Back to Journals » Advances in Medical Education and Practice » Volume 16
Pharmacogenetics Education for Pharmacy Students: Measuring Knowledge and Attitude Changes
Authors Alsayed AR ![]() , Abu Ajamieh M, Melhem M, Samara A, Hakooz N
, Abu Ajamieh M, Melhem M, Samara A, Hakooz N ![]()
Received 18 May 2025
Accepted for publication 2 September 2025
Published 30 September 2025 Volume 2025:16 Pages 1761—1779
DOI https://doi.org/10.2147/AMEP.S541244
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Ahmad R Alsayed,1 Mays Abu Ajamieh,2 Mais Melhem,3 Anas Samara,4 Nancy Hakooz5
1Department of Clinical Pharmacy and Therapeutics, Faculty of Pharmacy, Applied Science Private University, Amman, Jordan; 2Pharmaceutical Research Unit, Amman, Jordan; 3Al-Saudi Hospital, Ammam, Jordan; 4Department of Software Engineering, Bethlehem University, Bethlehem, Palestine; 5School of Pharmacy, The University of Jordan, Amman, Jordan
Correspondence: Ahmad R Alsayed, Department of Clinical Pharmacy and Therapeutics, Faculty of Pharmacy, Applied Science Private University, Amman, Jordan, Tel +962786770778, Email [email protected]; [email protected]
Purpose: This study aimed to assess the knowledge and attitudes changes of pharmacy students in Jordan toward pharmacogenetics (PGx) education.
Patients and Methods: The study has involved both quantitative and qualitative approaches. The quantities part investigates the pre- and post-test scores of 95 pharmacy students studying PGx at the University of Jordan. The surveys were administered before and after the educational intervention, which lasted 14 weeks. The qualitative aspect included focus group discussions, where the participants deeply revealed their perceptions of PGx.
Results: The study showed that 66.3% of students “strongly agreed that genes received from parents are the main influencers of medication response”, in comparison to 45.3% of the students at the baseline (p < 0.001). The belief that gene variants are correlated with the susceptibility to the side effects of drugs was one of the lessons that benefited the most, with an improvement from 45.3% to 72.6% (p < 0.001). At the end of the intervention, 75.8% of students approved PGx execution being pharmacists’ job, whereas 44.2% voted for it at the baseline (p < 0.001). Following the intervention, 75.8% of students strongly agreed that PGx testing should be part of pharmacy education, up from 61.1% (p = 0.016). The number of students that strongly agreed that genetic testing would make drug selection significantly improves from 55.8% to 78.9% (p = 0.002). Focus group interviews confirmed these findings. Students valued talking about tailored medication and promoted PGx to their future employers. According to several students, the PGx course should be mandatory for PharmD students and offered earlier for better practical use.
Conclusion: The PGx educational intervention improved students’ PGx knowledge and attitudes. The study underscores the need to integrate PGx into pharmacy courses to educate students about personalized medicine in clinical practice.
Keywords: pharmacogenetics, personalized medicine, pharmacy education, attitudes and knowledge, educational intervention, Jordan
Introduction
Pharmacogenomics (PGx) and pharmacogenetics are both dedicated to the study of genetic influences on drug response. Concerning precision medicine, PGx focuses only on drug response; however, it has a wider scope and different approach than pharmacogenetics. Historically, pharmacogenetics focused on examining the effects of single-gene variation on an individual’s drug response and has typically investigated polymorphisms in drug-metabolizing enzymes, transporters, or drug targets that could modify either pharmacokinetics or pharmacodynamics. PGx takes a more global look at the genome, examining the aggregate effect of many genetic variants across the whole genome on drug response (efficacy and safety). PGx combines high-throughput technologies, including next-generation sequencing and bioinformatics algorithms to uncover complicated gene–gene and gene–environment connections impacting therapeutic responses. Overall, they contribute to personalized medicine through the selection of drugs with greater efficacy and reduced toxicity or adverse reactions by way of drug dosage optimization.1–4
Personalized medicine and medication management depend on PGx, so knowledge in this field is growing relevant in pharmacy courses. Pharmacy courses incorporate PGx teaching in several ways: mandatory courses, interactive learning, and personal genomic testing among other things.5 Classes such as “Principles in Genetics and Pharmacogenomics” have shown to assist students in seeing their responsibilities in PGx.6 Personal DNA testing and other innovative courses have helped students become more confident and competent in PGx.7 By means of personal genomic testing, programs such as “Test2Learn” increase PGx teaching, therefore fostering better understanding and empathy among students.8
Pharmacy students generally perceive PGx as a clinically relevant tool, yet many feel inadequately prepared to apply this knowledge in practice. Surveys indicate that while students recognize the importance of PGx, they often report limited exposure and training, with many receiving only a few lectures on the topic. Despite this, students express positive attitudes towards the clinical relevance of PGx and show interest in practice-based training to enhance their readiness.9
Lack of faculty competence, lack of practice environments for experimental learning, and variation in the depth of PGx teaching across pharmacy schools are a few of the several obstacles standing in the way of PGx education’s spread.10,11 To address these challenges, strategies such as early exposure through foundational courses, incorporation into practice-based therapeutics courses, and the use of online resources and workshops have been suggested.10,11 Additionally, there is a need for standardized guidelines and increased accessibility to PGx testing to support pharmacists in clinical practice.12
Recent evidences collectively highlight the positive impact of pharmacogenomics educational interventions on the knowledge, confidence, and clinical competence of healthcare professionals and students.13,14 Omran et al13 conducted a broad systematic review of 50 studies assessing PGx educational interventions across various healthcare disciplines, concluding that the integration of active learning strategies—particularly clinical case-based teaching—consistently improved participants’ knowledge, attitudes, and practice of PGx.
