Back to Journals » Substance Abuse and Rehabilitation » Volume 17
Personalized Virtual Reality Future Selves Elicit Introspective Brain Activation in Early Substance Use Disorder Recovery
Authors Oberlin BG ![]() , Dzemidzic M, Shen YI, Nelson AJ
, Dzemidzic M, Shen YI, Nelson AJ
Received 9 February 2026
Accepted for publication 7 May 2026
Published 15 May 2026 Volume 2026:17 596437
DOI https://doi.org/10.2147/SAR.S596437
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rajendra Badgaiyan
Brandon G Oberlin,1– 4 Mario Dzemidzic,2,5 Yitong I Shen,1,3 Andrew J Nelson4
1Department of Psychiatry, Indiana University School of Medicine, Indianapolis, IN, USA; 2Department of Neurology, Indiana University School of Medicine, Indianapolis, IN, USA; 3Department of Psychology, Indiana University at Indianapolis, Indianapolis, IN, USA; 4Relate XR, LLC, Indianapolis, IN, USA; 5Department of Radiology and Imaging Sciences, Indiana University School of Medicine, Indianapolis, IN, USA
Correspondence: Brandon G Oberlin, Department of Psychiatry, Indiana University School of Medicine, 355 W 16th St Ste 4800, Indianapolis, IN, 46202, USA, Email [email protected]
Introduction: Substance use disorder (SUD) recovery typically requires transformative change and prioritizing long-term healthy goals. Unfortunately, successful recovery is threatened by relapse rates that typically exceed 50% in the first year. We previously reported on an experiential virtual reality (VR) SUD recovery intervention using personalized future self-avatars that produced emotional engagement and positive behavioral change, ie, stronger connection with the future self and future rewards, and reduced craving. Here, we used fMRI to identify brain engagement to a future self experience with divergent futures.
Methods: Twenty adults (14 males, 33 years old) in early SUD recovery (< 1 year) interacted with age-progressed versions of themselves in two different VR future “realities”: an SUD Future Self and a Recovery Future Self. Vivid lifelike visual and audio animation was augmented with a personalized narrative concerning future drug use and recovery. MRI immediately followed. Participants viewed videos of their future selves in the virtual environment and were directed to contemplate what they were seeing during MRI.
Results: Viewing and contemplating the future selves elicited activation in midline default mode regions (posterior cingulate and ventromedial prefrontal cortices), visual regions including the occipital and fusiform face areas, and left middle frontal gyrus. The Recovery Future Self produced significant left occipital face area activation compared with the SUD Future Self. Midline default mode activation correlated with VR-induced increases in delayed reward preference, and also with greater trait perseverance.
Discussion: Using digital selves as therapeutic agents reveals novel possible interventions and opens exciting new frontiers in behavior change methodology. Future studies targeting decision-making and future behavior could be informed by evaluating increased midline default mode engagement, with uniquely self-focused mechanisms signaled by executive network and face area coactivation. While preliminary, these data suggest promise for a range of new restorative experiences enabled by immersive digital therapeutics.
Plain Language Summary: High relapse rates in early substance use disorder recovery remains a serious challenge. To promote better outcomes, our team recently developed a virtual reality experience where people interacted with future versions of themselves. We used magnetic resonance imaging (MRI) to understand how the brain activated to this experience, and what brain responses were linked to relevant outcomes.
We worked with 20 adults in early recovery. Each person used a headset to experience immersive virtual reality and interact with two different future selves 15 years in the future: one who had returned to substance use, and one who had stayed in recovery. These digital future selves looked and sounded like the participants and were paired with a personalized story about future drug use and recovery. Right after the virtual reality session, participants were told to “think about what you see”, while they watched videos of these future selves and had their brains scanned.
When people viewed and reflected on their future selves, brain areas involved in self-reflection and imagining the future became activated, along with regions that process faces. The future selves triggered brain activation in “self-focused” brain networks and in face-processing regions. Activity in key “self-focused” brain regions was linked to choosing larger, delayed rewards over smaller, immediate ones, and to lower impulsivity.
These findings suggest that lifelike digital versions of people’s future selves engage brain systems that support thinking ahead, persistence, and valuing long-term outcomes, and that the degree of this heightened brain activity corresponds with behavior favoring a better future. This creates a promising new avenue for immersive digital therapeutic experiences to encourage lasting behavior change in early recovery from substance use disorder.
Keywords: SUD remission, addiction, therapeutic alliance, precision medicine
Introduction
Substance use disorder (SUD) is widely regarded as a chronic condition1 requiring effective long-term aftercare.2 Relapse occurs at high rates (50–90% within 6 months), even with evidence-based treatment,3–6 highlighting the urgent need for better treatment outcomes that include strong recovery support. Long-term outcomes are greatly improved by recovery support, up to doubling SUD remission in longitudinal follow-up years later.7 Emergent technologies show promise in improving SUD treatment aftercare, with virtual reality particularly attractive for its capacity to deliver highly salient personalized therapeutic experiences.
The ability to organize behavior for optimized future outcomes relies on the capacity for visualizing and identifying with possible futures and selves.8,9 When visualizing a personal future, those with SUD have shorter time horizons and less detailed imagined futures compared to controls.10–12 This impairment plausibly explains why those with SUD overly discount the value of delayed rewards13–15 and focus on the present rather than the future.16 Valuation of delayed rewards is directly linked to the degree of connection with the future self.17,18 Increasing the psychological connection to the future self with immersive digital simulations portraying future selves increases delayed reward preference19,20 and healthier behaviors.21 Construal-level theory22,23 predicts that making the abstract more concrete amplifies the salience of the future and, in the context of SUD remission, increases the attractiveness of recovery rewards and aversiveness of drug use. Therefore, immersive digital simulations using future selves could offer a practicable technique to promote adaptive, pro-recovery choices and healthier outcomes.
We created a highly personalized immersive virtual reality (VR) experience for participants in early SUD recovery that shows considerable promise.20 These vivid animated renderings of age-progressed selves narrated the events of two possible futures in their own voice. First traveling to the SUD Future, and then to the Recovery Future, participants experienced future selves who described profoundly divergent outcomes for the next 15 years. Face, body, voice, and content were tailored to enhance vividness—an important factor to increase prosocial behavior change.24 The spoken content was constructed from participants’ own stated costs and benefits, in the fashion of motivational interviewing.25 This experiential therapy integrated future self-continuity19,26 and self-discrepancy27,28 to increase salience and the psychological connection with future selves. Variations on the future self approach have been tested for reducing smoking29 and increasing exercise.21 Our VR experience was iteratively designed together with members of the local SUD recovery community and specifically intended to be emotional and transformative—echoing epiphany experiences often reported by those in recovery.30,31 While this intervention produced significant pro-recovery behavioral and self-reported improvements in a pilot study,20 the brain mechanisms governing these are unknown. Identifying brain areas that respond to the intervention and that correlate with key behavioral outcomes and traits can elucidate neurobiological mechanisms of action, informing target engagement and providing data for direct brain interventions (eg transcranial magnetic stimulation). Filling this knowledge gap is an important step toward advancing understanding of the brain basis of the broader category of future self-based approaches, a promising new therapeutic direction.
Brain activity related to the concept of “self” resides largely in cortical midline structures, especially the posterior cingulate cortex (PCC) and ventromedial prefrontal cortex (vmPFC).32 These central connectivity hubs33 comprise the medial components of the default mode network, a distributed resting-state network widely implicated in future-oriented and self-reflective thought, ie, prospection and introspection34,35 While initially described as deactivating during goal-directed tasks, considerable work now implicates the DMN, particularly in self-referential tasks such as autobiographical planning36–38 and imagining the future or past.39 Converging evidence suggests that the DMN integrates prior experiences, personal identity, simulations of the future, and action intent to create an internal narrative that guides behavior.40 We believe that maximizing brain responses to recovery messaging is best accomplished with potent narrative technique. Prior work demonstrates the power of VR to capture attention and elevate “presence” (the perception of being in a place).41 VR’s power to captivate is a function of sensory engagement,42,43 which mediates emotional outcomes,44 and surpasses non-immersive methods of narrative delivery.43,45
To best understand brain activation during an immersive VR experience, functional magnetic resonance imaging (fMRI) data would ideally be acquired during the VR experience. However, immersive VR using a head-mounted display is not readily deployed in MRI scanners, due to metallic components, and the serious limitations of presence and agency46 imposed by MRI-compliant immobility. However, we reasoned that a video from a recently experienced VR environment, containing VR self avatars, would be expected to elicit brain activity representing activation to the experience itself. We previously reported that our novel VR future self experience increased delayed reward preference and future self-continuity and decreased craving in early-recovering SUD participants.20 We hypothesize that viewing the future self during fMRI, immediately following an immersive VR experience with future selves, will increase activation in introspective and prospective brain regions, relative to the control condition. Specifically, we predict increased activation in posterior and anterior midline default mode regions, ie, the PCC and vmPFC to the future self We also hypothesize that this default mode activation will correlate with the recovery-related factors responding to the intervention—delayed reward preference, future self-continuity, and craving.20 We additionally performed exploratory correlations between brain responses and SUD-relevant traits and quality of life factors related to DSM-5 criteria for SUD diagnosis. Testing our a priori hypotheses and performing exploratory analyses can confirm or reveal regions and networks that are most relevant for this as well as other future self-based interventions. Specifically, our neuroimaging findings allow us to quantify the extent to which the three major networks (default mode, frontoparietal/central executive, salience)47 are implicated in early SUD recovery and addiction disorders, and further, to assess key differences in how different future selves engage the brain. Further, activation patterns will inform the general mechanism likely operating—that is, activation patterns in DMN would reflect a primarily introspective or prospective mechanism, whereas frontoparietal activation would suggest a more executive pathway. Other responses, such as in the amygdala or nucleus accumbens, would support a more affective or reward-related explanation, respectively.
