Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Pharmacogenetics in Tuberculosis-HIV Coinfected Populations: A Systematic Review of Genetic Variants Influencing Antiretroviral and Anti-Tuberculosis Drug Response
Authors Hardi H ![]() , Fitrianti Z, Mahata LE, Louisa M
, Fitrianti Z, Mahata LE, Louisa M
Received 24 July 2025
Accepted for publication 28 October 2025
Published 5 November 2025 Volume 2025:18 Pages 7203—7218
DOI https://doi.org/10.2147/JMDH.S555909
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Harri Hardi,1 Zahra Fitrianti,1 Liganda Endo Mahata,1,2 Melva Louisa3
1Clinical Pharmacology Specialist Study Program, Faculty of Medicine, Universitas Indonesia, Jakarta, Indonesia; 2Department of Pharmacology and Therapy, Faculty of Medicine, Universitas Andalas, Padang, West Sumatra, Indonesia; 3Department of Pharmacology and Therapeutics, Faculty of Medicine, Universitas Indonesia, Jakarta, Indonesia
Correspondence: Melva Louisa, Department of Pharmacology and Therapeutics, Faculty of Medicine, Universitas Indonesia, Jakarta, Indonesia, Email [email protected]
Abstract: Pharmacogenetics is a concept designed to tailor medication based on genetic profile to improve efficacy and reduce adverse effects. This personalized strategy shows considerable potential for populations facing complicated therapeutic challenges, such as the coinfected Tuberculosis (TB)-HIV population. This systematic review analyses pharmacogenes related to antiretroviral and anti-tuberculosis medications in the TB-HIV population. An analysis of 39 included studies indicated that efavirenz and CYP2B6*6 are the most extensively researched antiretroviral therapy (ART) and gene, respectively. Isoniazid and N-acetyltransferase 2 (NAT2) are the most extensively researched anti-TB drug and gene, respectively. Nevertheless, many studies relied solely on observational research and the investigation of pharmacokinetic characteristics. Research evaluated both the drug concentration of individual gene-drug interactions and the interactions between medications based on their genotypes. The NAT2 slow acetylator genotype is associated with elevated isoniazid levels, consequently increasing efavirenz plasma concentrations. Arylacetamide deacetylase (AADAC) polymorphisms that increased rifapentine plasma levels could also reduce dolutegravir plasma concentrations. Specific genes linked to significant outcomes in TB-HIV populations, such as pregnane X receptor (PXR) g.24087C>T, which increased the mortality rate. Consequently, a holistic approach to pharmacogenetics in TB-HIV populations is essential, considering all drug-gene-disease interactions. High-quality research, including randomized controlled trials (RCTs), is necessary for the implementation of pharmacogenetic testing in TB-HIV populations before it can be widely adopted in clinical practice, which is currently lacking.
Keywords: TB-HIV, pharmacogenes, NAT2, AADAC, PXR
Introduction
The coinfection of tuberculosis (TB) and HIV (TB-HIV) imposes a significant burden on developing countries. In 2023, TB infected 10.8 million individuals worldwide and resulted in 1.25 million deaths, of which 161,000 occurred in patients with HIV.1 TB, which accounts for 99% of cases in low- and middle-income countries (LMICs), incurred a cost of $10.9 billion in 2017 across 135 LMICs.1,2 The estimated overall economic loss from 2020 to 2050 due to TB is projected to be $30.0 trillion.3
Approximately 500,000 patients annually commence antiretroviral treatment (ART) concurrently with anti-tuberculosis (anti-TB) therapy.4 In this condition, a high quantity of medication, including a minimum of four anti-TB drugs and three ART, may lead to drug interactions and an elevated risk of adverse effects. This phenomenon results in a TB treatment success rate for HIV-positive individuals that is 47% lower than that of people without HIV.5
Anti-TB medications impart a unique property, which demonstrates that low anti-TB drug concentrations appear in HIV-TB coinfected individuals with low body weight despite adequate dosage.6 This data looks in contrast with typical medication pharmacokinetics in low body weight, hypothesizing that anti-TB drugs present a nonlinear relationship between body weight and drug clearance.7 This nonlinear relationship is further aggravated by the HIV disease state, which typically causes malnutrition and affects drug pharmacokinetics.8 HIV patients also exhibited decreased transmembrane efflux transporter P-glycoprotein (P-gp) pump function, reduced cytochrome P450 (CYP) expression, and an impairment in drug clearance.9 These alterations result in an interesting study in which CYP2D6 extensive metabolizers (EM) HIV patients demonstrated a shift to a poor metabolizer (PM) CYP2D6 phenotype.10
In the TB-HIV population, pharmacokinetic alterations occur alongside individual genetic variations that influence drug metabolism, which known as pharmacogenetics. Certain genes are recognized for their involvement in anti-TB and ART. The example of the NAT2 slow acetylator shows a reduced rate of isoniazid metabolism, resulting in elevated isoniazid concentrations and an increased risk of hepatotoxicity.11 Furthermore, individuals identified as CYP2B6 poor metabolizers exhibit elevated blood concentrations of efavirenz; therefore, it is advisable to reduce the initial dose of efavirenz.12 Beside pharmacogenetics factors, isoniazid increases efavirenz concentration by inhibiting CYP1A2 and CYP2A6, leading to complex drug-gene interactions in TB-HIV.13,14
Drug-gene interactions are influenced by specific genes, referred to as drug-gene-disease interactions. Host genetic determinants can affect susceptibility and treatment outcomes in patients with tuberculosis and HIV. Pharmacogenes, genes which influence drug metabolism, can affect the metabolic rates of CYPs, UGTs, and NATs in the context of TB-HIV. TB-HIV patients also exhibit various pharmacokinetic alterations that can affect the pharmacokinetics of anti-TB and ART. Alterations in pharmacokinetics can result in supratherapeutic or subtherapeutic drug concentrations, potentially increasing the risk of drug toxicity or treatment failure. Figure 1 illustrates the interaction between drugs, genes, and diseases within the framework of TB-HIV pharmacogenetics.The disparity between the genotypes of TB-HIV patients and the current interpretations of those genotypes suggest that pharmacogenetic studies in TB-HIV populations may yield intriguing and potentially unique findings compared to the general population. Such trials should be undertaken more frequently, as research indicates that pharmacogenetic testing for isoniazid is cost-effective in three developing countries: Brazil, South Africa, and India,15 highlighting the potential economic advantages of this test. In addition, the existing Clinical Pharmacogenetics Implementation Consortium (CPIC) guidelines solely address CYP2B6 genotyping and efavirenz dose in the HIV community,12 underscoring the urgent necessity for research that encompasses additional pharmacogenes, drugs, and TB-HIV populations.
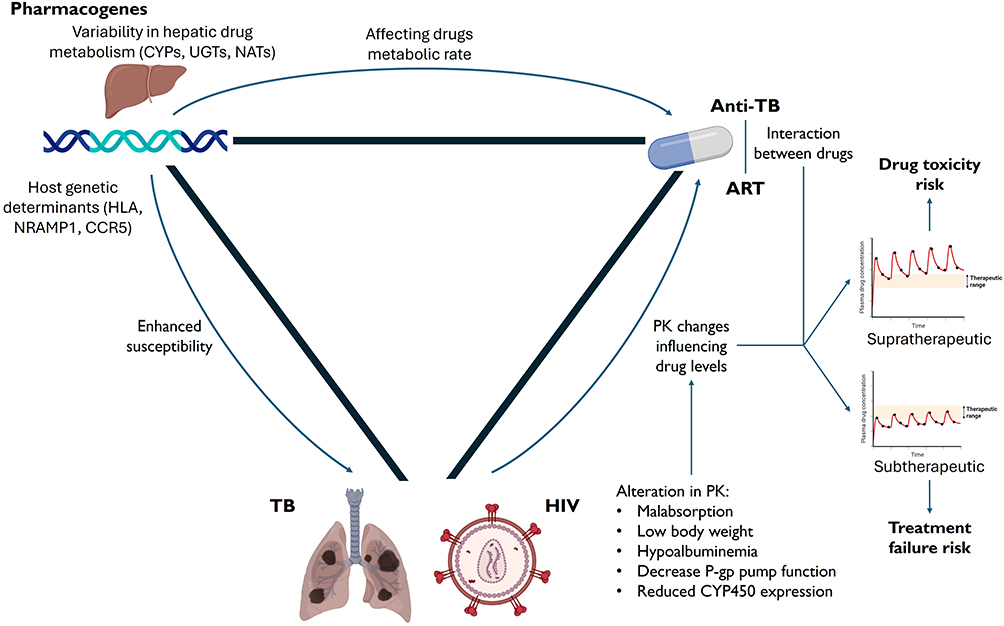 |
Figure 1 Drug-gene-disease interaction in the context of tuberculosis and HIV. Abbreviations: CYPs, cytochrome P450 enzymes; UGTs, uridine diphosphate glucuronosyltransferases; NATs, N-acetyltransferases; HLA, human leukocyte antigen; NRAMP1, natural resistance-associated macrophage protein 1; CCR5, C-C chemokine receptor type 5; TB, tuberculosis; HIV, human immunodeficiency virus; PK, pharmacokinetics; CYP450, cytochrome P450; anti-TB, antituberculosis; ART, antiretroviral therapy. |
Thus far, reviews have evaluated the interplay between TB-HIV,16 pharmacogenetics in TB,17 and pharmacogenetics in HIV.18 However, a review that concurrently assesses all three components together—pharmacogenetics, TB, and HIV—is still lacking. The integration of the drug-gene-disease approach is a crucial strategy for optimizing individualized treatment in TB-HIV. A comprehensive review of pharmacogenetic research in TB-HIV populations will enhances our understanding of the distinct pharmacogenetic properties and interpretation of this group compared to populations with only TB or HIV. Additionally, it identifies potential areas for further research. This systematic review is the first to concurrently assess pharmacogenetics in the TB-HIV population, aiming to clarify the pharmacogenetic factors related to ART and anti-TB medications in patients coinfected with TB and HIV.
