Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Perspective: Acknowledging a Hierarchy of Social Needs in Diabetes Clinical Care and Prevention
Authors Howell CR ![]() , Harada CN, Fontaine KR
, Harada CN, Fontaine KR ![]() , Mugavero MJ, Cherrington AL
, Mugavero MJ, Cherrington AL
Received 9 September 2022
Accepted for publication 22 December 2022
Published 19 January 2023 Volume 2023:16 Pages 161—166
DOI https://doi.org/10.2147/DMSO.S389182
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Antonio Brunetti
Carrie R Howell,1 Caroline N Harada,2 Kevin R Fontaine,3 Michael J Mugavero,4 Andrea L Cherrington1
1Department of Medicine, Division of Preventive Medicine, University of Alabama at Birmingham, Birmingham, AL, USA; 2Department of Medicine, Division of Gerontology, Geriatrics, and Palliative Care, University of Alabama at Birmingham, Birmingham, AL, USA; 3Department of Health Behavior, School of Public Health, University of Alabama at Birmingham, Birmingham, Al, USA; 4Department of Medicine, Division of General Internal Medicine, University of Alabama at Birmingham, Birmingham, AL, USA
Correspondence: Carrie R Howell, Department of Medicine, Division of Preventive Medicine, Medical Towers Suite 638, 1717 11th Avenue South, Birmingham, AL, 35294, USA, Email [email protected]
Abstract: The evidence of suboptimal social determinants of health (SDoH) on poor health outcomes has resulted in widespread calls for research to identify ways to measure and address social needs to improve health outcomes and reduce disparities. While assessing SDoH has become increasingly important in diabetes care and prevention research, little guidance has been offered on how to address suboptimal determinants in diabetes-related clinical care, prevention efforts, medical education and research. Not surprisingly, many patients experience multiple social needs – some that are more urgent (housing) than others (transportation/resources), therefore the order in which these needs are addressed needs to be considered in the context of diabetes care/outcomes. Here we discuss how conceptualizing diabetes related health through the lens of Maslow’s hierarchy of needs has potential to help prioritize individual social needs that should be addressed to improve outcomes in the context of population-level determinants in the communities where people live.
Keywords: social determinants of health, diabetes, clinical care, clinical education
Introduction
T2DM disproportionately impacts racial and ethnic minorities1,2 and those with low socioeconomic status,1 with marked geographic variations in diabetes and obesity prevalence across the US.3 Growing evidence suggests that social determinants of health (SDoH) contribute to diabetes inequities. Social determinants of health (SDoH) are defined as the conditions in which people are born, grow, live, work and age;4 are responsible for a large proportion of health inequity worldwide;4 and account for substantial variability in health outcomes.5 SDoH related to diabetes are evident across multiple levels of influence, including individual, interpersonal, community and society6 and multiple domains such as socioeconomic status, neighborhood and physical environment, health care, and social context.7
Adults with sub-optimal SDoH such as lower overall socioeconomic status (SES),8 lower levels of income,1 limited education,9 and unemployment10 are more likely to have diabetes. Geographically, living in a non-metropolitan (eg rural) area has been associated with increased diabetes incidence11 while built environment and neighborhood level factors such as lack of physical activity resources, poor food options, and lower neighborhood SES have been linked to diabetes risk.12 Healthcare access, such as lacking insurance13 and geographic access to providers,14 as well as housing insecurity15 and homelessness16 are other SDoH associated with poor outcomes among those with diabetes, while investigations examining population measures of residential segregation have produced mixed results with diabetes outcomes17,18 and incidence.19
The evidence of suboptimal SDoH on poor health outcomes has resulted in widespread calls for research – such as those from the Institute of Medicine, World Health Organization, and the Affordable Care Act’s Center for Medicare and Medicaid Innovation – to identify ways to measure and address SDoH to improve health outcomes and reduce disparities. SDoH are attributes that affect all individuals on a continuum of optimal to suboptimal, are usually measured at a population level, such as census tract or census block group, and are influenced by money and resource distribution.7 Manifestations of suboptimal SDoH at the individual level – eg social risk factors – result in a social need that, if met, will likely improve health outcomes. While assessing SDoH has become increasingly important in diabetes care and prevention research, little guidance has been offered on how to address suboptimal determinants in diabetes-related clinical care, prevention efforts, medical education and research.20,21 Indeed, health systems and providers have traditionally been ill equipped to screen and address SDoH. However, the growing inclusion of social needs/SDoH screeners into the health system highlights the need for guidance on how to make these data actionable and multiple efforts are currently ongoing.22 Further, and not surprisingly, many patients experience multiple social needs20 – some that are more urgent (housing) than others (transportation/resources) – therefore the order in which these needs are addressed needs to be considered in the context of diabetes care/outcomes. Thus, conceptualizing diabetes related health through the lens of Maslow’s hierarchy of needs23 has the potential to help providers, administrators and researchers anchor, comprehend and prioritize individual social needs (eg SDoH, social risks) that should be addressed to improve outcomes in the context of population-level determinants in the communities where people live.24
