Back to Journals » Pharmacogenomics and Personalized Medicine » Volume 13
Pharmacist Consult Reports to Support Pharmacogenomics Report Interpretation
Authors Bright D ![]() , Saadeh C
, Saadeh C ![]() , DeVuyst-Miller S, Sohn M, Choker A, Langerveld A
, DeVuyst-Miller S, Sohn M, Choker A, Langerveld A
Received 12 August 2020
Accepted for publication 23 October 2020
Published 10 December 2020 Volume 2020:13 Pages 719—724
DOI https://doi.org/10.2147/PGPM.S276687
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Martin H Bluth
David Bright,1 Claire Saadeh,2 Susan DeVuyst-Miller,2 Minji Sohn,1 Ashley Choker,3 Anna Langerveld3
1Department of Pharmaceutical Sciences, Ferris State University College of Pharmacy, Big Rapids, MI 49307, USA; 2Ferris State University College of Pharmacy, Big Rapids, MI 49307, USA; 3Genemarkers, LLC, Kalamazoo, MI 49007, USA
Correspondence: David Bright
Department of Pharmaceutical Sciences, Ferris State University College of Pharmacy, 220 Ferris Dr, Big Rapids, MI 49307, USA
Tel +1 231.591.2231
Email [email protected]
Background: The clinical implementation of pharmacogenomics (PGx) has often involved teams that include pharmacists. PGx laboratories often provide baseline information within the laboratory report that is based on Food and Drug Administration and Clinical Pharmacogenomics Implementation Consortium guidance, but information is often provided independent of concurrent disease states or medication use, among other clinical factors. Major challenges to widescale implementation of PGx include lack of physician experience or confidence in interpreting the data. The purpose of this paper is to describe how pharmacists can help further personalize PGx information and identify clinical recommendations for a given patient.
Methods: This work was performed as a secondary objective of a study evaluating genetic biomarkers of opioid addiction risk. This portion of the study utilized a descriptive analysis of pharmacist consult reports that consist of individualized, patient-level clinical recommendations that take into account current medications, current health conditions, and PGx data. A panel of 60 common PGx targets were tested among patients being treated for chronic pain or opioid use disorder (OUD). A pharmacist consult report was generated and compared with standard laboratory reporting of general PGx information.
Results: Of the 252 patients, PGx reports for 198 (78.6%) contained red and/or yellow clinical decision support flags for medications with actionable or informative PGx guidance for currently prescribed medications. Pharmacists recommended modifications to current prescriptions for 31 (53%) of the patients with actionable flags and 17 (12%) of the patients with informative flags. Drug classes most commonly included medications for cardiology, depression and anxiety, pain (opioids) and gastrointestinal management. Taken together, 24.2% of the actionable and informative flags had immediate clinical value based on the pharmacist’s review. An additional 217 (86%) received one or more clinical recommendations not related to PGx.
Conclusion: While PGx provides another opportunity for pharmacotherapy personalization, PGx data must be considered within the context of other patient-specific factors. Pharmacists were able to streamline the PGx report flags and identify other pharmacotherapy interventions following application of patient-specific data, thereby developing a brief report of recommendations for the patient’s prescriber(s). Engaging clinical pharmacists in the PGx clinical decision process may help to facilitate more widespread PGx implementation.
Keywords: Opioid, pharmacy, pharmacist, pharmacogenetics, pharmacogenomics
Introduction
Pharmacists have been increasingly involved in the clinical implementation of pharmacogenomics (PGx), the use of genetic information to optimize medication use.1,2 Groups including the clinical pharmacogenetics implementation consortium (CPIC) have assisted with the development and dissemination of evidence-based guidance for utilizing PGx in clinical practice.3 Work is underway by CPIC and others to enhance implementation via clinical decision support (CDS) in electronic health records (EHRs),4 but examples of successful and robust implementation are limited. More rapid and widespread adoption of PGx requires clinicians to be able to interpret laboratory reports without automated CDS tools.
Many PGx laboratories have provided information to the ordering health-care professional based on FDA and CPIC guidance, commonly in the form of a PDF report, to facilitate clinical decision making. Color coding/flags or similar keys are used to annotate drug-gene interactions in a way that seeks to clarify the clinical significance of the interaction.5 Evolving FDA guidance highlighted the need to further clarify laboratory annotations of “clinically actionable” and “informative” recommendations in the laboratory test reports, as definitions for these terms are neither universally understood nor agreed upon by a single review body.6 For context, red flags generally correspond with “medication has potentially reduced efficacy, increased toxicity or the patient has an increased risk for the indicated condition” and yellow flags correspond with “guidelines exist for adjusting dosage, increased vigilance or the patient has a moderate risk for the indicated condition.” Guidance was considered actionable if “recommendations (based upon expert groups and consortia) are suitable for implementation in a clinical setting” and informative if “there are insufficient or contradictory findings documenting the impact of a given genetic polymorphism or drug interaction; implementation in a clinical setting is optional”.
