Back to Journals » Infection and Drug Resistance » Volume 19
Pharmacist-Led Full-Course Pharmaceutical Care Model in Allergic Bronchopulmonary Aspergillosis: A Case Report-Based Approach to Optimizing Multidisciplinary Management
Authors Huang X, Zheng Y, Jin X, Zheng Q, Pan K
Received 17 September 2025
Accepted for publication 11 January 2026
Published 20 January 2026 Volume 2026:19 565067
DOI https://doi.org/10.2147/IDR.S565067
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Oliver Planz
Xi Huang,1,2 Yuhong Zheng,1 Xiaoli Jin,3 Qingxiu Zheng,4 Kunlei Pan4
1Department of Pharmacy, Wenzhou TCM Hospital of Zhejiang Chinese Medical University, Wenzhou, 325000, People’s Republic of China; 2Department of TCM Science and Research Center, Wenzhou TCM Hospital of Zhejiang Chinese Medical University, Wenzhou, 325000, People’s Republic of China; 3Department of Laboratory Medicine, Wenzhou TCM Hospital of Zhejiang Chinese Medical University, Wenzhou, 325000, People’s Republic of China; 4Department of Respiratory and Critical Care Medicine, Wenzhou TCM Hospital of Zhejiang Chinese Medical University, Wenzhou, 325000, People’s Republic of China
Correspondence: Kunlei Pan, Department of Respiratory and Critical Care Medicine, Wenzhou TCM Hospital of Zhejiang Chinese Medical University, Wenzhou, 325000, People’s Republic of China, Email [email protected]
Introduction: The management of allergic bronchopulmonary aspergillosis (ABPA) is complicated by prolonged, multi-drug regimens that carry a high risk of multi-system adverse drug reactions (ADRs). This complexity underscores the need for integrated, continuous pharmaceutical care to optimize safety and efficacy, yet standardized models for such care are lacking.
Case Presentation: We report the case of a patient with ABPA and comorbid chronic hepatitis B, who had a history of failed ABPA therapy. During the current therapeutic course, the patient not only sequentially developed steroid-induced diabetes, drug-induced liver injury, hyperlactatemia, visual disturbances, phototoxicity, and hypokalemia but also progressed to treatment-dependent ABPA. The patient successfully completed the over-two-year protocol through a pharmacist-led full-course pharmaceutical care model that integrated regimen evaluation, efficacy monitoring, comprehensive adverse reaction management, discharge education, and follow-up.
Conclusion: This case demonstrates that a full-course pharmaceutical care model enables timely detection and management of complex ADRs, optimizes therapeutic outcomes, and supports multidisciplinary decision-making. The model illustrates the pivotal role of the clinical pharmacist in improving medication safety and efficacy in ABPA, offering a replicable framework for promoting integrated, patient-centered care in pulmonary fungal diseases.
Keywords: full-course pharmaceutical care, work model, allergic bronchopulmonary aspergillosis, clinical pharmacist, case report
Introduction
Allergic bronchopulmonary aspergillosis (ABPA) is a complex allergic disease caused by an immune response to Aspergillus fumigatus (A. fumigatus).1 ABPA involves a hypersensitivity response that encompasses both an A. fumigatus-specific IgE-mediated type I reaction and an IgG-mediated type III reaction.2 The global prevalence of ABPA in adults with asthma is estimated at 2.5%.3 Due to atypical clinical symptoms and the need for specialized immunological and microbiological tests, ABPA is often misdiagnosed, diagnosed late, or treated improperly, leading to irreversible bronchopulmonary damage.2 Given the atypical presentations, prolonged multi-drug therapies, and high risk of multi-system adverse drug reactions (ADRs) in ABPA, there is a critical need for full-course pharmaceutical care. This model is defined as a comprehensive, medication-related service that spans the entire healthcare process, aiming to improve patient quality of life.4 This report details the clinical course of a patient with ABPA and chronic hepatitis B (CHB) who, amidst a two-year therapeutic course, developed multi-system ADRs and progressed to treatment-dependent ABPA. It outlines the pharmacist-led, full-course interventions that successfully navigated these challenges. The study aims to provide a practical framework for optimizing the management of such complex cases and for advancing the role of clinical pharmacists within multidisciplinary teams.
Case Presentation
A 42-year-old male weighing 78 kg was diagnosed with bronchial asthma over a decade ago. Three months prior, the patient experienced worsening dyspnea, especially after activity, accompanied by increased white frothy sputum. A chest CT showed bronchiectasis with infection. The diagnosis was ABPA. The patient was initially treated with voriconazole (VCZ) 200 mg twice daily but discontinued due to elevated liver enzymes. Two weeks before admission, the patient’s dyspnea worsened, occurring even with mild activity and slightly relieved at rest. He was admitted on September 29, 2022. He had a history of hypertension for over two years, regularly taking levamlodipine besylate 2.5 mg daily, and CHB. On admission, vital signs were stable, and physical examination revealed coarse breath sounds without rales. Laboratory tests showed Aspergillus-specific IgG >500 AU/mL (June 21, 2022), eosinophil count was 4.96×109/L (September 29, 2022), IgE >2500 IU/mL (September 30, 2022), Aspergillus-specific IgE 26.6 AU/mL (October 1, 2022), and sputum culture positive for A. fumigatus (October 11, 2022). The diagnosis included: ① ABPA; ② CHB; ③ Grade 1 hypertension (high risk); ④ Fatty liver; ⑤ Gallstones; ⑥ Prostatic calcification.
