Back to Journals » Drug Design, Development and Therapy » Volume 17
Pharmacokinetic Interactions Between Bazedoxifene and Cholecalciferol: An Open-Label, Randomized, Crossover Study in Healthy Male Volunteers
Authors Lee MH ![]() , Yoon SK, Kim H
, Yoon SK, Kim H ![]() , Cho YS, Han S
, Cho YS, Han S ![]() , Lee SH
, Lee SH ![]() , Bae KS
, Bae KS ![]() , Jung J
, Jung J ![]() , Hong SH
, Hong SH ![]() , Lim HS
, Lim HS
Received 7 December 2022
Accepted for publication 14 March 2023
Published 12 April 2023 Volume 2023:17 Pages 1107—1114
DOI https://doi.org/10.2147/DDDT.S399264
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tuo Deng
Moon Hee Lee,1 Seok-Kyu Yoon,1 Hyungsub Kim,2 Yong-Soon Cho,3 Sungpil Han,4 Shi Hyang Lee,1 Kyun-Seop Bae,1 Jina Jung,5 Sung Hee Hong,5 Hyeong-Seok Lim1
1Department of Clinical Pharmacology and Therapeutics, Asan Medical Center, University of Ulsan, Seoul, Republic of Korea; 2Department of Emergency Medical Services, College of Health Sciences, Eulji University, Seongnam, Republic of Korea; 3Department of Pharmacology and Clinical Pharmacology, Inje University College of Medicine, Busan, Republic of Korea; 4Department of Pharmacology, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea; 5Hanmi Pharmaceutical Co. Ltd., Seoul, Republic of Korea
Correspondence: Hyeong-Seok Lim, Department of Clinical Pharmacology and Therapeutics, Asan Medical Center, University of Ulsan, 88 Olympic-Ro 43-Gil, Songpa-Gu, Seoul, 05505, Republic of Korea, Tel +82-2-3010-4613, Fax +82-2-3010-4623, Email [email protected]
Purpose: The combined administration of bazedoxifene, a tissue-selective estrogen receptor modulator, and cholecalciferol can be a promising therapeutic option for postmenopausal osteoporosis patients. This study aimed to examine the pharmacokinetic interactions between these two drugs and the tolerability of their combined administration in healthy male subjects.
Patients and Methods: Thirty male volunteers were randomly assigned to one of the six sequences comprised of three treatments: bazedoxifene 20 mg monotherapy, cholecalciferol 1600 IU monotherapy, and combined bazedoxifene and cholecalciferol therapy. For each treatment, a single dose of the investigational drug(s) was administered orally, and serial blood samples were collected to measure the plasma concentrations of bazedoxifene and cholecalciferol. Pharmacokinetic parameters were calculated using the non-compartmental method. The point estimate and 90% confidence interval (CI) of the geometric mean ratio (GMR) were obtained to compare the exposures of combined therapy and monotherapy. The pharmacokinetic parameters compared were the maximum plasma concentration (Cmax) and the area under the plasma concentration-time curve from time zero to the last quantifiable concentration (AUClast). The safety and tolerability of the combined therapy were assessed in terms of the frequency and severity of adverse events (AEs).
Results: For bazedoxifene, the GMR (90% CI) of the combined therapy to monotherapy was 1.044 (0.9263– 1.1765) for Cmax and 1.1329 (1.0232– 1.2544) for AUClast. For baseline-adjusted cholecalciferol, the GMR (90% CI) of the combined therapy to monotherapy was 0.8543 (0.8005– 0.9117) for Cmax and 0.8056 (0.7445– 0.8717) for AUClast. The frequency of AEs observed was not significantly different between the combined therapy and monotherapy, and their severity was mild in all cases.
Conclusion: A mild degree of pharmacokinetic interaction was observed when bazedoxifene and cholecalciferol were administered concomitantly to healthy male volunteers. This combined therapy was well tolerated at the dose levels used in the present study.
