constructed. The intra-day accuracy was 90.5% to 101.2% (with a precision of 0.3 – 11.9%), and the inter-day accuracy was 98.6 – 102.6% (with a precision of 1.0 –5.6%).
For rosuvastatin, LC-MS/MS (Shimadzu UFLC, Shimadzu, Kyoto, Japan; 5500 QTRAP, AB Sciex, Foster City, CA, USA) was used to determine plasma concentrations using rosuvastatin-d6 sodium salt as the internal standard. Chromatographic separation was performed using a C18 column (2.0 mm ID ×75 mm L, 3 μm) at a flow rate of 0.2 mL/min, and the mobile phase was acetonitrile/deionized water/formic acid (45:55:0.1, v/v/v). The MRM transitions were m/z 482.1 → 258.1 for rosuvastatin and 488.1 → 264.1 for the internal standard. A calibration curve covering the range of 0.5 to 300 ng/mL was constructed. The intra-day accuracy was 98.5 – 103.3% (with a precision of 0.8 –3.1%), and the inter-day accuracy was 98.3 –101.8% (with a precision of 0.4 – 1.6%).
Pharmacokinetic analysis
The pharmacokinetic analysis included all the subjects who had completed the study according to the protocol. The pharmacokinetic parameters were assessed using non-compartmental method provided by Phoenix® WinNonlin® software (version 6.1, Pharsight, Mountain View, CA, USA). The maximum plasma drug concentration at steady state (Cmax,ss), minimum plasma drug concentration at steady state (Cmin,ss), and time to Cmax,ss (Tmax,ss) were directly obtained from the plasma concentration-time profiles. The area under the plasma concentration-time profiles during a dosing interval at steady state (AUCτ,ss) was calculated according to the linear trapezoidal rule. From Cohort 1, the AUCτ,ss and Cmax,ss of telmisartan and amlodipine were evaluated, and from Cohort 2, the AUCτ,ss and Cmax,ss of rosuvastatin were evaluated.
Statistical analysis
Pharmacokinetic drug interactions were assessed by comparing the co-administration of a telmisartan/amlodipine fixed dose tablet and rosuvastatin with each single agent administration for the principal parameters of systemic exposure (AUCτ,ss and Cmax,ss). The AUCτ,ss and Cmax,ss were log-transformed and a linear mixed-effect model was applied. An analysis of variance was performed with subject as random effects and treatment as fixed effect in SAS (version 9.3, SAS Institute, Inc., Cary, NC, USA). The results for AUCτ,ss and Cmax,ss were reported as 90% confidence intervals (CIs) surrounding the ratio of the geometric least-square means (GLSMs) of the pharmacokinetic parameters.
Safety analysis
The safety analysis included all the subjects who received at least one dose of any of the investigational products. Safety measurements included physical examination, clinical laboratory test results (including hematology, serum chemistry, and urinalysis), vital signs, 12-lead ECGs, and assessment of AEs. Descriptive statistics were used to summarize any clinically significant findings from physical examination, clinical laboratory test results, vital signs, and ECGs in each treatment arm.
Results
Disposition of subjects and demographics
In Cohort 1, forty-one subjects were enrolled and a total of 40 subjects received investigational products at least once. One subject withdrew consent before drug administration and was replaced by a newly enrolled subject. There were two drop-out subjects after drug administration, one because of consent withdrawal and one because of an AE; 38 subjects completed the study as a result. In Cohort 2, twenty subjects were enrolled and received investigational products at least once. There was one drop-out subject after drug administration due to consent withdrawal, and a total of 19 subjects completed the study.
Descriptive statistics were used to analyze demographic characteristics for subjects who had been administered investigational products at least once in both cohorts. In Cohort 1, arithmetic mean ± standard deviation (SD) for the subjects’ age, height, weight, and BMI was 23.35±2.21 years, 174.62±4.67 cm, 71.18±8.59 kg, and 23.28±2.54 kg/m2, respectively. In Cohort 2, arithmetic mean ± SD for the subjects’ age, height, weight, and BMI was 22.80±1.96 years, 174.40±6.66 cm, 71.75±10.76 kg, and 23.44±2.31 kg/m2, respectively.
