Back to Journals » The Application of Clinical Genetics » Volume 12
Pharmacogenetics of alcohol addiction: current perspectives
Authors Zastrozhin MS ![]() , Skryabin VY
, Skryabin VY ![]() , Miroshkin SS
, Miroshkin SS ![]() , Bryun EA, Sychev DA
, Bryun EA, Sychev DA
Received 25 February 2019
Accepted for publication 10 June 2019
Published 11 July 2019 Volume 2019:12 Pages 131—140
DOI https://doi.org/10.2147/TACG.S206745
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Martin Maurer
M S Zastrozhin,1,2 V Yu Skryabin,1 S S Miroshkin,1,2 E A Bryun,1,2 D A Sychev1,2
1Moscow Research and Practical Centre on Addictions of the Moscow Department of Healthcare, Moscow 109390, Russian Federation; 2Department of Addictology, Russian Medical Academy of Continuous Professional Education of the Ministry of Health of the Russian Federation, Moscow 123995, Russian Federation
Abstract: Genetics of alcohol addiction is currently a contradictive and complex field, where data in the most studies reflect methods’ limitations rather than meaningful and complementary results. In our review, we focus on the genetics of alcohol addiction, leaving genetics of acute alcohol intoxication out of the scope. A review of the literature on pharmacogenetic biomarkers development for the pharmacotherapy personalization reveals that today the evidence base concerning these biomarkers is still insufficient. In particular, now the researches with the design of randomized controlled trials and meta-analysis investigating the effect of the SNPs as biomarkers on the therapy efficacy are available for naltrexone only. For other medications, there are only a few studies in small samples. It decreases the possibilities to implement the pharmacogenetic algorithms for the pharmacotherapy personalization in patients with alcohol use disorders (AUD). In view of the importance of the precision approaches development not in addiction medicine only, but in other fields of medicine also to increase the efficacy and safety of the therapy, studies on pharmacogenetic biomarkers development for the medications used in patients with AUD (eg, naltrexone, disulfiram, nalmefene, acamprosate, etc.) remain relevant to this day.
Keywords: pharmacogenetics, pharmacogenomics, alcohol use disorder, naltrexone, acamprosate, nalmefene
Introduction
According to the latest data, harmful alcohol use resulted in an estimated 3 million deaths or 5.3% of all global deaths.1 Their leading causes are digestive diseases (21.3%), unintentional injuries (20.9%), cardiovascular diseases and diabetes (19.0%), infectious diseases (12.9%) and malignant neoplasms (12.6%).1
As with other addictive disorders, genetics influence alcohol use disorder (AUD) to a considerable degree, with heritability estimates of more than 60%.2,3 Previous reviews on the subject4,5 demonstrated that the advances in the field of pharmacogenetics in AUD are slow due to many difficulties and it is important to advance the precision medicine approaches for the treatment of AUD. According to available data of meta-analyses and systematic reviews, the following medications showed their efficacy in comparison with placebo: disulfiram,6 naltrexone,7 extended-release injectable naltrexone,7 acamprosate,7 nalmefene,8 baclofen,9 gabapentin,10 and topiramate.11 We may now consider the available scientific evidence bearing on the effects of single nucleotide polymorphisms (SNPs) on pharmacokinetics, pharmacodynamics, as well as on clinical efficacy and safety of the alcohol addiction treatment.
Disulfiram
Disulfiram exhibits an antidipsotropic effect. It inhibits the conversion of acetaldehyde, a toxic metabolite of alcohol, in acetic acid by blocking the aldehyde dehydrogenase 2 (ALDH2) in the liver and the brain, resulting in an accumulation of acetaldehyde.12 In addition, disulfiram inhibits dopamine β-hydroxylase (DβH) converting dopamine to norepinephrine.13 The DβH genetic polymorphism can affect the level of protein of the same name. In particular, 1021C>T polymorphism lowers the expression of DβH resulting in the reduced plasma DβH level.14 Thus, it was assumed that patients carrying this polymorphic marker would have a reduced plasma DβH level, which is likely to alter the efficacy of disulfiram in such patients: a lower baseline DβH level should enhance the disulfiram effect. Unfortunately, the only clinical trial enrolling 66 patients with alcohol addiction has not revealed any statistically significant difference neither in the efficacy level nor in the risk of adverse effects across the patients carrying T and C alleles.15 We also found another study conducted in patients with cocaine addiction that demonstrates a statistically significant effect of the polymorphism of the ankyrin repeat and kinase domain-containing 1 (ANKK1) genes and dopamine receptor D2 (DRD2) genes on disulfiram efficacy level.16 The investigation of these markers would probably allow developing recommendations on the personalized treatment of alcohol addiction with disulfiram to increase its efficacy and safety.
Thus, although disulfiram is included in the guidelines as a drug recommended for the alcohol addiction treatment, today there is no data on the pharmacogenetics of this medication. Further studies are required to develop the pharmacogenetic biomarkers affecting the efficacy and safety of disulfiram in patients suffering from alcohol addiction.
Naltrexone
Synthesized in 1963 by Endo laboratories, naltrexone is a nonspecific competitive opioid antagonist approved by The US Food and Drug Administration (FDA) for the treatment of alcohol addiction in 1994. It alters the subjective effects of ethanol intoxication and attenuates craving.17
Previous studies have suggested that genetic polymorphisms encoding μ-opioid receptors (OPRM1) may moderate the effect of naltrexone in patients suffering from alcohol addiction. Several works describe this gene as a predictor of both alcohol addiction and the efficacy of naltrexone treatment.18–23
There is the mixed evidence regarding the influence of the 118A>G functional polymorphism in the OPRM1 gene resulting in adenine (A) to guanine (G) substitution at the gene sequence position 118.24 Several studies19,25–31 demonstrated greater efficacy of naltrexone among the carriers of this polymorphism which has been associated with the increased binding affinity of the endogenous ligand β-endorphin for µ-opioid receptors.32 Meanwhile, other randomized clinical trials33–35 revealed no such pharmacogenetic effect. In addition, a recent systematic review that meta-analyzed eight eligible clinical studies found no significant difference between A allele homozygotes and those with at least one G allele.36 Hence, the effect of the 118A>G functional polymorphism on naltrexone response rates remains debatable.24
A study performed by Kranzler et al.37 showed that patients carrying GG genotype who are prone to the use of alcohol in the evenings and at night, against the background of naltrexone treatment, experienced a more pronounced reduction of craving at that time than the wild-type carriers did. According to a research conducted by Chen,31 patients carrying GG genotype who abuse alcohol and receive naltrexone, consume less alcohol after the treatment course in comparison with the patients who receive placebo or homozygous carriers of the wild-type allele A who also receive naltrexone.
However, the randomized clinical trial conducted by Schacht et al.24 demonstrated that the OPRM1 genotype did not significantly moderate the effects of naltrexone on drinking, but G-allele carriers who received naltrexone had an accelerated return to heavy drinking after the medication was stopped.