Globally, pharmacy education often lacks sufficient content on PGx principles and clinical applications, and pharmacy students in Jordan are no exception, even though pharmacogenetics is increasingly being acknowledged as a major component of personalized medicine. This calls for a timely reevaluation and reformation of pharmacy education so future pharmacists can better understand PGx and utilize it confidently. To address this gap, our current research evaluates the effectiveness of a structured educational intervention on pharmacy students’ knowledge and attitudes toward PGx. The aim of this study was to evaluate the knowledge and attitudes of pharmacy students in Jordan towards PGx before and after having taken a PGx course, using both quantitative and qualitative tools.
Materials and Methods
Study Design
This study involved a mixed-methods approach combining quantitative and qualitative designs to comprehensively evaluate the changes of knowledge and attitudes toward PGx education among pharmacy students in Jordan. The quantitative component involved a structured questionnaire to gather baseline and post-intervention data, while the qualitative component involved focus group discussions to explore in-depth perceptions and insights.15,16
Quantitative Component
Participants
A total of 95 pharmacy students from the University of Jordan participated in the study. The participants were selected from fourth- and fifth-year students enrolled in a PGx elective course during the academic year 2024–2025. This represents a convenience sample encompassing the entire class cohort.
Data Collection
An evaluation form was used to collect data on students’ knowledge and attitudes about PGx. The questionnaire included demographics, baseline knowledge, exposure to PGx, and specific knowledge and attitude questions related to PGx principles, clinical applications, and barriers to implementation.
Instrumentation
The survey instrument was divided into sections, according to a recent study,15 including:
- Demographics: Gender, age, specialty (BPharm or PharmD), year of study, and overall grade point average (GPA).
- Baseline Knowledge and Exposure: Questions on prior exposure to PGx courses or workshops and sources of information.
- Knowledge Assessment: A series of questions assessing knowledge of PGx principles, specific PGx tests, and the clinical impact of PGx on drug response.
- Attitude Assessment: Statements gauging personal beliefs, perceived responsibilities, and the relevance of PGx in clinical practice.
Designing and Implementing the Tutorial Intervention
The researchers’ own experiences and the current literature guided the development of the educational intervention. The material was checked and established to confirm the accurate and exact information supplied before the intervention started. Before starting the educational intervention, the first step of this study consisted of pre-testing students. The execution of the educational intervention constituted the second step. The third step consisted of taking the post-intervention evaluation. The fourth step involved a focus group conversation among intervention participants in order to get feedback about the intervention.
Two researchers (both with PhD degrees in clinical pharmacy and at least ten years’ experience in the field) supervised the educational intervention and data collection. Every survey was sent in English, the official language used at Jordanian Schools of pharmacy education. To guarantee face validity, three seasoned researchers with a varied spectrum of professional clinical knowledge and extensive experience in clinical investigations assessed the questionnaires prior to the current study.
Part 1: Pre-Intervention Part
After acquiring students’ informed consent, a pre-training data collection form and the ability to analyze a clinical case were used to assess students’ knowledge and skills regarding the PGx. Students were requested to complete a questionnaire to gather data on demographic variables during that period.
Part 2: The Delivery of the Intervention
The course consisted of lectures for 14 weeks. Throughout the weeks, tutorials were offered and included PGx knowledge, skills, and special sessions with healthcare experts who almost use PGx on a daily basis.
Part 3: Post-Intervention
An online post-intervention test was administered, similar to the contents of the questionnaire used before the start of the course.
Statistical Analysis
Quantitative data were analyzed using SPSS version 29 and R software version 4.3.3 to ensure comprehensive and robust analysis. Descriptive statistics were used to summarize students’ demographic and baseline knowledge-related data.
The Wilcoxon signed-rank test was performed to evaluate changes in knowledge and attitudes pre- and post-intervention, which is suitable for non-parametric data analysis. The McNemar test was used to analyze shifts in awareness and understanding of PGx concepts, highlighting changes in categorical variables before and after the educational tool.
R software was used to perform additional statistical tests that required complex modeling, ensuring thorough exploration and interpretation of the data.
Qualitative Component
Participants
Focus group discussions were conducted with a subset of students who completed the quantitative part. The students were selected based on their willingness to participate and represent diverse experiences and perspectives on PGx education.
Data Collection
A semi-structured interview guide was developed to facilitate focus group discussions. The guide included questions on:
- Motivation and Background: Reasons for enrolling in the PGx course and initial awareness.
- Curriculum and Content: Integration of PGx in the curriculum, perceived relevance, and depth of content covered.
- Teaching Methods and Resources: Effectiveness of various teaching methods and resources in enhancing understanding.
- Application and Practice: Confidence in applying pharmacogenetics knowledge in clinical settings and real-world examples of PGx in practice.
- Challenges and Barriers: Learning challenges and barriers to implementing PGx in pharmacy practice.