Methods
This systematic review has been registered in the International Prospective Register of Systematic Reviews (PROSPERO) under registration ID CRD420251057373 (www.crd.york.ac.uk/PROSPERO/view/CRD420251057373) and adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) standards. Studies involving TB-HIV patients who were evaluated for pharmacogenetic variation and who were administered anti-TB and ART medications were included in this systematic review. Because it might not be able to infer a state of disease and immunology of TB-HIV patients, we excluded studies that used anti-TB for prophylactic indication in HIV individuals. The outcomes of interest in this systematic review were the effectiveness of treatment, adverse effects, and blood drug concentration. We also excluded the study that had not compared the outcomes related to pharmacogenetic variance. Observational and clinical trial studies were incorporated into the analysis.
We performed a systematic search across three databases: PubMed, Scopus, and Web of Science, from their inception to June 1, 2025, utilizing the keywords: “Tuberculosis” AND “HIV” AND “Pharmacogenetic.” Furthermore, we obtained both ongoing and completed clinical studies from clinicaltrials.gov to incorporate the findings into our systematic review. The specific keywords for each database are outlined in Supplementary Table 1. No language limitations were imposed. Two authors (ZF and LEM) independently selected suitable papers according to established inclusion and exclusion criteria. Further differences were resolved with the third author (HH). The risk of bias was assessed using the Risk of Bias in Non-randomized Studies of Interventions (ROBINS-I),19 employing the same authors as in the systematic literature search methodology.
We collected information on genetic variance, anti-TB and ART medications, study demographics (country, race, and gender), and treatment effectiveness and side effects, along with pharmacokinetics parameters. The data was extracted by two different authors (ZF and LEM), and the third author (HH) discussed any discrepancies. We employed Web Plot Digitizer (https://automeris.io/) to obtain accurate values from graphs lacking specific data points. We also acquired the list of all anti-TB and ART medications, along with their interactions. All anti-TB and ART medications were sourced from the 2021 WHO HIV guidelines20 and the 2022 WHO tuberculosis guidelines.21 A comprehensive list of interactions between anti-TB and ART medications with CYP enzymes and transporter systems was obtained from the FDA drug interaction database.22
Results
From a total of 1810 screened papers and registers, we identified 39 that met the inclusion and exclusion criteria. The PRISMA flowchart illustrating the selection process is depicted in Figure 2. These included studies encompassed 29 pharmacokinetic studies, 8 population pharmacokinetic studies, and 2 studies that only evaluated drug-induced liver injury related to TB-HIV drugs, without evaluating pharmacokinetic parameters.
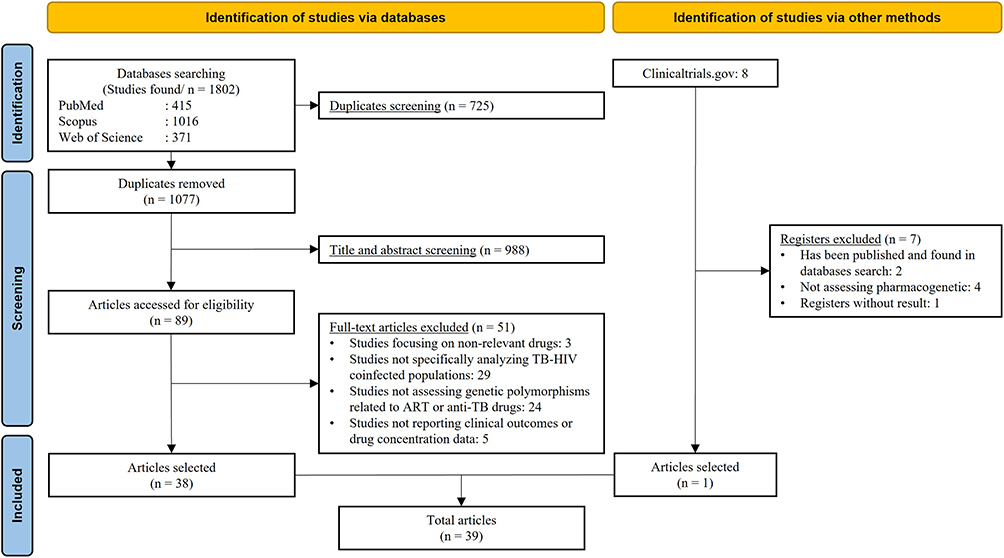 |
Figure 2 PRISMA flowchart. |
Out of the 39 publications considered, 24 were conducted in Africa, 8 in Asia, 1 in South America, and the remainder were carried out in various nations, either spanning multiple continents or lacking specific study locations. Thirty-five studies evaluated drug pharmacokinetic properties, with the majority focusing on efavirenz pharmacokinetic factors (21 studies). However, only seven, six, and two studies assessed effectiveness, adverse effects, and mortality related to TB-HIV, respectively. Comprehensive information regarding the characteristics of each study is presented in Supplementary Table 2.
We identified that 10 studies exhibit a serious risk of bias, 26 demonstrate a moderate risk of bias, and 3 present a low risk of bias. Most of the bias originated from participant selection, which employed consecutive sampling, and confounding bias due to the lack of stringent inclusion and exclusion criteria, resulting in differing baseline characteristics between groups. Several studies also exhibited bias resulting from missing data, which was attributable to a significant dropout rate. The risk of bias for each domain is illustrated in Supplementary Figure 1. Supplementary Table 3 delineated the risk of bias across each domain for each study.
According to the FDA’s drug interactions list, CYP3A4 and CYP2B6 are the primary CYPs involved in interactions with TB-HIV medications. Efavirenz is the sole substrate of CYP2B6, also functioning as an autoinducer, whereas rifampin can also stimulate CYP2B6. Several protease inhibitors (saquinavir, tipranavir, and darunavir), in addition to rilpivirine and maraviroc, are substrates of CYP3A4. Rifampin, efavirenz, and etravirine serve as inducers of CYP3A4 enzyme. Several TB-HIV pharmacotherapies also stimulated CYP2C19, 2C9, 1A2, 2C8, and 2D6 enzymes. TB-HIV medications additionally inhibit various transporter systems, including OATP1B1, OATP1B3, and OCT2. A comprehensive list of interactions between TB-HIV treatments and CYP enzymes, as well as transporters, is presented in Table 1. The complete results of the interactions between TB-HIV therapies and CYP enzymes are presented in Supplementary Table 4.
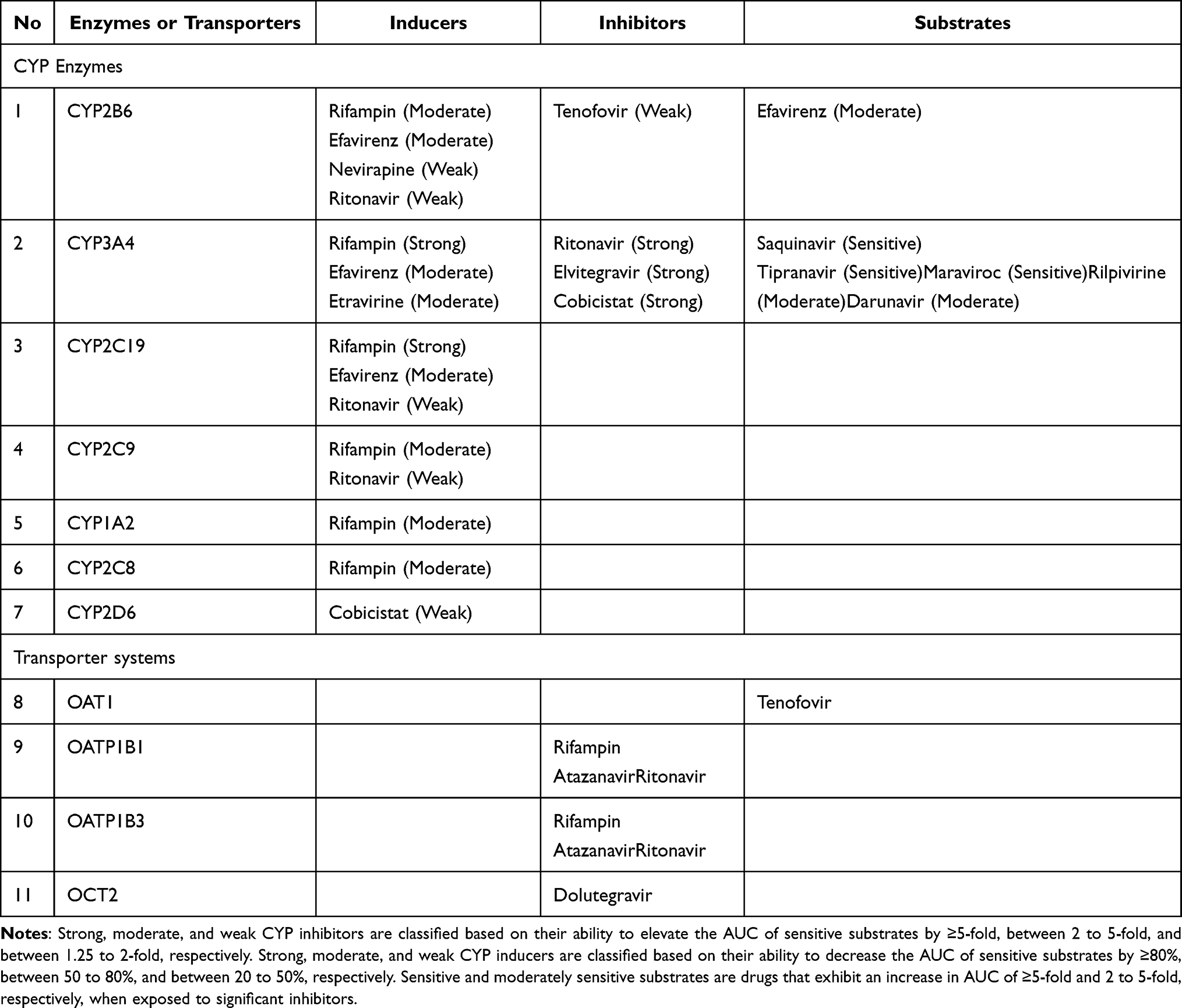 |
Table 1 CYP Enzymes or Transporters Associated with Tuberculosis or HIV Medications According to the FDA Drug Interactions List |
Genetic Variation Influencing Antiretroviral Response in TB-HIV Populations
We identified four antiretroviral agents that have been investigated for their association with genetic variation in TB-HIV coinfection: efavirenz, nevirapine, zidovudine, and dolutegravir. Efavirenz is the most studied drug in pharmacogenetic research within TB-HIV populations, involving three CYP genes (CYP2B6, CYP1A2, and CYP2A6) and the ABCB1 in its response. N-acetyltransferase 2 (NAT2), recognized for its role in isoniazid acetylation, polymorphism also contributes to the increased concentration and decreased oral clearance of efavirenz.23–25
We identified seven CYP2B6 variants that affect efavirenz drug concentration levels, with CYP2B6*6 (c.516G>T) being the most extensively studied in TB-HIV populations. Eighteen studies indicated that the CYP2B6*6 polymorphism may elevate plasma efavirenz concentrations,23,24,26–41 whereas four studies demonstrated a reduction in efavirenz oral clearance.25,28,42,43 A study also indicated that the CYP2B6*6 elevates efavirenz levels in cerebrospinal fluid (CSF).40 Studies have also evaluated pharmacokinetic parameters in children and pregnant women, revealing similar results concerning the CYP2B6*6 polymorphism.24,35,38
In comparison to the CYP2B6*6 with GG genotype, the GT genotype appears to elevate efavirenz levels by varying degrees, with the maximum increase being 1.8 times.30 Nevertheless, two studies did not see any rise in efavirenz concentration.26,33 The inconsistency is also apparent in the area under curve (AUC) increment, as one in five studies which assessed AUC did not observe a significant increase for the GT genotype compared to the GG genotype.28 However, all studies evaluating the TT genotype demonstrated significant higher plasma efavirenz levels relative to the GG genotype, ranging from 2.8 to 9.8 times. The AUC is also higher by 2.5 to 6.9 times. Several studies evaluated concentration and AUC at two distinct time points (after short-term and long-term treatment) and found no significant differences between the two groups.27,30,39,41 The details of research evaluating pharmacokinetic parameters in CYP2B6*6 polymorphism within TB-HIV patients are included in Supplementary Table 5.