Keywords: bazedoxifene, cholecalciferol, drug-drug interaction, pharmacokinetics, tolerability
Introduction
Osteoporosis is a skeletal disorder characterized by low bone mass and an increased risk of bone fracture. Bone mass reaches its peak in young adulthood, and increased bone resorption relative to bone formation leads to the lowering of bone mass. According to the World Health Organization, osteoporosis is defined as hip or lumbar spine bone marrow density of more than 2.5 standard deviations below the mean found in the young-adult population.1 Osteoporosis is a significant public health concern among the elderly due to the increased morbidity and mortality associated with bone fractures. It affects both sexes and all races, and its prevalence is expected to rise as the global population continues to age.1
The pharmacologic agents for the prevention and treatment of osteoporosis include calcium, vitamin D, bisphosphonates, calcitonin, estrogen, selective estrogen receptor modulator (SERM), parathyroid hormone, and anti-receptor activator of nuclear factor-kappa B ligand antibody (denosumab).2 The therapeutic potential of new treatment approaches, such as exosomes derived from endothelial cells or mesenchymal stem cells, has been investigated recently in animal models.3,4
Bazedoxifene, a third-generation SERM, exhibits tissue-selective action, functioning as an agonist in skeletal tissue but as an antagonist in breast and uterine tissues.5,6 Bazedoxifene has been approved for the treatment of postmenopausal osteoporosis by the European Medicines Agency, and conjugated estrogens/bazedoxifene have been approved for the prevention of postmenopausal osteoporosis by the United States Food and Drug Administration.7,8 Cholecalciferol, commonly known as vitamin D3, plays an important role in bone metabolism. Cholecalciferol is converted to calcifediol (25-hydroxycholecalciferol) in the liver and then to calcitriol (1,25-dihydroxycholecalciferol), the active form of vitamin D, in the kidney. Although vitamin D can be obtained from dietary intake and synthesized in the skin after exposure to sunlight, its deficiency is common. The National Osteoporosis Foundation recommends 800–1000 IU of vitamin D intake per day for individuals aged 50 and older.1
A fixed-dose combination formulation of bazedoxifene and cholecalciferol is a potentially promising therapeutic option for postmenopausal osteoporosis patients as it can improve treatment efficacy and medication compliance. Before developing a fixed-dose combination formulation, the pharmacokinetic (PK) interactions between bazedoxifene and cholecalciferol need to be assessed. This study aimed to examine the PK interactions between these drugs as well as their safety and tolerability when co-administered in healthy male subjects.
Materials and Methods
Study Design
The study was designed as an open-label, randomized, three-period, three-treatment, six-sequence, crossover clinical trial. Healthy male volunteers aged between 19 and 40 years with body mass index (BMI) between 19 and 28 kg/m2 were eligible for inclusion. Subjects were screened based on past medical history, physical examination including vital signs (blood pressure, heart rate, and body temperature), urine drug screening, clinical laboratory tests, serology tests, and 12-lead electrocardiogram (ECG). Subjects with a history of venous thromboembolism, hypercalciuria, renal stone, hepatobiliary disease, galactose intolerance, drug abuse, or clinically significant hypersensitivity reaction were excluded.
A total of 30 subjects were randomly assigned to six sequences comprised of three treatments: one tablet of 20 mg bazedoxifene (Viviant®; Pfizer Ltd., Seoul, Korea), two tablets of 800 IU cholecalciferol (HGP1501; Hanmi Pharmaceutical Co. Ltd., Seoul, Korea), or one tablet of 20 mg bazedoxifene along with two tablets of 800 IU cholecalciferol (Table 1). Outpatient visits were scheduled on day −10 of period 1 and day −9 of periods 2 and 3. At that time, subjects were provided with sunscreens (sun protection factor 50) and diaries to record their diet and activity. Subjects were asked to limit their exposure to sunlight by applying sunscreen and covering themselves with clothes and hats for outdoor activities. Subjects were required to refrain from taking dietary supplements and foods high in vitamin D content. Between two consecutive periods, there was a washout period of at least 14 days. These subjects were admitted to the Clinical Trial Center at Asan Medical Center (Seoul, Korea) the day before drug administration. The test drugs were administered orally under fasting conditions with 150 mL of water. After receiving the investigational drug(s), subjects were required to fast for four hours. Depending on the treatment, subjects were discharged on either day 2 (bazedoxifene monotherapy) or day 6 (cholecalciferol monotherapy or combined therapy). A follow-up visit was scheduled two weeks after the last dose.