Evidence demonstrating the naltrexone efficacy in patients from various ethnic groups and of both genders is essential for practice. Setiawan et al.38 investigated the effect of 6-days treatment with naltrexone in 40 volunteers (20 males and 20 females) who were social drinkers aged 18–50. At the end of each treatment period, all patients received a single dose of their preferred alcoholic beverage with the opportunity to work for the additional alcohol units using a progressive ratio breakpoint paradigm. The results showed that naltrexone use resulted in the reduced stimulant and euphorigenic effects of the priming dose of alcohol, especially in women and carriers of the A118G polymorphism of the OPRM1 gene; the participants with both of these traits were considered the most sensitive.
Data on the frequency of genetic polymorphisms in different ethnic groups are of particular interest. Among whites, Bond et al.32 revealed that the expected frequencies of homozygous G118 and heterozygous subjects are 2% and 20%, respectively, with the allelic frequency of the G118 variant of 11.5%, regardless of gender. In Asians, the frequency of the G118 variant is higher and varies from 35 to 47%: 35% in Chinese, 44% in Thais, 45% in Malays, 47% in Indians,39 and more than 49% in Japanese.40
Pharmacogenetic aspects of naltrexone use in patients carrying the functional polymorphisms of OPRK1 (rs997917) and OPRD1 (rs4654327) genes, as well as the combination of the A118G polymorphism of the OPRM1 gene and the VNTR polymorphism of the human dopamine transporter (DAT1) gene, are not investigated sufficiently. Several studies indicate the potential of further research investigating the joint effect of these two systems on the intensity of subjective feelings of alcohol intoxication.17,34,41,42
A correlation between the functional polymorphisms of OPRK1 (rs997917) and OPRD1 (rs4654327) genes and the efficacy of naltrexone treatment (versus placebo) was revealed. The study conducted by Ashenhurst demonstrated the changes in subjective response to alcohol and the rate of alcohol craving.43 Of the two OPRK1 SNPs examined, rs997917 demonstrated a significant effect on the alcohol-induced sedation. The TT homozygous patients reported the reduced feelings of alcohol sedation during the naltrexone use as compared to the C allele-carriers. Moreover, pharmacogenetic effects were also observed for a SNP in the OPRD1 gene: carriers of the A allele at this locus reported greater naltrexone-induced blunting of alcohol stimulation and craving in comparison with the G-allele homozygous patients.
Krupitsky et al revealed that the efficacy of naltrexone treatment in patients suffering from opioid addiction was different across the patients carrying different allelic variants of the opioid receptor genes and dopaminergic system genes.44 Thus, patients carrying the combination of СС or СТ genotypes of OPRK1 and TT genotype of DRD2 demonstrated better response to treatment, whereas a combination of the A118G polymorphism of the OPRM1 gene and the VNTR polymorphism of the DAT1 gene showed a significant effect on the subjective feelings of alcohol intoxication.
Although numerous studies demonstrate the efficacy of the extended-release injectable naltrexone for the alcohol addiction treatment (in comparison with placebo),45–48 at the moment the effects of genetic factors on the extended-release injectable naltrexone efficacy are not investigated sufficiently.49
Due to the contradictory results of the studies investigating the efficacy of naltrexone in patients suffering from AUD,33,50 genetic testing is not commonly used in clinical practice today. Hence, there is a need to strengthen the evidence base.
Acamprosate
FDA has approved acamprosate for the alcohol addiction treatment in 2004. Although the results of numerous studies confirm the efficacy of acamprosate in the treatment of AUD,7 its exact mechanism of action is still uncertain. It seems to modulate NMDA receptor transmission and GABAA transmission.51
Adverse effects registered in clinical trials included diarrhea, dizziness, and headaches.52
A double-blind, placebo-controlled trial conducted by Kiefer53 demonstrated a statistically significant effect of the GATA4 rs13273672 SNP on the duration of remission in patients with alcohol addiction who receive acamprosate. It was found that patients with the mutant allele G show the reduced time to relapse in comparison with those carrying the AA genotype. No such effect was revealed in the groups of patients who received naltrexone or placebo.
This effect probably results from the fact that GATA4 encodes a transcription factor of atrial natriuretic peptide (ANP).54 It was confirmed in a study conducted by Kiefer who investigated the plasma level of the ANP.53 Research suggests that the reduced ANP levels contribute to the dysregulation of the stress and anxiogenic systems of the brain, which is commonly found in patients with alcohol addiction.55 It was assumed that acamprosate has a more pronounced effect on the duration of remission in patients carrying the A allele due to the differences in the ANP level across the patients with different genotypes.
Moreover, studies demonstrate the effect of GRIN2B encoding the NMDA receptor GluN2B subunit on the duration of remission in patients who receive acamprosate.56 This study included 225 patients with alcohol addiction. It revealed that the minor allele A of the rs2058878 polymorphism is associated with the longer remission in comparison with the G allele. Unfortunately, this study had a serious limitation due to the absence of a placebo group. Therefore, the study results were inconclusive regarding the effect of the GRIN2B polymorphism on the efficacy of acamprosate.
Thus, despite the lack of data on acamprosate pharmacogenetics, this medication is considered effective and safe for the treatment of patients with alcohol addiction.
Nalmefene
Nalmefene is a selective opioid receptor antagonist acting as a μ- and δ- receptor antagonist and a partial κ receptor agonist.57,58 Although structurally nalmefene is similar to naltrexone, it exhibits a higher bioavailability rate and a longer plasma half-life, with a lower risk of liver toxicity.59
FDA has approved nalmefene for opioid overdose only (www.fda.org). Several clinical trials conducted in the US have not demonstrated a higher efficacy of nalmefene in the treatment of patients with AUD as an anticraving therapy in comparison with placebo.60,61 At the same time, three multi-site clinical trials conducted in Europe, where nalmefene was approved for the treatment of patients with AUD by the European Medicines Agency in February 2013,58,60 showed its efficacy in alcohol consumption reduction across patients suffering from alcohol addiction with high levels of consumption (more than 60 grams/daily for men and more than 40 grams/daily for women).
Due to the structural similarity to naltrexone, the use of nalmefene is associated with similar common adverse effects. Similarly to naltrexone, nalmefene can induce nausea and vomiting, when compared with placebo.7 At present, studies to evaluate if gastrointestinal side effects could lead to treatment interruption are lacking.62 Insomnia, dizziness, headache, decreased attention and paresthesia have also been reported in association with nalmefene use.63
Nalmefene is mostly metabolized in the liver to nalmephene 3-O-glucuronide by the UGT2B7 enzyme (mainly) and by the UGT1A3 and UGT1A8 enzymes.64 CYP3A4 isoenzyme also partly converts nalmephene into 3-O-sulphate nalmefene and nornalmefene, which do not show any pharmacological effect.
