Back to Journals » OncoTargets and Therapy » Volume 18
Personalized Treatment for Invasive Ductal Breast Carcinoma with Lung and Liver Metastases Based on Patient-Derived Organoids: A Case Report
Authors Zheng M, Yao L, Jing N, Wang Y, Wang X, Yang J
Received 13 May 2025
Accepted for publication 3 October 2025
Published 25 October 2025 Volume 2025:18 Pages 1189—1194
DOI https://doi.org/10.2147/OTT.S540143
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Yong Teng
Miaoli Zheng,1,* Liang Yao,2,* Na Jing,1 Yu Wang,1 Xianling Wang,1 Jun Yang2
1Department of Radiotherapy, Shanxi Province Cancer Hospital/Shanxi Hospital Affiliated to Cancer Hospital, Chinese Academy of Medical Sciences/Cancer Hospital Affiliated to Shanxi Medical University, Taiyuan, 030013, People’s Republic of China; 2Department of Breast Surgery, Shanxi Province Cancer Hospital/Shanxi Hospital Affiliated to Cancer Hospital, Chinese Academy of Medical Sciences/Cancer Hospital Affiliated to Shanxi Medical University, Taiyuan, 030013, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jun Yang, Department of Breast Surgery, Shanxi Province Cancer Hospital/Shanxi Hospital Affiliated to Cancer Hospital, Chinese Academy of Medical Sciences/Cancer Hospital Affiliated to Shanxi Medical University, No. 3 Zhigongxincun, Xinghualing District, Taiyuan, 030013, People’s Republic of China, Email [email protected] Xianling Wang, Department of Radiotherapy, Shanxi Province Cancer Hospital/Shanxi Hospital Affiliated to Cancer Hospital, Chinese Academy of Medical Sciences/Cancer Hospital Affiliated to Shanxi Medical University, No. 3 Zhigongxincun, Xinghualing District, Taiyuan, 030013, People’s Republic of China, Email [email protected]
Abstract: Patient-derived organoids (PDOs) are emerging as a potential preclinical tool in assessing cancer patients’ responses to various therapies. Here, we first described a case of invasive ductal breast carcinoma with lung and liver metastases who obtained efficient response to the sensitive drugs identified by PDOs. A 54-year-old woman came to hospital with the chief complaint of an unpainful mass in the right breast. In combination with relevant examinations, she was diagnosed with cT3N1M0 breast cancer with HER2 amplification, but developed lung and liver metastases after use of multiple therapies. After treatment with erebulin, carboplatin and inetetamab sensitive revealed by the organoid drug sensitivity testing, partial response in lung metastasis and stable disease in liver metastasis were achieved. This typical case suggests that for the individual patients with advanced refractory breast cancer, especially those exhausting the standard treatment options, the PDOs may serve as an effective model for assessing individual drug sensitivity to optimize treatment decisions and improve treatment response.
Keywords: invasive ductal carcinoma, liver metastasis, lung metastasis, patient-derived organoids, treatment response
Introduction
Breast cancer is the most frequently diagnosed cancer in women worldwide. Despite improved survival through implementation of screening programs and effective treatment modalities, breast cancer-related deaths are still a common cause of cancer deaths.1 According to the classification of cell morphology, growth and architecture patterns, breast cancer can be categorized into up to 21 histological subtypes, among which invasive ductal carcinoma (IDC) is most common, approximately accounting for 75% of all invasive breast cancers.2 The 5-year survival rate of breast cancer patients is reported nearly 100% after treatment, while for metastatic breast cancer the 5-year survival rate is only 30%.3,4 The aggressive nature and high mortality of metastatic breast cancer highlight the demand for more precise treatment.