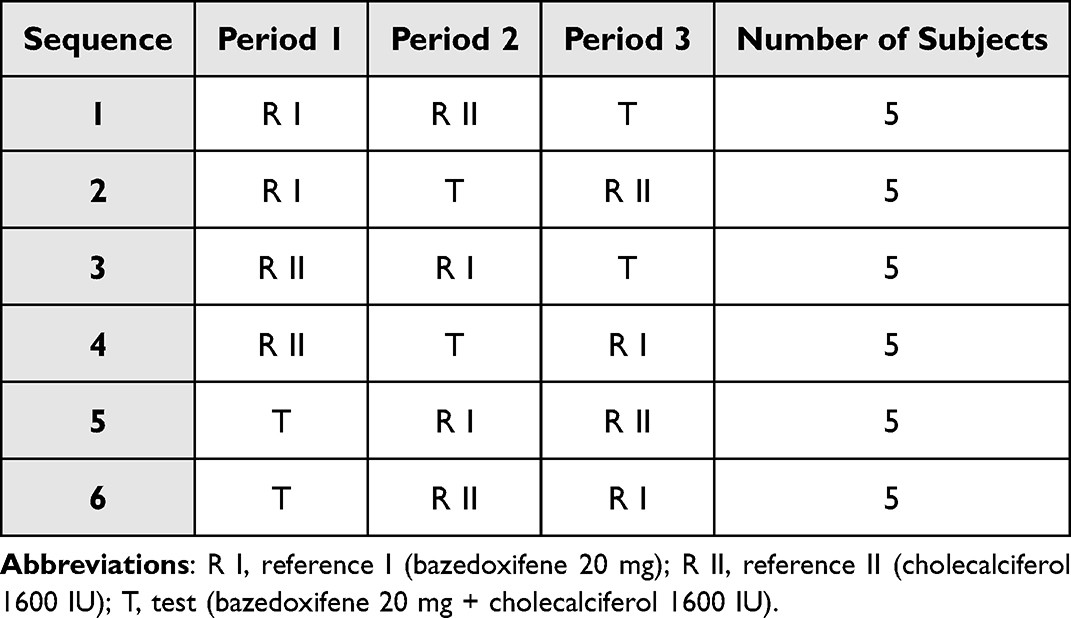 |
Table 1 Overall Study Design |
To determine the plasma bazedoxifene concentration, serial blood samples were collected at 0 (pre-dose), 1, 1.5, 2, 3, 4, 5, 6, 8, 10, 12, 14, 24, 48, 72, 96, and 120 hours after the dosing. To measure the baseline cholecalciferol level, blood samples were collected at 16, 12, 8, and 0 hours before the cholecalciferol dosing, and the average concentration for each individual was used as the baseline cholecalciferol concentration. Baseline-adjusted cholecalciferol concentrations were obtained by subtracting the baseline from the post-dose plasma cholecalciferol concentrations measured at 1, 1.5, 2, 3, 4, 5, 6, 8, 10, 12, 14, 16, 24, 48, 72, 96 and 120 hours after the treatment. If the baseline-adjusted cholecalciferol concentration had a negative value, zero was assigned.