No relevant pharmacokinetic interactions have been reported in clinical trials, but possible interactions with the potent UGT2B7 inhibitors, such as diclofenac and naproxene,65 ketoconazole,66 and low concentrations of amitriptyline,67 cannot be excluded. Contrarily, the concomitant use of the UGT2B7 inducer, such as different chemotherapeutic agents68 or dihydroartethmisine,69 may result in a decrease of plasma drug concentrations to the sub-therapeutic ranges.
Topiramate
Topiramate is a derivative of D-fructose, a naturally occurring monosaccharide.70 FDA has approved topiramate for the treatment of seizure disorder, migraine prevention, and chronic weight management (along with phentermine).61 Although the FDA has not currently approved topiramate for the AUD therapy, this medication is also a useful option for the AUD treatment.71 A randomized, double-blind, placebo-controlled trial revealed the anticraving properties of topiramate.72 Similar to other drugs used for the alcohol addiction treatment, it is thought to reduce mesolimbic dopaminergic activity.73
The use of topiramate is associated with the common adverse effects, such as paresthesia, dysgeusia, anorexia, difficulty with concentration or attention, nervousness, dizziness, and pruritus.74 The detailed analysis demonstrated that this medication causes the dose-related transient cognitive impairment including mental slowing and modest reductions in verbal fluency and working memory.75
Topiramate exerts effects through AMPA/kainate receptors containing the GluK1 and GluK2 subunits, which are encoded by genes GRIK1 and GRIK2, respectively.76 Kranzler et al revealed that the efficacy of topiramate is modulated by the SNP rs2832407 in GRIK1, the gene encoding the GluK1 receptor subunit.77,78 This provided the basis for studies of rs2832407 as a moderator of the response to topiramate. In addition, a previous pharmacogenetic analysis of the human laboratory pilot study79 showed that rs2832407 was associated with the severity of topiramate-induced side effects.80 The randomized clinical trial by Kranzler et al have not found an effect of the SNP on adverse events, suggesting that the kainate receptor does not play a unique role in mediating topiramate-related adverse effects.81
Topiramate may be a potential substrate for cytochrome P450 (CYP) 2C9, a CYP3A4 inducer and a CYP2C19 weak inhibitor.70 According to the package insert (Topina, Kyowa Hakko Kirin, Japan), this drug is chiefly metabolized by CYP3A4. Stiripentol is a potent inhibitor of CYP3A4, but interactions between topiramate and stiripentol have not been studied.82
Ondansetron
Ondansetron is a competitive serotonin 5-HT3 receptor antagonist.83 FDA has approved this medication for the prevention of nausea and vomiting caused by cancer chemotherapy, radiation therapy and surgery.84
The randomized controlled trial by Johnson et al demonstrated the efficacy of ondansetron in self-reported drinking reduction across the patients with the early-onset alcoholism.85 In this trial, patients who received ondansetron at low dosages (1 and 4 μg) have been found to reduce alcohol consumption and have increased abstinence.85 In the prospective, open-label study conducted by Kranzler et al, ondansetron given at a dose of 4 μg twice per day decreased the number of drinks per day, drinks per drinking day and alcohol-related problems in the early-onset alcohol-dependent patients, but not in the late-onset ones.86 However, according to the meta‐analysis of seven trials performed by Torrens et al, selective serotonin reuptake inhibitors are not effective in the treatment of AUD in patients without comorbid depression.87 Similarly, recent American Psychiatric Association (APA) practice guideline for the pharmacological treatment of patients with AUD do not recommend the use of any antidepressants unless the patient has a comorbid depression.88
Several studies demonstrated that genetic variations in the 5-HT transporter gene (SLC6A4) may modulate the severity of alcohol consumption and predict the treatment response to ondansetron.89–91 Johnson et al identified three genotypes in the HTR3A and HTR3B genes that were significantly associated with the efficacy of ondansetron treatment for AUD in European patients and showed that polymorphisms in the HTR3A-rs1150226-AG, HTR3A-rs1176713-GG, and/or HTR3B-rs17614942-AC genotypes, along with the SLC6A4-LL/TT genotypes, are predictors of the reduced drinking in response to ondansetron.90
Table 1 includes the data from all studies with statistically significant associations between the individual drug response and genetic polymorphism.
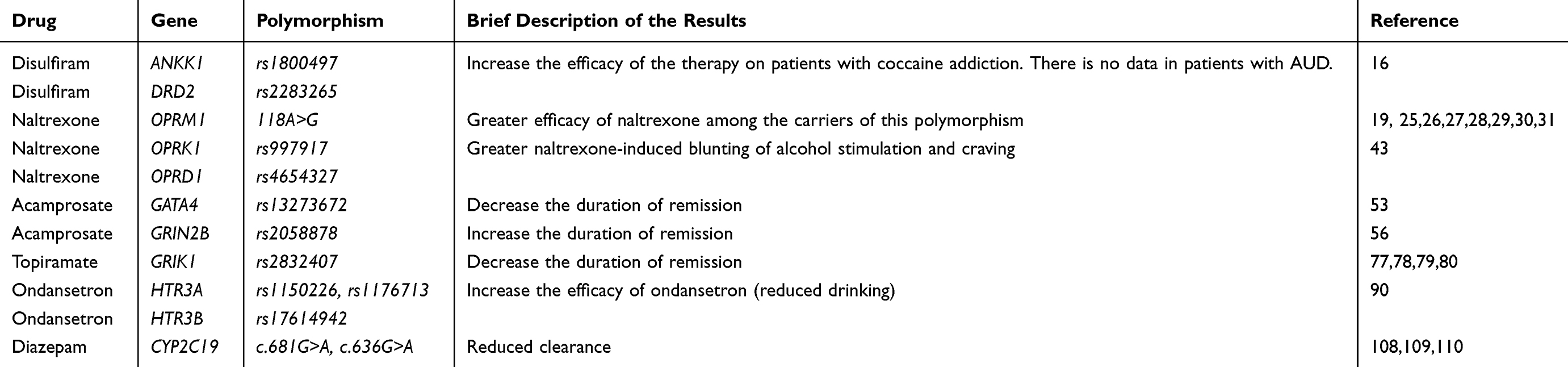 |
Table 1 The statistically significant associations between the individual drug response and genetic polymorphism |
Pharmacogenetics of alcohol withdrawal syndrome
Current researches strongly suggest that alcohol affects multiple neurotransmitter systems in the brain. It is well known that alcohol acts as a central nervous system (CNS) depressant since it enhances the activity of the major CNS inhibitory neurotransmitter, gamma-aminobutyric acid (GABA), and antagonizes the activity of the major CNS excitatory neurotransmitter, glutamate.92 When alcohol intake is abruptly reduced or discontinued, an overt hyperexcited state may follow. It manifests clinically by various symptoms and alcohol withdrawal syndrome (AWS) complications, ranging from mild tremor and anxiety to seizures, delirium tremens, and even death.93 AWS symptoms occur in more than 50% of patients with alcohol-related problems who require pharmacological treatment.94
Benzodiazepines have been used for the AWS therapy for more than 50 years.95 Benzodiazepines are effective due to the inhibitory GABA-signaling pathways stimulating, which is similar to the action of alcohol.96,97 Hence, these medications decrease the symptoms of AWS and shorten its course, along with the prevention of AWS-related seizures, delirium tremens, and death.96–98
There are currently 16 benzodiazepines licensed by the FDA. Diazepam was the second benzodiazepine to be used clinically (after chlordiazepoxide), after being approved for use in 1963.99 Diazepam and desmethyldiazepam, its active metabolite, have the most extended elimination half-lives, meaning that the levels of these substances decrease in a gradual, self-tapering manner, resulting in a reduced incidence and severity rates of the breakthrough symptoms and rebound phenomena.100 In the acute AWS, diazepam may provide symptomatic relief from agitation, tremor, delirium tremens, and hallucinations.