Two studies specifically addressed the dosage recommendations for efavirenz in relation to the CYP2B6*6 polymorphism within the TB-HIV group. A study in the Thai population indicated that efavirenz dosages should be 800, 600, and 200 mg daily for TB-HIV co-infected patients with GG, GT, and TT genotypes, respectively.43 A separate study with Ugandans indicated that the recommended dosages are 450 mg daily for GG or GT genotypes and 250 mg daily for TT genotypes.32
Besides CYP2B6*6, the CYP2B6*18 (c.983T>C) is the second most researched in the TB-HIV population, with five studies indicating it can elevate plasma efavirenz concentrations.23,24,34,35,38 In addition to elevating plasma concentration, certain variations may also reduce plasma concentration, including CYP2B6*11 (c.136A>G) and CYP2B6 g.18492T>C.29,31,32,44 Of note, three studies did not find a correlation between the CYP2B6 polymorphism and HIV-RNA copies or CD4 counts.26,30,44 A study assessed the side effects and concluded that CYP2B6 was not linked to drug-induced hepatotoxicity; however, this finding warrants further scrutiny due to the limited sample size of 32 subjects.34 Another study evaluating the incidence of drug-induced liver injury (DILI) indicated that patients with the CYP2B6 c.516G>T TT genotype are 2.05 times more susceptible to DILI than those with the GG genotype. Nonetheless, it did not evaluate efavirenz concentrations.45
In addition to elevating efavirenz concentrations, nevirapine concentrations are also heightened in patients possessing the CYP2B6*6 polymorphism. Nonetheless, akin to the trend observed in efavirenz concentration, it was only significant in week 6, not in week 12. The CYP2B6*6 polymorphism exhibited no significant difference in median CD4 levels during efavirenz treatment; however, there was a tendency for CD4 values to decline in patients with the TT genotype who received nevirapine. Notably, there is no significant difference in the prevalence of plasma HIV-1 RNA <50 copies/mL among patients with the CYP2B6*6 polymorphism.41 A further investigation into pharmacokinetic parameters in children revealed that the AUC, Cmin, and Cmax of nevirapine are significantly elevated in individuals with the CYP2B6*6 TT genotype compared to those with the GG and GT genotypes. Interestingly, the AUC in the TB-HIV population is significantly lower than that in the HIV-only population across the genotype.46 A separate study on ABCB-1 c.3435C>T indicated that this polymorphism does not influence nevirapine concentration; however, it affects virologic outcomes, with the TT genotype exhibiting a lower percentage of individuals achieving plasma HIV-1 RNA levels below 50 copies/mL.47
Additional studies have been performed on various ART, including UGT2B7*1c (c.735A>G), which has been significantly correlated with increased zidovudine clearance, resulting in reduced plasma concentrations.48 A study evaluating dolutegravir pharmacokinetics demonstrated that UGT1A1*80 (c.-364C>T) and arylacetamide deacetylase AADAC*2 (c.841G>A) significantly correlated with plasma dolutegravir concentrations, with the UGT1A1 C allele and AADAC A allele identified as risk alleles for lower dolutegravir plasma levels.49 A separate study indicated that the UGT1A1*28 polymorphism exhibited no significant correlation with dolutegravir plasma concentration.50 Comprehensive studies on single nucleotide polymorphisms (SNPs) in genes encoding cytochromes, transporters, and nuclear receptors significantly associated with ART response in the TB-HIV population are presented in Table 2.
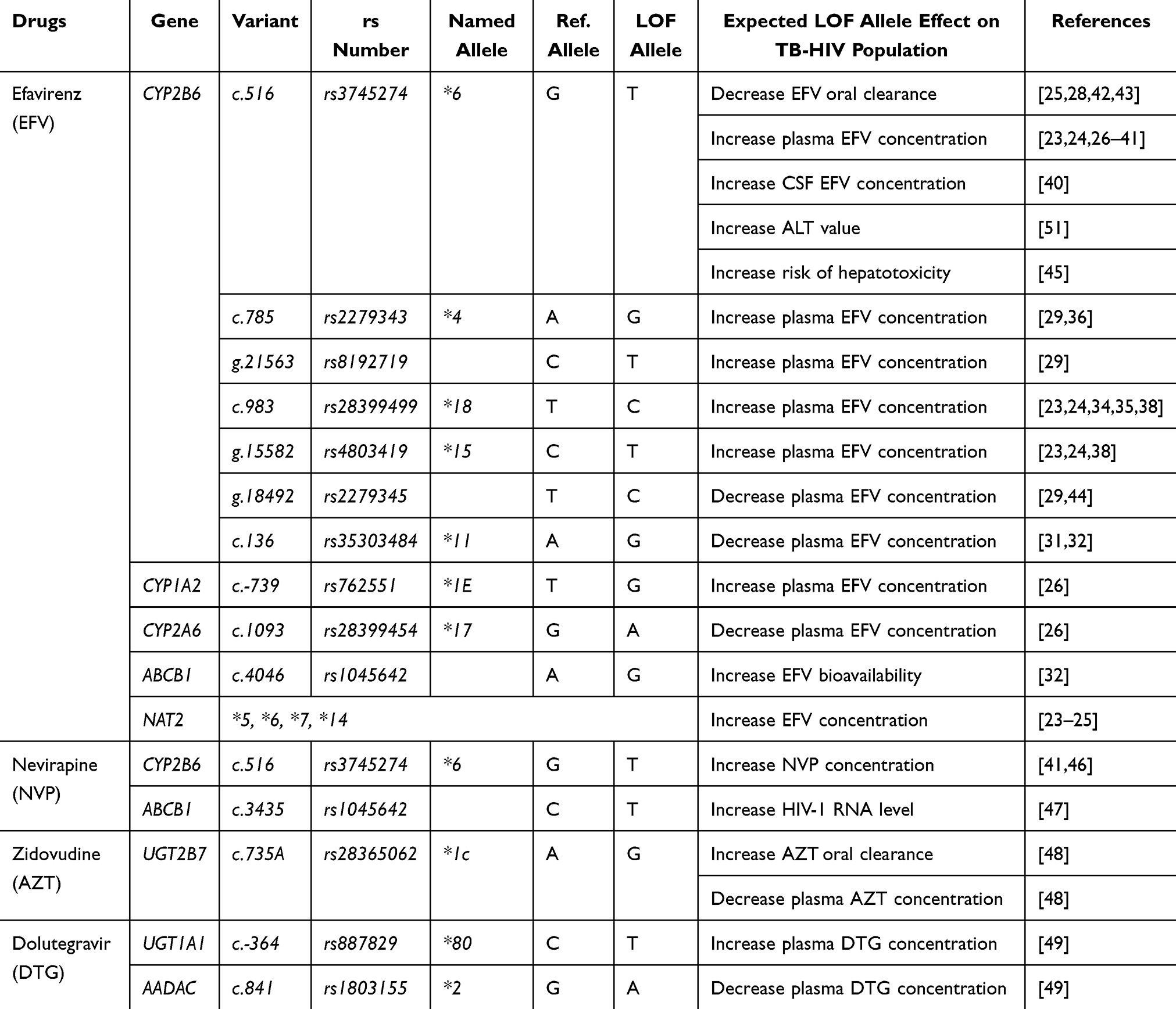 |
Table 2 Single Nucleotide Polymorphisms (SNPs) in Genes Encoding Cytochromes, Transporters, and Nuclear Receptors Significantly Associated with the Antiretroviral Response in the TB-HIV Population, Along with the Expected Effects of Loss of Function Alleles (LOF) Relative to Reference Alleles (Ref) |
Genetic Variation Influencing Anti-Tuberculosis Response in TB-HIV Populations