An inherent limitation of providing general PGx guidance via laboratory reports is that the information is often given independent of concurrent disease states, concurrent medication use, and other patient characteristics (eg, age and renal function). Similar to how pharmacists have previously demonstrated aptitude for pharmacotherapeutic optimization, recent studies indicate that pharmacists can provide a key role in interpreting PGx through individual consults to assist clinicians to optimize drug therapy.2,7 The purpose of this paper is to describe how pharmacists can help further personalize PGx information and identify clinical recommendations for a given patient. This work was performed as a secondary objective of a study designed to identify genetic mutations associated with opioid use disorder (OUD). Secondary objectives included an evaluation of PGx testing and establishing a workflow for incorporating pharmacists into the PGx testing process. This paper describes the secondary objective related to PGx process.
Methods
Patient Enrollment
Recruitment took place at several outpatient medical practices and addiction clinics in southwest Michigan. Patients enrolled in the study were required to meet the following criteria: (1) Patient had not had a prior PGx test, (2) Patient was at least 18 years of age at the time of enrollment in the study, (3) Patient received either buprenorphine or naltrexone for at least six continuous months prior to enrollment in the study, or at least one of the following long acting opioids (LAOs) for six months or longer: morphine, oxycodone, methadone, and fentanyl, (4) Patient did not take opioids for the purpose of managing cancer-related pain, and (5) Patient was sufficiently fluent in English, signed the informed consent form, and agreed to participate in the study. The study was approved by the Michigan Department of Health and Human Subjects and the Ferris State University Institutional Review Boards. Due to a non-interventional design, this study was not registered in a clinical trials database. All other aspects of the Declaration of Helsinki were followed.
PGx Testing
Testing took place at Genemarkers, LLC in Kalamazoo, MI, a CLIA certified laboratory.
The 60 single nucleotide polymorphisms (SNPs) tested were common pharmacokinetic and pharmacodynamic genes included on Genemarkers’ standard PGx testing panel at the time the study was conducted (Appendix I, study subjects were recruited between March 2018 and August 2018). Since then, the laboratory’s PGx testing panels have been updated to reflect changes in reporting based on FDA recommendations to delineate actionable vs informative data based on updated dosing guidelines. Diplotypes were exported from Applied Biosystems Genotyper software, with genotype and phenotype for the 60 PGx SNPs determined using Translational Software Inc. algorithms, which are commonly employed throughout the PGx laboratory industry. Translational Software Inc.’s algorithms generate “informative” vs “actionable” and red/yellow/green flags for automated clinical decision support notifications on each patient’s PGx laboratory test report.
Pharmacist Consult Process
To ensure greater consistency in report interpretation, a team of 3 clinical pharmacists reviewed each PGx report in the context of the patient’s concurrent medications and health conditions as provided. While clinical practice generally involves one clinician to provide a consult, 3 clinical pharmacists were identified to review the PGx report data (including automatically generated flags) with the intention of: 1) triangulation of result, and 2) to ensure that pharmacists with diverse clinical backgrounds reviewed the data. Pharmacists were selected with expertise in pharmacogenomics, pain management, and substance misuse, with collective practice experience in both inpatient and outpatient care. A list of clinical recommendations was developed by the pharmacist team for the patient using the available patient-specific data, plus information from the FDA, CPIC, and PharmGKB.8,9 Following consult report generation, one of the three pharmacists provided a subsequent review to verify the clinical recommendations. Data on whether the recommended changes were implemented into patient treatment was not collected as part of the study design as no attempt to intervene in prescribing practices was made during the study.
Data Analysis
Patient demographic and characteristics were summarized. Clinical recommendations from the pharmacist review were categorized into four types: (1) PGx-guided recommendations based on actionable flags, (2) PGx-guided recommendations based on informative flags, (3) PGx-guided recommendations not identified in the PGx report, and (4) recommendations not related to PGx. The number and percent of recommendations per each type were reported.