Benzodiazepines taken in toxic doses without other coingestants rarely cause a significant toxidrome.101 The classic presentation of an isolated benzodiazepine overdose consists of CNS depression with normal vital signs. At the same time, severe and fatal adverse events due to diazepam use are sporadic and are usually associated with interaction with other substances (such as opiates or alcohol).102 Chronic use of diazepam may result in tolerance, addiction and withdrawal syndrome.103
Diazepam is metabolized via CYP2C19 and CYP3A4 to desmethyldiazepam, which is found in the plasma at concentrations equivalent to diazepam. CYP2C9, CYP2B, and CYP3A5 are other isoenzymes involved in diazepam metabolism.104 It is thought that the variability in the clearance of many benzodiazepines, including diazepam, is due to the variability in CYP2C19 and CYP3A4 genotypes.104,105
The CYP2C19 gene is highly polymorphic, as 35 variant star (*) alleles are currently catalogued at the Human Cytochrome P450 (CYP) Allele Nomenclature Database.99 The CYP2C19*1 wild-type allele is associated with normal enzyme activity and the “normal metabolizer” phenotype, whereas the CYP2C19*17 allele is associated with increased enzyme activity and the “ultrarapid metabolizer” phenotype, respectively.106 CYP2C19*2 is the most common loss-of-function variant, containing a c.681G>A variant in exon 5. It results in an aberrant splice site and the production of a truncated, non-functioning protein. It is reported that the CYP2C19*2 allele frequencies are approximately 15% in Caucasians and Africans, and about 29–35% in Asians.106,107 CYP2C19*3 is another commonly tested loss-of-function variant, containing a c.636G>A variant in exon 4, which causes a premature stop codon. The CYP2C19*3 allele frequencies are about 2–9% in Asian populations, but rare in other racial groups. Other loss-of-function variants include CYP2C19*4-*8 and occur in less than 1% of the general population.106,107 “Intermediate CYP2C19 metabolizers” carry one copy of an allele encoding the reduced or absent function (eg, *1/*2), while “poor metabolizers” are homozygous or compound heterozygous for two loss-of-function alleles (eg, *2/*2, *2/*3).99 Studies have found that “poor metabolizers” have a lower plasma clearance of diazepam compared to “normal metabolizers”, and that diazepam had a longer plasma half-life in those individuals.108–110 One study found that CYP2C19 “poor metabolizers” took a longer period to emerge from general anesthesia than “normal” ones. This study also found that the “slow emergers” had lower levels of CYP3A4 mRNA.111 Despite the fact that CYP3A4 isoenzyme is also involved in the metabolism of diazepam, clinical studies investigating the effect of CYP3A4 and CYP3A5 variants on benzodiazepine metabolism show the conflicting results.112–115
Conclusion
A review of the literature on pharmacogenetic biomarkers development for the pharmacotherapy personalization reveals that today the evidence base concerning these biomarkers is still insufficient. In particular, now the researches with the design of randomized controlled trials and meta-analysis investigating the effect of the SNPs as biomarkers on the therapy efficacy are available for naltrexone only. For other medications, there are only a few studies. These studies are conducted on small cohorts of patients; sometime the placebo and/or control arms are missing; the design of the pharmacological study is not properly described, or the dose of the medication is not specific; different genetic variants can impact the treatment response. It strongly reduces the possibilities to implement the pharmacogenetic algorithms for the pharmacotherapy personalization in patients with AUD.
Thus, we believe that the low interest in the results of research in the field of pharmacogenetics of addictions could be increased by the following ways:
- Improve a research design according to higher levels of evidence by the Oxford CEBM Levels of Evidence so that it’ll be prospective, include the main group and the comparison group, and include blinding and randomization;
- Use the advanced research methods: next-generation sequencing, including Roche/454 Life Sciences, Illumina/Solexa, SOLiD and others;
- Develop meta-analyzes and systematic reviews, but this requires the results of more evidence-based research;
- Conducting pharmacoeconomic studies in the field of pharmacogenetics of addictions.
We would like to emphasize the importance of developing the pharmacogenetic decision support systems, which will allow implementing the results of research in the field of pharmacogenetics into clinical practice, resulting in the risk reduction of the adverse drug reactions and pharmacoresistance.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization.Global Status Report on Alcohol and Health 2018. Geneva: World Health Organization; 2018. Licence: CC BY-NC-SA 3.0 IGO.
2. Goldman D, Oroszi G, Ducci F. The genetics of addictions: uncovering the genes. Nat Rev Genet. 2005;6(7):521–532. doi:10.1038/nrg1635
3. Enoch MA, Goldman D. The genetics of alcoholism and alcohol abuse. Curr Psychiatry Rep. 2001;3(2):144–151.
4. Ramoz N, Schumann G, Gorwood P. Genetic and pharmacogenetic aspects of alcohol-dependence. Curr Pharmacogenom. 2006;4(1):19–32. doi:10.2174/157016006776055383
5. Rinker JA, Mulholland PJ. Promising pharmacogenetic targets for treating alcohol use disorder: evidence from preclinical models. Pharmacogenomics. 2017;18(6):555–570. doi:10.2217/pgs-2016-0193
6. Skinner MD, Lahmek P, Pham H, Aubin HJ. Disulfiram efficacy in the treatment of alcohol dependence: a meta-analysis. PLoS One. 2014;9(2):e87366. doi:10.1371/journal.pone.0087366
7. Jonas DE, Amick HR, Feltner C, et al. Pharmacotherapy for adults with alcohol use disorders in outpatient settings: a systematic review and meta-analysis. JAMA. 2014;311(18):1889–1900. doi:10.1001/jama.2014.3628
8. Palpacuer C, Duprez R, Huneau A, et al. Pharmacologically controlled drinking in the treatment of alcohol dependence or alcohol use disorders: a systematic review with direct and network meta-analyses on nalmefene, naltrexone, acamprosate, baclofen and topiramate. Addiction. 2018;113(2):220–237. doi:10.1111/add.13974
9. Pierce M, Sutterland A, Beraha EM, Morley K, van Den Brink W. Efficacy, tolerability, and safety of low-dose and high-dose baclofen in the treatment of alcohol dependence: a systematic review and meta-analysis. Eur Neuropsychopharmacol. 2018;28(7):795–806. doi:10.1016/j.euroneuro.2018.03.017
10. Mason BJ, Quello S, Goodell V, Shadan F, Kyle M, Begovic A. Gabapentin treatment for alcohol dependence: a randomized clinical trial. JAMA Intern Med. 2014;174(1):70–77. doi:10.1001/jamainternmed.2013.11950
11. Blodgett JC, Del Re AC, Maisel NC, Finney JW. A meta-analysis of topiramate’s effects for individuals with alcohol use disorders. Alcohol Clin Exp Res. 2014;38(6):1481–1488. doi:10.1111/acer.12411
12. Petersen EN. The pharmacology and toxicology of disulfiram and its metabolites. Acta Psychiatr Scand Suppl. 1992;369:7–13.