Blood samples used for the drug concentration measurements were drawn into ethylenediaminetetraacetic acid K2 tubes. Plasma was separated by centrifugation at 1800 × g for 8 minutes at 4 °C and stored in Eppendorf tubes at −70 °C until analysis. At the analytical laboratory (BioCore Co. Ltd., Seoul, Korea), samples were thawed at room temperature. The plasma concentrations of bazedoxifene and cholecalciferol were assayed using validated liquid chromatography with tandem mass spectrometry (LC-MS/MS). Bazedoxifene samples were prepared by liquid-liquid extraction, and cholecalciferol samples by protein precipitation and solid-phase extraction. Liquid chromatography was conducted using a Shimadzu UFLC system (Shimadzu Corp., Kyoto, Japan). For tandem mass spectrometry, a SCIEX TQ5500 mass spectrometer (AB Sciex LLC, MA, USA) was used. The calibration curves covered the ranges of 0.1–20 ng/mL for bazedoxifene and 0.1–10 ng/mL for cholecalciferol. For bazedoxifene, the accuracy of LC-MS/MS was 91.8–113.0%, and the precision was 0.1–5.5%. For cholecalciferol, the accuracy of LC-MS/MS was 92.7–105.6%, and the precision was 0.2–4.5%. The lower limit of quantification was 0.1 ng/mL for both compounds.
The study protocol was approved by the Institutional Review Board (IRB) of Asan Medical Center (IRB number: 2017–0227) and by the Korean Ministry of Food and Drug Safety. The study was registered at ClinicalTrials.gov (NCT03089112). All subjects provided written informed consent before receiving screening tests. All study procedures were conducted in accordance with the ethical principles stated in the Declaration of Helsinki and by the Good Clinical Practice Guidelines of the International Council for Harmonisation.9,10 The study was conducted from March 31, 2017 to June 16, 2017.
Pharmacokinetic Analysis
The PK parameters of bazedoxifene and cholecalciferol in each subject were analyzed by the non-compartmental method using Phoenix WinNonlin® version 6.4 (Certara, NJ, USA). This analysis was based on the actual sampling time. The maximum plasma concentration (Cmax) and the time to reach Cmax (Tmax) were determined from the observed values. The terminal elimination rate constant (λz) was estimated by linear regression analysis of the terminal portion of the semilogarithmic concentration-time curve. The terminal elimination half-life (t1/2β) was calculated as the natural log of two divided by λz. Demographic data and PK parameters were summarized using descriptive statistics. The Cmax and the values for the area under the plasma concentration-time curve from time zero to the last quantifiable concentration (AUClast) were log-transformed to compare the drug exposure between the combined therapy and monotherapy. The point estimate and 90% confidence interval (CI) for the geometric mean ratio (GMR) of the combined therapy to monotherapy were obtained for Cmax and AUClast.
Safety and Tolerability Assessment
Safety and tolerability were assessed throughout the study by physical examinations, laboratory tests (complete blood count, blood chemistry, and urinalysis), 12-lead ECG, and monitoring of adverse events (AEs). AEs were coded according to the Medical Dictionary for Regulatory Activities (MedDRA® version 19.1) and recorded in terms of symptom/sign, onset, duration, severity, relationship to the investigational drug(s), action taken, and outcome.
Results
Study Participants
Of the 30 study participants who received the investigational drug(s) at least once, 27 subjects completed the study (Figure 1). Two subjects withdrew their consent to participate, and one subject was excluded at the investigator’s discretion due to a medical need for concomitant medication that could potentially affect the PK data. Participant demographics, including age, weight, height, and BMI, are summarized in Table 2. The mean ± standard deviation (SD) values were 28.63 ± 4.18 years for age, 71.53 ± 6.99 kg for weight, 173.55 ± 4.80 cm for height, and 23.75 ± 2.09 kg/m2 for BMI. All subjects who received the investigational drug(s) at least once were included in the safety and tolerability assessment.