Hierarchy of Diabetes Related Social Needs
A well-known theory of human motivation, Maslow’s hierarchy of needs23 suggests that humans are motivated to achieve basic needs, represented visually as a hierarchical pyramid with the bottom level consisting of physiological needs progressing to more complex needs at the top indicating fulfillment of individual potential (eg self-actualization). Originally, Maslow stated that needs at each level must be met in order to move on the next level; however, later work indicated that levels should be thought of as overlapping.25
Here we show (Figure 1) a conceptual hierarchy of diabetes related social needs derived using concepts from Maslow’s hierarchy,24 the Healthy People 2020 SDoH framework (5 key areas)26 and the Community Energy Balance Framework (multiple system levels of influence).27 This hierarchy follows the 5 levels of Maslow’s original pyramid: physiological, safety and security, belonging, esteem and actualization. We then categorize these social needs as being either at the individual/family system or the community/society system. Examples of SDoH are given for each hierarchy (rows in pyramid) and system level (columns in pyramid) and are not meant to be inclusive of all SDoH/social needs. In following the hierarchy, lower-level SDoH will take priority (in terms of an individual’s motivation towards diabetes health) over higher level SDoH with overlap between levels. For instance, an individual who is homeless should have their housing needs met at the physiological level before addressing higher level social needs such as securing employment (safety and security) and establishing social networks (belonging). Framing social needs in this way places emphasis on the fact that if basic needs (eg, food/shelter) are not being met, an individual cannot progress to higher levels (eg, developing and sustaining healthy behaviors, self-efficacy) in order to pursue optimal health. In terms of community and societal systems, neighborhoods that have less favorable attributes (eg lower SES, higher crime) are not able to “progress” to higher levels where social cohesion, social capital and less discrimination is perceived. This level in the framework is largely shaped by policy and systems and will require research and intervention efforts in this realm to achieve progress in outcomes as opposed to individual clinical care and research investigations. However, knowing where an individual falls in this hierarchy of community and society can give perspective to the lived experience of the patient and how this may influence their diabetes health in positive or negative ways.
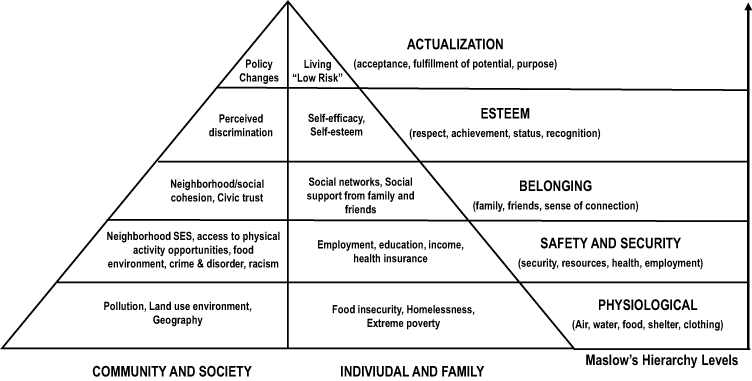 |
Figure 1 A social hierarchy of needs related to diabetes showing social needs as being either at the individual/family system or the community/society system. Examples of social determinants of health (SDoH) are given for each hierarchy (rows in pyramid) and system level (columns in pyramid) and are not meant to be inclusive of all social needs. In following the hierarchy, lower-level SDoH will take priority in terms of an individual’s motivation towards diabetes health over higher level SDoH. |
Implications for Clinical Care at the Individual Level
Maslow’s concepts of motivation lend well as a simple and familiar theoretical basis for healthcare providers working with patients who have social risks: basic social needs should be addressed, or at the very least acknowledged, in order for individuals to focus on their health and well-being. In fact, one study recently applied the concepts of Maslow’s hierarchy to formative work with patients with Type 1 diabetes to understand the multiple system of needs these patients experience.28
Unfortunately, social needs are often not addressed at the clinical encounter, despite the increase in social risk screeners and integration of SDoH into the electronic medical record. Presenting social needs/SDoH in this hierarchy provides a visual context/cue that most providers should be able to interpret and apply to their routine care of diabetes patients in several ways. First, is acknowledging where the patient falls within the hierarchy. This includes accessing available SDoH or risk screener data, both at the individual and neighborhood level, prior to or during the course of the medical encounter and talking with patients about their experiences and concerns.29 Second, is addressing social needs of the diabetes patient in the context of care by individualizing treatment plans as an interprofessional care team. This can include prioritizing health screenings, care coordination programs (eg community health workers), or referrals