Results
Of the 394 patients recruited into the study, a comprehensive medication list was available for 252 patients; 183 from the OUD cohort and 69 from the chronic pain cohort. Several of the recruiting sites were specialty clinics with limited scope of practice; thus, they did not have current, comprehensive medication lists for the patients. The pharmacy consult results described in this paper include all 252 patients. Characteristics of the 252 patients are summarized in Table 1.
 |
Table 1 Patient Characteristics of 252 Patients |
Of the 252 patients, reports for 198 (78.6%) contained red and/or yellow flags for medications with actionable or informative PGx guidance for currently prescribed medications. Of these, 59 (29.7%) had flags with actionable PGx guidance and 139 (55%) had flags corresponding with informative guidance. Through the consult process, the pharmacists recommended modifications to current prescriptions for 31 (53%) of the patients with actionable flags and 17 (12%) of the patients with informative flags (Figure 1). Drug classes most commonly included medications for cardiology, depression and anxiety, pain (opioids) and gastrointestinal management (Table 1). Taken together, 24.2% of the actionable and informative flags had immediate clinical value based on the pharmacist’s review. An additional 15 of 252 patients (6%) received pharmacist-identified PGx-guided recommendations not flagged.
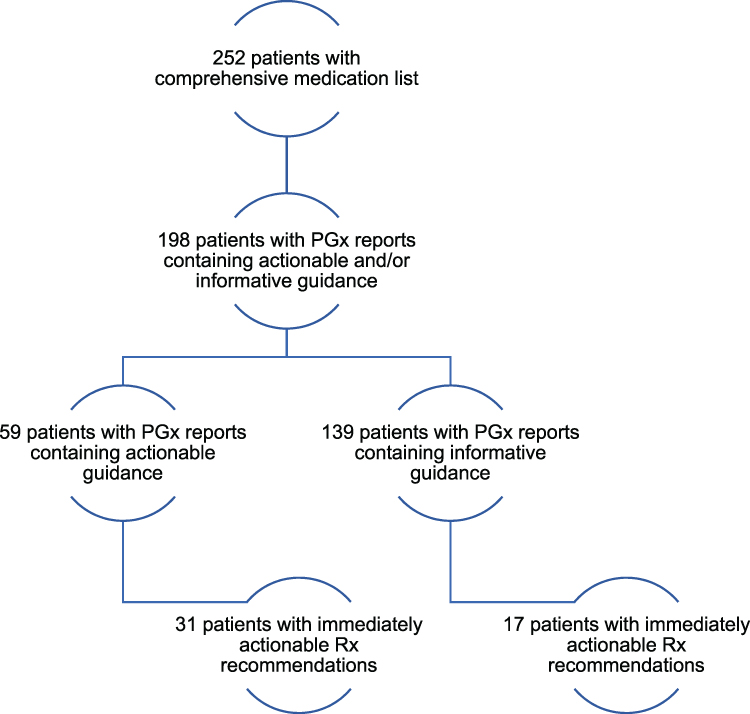 |
Figure 1 Overview of pharmacy consult results. |
The pharmacy consult process produced additional medication recommendations related to PGx that were not identified in the automated clinical decision support notification process because either 1) the condition did not appear to be treated with medication or 2) there was not an immediate prescribing need. Examples of recommendations for untreated conditions included initiating a medication to treat uncontrolled anxiety or depression, with attention to a CYP2C19 and/or CYP2D6 genotype; examples of recommendations for future prescribing included avoiding tramadol or codeine for future pain management in patients with CYP2D6 UM and/or PM genotypes, and to carefully titrate methadone if being used to treat OUD or chronic pain in patients with altered CYP2B6 genotypes.
The pharmacy consult process appeared to serve as a means for identifying additional prescribing issues not related to PGx. Of the 252 patients, 217 (86%) received one or more clinical recommendations not related to PGx. The most common recommendation was to add a naloxone prescription to the current prescription of opioids or medications for OUD (77% of 252). Also, 34% received a recommendation to add or increase short-acting opioids (SAO) to the current prescription of opioids as a breakthrough pain agent, and 15% received a recommendation to initiate gabapentin or titrate the dose of gabapentin. While pharmacist consult reports may not be a consistent part of routine clinical practice, pharmacist input in complex pharmacotherapy decisions that involve PGx is not uncommon.
Discussion
PGx testing can improve medication management for both immediate and future needs by tailoring prescribing to each patient’s metabolism status as determined by genetics. However, the amount of data described in a typical PGx lab report can be onerous to a clinician with limited familiarity in pharmacogenomics, particularly as data is generated independent of the patient’s clinical history and current conditions. Recent reports have suggested that up to 50% of physicians surveyed are not comfortable interpreting genetic laboratory reports.10–12 This paper adds to the growing body of evidence that clinical pharmacists can help improve the utility of PGx and improve prescribing.2,9,13–15 In addition, this study described a process for reducing PGx laboratory report information to a single page of patient-specific clinical recommendations. Furthermore, while clinical decision support tools are becoming more routine for pharmacogenomic management, the pharmacists in this study were able to reduce the number of report-based alerts independent of sophisticated clinical decision support informatics.