The treatment plan included glucocorticoids to suppress the allergic response to Aspergillus and antifungal drugs to clear airway colonization, preventing irreversible bronchial and lung damage. Given the patient’s history of CHB and fatty liver, and previous drug-induced liver injury, the clinical pharmacist recommended methylprednisolone, which does not require hepatic metabolism, at an equivalent dose of 0.4 mg/kg. The physician adopted this recommendation, and the patient was started on methylprednisolone 16 mg twice daily on September 29, 2022. Following a prior episode of self-discontinued VCZ due to elevated liver enzymes, which occurred without TDM or clinical pharmacist input, a maintenance dose of 200 mg q12h was therefore started on September 29, 2022. TDM for VCZ was recommended seven days after starting treatment by the clinical pharmacist, with a target trough concentration of 0.5–5 mg/L. On October 12, 2022, the patient’s VCZ trough concentration was 3.6 mg/L, which was within the therapeutic range and correlated with clinical improvement in the patient’s respiratory distress. On September 30, 2022, quantitative hepatitis B serology showed only positive HBeAg and HBcAb, with HBV-DNA below the lower limit of detection. Given the patient’s history of CHB and the need for long-term glucocorticoid therapy, the hepatology department recommended entecavir 0.5 mg once daily to prevent HBV reactivation, with regular monitoring of liver function, HBV serology, and HBV-DNA every 3–6 months. The clinical pharmacist concurred with this recommendation and assumed responsibility for monitoring medication safety.
The clinical pharmacist monitored blood glucose, blood pressure, and weight to assess and manage glucocorticoid-related complications. On September 30, 2022, HbA1c was 6.1%, and preprandial blood glucose levels were elevated, consistent with steroid-induced diabetes. As methylprednisolone therapy could not be discontinued, glycemic control was achieved through a series of regimen adjustments: initial management with metformin, followed by miglitol, and ultimately a combination of insulin glargine and insulin aspart. This sequential therapy successfully maintained FBG at 4–7 mmol/L and PBG at 5–10 mmol/L. Blood pressure was controlled with levamlodipine 2.5 mg daily, ranging from 120/80 to 140/90 mmHg.
In view of the patient’s history of self-discontinuing VCZ due to elevated transaminases, the clinical pharmacist closely monitored liver function throughout the subsequent treatment course. On October 25, 2022, the patient developed elevated ALT (136 U/L) after 27 days of VCZ therapy, consistent with drug-induced liver injury. The VCZ trough concentration was 2.18 µg/mL. The patient was treated with reduced glutathione and compound glycyrrhizin tablets, leading to significant improvement in liver function, with normalization achieved by November 23, 2022.
The patient developed steroid-induced diabetes and was started on metformin 500 mg twice daily on October 3, 2022. On October 6, 2022, entecavir 0.5 mg nightly was initiated for CHB. Against the background of the patient’s impaired liver function, and in light of the additional risk posed by the concomitant use of metformin and entecavir, the clinical pharmacist closely monitored lactate levels. On October 25, 2022, the patient’s laboratory results showed a lactate level of 3.75 mmol/L and a pH of 7.43, meeting the diagnostic criteria for hyperlactatemia. On the premise that all nucleoside analogs (NAs) can precipitate hyperlactatemia, and considering the substitutable nature of metformin, a switch to miglitol was recommended. However, after metformin cessation, the patient’s lactate levels continued to rise. The clinical pharmacist accordingly advised the discontinuation of entecavir along with fluid resuscitation. The physician endorsed this recommendation. Following the cessation of entecavir on November 3, 2022, the lactate level decreased to 1.81 mmol/L by November 15, 2022.
On November 1, 2022, the patient reported blurred vision after 33 days of VCZ therapy. On November 4, 2022, the VCZ trough concentration was 2.18 µg/mL. The clinical pharmacist attributed the visual disturbance to VCZ. Without any intervention, the patient experienced spontaneous resolution or improvement after close observation.
Later, on January 11, 2023, gray-black pigmentation developed in sun-exposed areas after 43 days of VCZ therapy. Recognizing this as VCZ-associated phototoxicity, the clinical pharmacist advised proactive sun protection measures, such as regular sunscreen use, wearing hats, and avoiding direct sunlight, to mitigate progression. Skin pigmentation gradually improved after VCZ discontinuation.
To address this VCZ-induced liver dysfunction, treatment with compound glycyrrhizin tablets was initiated on October 25, 2022. The clinical pharmacist proactively monitored electrolyte levels, particularly potassium, in light of the known hypokalemia risks associated with VCZ, methylprednisolone, and compound glycyrrhizin. On February 7, 2023, monitoring revealed significant hypokalemia (potassium 2.86 mmol/L). In response, the clinical pharmacist recommended a dual strategy: substituting compound glycyrrhizin with bicyclol and initiating potassium supplementation. Following the implementation of these recommendations, serum potassium levels stabilized and were maintained at approximately 3.5 mmol/L thereafter.