to resources such as food banks and transportation services.29,30 In fact, the ADA Standards of Care provide assessment and treatment considerations for patient’s experiencing certain social needs such as homelessness and food insecurity which can guide practitioners in tailoring care.31 Third, knowledge of the hierarchy of suboptimal SDoH that are influencing a diabetes patient can guide how clinicians counsel their patients on proper nutrition, engaging in physical activity and performing diabetes self-care. Patients lower on the hierarchy might benefit from additional services in order to be successful at engaging in healthy diabetes related behavior. For instance, patients may need diabetes health education materials adapted for low literacy; recommendations for home-based exercise programs if living in unsafe neighborhoods; or referral to transportation and food bank resources for food insecurity.32 On the other hand, diabetes patients in higher hierarchies might benefit more from behavioral interventions; access to social support networks; and traditional, structured weight loss programs. While this field is emerging, health services research that seeks to understand how to best embed SDoH approaches to diabetes clinical care are needed.
Implications for Population Health
The recent push for integration of SDoH measures and social risk screeners in the EMR has made it increasingly possible to use these data and indicators to identify groups at particularly high risk – both clinically and socially – for poor diabetes outcomes. Risk stratification and risk-based interventions have the potential to improve population level outcomes and reduce health disparities by delivering more intensive care to those at highest risk. Utilizing the hierarchy of social needs as a guide, health systems can compile aggregate individual and area level SDoH and social needs data to prioritize diabetes care and prevention efforts by social need level, thus allocating resources to fit the needs of their specific health system such as staffing for team-based care.30
Importantly, the hierarchy of social needs of diabetes serves as a visual reminder of how individual and population social needs are inextricably linked. Ultimately, results from successful efforts should provide data that can be used to inform systems and policy level changes as well as health improvement strategies in diabetes at the population level.
Implications for Research
Diabetes is dynamic, multifactorial, and complicated by an individual’s social context. Acknowledging a hierarchy of social needs in research planning (eg study design, targeted recruitment samples) and intervention design can help investigators understand the complex milieu in which an individual lives and how this interacts with diabetes health outcomes. In fact, one researcher applied Maslow’s hierarchy of needs to how individuals behaved during the COVID-19 pandemic and confirmed that individuals adhered to these levels of motivation.33 For instance, individuals risked their safety (exposure to the virus) to obtain food supplies but maintained their safety by forgoing social interactions.
This concept of physiological needs being met prior to safety needs should serve as a powerful reminder for diabetes researchers. It is likely that a proportion of individuals recruited into most research studies or epidemiological examinations are experiencing physiological needs that preclude them from being successful in either adherence or outcome improvement. Targeted recruitment and screening, as well as designing and testing interventions in individuals and populations across all levels, will provide much needed evidence to inform future research, population health efforts and policy decisions. Moreover, with growing emphasis on multilevel interventions, the proposed framework explicitly highlights the fundamental need to evaluate individual and family level SDoH attributes and interventions in the context of the community and societal determinants experienced by each individual research participant.
Implications for Clinical Education and Training
Importantly, the figure is a well-known model in the medical and psychology fields and has implications for clinical education and training. For instance, most medical school curricula are based on lists of topics or competencies, where all items seem to be of equal importance. Developing a curriculum based on a hierarchy could help guide the selection of components. Moreover, current training does not emphasize SDoH or social risks (eg not included in assigned readings or standardized testing) resulting in students having difficulty appreciating their relevance in medical care. This hierarchy visually reminds students that if you do not have food, it does not matter if you have scleroderma or interstitial nephritis or diabetes. Moreover, the hierarchy demonstrates how community factors are just as important as individual factors. Seeing SDoH as a hierarchy, with community-level and individual-level factors in parallel, would be useful in training. Lastly, most healthcare professionals are familiar with the distinct hierarchical pyramid, making the concept easy to grasp. This visualization is meant to provide a starting point to help frame how SDoH may be acknowledged or addressed in the context of diabetes outcomes and care.