- Feedback and Suggestions: Suggestions for improving PGx education and support needs.
Data Analysis
Qualitative data from focus group discussions were transcribed and analyzed using thematic analysis. Themes were identified through an iterative coding process, focusing on key areas of interest such as curriculum integration, teaching effectiveness, and application challenges. The analysis aimed to understand students’ perceptions and experiences with PGx education comprehensively. Specifically, two independent researchers coded the transcripts inductively, developing initial codes, which were then grouped into broader themes. Coding discrepancies were discussed and resolved by consensus. Inter-rater reliability was assessed using Cohen’s κ, which demonstrated substantial agreement (κ = 0.90).
Ethical Considerations
The study was conducted following ethical guidelines for research involving human participants. Informed consent was obtained from all participants, ensuring confidentiality and anonymity of responses, and they were fully informed about the aim of the research. The study received ethical approval from the University of Jordan. This study complies with the Declaration of Helsinki.
Results
Demographic Data
This study consisted of 95 participants; the majority of them were females (n = 83, 87.4%). The mean age of students was 22.2 years (SD = 0.921). The majority were Bachelor of Pharmacy (BPharm) students (65.3%), while 34.7% were Doctor of Pharmacy (PharmD) students. Most students were in their fifth year of study (84.2%), with 15.8% in the fourth year. Regarding academic performance, 22 (23.2%) students had an excellent overall grade, 47 (49.5%) had a very good grade, and 25 (26.3%) had a good grade (Table 1).
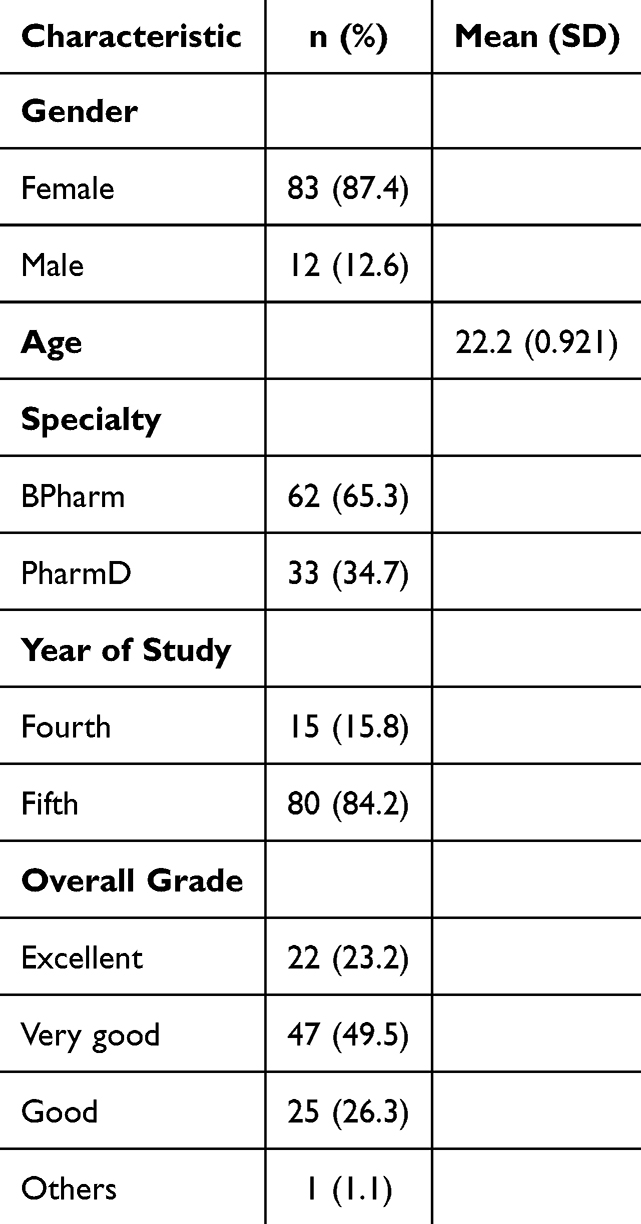 |
Table 1 Demographic Data of the Students (N = 95) |
Baseline Knowledge and Exposure to Pharmacogenetics
As shown in Table 2, 68 participants (71.6%) had not attended any course or workshop on PGx before this study, while 18 (18.9%) had attended once, and 9 (9.5%) had attended more than once. Most students (71.6%) had heard of PGx from university lectures. Other sources included scientific meetings (40.0%), conferences (28.4%), social media (69.5%), television (23.2%), and other sources (36.8%). The majority (89.5%) reported studying the concept of genetic variability in drug response during their university courses (Table 2).
 |
Table 2 Baseline Knowledge and Exposure to Pharmacogenetics |
Changes in Knowledge and Perceptions of Pharmacogenomics
Figure 1 represents the improvement in knowledge of pharmacogenetics after the educational intervention.
 |
Figure 1 Knowledge Towards Pharmacogenetics. The values inside the bars are the frequencies. |
Figure 2 presents a comparison of pharmacy students’ perceptions of the genetic influence on drug response and pharmacokinetics before and after an educational intervention. The results are depicted as percentages of responses to a series of statements, categorized by the level of agreement.
 |
Figure 2 Comparison of Pharmacy Students’ Perceptions of Genetic Influence on Drug Response and Pharmacokinetics Before and After Educational Intervention. |
Prior the educational intervention, 45.3% of students strongly agreed that genes inherited from the parents affect the responses to medications, with an additional 47.4% agreeing. Following the intervention, this perception strengthened, with 66.3% strongly agreeing and 29.5% agreeing, indicating a notable increase in the recognition of genetic factors in drug response (Figure 2).