The clinical pharmacist provided comprehensive discharge education and, jointly with the physician, executed a structured follow-up plan that included monitoring of symptoms, serum IgE, and imaging findings. Subsequently, the pharmacist meticulously documented the ensuing clinical evolution and treatment response. The patient completed a six-month course of VCZ and stopped on April 14, 2023. While on methylprednisolone 8 mg daily, IgE decreased to 539 IU/mL by April 14, 2023. During the first tapering of steroid, IgE levels gradually increased, rising to 722 IU/mL on May 11, 2023, and further to 1775 IU/mL on June 5, 2023. Similarly, during the second tapering of steroid, IgE levels continued to rise, increasing to 1260 IU/mL on February 28, 2024, and 1649 IU/mL on March 28, 2024. Each of the two attempts to reduce the dose of methylprednisolone was accompanied by an approximately 50% rise in serum total IgE over 4 weeks. Based on this clinical course consistent with treatment-dependent ABPA, the clinical pharmacist recommended omalizumab 375 mg subcutaneously every two weeks, which was approved by the physician. Notably, the serum total IgE level decreased by more than 50% within the first month of omalizumab therapy, and no drug-related adverse effects were observed during the treatment course.
Discussion
A. fumigatus is a thermotolerant fungus that can grow in both environmental and body temperatures. Adults inhale approximately 100 A. fumigatus conidia daily, which are about 2.5 µm in diameter and immunologically inert, allowing them to bypass upper respiratory defenses and reach the alveoli, where they germinate into hyphae and become trapped in bronchial mucus plugs.5 The pathogenesis of ABPA remains unclear, but host genetic susceptibility is considered a major factor, with polymorphisms in innate immune response pathways detected in ABPA patients.6 Studies have shown that surfactant protein A2 (SPA2), Toll-like receptors (TLRs) 4 and 9, and HLA-DR2 and DR5 genotypes alter susceptibility to ABPA.7–9 The shedding of A. fumigatus conidia produces β-D-glucan, galactomannan, fungal nucleic acids, and proteases, which stimulate type 2 innate lymphoid cells (ILC2s) to secrete large amounts of type 2 cytokines, promoting adaptive immune responses.10 The persistent presence of A. fumigatus in the airways and the combined innate and adaptive immune responses lead to airway inflammation dominated by eosinophils, airway hyperresponsiveness, elevated IgE, and mucus production in patients with ABPA. The radiographic manifestations of ABPA may present with a range of findings, from transient, recurrent, and migratory pulmonary infiltrates to permanent architectural damage.2 The clinical presentation of ABPA is often atypical, including poorly controlled asthma, fever, hemoptysis, fatigue, or even an absence of symptoms. This can easily be masked by the underlying primary disease. A comprehensive understanding of the pathogenesis, imaging features, clinical manifestations, diagnostic criteria, and main pathogens of ABPA forms the essential knowledge base that enables the clinical pharmacist to actively participate in evaluating and optimizing treatment strategies, as demonstrated in the management of the present case. Building upon this fundamental understanding of the disease pathogenesis, the core objectives of clinical management are to effectively control the immune-inflammatory response and eradicate fungal colonization in the airways.
Oral glucocorticoids are the cornerstone of ABPA treatment. Early use can effectively suppress Aspergillus-induced inflammation, preventing or reducing bronchiectasis and pulmonary fibrosis. The expert consensus recommends prednisone at an initial dose of 0.5 mg/kg once daily for two weeks, followed by gradual tapering.2 A randomised trial of glucocorticoids in acute-stage ABPA complicating asthma demonstrated the efficacy and safety of moderate-dose methylprednisolone.11 However, their use necessitates careful risk mitigation in patients with comorbidities such as CHB, the most significant comorbidity influencing pharmacotherapy decisions in this case. Glucocorticoids are immunosuppressive and can cause HBV reactivation, which may progress to liver failure. Anti-HBs levels are associated with HBV reactivation risk, with a 14% risk in anti-HBs-positive patients.12
ABPA is a hypersensitivity reaction to A. fumigatus, rarely caused by other fungi. A. fumigatus is a ubiquitous environmental pathogen whose small spores can reach the alveoli and persist in the airways through hyphal growth, contributing to chronic disease.13 While glucocorticoids can rapidly alleviate symptoms, they do not inhibit A. fumigatus growth or reduce allergen load. Antifungal drugs can reduce fungal burden, decreasing ongoing inflammation from Aspergillus antigens. Combined antifungal therapy can reduce glucocorticoid use, with a lower acute exacerbation rate within one year compared to glucocorticoid monotherapy.14 ABPA responds to triazole antifungals, with approximately 60% of patients responding to itraconazole (ITZ) and 80% to VCZ and posaconazole.15 ITZ is available in capsule and oral solution forms, with the oral solution having higher bioavailability. ITZ has nonlinear pharmacokinetics and significant interindividual variability, requiring therapeutic drug monitoring (TDM). The intraclass analysis of correlation between different triazoles and DILI showed the following ranking: itraconazole (5.06; 4.58–5.60) > VCZ (4.58; 4.29–4.90) > posaconazole (3.99; 3.47–4.59) > fluconazole (3.19; 2.93–3.47) > ketoconazole (2.28; 1.96–2.64).16 VCZ and systemic glucocorticoids are equally effective in achieving short-term remission and preventing ABPA exacerbations.17 Newer azoles (posaconazole, isavuconazole) have also been evaluated for ABPA but are typically reserved for patients unresponsive or intolerant to ITZ due to higher costs.18,19 Due to supply instability and lack of TDM for ITZ at our hospital, VCZ was used as an alternative. When administering a loading dose, monitoring of VCZ trough concentrations should be performed, with the first blood sample drawn no earlier than before the fifth dose.20 Without a loading dose, VCZ reaches steady-state levels within 4–7 days.20
Once the combined therapeutic strategy of glucocorticoids and antifungal agents was established, the key to ensuring its safe and effective execution lay in anticipating and managing the attendant risk of multi-system ADRs. Drawing on a profound understanding of the adverse reaction spectrum, its mechanisms, and the patient’s individual risk factors, the clinical pharmacist identified the core monitoring aspects for ABPA treatment. As outlined in Table 1, the clinical pharmacist provided proactive monitoring and counseling, explaining the rationale for surveillance and reassuring patients that most adverse effects are manageable. Through this proactive approach and encouraging active reporting by patients, treatment regimens can be promptly adjusted to reduce self-discontinuation of medication due to adverse reactions, thereby improving clinical efficacy and medication adherence. Over a two-year therapeutic course, the patient sequentially developed steroid-induced diabetes, drug-induced liver injury, hyperlactatemia, visual disturbances, phototoxicity, and hypokalemia.