Methods
Study Design Overview
Study procedures were as reported in Shen et al20 Briefly, participants were phone screened, interviewed in-person, and scheduled for a study day—avatars were constructed in the intervening time. On the study day, participants underwent VR habituation, personality and behavioral assessments (pre- and post-VR), the VR intervention, and fMRI. For 30 subsequent days, participants received daily smartphone reminders of their experience, “mRecovery”, and then provided longitudinal 30-day follow-up data. Study elements are illustrated in Figure 1, with the senior (first) author pictured as a participant.
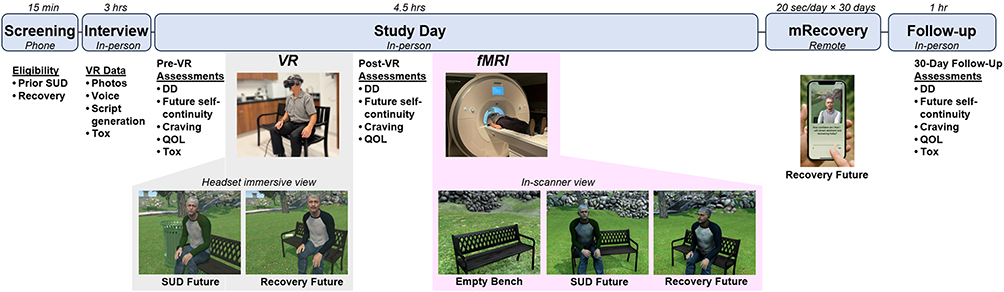 |
Figure 1 Study procedures. (Screening) initial eligibility confirmed. (Interview) detailed characteristics collected, including data required for creating personalized VR experiences. (Study Day) Prior to, and following the VR experience, participants performed tasks and assessments. The VR experience (gray background) comprised a brief habituation, then interaction with future selves. Following assessments, participants were scanned at 3T (pink background) while contemplating the virtual park and future selves shown. Views of videos displayed inside the VR headset and MRI head coil are shown in the lower level. See Figure 2 for a close-up view of the three avatars presented in the intervention. (mRecovery) daily images of the Recovery Future Self were sent to participants’ smartphones via MMS for 30 days. (Follow-up) Participants again completed assessments and self-reported drug/alcohol use. All in-person visits included toxicology screening (Tox); breath alcohol testing and urine screens. DD, delay discounting; QOL, quality of life survey. Approximate completion times shown above each study stage. |
Participants
Twenty participants were recruited from treatment centers and recovery houses in and around Indianapolis, Indiana, targeting adults in recovery from alcohol and/or substance use disorders (SUD). Initial eligibility was determined via phone screening (including demographics, substance use history, treatment history, medical conditions, and current medications) to determine initial eligibility, which was confirmed by detailed in-person interviews (below). Study inclusion criteria were as follows: in early SUD recovery, between 21 and 50 years old, English fluency, diagnosis, and treatment for use disorders of alcohol and/or illicit drugs, greater than 14 days abstinent from drug/alcohol use at the time of the study day (one participant with a single alcohol lapse 6 days prior to the study day was included), negative urine screen and breath alcohol results, and actively engaging in recovery activities. Early SUD recovery was defined as less than 1 year of continuous abstinence, in addition to a desire for an alcohol- and drug-free future. (NB: 15 out of 18 participants endorsed complete abstinence from alcohol and all illicit drugs, and three participants allowed for some future use under specific conditions: variously, use of marijuana if legalized, occasional drinking, and hallucinogens following 1 year of total abstinence). Note that for the purposes of this study, “SUD” refers to alcohol and illicit drug use disorders (excluding nicotine and caffeine), reflecting the concept and definition of “addiction” familiar to our research participants. While the DSM-5 recognizes nicotine and caffeine use disorders as SUD, these drugs are often viewed differently, and their use is generally tolerated or accepted by treatment programs and clients. Comorbid psychiatric conditions were permitted to maximize generalizability. Exclusions were contraindications for VR or MRI, current use of alcohol or illicit drugs, >1 lapse event between the interview and the study day, not self-identified as being “in recovery”, disorders or history of neurological disease of cerebral origin, head injury with > 20 min loss of consciousness, or left-handedness. Participants signed written informed consent documents and were compensated ($250 total) for study completion, which included the 30-day follow-up appointment. All recruiting and study procedures were approved by the Indiana University Institutional Review Board (IRB Protocol #1805574553), and the study complies with the Declaration of Helsinki. N=21 were reported in Shen et al20 but one of those participants was unable to complete MRI due to claustrophobia-related anxiety, resulting in the n=20 sample reported here. Two of these did not perform the delay discounting task at the follow-up due to Covid-19-related research restrictions. Participant characteristics are detailed in Table 1.
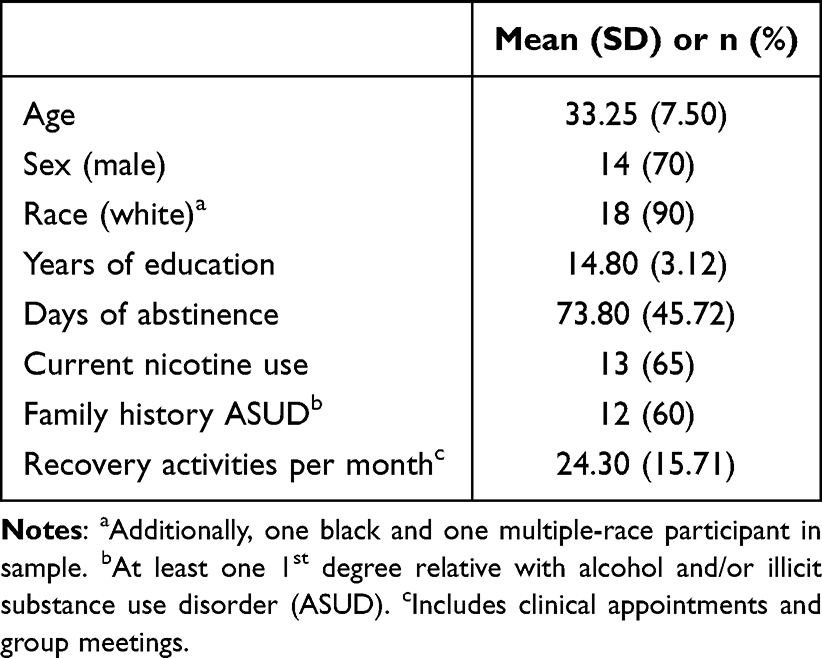 |
Table 1 Participant Characteristics (N = 20) |
Interview
The in-person interview comprised elaborated demographic information, nicotine use, family history of SUD, and quality of life survey. SUD symptom counts for alcohol and the three most-used substances were quantified with the SCID-5-RV48 structured clinical interview for DSM-5 disorders. The Timeline Follow-back (TLFB)49 characterized participants substance use patterns 35 days prior to treatment. Accuracy was enhanced with memorable event dates, past text messages, and any useful memory triggers. Alcohol and illicit drug use was characterized by type and amount, and SUD family history was quantified by degree of relatedness with probable SUD positive relatives. We also characterized current recovery-related activities, treatment history, and confidence in remaining abstinent. Participant-specific visual, audio, and content were collected for personalized avatar creation, detailed below.
Avatar and Script Generation
The avatars were constructed from studio-lit high-resolution photos (three face angles, two full-body angles, and close-ups of the eyes). Voice recording captured participants’ tonal quality, which was approximated with manual adjustment to Google’s text-to-speech engine. The phrasal template was personalized with information provided by the participant at the interview (names of loved ones, motivations for maintaining recovery, three specific costs and punishments of prior drug use, and three specific rewarding future goals, ie, “hopes and dreams”). The avatars were rendered three-dimensionally (Avatar SDK; https://avatarsdk.com/) with face aging features (custom texture and shader methods) and realistic eye movement and tracking (RandomEyes) implemented within an integrated VR environment (Unity 3D). The spoken script was synced with animated mouth and facial musculature. Some idiosyncratic features, primarily certain hairstyles and tattoos, required hand-editing to maximize personalization and realism. The two future selves were age-progressed to approximate 15 years into the future; this interval portrays sufficiently obvious visual markers of aging and is intermediate to delays commonly used in temporal discounting tasks.50 Close-up renditions of the first author were generated with the same methods to illustrate the visual differences between the avatars (Figure 2).
 |
Figure 2 Avatar renditions. Close view of avatars illustrating key visual aspects of aging and physical appearance outcomes. (A) The Present Self “guides” participants in Scene 1, the white room, and in Scene 4, the debrief. (B) The SUD Future Self represents 15 years of continued drug use, in appearance, posture, body language, and spoken content in Scene 2. (C) The Recovery Future Self embodies 15 years of sustained recovery, reflecting a healthier appearance, more satisfaction, and confidence in Scene 3. Social realism is maximized through avatars speaking to participants using an individually matched voice and precisely animated mouth movements and musculature; participants’ position is tracked with eye and head movement. |
Study Day Procedures
Urine screening (Wondfo Biotech, Ltd) and breathalyzer confirmed ongoing drug and alcohol abstinence, and participants were queried for ongoing self-identification with “recovery”. Daily nicotine users were provided an appropriately dosed nicotine patch (CVS Pharmacy, Inc.) per manufacturer’s recommendations to prevent withdrawal (unless refused, n=2). Vital signs were taken to confirm healthy state, and lack of MRI contraindications was confirmed.
Behavioral and Personality Assessments
Delay Discounting
An adjusting-amount delay discounting (DD) task quantified relative preference for delayed rewards.51,52 Choices between smaller immediate versus larger delayed monetary rewards adjusted the next trial’s immediate amount down or up, respectively, allowing the procedure to converge on indifference points for each delay. The $100 amount was delayed by 2 days, 1 week, 1 month, 6 months, 1 year, and 5 years in 30 choice trials (5 trials × 6 delays). Participants were instructed to choose according to their real preference, and that some choices would be selected at random and paid according to their choice. The actual payout was an additional $20 at the end of the study day, obfuscated by computer selection and rounding.
