Back to Journals » Integrated Pharmacy Research and Practice » Volume 12
Pharmaceutical Care Within Community Pharmacies: Tools Availability and Pharmacists’ Views, Wad-Medani, Sudan
Authors Eldooma I ![]() , Maatoug M, Yousif M
, Maatoug M, Yousif M
Received 6 December 2022
Accepted for publication 1 February 2023
Published 11 February 2023 Volume 2023:12 Pages 37—47
DOI https://doi.org/10.2147/IPRP.S399265
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Jonathan Ling
Video abstract presented by Ismaeil Eldooma.
Views: 500
Ismaeil Eldooma,1,2 Maha Maatoug,2 Mirghani Yousif2
1National Health Insurance Fund. Planning, Research, and Information, Gezira State, Sudan; 2Clinical Pharmacy & Pharmacy Practice Faculty of Pharmacy, University of Gezira, Wad Medani, Sudan
Correspondence: Ismaeil Eldooma, National Health Insurance Fund, Department of Planning, Research, and Information, Gezira State, Sudan, Tel +249123162135, Email [email protected]
Background: Pharmaceutical Care (PhC) services within community pharmacies (CPs) have become a vital issue in many developed countries.
Purpose: This study assessed the availability of PhC tools and pharmacists’ views towards PhC services within CPs in Sudan.
Methods: A cross-sectional study was conducted from December 2019 to August 2020 using a pretested self-administered questionnaire. The participants were 120 community pharmacists.
Results: Fifty-eight percent of respondents used to work in pharmacies near homes rather than within the marketplace. The study revealed that the overall tool availability of the assessed components and items was only 25% (Counselling areas 3%, Records 5%, Pharmacist identity 3%, Pharmacy phones 15%, Medical devices 38%, and Staff 29%). The result of pharmacists’ views towards the PhC concept, roles, and responsibilities showed a high level of agreement, at 88%, with a statistically insignificant difference between participants.
Conclusion: Tools available within CPs were lower than required. However, pharmacists’ views showed a high agreement level towards PhC concept roles and responsibilities. Community pharmacists, academic sectors, and regulatory authorities must start initiatives to improve the provision of PhC tools for better patient care service delivery.
Keywords: community pharmacies, community pharmacists, pharmaceutical care tools, pharmacists’ views, Sudan
Introduction
In recent years pharmacist roles within community pharmacy (CP) services were changed significantly. In the past, pharmacists’ roles were restricted only to compounding and dispensing.1 The current running and approved pharmacy practice philosophy is the Pharmaceutical Care (PhC) concept globally.2 Redesigning CP practice in Sudan as a response to the PhC concept is crucial, and pharmacists’ views should also comply with the new pharmaceutical services philosophy. In some countries, when implemented, PhC services within community pharmacies (CPs) showed positive outcomes and improved patients’ quality of life.3
CP practice is now evolving.4 PhC services within CPs have become essential and integrated parts of health systems in developed countries. For example, in Europe, PhC services within CPs continued to develop and spread in many countries.5 In Denmark, PhC services within CPs are consistent throughout the country.6 In China, the focus on integrating professional pharmacists within CPs started in 2009 as an essential change in the health system to improve the primary care service level.7 However, in developing countries, it continued to be in the product-oriented practice stage.8 In Sudan, although health professionals recommended the provision of PhC services within CPs, there is a significant gap in the current practice mode.9 Since PhC services have become the pharmacy mission, redesigning CP practice will be valuable. In many studies concerning PhC services, results showed improved health outcomes and decreased costs.10,11 In Sudan, the product-oriented approach of prescription dispensing is dominant and the primary focus of community pharmacists. Despite the minor PhC services provided, such as counseling of chronic illness and monitoring, expanding the community pharmacist roles towards PhC services is crucial.12 The current prescription handling within CPs lacks effective pharmacist interventions to improve patients’ knowledge and medication adherence behaviors.13 In Sudan, this research could support PhC services provision within CPs. This study aimed to assess the current situation of CPs regarding the availability of tools and the pharmacists’ views towards their roles, responsibilities, and confidence in the context of PhC services in Wad-Medani Locality, Gezira State, Sudan.
The situation of CPs’ and pharmacists’ views towards their current practice is determinant in the provision of PhC within CPs. The successful implementation of PhC services starts and ends with pharmacist-led interventions.14 One crucial question was, to what extent do pharmacists understand roles and responsibilities towards PhC services? Other important issues were the pharmacist’s confidence and perceptions towards their knowledge impact on patient’s medical treatment outcomes. Community pharmacists’ acceptance of pharmacy structure and practice redesigning to undertake appropriate PhC services provision is also vital. This study reflected the pharmacists’ acceptance of practice redesigning and pharmacists’ views towards responsibilities and roles compared to the availability of PhC tools within CPs. In Sudan, although health professionals recommended the provision of PhC services within CPs, the current practice does not comply with the globally recommended models.9 PhC requires responsibility bearing, commitment, and tools availability. Successful implementation of PhC services starts and ends with pharmacist-led interventions’.15 This study can become the starting point for adequate PhC services provision within CPs since there were no similar studies in Sudan, according to our knowledge.
Methods
Study Design and Components
A cross-sectional survey was conducted from December 2019 to August 2020. Participants were pharmacists who used to work within CPs in the Wad-Medani locality, Gezira State, Sudan. This study assessed and analyzed CPs’ situation regarding PhC tools and pharmacists’ views toward PhC services within CPs.
The Study Instrument and Data Collection
A self-administered questionnaire was designed based on published literature on PhC services. We used a Google Forms Editor Help website, Docs, and Spread Sheets to enter the collected survey data (Google 2019). The questionnaire contained Six sections of 42-points designed to assess the current status of PhC services provision within CPs. The instrument investigation of tools availability comprises three components (PhC signs, medical devices, and staff members) of 17 items assessed (separate counseling area, pharmacist distinction, pharmacy telephone number, medical devices = six devices, staff members = seven members, and patient pharmacy records). We used a Likert scale with 15 statements to measure pharmacists’ views toward responsibilities, roles, and confidence. The interpretation of Likert scale results followed these ranges: Strongly agree (4.3–5), Agree (3.5–4.3), Undecided (2.7–3.4), Disagree (1.9–2.6), and Strongly Disagree (1 to 1.8).
