Back to Journals » Patient Preference and Adherence » Volume 19
Pharmacist-Led Interventions to Improve Medication Adherence Among Patients with Multimorbidity: A Scoping Review
Authors Sholihah S, Rahayu FP ![]() , Farhana L
, Farhana L ![]() , Alshehri S, Alfian SD
, Alshehri S, Alfian SD ![]() , Abdulah R
, Abdulah R
Received 26 May 2025
Accepted for publication 3 November 2025
Published 14 November 2025 Volume 2025:19 Pages 3589—3602
DOI https://doi.org/10.2147/PPA.S542881
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Emma Veale
Shofuro Sholihah,1 Fima Perdani Rahayu,1 Lubna Farhana,1 Sameer Alshehri,2 Sofa Dewi Alfian,1,3 Rizky Abdulah1,3
1Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Sumedang, Indonesia; 2Department of Pharmaceutics and Industrial Pharmacy, College of Pharmacy, Taif University, Taif, Saudi Arabia; 3Center of Excellence for Pharmaceutical Care Innovation, Universitas Padjadjaran, Sumedang, Indonesia
Correspondence: Sofa Dewi Alfian, Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Jl. Raya Jatinangor KM 21, Jatinangor – Sumedang, 45363, Indonesia, Tel/Fax +62 022 7796200, Email [email protected]
Background: Patients with multimorbidity tend to have multiple medications or polypharmacy to achieve optimal outcomes, which may result in non-adherence to medication. Medication non-adherence in this population is relatively higher than in patients with a single disease because of more complex medication regimens and greater adverse drug reactions. Providing interventions is an essential solution in changing patients’ behavior towards medication adherence among patients with multimorbidity. Pharmacists could help patients achieve optimal outcomes by optimizing medication use, including improving medication adherence. This scoping review aims to identify evidence of the effectiveness and characterize pharmacist-led interventions in improving medication adherence among patients with multimorbidity.
Methods: A systematic search was conducted to identify relevant studies on PubMed, Scopus, CENTRAL, and through hand searching. Randomized controlled trial design studies performing interventions to improve medication adherence led by pharmacists among patients living with multimorbidity were included. We focused on original search with the key concepts of “multimorbidity”, “pharmacists”, and “medication adherence”. Narrative synthesis was used to extract and synthesize the data.
Results: Twelve studies that included participants with multimorbidity were reviewed. Nine of all twelve studies showed improvement of medication adherence in the intervention group with a p-value < 0.05, while three other studies indicated no significant difference between the intervention and control groups. All of the studies employed personalized interventions. Interventions used could be divided into counselling sessions, medication management, or using a supporting tool as a reminder of drug administration.
Conclusion: In nine out of twelve studies, interventions led by pharmacists were found to be effective in improving medication adherence in patients with multimorbidity. Effective interventions showed significant improvement in medication adherence in the intervention group compared with the usual care group. These interventions included counselling sessions, medication management, and the use of a supporting tool to remind patients about drug administration.
Keywords: multimorbidity, pharmacists, intervention, medication adherence
Introduction
Multimorbidity is known as the co-existence of two or more chronic illnesses in one person.1 Having multiple conditions is quite common, and such multimorbidity has been rising in prevalence over the years.1 The global prevalence of multimorbidity is 37.2%, with the subgroup study showing that multimorbidity is more prevalent in women (39.4%) than in men (32.8%) and is more common in adult populations above 60 years (51%).2 There are different patterns in multimorbidity, namely concordant and discordant.3 For the concordant clustering pattern, cardiometabolic clustering is a long-reported pattern in the general population.3 Cardiometabolic diseases, such as hypertension, diabetes, and chronic heart disease (CHD), are known as the three most prevalent patterns due to the overlapping etiology, risk factors, and bidirectional interactions.4 A study in the UK showed that the most common diseases among multimorbid patients were hypertension (18.2%) and depression or anxiety (10.3%).5 Another study from Indonesia stated that hypertension is the most common disease (23.2%) in all combinations of multimorbidity.6 Another study also identified that one of the patterns of multimorbidity with high prevalence includes cardiovascular and cardiometabolic disease, where cardiovascular and complex patterns are the leading causes of death.7
Patients with multimorbidity tend to have multiple medications or polypharmacy to achieve optimal outcomes, which can lead to medication non-adherence.8 According to a meta-analysis of individuals with multimorbidity, the prevalence of medication non-adherence was calculated at 42.6%.9 Due to more complicated regimens and greater side effects, individuals with multimorbidity are more susceptible to medication adherence issues than those who have just a single disease due to a greater number of drugs or polypharmacy and more complicated drug regimens, coupled with side effects.10 This condition can lead to medication non-adherence.11 Giving an intervention is an essential solution in changing patients’ behavior towards medication adherence among patients with multimorbidity.12 Pharmacist could help patients achieve optimal outcomes by optimizing medication use, reducing drug-related problems (DRPs), and increasing knowledge, thus improving patients’ quality of life through pharmacist-led interventions.13 Among patients with chronic diseases, pharmacist-led interventions, particularly counseling with behavioral components and tailored strategies, could significantly improve medication adherence in chronic disease,14 where patients with multimorbidity would benefit from personalized care.15 Several types of interventions to improve medication adherence in people with multimorbidity have been carried out before, some of which are self-management, medication review, and electronic health interventions, where interventions with self-management and medication review showed better effectiveness in improving medication adherence among people with multimorbidity.12