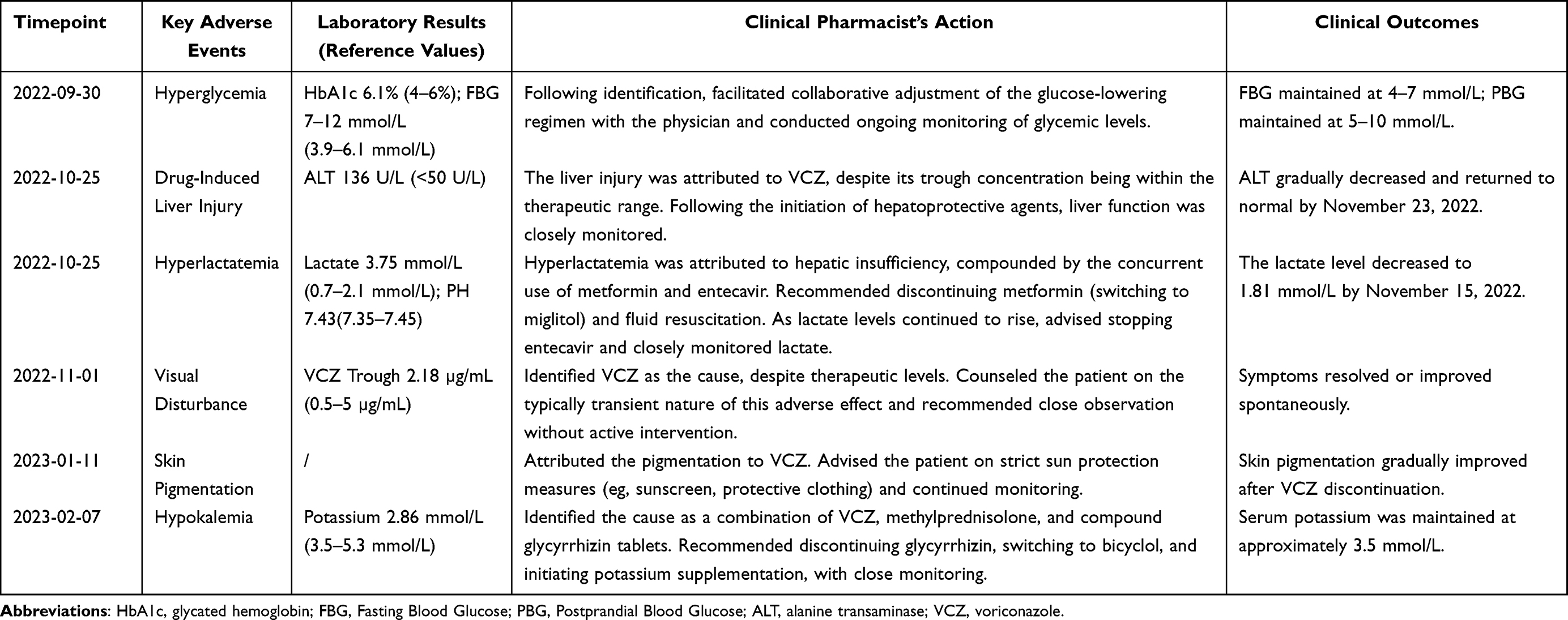 |
Table 1 Timeline of Key Adverse Events and Pharmacist Interventions |
Asians have a higher prevalence of CYP2C19 poor metabolism and are more susceptible to VCZ-induced hepatotoxicity. The incidence of VCZ-related liver injury is 8.3%, with a median onset of 11 days (range 4–28 days), predominantly presenting as elevated ALT.21 Most cases are mild to moderate, and liver function typically normalizes with continued VCZ and hepatoprotective therapy.21 The VCZ individualized medication guideline20 indicates that VCZ trough concentrations are significantly associated with hepatotoxicity, with lower rates in Asians with trough concentrations <5 mg/L. However, real-world studies show that even with TDM-guided dosing, hepatotoxicity rates remain relatively high, suggesting that VCZ-induced liver injury may be idiosyncratic.22 The mechanism of VCZ-induced liver injury is associated with oxidative stress, leading to cellular dysfunction and subsequent disturbances in energy metabolism, urea cycle, and nucleotide metabolism.23 Patients with VCZ-induced hepatotoxicity also exhibit corresponding compensatory protective responses, including cellular repair, energy production, and alteration to bile acid homeostasis.24 Reduced fatty acids oxidation and bile acid excretion may also serve as potential mechanisms underlying VCZ-associated hepatotoxicity.25
Fluid resuscitation is a crucial therapeutic intervention for hyperlactatemia. A prospective study26 found that patients with decompensated cirrhosis or liver dysfunction treated with nucleos(t)ide analogs (NAs) are at higher risk of lactic acidosis, requiring close monitoring. The mechanism of NA-induced lactic acidosis is not fully understood but may involve mitochondrial DNA depletion, impaired oxidative phosphorylation, and increased anaerobic glycolysis.26 In patients with normal hepatic and renal function, long-term use of metformin does not increase the risk of lactic acidosis, and its incidence with appropriate metformin therapy is comparable to that of other glucose-lowering treatments.27
Visual disturbances are common with VCZ, occurring in approximately 30% of patients, and include photophobia, blurred vision, color vision changes, and visual field defects.28 These effects can induce anxiety, fear, and increase the risk of falls and bed falls. Visual disturbances typically occur early in VCZ therapy, with considerable variability in the onset and duration of these effects among different patients.29 The association between VCZ serum concentrations and the incidence of visual disturbances remains uncertain.30 The mechanism of VCZ-induced visual disturbances may involve reversible dysfunction of retinal bipolar cells.31,32 VCZ-induced visual disturbances are usually reversible and transient, with a favorable prognosis.
VCZ-related skin reactions occur in approximately 20% of patients, with phototoxicity affecting over 40% of patients after 4–6 months of use, primarily manifesting as photosensitivity reactions, actinic keratosis, pseudoporphyria, and photodermatitis.33 In severe cases, squamous cell carcinoma and neuroendocrine carcinoma of the skin can occur.33 The mechanisms underlying VCZ-induced pigmentation are likely multifactorial and may involve adrenal insufficiency, CYP3A4-mediated inhibition of retinoic acid metabolism, and the photosensitizing properties of VCZ metabolites.34–36 Skin cancer induction by VCZ is caused by impaired DNA damage detection due to chromatin compaction.37