At baseline, 68.4% of students strongly agreed that individuals from different ethnicities might respond differently to drugs based on their genes, with 26.3% agreeing. Following the intervention, 77.9% strongly agreed, while 21.1% agreed, showing an increased understanding that genetic variability is critical in drug efficacy.
Similarly, 43.2% strongly agreed that pharmacokinetic differences among individuals can be attributed to genetic variations. These perceptions improved, with 72.6% strongly agreeing (Figure 2).
Pre-education, 56.8% strongly agreed that differences in drug response between individuals are due to genetic differences. Post-education, 65.3% strongly agreed with this statement, reflecting an increase in recognition of genetic influences on drug response.
Pre-education, 44.2% strongly agreed that some patients might not respond to drugs because of genetic mutations. Post-education, these perceptions strengthened, with 70.5% strongly agreeing, indicating a growing understanding of the role of genetic mutations in drug response failures (Figure 2).
Pre-education, 45.3% strongly agreed that some patients might be more prone to drug side effects due to their genetic makeup. Post-education, 72.6% strongly agreed, reflecting an increase in the acknowledgment of genetic predispositions to adverse drug reactions.
Furthermore, 45.3% strongly agreed at baseline that drug interactions with receptors or enzymes might depend on the patient’s genes. There was an increase in understanding, with 68.4% strongly agreeing, highlighting the educational impact on students’ comprehension of gene-drug interactions (Figure 2).
The results of the sign test for changes in PGx perceptions before and after the intervention are presented in Table 3. A significant shift in perception was observed in most of the questions (p < 0.05) (Table 3).
 |
Table 3 Sign Test Results of Response Changes in Pharmacogenomics Perceptions Before and After Intervention |
The students demonstrated a significant increase in their knowledge of basic PGx principles, specific PGx tests, and the impact of PGx on drug dosing and prescribing, all with p-values less than 0.001.
Specifically, significant improvements were observed in the understanding that genes inherited from parents affect drug response (p<0.001) and that differences in pharmacokinetics and drug interactions with receptors or enzymes are influenced by genetic factors (both p < 0.001). Furthermore, the perception that some patients might be more prone to drug toxicities or lack of response due to genetic differences also showed significant changes (p < 0.001 for both).
Regarding the relevance of PGx in pharmacy practice, students agreed that it is important to have a PGx course in the university curriculum (p = 0.016) and recognized the importance and relevance of PGx in pharmacy practice (p = 0.002). They also believed pharmacogenomic testing could improve patient outcomes and safety (p = 0.002). Additionally, they agreed that PGx testing will help them choose the right drug at the right dose as pharmacists (p < 0.001).
However, there were some areas where perceptions did not change significantly. For example, the belief that differences in drug response between individuals might be due to genetic differences (p = 0.188) and that different ethnicities might respond differently to drugs according to their genes (p = 0.061) did not show significant changes. [Similarly, no significant changes were observed in the perceptions of the ease of PGx testing (p = 0.144), the convenience of genotyping for all individuals (p = 0.795), and the concern that insurance companies might use genotyping unethically (p = 0.155).] During the focus group discussion, most students discussed that genetic testing and the ethical dimensions surrounding it are barriers for the implementation of PGx in Jordan.
Interestingly, the perception of pharmacists’ responsibility in implementing PGx testing before prescribing drugs approached significance but did not reach the threshold (p = 0.077). Confidence in applying PGx knowledge in future practice did not show significant improvement (p = 0.590). In the focus group conversation, students iterated that they need some improvements to the course in the form of first-hand experience and/or training through self-testing, lab visits.etc in order to become more confident about applying PGx in practice.
In summary, the intervention resulted in significant positive changes in the majority of perceptions related to PGx, highlighting the effectiveness of the education in enhancing participants’ understanding and attitudes toward this field.
Changes in Awareness and Knowledge
The McNemar test results with exact p-values (Table 4) highlighted significant changes in awareness and knowledge of pharmacogenetics concepts and their applications.