A review published prior to 2010 concluded that there was insufficient evidence of successful interventions to improve medication adherence in multiple chronic conditions, and psychosocial therapies were lacking.16 Given the significant advances in treatment and technology over the past five years, an update of the evidence is necessary. Other reviews aimed to select standardized interventions delivered by healthcare professional collaborations to improve medication adherence in people with multimorbidity; however, this study does not indicate whether one intervention is more effective than another.17 Another systematic review among people with multimorbidity was conducted, with most of the included interventions delivered by healthcare professionals other than pharmacists.18,19 One of these studies stated that patients with mental-physical multimorbidity may benefit from interventions that manage and coordinate healthcare processes to improve patients’ medication adherence.18 The other study stated that medication adherence in elderly adults with many comorbidities may be improved by self-management and electronic health treatments.19 The existing interventions to improve medication adherence could be effective, depending on the type of intervention for different conditions of multimorbidity; however, some of them could be less effective as the evidence for effective interventions was weak. This scoping review aims to identify evidence of the effectiveness and characterize pharmacist-led interventions in improving medication adherence among patients with multimorbidity.
Materials and Methods
This review was performed using the Joanna Briggs Institute definition for scoping review.20 The Preferred Reporting Items for Systematic Reviews extension for Scoping Reviews (PRISMA-ScR) guidance was provided as the guide for conducting this scoping review.21 The PRISMA-ScR checklists were available in Supplementary Data 1.
Eligibility Criteria
Original articles produced in the English language from 2011 up to September 2025 were reviewed. Articles will be eligible if they meet all the following inclusion criteria: (1) Randomized controlled trial design studies performing interventions to improve medication adherence led by pharmacists among patients living with multimorbidity; (2) Published in English; (3) Interventions targeting patients with multimorbidity; (4) published between 2011 onwards. Multimorbidity is defined as the coexistence of two or more chronic illnesses in one person.1 Studies involving the use of two or more drugs that might be interpreted as a treatment for two or more long-term illnesses were taken into consideration. Articles will be excluded if: (1) they are qualitative, opinion articles, conference presentations, books, letters, editorials, reviews, dissertations/theses, or abstracts; (2) they do not report medication adherence as a primary or secondary outcome; (3) the population targeted patients aged below 18 years old were also excluded.
Search Strategy
Articles were identified via searches of the electronic databases PubMed, Scopus, CENTRAL, and through hand searching. The PCC Framework (Population, Concept, Context) was used in this search strategy. Population: patients with multimorbidity, who have two or more chronic disease conditions. Concept: Any pharmacist-led intervention with medication adherence included in the outcome. Context: general healthcare settings. We limited our final search strategy to include only articles from 2011 onwards based on the earliest date of relevant articles. The full search strategy can be found in Supplementary Data 2.
Study Selection
The study selection of the articles was performed by two independent reviewers (SS and SDA). One author (SS) assessed the potential eligibility evaluation based on screening after the titles and abstracts. SS obtained and assessed the full texts of publications that might be eligible. The abstract and full-text screening were further independently verified by a second party (SDA). Any disagreements among the reviewers (SS and SDA) were resolved using consensus.
Data Extraction
One reviewer independently conducted the data extraction according to the predefined criteria. The following data from each included article were extracted: data setting and year, sample size and selection criteria, type of disease, adherence measurement, intervention, follow-up and duration, outcome measured, and funding.
Synthesis Method
A narrative synthesis of all reviewed studies was conducted to search for evidence for the effectiveness of pharmacist-led interventions in improving medication adherence among patients with multimorbidity.
Results
Search Results
Records were identified from databases: 1032 from PubMed, 440 from Scopus, 164 from CENTRAL, and 10 through hand searching, including grey literature. After eliminating duplicates, 1223 studies were screened for the title and abstracts according to inclusion and exclusion criteria. Following screening of titles and abstracts, 127 full texts were examined, resulting in 12 studies included in this scoping review. The study selection process is described in the PRISMA-ScR flow diagram in Figure 1.