Pharmacokinetics of telmisartan
From the results of Cohort 1, the geometric mean plasma concentration-time profiles of telmisartan when administered separately as a fixed dose combination of telmisartan/amlodipine or co-administered with rosuvastatin are shown in Figure 1. There was no statistically significant effect of co-administration on telmisartan pharmacokinetics (Table 1). The GLSM ratios and 90% CIs of telmisartan (when co-administered with rosuvastatin compared to separate administration as a telmisartan/amlodipine tablet) were 0.9829 (0.8334–1.1590) for Cmax,ss and 1.0003 (0.9342–1.0710) for AUCτ,ss.
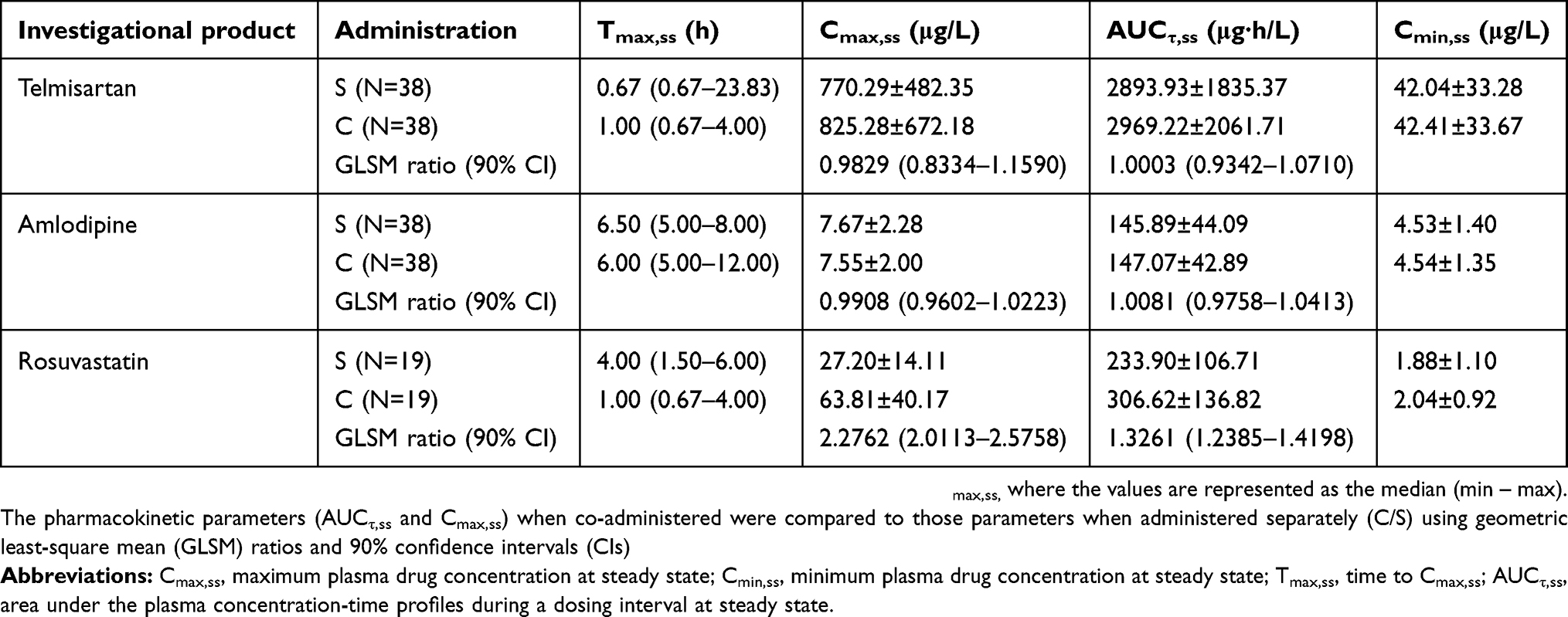 |
Table 1 Summary of pharmacokinetic parameters when telmisartan, amlodipine, and rosuvastatin were administered separately (S) or co-administered (C) |
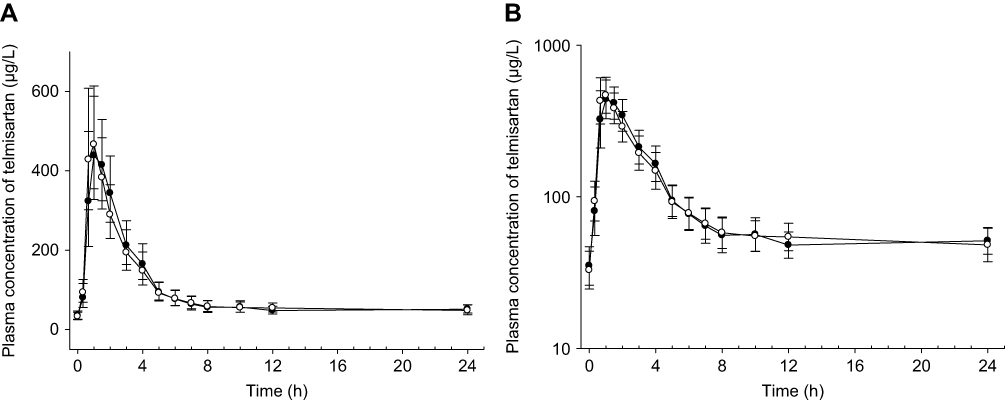 |
Figure 1 Geometric mean plasma concentration-time profiles of telmisartan when administered separately as a fixed dose combination of telmisartan/amlodipine 80 mg/5 mg (open circle) or co-administered with rosuvastatin 20 mg (closed circle).Notes: Linear (A) and semi-logarithmic (B) scale. Each point represents the geometric mean ±95% confidence intervals. |
Pharmacokinetics of amlodipine