13. Barth KS, Malcolm RJ. Disulfiram: an old therapeutic with new applications. CNS Neurol Disord Drug Targets. 2010;9:5–12.
14. Cubells JF, Zabetian CP. Human genetics of plasma dopamine beta-hydroxylase activity: applications to research in psychiatry and neurology. Psychopharmacology (Berl). 2004;174:463–476. doi:10.1007/s00213-004-1840-8
15. Mutschler J, Abbruzzese E, Witt SH, et al. Functional polymorphism of the dopamine beta-hydroxylase gene is associated with increased risk of disulfiram-induced adverse effects in alcohol-dependent patients. J Clin Psychopharmacol. 2012;32(4):578–580. doi:10.1097/JCP.0b013e31825ddbe6
16. Spellicy CJ, Kosten TR, Hamon SC, Harding MJ, Nielsen DA. ANKK1 and DRD2 pharmacogenetics of disulfiram treatment for cocaine abuse. Pharmacogenet Genomics. 2013;23(7):333–340. doi:10.1097/FPC.0b013e328361c39d
17. Anton RF, Voronin KK, Randall PK, Myrick H, Tiffany A. Naltrexone modification of drinking effects in a subacute treatment and bar-lab paradigm: influence of OPRM1 and dopamine transporter (SLC6A3) genes. Alcohol Clin Exp Res. 2012;36(11):2000–2007. doi:10.1111/j.1530-0277.2012.01807.x
18. Samochowiec A, Samochowiec J, Pełka-Wysiecka J, et al. The role of OPRM1 polymorphism in the etiology of alcoholism. Adv Clin Exp Med. 2019;28(2):199–202. doi:10.17219/acem/78592
19. Anton RF, Oroszi G, O’Malley S, et al. An evaluation of mu-opioid receptor (OPRM1) as a predictor of naltrexone response in the treatment of alcohol dependence: results from the Combined Pharmacotherapies and Behavioral Interventions for Alcohol Dependence (COMBINE) study. Arch Gen Psychiatry. 2008;65(2):135–144. doi:10.1001/archpsyc.65.2.135
20. Bouza C, Angeles M, Muñoz A, Amate JM. Efficacy and safety of naltrexone and acamprosate in the treatment of alcohol dependence: a systematic review. Addiction. 2004;99(7):811–828. Review. Erratum in: Addiction. 2005 Apr;100(4):573.Magro, Angeles [corrected to Angeles, Magro]. doi:10.1111/j.1360-0443.2004.00763.x
21. Kranzler HR, Van Kirk J. Efficacy of naltrexone and acamprosate for alcoholism treatment: a meta-analysis. Alcohol Clin Exp Res. 2001;25(9):1335–1341.
22. Rösner S, Hackl-Herrwerth A, Leucht S, Vecchi S, Srisurapanont M, Soyka M. Opioid antagonists for alcohol dependence. Cochrane Database Syst Rev. 2010;8(12):CD001867.
23. Schacht JP, Anton RF, Voronin KE, et al. Interacting effects of naltrexone and OPRM1 and DAT1 variation on the neural response to alcohol cues. Neuropsychopharmacology. 2012;38:414–422. doi:10.1038/npp.2012.195
24. Schacht JP, Randall PK, Latham PK, et al. Predictors of naltrexone response in a randomized trial: reward-related brain activation, OPRM1 genotype, and smoking status. Neuropsychopharmacology. 2017;42(13):2640–2653. doi:10.1038/npp.2017.74
25. Chamorro AJ, Marcos M, Miron-Canelo JA, Pastor I, Gonzalez-Sarmiento R, Laso FJ. Association of micro-opioid receptor (OPRM1) gene polymorphism with response to naltrexone in alcohol dependence: a systematic review and meta-analysis. Addict Biol. 2012;17(3):505–512. doi:10.1111/j.1369-1600.2012.00442.x
26. Oslin DW, Berrettini W, Kranzler HR, et al. A functional polymorphism of the mu-opioid receptor gene is associated with naltrexone response in alcohol-dependent patients. Neuropsychopharmacology. 2003;28(8):1546–1552. doi:10.1038/sj.npp.1300219
27. Kranzler HR, Armeli S, Covault J, Tennen H. Variation in OPRM1 moderates the effect of desire to drink on subsequent drinking and its attenuation by naltrexone treatment. Addict Biol. 2013;18(1):193–201. doi:10.1111/j.1369-1600.2012.00471.x
28. McGeary JE, Monti PM, Rohsenow DJ, Tidey J, Swift R, Miranda R
29. Kim SG, Kim CM, Choi SW, et al. A micro opioid receptor gene polymorphism (A118G) and naltrexone treatment response in adherent Korean alcohol-dependent patients. Psychopharmacology (Berl). 2009;201(4):611–618. doi:10.1007/s00213-008-1330-5
30. Ooteman W, Naassila M, Koeter MW, et al. Predicting the effect of naltrexone and acamprosate in alcohol-dependent patients using genetic indicators. Addict Biol. 2009;14(3):328–337. doi:10.1111/j.1369-1600.2009.00159.x
31. Chen AC, Morgenstern J, Davis CM, Kuerbis AN, Covault J, Kranzler HR. Variation in mu-opioid receptor gene (OPRM1) as a moderator of naltrexone treatment to reduce heavy drinking in a high functioning cohort. J Alcohol Drug Depend. 2013;1(1):101.