Four anti-TB medications have been assessed for pharmacogenetic variants in the TB-HIV population: rifampin, rifabutin, isoniazid, and ethambutol. Isoniazid was the most extensively researched medicine, with several genes implicated in its treatment effectiveness and side effects, including NAT2, Solute Carrier Organic Anion Transporter Family Member 1B1 (SLCO1B1), and pregnane X receptor (PXR). NAT2 was the most thoroughly investigated, with four variants (*5, *6, *13A, and *14) associated with an elevated risk of hepatotoxicity. The increased risk of hepatotoxicity in slow acetylators may be attributed to lower clearance capacity, resulting in higher isoniazid concentrations and AUC, as demonstrated in the included studies.51–53 A study showed that no increased risk of mortality was reported across TB-HIV patients with various NAT2 genotypes. However, rapid acetylators exhibited a 2.39-fold increase in mortality risk (95% CI: 0.94–6.07) compared to intermediate acetylators. This insignificant finding may stem from a limited sample size (30 in rapid acetylators and 50 in intermediate acetylators).54
Noteworthy discovery identified in PXR g.24087C>T. Patients with the PXR TT genotype had a 15.7% increase in neurotoxicity compared to those with the CC genotype, with an odds ratio of 2.9. The PXR TT genotype also exhibited a 12.5% increase in mortality rate, with an odds ratio of 4.6. This result might be derived from higher plasma isoniazid concentration observed in the TT genotype.51 Another gene potentially implicated in isoniazid metabolism is SLCO1B1 g.38664C>T; the TT genotype reduces plasma isoniazid levels and diminishes the risk of hepatotoxicity.51 This gene is also implicated in rifampin, which exhibits a lower concentration in TT genotypes.55 Additional genes have been examined for rifampin utilisation in TB-HIV populations, including SLCO1B3 c.334T>G, which increased bioavailability,56 and CYP2C19*17 (c.-806C>T), which doubled clearance rate.52 Another rifampin derivative, rifabutin, has been examined in a population pharmacokinetic research, which indicated that SLCO1B1*14 (c.463C>A) CC genotypes enhance rifabutin bioavailability by 30%.57
Ethambutol, another anti-TB medication, demonstrated that the CYP1A2 c.2159G>A variant was linked to a 50% decrease in relative bioavailability, necessitating a larger dosage for individuals with the GA or AA genotype.58 Detailed studies on single-nucleotide polymorphisms (SNPs) in genes encoding cytochromes, transporters, and nuclear receptors significantly associated with anti-TB response in the TB-HIV population are presented in Table 3. Additionally, research evaluated the pharmacogenetic factors associated with hepatotoxicity in the TB-HIV population without measuring drug levels, revealing that HLA-B*57, HLA-B*14, and ABCB1 c.3435C>T elevated the risk of hepatotoxicity by 30.1, 7.5, and 5.3 times, respectively.45,59 The complete results of each investigation pertaining to the examined gene are included in Supplementary Table 6.
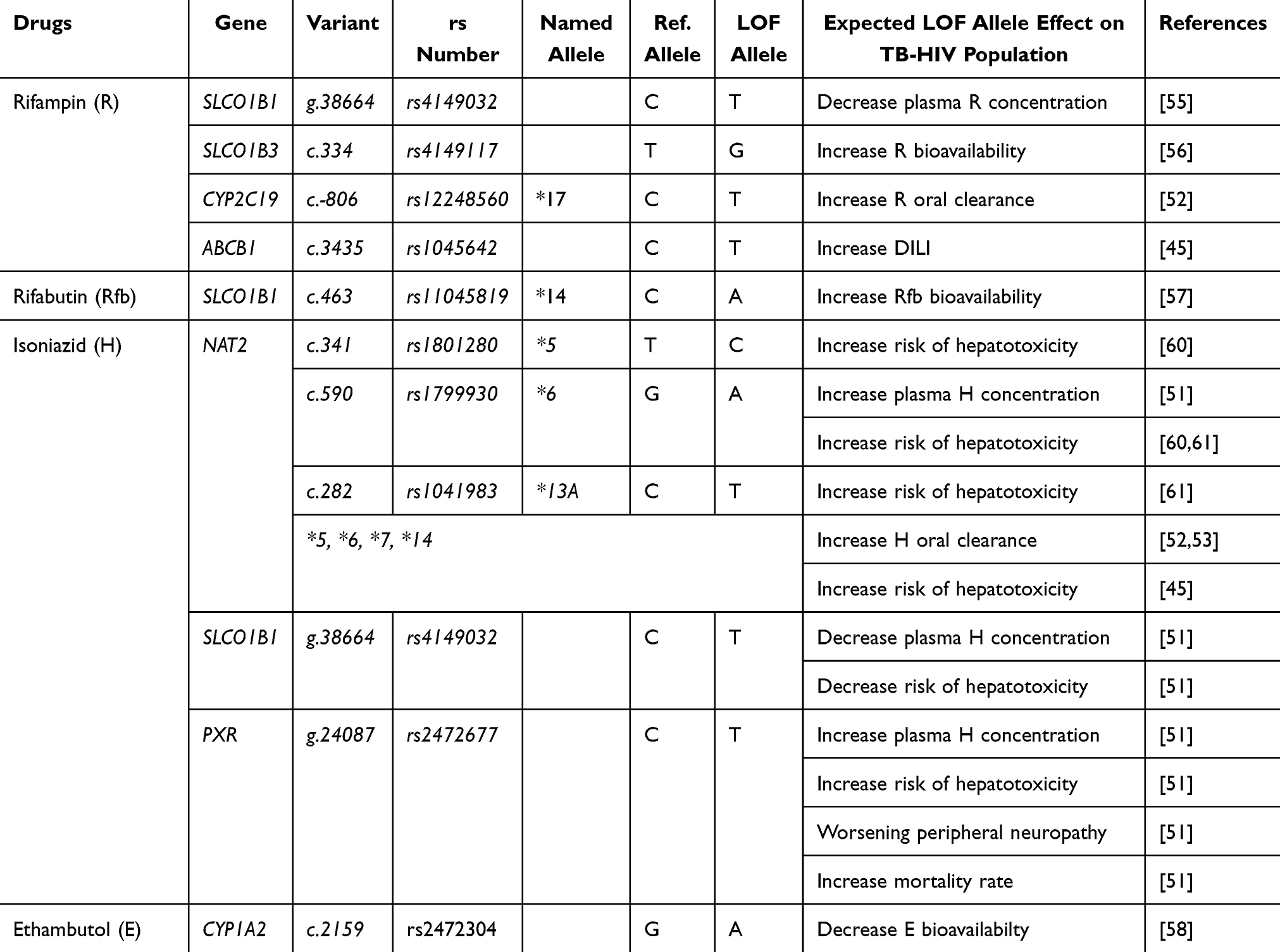 |
Table 3 Single Nucleotide Polymorphisms (SNPs) in Genes Encoding Cytochromes, Transporters, and Nuclear Receptors Significantly Associated with the Anti-Tuberculosis Response in the TB-HIV Population, Along with the Expected Effects of Loss of Function Alleles (LOF) Relative to Reference Alleles (Ref) |
Upon examining clinicaltrial.gov, we identified one active non-RCT, the PHINX trial (Pharmacogenetics-guided Isoniazid Dosing in TB-HIV; NCT05124678). This study will employ an isoniazid dosage of 10 mg/kg/day for fast/intermediate acetylators and 5 mg/kg/day for slow acetylators. The dose adjustment will occur solely during the intensive phase and revert to 5 mg/kg/day in the continuation phase. We compiled a summary of all pharmacogenetic research in the TB-HIV community, categorized by study type and outcome (changing pharmacokinetics or clinically significant), as illustrated in Figure 3.