Future Self-Continuity
The validated future self-continuity scale indexes the perceived psychological distance to the imagined future self.18 Participants endorsed future self-similarity and connectedness with Euler circle pairs labeled “Current Self” and “Future Self” that vary in degree of overlap. We used the original scale with two minor modifications: an additional option depicting complete overlap;18,20 and an expanded temporal window of 15 years matching the age progression represented in the paradigm (the first four participants rated according to 10 years).
SUPPS-P Impulsive Behavior Scale
Derived from the original UPPS scale containing four subscales and 45 items,53 this shortened version comprises 20 items across five subscales (negative urgency, lack of perseverance, lack of premeditation, sensation seeking, and positive urgency) and is a reliable and valid low-burden alternative for assessing impulsivity traits.54
Zimbardo Time Perspective Inventory (ZTPI Short Form)
This shortened version of the original contains 22 items in two subscales that quantify time perspective, ie, orientation to the Future or Present.16
Quality of Life (QOL)
The QOL survey55 quantifies key aspects of subjective well-being that tend to improve in SUD remission.56 This 16-item scale is rated on a 7-point Likert-type scale ranging from “Delighted” (7) to “Terrible” (1) with increments labeled “Pleased”, “Mostly Satisfied”, “Mixed”, “Mostly Dissatisfied”, “Unhappy” in 16 items across 6 domains (well-being, relations with people, social/community activities, personal development, recreation, and independence).
VR Questionnaire
Participants rated the VR experience on elements of presence,57 tolerability, cybersickness, and enjoyment. Items and scores were previously reported in Shen et al.20
VR Delivery
VR was delivered on a Samsung Odyssey (6DoF, 90Hz, 2880×1600 pixels per-eye, 110° horizonal FoV) running on an Acer Predator laptop (Intel Core i7 CPU, Nvidia GeForce GTX 1060 GPU). VR experiences were conducted in a cleared laboratory space with a metal park bench, with the researcher closely supervising, managing the cables, and preventing stumbles or collisions. Interpupillary distance, headband tightness, and earphone placement were adjusted for each participant prior to beginning the experiences.
VR Habituation
Participants experienced the virtual park, without avatars, for 4.62 ±1.79 minutes. The city park was nearly identical to the environment used for the intervention, complete with chirping birds, rustling of leaves in a breeze, and distant lawn mowing noise. Participants were instructed to sit on the park bench, which was spatially registered to a real metal park bench. This habituation session was designed to reduce novelty effects and familiarize participants to the environment where the key messaging would be delivered.
VR Intervention
The VR paradigm featured personalized avatars representing the Present Self and age-progressed SUD Future Self, and Recovery Future Self. The intervention was designed to take ~5 minutes to complete, although in practice took 5.12 ±0.53 minutes due to inter-subject variation. The intervention comprised four scenes: (1) white room introduction with Present Self, (2) SUD Future Self scenario, (3) Recovery Future Self scenario, and (4) debriefing in a white room with the Present Self. In scene 1 (white room setting), a disembodied narrator explained that this would be a simulated time travel experience 15 years into the future. Participants were instructed to turn around and view themselves in a mirror and move their head and hands. The mirrored Present Self matched participants’ movements via tracked head and hand positions and inverse kinematics solving for ~30 seconds to establish “body transfer”.19,58 The Present Self then appeared as a non-playable character and gestured to the participant to sit on the park bench. The Present Self referred to the participant, “I am you” and shared personal details. The Present Self addressed the participant in the first scene using first person inclusive plural language (eg, “We enjoy…”, or “our main reason for…”), but upon advancing to the future—scenes 2 and 3—the future self used first person singular retrospective language (eg, “I always thought…”, “Life turned out better than I imagined…”). The use of inclusive plural first person language was designed to increase connection with the future self by semantically reducing psychological distance. Participants were then asked to “Choose your future” with two possible options. After choosing, the intervention transitioned into scene 2 (city park setting) where participants met their SUD Future Self. The SUD Future Self was unkempt, hunched forward, avoided eye contact, and discussed the past 15 years’ costs and punishments (from interview responses). The scene closed with the SUD Future Self saying, “don’t let this happen to us”. After a brief transportation back to the white room for a different choice (Present Self: “choose a different future”), participants were transported to the city park to meet the Recovery Future Self in scene 3. The Recovery Future Self was poised and presented as healthy and positive, with a vague smile and steady eye contact. The Recovery Future Self described the past 15 years in terms of success and achievement of future goals (“hopes and dreams”). Finally, in scene 4, participants were transported back to the white room where they were debriefed by the Present Self. These closing comments highlighted the contingency between present action and future outcomes, promoted agency, and offered positive encouragement with confidence. The shirt colors were blue and green for SUD and Recovery futures selves for visual emphasis of different futures (randomized).
Neuroimaging
MRI Acquisition
Imaging was conducted using a Siemens 3T Prisma MRI scanner (Erlangen, Germany) with a 32-channel head coil array. Structural imaging included T1-weighted MPRAGE (5 min 12 sec, 1.05×1.05×1.2 mm3 voxels) and was followed by a pair of 16-second phase-reversed spin echo scans to assess field distortion (5 A-P and 5 P-A phase direction volumes, repetition/echo time; TR/TE= 1370/51.60 ms, other parameters matched the BOLD scan parameters detailed below). The 13 min 51 sec virtual park video viewing scan used a multiband echo planar imaging (MB EPI) sequence from the Center for Magnetic Resonance Imaging at University of Minnesota (1018 blood oxygenation level dependent (BOLD) volumes, gradient echo, MB factor 4, TR/TE = 810/29 ms, 56° flip angle, 2.5 mm/side isotropic voxels, 220×220 mm2 field of view, 48 slices59). Prior to the park video viewing task, participants completed a resting-state scan with eyes fixated on a white crosshair on the black background (10 min 7 sec, other parameters as in the park video scan). Following the virtual park videos, a delay discounting task and diffusion-weighted imaging were administered (diffusion-weighted imaging data will be reported elsewhere).
Virtual Park Videos
Participants viewed videos of the three-dimensional park environment and avatars from the VR intervention. Three different videos (one with only the empty bench in the middle of the park, and two showing the animated future self avatars sitting on the bench in the park) were designed to engage the recent memory of the VR intervention. Each video was a single 3-minute camera shot comprised a left-to-right dolly movement focusing on the avatar (or empty bench) from a viewpoint 2 meters away (constructed in Timeline and exported using Unity Recorder). The avatars were shown sitting on the bench as though waiting, using the same posture, dress, and mannerisms programmed for the intervention. Avatars did not interact with or acknowledge the viewer. This video presentation was intended to evoke the recent VR experience and engage introspection, positioning the viewer as an unseen observer. Participants were instructed to “Think about the place and person shown”. The videos were presented in the following fixed order: Empty Park Pre, SUD Future Self, Recovery Future Self, and Empty Park Post. To facilitate return to cognitive baseline, 30-second still images of the same park view were positioned after the Future Self videos with 15-second stills positioned prior to and following the entire video block. In videos featuring the park bench and avatars, participants were instructed to button-press when a leaf fell behind the bench at fixed times (twice; 46 and 120 seconds from video start) to verify attentional engagement.
Neuroimaging Analyses
Preprocessing
Image preprocessing used FEAT (FMRI Expert Analysis Tool) Version 6.00, part of the FMRIB Software Library FSL,60 including BOLD volume geometric distortion correction with topup/applytopup that utilized distortion field estimates from the spin echo field mapping scans, motion correction with mcflirt, brain extraction with bet, registration to each participant’s T1-weighted image and MNI152 standard space with flirt and fnirt, and 6mm FWHM Gaussian filter spatial smoothing. Subsequently, BOLD data were presented to FSL’s MELODIC version 3.15 to automatically estimate and retain an optimal number of independent components for each scan61 and perform denoising with an unsupervised ICA-AROMA62 classifier. The resulting denoised data were assessed for residual head motion, transformed to a standard Montreal Neurological Institute (MNI) space, and interpolated to 2mm isotropic voxels for subsequent statistical analyses in SPM12.63
Within-Subject BOLD fMRI Models
Within-subject fixed effects of the BOLD response to each of the conditions (eg, videos listed in 62) were estimated in SPM12 using the canonical hemodynamic response function (HRF). Six head motion parameters from realignment served as multiple regressors. The residual temporal autocorrelation was removed using SPM’s FAST approach appropriate for short TR data, while high-pass filter (1/128 Hz) removed low-frequency noise.64
Mobile Health (mRecovery)
Daily texts displaying an image of the Recovery Future Self were sent to participants for 30 days. These were designed to elicit memory of the VR experience and invoke a positive future. Image viewing was verified with a single query (“how confident am I that I will remain abstinent today?”) that required a response on a 0–100% sliding scale (Qualtrics). The system was tested with participants on their smartphones just prior to discharge on the study day. Participants were familiarized with the system and informed of bonus incentives for compliance.
30-Day Follow-Up Procedures
Longitudinal follow-up appointments included urine drug screen, breath alcohol testing, and self-reported drug use (positive responses triggered TLFB interview to quantify use amount, frequency, and type). Delay discounting, future self-continuity, and QOL were assessed again. All responses to the mRecovery reminders were logged. The actual follow-ups occurred at 37 ±8.8 days due to scheduling variability; n=2 completed follow-up over phone due to Covid-19-related disruptions.