Hypokalemia is a risk factor for QT prolongation, which can lead to torsades de pointes, ventricular fibrillation, and sudden death. Glycyrrhizin inhibits 11β-hydroxysteroid dehydrogenase 2, leading to cortisol-induced mineralocorticoid receptor activation, sodium retention, and potassium loss.38 VCZ-related hypokalemia occurs in 18.0% of patients, with 81.2% occurring within 14 days and 56.2% within one week, more commonly in females, those receiving intravenous VCZ, and those on concomitant antibiotics.39 The ratio of VCZ N-oxide (VNO) to VCZ trough concentration may reflect VCZ clearance, with reduced clearance being a risk factor for hypokalemia, suggesting routine monitoring of VNO trough concentrations.39 The mechanisms underlying VCZ-induced hypokalemia are not fully elucidated.
Treatment-dependent ABPA is defined as two or more ABPA exacerbations within three months of stopping glucocorticoids or after two attempts at tapering oral steroids, with worsening respiratory symptoms, imaging findings, or a 50% increase in serum total IgE within four weeks.40 ABPA is associated with elevated IgE, and omalizumab may help stabilize treatment-dependent ABPA. Omalizumab improves symptoms, reduces asthma exacerbations and hospitalizations, improves lung function, and reduces oral steroid use in ABPA.41 A Chinese multicenter study found that omalizumab effectively reduces acute exacerbation frequency and necessary glucocorticoid doses in adult ABPA patients with asthma, with age and BMI potentially influencing treatment outcomes.42
The eventual treatment outcome was satisfactory, an achievement underpinned by the clinical pharmacist’s provision of full-course pharmaceutical care. Using this case as an exemplar, this paper delineates and summarizes an efficient, multi-dimensional pharmaceutical care model for ABPA patients.
Recent years have witnessed rapid development of full-course pharmaceutical care in China, particularly in chronic disease management, with growing exploration of specialized care models for specific diseases.4 In this case, the full-course model was operationalized by integrating early pharmaceutical assessment, in-hospital monitoring, and post-discharge follow-up into a seamless continuum of care, with comprehensiveness and continuity as its guiding principles. Through systematic exploration and practice, clinical pharmacists have preliminarily established a full-course pharmaceutical care model for ABPA (see Figure 1 for workflow). In practice, clinical pharmacist multidisciplinary team interaction is dynamic and needs-based. Primary communication modalities include informal daily communication during ward rounds, formal pharmaceutical consultations, and scheduled multidisciplinary team (MDT) meetings, with communication frequency intrinsically linked to patients’ clinical status. Through comprehensive involvement in ABPA treatment management, clinical pharmacists facilitate early identification and intervention of ADRs, timely optimization of therapeutic regimens, and significant enhancement of pharmacotherapy safety/efficacy, patient compliance, and rational medication use. Emerging evidence indicates that the application of pharmacist-led, structured quality improvement approaches can effectively optimize therapeutic regimens, enhance multidisciplinary collaboration, and improve the safety and efficacy of clinical pharmacotherapy.43 However, standardized evaluation criteria and assessment systems for full-course pharmaceutical care models have not yet been specified in detail. The absence of unified standards has led to independent exploration based on local practices, resulting in variable quality of pharmaceutical care services and a need for improved homogeneity across implementations.