From the results of Cohort 1, the geometric mean plasma concentration-time profiles of amlodipine when administered separately as a fixed dose combination of telmisartan/amlodipine or co-administered with rosuvastatin are shown in Figure 2. There was no statistically significant effect of co-administration on amlodipine pharmacokinetics (Table 1). The GLSM ratios and 90% CIs of amlodipine (when co-administered with rosuvastatin compared to separate administration as a telmisartan/amlodipine tablet) were 0.9908 (0.9602–1.0223) for Cmax,ss and 1.0081 (0.9758–1.0413) for AUCτ,ss.
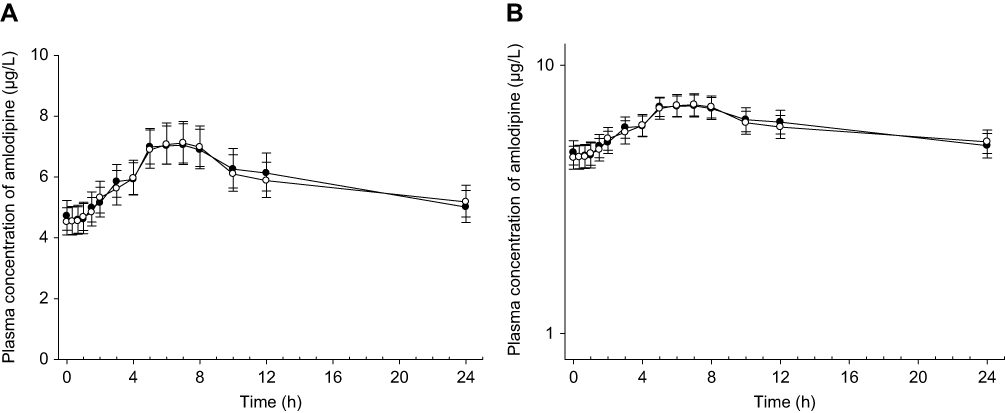 |
Figure 2 Geometric mean plasma concentration-time profiles of amlodipine when administered separately as a fixed dose combination of telmisartan/amlodipine 80 mg/5 mg (open circle) or co-administered with rosuvastatin 20 mg (closed circle). Notes: Linear (A) and semi-logarithmic (B) scale. Each point represents the geometric mean ±95% confidence intervals. |
Pharmacokinetics of rosuvastatin
From the results of Cohort 2, the geometric mean plasma concentration-time profiles of rosuvastatin when administered separately or co-administered with telmisartan/amlodipine fixed dose combination tablet are shown in Figure 3. The GLSM ratios and 90% CIs of rosuvastatin (when co-administered compared to rosuvastatin administered alone) were 2.2762 (2.0113–2.5758) for Cmax,ss and 1.3261 (1.2385–1.4198) for AUCτ,ss. Both Cmax,ss and AUCτ,ss of rosuvastatin showed statistically significant change (Table 1) and their 90% CIs did not meet the equivalence criteria.