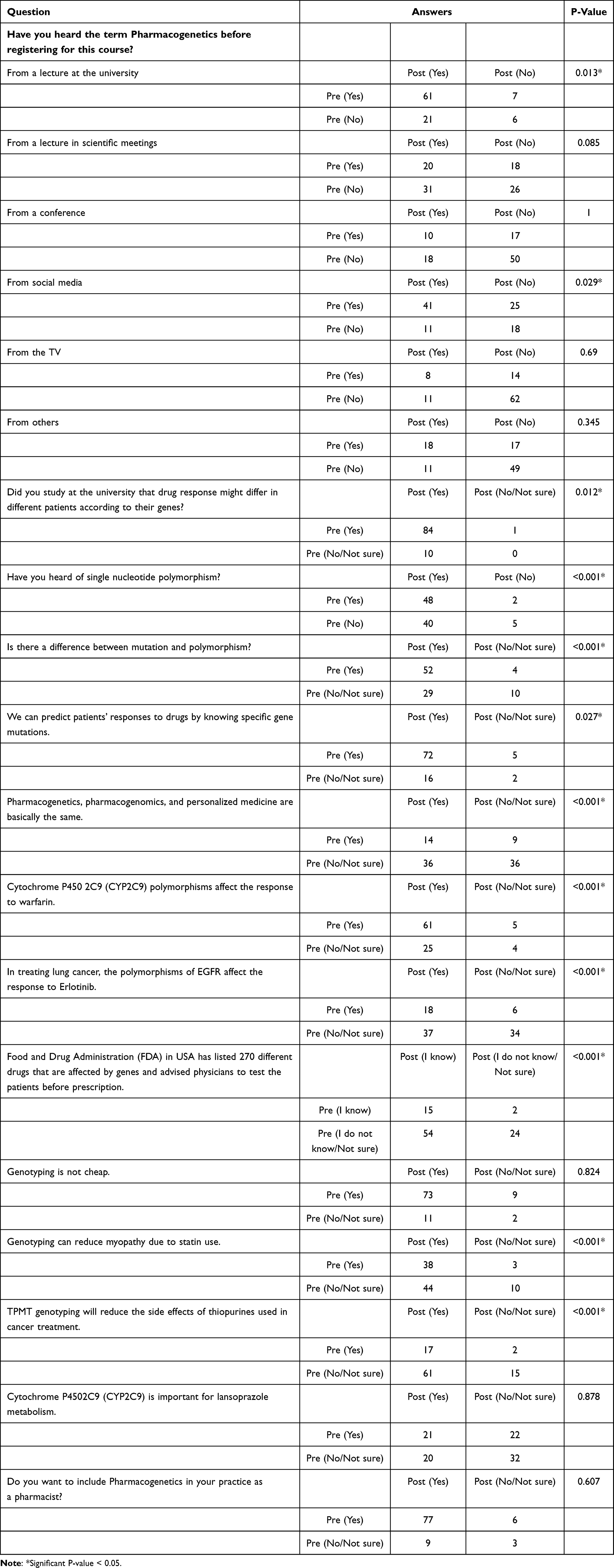 |
Table 4 Changes in Awareness and Knowledge of Pharmacogenetics as Measured by the McNemar Test |
Regarding the awareness of Pharmacogenetics terms, there was increased awareness from various sources such as university lectures (p = 0.013) and social media (p = 0.029). Significant improvements were seen in understanding the genetic impact on drug response and specific applications, such as CYP2C9 polymorphisms affecting warfarin response (p < 0.001) and the importance of genotyping in reducing side effects (p < 0.001) (Table 4).
Pharmacogenetics in Clinical Practice
Figure 3 presents a comparative analysis of students’ perceptions regarding various aspects of pharmacogenomics before and after an educational intervention. The responses are categorized across five levels: Strongly disagree, Disagree, Neutral, Agree, and Strongly agree. Several trends are observed, focusing on the percentage changes in the “Strongly agree” category.
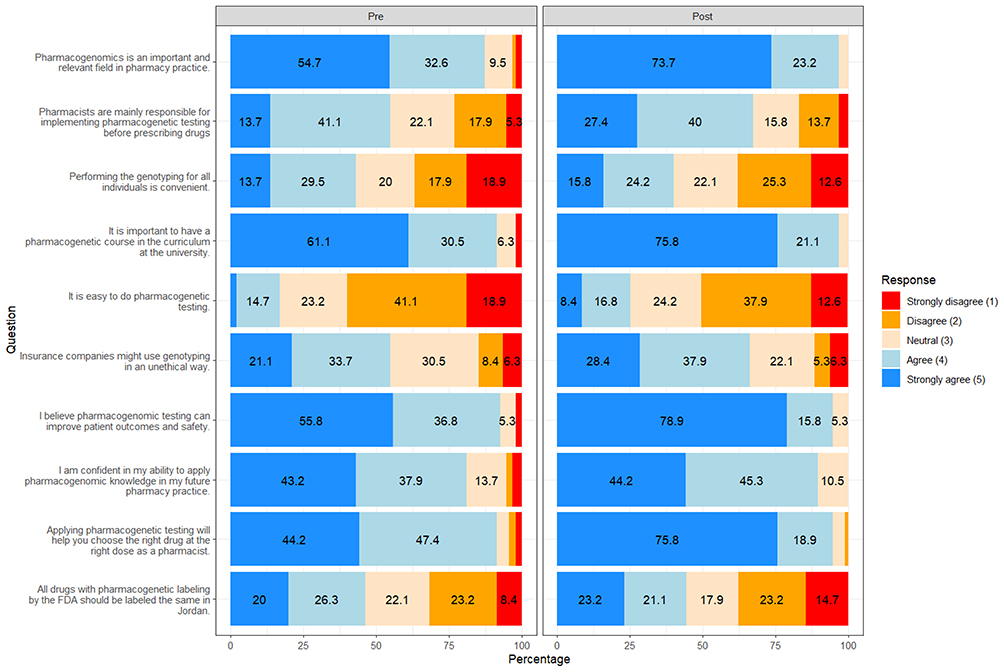 |
Figure 3 Pharmacy students’ attitudes toward the role and implementation of pharmacogenetics in clinical practice. The values inside the bars are the frequencies. |
For the statement “Pharmacogenomics is an important and relevant field in pharmacy practice”, there was an increase in the percentage of students who strongly agreed, rising from 54.7% before the intervention to 73.7% afterward, reflecting a 19.0% increase. Similarly, the perception that “Pharmacists are mainly responsible for implementing pharmacogenetic testing before prescribing drugs” also saw an increase in strong agreement, from 13.7% to 27.4%, indicating a 13.7% rise.