The validity of the questionnaire was achieved by experts and piloting through 20 CPs. Data were collected using paper-based self-administered questionnaires. The objective, goals, and future benefits and outcomes are summarized in the first section of the questionnaires to inform participants.
Sampling, Data Processing, Data Collection, and Analysis
We have received a list of the sample frame containing the CPs’ names and locations from the General Directorate of Pharmacy, Gezira State, Sudan. The total population was 217 CPs. The Raosoft® online software calculated the sample size. The confidence interval was 95%, and the margin of error was 5%.16 The sample size calculated was (n=139 CPs). To have a representative sampling, we grouped CPs into geolocation stratification regarding Wad-Medani city as the central location. The selected CPs were then grouped into the marketplace and near-home groups. The last grouping was to identify the distribution of pharmacies within the community because the CPs near homes are vital for PhC service provision through integration with the primary care service level. We used these two groups to compare and describe the demographic distribution accordingly and evaluate if there are differences between the two groups.
This research collected data from 120 CPs (response rate 120/139= 86%). Some pharmacies (17 CPs) were not working; due to some regulatory measures such as license freezing or sanctions for not complying with regulations, while others did not have pharmacists in charge (2 CPs). An Excel Data Sheet from Google Forms (EDS) was downloaded to the computer and imported into the analysis software (The Statistical Package of Social Science version 26= SPSS). The Cronbach’s Alpha test for Standardized Items showed acceptable truth of the collected data [α = 0.7; 0.673–0.740; CI= 95%]. Results for categorical data were described, analyzed, and interpreted.
Results
Tools Availability and Demographics Assessment
Demographic Characteristics
Results of CPs locations and grouping showed a high number of CPs distributed near homes, 76 (58%) rather than marketplaces. Most respondents reported permanent registration availability acquired from Sudan Medical Council 92 (77%). Females represented 56 (47%) of those who have received registration, and younger pharmacists aged 21 to 30 and 31 to 40 years represented 99 (83%). The females represented 76 (63%) of the total respondents (Table 1).
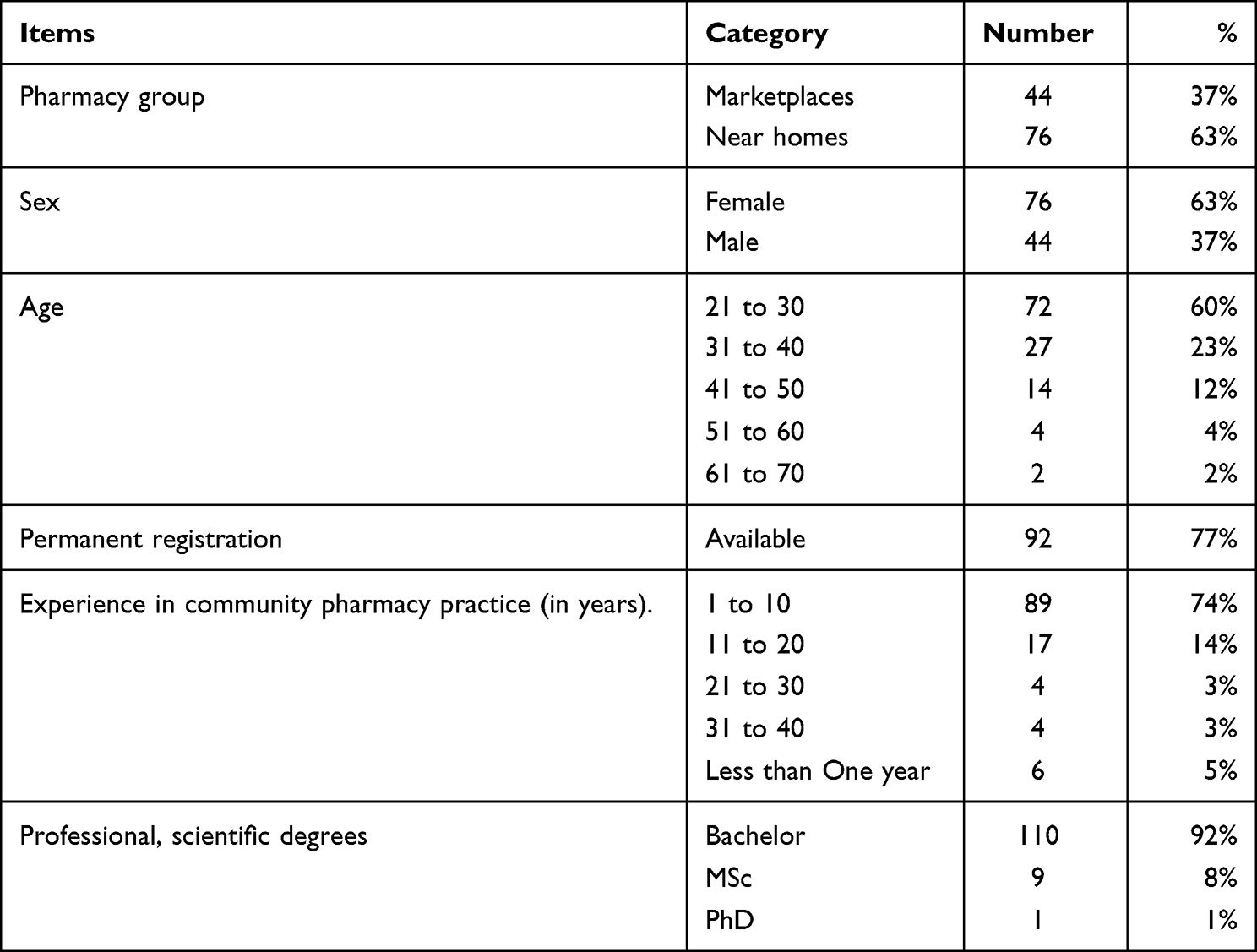 |
Table 1 Demographic Characteristics |
Pharmaceutical Care (PhC) Tools Availability
The assessments of PhC tools availability showed many vital indicators. The separate counseling area within CPs showed only 4 (3%), and the percentage of pharmacists committed to dressing lab coats for identity was only 4(3%). Results of patients’ records within the pharmacies showed only 6 (5%) availability. 18 (15%) of pharmacies have an accessible phone number for counseling purposes. Pharmacies having none of the recommended devices represented 81 (68%). However, 26 (22%) pharmacies had a weight balance device. (Table 2).