 |
Table 2 Demographic Characteristics of the Participants (n=30) |
 |
Figure 1 Subject disposition. |
Pharmacokinetic Findings
The 27 subjects who completed the study were included in the PK analysis set, and the PK parameters are presented in Table 3. For bazedoxifene, the Cmax values (mean ± SD) for monotherapy and combined therapy were 3.30 ± 0.92 ng/mL and 3.62 ± 1.39 ng/mL, respectively. The AUClast values (mean ± SD) for monotherapy and combined therapy were 44.32 ± 22.24 h∙ng/mL and 50.78 ± 24.98 h∙ng/mL, respectively. The mean plasma concentration-time profiles of bazedoxifene for monotherapy and combined therapy nearly overlapped (Figure 2A). For bazedoxifene, the GMR (90% CI) of the combined therapy to monotherapy was 1.044 (0.9263–1.1765) for Cmax and 1.1329 (1.0232–1.2544) for AUClast (Table 4).
 |
Table 3 Pharmacokinetic Parameters of Bazedoxifene and Baseline-Adjusted Cholecalciferol in Healthy Male Subjects (n=27) |
 |
Table 4 Geometric Mean Ratios of Combined Therapy to Monotherapy for AUClast and Cmax |
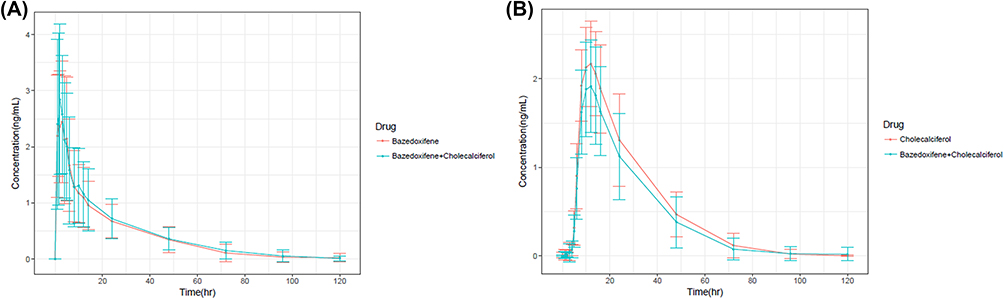 |
Figure 2 Mean plasma concentration-time curves: (A) bazedoxifene (B) baseline-adjusted cholecalciferol. The error bars denote standard deviations. |
For baseline-adjusted cholecalciferol, the Cmax values (mean ± SD) for monotherapy and combined therapy were 2.25 ± 0.47 ng/mL and 1.95 ± 0.54 ng/mL, respectively. The AUClast values (mean ± SD) for monotherapy and combined therapy were 59.43 ± 22.95 h∙ng/mL and 49.18 ± 24.40 h∙ng/mL, respectively. The mean plasma concentration-time profiles of baseline-adjusted cholecalciferol for monotherapy and combined therapy are shown in Figure 2B. For baseline-adjusted cholecalciferol, the GMR (90% CI) of combined therapy to monotherapy was 0.8543 (0.8005–0.9117) for Cmax and 0.8056 (0.7445–0.8717) for AUClast (Table 4).
Safety and Tolerability Findings
Seventeen subjects showed a total of 26 AEs after drug administration (Table 5). No serious AE occurred throughout the entire study. All AEs were mild in severity and resolved without any sequelae. The most common AE was nasopharyngitis (five events in five subjects). Clinically significant findings from the physical examination were phlebitis of the arm and venipuncture site bruise. Clinically significant laboratory abnormalities included increased blood levels of creatine phosphokinase and triglyceride and decreased blood levels of neutrophil count. No clinically significant abnormalities were found with respect to vital signs and 12-lead ECG. Twenty-five AEs were considered to have no or unlikely relationship with the investigational drugs. One AE, fatigue observed after combined therapy, was considered to have a possible relationship with the administered drugs.