Patient-derived organoids (PDOs), an in vitro 3D culture model, have been identified to be a potential platform for human cancers, which can highly recapitulate the histopathological and molecular features of the parental tumor. Importantly, they are not only conductive to understanding cancer biology but also promising in assessment of cancer patients’ responses to chemotherapy, radiotherapy, and targeted therapy.5–7 In a previous study, the organoids derived from human breast cancer tissues, including heavily treated samples, were cultured successfully, and the PDO-based drug-sensitive response signatures were found to predict the prolonged distant relapse-free survival of invasive breast cancer patients receiving adjuvant chemotherapy.8 Here, we first described a case of IDC with lung and liver metastases who achieved efficient response to the sensitive agents screened by PDOs after various standard treatment regimens were exhausted.
Case Presentation
A 54-year-old woman was admitted to our hospital with the chief complaint of an unpainful mass with the size of red dates in the right breast, not accompanied by nipple discharge. She previously had no history of allergy and inherited tumors. In May 2019, the patient accidentally found a mass in the right breast. The needle biopsy showed IDC, with ER (-), PR (-), HER2 (3+), and Ki-67 (70%+) through immunochemical staining. In combination with relevant examinations, she was diagnosed with cT3N1M0 breast cancer with HER2 amplification. Accordingly, AC-sequential TH neoadjuvant chemotherapy was used for 8 cycles, including doxorubicin liposomes (40 mg*4), cyclophosphamide (0.8 g*4), docetaxel (120 mg*4) and trastuzumab (8 mg/kg for the first time, then 6 mg/kg).
On November 14, 2019, a modified radical mastectomy for the right breast cancer was performed. Postoperative pathology showed IDC with partial degeneration of cancer cells, Miller Payne grade 2, and the tumor diameter of 1 cm. Vascular cancer emboli were observed, but without neural invasion. In addition, axillary lymph node metastasis occurred in 1 of the 12 lymph nodes. The tumor was assessed as ypT2N1M0. Considering that the pathological complete response was not achieved, TDM-1 was applied to improve the prognosis according to KATHERINE study.6 However, this patient was treated with trastuzumab and pertuzumab (840 mg for the first time, then 420 mg) due to high cost of TDM-1. On March 23, 2020, she received intensity-modulated radiation therapy, with the prescribed dose of 50 Gy/25f. In June 2022, the chest computerized tomography (CT) showed scattered nodules in both lungs, with the largest one close to 1.1 cm (Figure 1). Based on the medical history and imagining examinations, lung metastasis was suspected. After use of nab-paclitaxel (200 mg) for 12 weeks, dual-targeted therapy with trastuzumab and pertuzumab was used until April 2023. Re-examination of the chest CT indicated more increased nodules in both lungs, with the largest one close to 3.4 cm (Figure 1). On April 20, 2023, TDM-1 (200 mg) as the second-line salvage treatment was administered for 4 cycles. Although stable disease (SD) after two cycles was evaluated, the chest CT showed more increased nodules in lungs and some new nodules in the liver after four cycles. On August 28, 2023, the liver magnetic resonance imaging (MRI) indicated slightly longer T1/T2 signaling nodular shadows (1.4*1.2 cm) in the liver segment S8, with relatively clear boundary, suggesting liver metastasis (Figure 1).