In this study, the pharmacists created a manual process for analyzing standard laboratory PGx report guidance, combined with patient-specific medication and clinical condition data to assemble a set of simplified clinical recommendations that were communicated to the prescriber via a simple single-page recommendation sheet. Three pharmacists were involved in the process for the purpose of the study to ensure consistency of results and to reduce the risk of bias. The pharmacists involved in this study believe this could be accomplished in a clinical setting with only one pharmacist. The clinical setting would presumably offer greater access to patient medical records, which would help alleviate assumptions and “what-if’s” from the decision process and streamline execution of recommendations. Pharmacists that engage in clinical reviews to optimize drug therapy based on drug-drug, drug-condition, and other patient-specific factors would already have familiarized themselves with the patient’s history and drug therapy plans; therefore, adding a pharmacogenomic review at that point in the care process would be relatively efficient. The pharmacists also noted that reports were generated faster with experience, signaling that other clinicians may find that pharmacogenomic reviews can be completed more efficiently over time. An implementation study identifying process metrics and/or clinical outcomes may be warranted to further support or refute the notion that pharmacists can contribute efficiently and effectively to clinical implementation of pharmacogenomics. However, this study clarifies that implementation efforts that rely solely on clinical decision support tools may be limited in their ability to capture all potential recommendations, and may bring up many potential issues that may not be relevant to the patient’s immediate care.
The pharmacist’s clinical recommendations were compared with the flags identified in the standard PGx laboratory report. The pharmacy consult process identified 53% of the actionable flags and 12% of the informative flags as immediately clinically relevant. This finding supports the idea that not all flags in a PGx report should necessarily be acted upon if the patient is stable and not experiencing any difficulties. More specifically, involving a pharmacist in the process substantially reduced the number of flags for immediate clinical application. The lower percentage of pharmacist recommendations is likely a function of the point in the care process where the PGx testing occurred. A substantial portion of PGx guidance is related to identifying a starting dose of therapy that can later be titrated based on clinical response. Because testing took place long after much of the drug therapy was initiated, PGx guidance/flags that only informs starting doses would be relatively moot. This issue should not be taken to imply that PGx data is of limited value, but that pharmacists can help to ensure proper application of PGx throughout the care process. In addition, pharmacists identified additional recommendations (both PGx-related and general clinical recommendations) not highlighted in the report due to patient-specific factors not captured in the automatic clinical decision support notification process. Recommendations identified in this way often referenced CPIC, FDA, PharmGKB, and/or related clinical guidelines to the respective disease state(s) referenced and highlight the need for reviewing additional patient-specific characteristics, such as concurrent disease states and missing or extraneous medications. These additional recommendations reinforce that pharmacist participation in the care process may have benefits beyond PGx integration.
Limitations
The nature of the study design created a situation where pharmacists were not provided with treatment history and/or level of control/severity of clinical conditions. The list of clinical conditions provided may have also been incomplete. These limitations did not prevent recommendation generation, but recommendations often were given with qualifiers, such as “if appropriate per the associated condition”. While these are limitations of the analysis, they are not dissimilar from real-world consult requests where limited information may be provided to the consulting pharmacist and may additionally over- or underestimate necessary interventions. However, quantification of recommendations and associated statistics are provided not for the purpose of application to other patient populations, but only to objectively indicate that recommendations were observed related to actionable PGx, informative PGx, unflagged but PGx-related, and general (non-PGx) needs. Scalability of a consultation model could certainly be debated,16 but work to initiate a consult-based pharmacogenomics approach may create a simple starting point similar to other early PGx implementation models.17 Further work towards implementing robust clinical decision support tools within an electronic health record could follow this model over time as those services become more widely accessible. Finally, recommendations do have some clinical subjectivity, but efforts were made to mitigate the subjectivity by involving three pharmacists with diverse clinical backgrounds.
Conclusion
While PGx provides another opportunity for pharmacotherapy personalization, PGx data must be considered within the context of other patient-specific factors. Pharmacists were able to streamline the PGx report flags and identify other pharmacotherapy interventions following application of patient-specific data, thereby developing a brief report of recommendations for the patient’s prescriber(s). Engaging clinical pharmacists in the PGx clinical decision process may help to facilitate more widespread PGx implementation.