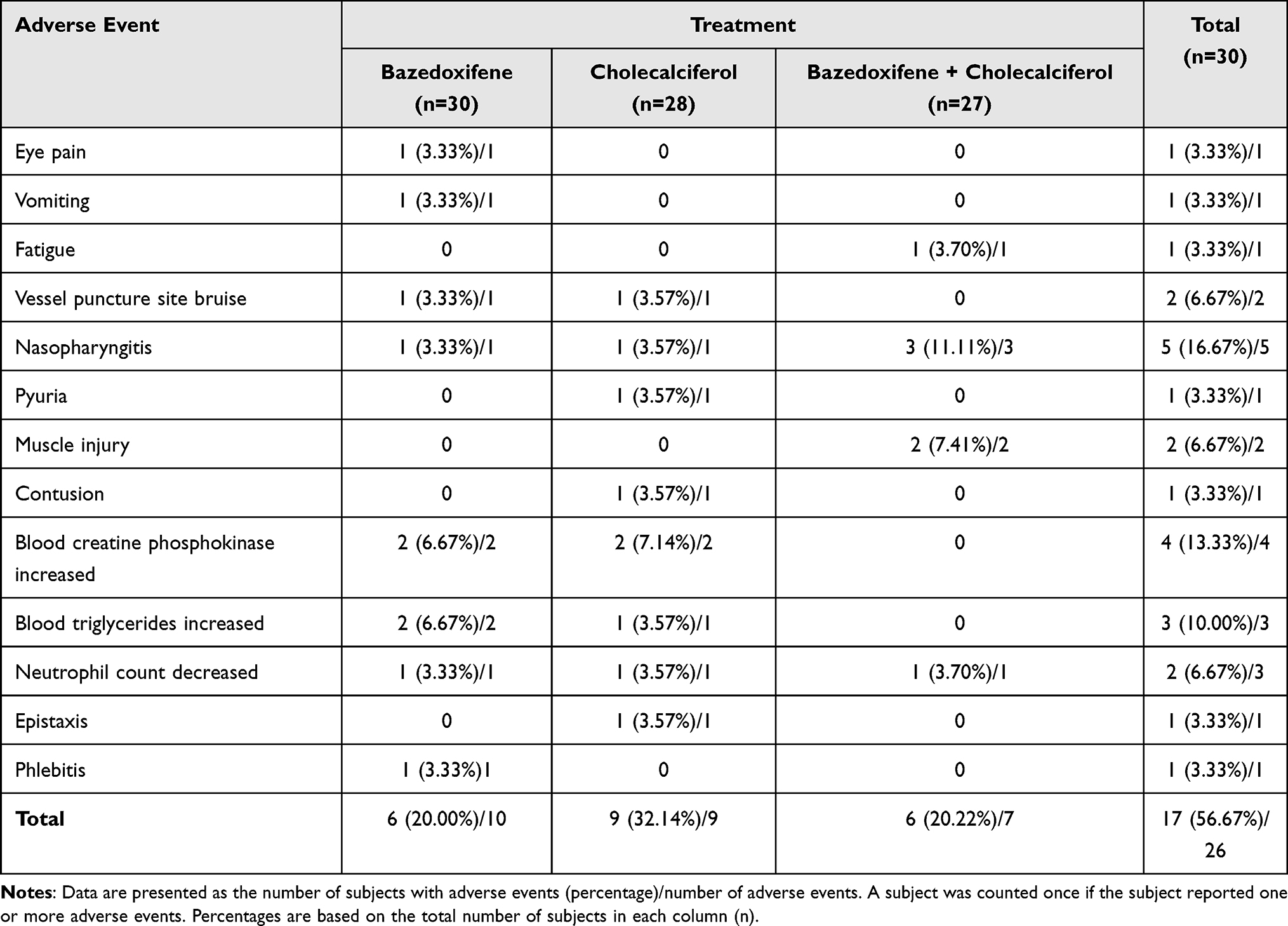 |
Table 5 Adverse Events in the Study Population After Drug Administration |
Discussion
This study investigated the PK characteristics of bazedoxifene and cholecalciferol, their PK interactions, and the safety and tolerability of combined therapy with these drugs in healthy male subjects.