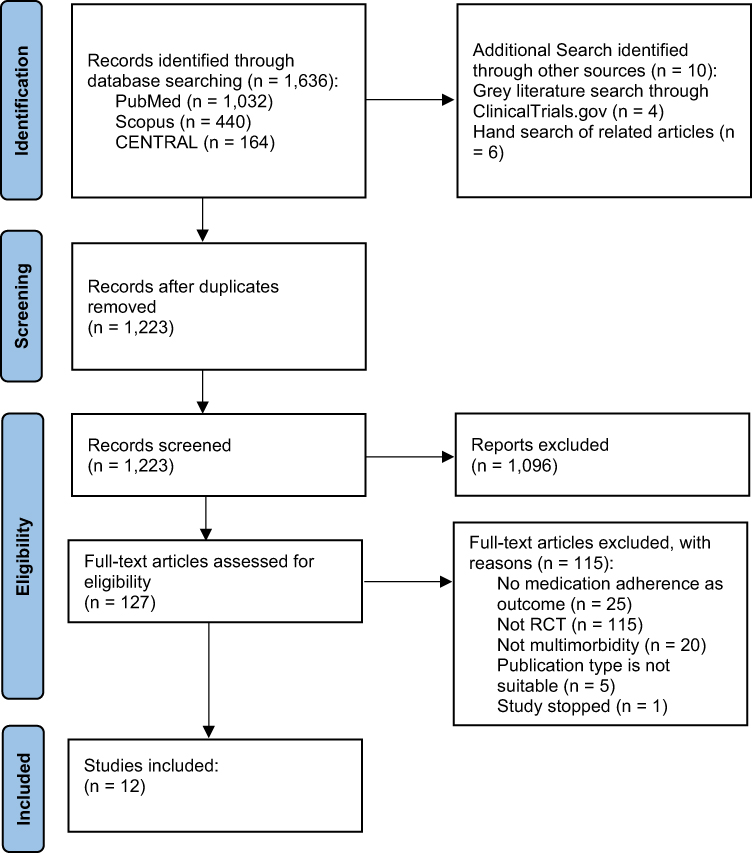 |
Figure 1 PRISMA-ScR flow diagram of the study selection. |
Study Characteristics
All twelve studies that included participants with two or more chronic conditions were reviewed. For the data setting, five studies were performed in Asian regions,22–26 two in Europe,27,28 four in America,29–32 and one in Africa.33 The population included mainly was adults, with eight studies including an adult population at least 18 years old,22–25,27,31–33 three studies included a specific elderly population (at least 65 years or 75 years old)28–30 while one study did not mention the specific population.26
Type of Disease
For the type of chronic conditions, six studies included patients with hypertension and diabetes mellitus,22–24,26,30,31 two studies included patients with hypertension, diabetes mellitus, and dyslipidemia29,32, two studies included patients with chronic kidney disease conditions,25,33 while two other studies only mentioned patients with chronic polypharmacy.27,28
Adherence Measurements
Nine studies use a questionnaire for adherence measurements, some of which were the Medication Adherence Report Scale (MARS-5),23 8-item Morisky Medication Adherence Scale (8-MMAS),22,27,31 Morisky-Green Test (MGT),24 4-item Morisky-Green-Levine (MGL) scale,33 Brief Medication Questionnaire (BMQ),25,26 and the Chilean Medication Adherence Questionnaire.29 Alongside the questionnaire, the study also employed objective methods, including the Medication Possession Ratio (MPR) and the Daily Polypharmacy Possession Ratio (DPPR).27 Two studies used pill counts as a method for adherence measurements.28,32 One study used the group-based trajectory method (GBTM).30
Interventions and Comparators
All of the studies employed personalized interventions. Interventions in ten studies were delivered through face-to-face appointments,22–29,31,33 with two studies also included home visits,22,28 and four studies also included telephone interviews for the follow-up sessions.22,24,27,30 Interventions used could be divided into counselling sessions, medication management, or using a supporting tool as a reminder of drug administration.
- CounsellingCounselling was delivered as educational counselling22–27,29–31,33 and also motivational counselling.23,30 Information provided in educational counselling was information about the disease and its management,26,33 types of drugs used by the patient, usage and dosage, precautions, adverse reactions, clinical targets, and the treatment methods for adverse reactions,24 a possible misconception of the drugs,26 also the purpose of their medications and potential drug-related problems.33
- Medication ManagementMedication management interventions may include medication reviews, following a plan for drug adjustments, as assessed by a pharmacist. In performing a medication review, the pharmacist assessed any potential DRPs and developed an individualized plan for the patients.22,25,27–29,33 The pharmacist also asks for advice from general practitioners for a medication adjustment plan. If necessary, a medication adjustment plan was then created considering the safety, efficacy, and adherence barriers.22
- Supporting ToolInterventions to improve medication adherence also used a supporting tool for drug administration. One of the studies used digital health medication dose reminders. Components of the digital health offering include a wearable sensor (patch), an ingestible sensor pill that can be co-encapsulated with a medication, and a web portal that enables medical staff to access data from the digital health offering.32
Comparators of all studies were usual care applied in each healthcare setting. The usual care mentioned refers to the care that a healthcare provider typically provides to their patients, excluding any intervention.