 |
Table 2 Tools Availability |
The overall availability of staff members identified compared to the virtual investigated staff members (7*120 = 840) was only 239 (29%) (Table 2). Results of staff categories showed 41 (34%) of available staff members were pharmacists only and a pharmacist with assistant 40 (33%), while staff members of a pharmacist, assistant, and cleaning worker results showed 16 (13%). Cashiers, counters, trainees, and technicians showed lower percentages > 5% (Table 3). The average availability of the investigated tool components regarding PhC services is only 25%.
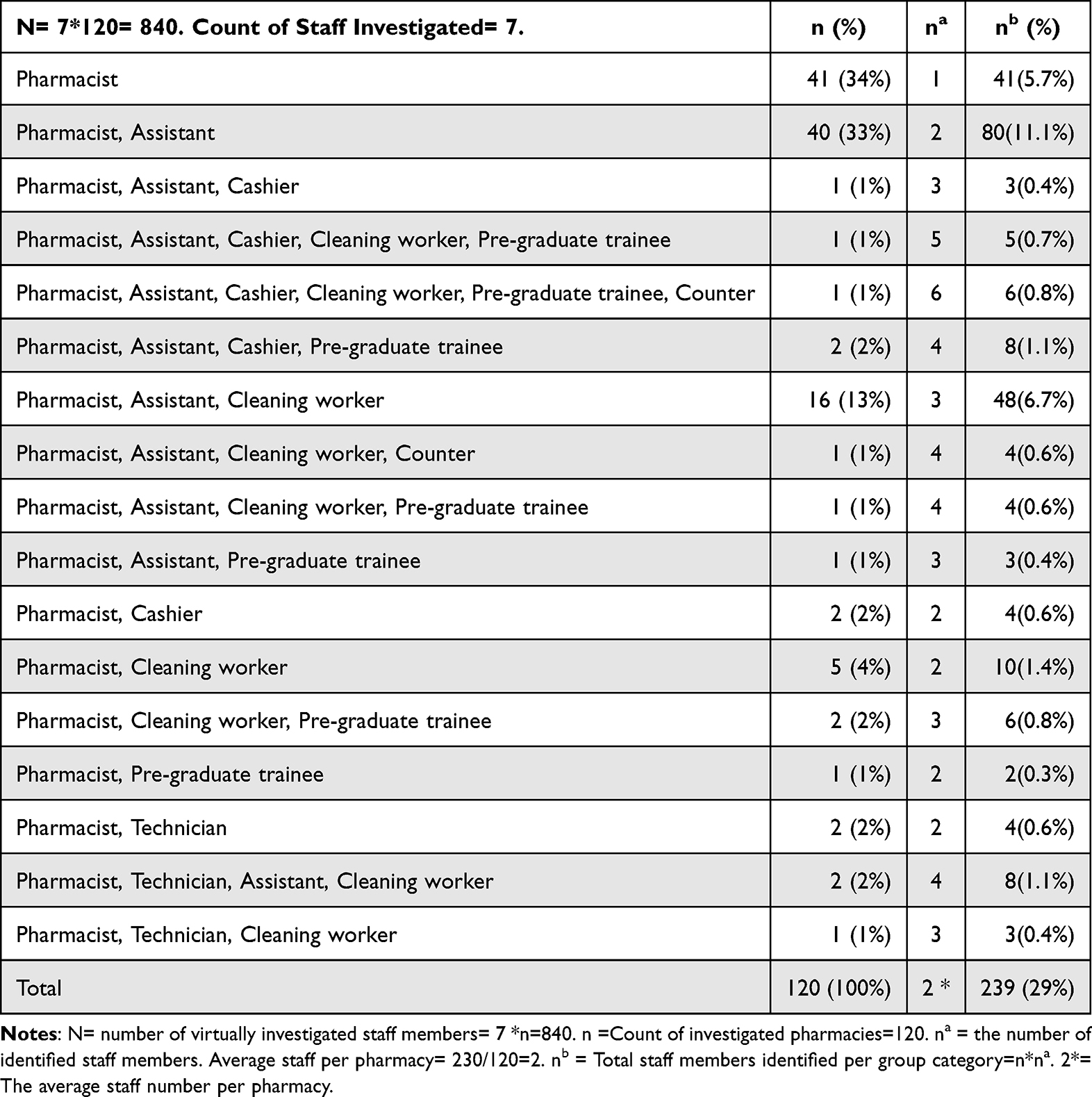 |
Table 3 Staff Members’ Categories |
Main Information Sources
Internet websites or databases as the primary sources of information represented 72 (60%), while 30 (25%) pharmacists depend on books and references. However, the drug information center represented only 3 (3%) (Table 4).