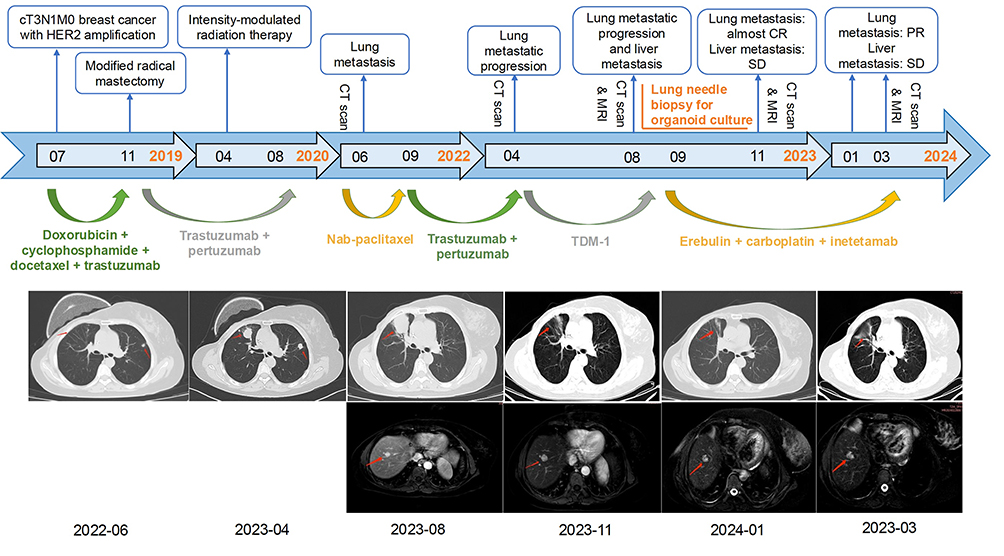 |
Figure 1 The treatment timeline of the patient and imaging changes at different time points. The red arrows point to the lesions in the lung through CT scans (upper) and liver using MRI examinations (lower). |
Needle biopsy of pulmonary nodules showed invasive cancer, not excluding from the breast cancer. Additionally, immunohistochemical results indicated ER (-), PR (-), HER2 (3+), Ki-67 (90%+), AE1/AE3 (+), CK7 (+), TTF-1 (-), Napsin-A (-), CK5 (70%+), Syn (-), P40 (20%), P63 (10%+) and GATA3 (+). Therefore, lung and liver metastases were further confirmed. After the patient was informed consent, the PDO from lung metastatic lesions of breast cancer was cultured strictly based on the protocols of Kingbio Medical (Chongqing) Co., Ltd., China. According to the culture procedure, the tissue was first washed, and then minced, digested, filtered, and finally placed in an incubator with 5% CO2 at 37°C for culture after adding Matrigel and Jiabili® culture medium. The status of organoid formation was observed using an optical microscope (Figure 2A). When the organoid presented typical saccular, solid spherical or dispersive base form, drug sensitivity testing was performed. The reagents associated with organoid culture and drug sensitivity testing were all provided by Kingbio Medical (Chongqing) Co., Ltd., China. It could be observed that the PDO was more sensitive to carboplatin, capecitabine, erebulin, and inetetamab than other drugs (Figure 2B). Thus, on September 25, 2023, a combination therapy of erebulin (2 mg d1,8), carboplatin (50 mg, d1) and inetetamab (350 mg, d1) was administrated. After two cycles, the chest CT showed significantly reduced masses alongside the horizontal fissure in the right upper lung lobe and nodular shadows in the lingual segment of the left upper lung lobe, almost achieving complete response (CR). The liver MRI indicated no significant changes in nodules of the liver segment 8 (Figure 1), and SD was assessed. After four and six cycles of treatment, CT and MRI examinations were both performed for assessing the therapeutic effect of the patient (Figure 1), and partial response in lung metastatic lesions and SD in liver metastatic lesions were achieved, respectively. Now, the patient was still treated with erebulin, carboplatin and inetetamab.