Effect of Interventions on Medication Adherence
Nine of all twelve studies showed significant improvement of medication adherence in the intervention group with p-value <0.05.22–26,29–32 Three other studies indicated no significant difference between the intervention and control groups in medication adherence.27,28,33
- CounsellingEight out of ten studies included counselling showed an improvement in medication adherence. For the two remaining studies, one had no significant difference in adherence between the two groups due to the unintentional selection of patients with high medication adherence and low levels of experience among recruited pharmacists,27 and the other one due to the absence of more intensive individualized follow-ups.33
- Medication ManagementHalf of the studies included medication management showed an improvement in medication adherence.22,25,29 One study employed a polymedication check, which did not reveal any significant differences.27 Two studies with medication review and therapy management also did not show any significant difference.28,33
- Supporting ToolA study using digital health medicine dose reminders has been shown to enhance medication adherence, particularly in individuals with lower adherence. The study found that the mean overall adherence for all patients was 86 ± 12%, and the mean on-time adherence was 69.7 ± 19.7%.32
Result of Syntheses
Results of syntheses are summarized in Table 1.
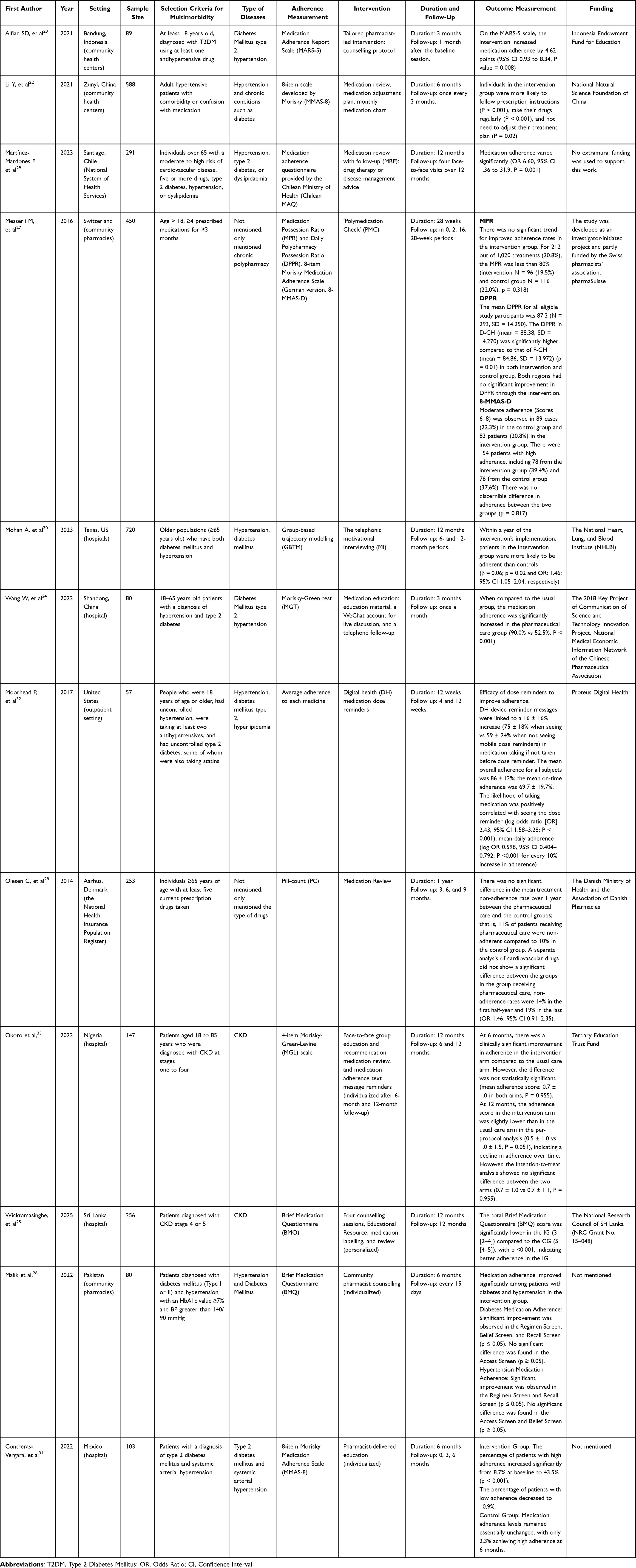 |
Table 1 Data Extraction of the Study |
Discussion
Medication adherence is a vital aspect to achieve optimal clinical results and to prevent disease progression or long-term complications. Improving medication adherence can be achieved by providing targeted interventions, which may be an essential solution in changing patients’ behavior towards medication adherence among those with multimorbidity. This review synthesised data from twelve studies with multimorbidity patients to search for evidence of the effectiveness and to characterize the pharmacist-led interventions in improving medication adherence among patients with multimorbidity. All of the population included were adults, with some studies specifying the elderly population, as chronic conditions were associated with an increased age. In high-income countries such as the European region or the United States, some of them use advanced services, such as standardized terms for interventions, such as Medication Review with Follow-up (MRF), Motivational Interviewing (MI), or Polymedication Check (PMC), which use a more structured method to optimize the use of medication. A previous study stated that in many low- and middle-income countries (LMICs), the capacity and experience to develop continuing professional development (CPD) for pharmaceutical services, such as enhancing patients’ medication adherence, are limited.34 This may be the reason why interventions in high-income countries are more advanced and structured. For the type of the disease, half of the study focused only on type 2 diabetes mellitus and hypertension, as they are included as chronic conditions with the highest rates of noncompliance with medication.35
All the studies performed tailored interventions that assessed the adherence problem before individualizing them. The pharmacist gathered information about patients’ non-adherence behaviors, then established individualized interventions and created an individualized plan based on predictors of lower adherence trajectories. In several studies, the pharmacist also assessed for drug-related problems in each patient as baseline information for medication management.22,27–29 Two studies screened and checked for adherence problems and then provided an adherence protocol to support the pharmacy staff in deciding which intervention could be applied, using the adherence intervention wheel23,27 or polymedication check protocol.27 For the follow-up sessions, the pharmacist evaluated the intervention through a telephone interview, a follow-up consultation, or a messaging mobile app. Previous reviews on patients with cardiovascular diseases showed that tailored interventions are a vital part of improving medication adherence. Tailored interventions involve an integrated process of identifying non-adherent patients, detecting barriers to medication adherence, and providing solutions tailored to those barriers. These interventions are key to delivering tailored interventions to patients’ specific barriers to medication adherence.36 Another previous study also showed that patient-tailored treatment programs in clinical practice can improve adherence by considering individual patients’ characteristics, thereby resolving long-standing non-adherence issues in patients with multimorbidity.37