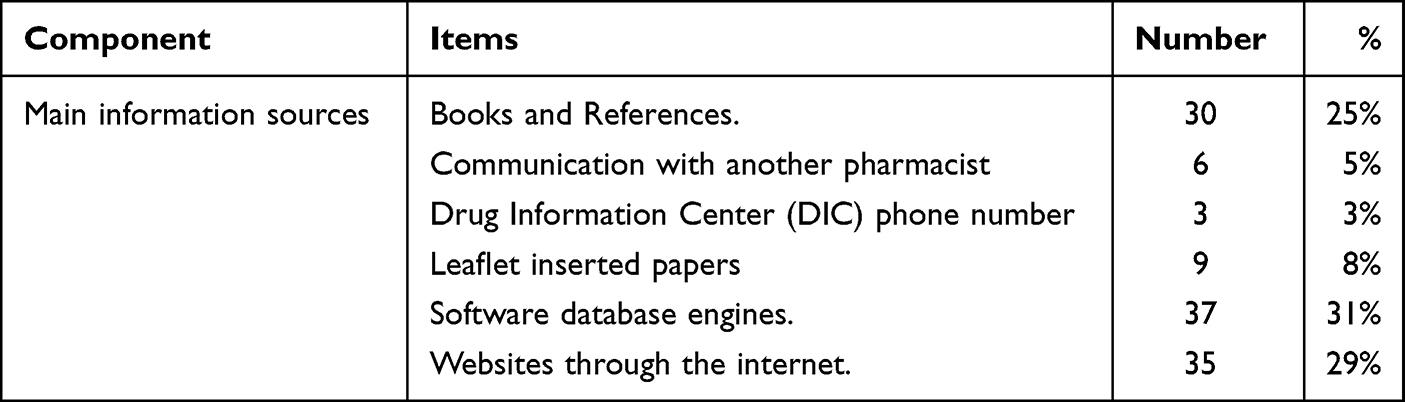 |
Table 4 Main Information Sources for Pharmacists |
Communication with Physicians
Communication with the physicians as a means for better PhC service provision showed that 72 (60%) of pharmacists had communicated with the physicians, of which 45 (38%) were working in CPs near homes (Table 5).
 |
Table 5 Communication with Physicians Six Months Ago |
Community Pharmacists’ Understanding of Roles, Responsibilities, and Acceptance of PhC Services Provision Within CPs
Results of 5-point Likert scale measures showed that the overall mean scores for understanding roles and responsibilities within CPs were 87.27% [mean= 4.36, SD ± 0.73, mean < 3(Undecided)]. The participants’ views were within the strongly agreed direction (4.3 to 5) (Table 5). Results also showed the mean scores of pharmacists’ confidence towards services provision effectiveness on patient medical treatment outcomes was 88.15% [mean=4.41; SD ± 0.81, mean < 3 (Undecided)]. The direction of participants’ views was also within the strongly agreed direction (range 4.3 to 5).
The pharmacists’ acceptance of CP structure redesigning to provide PhC services was 88.6% [mean = 4.43, SD ± 0.62, mean scores < 3(Undecided)]. The direction of participants’ views was also within the strongly agreed path (range 4.3 to 5).
Comparing Results of the Pharmacy Groups (Near Homes and Marketplaces)
Pharmacists’ views towards PhC services provided by CPs were compared according to pharmacy groups (pharmacies near homes and at the marketplace). There was no significant statistical difference between views regarding CP groups. All answers showed a P value(sig) < 0.05 [P value = 0.54 < 0.05, df = 1 to 4]. Nevertheless, the overall tools availability results showed only 25%; pharmacists’ views towards accepting change and redesigning the current practice towards PhC service provision was 88.6%.
Results of communication with the physician also showed no significant statistical difference between pharmacists working within CPs near homes and the marketplaces [df = 1, P value (sig) = 0. 257 < 0.05].
Discussion
Situational assessment and investigation of PhC services provision and professionals are vital in redesigning health systems to improve outcomes and service user satisfaction.7,17–20 PhC service models differ between countries.21 PhC within CPs is vital for better medication use outcomes. In some countries, the digitalized care services for drug-drug interaction identification and electronic -health services were also used and assessed within the context of PhC services provided by CPs.18,20 We assessed the CPs’ situation, pharmacists’ views, responsibilities, roles, and acceptance regarding the PhC concept, compared and analyzed the results.
Demographic results showed that 58% of the CPs were near homes. This result reflected the suitable availability of accessible CPs to serve the community since CPs’ principal role is to help people in outpatients and near their homestay.22 The pharmacists require permanent registration approval to practice legally within CPs. However, in this study, pharmacists having permanent registration represented 77%, so some pharmacists had not yet acquired the registration. The female gender represented 47%. Younger pharmacists aged 21 to 40 represented 83%, of which 58% were females (Table 1). The reason behind the prevalence of a higher number of female gender may be the increased number of female graduates. These results, when compared to a previous study conducted in Sudan, respondents aged 21 to 30 years were 73%, BPharm 94%, and One to 10 years of experience 67%.23 The current demographic distribution of CPs and pharmacists was acceptable (based on population construction, in which the females’ count is higher than the males’). However, pharmacists over 40 years who by default have good experience represented only 18%; some reasons may be associated with this result. Whatever the demographic distribution of CPs, the availability of some tools for PhC service provision is essential.
The separate counseling area is an essential item of the tools component that can be created within CPs. Results showed that only 3% of the investigated pharmacies have. Separate counseling areas are signs of PhC service provision. Lack of adequate counseling area may affect pharmacists’ and patients’ interactions.24 It is necessary to create a separate counseling area within pharmacies for appropriate PhC services provision.25 The second essential item is the pharmacist’s professional identity. Professional identity, behavioral norms, and values are interrelated and vital satisfaction factors for adequate PhC service provision.26 However, results showed that only 3% of pharmacists dressed in lab coats for identity. Accordingly, Sudanese community pharmacists lack identity among the pharmacy staff members. Lacking identity may affect the satisfaction of both pharmacists and patients.27,28 The availability of identified and distinct pharmacists in a separate counseling area may motivate the provision of PhC services and satisfy clients with an improved perception of pharmacy and pharmacists.29 The Patients’ pharmacy records are considered to be essential also. This study identified only 5% of records availability. However, these records did not comply with PhC services data records. There was no sort of computerized system. In some previous studies, researchers advised pharmacists to proactively ask new patients for some information and conduct documentation (subjective and objective) to improve medication use risk management.30 One of the most vital pieces of information to be recorded is the patient phone number. Phone numbers can help to monitor treatment outcomes in a scheduled follow-up through a callback.31,32 There was no public phone number in most pharmacies, only 15%.