32. Bond C, LaForge KS, Tian M, et al. Single-nucleotide polymorphism in the human mu opioid receptor gene alters beta-endorphin binding and activity: possible implications for opiate addiction. Proc Natl Acad Sci U S A. 1998;95(16):9608–9613. doi:10.1073/pnas.95.16.9608
33. Coller JK, Cahill S, Edmonds C, et al. OPRM1 A118G genotype fails to predict the effectiveness of naltrexone treatment for alcohol dependence. Pharmacogenet Genomics. 2011;21(12):902–905. doi:10.1097/FPC.0b013e32834c5445
34. Gelernter J, Gueorguieva R, Kranzler HR, et al.; VA Cooperative Study No.425 Study Group. Opioid receptor gene (OPRM1, OPRK1, and OPRD1) variants and response to naltrexone treatment for alcohol dependence: results from the VA cooperative study. Alcohol Clin Exp Res. 2007;31(4):555–563. doi:10.1111/j.1530-0277.2007.00339.x
35. Oslin DW, Leong SH, Lynch KG, et al. Naltrexone vs placebo for the treatment of alcohol dependence: a randomized clinical trial. JAMA Psychiatry. 2015;72(5):430–437. doi:10.1001/jamapsychiatry.2014.3053
36. Jonas DE, Amick HR, Feltner C, et al. Genetic polymorphisms and response to medications for alcohol use disorders: a systematic review and meta-analysis. Pharmacogenomics. 2014;15(13):1687–1700. doi:10.2217/pgs.14.121
37. Kranzler HR, Edenberg HJ. Pharmacogenetics of alcohol and alcohol dependence treatment. Curr Pharm Des. 2010;16:2141–2148. doi:10.2174/138161210791516387
38. Setiawan E, Pihl RO, Cox SM, et al. The effect of naltrexone on alcohol’s stimulant properties and self-administration behavior in social drinkers: influence of gender and genotype. Alcohol Clin Exp Res. 2011;35(6):1134–1141. doi:10.1111/j.1530-0277.2011.01446.x
39. Tan EC, Tan CH, Karupathivan U, Yap EP. Mu opioid receptor gene polymorphisms and heroin dependence in Asian populations. Neuroreport. 2003;14(4):569–572. doi:10.1097/01.wnr.0000061020.47393.fc
40. Gelernter J, Kranzler H, Cubells J. Genetics of two mu opioid receptor gene (OPRM1) exon I polymorphisms: population studies, and allele frequencies in alcohol- and drug-dependent subjects. Mol Psychiatry. 1999;4(5):476–483.
41. Fuke S, Suo S, Takahashi N, Koike H, Sasagawa N, Ishiura S. The VNTR polymorphism of the human dopamine transporter (DAT1) gene affects gene expression. Pharmacogenom J. 2001;1(2):152–156. doi:10.1038/sj.tpj.6500026
42. Ray LA, Bujarski S, Squeglia LM, Ashenhurst JR, Anton RF. Interactive effects of OPRM1 and DAT1 genetic variation on subjective responses to alcohol. Alcohol Alcohol. 2014;49:261–270. doi:10.1093/alcalc/agt183
43. Ashenhurst JR, Bujarski S, Ray LA. Delta and kappa opioid receptor polymorphisms influence the effects of naltrexone on subjective responses to alcohol. Pharmacol Biochem Behav. 2012;103(2):253–259. doi:10.1016/j.pbb.2012.08.019
44. Krupitsky ЕМ, Kibitov АО, Blokhina ЕА, et al. Stabilization of remission in patients with opioid dependence with naltrexone implant: a pharmacogenetic approach. Zh Nevrol Psikhiatr Im S S Korsakova. 2015;115(4 Pt 2):14–23. doi:10.17116/jnevro20151154214-23
45. Rohsenow DJ, Monti PM, Hutchison KE, Swift RM, Colby SM, Kaplan GB. Naltrexone’s effects on reactivity to alcohol cues among alcoholic men. J Abnorm Psychol. 2000;109(4):738–742.
46. Mannelli P, Peindl K, Masand PS, Patkar AA. Long-acting injectable naltrexone for the treatment of alcohol dependence. Expert Rev Neurother. 2007;7(10):1265–1277. doi:10.1586/14737175.7.10.1265
47. Johnson BA, Ait-Daoud N, Aubin HJ, et al. A pilot evaluation of the safety and tolerability of repeat dose administration of long-acting injectable naltrexone (Vivitrex) in patients with alcohol dependence. Alcohol Clin Exp Res. 2004;28(9):1356–1361.
48. Beatty A, Stock C. Efficacy of long-acting, injectable versus oral naltrexone for preventing admissions for alcohol use disorder. Ment Health Clin. 2018;7(3):106–110. doi:10.9740/mhc.2017.05.106
49. Helton SG, Lohoff FW. Pharmacogenetics of alcohol use disorders and comorbid psychiatric disorders. Psychiatry Res. 2015;230(2):121–129. doi:10.1016/j.psychres.2015.09.019
50. Mitchell JM, Fields HL, White RL, Meadoff TM, Joslyn G, Rowbotham MC. The Asp40 mu-opioid receptor allele does not predict naltrexone treatment efficacy in heavy drinkers. J Clin Psychopharmacol. 2007;27:112–115. doi:10.1097/JCP.0b013e31802e68b0
51. Kalk NJ, Lingford-Hughes AR. The clinical pharmacology of acamprosate. Br J Clin Pharmacol. 2014;77(2):315–323. doi:10.1111/bcp.12070
52. Caputo F, Vignoli T, Grignaschi A, Cibin M, Addolorato G, Bernardi M. Pharmacological management of alcohol dependence: from mono-therapy to pharmacogenetics and beyond. Eur Neuropsychopharmacol. 2014;24(2):181–191. doi:10.1016/j.euroneuro.2013.10.004
53. Kiefer F, Witt SH, Frank J, et al. Involvement of the atrial natriuretic peptide transcription factor GATA4 in alcohol dependence, relapse risk and treatment response to acamprosate. Pharmacogenomics J. 2011;11(5):368–374. doi:10.1038/tpj.2010.51
54. McBride K, Nemer M. Regulation of the ANF and BNP promoters by GATA factors: lessons learned for cardiac transcription. Can J Physiol Pharmacol. 2001;79(8):673–681.
55. Jorde A, Bach P, Witt SH, et al. Genetic variation in the atrial natriuretic peptide transcription factor GATA4 modulates amygdala responsiveness in alcohol dependence. Biol Psychiatry. 2014;75(10):790–797. doi:10.1016/j.biopsych.2013.10.020
56. Karpyak VM, Biernacka JM, Geske JR, et al. Genetic markers associated with abstinence length in alcohol-dependent subjects treated with acamprosate. Transl Psychiatry. 2014;7(4):e462.
57. Swift RM. Naltrexone and nalmefene: any meaningful difference?. Biol Psychiatry. 2013;73:700–701.
58. Soyka M, Lieb M. Recent developments in pharmacotherapy of alcoholism. Pharmacopsychiatry. 2015;48:123–135. doi:10.1055/s-0035-1547237
59. Franck J, Jayaram-Lindström N. Pharmacotherapy for alcohol dependence: status of current treatments. Curr Opin Neurobiol. 2013;23:692–699. doi:10.1016/j.conb.2013.05.005
60. Lyon J. More treatments on deck for alcohol use disorder. JAMA. 2017;317:2267–2269. doi:10.1001/jama.2017.5254
61. Shen WW. Anticraving therapy for alcohol use disorder: A clinical review. Neuropsychopharmacol Rep. 2018;38(3):105–116. doi:10.1002/npr2.12028
62. Antonelli M, Ferrulli A, Sestito L, et al. Alcohol addiction – the safety of available approved treatment options. Expert Opin Drug Saf. 2018;17(2):169–177. doi:10.1080/14740338.2018.1404025
63. Gual A, He Y, Torup L, van Den Brink W, Mann K. ESENSE 2 study group. A randomised, double-blind, placebo-controlled, efficacy study of nalmefene, as-needed use, in patients with alcohol dependence. Eur Neuropsychopharmacol. 2013;23:1432–1442. doi:10.1016/j.euroneuro.2013.02.006
64. Guerzoni S, Pellesi L, Pini LA, Caputo F. Drug-drug interactions in the treatment for alcohol use disorders: A comprehensive review. Pharmacol Res. 2018;133:65–76.