Power and Statistical Analysis
Planned Analyses
The study was powered for behavioral effects, with N=18 sufficient at power = 80% and alpha =0.05 (G*Power 3.1.9.7) based estimates from prior work,19 as previously reported.20 Planned analyses included random effects models of brain responses to avatars [Futures > Empty Park], and the inverse [Empty Park > Futures]. The empty park control contained all visual and audio elements of the experience except the future self avatar. Significant brain responses to futures were tested for associations with effects (behavioral and self-report) previously reported in Shen et al,20 ie, increased delayed reward preference, increased future self-continuity, and decreased craving. These were Δ%DD AUC, Δfuture self-similarity, and Δfuture self-connectedness, and Δcraving for pre-VR versus study day and pre-VR versus follow-up; 8 factors total. Alpha was set to 0.05 for all analyses. Significant clusters (functional regions of interest; fROIs) were tested for correlation with SUD recovery-specific outcomes, with false discovery rate set to <5%, ie, Benjamini–Hochberg;65 q<05 satisfied by p<0.00625 (8 tests) for each cluster. Means and standard deviations are reported as (M ±SD) in text and tables.
Exploratory Analyses
Exploratory correlations were performed with 13 potentially informative factors, where 7 related to SUD traits, and 6 to QOL aspects reflecting DSM criteria expected to improve in recovery. SUD trait-related factors were as follows: ZTPI Future, ZTPI Present, and 5 SUPPS subscales. Changes in QOL (delta between study day and 30 days later) were as follows: Health, Family, Love/Romance, Work, Social life, and Recreation. Exploratory analyses tested for associations with brain activation in 13 factors total. Significant clusters were tested for correlation, with false discovery rate q<0.05 satisfied by p<0.00385 (13 tests) for each cluster in exploratory analyses.
Statistical Models
This future visualization intervention was designed to increase delayed reward preference and future self-continuity by increasing focus on the future. We combined both futures (SUD and Recovery) together for analyses, as both represented plausible outcomes for people in early recovery. Both empty parks were combined for the control condition. A group-level random effects model was constructed from participant-level contrasts of virtual park videos to yield [Futures > Empty Park] and [Empty Park > Futures] contrasts in SPM12. Significant clusters were identified by meeting family-wise error correction pFWE < 0.05 at a cluster-forming threshold of puncorr <0.001 (corresponding cluster size k ≥ 108). To identify behavioral intervention responses correlating with brain activation, mean contrast values were extracted from each cluster (MarsBar toolbox; https://github.com/marsbar-toolbox/marsbar). Correlations between extracted values and key behavioral changes were tested in SPSS (v29; IBM). We performed exploratory correlations between 13 key SUD and QOL factors and both [Futures > Empty Park] and [Empty Park > Futures] contrasts. To examine if the two futures differed from each other, [SUD Future > Recovery Future] and [Recovery Future > SUD Future] were examined for differences within areas activated by any future thinking (ie, masked by [Futures > Empty Park]).
Results
Neuroimaging
fMRI activation and correlations are reported below. Behavioral and self-reported data were previously reported in Shen et al20 including sustained drug/alcohol abstinence at 30 days for 18 out of 21 participants.
Virtual Park Videos Whole-Brain Results
Videos of avatars sitting on the park bench (versus control) elicited activation primarily in midline and left lateral default mode network as well as visual attention areas. Seven significant clusters of activation in the [Futures > Empty Park] contrast were detected: posterior cingulate cortex, ventromedial prefrontal cortex (extending caudally into subgenual anterior cingulate), bilateral inferior occipital cortex (extending dorsally into left angular gyrus) that included occipital and fusiform face areas, left fusiform gyrus, left superior frontal gyrus, and left middle frontal gyrus, Figure 3. The opposite contrast [Empty Park > Futures], indicating deactivation, included bilateral lingual gyrus, supramarginal gyrus, precuneus, bilateral lateral temporal area (planum temporale), and right middle frontal gyrus; see Table 2 for details.
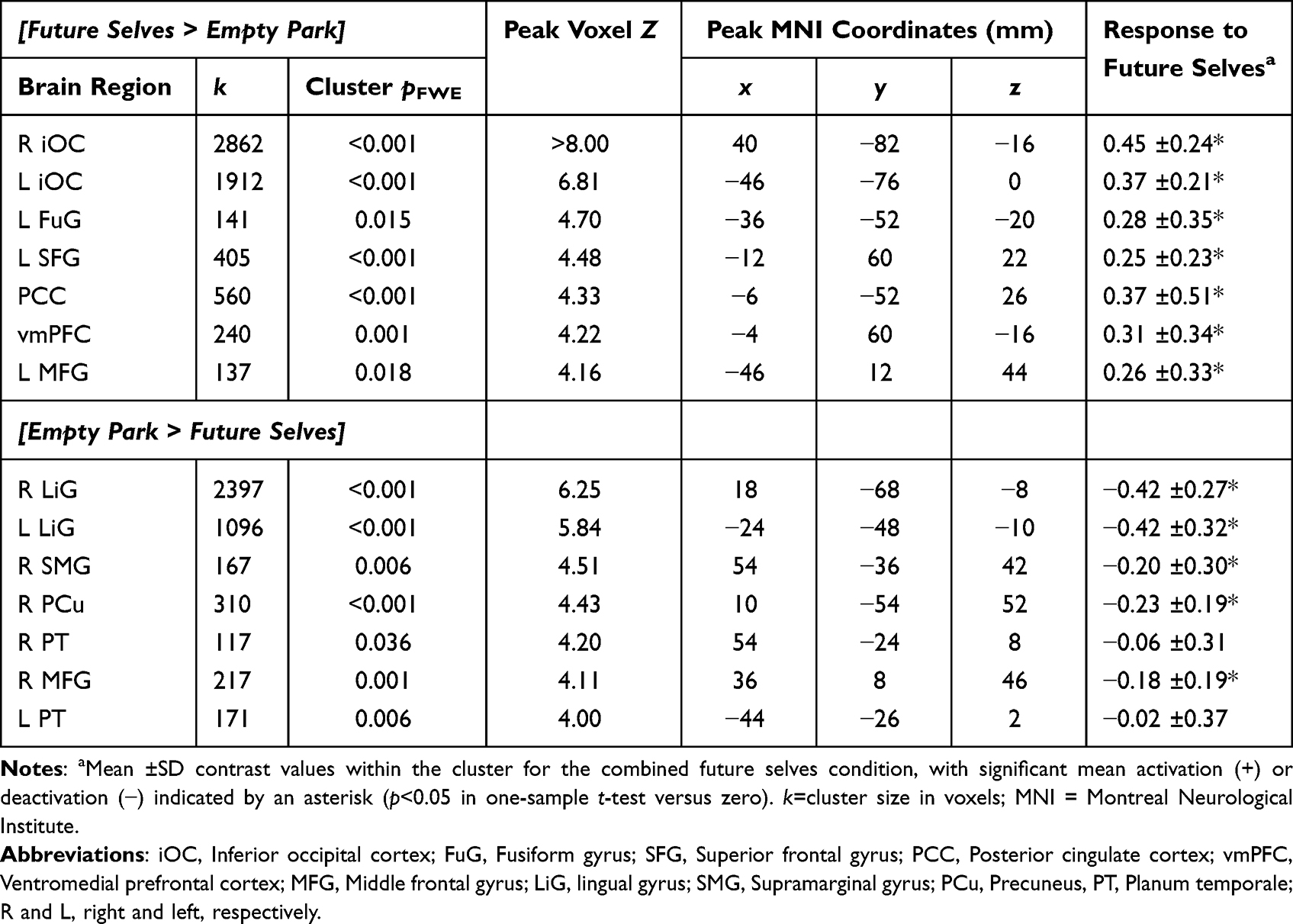 |
Table 2 Significant Clusters: Viewing Virtual Future Selves and Park |
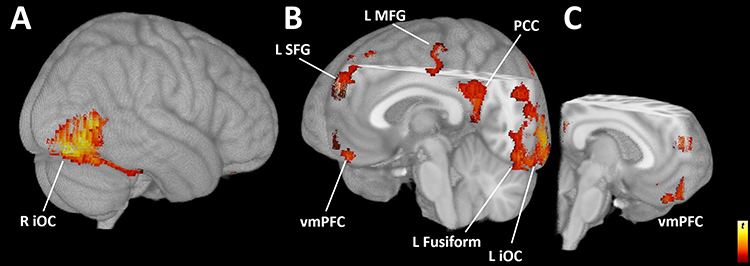 |
Figure 3 Activation during future self contemplation. Activation in the [Futures > Empty Park] contrast produced 7 significant clusters. (A) View from rear right illustrates the right inferior occipital cortex (R iOC); (B) the cutaway view from the left front shows the ventromedial prefrontal cortex (vmPFC), left superior frontal gyrus (L SFG), left middle frontal gyrus (L MFG), the posterior cingulate cortex (PCC), and left inferior occipital cortex (L iOC); (C) the cutaway complement further illustrates vmPFC, PCC, and SFG; displayed at puncorr<0.001, k>100. |
Activation Correlated with Recovery-Relevant Responses
Eight behavioral and psychological responses to the VR intervention20 were tested for correlation with mean contrast values from significant clusters from both [Futures > Empty Park] and [Empty Park > Futures]. The percent change in DD from pre-VR to the 30-day follow-up was correlated with activation to the future selves [Futures > Empty Park], in the posterior cingulate cortex r(16)=.644, p=0.004, q<0.05 and ventromedial prefrontal cortex r(16)=.621, p=0.006, q<0.05; Figure 4. No other significant results were detected in [Futures > Empty Park] contrast, and no significant correlations were detected in any regions from the [Empty Park > Futures] contrast. Post hoc analyses indicated that both future selves contributed to these effects; PCC, SUD r(16)=.72, p<0.001, Recovery r(16)=.44, p=0.066; vmPFC SUD r(16)=.58, p=0.012, Recovery r(16)=.54, p=0.021.