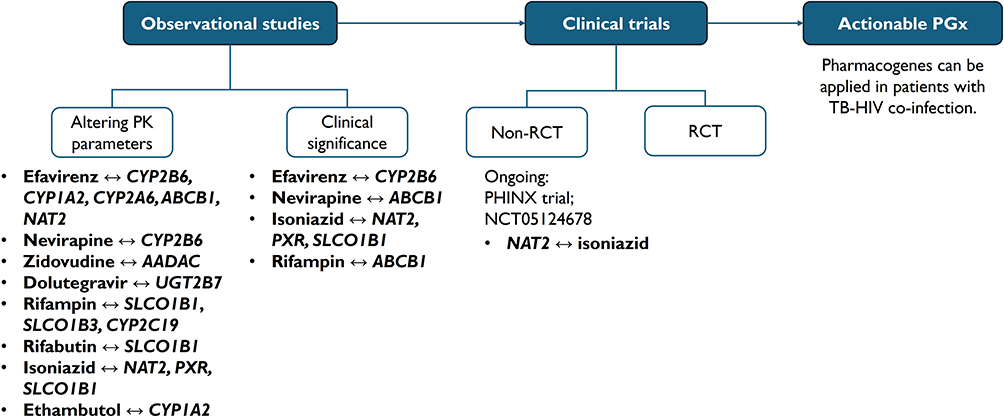 |
Figure 3 Schematic overview of the current progress in pharmacogenetics among TB-HIV coinfected populations. Actionable pharmacogenetic (actionable PGx) in clinical practice should be supported by high-quality evidence, such as clinical trials or robust observational studies. Abbreviations: PK, pharmacokinetics; RCT, randomized controlled trial. |
Discussions
Our analysis of 39 included studies indicated that the interpretation of pharmacogenetic results in TB-HIV populations may differ from that in patients with only TB or HIV. For instance, rifampin acts as an inducer of CYP2B6, while the polymorphism of CYP2B6 influences the dosage of efavirenz. This necessitates a higher dosage in TB-HIV populations for each variant of CYP2B6*6, as demonstrated in the simulated suggested doses by Chaivichacharn et al.43 The efavirenz dosage required is merely 400, 300, and 100 mg for HIV monoinfected individuals, whereas it escalates to 800, 600, and 200 mg in TB-HIV coinfected patients for GG, GT, and TT genotypes, respectively. The recommendation for GG genotypes in TB-HIV populations exceeds the HIV guidelines, which indicate that 400 mg of efavirenz is adequate in HIV treatment.20
This dosage recommendation, derived from a study, may necessitate caution before being used for all TB-HIV groups. A study including Ugandans revealed that the suggested dosages are substantially lower, specifically 450 mg daily for GG or GT and 250 mg daily for TT genotypes.32 The variation in dose recommendations may be attributed to many characteristics that influence efavirenz concentration. A study identifying potential factors influencing varying efavirenz concentrations revealed a significant inverse correlation between body weight and body mass index with efavirenz concentration.62 The recommended dosage derived from pharmacokinetic modelling should also be implemented cautiously while considering additional factors. For instance, efavirenz 400 mg is regarded as more tolerable due to its lower incidence of neurotoxicity and smaller tablet size relative to the 600 mg tablet.63
The use of pharmacogenetic testing results in clinical practice may be more complicated than it appears. For instance, the recommended 450 mg dose is complex, as it necessitates patients to consume three tablets (eg, two 200 mg tablets and one 50 mg tablet), potentially reducing adherence to ART. To date, the most fixed-dose combination of efavirenz available in LMICs is the 600 mg preparation. Consequently, guidelines from countries such as South Africa and India continue to recommend 600 mg efavirenz as the appropriate initial dosage.64,65 Therefore, the pharmacogenetic approach should be applied carefully, considering the factor of drug availability and preparation. The use of alternative ART regimens, such as dolutegravir, which is currently recommended as first-line therapy, is advised for patients with polymorphisms in CYP2B6.
The interaction between anti-TB and ART medications is elucidated in Table 1. CYP3A4 is the most interacting enzyme in TB-HIV individuals. In pharmacogenetics, CYP3A4 is not the main concern due to the unimodal distribution of enzyme activity and the extensive variability in hepatic protein expression.66 However, CYP3A4*22 has garnered greater interest recently due to its high minor allele frequencies (3–5%) and considerably influences the pharmacokinetics of various medications.67 This variance has also been examined in ART, such as tenofovir, which can elevate tenofovir alafenamide plasma levels by 39%.68 Consequently, studies evaluating CYP3A4*22 in the TB-HIV group may be necessary.
The FDA drug interaction list only incorporated the significant in vivo interactions. Moreover, several in vitro drug interactions remain unproven in vivo, such as ethambutol, which markedly inhibit CYP1A2 and CYP2E1.69 An included study indicated that the ethambutol CYP1A2 c.2159G>A variant was associated with a 50% reduction in relative bioavailability, which could not be elucidated by the mechanism theory.58 This sporadic outcome raises the hypothesis that CYP1A2 polymorphism may be linked with another unknown genetic variant contributing to reduced ethambutol bioavailability. However, this remains speculative and requires further investigation.
The FDA list has also not mentioned the interaction between efavirenz and isoniazid, as demonstrated by this study. We identified three studies that showed the association between NAT2 slow acetylator and elevated efavirenz concentrations.23–25 NAT2 slow acetylator will result in elevated isoniazid concentrations in persons possessing this trait. Isoniazid is an in vitro inhibitor of CYP1A2, 2A6, 2C19, and 3A4. At the same time, the metabolism of efavirenz to 8-OH-EFV is reliant on CYP2B6, followed by CYP1A2, 3A5, and 3A4.13,14 The metabolism of efavirenz to 7-OH-EFV is also contingent upon CYP2A6 and CYP2B6.14 The interaction of isoniazid, a CYP1A2 and 2A6 inhibitor, with efavirenz, a substrate of these enzymes, will result in elevated efavirenz concentrations in individuals with NAT2 slow acetylator.
The FDA list does also not mention nevirapine’s role as a substrate of CYP3A4 and CYP2B6. The concurrent use of anti-TB and ART medications results in a reduction of nevirapine AUC by 44.2%, 31.9%, and 46.9% in GG, GT, and TT genotypes, respectively, when compared to patients receiving only ART.46 Isoniazid acts as an inhibitor of CYP3A4; however, it only partially mitigates the induction effect of rifampin on CYP3A4 during combination therapy. Rifampin has the potential to decrease the AUC of nevirapine by 46%, whereas isoniazid induces an increase of only 24%.70,71 Therefore, TB-HIV patients are likely to exhibit significantly lower nevirapine concentrations, suggesting a potential need for an increased dosage in those with the GG genotype.
The connection among drug, gene, and disease has also occurred in the context of AADAC polymorphism and dolutegravir plasma concentration. AADAC is accountable for the deacetylation of the rifampin drug class, which includes rifapentine. The AADAC*2 (c.841G>A) variant markedly elevated plasma levels of rifapentine, a strong inducer of CYP3A4.72,73 Due to dolutegravir’s role as a minor substrate of CYP3A4,74 plasma levels of dolutegravir were markedly reduced in patients with TB-HIV undergoing rifapentine-based tuberculosis treatment. No notable variations in plasma dolutegravir levels were seen when the patient abstained from rifapentine consumption, irrespective of their AADAC genotype.49 This finding underscores the necessity of evaluating patients holistically, considering additional disorders rather than solely focusing on the gene relevant to a medication.
Pharmacogenetic testing should not only influence drug plasma levels but also improve efficacy and diminish adverse reactions. Certain drugs may exhibit variations in drug levels due to polymorphism; nevertheless, these alterations are insufficient to affect their efficacy or safety profile. Notably, three included studies on efavirenz pharmacogenetics found no connection between CYP2B6 polymorphism and HIV-RNA copies or CD4 counts.26,30,44 Our findings may have differed from the current CPIC efavirenz genotyping guidelines, which recommend CYP2B6 testing.12 The disparity could result from TB-HIV populations that also consumed rifampin, a known CYP2B6 inducer. The administration of a CYP inducer may result in people exhibiting a greater metabolizer phenotype, referred to as the phenoconversion phenomenon.75 However, three included cohort studies with limited sample sizes may be inadequate to establish conclusions concerning CYP2B6 testing recommendations in TB-HIV groups. Consequently, additional studies with larger sample sizes and higher quality should be undertaken.
Besides the well-known genes, such as CYP2B6 and efavirenz, further analysis of lesser-studied genes is warranted. The PXR g.24087C>T variant was a notable discovery in the TB-HIV individuals, since it heightened the risk of hepatotoxicity, exacerbated peripheral neuropathy, and elevated mortality rates.51 PXR is a ligand-dependent transcription factor that modifies the heme production pathway during rifampin-isoniazid treatment, leading to an elevation of the endogenous hepatotoxin protoporphyrin IX in the liver.76 The PXR polymorphism has significant appearance, with CT and TT genotypes seen at 51.1% and 13.6%, respectively.51 Several treatments have been investigated in vitro for rifampin-isoniazid hepatotoxicity mediated by PXR, including ursolic acid and oleanolic acid; however, no clinical trials have been conducted.77,78
Certain PXR mutations exert an opposing effect, reducing DILI associated with anti-TB, such as rs3814055 and rs7643645.79,80 PXR is the key receptor involved in the autoinduction of rifampin and efavirenz, where both compounds function as substrates and inducers of CYP. The receptor is activated by binding with rifampin and efavirenz, translocating into the nucleus, and binds to the promoter regions of the CYP2B6, 3A4/5, and 2A6 genes, leading to autoinduction.81 The process of autoinduction does not occur over a short duration; it may take up to 16 weeks with efavirenz.82 Interestingly, this autoinduction process is significant only in HIV patients without TB. A study indicated that there were no significant differences in efavirenz concentrations between short-term (4 weeks) and long-term (16 weeks) treatment in TB-HIV individuals.39 The results indicate that CYP2B6 has been induced by rifampin, and the autoinduction of efavirenz did not provide additional induction of CYP2B6.
Another study indicated that HLA-B*57 and *14 significantly elevated the incidence of DILI in patients receiving anti-TB and ARV by 30.1 and 7.5 times, respectively. This study also demonstrated an association between HLA-B*57 and mild-to-moderate liver injury, in addition to an association between HLA-B*14 and severe liver injury.59 Although HLA-B*57 is associated with abacavir hypersensitivity, this study’s antiretroviral regimen does not incorporate abacavir, hence eliminating the potential for abacavir-related hypersensitivity.83 The study showed that the predominant pattern of DILI in TB-HIV was cholestatic, contrasting with the hepatocellular pattern typically observed in DILI among tuberculosis patients;84 thus, antiretroviral agents are likely the primary contributors to DILI in TB-HIV populations. The cholestatic pattern of DILI appeared to have a lesser severity compared to the hepatocellular pattern.84 Consequently, it appears that HLA-B*57 is associated with ART, while HLA-B*14 is linked to anti-TB medication; nevertheless, this assertion requires validation through additional research focusing on these HLAs.