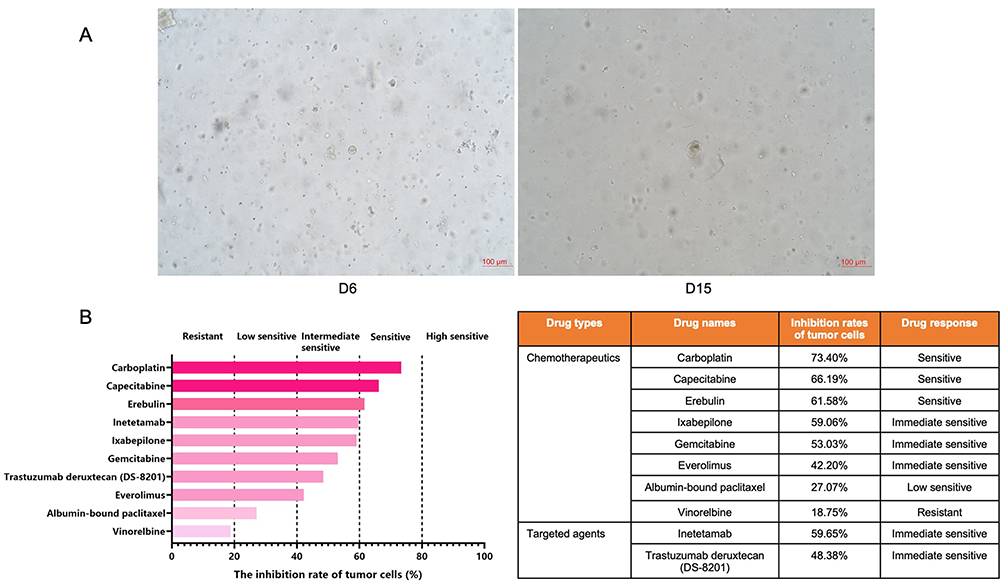 |
Figure 2 The formation status of the patient-derived organoid from lung metastatic lesions in a patient with invasive ductal carcinoma on day 6 and day 15 (A) and the drug sensitivity results (B). According to the inhibition rates of tumor cells, 5 categories are adopted in this study, including high sensitive (>80%), sensitive (60%-80%), intermediate sensitive (40%-60%), low sensitive (20%-40%) and resistant (<20%). |
Discussion
Breast cancer patients with distant metastasis were reported to have the 5-year survival rate of less than 20%.9,10 Although multiple therapies are used for distant metastasis, the survival rate of patients is still low. The recently developed PDOs have been confirmed potential for evaluating the responses to various cancer therapies.5–7 In this study, we successfully established the PDO model for IDC with lung and liver metastases, based on which the combination regimen of drugs sensitive to the patient was used, and the disease was finally under control following failure in multiple standard treatments.
It is estimated that metastatic breast cancer occurs in over half a million women worldwide each year, which can lead to 90% of breast cancer deaths.11 Lung, liver, bone, and brain are the most frequent metastatic sites in breast cancer and are related to the poor prognosis of patients.12 Lung metastasis preferentially occurs in triple-negative breast cancer (TNBC), while bone metastasis is commonly diagnosed in luminal breast cancer.13 It was reported that the incidence of lung metastasis in TNBC could reach up to 40%, significantly higher than that in non-TNBC.14 According to immunochemical results, the case in our study was diagnosed with HER2-positive breast cancer and experienced lung metastasis. By analyzing the survival outcomes of breast cancer patients with lung metastasis, Yhim et al found that the clinical outcomes of patients with HER2-positive breast cancer and TNBC were worse by comparison to those with hormone receptor-positive breast cancer.15 Notably, HER2-positive breast cancer was identified to be associated with a higher risk of liver metastasis.16 As shown in our study, the patient still suffered from liver metastasis, although various treatment strategies were used.
For advanced breast cancer, a major obstacle to effective treatment is resistance to therapy. In the past few years, tumor organoids have emerged as a promising preclinical model for studying the evolution of tumors, assess the drug efficacy, and explore the mechanism of tumor metastasis.17 By establishing an organoid biobank from breast cancer, Shu et al found that PDOs could not only predict the patient response to neoadjuvant chemotherapy but also be used for screening the drugs with various functions on different patients.18 PDOs also showed a good concordance with original tumors regarding histopathology, hormone receptor levels and HER2 receptor status. For breast cancer patients who had received multiple lines of treatment and showed drug resistance, the PDOs established from their metastatic tissues were also resistant to the same drugs. Meanwhile, for multi-drug-resistant patients with metastatic breast cancer, PDO-based drug screening could help to predict the sensitive drugs.8 Importantly, metastatic breast cancer patients receiving organoid-guided treatment had prolonged progression-free survival and improved disease control by contrast to those receiving the treatment of physician’s choice, further suggesting that PDO-based drug screening contributed to overcoming drug resistance and optimizing treatment strategies for metastatic breast cancer.19 In our study, we generated a PDO model for an IDC patient with distant metastasis after multiple standard therapies were exhausted, and a good response was obtained after use of the effective drugs identified by the PDO. Notably, after the PDO-guided treatment for two cycles, the lung metastases showed significant regression through the CT, nearly approaching CR, while the liver metastases were evaluated as stable by MRI. This inconsistent clinical manifestations between lung and liver metastases might be associated with the disease complexity at an advanced stage, including significant heterogeneity at different metastatic sites and differences in sensitivity to cytotoxic drugs in different regions. Moreover, the size of lesions displayed through radiological examinations may not reflect the real image of tumor lesions, as different regression patterns after treatment can affect our evaluation on the therapeutic effect. For instance, fragmented sieve regression makes it difficult to clearly determine the tumor boundary, consequently leading to unclear imaging findings.