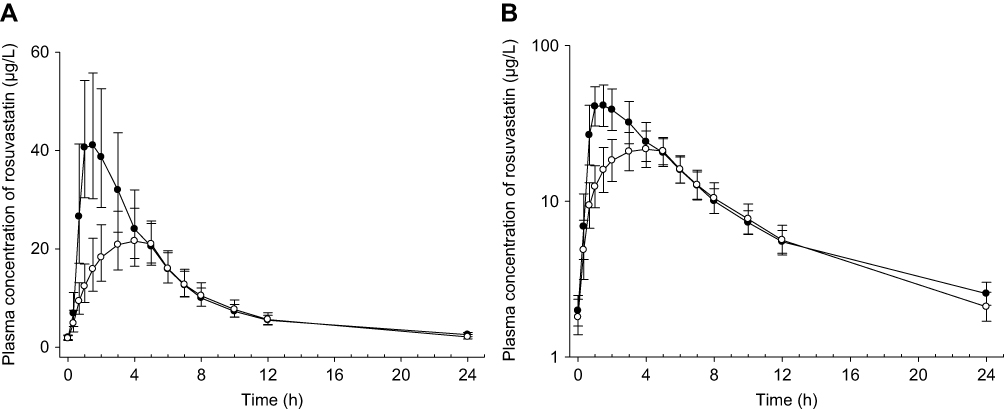 |
Figure 3 Geometric mean plasma concentration-time profiles of rosuvastatin 20 mg when administered separately (open circle) or co-administered with telmisartan/amlodipine 80 mg/5 mg (closed circle). Notes: Linear (A) and semi-logarithmic (B) scale. Each point represents the geometric mean ±95% confidence intervals. |
Safety and tolerability of telmisartan, amlodipine, and rosuvastatin
In Cohort 1, thirteen AEs were reported from 12 subjects who were administered the investigational products at least once; these AEs included fatigue, headache, dizziness, and abdominal pain. One subject from Cohort 1 had a nail injury during the study period and was dropped out of the study because surgical intervention and concomitant medication were required. This AE was not related to the investigational products, and the subject recovered without sequelae. In Cohort 2, twelve AEs were reported from 7 subjects who were administered investigational products at least once; these AEs included dizziness, fatigue, and rash. (Table 2)
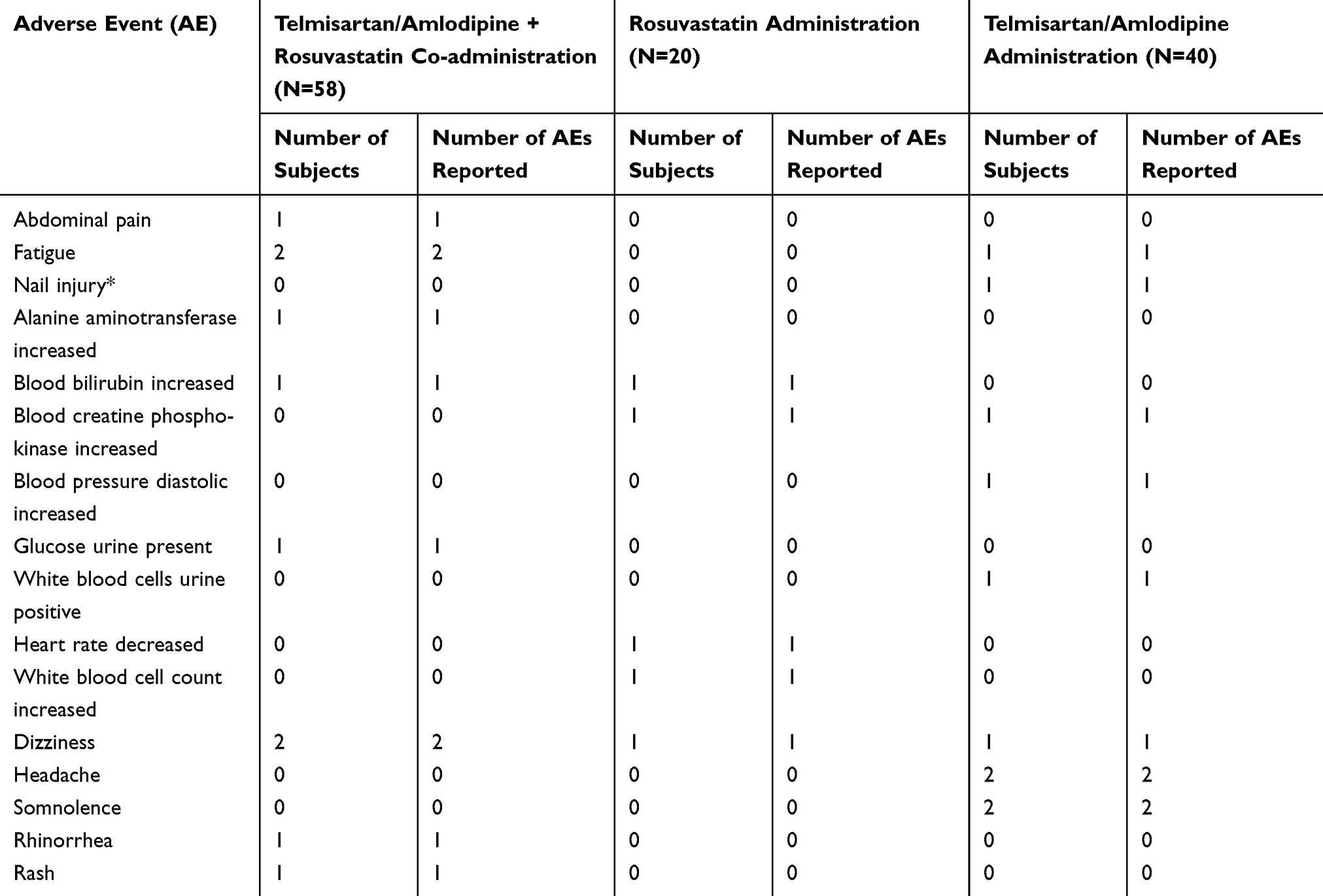 |
Table 2 Summary of adverse events (AEs) when telmisartan/amlodipine and rosuvastatin were administered separately or co-administered |
There were no serious AEs reported, and all the AEs were of mild severity. Any clinically significant changes in the laboratory test results or in the vital signs, such as increased blood bilirubin and bradycardia, were recovered spontaneously without further treatments by the end of the study. No clinically significant changes in the 12-lead ECGs and physical examination were reported.
Discussion
The pharmacokinetic parameters when telmisartan/amlodipine fixed dose combination tablet and rosuvastatin were administered separately or concurrently were compared. Subsequently, the calculated values of Cmax,ss and AUCτ,ss of telmisartan and amlodipine when co-administered with rosuvastatin were similar to the results obtained when they were administered alone as a fixed dose combination. For rosuvastatin, the Cmax,ss and AUCτ,ss values were increased by 128% and 33%, respectively, when rosuvastatin was administered concurrently with telmisartan/amlodipine.