In addition to efficacy and adverse effects, cost is a crucial consideration in the implementation of pharmacogenetics in LMICs. Cost-effectiveness studies have been performed for numerous TB and HIV medications, including efavirenz and isoniazid; however, no research has specifically examined the TB-HIV population.15,85,86 Genotyping for efavirenz can decrease total expenses by recommending reduced dosages for individuals with IM and PM phenotypes, as these lower doses maintain comparable efficacy while minimizing adverse effects.86 Genotyping for isoniazid is cost-effective in three developing countries: Brazil, South Africa, and India, with incremental cost-effectiveness ratios (ICER) of $476, $1,780, and $546, respectively.15 The ICER value is relatively low and can likely be applied in other LMICs, given that the willingness to pay is determined by the gross domestic product (GDP) per capita of each country.87 Cost-effectiveness studies of pharmacogenetic testing in TB-HIV patients should be conducted to ascertain the precise value of the ICER for this testing in this TB-HIV population.The implementation of pharmacogenetic testing in LMICs is significantly hindered by the lack of national policies, inadequate reimbursement for testing, and a poorly developed healthcare system for incorporating pharmacogenetic data.88 High-quality research, such as randomized controlled trials in pharmacogenetic testing of a gene, is crucial in advocating for government implementation, particularly in TB-HIV communities where it remains insufficient. High-quality research on pharmacogenes, such as CYP2C19, in LMICs remains limited, despite its prevalence and frequent examination in developed nations.89 Consequently, LMICs should be encouraged to do high-quality research to tackle pertinent challenges and to push for implementation.
The highest quality of pharmacogenetic research is the randomized controlled trials (RCTs) in pharmacogenetics-based therapy, which involves one group receiving the standard TB-HIV dosage and another group receiving a dosage determined by pharmacogenetic testing. This research has been conducted on isoniazid dosing according to NAT2 genotype in tuberculosis patients without HIV, yielding significant results.90 Nonetheless, research in TB-HIV populations is lacking, likely due to challenges in sampling and ethical concerns. A study closely related to this high standard is the ongoing PHINX trial which has been explained in the result section.
The implementation of isoniazid dosage in clinical practice should be deferred until the results of the PHINX trial are obtained. Additionally, the application of other TB-HIV drugs based on pharmacogenetic testing should rely on this type of research. The correlation between increased or decreased AUC in a gene polymorphism and the corresponding success rate or side effects in an individual may not exhibit consistency. Moreover, variations in success rates or side effects associated with different polymorphisms should not guide adjustments in drug dosage. Variations in drug dosage may result in differing side effects and success rates due to distinct mechanisms of action.91 Observational studies may provide insights into the gene of interest related to a drug; however, application should rely on clinical trials utilizing various drug dosages, with RCTs serving as the gold standard for implementation. Prospective trials demonstrating clinical utility may offer an acceptable substitute for integrating a gene into clinical practice as a clinically significant gene.92
This systematic review presents multiple limitations. First, high heterogeneity is observed due to the inclusion of various races, as the implementation of pharmacogenetic studies in countries with differing racial demographics presents significant challenges. Second, many studies have not evaluated the drug’s effectiveness and side effects, resulting in uncertainty regarding the implementation of dosage recommendations. Third, many studies exhibit a low participant, likely attributable to challenges in sample recruitment and obtaining funding. Therefore, high-quality studies are necessary for TB-HIV populations.
The limited number of participants may result in broad confidence intervals, making it challenging to achieve statistically significant outcomes. A study involving TB-HIV patients indicated that rapid acetylators had a 2.39-fold increase in mortality risk (95% CI: 0.94–6.07) relative to intermediate acetylators.54 This result may be integrated through meta-analysis with subsequent research exhibiting comparable outcomes and tested genes. However, some pharmacogenetic studies may be poorly executed, preventing the conduct of a meta-analysis that could enhance sample size and increase the power to detect significant associations. Our included studies demonstrate that some do not specify race, while others fail to categorize outcomes by genotype. Additional pharmacogenetic studies adhering to the STROPS (Strengthening the Reporting of Pharmacogenetic Studies) guidelines are necessary for enhanced conduct and reporting in the field of pharmacogenetics.93
Additional pharmacogenes, apart from the link between CYP2B6 genotype and efavirenz that has been stated in the CPIC guideline, warrant investigation in TB-HIV populations according to this systematic review. Research evaluating NAT2 and its association with mortality risk, investigations into newer antiretroviral and anti-tuberculosis medications like dolutegravir and rifapentine, as well as studies on lesser-explored genes with relevance to our systematic review, such as PXR and AADAC, should be pursued. Additional novel genes associated with medication efficacy and adverse drug reactions in TB-HIV populations can also be identified by genome-wide association studies (GWAS), which are lacking in all studies included in this systematic review.
Conclusions
The CYP2B6 polymorphism associated with efavirenz medication and the NAT2 polymorphism related to isoniazid treatment were the most extensively researched drug-gene interactions in the TB-HIV group. CYP2B6 polymorphism primarily affected efavirenz plasma concentrations, whereas the NAT2 polymorphism was associated with an increased incidence of hepatotoxicity. Various drug plasma levels are influenced by their interactions with other plasma drug levels. For instance, efavirenz plasma levels could shift due to NAT polymorphisms affecting isoniazid levels, while dolutegravir plasma levels can be altered by AADAC polymorphisms that impact rifapentine plasma levels. Certain genes associated with notable outcomes in TB-HIV populations, such as PXR g.24087C>T, which elevated the mortality rate. Thus far, research on TB-HIV populations is exclusively reliant on observational data; high-quality studies, such as RCTs, must be conducted prior to the implementation of pharmacogenetic testing in clinical practice and guidelines.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific support from Public, Commercial, or Non-Profit Agencies.
Disclosure
The authors of this publication have no affiliations or engagements with any organization or entity that holds a financial or non-financial interest in the subject matter or materials addressed.
References
1. WHO. Global Tuberculosis Report 2024. Geneva: WHO; 2024.
2. Su Y, Garcia Baena I, Harle AC, et al. Tracking total spending on tuberculosis by source and function in 135 low-income and middle-income countries, 2000–17: a financial modelling study. Lancet Infect Dis. 2020;20(8):929–942. doi:10.1016/S1473-3099(20)30124-9
3. Silva S, Arinaminpathy N, Atun R, Goosby E, Reid M. Economic impact of tuberculosis mortality in 120 countries and the cost of not achieving the sustainable development goals tuberculosis targets: a full-income analysis. Lancet Glob Health. 2021;9(10):e1372–9. doi:10.1016/S2214-109X(21)00299-0
4. Semvua HH, Kibiki GS, Kisanga ER, Boeree MJ, Burger DM, Aarnoutse R. Pharmacological interactions between rifampicin and antiretroviral drugs. Ther Drug Monit. 2015;37(1):22–32.
5. Chaves Torres NM, Quijano Rodríguez JJ, Porras Andrade PS, Arriaga MB, Netto EM. Factors predictive of the success of tuberculosis treatment: a systematic review with meta-analysis. PLoS One. 2019;14(12):e0226507.
6. Sekaggya-Wiltshire C, Chirehwa M, Musaazi J, et al. Low antituberculosis drug concentrations in HIV-tuberculosis-coinfected adults with low body weight: is it time to update dosing guidelines? Antimicrob Agents Chemother. 2019;63(6).
7. Guiastrennec B, Ramachandran G, Karlsson MO, et al. Suboptimal antituberculosis drug concentrations and outcomes in small and HIV‐coinfected children in India: recommendations for dose modifications. Clin Pharmacol Ther. 2018;104(4):733–741.
8. Verrest L, Wilthagen EA, Beijnen JH, Huitema ADR, Dorlo TPC. Influence of malnutrition on the pharmacokinetics of drugs used in the treatment of poverty-related diseases: a systematic review. Clin Pharmacokinet. 2021;60(9):1149–1169.
9. Christensen H, Hermann M. Immunological response as a source to variability in drug metabolism and transport. Front Pharmacol. 2012; 3:8. doi:10.3389/fphar.2012.00008
10. O’Neil WM, Gilfix BM, Markoglou N, Di Girolamo A, Tsoukas CM, Wainer IW. Genotype and phenotype of cytochrome P 450 2D6 in human immunodeficiency virus-positive patients and patients with acquired immunodeficiency syndrome. Eur J Clin Pharmacol. 2000;56(3):231–240. doi:10.1007/s002280000116
11. Surarak T, Chumnumwat S, Nosoongnoen W, Tragulpiankit P. Efficacy, safety, and pharmacokinetics of isoniazid affected by NAT2 polymorphisms in patients with tuberculosis: a systematic review. Clin Transl Sci. 2024;17(4). doi:10.1111/cts.13795
12. Desta Z, Gammal RS, Gong L, et al. clinical pharmacogenetics implementation consortium (CPIC) guideline for CYP2B6 and efavirenz-containing antiretroviral therapy. Clin Pharmacol Ther. 2019;106(4):726–733. doi:10.1002/cpt.1477
13. Wen X, Wang J-S, Neuvonen PJ, Backman JT. Isoniazid is a mechanism-based inhibitor of cytochrome P 450 1A2, 2A6, 2C19 and 3A4 isoforms in human liver microsomes. Eur J Clin Pharmacol. 2002;57(11):799–804. doi:10.1007/s00228-001-0396-3
14. Bienvenu E, Ashton M, Äbelö A. Influence of CYP2B6 516G > T and long term HAART on population pharmacokinetics of efavirenz in rwandan adults on HIV and tuberculosis cotreatment. Pharmacol Pharm. 2015;06(11):533–546. doi:10.4236/pp.2015.611055
15. Rens NE, Uyl-de Groot CA, Goldhaber-Fiebert JD, Croda J, Andrews JR. Cost-effectiveness of a pharmacogenomic test for stratified isoniazid dosing in treatment of active tuberculosis. Clin Infect Dis. 2020;71(12):3136–3143. doi:10.1093/cid/ciz1212
16. Pooranagangadevi N, Padmapriyadarsini C. Treatment of tuberculosis and the drug interactions associated with HIV-TB co-infection treatment. Front Tropical Dis. 2022;3. doi:10.3389/fitd.2022.834013
17. Richardson M, Kirkham J, Dwan K, Sloan DJ, Davies G, Jorgensen AL. CYP genetic variants and toxicity related to anti-tubercular agents: a systematic review and meta-analysis. Syst Rev. 2018;7(1):204. doi:10.1186/s13643-018-0861-z
18. Yu ZJ, Mosher EP, Bumpus NN. Pharmacogenomics of antiretroviral drug metabolism and transport. Annu Rev Pharmacol Toxicol. 2021;61(1):565–585. doi:10.1146/annurev-pharmtox-021320-111248
19. Sterne JA, Hernán MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ;2016:i4919. doi:10.1136/bmj.i4919
20. WHO. Consolidated Guidelines on HIV Prevention, Testing, Treatment, Service Delivery and Monitoring: Recommendations for a Public Health Approach. Geneva: WHO; 2021.