Medical activities within CPs, including blood pressure and sugar monitoring, case assessment, treatment plan setting and evaluation, and routine counseling, are provided in developed countries.33,34 In this study, many pharmacies did not have any recommended medical devices for PhC service provision (68%). However, 22% of pharmacies have weight-balance scale devices (Table 2). In some studies, researchers recommended that pharmacists must be innovators in following ideal practical methods to improve and monitor medication use and disease management outcomes.35 Some published literature states that pharmacists can use many medical devices for PhC services provision. The Blood Glucose Monitor(BGM), Blood Pressure Monitor (BPM), Body Temperature Thermometer (BTT), Weighing Balance Scale (WBS), nebulizers, Metered Dose Inhaler (MDI), and Insulin Pens (IP) have been used effectively by community pharmacists.36 The appropriate PhC services, besides the recommended tools, require accessible and reliable information sources.
Reliable and accessible information sources can be reference books, computer databases, internet websites, and published literature.37–40 This study revealed that 60% of pharmacists depend on internet websites and software databases as significant information sources, while 25% on books. However, drug information centers represented only 3% (Table 4). In Switzerland, although the Swiss drug reference book is popular, 88% of pharmacists have access to the internet within pharmacies.41 A recently published study in Ethiopia showed that 46% of pharmacists use books, and 44% use the internet as information sources.17 Well-designed and equipped counseling area with accessible information sources also requires organized and complete staff since pharmacists alone cannot provide adequate and satisfied professional PhC services.
Organized staff members will support pharmacists with enough time to provide appropriate PhC service.42 However, this study showed a lone pharmacist 34% and a pharmacist working with an assistant 33%. Cashiers, cleaning workers, and technicians represented lower than 5% (Table 4). Complete staff and well-designed PhC service within CPs will positively impact patients when integrated with other healthcare providers.42,43
Pharmacists can integrate PhC services in CPs with physicians. This study showed 60% communication with physicians during work, of which 38% of pharmacists work within CPs near homes (Table 5). This result indicates integration evolvement, which may be due to the evolution of information technology (cell phones spreading).
According to this research results and discussion, the current practice of PhC services within CPs in Sudan requires redesigning and new model adoption. Changing the current situation depends on pharmacists’ views towards the PhC concept, pharmacists’ responsibilities, and roles. This study revealed the levels of community pharmacists’ agreement towards roles and responsibilities in PhC provision within CPs. Among nine statements, responses concerning views towards roles and responsibilities showed 87.27% of positive responses for most participants’ (strongly agree and agree) [mean = 4.36 ± 0.73] (Table 6). Participants’ responses showed no significant variations between respondents [t test = 0.19 > t table =1.984; n< 100]. This result complies with the American Society of Health-System Pharmacists (ASHSP) goals.44 Despite this, community pharmacists were aware of undertaking the duties of PhC within CPs. Pharmacists within the health systems must be accountable for the medication use processes, engage with other health care providers, set up a strategic vision for the pharmacy administration, and advocate for reforming pharmacy practice.45 On the other hand, conducting effective PhC services requires confident pharmacists in the pharmacy profession.46
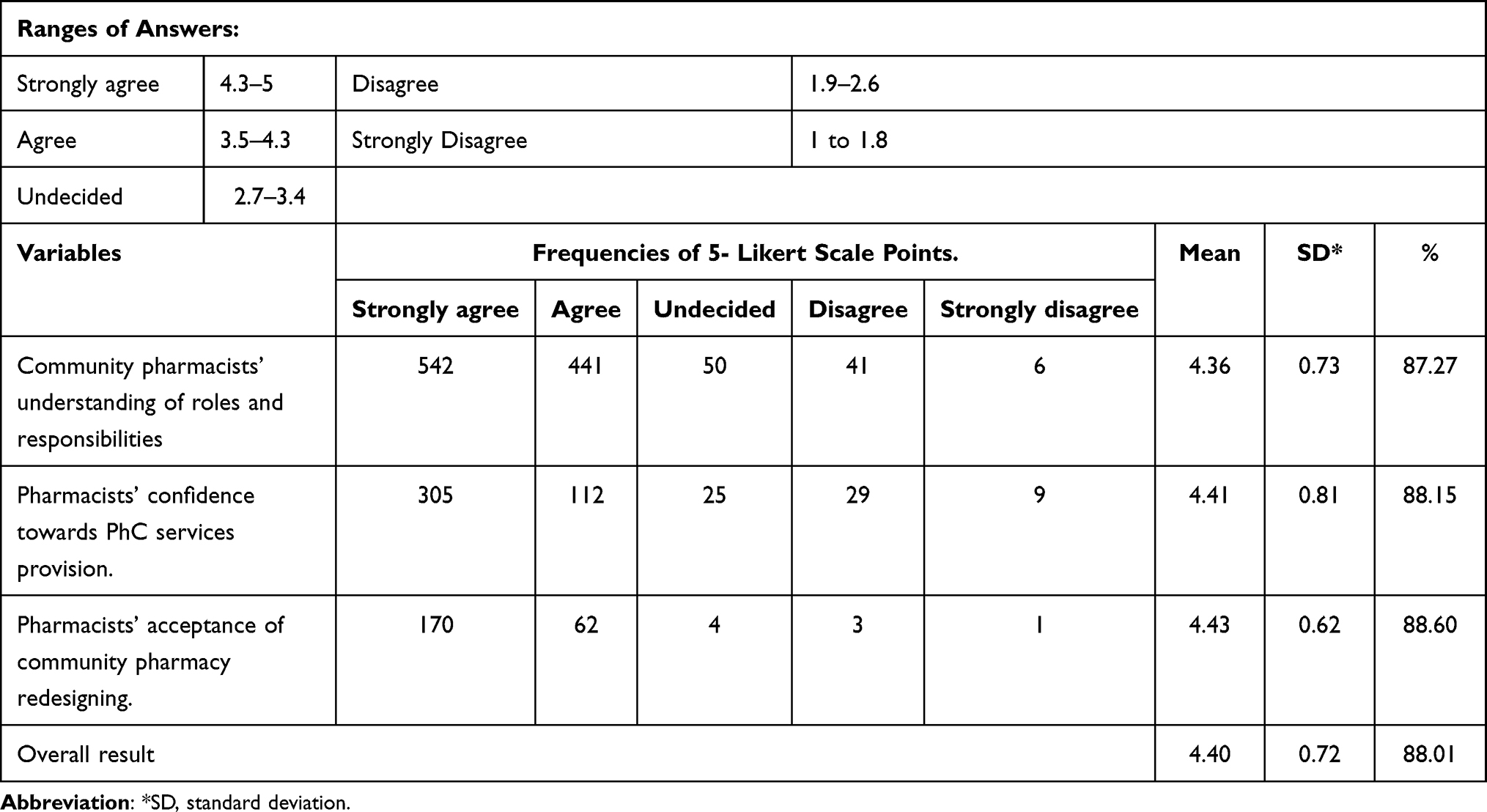 |
Table 6 Five Points Likert Scale Measures Results |
Confident pharmacists trust their identity in counseling through their acquired knowledge.47 The confident pharmacist dispenses medications to patients, has expertise in the safe use of medicines, conducts screenings, provides advanced services, undertakes follow-up of patients, have roles in health promotion with trustfulness that they can achieve the best outcomes. Many studies showed the rare availability of confident pharmacists in clinical decision-making.45 Pharmacists are knowledgeable about patients’ medical treatment outcomes within CPs regarding PhC services.48–51 In this study, pharmacists’ confidence level towards their impact on patients’ medical treatment showed 88.15% confidence [mean = 4.41, ± 0.81 and mean scores < 3] (Table 6). Participants’ responses showed insignificant variation for all statements in this construct [t test = 0.24 > t table =1.984, n< 100].