Conclusion
While Maslow focused on the needs of individuals that should be met to achieve self-actualization, he also believed that society played a role in meeting the needs of individuals: optimal societies seek to satisfy the basic needs of its population and offers the opportunity of self-actualization. Here we highlight not only an individual’s hierarchy of social needs but also acknowledge the social needs in communities and society which may help guide diabetes related clinical care, research, training, policy and action. As diabetes related healthcare increasingly shifts towards a social needs lens, focusing on supporting individuals and policies at the appropriate hierarchies will provide opportunities for both people, communities, and society to advance towards “diabetes self-actualization” which should translate into better outcomes for all.
Funding
This work was supported by funding from the the National Institute on Minority Health and Health Disparities (Howell - 1K01 MD0172706). The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding agency supporting this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Beckles GL, Chou CF. Disparities in the prevalence of diagnosed diabetes - United States, 1999–2002 and 2011–2014. MMWR Morb Mortal Wkly Rep. 2016;65(45):1265–1269. doi:10.15585/mmwr.mm6545a4
2. Bullard KM, Cowie CC, Lessem SE, et al. Prevalence of diagnosed diabetes in adults by diabetes type - United States, 2016. MMWR Morb Mortal Wkly Rep. 2018;67(12):359–361. doi:10.15585/mmwr.mm6712a2
3. Thornton PL, Kumanyika SK, Gregg EW, et al. New research directions on disparities in obesity and type 2 diabetes. Ann N Y Acad Sci. 2020;1461(1):5–24. doi:10.1111/nyas.14270
4. World Health Organization. Closing the gap in a generation: health equity through action on the social determinants of health; 2020. Available from: http://www.who.int/social_determinants/thecommission/finalreport/en/index.html.
5. Forouzanfar MH, Alexander L, Anderson HR, et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386(10010):2287–2323. doi:10.1016/S0140-6736(15)00128-2
6. Alvidrez J, Castille D, Laude-Sharp M, Rosario A, Tabor D. The national institute on minority health and health disparities research framework. Am J Public Health. 2019;109(S1):S16–S20. doi:10.2105/ajph.2018.304883
7. Hill-Briggs F, Adler NE, Berkowitz SA, et al. Social determinants of health and diabetes: a scientific review. Diabetes Care. 2020. doi:10.2337/dci20-0053
8. Agardh E, Allebeck P, Hallqvist J, Moradi T, Sidorchuk A. Type 2 diabetes incidence and socio-economic position: a systematic review and meta-analysis. Int J Epidemiol. 2011;40(3):804–818. doi:10.1093/ije/dyr029
9. Borrell LN, Dallo FJ, White K. Education and diabetes in a racially and ethnically diverse population. Am J Public Health. 2006;96(9):1637–1642. doi:10.2105/AJPH.2005.072884
10. Varanka-Ruuska T, Rautio N, Lehtiniemi H, et al. The association of unemployment with glucose metabolism: a systematic review and meta-analysis. Int J Public Health. 2018;63(4):435–446. doi:10.1007/s00038-017-1040-z
11. Rural Health Information Hub. Diagnosed diabetes prevalence in metro and nonmetro counties, 2006–2017. Available from: https://www.ruralhealthinfo.org/charts/38.