65. Joo J, Kim YW, Wu Z, et al. Screening of non-steroidal anti-inflammatory drugs for inhibitory effects on the activities of six UDP-glucuronosyltransferases (UGT1A1, 1A3, 1A4, 1A6, 1A9 and 2B7) using LC-MS/MS. Biopharm Drug Dispos. 2015;36:258–264. doi:10.1002/bdd.1933
66. Takeda S, Kitajima Y, Ishii Y, et al. Inhibition of UDP-glucuronosyltransferase 2b7-catalyzed morphine glucuronidation by ketoconazole: dual mechanisms involving a novel noncompetitive mode. Drug Metab Dispos. 2006;34:1277–1282. doi:10.1124/dmd.106.009738
67. Uchaipichat V, Mackenzie PI, Elliot DJ, Miners JO. Selectivity of substrate (trifluoperazine) and inhibitor (amitriptyline, androsterone, canrenoic acid, hecogenin, phenylbutazone, quinidine, quinine, and sulfinpyrazone) “probes” for human udpglucuronosyltransferases. Drug Metab Dispos. 2006;34:449–456. doi:10.1124/dmd.105.007369
68. Hu DG, Mackenzie PI, Lu L, Meech R, Mckinnon RA. Induction of human UDP-Glucuronosyltransferase 2B7 gene expression by cytotoxic anticancer drugs in liver cancer HepG2 cells. Drug Metab Dispos. 2015;43:660–668. doi:10.1124/dmd.114.062380
69. Zang M, Zhu F, Zhao L, et al. The effect of UGTs polymorphism on the auto-induction phase II metabolism-mediated pharmacokinetics of dihydroartemisinin in healthy Chinese subjects after oral administration of a fixed combination of dihydroartemisininpiperaquine. Malar J. 2014;13:478. doi:10.1186/1475-2875-13-478
70. Guglielmo R, Martinotti G, Quatrale M, et al. Topiramate in alcohol use disorders: review and update. CNS Drugs. 2015;29(5):383–395. doi:10.1007/s40263-015-0244-0
71. Manhapra A, Chakraborty A, Arias AJ. Topiramate pharmacotherapy for alcohol use disorder and other addictions: a narrative review. J Addict Med. 2019;13(1):7–22. doi:10.1097/ADM.0000000000000443
72. Johnson BA, Ait-Daoud N, Bowden CL, et al. Oral topiramate for treatment of alcohol dependence: a randomised controlled trial. Lancet. 2003;361:1677–1685. doi:10.1016/S0140-6736(03)13370-3
73. Goh ET, Morgan MY. Review article: pharmacotherapy for alcohol dependence - the why, the what and the wherefore. Aliment Pharmacol Ther. 2017;45(7):865–882. doi:10.1111/apt.13965
74. Johnson BA, Rosenthal N, Capece JA, et al.; Topiramate for Alcoholism Advisory Board; Topiramate for Alcoholism Study Group. Topiramate for treating alcohol dependence: a randomized controlled trial. JAMA. 2007;298(14):1641–1651. doi:10.1001/jama.298.14.1641
75. Knapp CM, Ciraulo DA, Sarid-Segal O, et al. Zonisamide, topiramate, and levetiracetam: efficacy and neuropsychological effects in alcohol use disorders. J Clin Psychopharmacol. 2015;35(1):34–42. doi:10.1097/JCP.0000000000000246
76. White HS, Brown SD, Woodhead JH, Skeen GA, Wolf HH. Topiramate modulates GABA-evoked currents in murine cortical neurons by a nonbenzodiazepine mechanism. Epilepsia. 2000;41(Suppl 1):S17–S20.
77. Morley KC, Kranzler HR, Luquin N, et al. Topiramate versus naltrexone for alcohol use disorder: study protocol for a genotype-stratified, double-blind randomised controlled trial (TOP study). Trials. 2018;19(1):443. doi:10.1186/s13063-018-2824-z
78. Kranzler HR, Armeli S, Wetherill R, et al. Self-efficacy mediates the effects of topiramate and GRIK1 genotype on drinking. Addict Biol. 2016;21(2):450–459. doi:10.1111/adb.12207
79. Miranda R
80. Ray LA, Miranda R
81. Kranzler HR, Armeli S, Feinn R, Tennen H, Gelernter J, Covault J. GRIK1 genotype moderates topiramate's effects on daily drinking level, expectations of alcohol's positive effects, and desire to drink. Int J Neuropsychopharmacol. 2014 Oct;17(10):1549-56. doi:10.1017/S1461145714000510. Epub 2014 Apr 30.
82. Yamamoto Y, Takahashi Y, Imai K, Kagawa Y, Inoue Y. Effect of CYP inducers/inhibitors on topiramate concentration: clinical value of therapeutic drug monitoring. Ther Drug Monit. 2017;39(1):55–61. doi:10.1097/FTD.0000000000000367
83. Shen WW. Clinical Psychopharmacology for the 21st Century.
84. Attilia F, Perciballi R, Rotondo C, et al.; Interdisciplinary Study Group CRARL - SITAC - SIPaD - SITD - SIPDip. Pharmacological treatment of alcohol use disorder. Scientific evidence. Riv Psichiatr. 2018;53(3):123–127. doi:10.1708/2925.29414
85. Johnson BA, Roache JD, Javors MA, et al. Ondansetron for reduction of drinking among biologically predisposed alcoholic patients: a randomized controlled trial. JAMA. 2000;284(8):963–971.