Interventions to improve medication adherence delivered by pharmacists were significantly more effective than those offered by other healthcare professionals.38 Pharmacists, as healthcare professionals specializing in the use of medication, are well-suited to educate patients about their medications. The patient’s medication types, dose and usage, safety measures, adverse responses, clinical goals, and adverse reaction management techniques were all covered in the educational counseling,24 also the purpose of their medications and potential DRPs.28 Educational counselling in most of the studies provided for their individualized problems, as the pharmacist assessed any gaps in patients’ knowledge and then delivered educational consultation or clarified any misconceptions. Individualized educational counselling could also be provided only for those who needed it (eg, patients who had risk behaviors).22 Easy-to-understand texts, comics, music, videos, and other popular science works could be used as educational resources to give personalized medicine advice.24
Pharmacist-led interventions used in these articles could be divided into counselling sessions, medication management, or using a supporting tool as a reminder of drug administration. In counselling sessions, the pharmacist provided educational counselling and/or motivational counselling to each patient about the use of their medication. In educational counselling, pharmacists provided individualized education plans to address risk behaviors and improve patients’ knowledge about the diseases and medication adherence.22 One study provided educational counselling along with other strategies like integrating medication routines into daily activities to address issues about forgetfulness and lack of knowledge, as they were the most common barriers identified.23 Other than educational counselling, some of the studies also provided motivational counselling. Motivational counselling was used to identify and address adherence barriers such as lack of motivation, concerns about side effects, and misconceptions about the necessity of antihypertensive drugs.23 Pharmacist counselling enhanced treatment awareness and dispelled misconceptions, leading to better adherence.25 Previous meta-analysis about the association of pharmacist intervention counselling with medication adherence also reported that pharmacist educational counselling significantly increases medication adherence compared to no counseling.39
Other than counselling sessions, other studies also used medication management as an intervention. Medication review, as one component of medication management, is often used in these articles to improve adherence. A medication review is defined as an evaluation of a patient’s medications to optimize medication use and improve health outcomes, involving the detection of drug-related problems and the recommendation of interventions.27 Two studies22,29 used medication review as the primary intervention, followed by individualized educational counselling if needed. The results showed that there was a significant improvement in medication adherence. One study also reported that participants in the intervention group did not need to modify their treatment regimen (P < 0.001).22 Other three studies that used medication management showed no significant difference in the intervention group. One study28 used only medication review as an intervention, showed that the adherence rate was high in both intervention and control groups, and there was no significant difference in treatment non-adherence between the pharmaceutical care group and the control group. However, this study did not measure baseline treatment adherence, as adherence rates were considered equal in both groups due to the randomization method. Other than that, this study used pill counts as an adherence measurement tool and had a 6-month follow-up period, which can introduce bias to the results. Patients might have purchased new pill boxes that were not displayed to the pill-counting nurse just before the 6-month appointment, or they might not have informed the nurse of a change in the practitioner’s prescribed dosages. In another study, pharmacists reviewed all medicines currently used by the patient and provided a structured face-to-face counselling session, showing that there was no significant trend for improved adherence rates in the intervention group. This study identifies several probable reasons for the lack of a substantial difference in medication adherence between the intervention and control groups, including high baseline adherence, selection bias resulting in the unintentional selection of patients who were already well-organized and had established therapies, motivational bias, and a short study duration. The other study, which included both medication review and pharmacist counseling, suggests that the lack of a significant difference in medication adherence between the intervention and control groups may be due to the absence of sustained, intensive, and individualized follow-ups for the intervention group. None of these three studies mentioned that the probable reason for the lack of a significant difference is the method used for the intervention.