The terminal elimination half-life of bazedoxifene was approximately 27 hours, and that of cholecalciferol was 13 hours in our study. The washout period of 14 days should therefore have been sufficient for both investigational drugs to be fully eliminated by the next period. The blood samples obtained up to 120 hours after dosing provided sufficient information for characterizing the exposures to bazedoxifene and cholecalciferol.
Previous studies on bazedoxifene pharmacokinetics have indicated a Tmax of 1–2 hours and a half-life of approximately 28 hours.11 As shown in Figure 2 and Table 3, bazedoxifene was rapidly absorbed when administered alone or in combination with cholecalciferol, showing median Tmax values of 2.00 h and 1.53 h, respectively. The Tmax of cholecalciferol is known to be approximately 15 hours. In our study, the median Tmax of cholecalciferol was 11.98 h when administered alone, similar to the 12.00 h value found for its co-administration with bazedoxifene.
In a recent study on bazedoxifene, the mean Cmax and AUClast in healthy male subjects after a single 20 mg oral dose were 3.191 ng/mL and 44.697 h·ng/mL, respectively.12 These numbers are consistent with the results of the current study (3.30 ng/mL and 44.32 h·ng/mL). The PK parameters Cmax and AUClast were used in our analyses to compare the combined therapy and monotherapy exposures. With bazedoxifene, the 90% CI for the GMR of the combined therapy to bazedoxifene monotherapy for Cmax fell within the 0.80–1.25 range, and for AUClast it was nearly within the above-mentioned range.
In the case of cholecalciferol, the AUClast was lower when this drug was co-administered with bazedoxifene, as indicated by the GMR of 0.8056 and associated 90% CI of 0.7445–0.8717. Bazedoxifene and cholecalciferol are drugs that exhibit wide therapeutic ranges.13–15 Cholecalciferol is known to reach a sigmoidal dose-response curve plateau at a dose of 600 IU.15 Hence, based on the GMRs observed in our exploratory study, the difference in the AUClast for cholecalciferol is unlikely to have clinical significance in treatment efficacy at the dose level used in our protocol.
All of the AEs observed in our study population were mild, and the frequency of AEs in subjects who received combined therapy was not significantly different from that in subjects who received monotherapy. The most common AE observed in our present trial cohort was nasopharyngitis, which we considered unrelated to the investigational drugs.
One limitation of the present study was that the participants were all healthy men. The study was exploratory in nature, and male subjects were included to facilitate enrollment and minimize health risks to subjects. Drug-drug interaction studies are often conducted with male subjects, and the results are applied to women as well as men because gender does not seem to affect the pattern of drug-drug interaction for many drugs. Assuming that the PK interactions would follow the same pattern in men and women, this study was conducted in men instead of women. Additional studies in postmenopausal women with osteoporosis and patients with different pathophysiological conditions will help further characterize the PK interactions between bazedoxifene and cholecalciferol.
Conclusion
The combined therapy of 20 mg bazedoxifene (one tablet) and 1600 IU cholecalciferol (two tablets of 800 IU) was safe and well tolerated in healthy male subjects. In this present study, the oral co-administration of bazedoxifene with cholecalciferol tended to decrease the cholecalciferol exposure slightly. Considering that both drugs have wide therapeutic ranges, dose adjustment of cholecalciferol may not be necessary for its co-administration with bazedoxifene.
Abbreviations
AE, adverse event; AUClast, area under the concentration-time curve from time zero to the last quantifiable concentration; BMI, body mass index; CI, confidence interval; Cmax, maximum plasma concentration; ECG, electrocardiogram; GMR, geometric mean ratio; IRB, Institutional Review Board; LC-MS/MS, liquid chromatography with tandem mass spectrometry; λz, terminal elimination rate constant; PK, pharmacokinetic; SD, standard deviation; SERM, selective estrogen receptor modulator; Tmax, time to reach Cmax; t1/2β, terminal elimination half-life.