12. Bilal U, Auchincloss AH, Diez-Roux AV. Neighborhood environments and diabetes risk and control. Curr Diab Rep. 2018;18(9):62. doi:10.1007/s11892-018-1032-2
13. Kazemian P, Shebl FM, McCann N, Walensky RP, Wexler DJ. Evaluation of the Cascade of Diabetes Care in the United States, 2005–2016. JAMA Intern Med. 2019;179(10):1376–1385. doi:10.1001/jamainternmed.2019.2396
14. Lu H, Holt JB, Cheng YJ, Zhang X, Onufrak S, Croft JB. Population-based geographic access to endocrinologists in the United States, 2012. BMC Health Serv Res. 2015;15:541. doi:10.1186/s12913-015-1185-5
15. Berkowitz SA, Kalkhoran S, Edwards ST, Essien UR, Baggett TP. Unstable housing and diabetes-related emergency department visits and hospitalization: a nationally representative study of safety-net clinic patients. Diabetes Care. 2018;41(5):933–939. doi:10.2337/dc17-1812
16. Axon RN, Gebregziabher M, Dismuke CE, et al. Differential impact of homelessness on glycemic control in veterans with type 2 diabetes mellitus. J Gen Intern Med. 2016;31(11):1331–1337. doi:10.1007/s11606-016-3786-z
17. Cummings DM, Patil SP, Long DL, et al. Does the association between hemoglobin A(1c) and risk of cardiovascular events vary by residential segregation? The Reasons for Geographic and Racial Differences in Stroke (REGARDS) study. Diabetes Care. 2021;44(5):1151–1158. doi:10.2337/dc20-1710
18. Kershaw KN, Pender AE. Racial/ethnic residential segregation, obesity, and diabetes mellitus. Curr Diab Rep. 2016;16(11):108. doi:10.1007/s11892-016-0800-0
19. Mayne SL, Loizzo L, Bancks MP, et al. Racial residential segregation, racial discrimination, and diabetes: the coronary artery risk development in young adults study. Health Place. 2020;62:102286. doi:10.1016/j.healthplace.2020.102286
20. Chambers EC, McAuliff KE, Heller CG, Fiori K, Hollingsworth N. Toward understanding social needs among primary care patients with uncontrolled diabetes. J Prim Care Community Health. 2021;12:2150132720985044. doi:10.1177/2150132720985044
21. Siegel KR, Gregg EW, Duru OK, et al. Time to start addressing (and not just describing) the social determinants of diabetes: results from the NEXT-D 2.0 network. BMJ Open Diabetes Res Care. 2021;9(Suppl 1). doi:10.1136/bmjdrc-2021-002524
22. Kreuter MW, Thompson T, McQueen A, Garg R. Addressing social needs in health care settings: evidence, challenges, and opportunities for public health. Annu Rev Public Health. 2021;42:329–344. doi:10.1146/annurev-publhealth-090419-102204
23. Maslow AH. Motivation and personality. In: Harper’s Psychological Series.
24. Jackson JC, Santoro MJ, Ely TM, et al. Improving patient care through the prism of psychology: application of Maslow’s hierarchy to sedation, delirium, and early mobility in the intensive care unit. J Crit Care. 2014;29(3):438–444. doi:10.1016/j.jcrc.2014.01.009
25. Maslow A, Lewis K. Maslow’s hierarchy of needs. Salenger Incorporated. 1987;14:987.
26. US Department of Health and Human Services. Healthy people 2020: social determinants of health. Available from: https://www.healthypeople.gov/2020/topics-objectives/topic/social-determinants-of-health.
27. Kumanyika S, Taylor WC, Grier SA, et al. Community energy balance: a framework for contextualizing cultural influences on high risk of obesity in ethnic minority populations. Prev Med. 2012;55(5):371–381. doi:10.1016/j.ypmed.2012.07.002
28. Beran D. Developing a hierarchy of needs for Type 1 diabetes. Diabet Med. 2014;31(1):61–67. doi:10.1111/dme.12284
29. Gottlieb L, Sandel M, Adler NE. Collecting and applying data on social determinants of health in health care settings. JAMA Intern Med. 2013;173(11):1017–1020. doi:10.1001/jamainternmed.2013.560
30. Gottlieb L, Tobey R, Cantor J, Hessler D, Adler NE. Integrating social and medical data to improve population health: opportunities and barriers. Health Aff. 2016;35(11):2116–2123. doi:10.1377/hlthaff.2016.0723
31. American Diabetes Association. Improving care and promoting health in populations: standards of medical care in diabetes—2021. Am Diabetes Assoc. 2021;44:S7–S14.
32. Haire-Joshu D, Hill-Briggs F. The next generation of diabetes translation: a path to health equity. Annu Rev Public Health. 2019;40:391–410. doi:10.1146/annurev-publhealth-040218-044158
33. Ryan BJ, Coppola D, Canyon DV, Brickhouse M, Swienton R. COVID-19 community stabilization and sustainability framework: an integration of the Maslow hierarchy of needs and social determinants of health. Disaster Med Public Health Prep. 2020;14(5):623–629. doi:10.1017/dmp.2020.109
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.