Lastly, only one study used a reminder tool for the intervention group. This study found that digital health medication dose reminders offer benefits in improving medication adherence, particularly for patients with lower adherence.32
Strengths and Limitations
This is the first review to search for evidence of the effectiveness and to characterize the pharmacist-led interventions in improving medication adherence among patients with multimorbidity, to the best of the authors’ knowledge. Nevertheless, this scoping review has several limitations. First, it is possible that not all studies on interventions intended to enhance medication adherence among patients with multimorbidity were located during searches of research papers, because of the difficulty in identifying the term multimorbidity in research papers. For example, several studies only used the term chronic illnesses included in the survey, but did not use the terms multimorbidity or comorbidity. Second, interventions to improve medication adherence in this population are frequently combined, which may have a potential for overlap in classification. Third, no critical appraisal of the included studies was conducted, consistent with the methodological framework of scoping reviews. As a result, the strength and quality of the evidence could not be evaluated, and the findings should be interpreted with caution. Fourth, the review was limited to studies published from 2011 onwards, which may have excluded earlier research that could provide additional insights into the topic. Finally, the synthesis was descriptive in nature, focusing on mapping and summarizing the existing literature on pharmacist-led interventions to improve medication adherence, without conducting a quantitative analysis. This approach limits the ability to conclude the magnitude or direction of effects across studies. In future studies, the use of quantitative approaches, such as meta-analysis, should be considered to allow for a more rigorous synthesis of the evidence. This would enable researchers to draw stronger conclusions about the magnitude and direction of effects across pharmacist-led interventions aimed at improving medication adherence studies, providing clearer insights into the effectiveness and impact of interventions in this area.
Implications for Research and Practice
This scoping review identified that the studies were most likely performed on individualized interventions based on the individual’s behavior or medication problems. In nine out of twelve studies, it was found that interventions led by pharmacists are most likely effective in improving medication adherence among patients with multimorbidity. Nevertheless, several studies did not consider patients’ baseline adherence levels, resulting in no significant improvement in adherence being reported. Future studies should evaluate the adherence baseline and choose specific study populations who may benefit from a medication adherence improvement intervention program. There are also several implications in practice, especially in clinical pharmacist practice. Current health facilities primarily focus on patients with single diseases and do not adequately consider those with more complex conditions, such as multimorbidity. This review can serve as a valuable resource for pharmacists in developing effective intervention programs to enhance medication adherence in this population. Pharmacists, being specialists in pharmaceuticals, are ideally positioned to help patients understand the necessity and rationale behind drug administration. Pharmacist educational counseling may enhance patients’ comprehension of the necessity and rationale for medication adherence. In the context of medication management, a pharmacist could provide a medication review to assess patients’ drug-related problems and provide a supporting tool to help patients adhere to their medications.
Conclusion
In nine out of twelve studies, interventions led by pharmacists were found to be effective in improving medication adherence in patients with multimorbidity. These interventions included counselling sessions, medication management, and the use of a supporting tool to remind patients about drug administration. Effective interventions showed significant improvement in medication adherence in the intervention group compared with the usual care group. However, their impact remains variable due to differences in the type of pharmacist-led intervention. In future studies, the use of quantitative approaches, such as meta-analysis, should be considered to allow for a more rigorous synthesis of the evidence.
Acknowledgments
The authors would like to express their gratitude to Universitas Padjadjaran for supporting this research. Special thanks to our mentors for their valuable insights and guidance throughout the research process.
Funding
This research is funded by the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science and Technology and managed under the EQUITY Program (Contract No. 4303/B3/DT.03.08/2025 and 3927/UN6.RKT/HK.07.00/2025).
Disclosure
All authors report no conflicts of interest in this study.