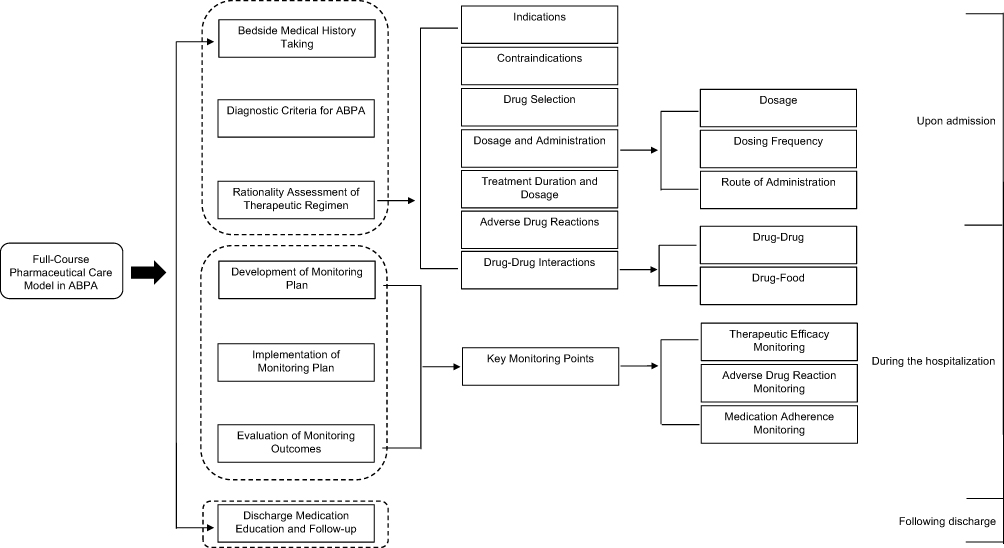 |
Figure 1 Full-course pharmaceutical care model for patients with allergic bronchopulmonary aspergillosis (ABPA), illustrating each stage from clinical assessment and therapeutic regimen evaluation to monitoring, education, and follow-up. |
Conclusion
The treatment duration for ABPA varies based on disease severity, typically exceeding six months. This complex and prolonged treatment process represents a critical area for clinical pharmacists to integrate into clinical teams, demonstrate specialized expertise, and serves as a key entry point for advancing high-quality pharmaceutical care. It fully demonstrates the value of pharmacists in patient management.
The pharmacist-led, full-course care model ensures continuous, comprehensive pharmaceutical support across all treatment phases through early medication evaluation at admission, dynamic in-hospital monitoring with personalized guidance, and structured post-discharge follow-up that extends into community and home settings. This integrated approach enhances medication safety and efficacy, thereby improving patient quality of life.
This model underscores the indispensable role of the clinical pharmacist in enhancing the safety and efficacy of pharmacotherapy for complex respiratory conditions like ABPA. It provides a replicable framework for implementing structured pharmaceutical care in pulmonary fungal diseases and highlights a strategic pathway for advancing high-quality, patient-centered pharmacy services within multidisciplinary teams.
Abbreviations
CT, computed tomography; IgG, immunoglobulin G; ALT, alanine transaminase; HbA1c, glycated hemoglobin; IgE, immunoglobulin E; DILI, drug-induced liver injury; FBG, Fasting Blood Glucose; PBG, Postprandial Blood Glucose; CHB, Chronic hepatitis B.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Patient Consent and Ethics Statement
The whole research process follows the ethical standards of the institutional and/or national research committee and the Declaration of Helsinki. This study was approved by the Ethics Committee of Wenzhou TCM Hospital of Zhejiang Chinese Medical University (WZY2025-LW-059-01). The patient provided informed consent for the publication of the case.
Acknowledgments
We thank all study participants.
Funding
This work was supported by the Special Research Project of the Afliated Hospital of Zhejiang Chinese Medical University [grant numbers: 2023FSYYZY25] and Wenzhou City Science and Technology Project [grant numbers: Y2023258].
Disclosure
The authors have no conflicts of interest to disclose for this work.
References
1. Agarwal R, Muthu V, Sehgal IS, Dhooria S, Prasad KT, Aggarwal AN. Allergic bronchopulmonary Aspergillosis. Clin Chest Med. 2022;43(1):99–9. doi:10.1016/j.ccm.2021.12.002
2. Asthma Group of Chinese Thoracic Society. Expert consensus on the diagnosis and treatment of allergic bronchopulmonary aspergillosis(2022 update). Chin J Tuberc Respir Dis. 2022;45(12):1169–1179. in Chinese.