In a previous study, Sudanese community pharmacists accepted PhC practice services with some interventions recommended.52 This study also revealed the acceptance of CP structure redesigning for PhC services provision. Pharmacists’ acceptance of CP structure changing and redesigning was 88.6% [mean = 4.387± 0.62, scores < the mean = 3] (Table 6). Participants’ answers showed insignificant statistical variation between pharmacists in the construct [t test = 0.22 > t table =1.984, n< 100].
Regarding the pharmacist views result, Sudanese pharmacists understand their roles and responsibilities towards PhC service very well, with a high acceptance of the PhC concept. Pharmacists also perceive themselves as confident towards their knowledge impact on clinical outcomes, and this criterion will support current practice improvement and reform.
Results showed insignificant statistical differences in views of pharmacists working within pharmacies near homes and the marketplace regarding responsibilities and roles towards PhC service statements [P value(sig) ≥ 0.05, df = 1 to 4]. The overall PhC tools availability showed only 25% availability; nevertheless, the pharmacists’ views towards acceptance of changing current practices were 88.6%. Results of communication with physicians for better PhC service provision also showed no significant difference between pharmacy groups (near homes = 40% and marketplaces = 60%, df = 1, P value < 0.05, sig = 0.257), pharmacists’ communication with physicians represented higher percentage 58% for CPs near to homes. Regarding these results, it is evident that reforming practices within CPs toward PhC services is possible. Acceptance of CPs structure redesigning within the context of PhC services was also good. Pharmacy professionals in Sudan can start developing new models of CP practice within the context of PhC services.
Conclusion
CP practice in Sudan has stayed in the traditional (product dispensing-oriented) stage. PhC services within CPs require supportive tools availability. In this study tools, availability results did not comply with the evolving CP practice in developed countries. Successful development of current practice requires redesigning of system and practice towards the phC service context. Community pharmacists’ views appeared with a high level of agreement towards PhC services roles, responsibilities, concepts, pharmacists’ knowledge confidence, and redesigning of CP structure components. Regulatory authorities can support the CP reform through regulations and policy setting regarding these findings. Pharmacists are responsible and trusted fully in their roles and knowledge. Shifting from the current traditional CP practice to a patient-centered and outcome-oriented approach was highly acceptable among participants. The change of current practice requires tools gap filling with supportive and legal regulations to implement PhC models. Community pharmacists, academic sectors, and regulatory authorities must start initiatives to improve the current practices. Pharmacists should establish PhC models adapted to the Sudanese situation within CPs in the coming years.
Abbreviations
PhC, Pharmaceutical Care; CP, Community Pharmacy; df, degree of freedom; SD, standard deviation; B Pharm, Bachelor of Pharmacy.
Data Sharing Statement
The data sets analyzed in the current study are available from the corresponding author and can be provided upon request.
Ethical Approval and Consent to Participation
The Department of Clinical Pharmacy and Pharmacy Practice accepted this research’s final manuscript. The Ministry of Health in Gezira State, the Research Department, and the Health Sector Ethical Review Committee, University of Gezira, provided the ethical clearance (Reference number: 37-21). All Authors confirmed adherence to the terms of the Helsinki Agreement. We informed all participants about the research purpose through a written brief introduction (in Arabic) in the first section of the questionnaires, illustrating the purpose and future benefits of the collected research data for the pharmacists and patients. The questionnaire contains an agreement statement “By filling out this questionnaire, agreement to be a participant in this research is confirmed, study and you are aware of what it involves.” All participants provided a paper-based self-administered questionnaire after a verbal agreement to participate.