The increased Cmax,ss and AUCτ,ss values of rosuvastatin reported in this study when rosuvastatin is administered with telmisartan/amlodipine are consistent with previous studies.14,15 The pharmacokinetic parameters of amlodipine were unchanged, also consistent with previous studies. However, unlike previous reports, rosuvastatin did not affect the pharmacokinetic parameters of telmisartan when administered concurrently in this study. The change in the absorption phase of rosuvastatin is evident (Figure 1) with a shortened Tmax,ss, and the mechanism of this change was speculated to be due to intervention in hepatic uptake and a possible change to biliary excretion transporters.15
Statins generally have low absolute bioavailability, which is indicative of extensive first-pass extraction.16 Rosuvastatin is not an exception, with the absolute bioavailability value of approximately 20%.17 It is also a known substrate for organic anion-transporting polyprotein 1B1/1B3 (OATP1B1/1B3) and breast cancer resistance protein (BCRP), a hepatic uptake transporter and an efflux transporter, respectively.13,18 Medications such as cyclosporine and some protease inhibitors are inhibitors of these transporters and significant pharmacokinetic interactions have already been reported. While rosuvastatin is being transported to the liver by OATP1B1 and 1B3, its uptake may be interrupted by telmisartan, as telmisartan and its metabolites are also transported by OATP1B3.19–21 Telmisartan and its metabolites can also compete for BCRP, which could explain the increase in plasma rosuvastatin exposure through the reduced efflux of rosuvastatin into bile. BCRP may also be inhibited by amlodipine,22 which could further increase plasma rosuvastatin exposure.
The clinical significance of the increased Cmax,ss and AUCτ,ss values of rosuvastatin is another matter. According to the prescribing information of rosuvastatin, there are several drug interaction studies that reported clinical significance; for example, cyclosporine increases the Cmax,ss and AUCτ,ss values of rosuvastatin 11 and 7-fold respectively and dose adjustment is necessary.13 This is because liver is the target organ for statins; increasing the plasma exposure of rosuvastatin has no therapeutic benefits, but rather increases the risk of myopathy.23 However, drugs such as darunavir/ritonavir and tipranavir/ritonavir were reported to increase the Cmax,ss and AUCτ,ss values of rosuvastatin to a certain extent (the former, 2.4 and 1.5-fold respectively; the latter, 2.2 and 1.4-fold respectively), but this interaction was not considered to be clinically significant and dose adjustment was not necessary.13 As this study reported similar increases to those reported by darunavir/ritonavir and tipranavir/ritonavir, the effect of telmisartan/amlodipine on the systemic exposure of rosuvastatin can also be considered as clinically insignificant.
The fact that rosuvastatin clearance is not significantly dependent on cytochrome P450 (CYP) 3A4 was a reason that rosuvastatin was selected in the current study.13 Statins such as simvastatin and lovastatin could show an increased systemic exposure when administered with CCBs such as amlodipine and diltiazem because of CYP3A4 related metabolism.24 Rosuvastatin, however, is not one of such statins. On the other hand, ARBs such as telmisartan rarely show significant interactions with CCBs or statins; only a few pharmacokinetic interactions between ARBs and statins had been reported, such as the one between fimasartan and atorvastatin.11,25,26 Although telmisartan/amlodipine was selected in our study because it was the best-selling antihypertensive combination in South Korea, further studies that investigate the pharmacokinetic interaction between ARBs, CCBs and statins may help in decision making process of developing new fixed dose combination.
The pharmacokinetic interaction was evaluated in this study by implementing a two-cohort, single-sequence crossover design. This design was needed because of amlodipine, a drug that has a longer elimination half-life of 30 to 50 hrs compared to the other two investigational products.12 A clinical trial design with a two-sequence crossover would have required more extensive blood sampling and longer study duration, which could be a burden for the study participants. Although the investigational products were generally well tolerated, and the reported AEs were expected symptoms and signs such as dizziness and fatigue, ethical considerations were taken to minimize the risks. Nevertheless, an appropriately designed two-sequence crossover study is needed to confirm the results of this study, because of a limitation that the study design implemented in our study enrolled different number of subjects between cohorts. The difference in sample size was because of the different intra-subject coefficient of variation (CV) used to calculate the sample size in two cohorts. In Cohort 1, the median value of telmisartan’s intra-subject CV, 30%, was used, which was greater than the intra-subject CV of rosuvastatin (20%) used to calculate the sample size in Cohort 2. Therefore, further studies that would implement two-sequence crossover design should consider this difference and calculate the adequate sample size.