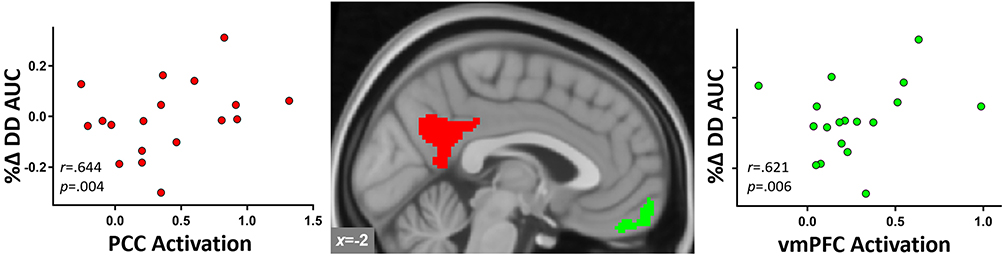 |
Figure 4 Brain responses to futures correlated with increased delayed reward preference. [Futures > Empty Park] activation (mean contrast values) in posterior and anterior medial default mode regions (center). Activation in the (left) posterior cingulate (red), and (right) ventromedial prefrontal cortex (green) correlated with changes in delay discounting (AUC; area under the curve) from pre-VR to the 30-day follow-up, qs<0.05. |
Exploratory Correlations with SUD Traits and QOL Changes
Activation in the posterior cingulate cortex cluster correlated with greater perserverence; that is, negatively with UPPS Lack of Perseverance r(18)=−.636, p=0.003, q<0.05; Figure 5, as measured in the UPPS inventory. No other significant results were detected in [Futures > Empty Park] contrast, and no significant correlations were detected in any regions from the [Empty Park > Futures] contrast.
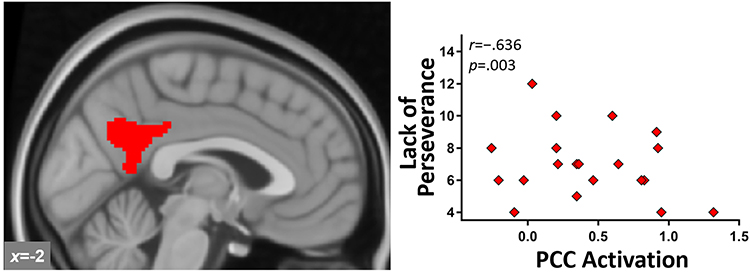 |
Figure 5 Posterior cingulate activation and impulsivity. [Futures > Empty Park] activation in posterior cingulate cortex (left) negatively correlated with the UPPS Lack of Perseverance trait impulsivity measure (right), q<0.05. |
Recovery and SUD Futures
Significant activation was detected in the [Recovery Future > SUD Future] in the inferior occipital cortex (occipital face area), Figure 6, but no activation was detected in the opposite contrast [SUD Future > Recovery Future].
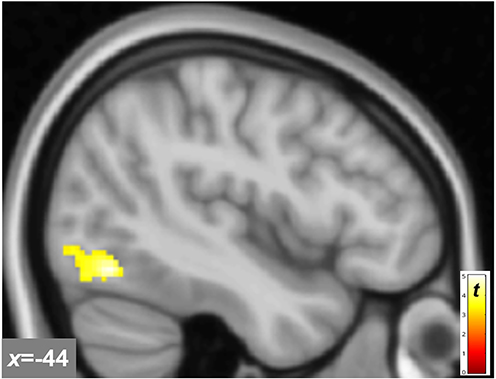 |
Figure 6 Brain activation to recovery future. [Recovery Future > SUD Future] elicited significant activation in the occipital face area of the left inferior occipital cortex. |
Discussion
We previously demonstrated that interactions with age-progressed selves in an SUD or recovery future increased connection with the future self, increased valuation of future rewards, and reduced craving.20 To ascertain what brain systems were engaged by the VR experience, we presented a video of the future selves in the same virtual park during fMRI. This was designed to evoke the same prospective and introspective processing that occurred during the immersive VR experience. Brain activation to the future selves was largely concentrated in default mode and visual attention regions. The activation to future selves in midline default mode (PCC and vmPFC) correlated with increased valuation of delayed rewards. Further, PCC activation to the future selves correlated with greater perseverance (trait impulsivity subscale). While activation between the SUD Future Self and Recovery Future Self mostly overlapped, greater activation to the Recovery Future Self was detected in the inferior occipital cortex, indicating engagement of visual attention and associative processes specific to the recovery future. These findings suggest that this novel intervention recruits default mode network activity, and that this inwardly focused cognition shifts behavioral preference toward the future.
The visual scene presented during fMRI was designed to project attention into imagined and “pre-experienced” futures, ie, by simultaneously eliciting autobiographical mental time travel, perspective-taking, introspection, and prospection. The intervention engages four major modes of prospection: simulation, prediction, intention, and planning.66 A large body of work supports the central role of the DMN in these internally generated processes, ie, stimulus-independent thought34,35,40,67 In our study, these internal states are induced by visual stimuli, which include the age-progressed self (future self avatars) and the environmental context representing the non-self future (city park), ie, other aspects of the future minus the future self. Tasks such as mental time travel, mental simulation, and scene construction recruit DMN regions in these prospective and introspective processes,68–71 with particular focus on the self.72 Activation to future selves in the current study reflects activity in the central hubs of the DMN; the PCC and vmPFC33,73 supporting the DMN’s role in animating a deep internal narrative. While cognitive processes engaged by “thinking about what you see” (instructions provided to participants for viewing the empty park bench or future selves during MRI) are technically unknowable, we infer that participants contemplated their personal futures, as they were immersed in an experience with future selves in the same visual environment just an hour earlier.
The VR intervention is designed to induce mental projection into the future that is both semantic (general) and episodic (specific). That is, participants interact with two semantic future selves that have lived according to divergent general strategies—one continuing to misuse drugs, and the other engaged in recovery. The episodic elements narrated by the future selves are events such as drunk driving accident (SUD future) or becoming a homeowner (recovery future). The park + avatar video during fMRI evokes the VR future simulation (albeit without avatar interaction) in a manner designed to induce contemplation. The semantic aspects are presumably linked to mind wandering, and therefore DMN activation, but the combined episodic elements might be expected to engage brain areas linked to intention and planning, ie, frontoparietal network. Converging evidence suggests that when planning is mixed with introspection (as in the current study), default mode systems co-activate with networks mediating goal-directed behavior, particularly the frontoparietal network. Prior work demonstrated that autobiographical planning produced correlated DMN and frontoparietal network activity, whereas a simple visuospatial planning task did not.36 Other research examining the preparatory phase of verbal working memory execution indicates DMN coactivation with frontoparietal and inferior occipital cortex, ie, visual attention and association networks.74 Consistent with executive engagement, our findings in the left MFG (dorsal aspect) and left iOC (angular gyrus extent) overlap with the frontoparietal network,73 demonstrating at least left-lateralized frontoparietal coactivation. Contemplating a primed personal future after an immersive VR experience (containing both semantic and episodic elements) activates introspective default mode and executive frontoparietal network regions simultaneously. Future permutations of the intervention could target semantic or episodic aspects differentially, to maximize introspection or prospection, respectively. This would be presumed to favor DMN or frontoparietal activity in either case, and one could imagine a precision medicine approach delivering a personality (or neuroimaging)-based experience tuned to specific patient needs potentially yielding stronger results than a unitary experience.
The degree of midline default mode activation to future selves appeared to index capacity for increasing delayed reward preference. Discounting of delayed rewards decreased after the intervention, suggesting that the future self VR experience shifted attention and preference toward future rewards. Prior work indicates that the key regions responsible for performing delay discounting tasks are largely localized to the default mode, frontoparietal, and salience (resting state-defined) networks,75–79 which are implicated in psychopathology more generally (the “triple network model”).80 While delay discounting is a complex decision task that recruits various brain regions to execute, the brain regions that respond specifically to interventions that increase delayed reward preference fall largely within the midline default mode regions PCC and vmPFC.81,82 Moreover, the self-referential “cortical midline system”, which is deeply involved with the self, familiarity, and making self/other distinctions,32,67,72,83 comprises the midline components of the default mode network. In the current work, PCC activation to the future selves correlated with lower trait impulsivity (lack of perseveration), suggesting a possible trait-level influence. Prior meta-analytic work indicates that posterior midline DMN (PCC/precuneus) responds acutely to interventions to increase delayed reward preference,81 PCC connectivity differentiates alcohol use disorder (AUD) from controls,84 posterior midline DMN within-network connectivity was greater in AUD than control and impulsivity negatively correlated with posterior midline DMN and vmPFC connectivity85 —together these data suggest a link between impulsive choice, PCC function, and trait impulsivity in SUD. The present data combined with prior demonstrations of the functional relationship between the PCC and vmPFC with self-focused thinking, prospection, and augmented delayed reward preference advances a mechanistic explanation: making the future self more real and “tangible” increases prospective brain activation and shifts preference towards future rewards.
Activation specifically to the Recovery Future Self, relative to the SUD Future Self, was localized in the occipital face area, outside the default mode network. The occipital face area integrates visual face perception86 with episodic and semantic information87,88 as part of the larger visual ventral stream (a brain system that derives object identity from raw visual information)89,90 In concert with the adjacent fusiform face area and lateral occipital cortex, the occipital face area comprises key nodes in the core early face-processing network.91,92 Beyond semantic information linked to face identity, this region also responds to episodic recall.39 Further, functional connectivity with this location and lateral prefrontal cortex in episodic simulation93 or with joint default mode and frontoparietal activation to mental simulation94 indicates its role in visual scene construction. Given that the Recovery Future Self delivered specific verbal messaging about a particular future, this information is presumably encoded with the visual information, linking this specific face to a panoply of semantic details about an imagined future—one in which recovery from addiction has provided considerable benefit compared with the alternative. While it is perhaps surprising that two future selves representing diametrically opposed futures yielded very similar brain activation, there are likely important differences at the individual level that may be difficult to isolate in a limited sample. Anecdotally, participants appeared to be moved by one or the other future variously, and this appeared to be at least partly personality dependent. Future efforts will characterize this tendency and examine corresponding brain activation to mark efficacy or as a personalized medicine approach. In most cases, participants “bought in” to the narrative, focusing on the emotional and contemplative aspects of the experience (see Supplemental in Shen et al20 for transcribed participant feedback).