The importance of having a pharmacogenetic course in the university curriculum was recognized more strongly post-intervention, with 75.8% of students strongly agreeing, up from 61.1%, showing a 14.7% increase.
There was also a notable rise in the belief that “Pharmacogenomic testing can improve patient outcomes and safety”, with the percentage of students who strongly agreed to increase by 23.1%, from 55.8% to 78.9%. Additionally, confidence in applying pharmacogenomic knowledge in future pharmacy practice slightly improved, with strong agreement rising by 1.0%, from 43.2% to 44.2%.
Furthermore, the belief that “Applying pharmacogenetic testing will help choose the right drug at the right dose as a pharmacist” saw a substantial increase, with 75.8% of students strongly agreeing post-intervention, compared to 44.2% pre-intervention, reflecting a 31.6% rise. Finally, the statement regarding the uniform labeling of drugs with pharmacogenomic labeling by the FDA in Jordan saw a modest increase in strong agreement, rising from 20.0% to 23.2%, a 3.2% increase (Figure 3).
Figure 4 shows participants’ responses before and after an educational intervention regarding their interest in pharmacogenetics, both in postgraduate studies and in future pharmacy practice. The question “Would you consider Pharmacogenetics in your postgraduate studies (MSc, PhD)?” indicated a notable shift in attitudes post-intervention. The percentage of participants answering “Yes” decreased slightly from 68.9% pre-intervention (n = 56) to 54.7% post-intervention (n = 52). Interestingly, the proportion of participants who were “Not sure” increased from 22 (27.4%) to 23.2% (n = 22), while those stating “No” decreased from 7.4% (n = 6) to 4.2% (n = 4). The number who expressed no interest in postgraduate studies rose marginally from 3.2% (n = 3) pre- to 11.6% (n = 11) post-intervention.
 |
Figure 4 Future Plans for Incorporating Pharmacogenetics in Professional Practice. |
In contrast, the question “Do you want to include Pharmacogenetics in your practice as a pharmacist?”, a clear positive trend is evident. Following the intervention, 90.5% (n = 86) of participants expressed a desire to include pharmacogenetics in their practice, up from 87.4% (n = 83) pre-intervention. Additionally, “Not sure” responses decreased from 9.5% (n = 9) to 8.4% (n = 8), and “No” responses fell from 3.2% (n = 3) to only 1.1% (n = 1). This indicates a strengthened professional commitment to incorporating pharmacogenetics into pharmacy practice following the educational exposure.
These results imply that although enthusiasm for applying pharmacogenetics in actual clinical practice was reinforced after the intervention, opinions on pursuing additional PGx education were not necessarily common. The lower percentage of “Yes” responses for graduate studies might perhaps reflect a more realistic appreciation of the complexity of the field and time needed to prepare for it. In contrast, the substantial increase in intent to incorporate pharmacogenetics into practice demonstrates the intervention’s impact in strengthening its clinical relevance and applicability (Figure 4).
Table 5 provides a comprehensive summary of the focus group discussions. The results highlight several key areas of interest, motivation, awareness, and perceptions among the students.
 |
Table 5 Comprehensive Summary of Focus Group Responses on Pharmacogenetics Education in Pharmacy Curriculum |
The main motivations for students enrolling in the pharmacogenetics course were positive peer feedback, a growing interest in personalized medicine, and a better understanding of the interaction between genetics and drug effectiveness. Prior to the course, awareness of pharmacogenetics varied, with most students possessing only a superficial sense gained from brief mentions in other classes such as pharmacotherapy and biotechnology.
After taking the course, the students reported a substantial increase in their understanding of PGx. They now understand the clinical applications of PGx, and they are familiar with critical resources.
There was a divide in opinions regarding the course’s appropriate timing and mandatory status. Some students felt the course should be taken earlier in their studies, possibly in the third year, to allow more time for applying the knowledge in clinical settings. Others believed the fifth-year timing was appropriate, aligning with their more advanced clinical training. The consensus, however, was that the course should be mandatory, especially for PharmD students, given the increasing importance of PGx in modern pharmacy practice.
The students identified online resources, lectures, and guest lecturers as the most effective teaching methods. However, there was a strong desire for more practical exposure, such as lab work, field visits, and practical demonstrations, particularly in understanding complex topics. The absence of technological tools like simulation software or genetic testing kits in their education was noted, and students expressed interest in incorporating these tools into the curriculum.
Students expressed varying levels of confidence in applying PGx knowledge in clinical settings, with higher confidence reported in cases involving drugs with serious side effects, such as warfarin or oncology drugs. Real-world examples highlighted the potential of PGx to improve clinical decision-making, particularly in cases where genetic testing could alleviate patient concerns about side effects from drugs.
Students suggested several improvements to the PGx curriculum, including the integration of bioinformatics, guest lecturers, and the inclusion of practical demonstrations and field visits. These improvements were seen as essential for bridging the gap between theoretical knowledge and its practical application in clinical settings.