Only male subjects were recruited in this study due to practical reasons, mainly that recruiting and assigning separate hospital wards for female participants were difficult in the current research site. Some previous studies have reported changes in pharmacokinetic characteristics of the investigational products according to gender and body mass,27,28 and there is a possibility that the results of this study might change if female participants were recruited. Further studies that involve equal number of male and female participants could be useful. On the other hand, the effect of BMI on pharmacokinetic parameters, namely Cmax,ss and AUCτ,ss, was evaluated using correlation analysis, and for each investigational product, BMI had weak to moderate negative correlation to the pharmacokinetic parameters (data not shown). However, the correlation coefficients did not change significantly between treatments, hence the difference in the pharmacokinetics of the co-administration when compared to separate administration was not due to BMI.
Conclusion
In conclusion, the pharmacokinetic parameters of telmisartan and amlodipine met the pharmacokinetic equivalent criteria, but the pharmacokinetic parameters of rosuvastatin were affected when telmisartan/amlodipine was administered in combination. The increase in systemic exposure of rosuvastatin caused by telmisartan/amlodipine co-administration would not be clinically significant in practice.
Data sharing statement
The individual deidentified participant data will not be shared due to the sponsor’s (Yuhan Corporation) request.
Funding
This study was sponsored by Yuhan Corporation, Republic of Korea.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
Yeji Lim is a paid employee of Yuhan Corporation. The authors report no other conflicts of interest in this work.
References
1. World Health Organization Cardiovascular Disease Fact Sheet. Geneva: World Health Organization; 2017. Available from: https://www.who.int/en/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds). Accessed March 27, 2019.
2. Dalal JJ, Padmanabhan TN, Jain P, Patil S, Vasnawala H, Gulati A. LIPITENSION: interplay between dyslipidemia and hypertension. Indian J Endocrinol Metab. 2012;16(2):240–245. doi:10.4103/2230-8210.93742
3. Castelli WP, Anderson K. A population at risk. Prevalence of high cholesterol levels in hypertensive patients in the framingham study. Am J Med. 1986;80(2A):23–32.
4. Jackson R, Lawes CM, Bennett DA, Milne RJ, Rodgers A. Treatment with drugs to lower blood pressure and blood cholesterol based on an individual’s absolute cardiovascular risk. Lancet. 2005;365(9457):434–441. doi:10.1016/S0140-6736(05)17833-7
5. Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American college of cardiology/American heart association task force on clinical practice guidelines. J Am Coll Cardiol. 2018;71(19):e127–e248. doi:10.1016/j.jacc.2017.11.006
6. Goff DC
7. National Clinical Guideline Centre (UK). Lipid Modification: Cardiovascular Risk Assessment and the Modification of Blood Lipids for the Primary and Secondary Prevention of Cardiovascular Disease. London: National Institute for Health and Care Excellence (UK); 2014. (NICE Clinical Guidelines, No. 181.). Available from: https://www.ncbi.nlm.nih.gov/books/NBK248067/. accessed March 27, 2019.
8. Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA guideline on the management of blood cholesterol: a report of the American college of cardiology/American heart association task force on clinical practice guidelines. J Am Coll Cardiol. 2018. Epub. doi:10.1016/j.jacc.2018.11.003
9. James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the eighth Joint National Committee (JNC 8). JAMA. 2014;311(5):507–520. doi:10.1001/jama.2013.284427
10. Wald DS, Law M, Morris JK, Bestwick JP, Wald NJ. Combination therapy versus monotherapy in reducing blood pressure: meta-analysis on 11,000 participants from 42 trials. Am J Med. 2009;122(3):290–300. doi:10.1016/j.amjmed.2008.09.038
11. TWYNSTA® (Telmisartan/Amlodipine) Tablets: US Prescribing Information. Ridgefield (CT): Boehringer Ingelheim Pharmaceuticals Inc.; Oct 2009.
12. NORVASC® (Amlodipine Besylate) Tablets: US Prescribing Information. New York (NY): Pfizer Inc.; Jan 2010.
13. CRESTOR® (Rosuvastatin Calcium) Tablets: US Prescribing Information. Gaithersburg (MD): AstraZeneca Pharmaceuticals LP; May 2016.