21. WHO. WHO Consolidated Guidelines on Tuberculosis. Module 4: Treatment-Drug-Susceptible Tuberculosis Treatment. Geneva: WHO; 2022.
22. FDA. For healthcare professionals | FDA’s examples of drugs that interact with CYP enzymes and transporter systems [Internet]. 2024. Available from: https://www.fda.gov/drugs/drug-interactions-labeling/healthcare-professionals-fdas-examples-drugs-interact-cyp-enzymes-and-transporter-systems#table%201.
23. Luetkemeyer AF, Rosenkranz SL, Lu D, et al. Combined effect of CYP2B6 and NAT2 genotype on plasma efavirenz exposure during rifampin-based antituberculosis therapy in the STRIDE study. Clin Infect Dis. 2015;60(12):1860–1863. doi:10.1093/cid/civ155
24. Dooley KE, Denti P, Martinson N, et al. Pharmacokinetics of efavirenz and treatment of HIV-1 among pregnant women with and without tuberculosis coinfection. J Infect Dis. 2015;211(2):197–205. doi:10.1093/infdis/jiu429
25. Bertrand J, Verstuyft C, Chou M, et al. Dependence of efavirenz- and rifampicin-isoniazid–based antituberculosis treatment drug-drug interaction on CYP2B6 and NAT2 genetic polymorphisms: ANRS 12154 study in cambodia. J Infect Dis. 2014;209(3):399–408. doi:10.1093/infdis/jit466
26. Bienvenu E, Swart M, Dandara C, Ashton M. The role of genetic polymorphisms in cytochrome P450 and effects of tuberculosis co-treatment on the predictive value of CYP2B6 SNPs and on efavirenz plasma levels in adult HIV patients. Antiviral Res. 2014;102:44–53. doi:10.1016/j.antiviral.2013.11.011
27. Habtewold A, Makonnen E, Amogne W, et al. Is there a need to increase the dose of efavirenz during concomitant rifampicin-based antituberculosis therapy in Sub-Saharan Africa? The HIV-TB pharmagene study. Pharmacogenomics. 2015;16(10):1047–1064. doi:10.2217/pgs.15.35
28. Kwara A, Lartey M, Sagoe KW, et al. Pharmacokinetics of efavirenz when Co-administered with rifampin in TB/HIV Co-infected patients: pharmacogenetic effect of CYP2B6 variation. J Clin Pharmacol. 2008;48(9):1032–1040. doi:10.1177/0091270008321790
29. Manosuthi W, Sukasem C, Lueangniyomkul A, et al. Impact of pharmacogenetic markers of CYP2B6, clinical factors, and drug-drug interaction on efavirenz concentrations in HIV/tuberculosis-coinfected patients. Antimicrob Agents Chemother. 2013;57(2):1019–1024. doi:10.1128/AAC.02023-12
30. Mugusi S, Habtewold A, Ngaimisi E, et al. Impact of population and pharmacogenetics variations on efavirenz pharmacokinetics and immunologic outcomes during anti-tuberculosis co-therapy: a parallel prospective cohort study in two Sub-Sahara African populations. Front Pharmacol. 2020;11.
31. Mukonzo JK, Nanzigu S, Waako P, Ogwal-Okeng J, Gustafson LL, Aklillu E. cyp2b6 genotype, but not rifampicin-based anti-tb cotreatments, explains variability in long-term efavirenz plasma exposure. Pharmacogenomics. 2014;15(11):1423–1435. doi:10.2217/pgs.14.73
32. Mukonzo JK, Bisaso RK, Ogwal-Okeng J, Gustafsson LL, Owen JS, Aklillu E. CYP2B6 genotype-based efavirenz dose recommendations during rifampicin-based antituberculosis cotreatment for A Sub-Saharan Africa population. Pharmacogenomics. 2016;17(6):603–613. doi:10.2217/pgs.16.7
33. von Braun A, Castelnuovo B, Ledergerber B, et al. High efavirenz serum concentrations in TB/HIV-coinfected Ugandan adults with a CYP2B6 516 TT genotype on anti-TB treatment. J Antimicrob Chemother. 2018. doi:10.1093/jac/dky379
34. Cerrone M, Wang X, Neary M, et al. Pharmacokinetics of efavirenz 400 mg once daily coadministered with isoniazid and rifampicin in human immunodeficiency virus–infected individuals. Clin Infect Dis. 2019;68(3):446–452.
35. Gausi K, Wiesner L, Norman J, et al. Pharmacokinetics and drug‐drug interactions of isoniazid and efavirenz in pregnant women living with HIV in high TB incidence settings: importance of genotyping. Clin Pharmacol Ther. 2021;109(4):1034–1044.
36. Gengiah TN, Botha JH, Yende-Zuma N, Naidoo K, Karim SSA. Efavirenz dosing: influence of drug metabolizing enzyme polymorphisms and concurrent tuberculosis treatment. Antivir Ther. 2015;20(3):297–306.
37. Kwara A, Lartey M, Sagoe KW, Court MH. Paradoxically elevated efavirenz concentrations in HIV/tuberculosis-coinfected patients with CYP2B6 516TT genotype on rifampin-containing antituberculous therapy. AIDS. 2011;25(3):388–390.
38. McIlleron HM, Schomaker M, Ren Y, et al. Effects of rifampin-based antituberculosis therapy on plasma efavirenz concentrations in children vary by CYP2B6 genotype. AIDS. 2013;27(12):1933–1940.
39. Ngaimisi E, Mugusi S, Minzi O, et al. Effect of rifampicin and CYP2B6 genotype on long-term efavirenz autoinduction and plasma exposure in HIV patients with or without tuberculosis. Clin Pharmacol Ther. 2011;90(3):406–413.
40. Nightingale S, Chau TTH, Fisher M, et al. Efavirenz and metabolites in cerebrospinal fluid: relationship with CYP2B6 c.516G→T genotype and perturbed blood-brain barrier due to tuberculous meningitis. Antimicrob Agents Chemother. 2016;60(8):4511–4518.
41. Uttayamakul S, Likanonsakul S, Manosuthi W, et al. Effects of CYP2B6 G516T polymorphisms on plasma efavirenz and nevirapine levels when co-administered with rifampicin in HIV/TB co-infected Thai adults. AIDS Res Ther. 2010;7(1):8.
42. Kitabi EN, Minzi OMS, Mugusi S, et al. Long-term efavirenz pharmacokinetics is comparable between Tanzanian HIV and HIV/Tuberculosis patients with the same CYP2B6*6 genotype. Sci Rep. 2018;8(1):16316.
43. Chaivichacharn P, Avihingsanon A, Manosuthi W, et al. Dosage optimization of efavirenz based on a population pharmacokinetic–pharmacogenetic model of HIV-infected patients in Thailand. Clin Ther. 2020;42(7):1234–1245.
44. Manosuthi W, Sukasem C, Thongyen S, Nilkamhang S, Manosuthi S, Sungkanuparph S. CYP2B6 18492T→C polymorphism compromises efavirenz concentration in coinfected HIV and tuberculosis patients carrying CYP2B6 haplotype *1/*1. Antimicrob Agents Chemother. 2014;58(4):2268–2273.
45. Yimer G, Ueda N, Habtewold A, et al. Pharmacogenetic & pharmacokinetic biomarker for efavirenz based ARV and rifampicin based anti-TB drug induced liver injury in TB-HIV infected patients. PLoS One. 2011;6(12):e27810.
46. Enimil A, Antwi S, Yang H, et al. Effect of first-line antituberculosis therapy on nevirapine pharmacokinetics in children younger than three years old. Antimicrob Agents Chemother. 2019;63(10).
47. Uttayamakul S, Likanonsakul S, Manosuthi W, Wichukchinda N, Shioda T, Khusmith S. Influence of ABCB-1 C3435T polymorphisms on plasma nevirapine and efavirenz levels and their effects on virologic and immunological outcomes in HIV/TB co-infected Thai adults under anti-retroviral therapy. Southeast Asian J Trop Med Public Health. 2012;43(1):78–88.
48. Kwara A, Lartey M, Boamah I, et al. Interindividual variability in pharmacokinetics of generic nucleoside reverse transcriptase inhibitors in TB/HIV‐coinfected Ghanaian patients: UGT2B7 *1c Is associated with faster zidovudine clearance and glucuronidation. J Clin Pharmacol. 2009;49(9):1079–1090.
49. Covington N, Luetkemeyer AF, Imperial MZ, et al. Pharmacogenetics of plasma dolutegravir exposure during 1-month rifapentine/isoniazid treatment of latent tuberculosis. Pharmacogenet Genomics. 2025;35(4):140–144.
50. Kengo A, Gausi K, Nabisere R, et al. Unexpectedly low drug exposures among Ugandan patients with TB and HIV receiving high-dose rifampicin. Antimicrob Agents Chemother. 2023;67(11).
51. Calcagno A, Cusato J, Sekaggya‐Wiltshire C, et al. The influence of pharmacogenetic variants in HIV/tuberculosis coinfected patients in Uganda in the south study. Clin Pharmacol Ther. 2019;106(2):450–457.
52. Sundell J, Bienvenu E, Birgersson S, Äbelö A, Ashton M. Effects of enzyme induction and polymorphism on the pharmacokinetics of isoniazid and rifampin in tuberculosis/HIV patients. Antimicrob Agents Chemother. 2022;66(10).