References
1. WHO. Multimorbidity. World Health Organization; 2016.
2. Chowdhury SR, Chandra Das D, Sunna TC, Beyene J, Hossain A. Global and regional prevalence of multimorbidity in the adult population in community settings: a systematic review and meta-analysis. EClinicalMedicine. 2023;57. doi:10.1016/j.eclinm.2023.101860
3. Asogwa OA, Quansah DY, Boakye D, Ezewuiro ON, Boateng D. Prevalence, patterns, and determinants of multimorbidity among childhood and adult cancer survivors: a systematic review. Crit Rev Oncol Hematol. 2023;192. doi:10.1016/j.critrevonc.2023.104147
4. Cheng X, Ma T, Ouyang F, Zhang G, Bai Y. Trends in the prevalence of cardiometabolic multimorbidity in the United States, 1999–2018. Int J Environ Res Public Health. 2022;19(8). doi:10.3390/ijerph19084726
5. Cassell A, Edwards D, Harshfield A, et al. The epidemiology of multimorbidity in primary care: a retrospective cohort study. Br J Gen Pract. 2018;68(669):e245–e251. doi:10.3399/bjgp18X695465
6. Griselda M, Alfian SD, Wicaksono IA, Wawruch M, Abdulah R. Findings from the Indonesian family life survey on patterns and factors associated with multimorbidity. Sci Rep. 2023;13(1). doi:10.1038/s41598-023-42603-2
7. Alvarez-Galvez J, Ortega-Martin E, Ramos-Fiol B, Suarez-Lledo V, Carretero-Bravo J. Epidemiology, mortality, and health service use of local-level multimorbidity patterns in South Spain. Nat Commun. 2023;14(1). doi:10.1038/s41467-023-43569-5
8. González-Bueno J, Sevilla-Sánchez D, Puigoriol-Juvanteny E, Molist-Brunet N, Codina-Jané C, Espaulella-Panicot J. Improving medication adherence and effective prescribing through a patient-centered prescription model in patients with multimorbidity. Eur J Clin Pharmacol. 2022;78(1):127–137. doi:10.1007/s00228-021-03207-9
9. Foley L, Larkin J, Lombard-Vance R, Murphy AW, Molloy GJ. Prevalence and predictors of medication non-adherence among patients with multimorbidity: a systematic review protocol. HRB Open Res. 2019;2:29. doi:10.12688/hrbopenres.12961.1
10. Lee E, Choi MK. Factors associated with medication adherence among older adults with multimorbidity: a culture perspective. Geriatr Nurs. 2024;55:297–303. doi:10.1016/j.gerinurse.2023.11.018
11. González-Bueno J, Sevilla-Sánchez D, Puigoriol-Juvanteny E, Molist-Brunet N, Codina-Jané C, Espaulella-Panicot J. Factors associated with medication non-adherence among patients with multimorbidity and polypharmacy admitted to an intermediate care center. Int J Environ Res Public Health. 2021;18(18):9606. doi:10.3390/ijerph18189606
12. Yang C, Lee DTF, Wang X, Chair SY. Effects of a nurse-led medication self-management intervention on medication adherence and health outcomes in older people with multimorbidity: a randomised controlled trial. Int J Nurs Stud. 2022;134. doi:10.1016/j.ijnurstu.2022.104314
13. Eldooma I, Maatoug M, Yousif M. Outcomes of pharmacist-led pharmaceutical care interventions within community pharmacies: narrative review. Integr Pharm Res Pract. 2023;12:113–126. doi:10.2147/iprp.s408340
14. Farhana L, Rahayu FP, Sholihah S, Sweileh W, Abdulah R, Alfian SD. Effectiveness of pharmacist-led intervention on medication adherence in chronic diseases: a systematic review of randomized controlled trials. Patient Prefer Adherence. 2025;19:2161–2178. doi:10.2147/PPA.S530503
15. Co W, Feng L, Smith-Ray R, et al. Author affiliation pharmacists as clinical care partners: how a pharmacist-led intervention is associated with improved medication adherence in older adults with common chronic conditions. J Manage Care Specialty Pharm. 2024;30.
16. Williams A, Manias E, Walker R. Interventions to improve medication adherence in people with multiple chronic conditions: a systematic review. J Adv Nurs. 2008;63(2):132–143. doi:10.1111/j.1365-2648.2008.04656.x
17. González-Bueno J, Calvo-Cidoncha E, Nieto-Martín MD, Pérez-Guerrero C, Ollero-Baturone M, Santos-Ramos B. Selection of interventions aimed at improving medication adherence in patients with multimorbidity. Eur J Hosp Pharm. 2019;26(1):39–45. doi:10.1136/ejhpharm-2017-001240
18. Lammila-Escalera E, Greenfield G, Pan Z, Nicholls D, Majeed A, Hayhoe B. Interventions to improve medication adherence in adults with mental–physical multimorbidity in primary care: a systematic review. Br J Gen Pract. 2024;74(744):e442–e448. doi:10.3399/BJGP.2023.0406
19. Yang C, Zhu S, Lee DTF, Chair SY. Interventions for improving medication adherence in community-dwelling older people with multimorbidity: a systematic review and meta-analysis. Int J Nurs Stud. 2022;126. doi:10.1016/j.ijnurstu.2021.104154