3. Denning DW, Pleuvry A, Cole DC. Global burden of allergic bronchopulmonary aspergillosis with asthma and its complication chronic pulmonary aspergillosis in adults. Med Mycol. 2013;51(4):361–370. doi:10.3109/13693786.2012.738312
4. Zhao Y, Ju X, Li X, Dong Z. Research hotspot and development trend of integrated pharmaceutical care in China based on CiteSpace and VOSviewer. Chin J Clin Pharm. 2025;34(06):422–430. in Chinese.
5. Kwon-Chung KJ, Sugui JA. Aspergillus fumigatus–what makes the species a ubiquitous human fungal pathogen. Plos Pathog. 2013;9(12):e1003743. doi:10.1371/journal.ppat.1003743
6. Carvalho A, Cunha C, Pasqualotto AC, Pitzurra L, Denning DW, Romani L. Genetic variability of innate immunity impacts human susceptibility to fungal diseases. Int J Infect Dis. 2010;14(6):e460–468. doi:10.1016/j.ijid.2009.06.028
7. Saxena S, Madan T, Shah A, Muralidhar K, Sarma PU. Association of polymorphisms in the collagen region of SP-A2 with increased levels of total IgE antibodies and eosinophilia in patients with allergic bronchopulmonary aspergillosis. J Allergy Clin Immunol. 2003;111(5):1001–1007. doi:10.1067/mai.2003.1395
8. Carvalho A, Pasqualotto AC, Pitzurra L, Romani L, Denning DW, Rodrigues F. Polymorphisms in toll-like receptor genes and susceptibility to pulmonary aspergillosis. J Infect Dis. 2008;197(4):618–621. doi:10.1086/526500
9. Chauhan B, Santiago L, Hutcheson PS, et al. Evidence for the involvement of two different MHC class II regions in susceptibility or protection in allergic bronchopulmonary aspergillosis. J Allergy Clin Immunol. 2000;106(4):723–729. doi:10.1067/mai.2000.109913
10. Kita H. ILC2s and fungal allergy. Allergol Int. 2015;64(3):219–226. doi:10.1016/j.alit.2015.04.004
11. Agarwal R, Aggarwal AN, Dhooria S, et al. A randomised trial of glucocorticoids in acute-stage allergic bronchopulmonary aspergillosis complicating asthma. Eur Respir J. 2016;47(2):490–498. doi:10.1183/13993003.01475-2015
12. Paul S, Dickstein A, Saxena A, et al. Role of surface antibody in hepatitis B reactivation in patients with resolved infection and hematologic malignancy: a meta-analysis. Hepatology. 2017;66(2):379–388. doi:10.1002/hep.29082
13. Arastehfar A, Carvalho A, Houbraken J, et al. Aspergillus fumigatus and aspergillosis: from basics to clinics. Stud Mycol. 2021;100:100115. doi:10.1016/j.simyco.2021.100115
14. Agarwal R, Muthu V, Sehgal IS, et al. A randomised trial of prednisolone versus prednisolone and itraconazole in acute-stage allergic bronchopulmonary aspergillosis complicating asthma. Eur Respir J. 2021;59(4):2101787. doi:10.1183/13993003.01787-2021
15. Hu B, Pan J, Gao X, eds. Harrison’s TM Infectious Diseases.
16. Zhou ZX, Yin XD, Zhang Y, et al. Antifungal drugs and drug-induced liver injury: a real-world study leveraging the FDA adverse event reporting system database. Front Pharmacol. 2022;13:891336. doi:10.3389/fphar.2022.891336
17. Agarwal R, Dhooria S, Sehgal IS, et al. A randomised trial of voriconazole and prednisolone monotherapy in acute-stage allergic bronchopulmonary aspergillosis complicating asthma. Eur Respir J. 2018;52(3):1801159. doi:10.1183/13993003.01159-2018
18. Chishimba L, Niven RM, Cooley J, Denning DW. Voriconazole and posaconazole improve asthma severity in allergic bronchopulmonary aspergillosis and severe asthma with fungal sensitization. J Asthma. 2012;49(4):423–433. doi:10.3109/02770903.2012.662568
19. Jacobs SE, Saez-Lacy D, Wynkoop W, Walsh TJ. Successful treatment of allergic bronchopulmonary aspergillosis with isavuconazole: Case report and review of the literature. Open Forum Infect Dis. 2017;4(2):ofx040. doi:10.1093/ofid/ofx040
20. Chen K, Zhang X, Ke X, Du G, Yang K, Zhai S. Individualized medication of voriconazole: a practice guideline of the division of therapeutic drug monitoring, Chinese pharmacological society. Ther Drug Monit. 2018;40(6):663–674. doi:10.1097/FTD.0000000000000561
21. Chen F, Hu S, Liu J, Hu S. Liver injury associated with voriconazole: a real-world study. Chin J Hosp Pharm. 2021;41(19):2006–2010. in Chinese.