Acknowledgment
We are grateful to all participants in CPs in the Wad Medani locality, Gezira State. We appreciate the Faculty of Pharmacy, the University of Gezira Staff members, and especially the Department of Clinical Pharmacy and Pharmacy Practice for their great opinions and comprehensive discussion during manuscript preparation.
Funding
No financial support to conduct this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zineldin M. The quality of health care and patient satisfaction: an exploratory investigation of the 5Qs model at some Egyptian and Jordanian medical clinics. Int J Health Care Quality Assurance. 2006;19(1):60–92. doi:10.1108/09526860610642609
2. Azzopardi LM. Validation Instruments for Community Pharmacy: Pharmaceutical Care for the Third Millennium. CRC Press; 2000.
3. van Mil JF, Schulz M. A review of pharmaceutical care in community pharmacy in Europe. Harvard Health Policy. 2006;7(1):155–168.
4. George PP, Molina JA, Cheah J, Chan SC, Lim B. The evolving role of the community pharmacist in chronic disease management-a literature review. Ann Acad Med Singapore. 2010;39(11):861–867.
5. Costa FA, Scullin C, Al-Taani G, et al. provision of pharmaceutical care by community pharmacists across Europe: is it developing and spreading? J Eval Clin Pract. 2017;23(6):1336–1347. doi:10.1111/jep.12783
6. Abrahamsen B, Burghle AH, Rossing C. Pharmaceutical care services available in Danish community pharmacies. Int J Clin Pharm. 2020;42(2):315–320. doi:10.1007/s11096-020-00985-7
7. Jiang M, Liu J. Community pharmacy practice in China: past, present, and future. Int J Clin Pharm. 2013;35(4):520–528. doi:10.1007/s11096-013-9789-5
8. Azhar S, Hassali MA, Ibrahim MIM, Ahmad M, Masood I, Shafie A. The role of pharmacists in developing countries: the current scenario in Pakistan. Human Resources Health. 2009;7(1):1–6.
9. Ibrahim A, Scott J. Community pharmacists in Khartoum State, Sudan: their current roles and perspectives on pharmaceutical care implementation. Int J Clin Pharmacy. 2013;35(2):236–243. doi:10.1007/s11096-012-9736-x
10. Helper CD, Strand LM. Opportunities and responsibilities in pharmaceutical care. Am J Hosp Pharm. 1990;47(3):533–543.
11. Schommer JC. The roles of pharmacists, patients, and contextual cues in pharmacist-patient communication. J Am Pharm Assoc. 1994;2:5845.
12. Ibrahim A, Scott J. Community pharmacists in Khartoum State, Sudan: their current roles and perspectives on pharmaceutical care implementation. Int J Clin Pharm. 2013;35(2):236–243.
13. Dahab AA, Ahmed EA, Elrahman YMA, Hamad FF, Ahmed OHAA, Abobakr. A. Improving Adherence to Prescribed Antidiabetics and Cardiovascular Medications in Primary Health Care Centers in Nyala City, South Darfur State-Sudan. BMC. 2013;1:58.
14. Brown CM, Barner JC, Shepherd M. Issues and barriers related to the provision of pharmaceutical care in community health centers and migrant health centers. J Am Pharmaceutical Assoc. 2003;43(1):75–77.
15. McDonough RP, Rovers JP, Currie JD, Hagel H, Vallandinghanl J, Sobotka J. Obstacles to the implementation of pharmaceutical care in the community setting. J Am Pharmaceutical Assoc. 1998;38(1):87–95.
16. Raosoft I. 2004. Available from: http://www.raosoft.com/.
17. Demissie F, Buno H, Paulos G. Assessment of Pharmaceutical Service Quality Provided in Community Drug Retail Outlets in Selected Towns, South West Ethiopia. Int Pharm Res Practice. 2022;117–126. doi:10.2147/IPRP.S375155
18. Spanakis M, Sfakianakis S, Kallergis G, Spanakis EG, Sakkalis V. PharmActa: personalized pharmaceutical care eHealth platform for patients and pharmacists. J Biomed Inform. 2019;100:103336. doi:10.1016/j.jbi.2019.103336
19. Oparah AC, Kikanme LC. Consumer satisfaction with community pharmacies in Warri, Nigeria. Res Soc Adm Pharmacy. 2006;2(4):499–511. doi:10.1016/j.sapharm.2006.02.004
20. Hammar T, Hamqvist S, Zetterholm M, Jokela P, Ferati M. Current Knowledge about Providing Drug–Drug Interaction Services for Patients—A Scoping Review. Pharmacy. 2021;9(2):69. doi:10.3390/pharmacy9020069
21. Farris KB, Fernandez-Llimos F, Benrimoj S. Pharmaceutical Care in Community Pharmacies: Practice and Research from Around the World. Vol. 39. Los Angeles, CA: SAGE Publications Sage CA; 2005:1539–1541.
22. Nazar H, Nazar Z, Portlock J, Todd A, Slight S. A systematic review of the role of community pharmacies in improving the transition from secondary to primary care. Br J Clin Pharmacol. 2015;80(5):936–948. doi:10.1111/bcp.12718
23. Mohamed SS, Mahmoud AA, Ali A. The role of Sudanese community pharmacists in patients’ self-care. Int J Clin Pharmacy. 2014;36(2):412–419. doi:10.1007/s11096-013-9911-8
24. Eades CE, Ferguson JS, O’Carroll RE. Public health in community pharmacy: a systematic review of pharmacist and consumer views. BMC Public Health. 2011;11(1):582. doi:10.1186/1471-2458-11-582
25. Hattingh HL, Emmerton L, Tin P, Green C. Utilization of community pharmacy space to enhance privacy: a qualitative study. Health Exp. 2016;19(5):1098–1110. doi:10.1111/hex.12401
26. Janke KK, Bloom TJ, Boyce EG, et al. A Pathway to Professional Identity Formation: report of the 2020-2021 AACP Student Affairs Standing Committee. Am J Pharm Educ. 2021;0002–9459.