Regarding the clinical application of PDOs, there are several significant challenges that should be addressed. First, it is very necessary to standardize the protocols for organoid culture and drug sensitivity testing to make the results repeatable. By standardizing culturing techniques, the consistency between organoid models and patients’ tumors in the aspects of gene expression profiles, drug sensitivity, and drug resistance can be enhanced, thereby enabling more accurate prediction of patients’ responses to specific treatment regimens. This advancement will provide support for clinicians to develop more personalized and effective therapeutic strategies. Second, the currently constructed PDOs are mainly from epithelial cells. The organoids from non-epithelial cells should also be established to further guide the tumor treatment, such as lung cancer.20 Third, some certain in vivo components like immune cells and fibroblasts are absent in PDOs. Recent studies are attempting to develop new technological platforms to assess the individual response to immunotherapy through coculture of PDOs with tumor infiltrating lymphocytes and peripheral blood mononuclear cells.21,22 Importantly, metastasis is tough to evaluate with PDOs, as a tumor has both temporal and spatial invasiveness in the body.23 Nevertheless, the PDOs derived from metastatic tumor tissues provide scientists with a means to study how cancer cells invade distant organs. Combined with real-time imaging and spatial omics technologies, significant breakthroughs are expected to be achieved in this field. Although our study was a single case, it was not hard to see the importance of PDOs in predicting the personalized treatment for individual patients. In addition, the long-term survival outcome of the patient was missing. In the future, the studies with large sample size and long follow-up duration should be performed to further support our findings.
Conclusion
Through establishment of PDOs from the metastatic lesions of an IDC patient, we demonstrated that this patient obtained a good response to the sensitive drugs screened by the PDO after failure in multiple standard treatments. This unique case highlights that for the individual patients with advanced refractory breast cancer, especially those exhausting the standard treatment options, the PDOs may serve as an effective model for assessing individual drug sensitivity to optimize treatment decisions and improve treatment response.
Ethics Approval and Consent to Participate
Written informed consent was obtained from the patient for publication of the health information in anonymised form. Institutional review board approval was not required, given the patient provided written consent.
Consent for Publication
All authors approved the publication of the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74:229–263. doi:10.3322/caac.21834
2. Lebeau A, Denkert C. Updated WHO classification of tumors of the breast: the most important changes. Pathologe. 2021;42:270–280. doi:10.1007/s00292-021-00934-9
3. DeSantis CE, Ma J, Gaudet MM, et al. Breast cancer statistics, 2019. CA Cancer J Clin. 2019;69:438–451. doi:10.3322/caac.21583
4. Waks AG, Winer EP. Breast cancer treatment: a review. JAMA. 2019;321:288–300. doi:10.1001/jama.2018.19323
5. Yao Y, Xu X, Yang L, et al. Patient-derived organoids predict chemoradiation responses of locally advanced rectal cancer. Cell Stem Cell. 2020;26:17–26.e6. doi:10.1016/j.stem.2019.10.010
6. Vlachogiannis G, Hedayat S, Vatsiou A, et al. Patient-derived organoids model treatment response of metastatic gastrointestinal cancers. Science. 2018;359:920–926. doi:10.1126/science.aao2774
7. Ganesh K, Wu C, O’Rourke KP, et al. A rectal cancer organoid platform to study individual responses to chemoradiation. Nat Med. 2019;25(10):1607–1614. doi:10.1038/s41591-019-0584-2
8. Chen P, Zhang X, Ding R, et al. Patient-derived organoids can guide personalized-therapies for patients with advanced breast cancer. Adv Sci. 2021;8:e2101176.