53. Sundell J, Bienvenu E, Janzén D, Birgersson S, Äbelö A, Ashton M. Model‐based assessment of variability in isoniazid pharmacokinetics and metabolism in patients co‐infected with tuberculosis and HIV: implications for a novel dosing strategy. Clin Pharmacol Ther. 2020;108(1):73–80.
54. Kasamatsu A, Miyahara R, Yoneoka D, et al. One-year mortality of tuberculosis patients on isoniazid-based treatment and its association with rapid acetylator NAT2 genotypes. Inter J Infect Dis. 2025;155:107895.
55. Gengiah TN, Botha JH, Soowamber D, Naidoo K, Abdool Karim SS. Low rifampicin concentrations in tuberculosis patients with HIV infection. J Infect Developing Countries. 2014;8(08):987–993.
56. Sundell J, Bienvenu E, Äbelö A, Ashton M. Effect of efavirenz-based ART on the pharmacokinetics of rifampicin and its primary metabolite in patients coinfected with TB and HIV. J Antimicrob Chemother. 2021;76(11):2950–2957.
57. Hennig S, Naiker S, Reddy T, et al. Effect of SLCO1B1 polymorphisms on rifabutin pharmacokinetics in African HIV-infected patients with tuberculosis. Antimicrob Agents Chemother. 2016;60(1):617–620.
58. Sundell J, Bienvenu E, Birgersson S, Äbelö A, Ashton M. Population pharmacokinetics and pharmacogenetics of ethambutol in adult patients coinfected with tuberculosis and HIV. Antimicrob Agents Chemother. 2020;64(2).
59. Petros Z, Kishikawa J, Makonnen E, Yimer G, Habtewold A, Aklillu E. HLA-B*57 allele is associated with concomitant anti-tuberculosis and antiretroviral drugs induced liver toxicity in ethiopians. Front Pharmacol. 2017;8.
60. Cho FN, Achidi EA, Enoh JE, et al. Drug-induced hepatotoxicity and association with slow acetylation variants NAT2*5 and NAT2*6 in Cameroonian patients with tuberculosis and HIV co-infection. BMC Infect Dis. 2024;24(1):759.
61. Araujo-Mariz C, Militão de Albuquerque M de FP, Lopes EP, et al. Hepatotoxicity during TB treatment in people with HIV/AIDS related to NAT2 polymorphisms in Pernambuco, Northeast Brazil. Ann Hepatol. 2020;19(2):153–160.
62. Poeta J, Linden R, Antunes MV, et al. Plasma concentrations of efavirenz are associated with body weight in HIV-positive individuals. J Antimicrob Chemother. 2011;66(11):2601–2604.
63. Group ENCORE1S, Carey D, Puls R, et al. Efficacy and safety of efavirenz 400 mg daily versus 600 mg daily: 96-week data from the randomised, double-blind, placebo-controlled, non-inferiority ENCORE1 study. Lancet Infect Dis. 2015;15(7):793–802.
64. Wessels J, Wilkinson L, editors.. ART Clinical Guidelines for the Management of HIV in Adults, Pregnancy and Breastfeeding, Adolescents, Children, Infants and Neonates.
65. NACO. National Guidelines for HIV Care and Treatment. New Delhi: National AIDS Control Organisation; 2021.
66. Pratt VM, Cavallari LH, Fulmer ML, et al. CYP3A4 and CYP3A5 genotyping recommendations. J Mol Diagn. 2023;25(9):619–629.
67. Mulder TAM, van Eerden RAG, de With M, et al. CYP3A4*22 genotyping in clinical practice: ready for implementation? Front Genet. 2021;12.
68. Cerrone M, Alfarisi O, Neary M, et al. Rifampicin effect on intracellular and plasma pharmacokinetics of tenofovir alafenamide. J Antimicrob Chemother. 2019;74(6):1670–1678.
69. Lee SY, Jang H, Lee JY, Kwon K, Oh SJ, Kim SK. Inhibition of cytochrome P450 by ethambutol in human liver microsomes. Toxicol Lett. 2014;229(1):33–40.
70. Decloedt EH, Mwansa-Kambafwile J, van der Walt JS, et al. The pharmacokinetics of nevirapine when given with isoniazid in South African HIV-infected individuals [Short communication]. Int J Tuberc Lung Dis. 2013;17(3):333–335.
71. Ramachandran G, Hemanthkumar AK, Rajasekaran S, et al. Increasing nevirapine dose can overcome reduced bioavailability due to rifampicin coadministration. J Acquir Immune Defic Syndr. 2006;42(1):36–41.
72. Weiner M, Gelfond J, Johnson-Pais TL, et al. Decreased plasma rifapentine concentrations associated with AADAC single nucleotide polymorphism in adults with tuberculosis. J Antimicrob Chemother. 2021;76(3):582–586.
73. Williamson B, Dooley KE, Zhang Y, Back DJ, Owen A. Induction of influx and efflux transporters and cytochrome P450 3A4 in primary human hepatocytes by rifampin, rifabutin, and rifapentine. Antimicrob Agents Chemother. 2013;57(12):6366–6369.
74. Castellino S, Moss L, Wagner D, et al. Metabolism, excretion, and mass balance of the HIV-1 integrase inhibitor dolutegravir in humans. Antimicrob Agents Chemother. 2013;57(8):3536–3546.
75. Klomp SD, Manson ML, Guchelaar HJ, Swen JJ. Phenoconversion of cytochrome P450 metabolism: a systematic review. J Clin Med. 2020;9(9).
76. Li F, Lu J, Cheng J, et al. Human PXR modulates hepatotoxicity associated with rifampicin and isoniazid co-therapy. Nat Med. 2013;19(4):418–420.
77. Lin YN, Chen CJ, Chang HY, et al. Oleanolic acid-mediated inhibition of pregnane X receptor and constitutive androstane receptor attenuates rifampin-isoniazid cytotoxicity. J Agric Food Chem. 2017;65(39):8606–8616.
78. Chang HY, Chen CJ, Ma WC, et al. Modulation of pregnane X receptor (PXR) and constitutive androstane receptor (CAR) activation by ursolic acid (UA) attenuates rifampin-isoniazid cytotoxicity. Phytomedicine. 2017;36:37–49.
79. Wang Y, Xiang X, Huang WW, et al. Association of PXR and CAR polymorphisms and antituberculosis drug-induced hepatotoxicity. Sci Rep. 2019;9(1):2217.
80. Zhang J, Zhao Z, Bai H, et al. Genetic polymorphisms in PXR and NF-κB1 influence susceptibility to anti-tuberculosis drug-induced liver injury. PLoS One. 2019;14(9):e0222033.
81. Faucette SR, Zhang TC, Moore R, et al. Relative activation of human pregnane X receptor versus constitutive androstane receptor defines distinct classes of CYP2B6 and CYP3A4 inducers. J Pharmacol Exp Ther. 2007;320(1):72–80.
82. Ngaimisi E, Mugusi S, Minzi OM, et al. Long-term efavirenz autoinduction and its effect on plasma exposure in HIV patients. Clin Pharmacol Ther. 2010;88(5):676–684.
83. Sousa-Pinto B, Pinto-Ramos J, Correia C, et al. Pharmacogenetics of Abacavir hypersensitivity: a systematic review and meta-analysis of the association with HLA-B*57:01. J Allergy Clin Immunol. 2015;136(4):1092–1094.e3.
84. Yimer G, Gry M, Amogne W, et al. Evaluation of patterns of liver toxicity in patients on antiretroviral and anti-tuberculosis drugs: a prospective four arm observational study in ethiopian patients. PLoS One. 2014;9(4):e94271.
85. Martín AS, Gómez AI, García-Berrocal B, et al. Dose reduction of efavirenz: an observational study describing cost–effectiveness. Pharmacokinetics Pharmacogenetics Pharmacogenomics. 2014;15(7):997–1006.
86. Schackman BR, Haas DW, Park SS, Li XC, Freedberg KA. Cost–effectiveness of CYP2B6 genotyping to optimize efavirenz dosing in HIV CLINICAL PRACTICE. Pharmacogenomics. 2015;16(18):2007–2018.
87. Hardi H, Barinda A. One step ahead in realizing pharmacogenetics in low- and middle-income countries: what should we do?. J Multidiscip Healthc. 2024;17:5061–5062.
88. Omran S, Leong SL, Blebil A, Mohan D, Ang WC, Teoh SL. The needs and gaps in pharmacogenomics knowledge and education among healthcare professionals in Malaysia: a multisite Delphi study. Clin Transl Sci. 2024;17(11).
89. Hardi H, Barinda AJ, Mahata LE, Fitrianti Z. CYP2C19 variability and clinical outcomes of clopidogrel, proton pump inhibitors, and voriconazole in Southeast Asia: a systematic review and meta-analysis. Front Pharmacol. 2025.
90. Azuma J, Ohno M, Kubota R, et al. NAT2 genotype guided regimen reduces isoniazid-induced liver injury and early treatment failure in the 6-month four-drug standard treatment of tuberculosis: a randomized controlled trial for pharmacogenetics-based therapy. Eur J Clin Pharmacol. 2013;69(5):1091–1101.
91. Sorich MJ, Rowland A, Wiese MD. Pharmacogenomic substudies of randomized controlled trials: consideration of safety outcomes. Ther Adv Drug Saf. 2014;5(2):62–66.
92. Stevenson JM, Smith DM, Tuteja S, Patel JN. Navigating pharmacogenomic testing in practice: who to test and when to test. Clin Pharmacol Ther. 2025;118(3):561–566.
93. Chaplin M, Kirkham JJ, Dwan K, Sloan DJ, Davies G, Jorgensen AL. STrengthening the reporting of pharmacogenetic studies: development of the STROPS guideline. PLoS Med. 2020;17(9):e1003344.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.