14. Son M, Kim Y, Lee D, et al. Pharmacokinetic interaction between rosuvastatin and telmisartan in healthy Korean male volunteers: a randomized, open-label, two-period, crossover, multiple-dose study. Clin Ther. 2014;36(8):1147–1158. doi:10.1016/j.clinthera.2014.06.007
15. Son M, Guk J, Kim Y, et al. Pharmacokinetic interaction between rosuvastatin, telmisartan, and amlodipine in healthy male Korean subjects: a randomized, open-label, multiple-dose, 2-period crossover study. Clin Ther. 2016;38(8):1845–1857. doi:10.1016/j.clinthera.2016.06.011
16. Schachter M. Chemical, pharmacokinetic and pharmacodynamic properties of statins: an update. Fundam Clin Pharmacol. 2005;19(1):117–125. doi:10.1111/j.1472-8206.2004.00299.x
17. Martin PD, Warwick MJ, Dane AL, Brindley C, Short T. Absolute oral bioavailability of rosuvastatin in healthy white adult male volunteers. Clin Ther. 2003;25(10):2553–2563.
18. Ho RH, Tirona RG, Leake BF, et al. Drug and bile acid transporters in rosuvastatin hepatic uptake: function, expression, and pharmacogenetics. Gastroenterology. 2006;130(6):1793–1806. doi:10.1053/j.gastro.2006.02.034
19. Ishiguro N, Maeda K, Kishimoto W, et al. Predominant contribution of OATP1B3 to the hepatic uptake of telmisartan, an angiotensin II receptor antagonist, in humans. Drug Metab Dispos. 2006;34(7):1109–1115. doi:10.1124/dmd.105.009175
20. Ishiguro N, Maeda K, Saito A, et al. Establishment of a set of double transfectants coexpressing organic anion transporting polypeptide 1B3 and hepatic efflux transporters for the characterization of the hepatobiliary transport of telmisartan acylglucuronide. Drug Metab Dispos. 2008;36(4):796–805. doi:10.1124/dmd.107.018903
21. Miura M, Satoh S, Inoue K, Saito M, Habuchi T, Suzuki T. Telmisartan pharmacokinetics in Japanese renal transplant recipients. Clin Chim Acta. 2009;399(1–2):83–87. doi:10.1016/j.cca.2008.09.020
22. Takara K, Matsubara M, Yamamoto K, et al. Differential effects of calcium antagonists on ABCG2/BCRP-mediated drug resistance and transport in SN-38-resistant HeLa cells. Mol Med Rep. 2012;5(3):603–609. doi:10.3892/mmr.2011.734
23. Petyaev IM. Improvement of hepatic bioavailability as a new step for the future of statin. Arch Med Sci. 2015;11(2):406–410. doi:10.5114/aoms.2015.50972
24. Wiggins BS, Saseen JJ, Page RL
25. Choi Y, Lee S, Jang IJ, Yu KS. Pharmacokinetic interaction between fimasartan and atorvastatin in healthy male volunteers. Drug Des Devel Ther. 2018;12:2301–2309. doi:10.2147/DDDT.S165171
26. Bohler S, Pittrow D, Bramlage P, Kirch W. Drug interactions with angiotensin receptor blockers. Expert Opin Drug Saf. 2005;4(1):7–18.
27. Zhou YT, Yu LS, Zeng S, Huang YW, Xu HM, Zhou Q. Pharmacokinetic drug-drug interactions between 1,4-dihydropyridine calcium channel blockers and statins: factors determining interaction strength and relevant clinical risk management. Ther Clin Risk Manag. 2014;10:17–26. doi:10.2147/TCRM.S55512
28. Abad-Santos F, Novalbos J, Galvez-Mugica MA, et al. Assessment of sex differences in pharmacokinetics and pharmacodynamics of amlodipine in a bioequivalence study. Pharmacol Res. 2005;51(5):445–452. doi:10.1016/j.phrs.2004.11.006
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.