86. Kranzler HR, Pierucci-Lagha A, Feinn R, Hernandez-Avila C. Effects of ondansetron in early- versus late-onset alcoholics: a prospective, open-label study. Alcohol Clin Exp Res. 2003;27(7):1150–1155. doi:10.1097/01.ALC.0000075547.77464.76
87. Torrens M, Fonseca F, Mateu G, Farré M. Efficacy of antidepressants in substance use disorders with and without comorbid depression: a systematic review and meta‐analysis. Drug Alcohol Depend. 2005;78:1–22. doi:10.1016/j.drugalcdep.2004.09.004
88. Reus VI, Fochtmann LJ, Bukstein O, et al. The American Psychiatric Association practice guideline for the pharmacological treatment of patients with alcohol use disorder. Am J Psychiatry. 2018;175:86–90. doi:10.1176/appi.ajp.2017.1750101
89. Johnson BA, Ait-Daoud N, Seneviratne C, et al. Pharmacogenetic approach at the serotonin transporter gene as a method of reducing the severity of alcohol drinking. Am J Psychiatry. 2011;168(3):265–275. doi:10.1176/appi.ajp.2011.11020284
90. Johnson BA, Seneviratne C, Wang XQ, Ait-Daoud N, Li MD. Determination of genotype combinations that can predict the outcome of the treatment of alcohol dependence using the 5-HT(3) antagonist ondansetron. Am J Psychiatry. 2013;170(9):1020–1031. doi:10.1176/appi.ajp.2013.12091163
91. Soyka M, Müller CA. Pharmacotherapy of alcoholism - an update on approved and off-label medications. Expert Opin Pharmacother. 2017;18(12):1187–1199. doi:10.1080/14656566.2017.1349098
92. Erdozain AM, Callado LF. Neurobiological alterations in alcohol addiction: a review. Adicciones. 2014;26(4):360–370.
93. Schuckit MA. Recognition and management of withdrawal delirium (Delirium Tremens). N Engl J Med. 2014;371(22):2109–2113. doi:10.1056/NEJMoa1410490
94. Saitz R. Clinical practice. Unhealthy alcohol use. N Engl J Med. 2005;352:596–607. doi:10.1056/NEJMcp042262
95. Kaim SC, Kaim SC, Klett CJ, Klett CJ, Rothfeld B, Rothfeld B. Treatment of the acute alcohol withdrawal state: a comparison of four drugs. Am J Psychiatry. 1969;125(12):1640–1646. doi:10.1176/ajp.125.12.1640
96. Perry EC. Inpatient management of acute alcohol withdrawal syndrome. CNS Drugs. 2014;28(5):401–410. doi:10.1007/s40263-014-0163-5
97. Mirijello A, D’Angelo C, Ferrulli A, et al. Identification and management of alcohol withdrawal syndrome. Drugs. 2015;75(4):353–365. doi:10.1007/s40265-015-0358-1
98. Mayo-Smith MF, Beecher LH, Fischer TL, et al.; Working Group on the Management of Alcohol Withdrawal Delirium, Practice Guidelines Committee, American Society of Addiction Medicine. Management of alcohol withdrawal delirium. An evidence-based practice guideline. Arch Intern Med. 2004;164(13):1405–1412. doi:10.1001/archinte.164.13.1405
99. Dean L. Diazepam Therapy and CYP2C19 Genotype. In: Pratt V, McLeod H, Rubinstein W, Dean L, Kattman B, Malheiro A, editors. Medical Genetics Summaries. Bethesda (MD): National Center for Biotechnology Information (US); 2012–2016 Aug 25.
100. Weintraub SJ. Diazepam in the treatment of moderate to severe alcohol withdrawal. Review CNS Drugs. 2017;31(2):87–95. doi:10.1007/s40263-016-0403-y
101. Kang M, Ghassemzadeh S. Toxicity, Benzodiazepine. StatPearls. Treasure Island (FL): StatPearls Publishing; 2018 Jan 31.
102. Calcaterra NE, Barrow JC. Classics in chemical neuroscience: diazepam (valium). ACS Chem Neurosci. 2014;5(4):253–260. doi:10.1021/cn5000056
103. Uusi-Oukari M, Korpi ER. Regulation of GABA(A) receptor subunit expression by pharmacological agents. Pharmacol Rev. 2010;62(1):97–135. doi:10.1124/pr.109.002063
104. Fukasawa T, Suzuki A, Otani K. Effects of genetic polymorphism of cytochrome P450 enzymes on the pharmacokinetics of benzodiazepines. J Clin Pharm Ther. 2007;32(4):333–341. doi:10.1111/jcp.2007.32.issue-4
105. Qin XP, Xie HG, Wang W, et al. Effect of the gene dosage of CgammaP2C19 on diazepam metabolism in Chinese subjects. Clin Pharmacol Ther. 1999;66(6):642–646. doi:10.1016/S0009-9236(99)90075-9
106. Scott SA, Sangkuhl K, Shuldiner AR, et al. PharmGKB summary: very important pharmacogene information for cytochrome P450, family 2, subfamily C, polypeptide 19. Pharmacogenet Genomics. 2012;22(2):159–65.29. doi:10.1097/FPC.0b013e32834d4962
107. Scott SA, Sangkuhl K, Gardner EE, et al.; Clinical Pharmacogenetics Implementation Consortium. Clinical pharmacogenetics implementation consortium guidelines for cytochrome P450-2C19 (CYP2C19) genotype and clopidogrel therapy. Clin Pharmacol Ther. 2011;90(2):328–332. doi:10.1038/clpt.2011.132
108. Sohn DR, Kusaka M, Ishizaki T, et al. Incidence of S-mephenytoin hydroxylation deficiency in a Korean population and the interphenotypic differences in diazepam pharmacokinetics. Clin Pharmacol Ther. 1992;52(2):160–169. doi:10.1038/clpt.1992.125
109. Zhang YA, Reviriego J, Lou YQ, Sjöqvist F, Bertilsson L. Diazepam metabolism in native Chinese poor and extensive hydroxylators of S-mephenytoin: interethnic differences in comparison with white subjects. Clin Pharmacol Ther. 1990;48(5):496–502. doi:10.1038/clpt.1990.185
110. Wan J, Xia H, He N, Lu YQ, Zhou HH. The elimination of diazepam in Chinese subjects is dependent on the mephenytoin oxidation phenotype. Br J Clin Pharmacol. 1996;42(4):471–474. doi:10.1111/j.1365-2125.1996.tb00010.x
111. Inomata S, Nagashima A, Itagaki F, et al. CYP2C19 genotype affects diazepam pharmacokinetics and emergence from general anesthesia. Clin Pharmacol Ther. 2005;78(6):647–655. doi:10.1016/j.clpt.2005.08.020
112. He P, Court MH, Greenblatt DJ, von Moltke LL. Factors influencing midazolam hydroxylation activity in human liver microsomes. Drug Metab Dispos. 2006;34(7):1198–1207. doi:10.1124/dmd.105.008904
113. He P, Court MH, Greenblatt DJ, von Moltke LL. Genotype-phenotype associations of cytochrome P450 3A4 and 3A5 polymorphism with midazolam clearance in vivo. Clin Pharmacol Ther. 2005;77(5):373–387. doi:10.1016/j.clpt.2004.11.112
114. Maekawa K, Yoshimura T, Saito Y, et al. Functional characterization of CYP3A4.16: catalytic activities toward midazolam and carbamazepine. Xenobiotica. 2009;39(2):140–147. doi:10.1080/00498250802617746
115. Park JY, Kim KA, Park PW, et al. Effect of CYP3A5*3 genotype on the pharmacokinetics and pharmacodynamics of alprazolam in healthy subjects. Clin Pharmacol Ther. 2006;79(6):590–599. doi:10.1016/j.clpt.2006.02.008
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.