Disclosure
The authors report a patent pending related to this study. Support for this research was funded in part by a grant from the Michigan Department of Health and Human Services. Dr Anna Langerveld has an ownership interest in Genemarkers, LLC and Ms Ashley Choker is an employee of Genemarkers, LLC. The authors report no other conflicts of interest in this work.
References
1. Relling MV, Evans WE. Pharmacogenomics in the clinic. Nature. 2015;526(7573):343–350. doi:10.1038/nature15817
2. Owusu-Obeng A, Weitzel KW, Hatton RC, et al. Emerging roles for pharmacists in clinical implementation of pharmacogenomics. Pharmacother. 2014;34(10):1102–1112. doi:10.1002/phar.1481
3. Relling MV, Klein TE, Gammas RS, Whirl-Carrillo M, Hoffman J, Caudle KE. The Clinical Pharmacogenetics Implementation Consortium: 10 years later. Clin Pharmacol Ther. 2020;107(1):171–175. doi:10.1002/cpt.1651
4. Hoffman JM, Dunnenberger HM, Hicks JK, et al. Developing knowledge resources to support precision medicine: principles from the Clinical Pharmacogenetics Implementation Consortium (CPIC). J Am Med Inform Assoc. 2016;23(4):796–801. doi:10.1093/jamia/ocw027
5. Hilden MP, Bright DR, Kisor DF, Christensen H. Pharmacogenomics: a practical primer for senior care pharmacists. Sr Care Pharm. 2019;34(6):363–369. doi:10.4140/TCP.n.2019.363
6. Food and Drug Administration. FDA announces collaborative review of scientific evidence to support associations between genetic information and specific medications; February 2020. Available from: https://www.fda.gov/news-events/press-announcements/fda-announces-collaborative-review-scientific-evidence-support-associations-between-genetic.
7. Bright DR, Greco AJ, Langerveld A, Kisor DF. Clinical implementation of personalized medicine in community pharmacies: considerations for clinicians. Per Med. 2017;14(6):471–475. doi:10.2217/pme-2017-0050
8. Food and Drug Administration. Table of pharmacogenetic associations; February 2020. Available from: https://www.fda.gov/medical-devices/precision-medicine/table-pharmacogenetic-associations.
9. Clinical Pharmacogenetics Implementation Consortium. Guidelines; July 2019. Available from: http://www.cpicpgx.org/guidelines.
10. Frigon M-P, Blackburn M-È, Dubois-Bouchard C, Gagnon A-L, Tardif S, Tremblay K. Pharmacogenetic testing in primary care practice: opinions of physicians, pharmacists and patients. Pharmacogenomics. 2019;20(8):589–598. doi:10.2217/pgs-2019-0004
11. Kim W-Y, Kim H-S, Oh M, Shin J-G. Survey of physicians’ views on the clinical implementation of pharmacogenomics-based personalized therapy. Trans Clin Pharmacol. 2020;28(1):34–42. doi:10.12793/tcp.2020.28.e6
12. Owusu Obeng A, Fei K, Levy K, et al. Physician-reported benefits and barriers to clinical implementation of genomic medicine: a multi-site IGNITE-network survey. J Pers Med. 2018;8(3):24. doi:10.3390/jpm8030024
13. Bank PCD, Swen JJ, Schaap RD, et al. A pilot study of the implementation of pharmacogenomic pharmacist initiated pre-emptive testing in primary care. Eur J Hum Genet. 2019;27(10):1532–1541. doi:10.1038/s41431-019-0454-x
14. American Society of Health-System Pharmacists. ASHP statement on the pharmacist’s role in clinical pharmacogenomics. Am J Health Syst Pharm. 2015;72(7):579–581. doi:10.2146/sp150003
15. Bain KT, Schwartz EJ, Knowlton OV, Knowlton CH, Turgeon J. Implementation of a pharmacist-led pharmacogenomics service for the program of all-inclusive care for the elderly (PHARM-GENOME-PACE). J Am Pharm Assoc. 2018;58(3):281–289. doi:10.1016/j.japh.2018.02.011
16. Empey PE, Stevenson JM, Tuteja S, et al. Multisite investigation of strategies for the implementation of CYP2C19 genotype-guided antiplatelet therapy. Clin Pharmacol Ther. 2018;104(4):664–674. doi:10.1002/cpt.1006
17. Hicks JK, Aquilante C, Dunnenberger HM, et al. Precision pharmacotherapy: integrating pharmacogenomics into clinical pharmacy practice. J Am Coll Clin Pharm. 2019;2(3):303–313. doi:10.1002/jac5.1118
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.