Identifying key brain regions to mark successful SUD recovery is not as straightforward as might be presumed. Most prior work attempting to answer this question used drug cue reactivity paradigms to mark success or failure; however, the utility of this approach may be limited to identifying regions rather than clear directional interpretations. That is, greater brain activation to drug cues could reflect either drug reward drive (implying greater risk) or active resistance to temptation, ie, recovery reward drive and abstinence-related payoffs (suggesting lower risk). One or the other interpretation may be favored by particular paradigms or even vary between individuals. Nonetheless, considerable prior work implicates midline default regions PCC and vmPFC in predicting abstinence in early recovery. PCC activation to visual cocaine cues correlated with worse treatment outcomes and differentiated abstainers from relapsers.95 During an executive functioning task, PCC activation was a predictor of relapse in the comparison of smoking satiety versus short-term abstinence.96 As the PCC is a structural and functional rich club,97 its central role in connectivity might be the most informative. Broadly, greater PCC connectivity with other networks and within the default mode network tends to be associated with better SUD treatment outcomes.98 Activation in the anterior aspect of the midline default mode network, ie, the vmPFC, predicts abstinence-related outcomes, but with mixed directionality Using visual alcohol cues, activation in the vmPFC correlated with craving and time to first relapse,99 whereas greater activation to neutral relaxing cues predicted relapse to alcohol.100,101 However, greater vmPFC responsivity to visual heroin cues predicted better treatment adherence.102 Beyond the default mode network, left-lateralized frontoparietal (EEG) connectivity between the dlPFC and posterior parietal cortex differentiated early recovering AUD sustaining abstinence versus those who relapsed.103 This pattern of frontoparietal connectivity resembles the left-lateralized frontoparietal and midline default mode coactivation observed in the present report. Together, the regions and networks showing activation and behavioral correlation reported here map onto key regions that predict relapse and may underly recovery-related brain function.
Limitations
Some limitations should be acknowledged. While significant findings in this modest sample are promising104 and informed the approach (a larger ongoing randomized controlled trial based on these methods), results in a larger sample would enhance generalizability and confidence. We detected main effects and correlations of activations to future selves relative to the control condition in early recovery SUD, but we cannot extrapolate these findings to non-treatment seeking individuals or healthy controls. Main effects of activation to a personal future were identified, insofar as the virtual park video viewing reflected brain activation to the VR experience. As fMRI was performed within an hour of the VR experience, and the park viewing was a video of the same 3D environment (and avatars), this is presumably a reasonable assumption. The current study design does not resolve the possibility that observed effects were driven, at least in part, by individual differences in emotional lability, ie, that highly arousable participants could respond more to any intervention, both in brain and behavior. While one might speculate that the ideal control condition for detecting activation to a future self would be the Present Self, recall that the VR experience never showed the Present Self in the virtual park. That is, the Present Self was never associated with the virtual park. Thus, to best capture the effect of the future selves—the putative active ingredient of this experiential therapy—the proper control is the park without either future self in the visual field. Another limitation is the use of a fixed order during imaging, which potentially limited the capacity to detect differences between the two futures. The fixed order reflected the VR presentation order, which was fixed for clinical reasons (recency effect favoring the optimistic future was designed to lower the psychological danger potentially caused by the SUD future self). A larger sample with only one future self in a between-subjects design could resolve this issue. VR development necessarily limited subject numbers, precluding this approach in this study. One final consideration is the possibility that the spoken content alone—the personalized events for the SUD future and Recovery future—might elicit similar DMN activation as observed here when delivered by future self avatars, although we expect that the effect would be less pronounced than fully immersive content delivery. Future studies are warranted to evaluate this possibility.
Conclusion
VR permits bringing experiential therapies to life and implementing them in the clinic. We demonstrated that an autobiographical future simulation elicits positive pro-recovery effects (reduced impulsive choice and craving and increased identification with the personal future, along with low rates of relapse). This intervention produces semantic (introspective, contemplative) midline DMN and episodic (prospective, executive planning) frontoparietal coactivation while evoking general and specific SUD recovery elements. Our current report on brain engagement suggests that introspective and executive brain networks are involved with this reoriented future-focus, which corresponds with positive behavioral changes. The nascent digital therapeutic space is replete with new possibilities, allowing emerging technology to augment existing evidence-based techniques.
Acknowledgments
We are grateful to Dr. Elizabeth Lungwitz, research MRI personnel of the Research Imaging Core in the Medical Imaging Research Institute, Department of Radiology and Imaging Sciences, Dr. Yu-Chien Wu, Michele Dragoo, Traci Day, and Robert Bryant for excellent technical assistance. We additionally thank the anonymous reviewers and editors for their insightful comments. An initial draft of this manuscript was uploaded to MedRxiv as a preprint: https://www.medrxiv.org/content/10.64898/2026.01.23.26344667v1.
Funding
This study was funded by the Indiana Clinical and Translational Sciences Institute Project Development Team (PRMC UL1TR001108) and the Indiana University Department of Psychiatry. These sponsors had no role in the study design or manuscript publication.
Disclosure
BGO and AJN are co-founders of Relate XR, LLC, and inventors on a patent awarded to Indiana University on technology described in this manuscript: “AVATAR-BASED BEHAVIOR CHANGING SYSTEM AND METHOD” US 12,406,421 B2, issued 9/2/2025. The authors report no other conflicts of interest in this work.
References
1. NIDA. What is drug addiction? Available from: https://nida.nih.gov/publications/drugs-brains-behavior-science-addiction/drug-misuse-addiction#ref.
2. ASAM. The ASAM standards of care for the addiction specialist physician; 2014. Available from:https://downloads.asam.org/sitefinity-production-blobs/practice-support/asam-standards-of-care_81caf74b-f259-4f2a-82ea-8b27f3335a14.pdf?sfvrsn=338068c2_0.
3. Weiss RD, Potter JS, Fiellin DA, et al. Adjunctive counseling during brief and extended buprenorphine-naloxone treatment for prescription opioid dependence: a 2-phase randomized controlled trial. Arch Gen Psychiatry. 2011;68(12):1238–18. doi:10.1001/archgenpsychiatry.2011.121
4. Brecht M-L, Herbeck D. Time to relapse following treatment for methamphetamine use: a long-term perspective on patterns and predictors. Drug Alcohol Depend. 2014;139:18–25. doi:10.1016/j.drugalcdep.2014.02.702
5. Brecht M-L, Anglin MD, Dylan M. Coerced treatment for methamphetamine abuse: differential patient characteristics and outcomes. Am J Drug Alcohol Abuse. 2005;31(2):337–356. doi:10.1081/ADA-56764
6. Moeeni M, Razaghi EM, Ponnet K, Torabi F, Shafiee SA, Pashaei T. Predictors of time to relapse in amphetamine-type substance users in the matrix treatment program in Iran: a Cox proportional hazard model application. BMC Psychiatry. 2016;16(1):265. doi:10.1186/s12888-016-0973-8
7. Chi FW, Parthasarathy S, Mertens JR, Weisner CM. Continuing care and long-term substance use outcomes in managed care: early evidence for a primary care-based model. Psychiatric Serv. 2011;62(10):1194–1200. doi:10.1176/ps.62.10.pss6210_1194
8. Markus H, Nurius P. Possible selves. Am Psychologist. 1986;41(9):954. doi:10.1037/0003-066X.41.9.954
9. Bixter MT, McMichael SL, Bunker CJ, et al. A test of a triadic conceptualization of future self-identification. PLoS One. 2020;15(11):e0242504. doi:10.1371/journal.pone.0242504
10. Manganiello JA. Opiate addiction: a study identifying three systematically related psychological correlates. Int J Addict. 1978;13(5):839–847. doi:10.3109/10826087809039307
11. Petry NM, Bickel WK, Arnett M. Shortened time horizons and insensitivity to future consequences in heroin addicts. Addiction. 1998;93(5):729–738. doi:10.1046/j.1360-0443.1998.9357298.x
12. Mercuri K, Terrett G, Henry JD, Bailey PE, Curran HV, Rendell PG. Episodic foresight deficits in long-term opiate users. Psychopharmacology. 2015;232(7):1337–1345. doi:10.1007/s00213-014-3772-2
13. Amlung M, Marsden E, Holshausen K, et al. Delay discounting as a transdiagnostic process in psychiatric disorders: a meta-analysis. JAMA Psychiatry. 2019;76(11):1176. doi:10.1001/jamapsychiatry.2019.2102
14. Amlung M, Vedelago L, Acker J, Balodis I, MacKillop J. Steep delay discounting and addictive behavior: a meta-analysis of continuous associations. Addiction. 2017;112(1):51–62. doi:10.1111/add.13535
15. MacKillop J, Amlung MT, Few LR, Ray LA, Sweet LH, Munafo MR. Delayed reward discounting and addictive behavior: a meta-analysis. Psychopharmacology. 2011;216(3):305–321. doi:10.1007/s00213-011-2229-0
16. Keough KA, Zimbardo PG, Boyd JN. Who’s smoking, drinking, and using drugs? Time perspective as a predictor of substance use. Basic Appl Soc Psychol. 1999;21(2):149–164. doi:10.1207/S15324834BA210207
17. Bartels DM, Rips LJ. Psychological connectedness and intertemporal choice. J Exp Psychol. 2010;139(1):49. doi:10.1037/a0018062
18. Ersner-Hershfield H, Garton MT, Ballard K, Samanez-Larkin GR, Knutson B. Don’t stop thinking about tomorrow: individual differences in future self-continuity account for saving. Judgm Decis Mak. 2009;4(4):280–286. doi:10.1017/S1930297500003855
19. Hershfield HE, Goldstein DG, Sharpe WF, et al. Increasing saving behavior through age-progressed renderings of the future self. J Mark Res. 2011;48:S23–S37. doi:10.1509/jmkr.48.SPL.S23
20. Shen YI, Nelson AJ, Oberlin BG. Virtual reality intervention effects on future self-continuity and delayed reward preference in substance use disorder recovery: pilot study results. Discov Ment Health. 2022;2(1):19. doi:10.1007/s44192-022-00022-1
21. Fox J, Bailenson JN. Virtual self-modeling: the effects of vicarious reinforcement and identification on exercise behaviors. Media Psychol. 2009;12(1):1–25. doi:10.1080/15213260802669474
22. Trope Y, Liberman N. Construal-level theory of psychological distance. Psychol Rev. 2010;117(2):440. doi:10.1037/a0018963
23. Mishra AN, Raj A, Pani AK. Construal level research in decision making: analysis and pushing forward the debate using bibliometric review and thematic analysis. Mishra Arindra N. 2020;2020:106–135.