22. Ma J, Wang Y, Ma S, Li J. The investigation and prediction of voriconazole-associated hepatotoxicity under therapeutic drug monitoring. Annu Int Conf IEEE Eng Med Biol Soc. 2023;2023:1–4. doi:10.1109/EMBC40787.2023.10340343
23. Wu SL, Wei TY, Lin SW, Su KY, Kuo CH. Metabolomics investigation of voriconazole-induced hepatotoxicity in mice. Chem Res Toxicol. 2019;32(9):1840–1849. doi:10.1021/acs.chemrestox.9b00176
24. Wu SL, Cheng CN, Wang CC, Lin SW, Kuo CH. Metabolomics analysis of plasma reveals voriconazole-induced hepatotoxicity is associated with oxidative stress. Toxicol Appl Pharmacol. 2020;403:115157. doi:10.1016/j.taap.2020.115157
25. Du Q, Teng M, Yang L, et al. Metabolic characteristics of voriconazole - Induced liver injury in rats. Chem Biol Interact. 2023;383:110693. doi:10.1016/j.cbi.2023.110693
26. Triantos C, Kalafateli M, Aggeletopoulou I, et al. Lactate serum concentrations during treatment with nucleos(t)ide analogues in hepatitis B with or without cirrhosis. Eur J Gastroenterol Hepatol. 2017;29(9):998–1003. doi:10.1097/MEG.0000000000000924
27. Salpeter SR, Greyber E, Pasternak GA, Salpeter EE. Risk of fatal and nonfatal lactic acidosis with metformin use in type 2 diabetes mellitus. Cochrane Database Syst Rev. 2010;(1):CD002967. doi:10.1002/14651858.CD002967.pub3
28. Ren X, Zhang X, Zhan Y, Zhang C, Feng Y. Analysis of 99 cases of voriconazole -induced visual impairment. Chin J Clin Pharmacol. 2022;38(06):589–591. in Chinese.
29. Tian N, He Q, Zhu L, et al. Analysis of 75 cases of visual impairment induced by voriconazole. Drugs Clinic. 2023;38(01):207–212. in Chinese.
30. Jin H, Wang T, Falcione BA, et al. Trough concentration of voriconazole and its relationship with efficacy and safety: a systematic review and meta-analysis. J Antimicrob Chemother. 2016;71(7):1772–1785. doi:10.1093/jac/dkw045
31. Kinoshita J, Iwata N, Ohba M, Kimotsuki T, Yasuda M. Mechanism of voriconazole-induced transient visual disturbance: reversible dysfunction of retinal ON-bipolar cells in monkeys. Invest Ophthalmol Vis Sci. 2011;52(8):5058–5063. doi:10.1167/iovs.11-7183
32. Zrenner E, Tomaszewski K, Hamlin J, Layton G, Wood N. Effects of multiple doses of voriconazole on the vision of healthy volunteers: a double-blind, placebo-controlled study. Ophthalmic Res. 2014;52(1):43–52. doi:10.1159/000359952
33. Chai S, Zhan JL, Zhao LM, Liu XD. Safety of triazole antifungals: a pharmacovigilance study from 2004 to 2021 based on FAERS. Ther Adv Drug Saf. 2022;13:20420986221143266. doi:10.1177/20420986221143266
34. Majumder M, Datta AK, Chakraborty U. Primary adrenal insufficiency and hyperpigmentation. Am J Med. 2023;136(11):1076–1077. doi:10.1016/j.amjmed.2023.07.011
35. Morlière P, Silva AMS, Seixas RSGR, et al. Photosensitisation by voriconazole-N-oxide results from a sequence of solvent and pH-dependent photochemical and thermal reactions. J Photochem Photobiol B. 2018;187:1–9. doi:10.1016/j.jphotobiol.2018.07.023
36. Benitez LL, Carver PL. Adverse effects associated with long-term administration of azole antifungal agents. Drugs. 2019;79(8):833–853. doi:10.1007/s40265-019-01127-8
37. Giovannini S, Weibel L, Schittek B, et al. Skin cancer induction by the antimycotic drug voriconazole is caused by impaired DNA damage detection due to chromatin compaction. J Invest Dermatol. 2024;144(11):2465–2476. doi:10.1016/j.jid.2024.03.050
38. Ceccuzzi G, Rapino A, Perna B, et al. Liquorice toxicity: A comprehensive narrative review. Nutrients. 2023;15(18):3866. doi:10.3390/nu15183866
39. Cheng L, Liu Z, Yu M, Lin L, Xiong L, Dai Q. Hypokalemia and hyponatremia in adult patients receiving voriconazole therapeutic drug monitoring. J Clin Pharmacol. 2024;64(4):461–468. doi:10.1002/jcph.2381
40. Agarwal R, Sehgal IS, Muthu V, et al. Revised ISHAM-ABPA working group clinical practice guidelines for diagnosing, classifying and treating allergic bronchopulmonary aspergillosis/mycoses. Eur Respir J. 2024;63(4):2400061. doi:10.1183/13993003.00061-2024
41. Jin M, Douglass JA, Elborn JS, et al. Omalizumab in allergic bronchopulmonary aspergillosis: a systematic review and meta-analysis. J Allergy Clin Immunol Pract. 2023;11(3):896–905. doi:10.1016/j.jaip.2022.12.012
42. Chen P, Yu Y, He L, et al. Efficacy of omalizumab in adult patients with allergic bronchopulmonary aspergillosis: a multicentre study in China. Clin Exp Med. 2024;24(1):6. doi:10.1007/s10238-023-01267-y
43. Sallam M, Snygg J. Improving antimicrobial stewardship program using the lean six sigma methodology: a descriptive study from Mediclinic Welcare Hospital in Dubai, the UAE. Healthcare. 2023;11(23):3048. doi:10.3390/healthcare11233048
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.