In conclusion, the focus group conversations expose a general strong desire and perceived need for PGx knowledge included within the pharmacy curriculum. Although the course has effectively improved students’ knowledge and understanding, more practical, hands-on learning chances and more integration of PGx into the larger pharmacy education and practice clearly demand.
Discussion
This study evaluated the effect of a structured educational intervention on pharmacy students’ knowledge and attitudes regarding PGx in Jordan. The results highlighted a remarkable increase in students’ comprehension of essential PGx principles, their capacity to associate genetic variation with drug response, and their perspectives on incorporating PGx into pharmacy practice. These findings demonstrate the impact of standardized PGx education in preparing students for careers in precision medicine.
A major finding was the increase in students’ agreement with important PGx concepts after receiving the education intervention. In fact, one example, knowledge of how genetic mutations are able to affect drug response, was strongly agreed upon by 44.2% of students post assessment intake, and 70.5% of students post assessment outtake (p < 0.001). Similar gains were made in awareness of gene–drug interactions and the genetic basis of adverse drug reactions and pharmacokinetics. These findings align with prior studies showing that PGx education improves students’ knowledge and confidence. Assem et al7 found that personal DNA testing markedly enhanced students’ perceived competence in PGx, whereas Adams et al8 reported enhanced empathy and comprehension subsequent to the implementation of educational genomic testing.
There were also statistically significant increases in perceived relevance of PGx in clinical practice. After the intervention, the percentage of students who strongly agreed that PGx should be included in pharmacy education (75.8% vs 61.1%; p = 0.016) and that PGx could enhance patient outcomes and safety (78.9% vs 39.5%; p = 0.002) increased significantly. Coriolan et al9 confirmed these findings and reported that from our review of students’ opinions and training in PGx.
Qualitative findings also contributed towards a richer interpretation of these results. Student comments in focus groups showed appreciation of the course content and the sense that it filled an important gap in their education. But they expressed a need for more focused hands-on experience and earlier introduction of PGx in the curriculum. These findings align with the previous recommendations for increased experiential education and training in PGx.17,18 The moderate confidence in using PGx knowledge in real life encountered by students after the intervention was similar to previous studies,9,19 which suggested a need for students to have practice-based training settings to supplement their knowledge after theoretical learning.
The current study adds more evidence on PGx education in the Middle East particularly in Jordan compared to the other external undertaken studies. Yet, evidence from North America and Europe dominates the findings from previous studies, and this study fills a regional gap in the existing literature and offers culturally relevant data to inform curriculum design.
Pharmacy students generally feel underprepared for PGx practice, despite recognizing its importance in clinical settings. While educational interventions have shown promise in improving confidence and competence, gaps remain in readiness for practical application.
Many pharmacy students have a moderate understanding of PGx, with knowledge levels varying based on academic exposure and the institution attended. Students generally recognize the clinical relevance of PGx and express a desire to learn more about its application in practice.12,19,20
Courses that include hands-on components, such as DNA testing and genotyping, have been effective in enhancing students’ understanding and confidence in PGx. These interventions help students appreciate the potential of PGx in personalized medicine and improve their readiness to apply this knowledge in clinical settings.17,18
Despite positive attitudes towards PGx, many students feel inadequately prepared to implement it in practice. This is often due to limited exposure in their curriculum, with many students receiving only a few lectures on the topic. Practice-based training, such as PGx rotations, is seen as beneficial for better preparation.9,21
In recent studies, students and pharmacists stated several barriers to the implementation of PGx, including limited accessibility to testing, lack of standardized guidelines, and concerns about misinterpretation of test results.12,19
This study does provide meaningful insights regarding the effectiveness of PGx education, but some limitations must be recognized. First, the research was carried out in only one institution with relatively low sample size, which may limit the generalization of the results to other pharmacy schools in Jordan or worldwide. Second, the restraint of the intervention period and the use of self-reported attitudes alone may be insufficient to address the sustained retention of knowledge or the ability to implement PGx in the real-world clinical setting. Also, while focus groups provided qualitative detail, they relied on self-selected participants, which may have generated response bias in addition to the possible social desirability bias in focus group responses. Lastly, a lack of experiential learning or opportunities to perform PGx testing in practice may have limited students’ confidence and readiness for the practice setting.
In summary, the results highlight the need for the implementation of structured, experiential-based PGx education within pharmacy curricula. They should also work to incorporate practical components such as case-based learning, simulation tools, and awareness of genetic testing technologies into future initiatives as a way to prepare students for eventual clinical implementation.
Conclusion
This study showed that a structured PGx educational intervention significantly improved pharmacy students’ knowledge and attitudes relevant to the clinical application of PGx. Study findings highlight the critical need to incorporate broader PGx education into the curricula of pharmacy colleges to prepare future pharmacists for practice in precision medicine. A move towards such initiatives alongside practical experiences for students and institutional implementation can only help prepare our pharmacy graduates for practicing PGx as part of the wider optimization of patient care. Also, this study calls for experiential/practical modules in PGx education based on the students feedback.