24. Van Gelder JL, Luciano EC, Weulen Kranenbarg M, Hershfield HE. Friends with my future self: longitudinal vividness intervention reduces delinquency. Criminology. 2015;53(2):158–179. doi:10.1111/1745-9125.12064
25. Bischof G, Bischof A, Rumpf H-J. Motivational interviewing: an evidence-based approach for use in medical practice. Dtsch Arztebl Int. 2021;118(7):109. doi:10.3238/arztebl.m2021.0014
26. Hershfield HE. Future self-continuity: how conceptions of the future self transform intertemporal choice. Ann N Y Acad Sci. 2011;1235(1):30. doi:10.1111/j.1749-6632.2011.06201.x
27. Ogilvie DM. The undesired self: a neglected variable in personality research. J Person Soc Psycholo. 1987;52(2):379. doi:10.1037/0022-3514.52.2.379
28. Paternoster R, Bushway S. Desistance and the “feared self”: toward an identity theory of criminal desistance. J Crim Law Criminol. 2009;2009:1103–1156.
29. Şenel G, Slater M. Conversation with Your Future Self About Nicotine Dependence. Springer; 2020:216–223.
30. Galanter M, Dermatis H, Santucci C. Young people in alcoholics anonymous: the role of spiritual orientation and AA member affiliation. J Addict Dis. 2012;31(2):173–182. doi:10.1080/10550887.2012.665693
31. Lawford CK. Moments of Clarity: Voices From the Front Lines of Addiction and Recovery. Harper Collins; 2009.
32. Northoff G. Personal identity and cortical midline structure (CMS): do temporal features of CMS neural activity transform into “self-continuity”? Psychol Inq. 2017;28(2–3):122–131. doi:10.1080/1047840X.2017.1337396
33. Tomasi D, Wang R, Wang G-J, Volkow ND. Functional connectivity and brain activation: a synergistic approach. Cereb Cortex. 2014;24(10):2619–2629. doi:10.1093/cercor/bht119
34. Andrews-Hanna JR. The brain’s default network and its adaptive role in internal mentation. Neuroscientist. 2012;18(3):251–270. doi:10.1177/1073858411403316
35. Spreng RN, Grady CL. Patterns of brain activity supporting autobiographical memory, prospection, and theory of mind, and their relationship to the default mode network. J Cognitive Neurosci. 2010;22(6):1112–1123. doi:10.1162/jocn.2009.21282
36. Spreng RN, Stevens WD, Chamberlain JP, Gilmore AW, Schacter DL. Default network activity, coupled with the frontoparietal control network, supports goal-directed cognition. Neuroimage. 2010;53(1):303–317. doi:10.1016/j.neuroimage.2010.06.016
37. Spreng RN. The fallacy of a “task-negative” network. Front Psychol. 2012;3:145. doi:10.3389/fpsyg.2012.00145
38. Spreng RN, Gerlach KD, Turner GR, Schacter DL. Autobiographical planning and the brain: activation and its modulation by qualitative features. J Cognitive Neurosci. 2015;27(11):2147–2157. doi:10.1162/jocn_a_00846
39. Addis DR, Pan L, Vu M-A, Laiser N, Schacter DL. Constructive episodic simulation of the future and the past: distinct subsystems of a core brain network mediate imagining and remembering. Neuropsychologia. 2009;47(11):2222–2238. doi:10.1016/j.neuropsychologia.2008.10.026
40. Menon V. 20 years of the default mode network: a review and synthesis. Neuron. 2023;111(16):2469–2487. doi:10.1016/j.neuron.2023.04.023
41. Slater M. Immersion and the illusion of presence in virtual reality. Br J Psychol. 2018;109(3):431–433. doi:10.1111/bjop.12305
42. AnNing A, Ahmad M. The influence of multi-sensory feedback on immersive virtual reality experience is analyzed. ESP Int J Adv Sci Technol. 2024;2(1):39–44.
43. Liu X, Yang S, Wang Y, et al. Comparison of the effectiveness of immersive and non-immersive virtual reality in the treatment of vertigo in patients with peripheral vestibular dysfunction: a systematic review and meta-analysis. Front Neurol. 2025;16:1638868. doi:10.3389/fneur.2025.1638868
44. Buche H, Michel A, Anders R, Blanc N. The role of engagement in virtual reality to enhance emotional well-being in breast cancer patients: a mediation analysis. Cancers. 2025;17(5):840. doi:10.3390/cancers17050840
45. Touloudi E, Hassandra M, Galanis E, et al. Effectiveness and acceptance of virtual reality vs. traditional exercise in obese adults: a pilot randomized trial. Front Sport Active Liv. 2025;7:1520068. doi:10.3389/fspor.2025.1520068
46. Makransky G, Petersen GB. The cognitive affective model of immersive learning (CAMIL): a theoretical research-based model of learning in immersive virtual reality. Educ Psychol Rev. 2021;33(3):937–958. doi:10.1007/s10648-020-09586-2
47. Sutherland MT, McHugh MJ, Pariyadath V, Stein EA. Resting state functional connectivity in addiction: lessons learned and a road ahead. Neuroimage. 2012;62(4):2281–2295. doi:10.1016/j.neuroimage.2012.01.117
48. First MB, Williams JBW, Karg RS, Spitzer RL. SCID-5 for DSM-5, Research Version; SCID-5-RV. Structured Clinical Interview for DSM-5—research Version. American Psychiatric Association; 2015.
49. Sobell MB, Sobell LC, Klajner F, Pavan D, Basian E. The reliability of a timeline method for assessing normal drinker college students’ recent drinking history: utility for alcohol research. Addict Behav. 1986;11(2):149–161. doi:10.1016/0306-4603(86)90040-7
50. Madden GJ, Petry NM, Badger GJ, Bickel WK. Impulsive and self-control choices in opioid-dependent patients and non-drug-using control participants: drug and monetary rewards. Exp Clin Psychopharmacol. 1997;5(3):256–262. doi:10.1037/1064-1297.5.3.256
51. Du W, Green L, Myerson J. Cross-cultural comparisons of discounting delayed and probabilistic rewards. Psychol Rec. 2002;52(4):479–492. doi:10.1007/BF03395199
52. Oberlin BG, Albrecht DS, Herring CM, et al. Monetary discounting and ventral striatal dopamine receptor availability in nontreatment-seeking alcoholics and social drinkers. Psychopharmacology. 2015;232(12):2207–2216. doi:10.1007/s00213-014-3850-5
53. Whiteside SP, Lynam DR. The five factor model and impulsivity: using a structural model of personality to understand impulsivity. Person individ Diff. 2001;30(4):669–689. doi:10.1016/S0191-8869(00)00064-7
54. Cyders MA, Littlefield AK, Coffey S, Karyadi KA. Examination of a short English version of the UPPS-P Impulsive Behavior Scale. Addict Behav. 2014;39(9):1372–1376. doi:10.1016/j.addbeh.2014.02.013
55. Flanagan JC. A research approach to improving our quality of life. Am Psychologist. 1978;33(2):138. doi:10.1037/0003-066X.33.2.138
56. Tracy EM, Laudet AB, Min MO, et al. Prospective patterns and correlates of quality of life among women in substance abuse treatment. Drug Alcohol Depend. 2012;124(3):242–249. doi:10.1016/j.drugalcdep.2012.01.010
57. Sheridan TB. Musings on telepresence and virtual presence. Presence. 1992;1(1):120–126. doi:10.1162/pres.1992.1.1.120
58. Yee N, Bailenson J. The Proteus effect: behavioral modification via transformations of digital self-representation. Hum Commun Res. 2007;33(3):271–290. doi:10.1111/j.1468-2958.2007.00299.x
59. Moeller S, Yacoub E, Olman CA, et al. Multiband multislice GE-EPI at 7 tesla, with 16-fold acceleration using partial parallel imaging with application to high spatial and temporal whole-brain fMRI. Magnet Reson Med. 2010;63(5):1144–1153. doi:10.1002/mrm.22361
60. Jenkinson M, Beckmann CF, Behrens TE, Woolrich MW, Smith SM. Fsl. Neuroimage. 2012;62(2):782–790. doi:10.1016/j.neuroimage.2011.09.015
61. Beckmann CF, Smith SM. Probabilistic independent component analysis for functional magnetic resonance imaging. IEEE Transact Med Imaging. 2004;23(2):137–152. doi:10.1109/TMI.2003.822821
62. Pruim RHR, Mennes M, van Rooij D, Llera A, Buitelaar JK, Beckmann CF. ICA-AROMA: a robust ICA-based strategy for removing motion artifacts from fMRI data. Neuroimage. 2015;112:267–277. doi:10.1016/j.neuroimage.2015.02.064