9. Gennari A, Conte P, Rosso R, et al. Survival of metastatic breast carcinoma patients over a 20-year period: a retrospective analysis based on individual patient data from six consecutive studies. Cancer. 2005;104(8):1742–1750. doi:10.1002/cncr.21359
10. Gligorov J, Lotz JP. Optimal treatment strategies in postmenopausal women with hormone-receptor-positive and HER2-negative metastatic breast cancer. Breast Cancer Res Treat. 2008;112:53–66. doi:10.1007/s10549-008-0232-x
11. Soni A, Ren Z, Hameed O, et al. Breast cancer subtypes predispose the site of distant metastases. Am J Clin Pathol. 2015;143:471–478. doi:10.1309/AJCPYO5FSV3UPEXS
12. Largillier R, Ferrero JM, Doyen J, et al. Prognostic factors in 1038 women with metastatic breast cancer. Ann Oncol. 2008;19(12):2012–2019. doi:10.1093/annonc/mdn424
13. Jin L, Han B, Siegel E, et al. Breast cancer lung metastasis: molecular biology and therapeutic implications. Cancer Biol Ther. 2018;19(10):858–868. doi:10.1080/15384047.2018.1456599
14. Foulkes WD, Smith IE, Reis-Filho JS. Triple-negative breast cancer. N Engl J Med. 2010;363(20):1938–1948. doi:10.1056/NEJMra1001389
15. Yhim HY, Han SW, Oh DY, et al. Prognostic factors for recurrent breast cancer patients with an isolated, limited number of lung metastases and implications for pulmonary metastasectomy. Cancer. 2010;116:2890–2901. doi:10.1002/cncr.25054
16. Gerratana L, Fanotto V, Bonotto M, et al. Pattern of metastasis and outcome in patients with breast cancer. Clin Exp Metastasis. 2015;32(2):125–133. doi:10.1007/s10585-015-9697-2
17. Bhattacharya A, Alam K, Roy NS, et al. Exploring the interaction between extracellular matrix components in a 3D organoid disease model to replicate the pathophysiology of breast cancer. J Exp Clin Cancer Res. 2023;42(1):343. doi:10.1186/s13046-023-02926-4
18. Shu D, Shen M, Li K, et al. Organoids from patient biopsy samples can predict the response of BC patients to neoadjuvant chemotherapy. Ann Med. 2022;54:2581–2597. doi:10.1080/07853890.2022.2122550
19. Lin YY, Gao HF, Li H, et al. Clinical efficacy of tumor organoid-guided cancer therapy for locally advanced unresectable or metastatic breast cancer. Int J Cancer. 2024;155:697–709. doi:10.1002/ijc.34945
20. Vazquez-Armendariz AI, Tata PR. Recent advances in lung organoid development and applications in disease modeling. J Clin Invest. 2023;133(22):e170500. doi:10.1172/JCI170500
21. Neal JT, Li X, Zhu J, et al. Organoid modeling of the tumor immune microenvironment. Cell. 2018;175:1972–1988.e16. doi:10.1016/j.cell.2018.11.021
22. Dijkstra KK, Cattaneo CM, Weeber F, et al. Generation of tumor-reactive T cells by co-culture of peripheral blood lymphocytes and tumor organoids. Cell. 2018;174:1586–1598.e12. doi:10.1016/j.cell.2018.07.009
23. Marx V. Closing in on cancer heterogeneity with organoids. Nat Methods. 2024;21:551–554. doi:10.1038/s41592-024-02231-8
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.