Acknowledgments
We would like to thank Anas Nizar for his assistance in the statistical analysis and also the participating students.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Weinshilboum RM, Wang L. Pharmacogenetics and pharmacogenomics: development, science, and translation. Ann Rev Genomics Hum Genet. 2006;7(1):223–245. doi:10.1146/annurev.genom.6.080604.162315
2. Zihlif M, Zakaraya Z, Al-Shudiefat AAR, Alsayed AR. Association between toll-like receptor 4 gene and inflammatory bowel disease among Jordanian patients. Pharmacy Pract. 2024;22(4):1–7. doi:10.18549/PharmPract.2024.4.3005
3. Zihlif M, Zakaraya Z, Habahbeh L, et al. Beta2-adrenergic receptor polymorphisms among healthy Jordanian population. Pharmacy Pract. 2024;22(4):1–6.
4. Zihlif M, Tanina N, Batah A, et al. The medicinal plants effects on the gene expression of cytochrome P450 and P-glycoprotein in cultured colon and breast cancer cell line. Pharmacy Pract. 2024;22(2):1–7.
5. Duong Nguyen TT, Tanoli Z, Hassan S, et al. PGxDB: an interactive web-platform for pharmacogenomics research. Nucleic Acids Res. 2024;53(D1):D1486–D1497. doi:10.1093/nar/gkae1127
6. Zheng MH, Guo B, Yuan LQ, et al. The interplay between the renin-angiotensin-aldosterone system and parathyroid hormone. Front Endocrinol. 2020;11(Pt 2). doi:10.3389/fendo.2020.00539
7. Assem M, Broeckel U, MacKinnon GE. Assessing learners’ attitudes towards pharmacogenomics using their own pharmacogenomics testing results. American J Pharmaceutical Educ. 2020;85(4).
8. Adams SM, Anderson KB, Coons JC, et al. Advancing pharmacogenomics education in the core PharmD curriculum through student personal genomic testing. American J Pharmaceutical Educ. 2016;80(1):3. doi:10.5688/ajpe8013
9. Coriolan S, Arikawe N, Moscati A, et al. Pharmacy students’ attitudes and perceptions toward pharmacogenomics education. Am J Health Syst Pharm. 2019;76(11):836–845.
10. Shatnawi A, Khanfar NM, Latif DA, Shear M. A comparative study of the depth, breadth, and perception of pharmacogenomics instruction in a subgroup of US pharmacy curricula. Curr Pharm Teach Learn. 2019;11(5):476–484. doi:10.1016/j.cptl.2019.02.010
11. Weitzel KW, Aquilante CL, Johnson S, Kisor DF, Empey PE. Educational strategies to enable expansion of pharmacogenomics-based care. Am J Health Syst Pharm. 2016;73(23):1986–1998. doi:10.2146/ajhp160104
12. Odeh M, Sbitan L, Alzraikat N, Tanous H, Al-Diery T. Precision medicine in pharmacy: assessing pharmacogenomics competence among pharmacists and pharmacy students. J Pharmaceutical Policy Pract. 2024;17(1):2354879. doi:10.1080/20523211.2024.2354879
13. Omran S, Leong SL, Blebil A, Mohan D, Teoh SL. Effectiveness of pharmacogenomics educational interventions on healthcare professionals and health professions students: a systematic review. Res Social Administrative Pharm. 2023;19(11):1399–1411. doi:10.1016/j.sapharm.2023.07.012
14. Soueid R, Michael TJ, Cairns R, Charles KA, Stocker SL. A scoping review of pharmacogenomic educational interventions to improve knowledge and confidence. American J Pharmaceutical Educ. 2024;88(3):100668. doi:10.1016/j.ajpe.2024.100668
15. Alsayed AR, Hasoun L, Al-Dulaimi A, et al. Evaluation of the effectiveness of educational medical informatics tutorial on improving pharmacy students’ knowledge and skills about the clinical problem-solving process. Pharmacy Pract. 2022;20(2):2652. doi:10.18549/PharmPract.2022.2.2652
16. Fino LB, Alsayed AR, Basheti IA, Saini B, Moles R, Chaar BB. Implementing and evaluating a course in professional ethics for an undergraduate pharmacy curriculum: a feasibility study. Curr Pharm Teach Learn. 2022;14(1):88–105. doi:10.1016/j.cptl.2021.11.031
17. Bailey SL, Klejna ER, Capasso S, Kinney SR. Development of a laboratory-based pharmacogenomics independent study and advanced pharmacy practice experience: connecting basic science to clinical application. Curr Pharm Teach Learn. 2021;13(9):1236–1243. doi:10.1016/j.cptl.2021.06.043
18. Krynetskiy E, Calligaro IL. Introducing pharmacy students to pharmacogenomic analysis. American J Pharmaceutical Educ. 2009;73(4):71. doi:10.1016/S0002-9459(24)00566-7
19. Arafah A, Rehman MU, Syed W, Babelghaith SD, Alwhaibi A, Al Arifi MN. Knowledge, attitude and perception of pharmacy students towards pharmacogenomics and genetics: an observational study from King Saud University. Genes. 2022;13(2):269. doi:10.3390/genes13020269
20. Shah S, Hanif M, Khan HU, et al. Knowledge, attitudes and practices of pharmacogenomics among senior pharmacy students: a cross sectional study from Punjab, Pakistan. Pharmacogenomics Personalized Med. 2022;429–439.
21. Marcinak R, Paris M, Kinney SR. Pharmacogenomics education improves pharmacy student perceptions of their abilities and roles in its use. American J Pharmaceutical Educ. 2018;82(9):6424. doi:10.5688/ajpe6424
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.