20. Aromataris E, Lockwood C, Porritt K, Pilla B, Jordan Z, editors.. JBI Manual for Evidence Synthesis. JBI; 2024.
21. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
22. Li Y, Liu G, Liu C, et al. Effects of pharmacist intervention on community control of hypertension: a randomized controlled Trial in Zunyi, China. Glob Health Sci Pract. 2021;9(4):890–904. doi:10.9745/GHSP-D-20-00505
23. Alfian SD, van Boven JFM, Abdulah R, Sukandar H, Denig P, Hak E. Effectiveness of a targeted and tailored pharmacist-led intervention to improve adherence to antihypertensive drugs among patients with type 2 diabetes in Indonesia: a cluster randomised controlled trial. Br J Clin Pharmacol. 2021;87(4):2032–2042. doi:10.1111/bcp.14610
24. Wang W, Geng L, Sun C, Li H, Wang J. Efficacy of pharmaceutical care in patients with type 2 diabetes mellitus and hypertension: a randomized controlled trial. Int J Clin Pract. 2022;2022:7681404. doi:10.1155/2022/7681404
25. Wickramasinghe D, Lynch C, Coombes J, Jayamanne S, Silva SD. Impact of clinical pharmacy services on medication adherence and quality of life in pre-dialysis patients with CKDu: a randomized controlled trial from Sri Lanka. BMC Nephrol. 2025;26(1). doi:10.1186/s12882-025-04301-1
26. Malik M, Hussain A, Aslam U, et al. Effectiveness of community pharmacy diabetes and hypertension care program: an unexplored opportunity for community pharmacists in Pakistan. Front Pharmacol. 2022:13. doi:10.3389/fphar.2022.710617
27. Messerli M, Blozik E, Vriends N, Hersberger KE. Impact of a community pharmacist-led medication review on medicines use in patients on polypharmacy--a prospective randomised controlled trial. BMC Health Serv Res. 2016;16:145. doi:10.1186/s12913-016-1384-8
28. Olesen C, Harbig P, Buus KM, Barat I, Damsgaard EM. Impact of pharmaceutical care on adherence, hospitalisations and mortality in elderly patients. Int J Clin Pharm. 2014;36(1):163–171. doi:10.1007/s11096-013-9898-1
29. Martínez-Mardones F, Benrimoj SI, Ahumada-Canale A, Plaza-Plaza JC, Garcia-Cardenas V. BC clinical impact of medication reviews with follow-up in cardiovascular older patients in primary care: a cluster-randomized controlled trial. Br J Clin Pharmacol. 2023;89(7):2131–2143. doi:10.1111/bcp.15682
30. Mohan A, Majd Z, Johnson ML, et al. A motivational interviewing intervention to improve adherence to ACEIs/ARBs among nonadherent older adults with comorbid hypertension and diabetes. Drugs Aging. 2023;40(4):377–390. doi:10.1007/s40266-023-01008-6
31. Contreras-Vergara A, Sifuentes-Franco S, Haack S, et al. Impact of pharmaceutical education on medication adherence and its clinical efficacy in patients with type 2 diabetes and systemic arterial hypertension. Patient Prefer Adherence. 2022;16:1999–2007. doi:10.2147/PPA.S370323
32. Moorhead P, Zavala A, Kim Y, Virdi NS. Efficacy and safety of a medication dose reminder feature in a digital health offering with the use of sensor-enabled medicines. J Am Pharm Assoc. 2017;57(2):155–161.e1. doi:10.1016/j.japh.2016.12.067
33. Okoro RN, Umate I, Ohieku JD, Yakubu SI, Adibe MO. The impact of pharmacist-led interventions on blood pressure control among patients with chronic kidney disease: a randomized controlled trial. JACCP. 2022;5(10):1062–1074. doi:10.1002/jac5.1677
34. Babar ZUD. Ten recommendations to improve pharmacy practice in low and middle-income countries (LMICs). J Pharm Policy Pract. 2021;14(1). doi:10.1186/s40545-020-00288-2
35. Alosaimi K, Alwafi H, Alhindi Y, et al. Medication adherence among patients with chronic diseases in Saudi Arabia. Int J Environ Res Public Health. 2022;19(16):10053. doi:10.3390/ijerph191610053
36. Xu HY, Yu YJ, Zhang QH, Hu HY, Li M. Tailored interventions to improve medication adherence for cardiovascular diseases. Front Pharmacol. 2020;11. doi:10.3389/fphar.2020.510339
37. Pradipta IS, Aprilio K, Ningsih YF, Pratama MAA, Alfian SD, Abdulah R. Treatment nonadherence among multimorbid chronic disease patients: evidence from 3515 subjects in Indonesia. Medicina. 2024;60(4). doi:10.3390/medicina60040634
38. Conn VS, Ruppar TM. Medication adherence outcomes of 771 intervention trials: systematic review and meta-analysis. Prev Med. 2017;99:269–276. doi:10.1016/j.ypmed.2017.03.008
39. Kelly WN, Ho MJ, Smith T, Bullers K, Kumar A. Association of pharmacist intervention counseling with medication adherence and quality of life: a systematic review and meta-analysis of randomized trials. J Am Pharm Assoc. 2023;63(4):1095–1105. doi:10.1016/j.japh.2023.04.024
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.