63. Ashburner J, Barnes G, Chen -C-C, et al. SPM12 manual. Wellcome Trust Centre Neuroimaging. 2014;2464(4):53.
64. Olszowy W, Aston J, Rua C, Williams GB. Accurate autocorrelation modeling substantially improves fMRI reliability. Nat Commun. 2019;10(1):1220. doi:10.1038/s41467-019-09230-w
65. Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J R Stat Soc. 1995;57(1):289–300. doi:10.1111/j.2517-6161.1995.tb02031.x
66. Szpunar KK, Spreng RN, Schacter DL. A taxonomy of prospection: introducing an organizational framework for future-oriented cognition. Proc Natl Acad Sci. 2014;111(52):18414–18421. doi:10.1073/pnas.1417144111
67. Andrews-Hanna JR, Smallwood J, Spreng RN. The default network and self-generated thought: component processes, dynamic control, and clinical relevance. Ann N Y Acad Sci. 2014;1316(1):29–52. doi:10.1111/nyas.12360
68. Schacter DL, Addis DR, Buckner RL. Remembering the past to imagine the future: the prospective brain. Nat Rev Neurosci. 2007;8(9):657–661. doi:10.1038/nrn2213
69. Cabeza R, Mangels J, Nyberg L, et al. Brain regions differentially involved in remembering what and when: a PET study. Neuron. 1997;19(4):863–870. doi:10.1016/S0896-6273(00)80967-8
70. Foster BL, Dastjerdi M, Parvizi J. Neural populations in human posteromedial cortex display opposing responses during memory and numerical processing. Proc Natl Acad Sci. 2012;109(38):15514–15519. doi:10.1073/pnas.1206580109
71. Addis DR, Wong AT, Schacter DL. Remembering the past and imagining the future: common and distinct neural substrates during event construction and elaboration. Neuropsychologia. 2007;45(7):1363–1377. doi:10.1016/j.neuropsychologia.2006.10.016
72. Qin P, Northoff G. How is our self related to midline regions and the default-mode network? Neuroimage. 2011;57(3):1221–1233. doi:10.1016/j.neuroimage.2011.05.028
73. Yeo BT, Krienen FM, Sepulcre J, et al. The organization of the human cerebral cortex estimated by intrinsic functional connectivity. J Neurophysiol. 2011;106(3):1125–1165. doi:10.1152/jn.00338.2011
74. Koshino H, Minamoto T, Yaoi K, Osaka M, Osaka N. Coactivation of the default mode network regions and working memory network regions during task preparation. Sci Rep. 2014;4(1):5954. doi:10.1038/srep05954
75. McClure SM, Laibson DI, Loewenstein G, Cohen JD. Separate neural systems value immediate and delayed monetary rewards. Science. 2004;306(5695):503–507. doi:10.1126/science.1100907
76. Kable JW, Glimcher PW. The neural correlates of subjective value during intertemporal choice. Nat Neurosci. 2007;10(12):1625–1633. doi:10.1038/nn2007
77. Kable JW, Glimcher PW. An “as soon as possible” effect in human intertemporal decision making: behavioral evidence and neural mechanisms. J Neurophysiol. 2010;103(5):2513–2531. doi:10.1152/jn.00177.2009
78. Wesley MJ, Bickel WK. Remember the future II: meta-analyses and functional overlap of working memory and delay discounting. Biol Psychiatry. 2014;75(6):435–448. doi:10.1016/j.biopsych.2013.08.008
79. Moro AS, Saccenti D, Ferro M, Scaini S, Malgaroli A, Lamanna J. Neural correlates of delay discounting in the light of brain imaging and non-invasive brain stimulation: what we know and what is missed. Brain Sci. 2023;13(3):403. doi:10.3390/brainsci13030403
80. Menon V. Large-scale brain networks and psychopathology: a unifying triple network model. Trends cognit sci. 2011;15(10):483–506. doi:10.1016/j.tics.2011.08.003
81. Oberlin BG, Shen YI, Kareken DA. Alcohol use disorder interventions targeting brain sites for both conditioned reward and delayed gratification. Neurotherapeutics. 2020;17(1):70–86. doi:10.1007/s13311-019-00817-1
82. Stawarczyk D, D’Argembeau A. Neural correlates of personal goal processing during episodic future thinking and mind-wandering: an ALE meta-analysis. Hum Brain Mapp. 2015;36(8):2928–2947. doi:10.1002/hbm.22818
83. Musholt K. A philosophical perspective on the relation between cortical midline structures and the self. Front Human Neurosci. 2013;7:536. doi:10.3389/fnhum.2013.00536
84. Kamarajan C, Ardekani BA, Pandey AK, et al. Random forest classification of alcohol use disorder using fMRI functional connectivity, neuropsychological functioning, and impulsivity measures. Brain Sci. 2020;10(2):115. doi:10.3390/brainsci10020115
85. Zhu X, Cortes CR, Mathur K, Tomasi D, Momenan R. Model-free functional connectivity and impulsivity correlates of alcohol dependence: a resting-state study. Addict Biol. 2017;22(1):206–217. doi:10.1111/adb.12272
86. Haxby JV, Hoffman EA, Gobbini MI. The distributed human neural system for face perception. Trends Cognit Sci. 2000;4(6):223–233. doi:10.1016/S1364-6613(00)01482-0
87. Ambrus GG, Amado C, Krohn L, Kovács G. TMS of the occipital face area modulates cross-domain identity priming. Brain Struct Funct. 2019;224(1):149–157. doi:10.1007/s00429-018-1768-0
88. Eick CM, Kovács G, Rostalski S-M, Röhrig L, Ambrus GG. The occipital face area is causally involved in identity-related visual-semantic associations. Brain Struct Funct. 2020;225(5):1483–1493. doi:10.1007/s00429-020-02068-9
89. Rust NC, DiCarlo JJ. Selectivity and tolerance (“invariance”) both increase as visual information propagates from cortical area V4 to IT. J Neurosci. 2010;30(39):12978–12995. doi:10.1523/JNEUROSCI.0179-10.2010
90. Ritchie JB, Montesinos S, Carter MJ. What is a visual stream? J Cognitive Neurosci. 2024;36(12):2627–2638. doi:10.1162/jocn_a_02191
91. Nagy K, Greenlee MW, Kovács G. The lateral occipital cortex in the face perception network: an effective connectivity study. Front Psychol. 2012;3:141. doi:10.3389/fpsyg.2012.00141
92. Gschwind M, Pourtois G, Schwartz S, Van De Ville D, Vuilleumier P. White-matter connectivity between face-responsive regions in the human brain. Cereb Cortex. 2012;22(7):1564–1576. doi:10.1093/cercor/bhr226
93. Demblon J, Bahri MA, D’Argembeau A. Neural correlates of event clusters in past and future thoughts: how the brain integrates specific episodes with autobiographical knowledge. NeuroImage. 2016;127:257–266. doi:10.1016/j.neuroimage.2015.11.062
94. Gerlach KD, Spreng RN, Gilmore AW, Schacter DL. Solving future problems: default network and executive activity associated with goal-directed mental simulations. Neuroimage. 2011;55(4):1816–1824. doi:10.1016/j.neuroimage.2011.01.030
95. Kosten TR, Scanley BE, Tucker KA, et al. Cue-induced brain activity changes and relapse in cocaine-dependent patients. Neuropsychopharmacology. 2006;31(3):644–650. doi:10.1038/sj.npp.1300851
96. Loughead J, Wileyto EP, Ruparel K, et al. Working memory-related neural activity predicts future smoking relapse. Neuropsychopharmacology. 2015;40(6):1311–1320. doi:10.1038/npp.2014.318
97. Lord AR, Li M, Demenescu LR, et al. Richness in functional connectivity depends on the neuronal integrity within the posterior cingulate cortex. Front Neurosci. 2017;11:184. doi:10.3389/fnins.2017.00184
98. Wilcox CE, Abbott CC, Calhoun VD. Alterations in resting-state functional connectivity in substance use disorders and treatment implications. Prog Neuro Psychopharmacol Biol Psychiatry. 2019;91:79–93. doi:10.1016/j.pnpbp.2018.06.011
99. Bach P, Kirsch M, Hoffmann S, et al. The effects of single nucleotide polymorphisms in glutamatergic neurotransmission genes on neural response to alcohol cues and craving. Addict Biol. 2015;20(6):1022–1032. doi:10.1111/adb.12291
100. Seo D, Lacadie CM, Tuit K, Hong K-I, Constable RT, Sinha R. Disrupted ventromedial prefrontal function, alcohol craving, and subsequent relapse risk. JAMA psychiatry. 2013;70(7):727. doi:10.1001/jamapsychiatry.2013.762
101. Blaine SK, Seo D, Sinha R. Peripheral and prefrontal stress system markers and risk of relapse in alcoholism. Addict Biol. 2017;22(2):468–478. doi:10.1111/adb.12320
102. Wang A, Elman I, Lowen S, et al. Neural correlates of adherence to extended-release naltrexone pharmacotherapy in heroin dependence. Transl Psychiatry. 2015;5(3):e531. doi:10.1038/tp.2015.20
103. Januszko P, Gmaj B, Piotrowski T, et al. Delta resting-state functional connectivity in the cognitive control network as a prognostic factor for maintaining abstinence: an eLORETA preliminary study. Drug Alcohol Depend. 2021;218:108393. doi:10.1016/j.drugalcdep.2020.108393
104. Lenth RV. Some practical guidelines for effective sample size determination. Am Stat. 2001;55(3):187–193. doi:10.1198/000313001317098149
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Awareness and Predictors of the Use of Bioinformatics in Genome Research in Saudi Arabia
Alomair L, Abolfotouh MA
International Journal of General Medicine 2023, 16:3413-3425
Published Date: 11 August 2023