27. Elvey R, Hassell K, Hall J. Who do you think you are? Pharmacists’ perceptions of their professional identity. Int J Pharm Practice. 2013;21(5):322–332. doi:10.1111/ijpp.12019
28. Noble C, Coombes I, Nissen L, Shaw PN, Clavarino A. Making the transition from pharmacy student to pharmacist: Australian interns’ perceptions of professional identity formation. Int J Pharmacy Practice. 2015;23(4):292–304. doi:10.1111/ijpp.12155
29. Costa FA, Scullin C, Al‐Taani G, et al. provision of pharmaceutical care by community pharmacists across Europe: is it developing and spreading? J Evaluation Clin Practice. 2017;23(6):1336–1347.
30. Floor-Schreudering A, De Smet PA, Buurma H, Egberts AC, Bouvy ML. Documentation Quality in Community Pharmacy: completeness of Electronic Patient Records After Patients’ First Visits. Ann Pharmacother. 2009;43(11):1787–1794. doi:10.1345/aph.1M242
31. Westfall GR, Narducci W. A Community-Pharmacy-Based Callback Program for Antibiotic Therapy: assessment of outcomes through the type of mechanism used in this study is a vital component of pharmaceutical care. J Am Pharm Assoc. 1997;37(3):330–334.
32. Deane FP, Kelly PJ, Crowe TP, Lyons GC. The feasibility of telephone follow-up interviews for monitoring treatment outcomes of Australian residential drug and alcohol treatment programs. Substance Abuse. 2014;35(1):21–29. doi:10.1080/08897077.2013.789815
33. Newman TV, San-Juan-Rodriguez A, Parekh N, et al. Impact of community pharmacist-led interventions in chronic disease management on clinical, utilization, and economic outcomes: an umbrella review. Res Soc Amp. 2020;16(9):1155–1165. doi:10.1016/j.sapharm.2019.12.016
34. Green BB, Cook AJ, Ralston JD, et al. Effectiveness of home blood pressure monitoring, Web communication, and pharmacist care on hypertension control: a randomized controlled trial. JAMA. 2008;299(24):2857–2867. doi:10.1001/jama.299.24.2857
35. Rovers JP. A Practical Guide to Pharmaceutical Care. Amer Pharmacists Assn; 2003.
36. Fathelrahman A. Medical Devices-Related Counseling Practices Among Community Pharmacists: a Nationwide Cross-Sectional Study from Saudi Arabia. Integrated Pharm ResAmp. 2021;10:113. doi:10.2147/IPRP.S310027
37. Zehnder S, Beutler M, Bruppacher R, Ehrenhöfer T, Hersberger KEJPW. Needs and use of drug information sources in community pharmacies: a questionnaire-based survey in German-speaking Switzerland. Science. 2004;26(4):197–202.
38. Semple SJ, Hotham E, Rao D, et al. Community pharmacists in Australia: barriers to information provision on complementary and alternative medicines. Pharm World Amp. 2006;28(6):366–373. doi:10.1007/s11096-006-9058-y
39. Ball DE, Al-Othman F. Drug information resources at private community pharmacies in Kuwait. Practice. 2007;16(2):107–109.
40. Al-Farsi SM, Al Rahbi HAM, Chime H. Information resources available at community pharmacies in Oman. J Phys Chem Lett. 2014;5(6):2320. doi:10.1021/jz501078s
41. Zehnder S, Beutler M, Bruppacher R, Ehrenhöfer T, Hersberger KE. Needs and use of drug information sources in community pharmacies: a questionnaire-based survey in German-speaking Switzerland. Pharm World Sci. 2004;26(4):197–202. doi:10.1023/B:PHAR.0000035881.17853.e0
42. Lee MP, Ray M. Planning for pharmaceutical care. Am J Hospital Pharm. 1993;50(6):1153–1158.
43. Eickhoff C, Schulz M. Pharmaceutical care in community pharmacies: practice and research in Germany. Ann Pharmacother. 2006;40(4):729–735. doi:10.1345/aph.1G458
44. Ponto J. ASHP statement on the pharmacist’s role in antimicrobial stewardship and infection prevention and control. Am J Health Syst Pharm. 2010;67(7):575–577.
45. Blake KB, Madhavan S. Perceived barriers to provision of medication therapy management services (MTMS) and the likelihood of a pharmacist working in a pharmacy that provides MTMS. Ann Pharmacother. 2010;44(3):424–431. doi:10.1345/aph.1M386
46. Montgomery AT, Kälvemark-Sporrong S, Henning M, Tully MP, Kettis-Lindblad A. Implementation of a pharmaceutical care service: prescriptionists’, pharmacists’, and doctors’ views. Science. 2007;29(6):593–602.
47. Shoji M, Onda M, Okada H, Sakane N, Nakayama T. The change in pharmacists’ attitude, confidence, and job satisfaction following participation in a novel hypertension support service. Int J Pharm Pract. 2019;27(6):520–527. doi:10.1111/ijpp.12550
48. Kovačević M, Ćulafić M, Jovanović M, Vučićević K, Kovačević SV, Miljković B. Impact of community pharmacists’ interventions on asthma self-management care. Res Soc Adm Pharm. 2018;14(6):603–611. doi:10.1016/j.sapharm.2017.07.007
49. Hijazi MA, Shatila H, El-Lakany A, Al Rifai H, Aboul-Ela M, Naja F. Role of community pharmacists in weight management: results of a national study in Lebanon. BMC. 2020;20(1):1–12.
50. Smith M. Pharmacists’ role in improving diabetes medication management. Technology. 2009;3(1):175–179.
51. Mishriky J, Stupans I, Chan VJPP. Expanding the role of Australian pharmacists in community pharmacies in chronic pain management-a narrative review. BMC. 2019;17(1):548.
52. Mohamed SS, Mahmoud AA, Ali AA. The role of Sudanese community pharmacists in patients’ self-care. Int J Clin Pharm. 2014;36(2):412–419.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.