Data Sharing Statement
The authors do not intend to share individual de-identified participant data of this study due to confidentiality.
Funding
This study was sponsored by Hanmi Pharmaceutical Co. Ltd.
Disclosure
Hyeong-Seok Lim has received grants from Hanmi Pharmaceutical Co. Ltd. for a range of research projects, including the study reported in this article. Jina Jung and Sung Hee Hong are employees of Hanmi Pharmaceutical Co. Ltd. The remaining authors declare no competing interests in relation to this article.
References
1. Cosman F, de Beur SJ, LeBoff MS, et al. National Osteoporosis Foundation. Clinician’s guide to prevention and treatment of osteoporosis. Osteoporos Int. 2014;25(10):2359–2381. doi:10.1007/s00198-014-2794-2
2. Rejnmark L, Mosekilde L. New and emerging antiresorptive treatments in osteoporosis. Curr Drug Saf. 2011;6(2):75–88. doi:10.2174/157488611795684686
3. Song H, Li X, Zhao Z, et al. Reversal of osteoporotic activity by endothelial cell-secreted bone targeting and biocompatible exosomes. Nano Lett. 2019;19(5):3040–3048. doi:10.1021/acs.nanolett.9b00287
4. Zeng ZL, Xie H. Mesenchymal stem cell-derived extracellular vesicles: a possible therapeutic strategy for orthopaedic diseases: a narrative review. Biomater Transl. 2022;3(3):175–187. doi:10.12336/biomatertransl.2022.03.002
5. Komm BS, Kharode YP, Bodine PV, Harris HA, Miller CP, Lyttle CR. Bazedoxifene acetate: a selective estrogen receptor modulator with improved selectivity. Endocrinology. 2005;146(9):3999–4008. doi:10.1210/en.2005-0030
6. Stump AL, Kelley KW, Wensel TM. Bazedoxifene: a third-generation selective estrogen receptor modulator for treatment of postmenopausal osteoporosis. Ann Pharmacother. 2007;41(5):833–839. doi:10.1345/aph.1H428
7. Conbriza. European medicines agency; 2009. Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/conbriza.
8. DUAVEE. Drug Label (NDA 022247). Silver Spring, MD: US Food and Drug Administration; 2013.
9. World Medical Association. World medical association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
10. Guideline for Good Clinical Practice E6(R2). International council for harmonisation of technical requirements for pharmaceuticals for human use; 2016. Available from: https://database.ich.org/sites/default/files/E6_R2_Addendum.pdf.
11. Gatti D, Rossini M, Sblendorio I, Lello S. Pharmacokinetic evaluation of bazedoxifene for the treatment of osteoporosis. Expert Opin Drug Metab Toxicol. 2013;9(7):883–892. doi:10.1517/17425255.2013.794221
12. Yeun JS, Kan HS, Lee M, et al. Pharmacokinetic comparison of two bazedoxifene acetate 20 mg tablet formulations in healthy Korean male volunteers. Transl Clin Pharmacol. 2020;28(2):102–108. doi:10.12793/tcp.2020.28.e7
13. Archer DF, Pinkerton JV, Utian WH, et al. Bazedoxifene, a selective estrogen receptor modulator: effects on the endometrium, ovaries, and breast from a randomized controlled trial in osteoporotic postmenopausal women. Menopause. 2009;16(6):1109–1115. doi:10.1097/gme.0b013e3181a818db
14. Kawate H, Takayanagi R. Efficacy and safety of bazedoxifene for postmenopausal osteoporosis. Clin Interv Aging. 2011;6:151–160. doi:10.2147/CIA.S15711
15. Institute of Medicine. Dietary Reference Intakes for Calcium and Vitamin D. Washington, DC: The National Academies Press; 2011.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.