Back to Journals » Psoriasis: Targets and Therapy » Volume 16
Personalized Medicine in Psoriasis – A Long Road Ahead?
Authors Hillary TM ![]()
Received 10 January 2026
Accepted for publication 2 June 2026
Published 29 June 2026 Volume 2026:16 595079
DOI https://doi.org/10.2147/PTT.S595079
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Enzo Errichetti
Tom M Hillary
Department of Dermatology, University Hospital Leuven, Leuven, Belgium
Correspondence: Tom M Hillary, Department of Dermatology, University Hospital Leuven, Herestraat 49, Leuven, Vlaams-Brabant, 3000, Belgium, Tel +3216337950, Email [email protected]
Background: Biologic therapies targeting IL‑17 and IL‑23 have revolutionized psoriasis management, enabling rapid and durable disease control. Yet treatment selection still follows a trial‑and‑error approach, and clinically validated biomarkers for personalization remain absent.
Objective: To outline current challenges in biomarker development for psoriasis and describe the design and aims of the PICASSO prospective cohort as a platform for future personalized medicine.
Current Challenges: Despite evidence that IL‑17/IL‑23 inhibitors may induce disease modification through effects on effector, memory, and regulatory immune cells, reliable predictive or prognostic biomarkers have not emerged. Barriers include complex pathogenesis, universally high biologic efficacy reducing need for stratification, inconsistent findings from genetic or transcriptomic studies, and the multifactorial nature of comorbidities.
Methods (Picasso (ProspectIve Cohort psoriASiS FOllow-Up)): PICASSO is a 10‑year prospective biobank/registry enrolling patients within three years of disease onset. Biological samples are longitudinally linked to clinical and epidemiological data, with follow‑ups every 2.5 years. The ultimate aim is to identify biomarkers predicting disease trajectory.
Conclusion: Personalized psoriasis care requires biomarkers predicting progression and comorbidity risk. PICASSO represents a step toward disease‑modifying, preventive precision medicine.
Keywords: personalized treatment, research, dermatology, disease modification
Introduction
In the past two decades we have witnessed an exceptional therapeutic revolution in psoriasis. Biologics targeting interleukin-17 and interleukin-23 have enabled rapid, deep and durable disease control, transforming patient outcomes. Despite this progress, clinical practice still relies on a “trial-and-error” strategy, guided largely by physicians’ experience rather than objective parameters and oftentimes still resulting in a frustrating patient journey. Personalized medicine in psoriasis remains aspirational, particularly when compared with oncology, where validated biomarkers now guide treatment selection and predict prognosis.1
Recently, it was shown that IL17 and IL23-inhibitors not only reduce inflammatory effector cells in the skin but also inflammatory memory cells, besides increasing regulatory T cells. These changes could possibly account for the observation of durable disease-free periods, also after treatment cessation.2–4 This is referred to as disease modification, and in the context of psoriasis this should imply5
- Total skin clearance,
- Long-term disease-free periods after treatment cessation,
- Prevention of onset of comorbidities.
Background
For several reasons clinically useful predictive and prognostic biomarkers for psoriasis have not yet been identified. First, the pathogenesis is complex, involving interactions between genetic variants, immune pathways and environmental triggers. Second, cytokine blockade (eg IL17 or IL23) demonstrates high efficacy across all patient groups, reducing the immediate clinical pressure to stratify responders.6 Third, early studies linking genetic (eg. HLA-Cw6) or transcriptomic signatures to treatment outcomes have not translated into reproducible clinically differentiating tools.7 Finally, the multifactorial nature of comorbidity development complicates prediction.
In an era where full skin clearance is a feasible goal in daily practice, research should focus on the real unmet need: to identify biomarkers that predict disease progression and comorbidity risk, allowing proactive, preventive interventions. Without such markers, even our most effective drugs are deployed reactively, and opportunities for disease modification may be missed.
Ongoing pharmacokinetic trials such as BeNeBio (NCT04340076) and Helios (NCT06398106) are evaluating personalized dosing strategies by linking drug levels to outcomes. While valuable, these studies remain focused on optimizing treatment regimens rather than predicting long-term disease evolution. Multi-omics research has revealed promising candidates, yet reproducibility and validation across large, prospective cohorts are lacking.8 In sum, psoriasis lacks a single clinically actionable biomarker for either treatment stratification or prognosis.
Methods: The PICASSO Project (ProspectIve Cohort psoriASiS fOllow-up)
To address these challenges, we established the PICASSO (ProspectIve Cohort psoriASiS fOllow-up; NCT05122039) project, an observational 10-year prospective biobank and register, specifically designed to capture psoriasis patients early in their disease, and follow-up for sufficient time to grasp the evolution of both cutaneous disease and comorbidities. Patients with disease duration under three years are eligible and biological samples are linked to clinical and epidemiological data. (Figure 1) Study visits are repeated every 2.5 years. A limited number of healthy controls (n=50) will be included as a study specific control group. By prospectively following this inception cohort, PICASSO aims to:
- Identify biomarkers predictive of disease severity trajectories.
- Detect early signatures associated with psoriatic arthritis or cardiovascular comorbidity development.
- Explore multi-omics integration (genomic, transcriptomic, proteomic, and microbiome) to capture disease heterogeneity.
- Provide an open scientific resource for hypothesis-driven and exploratory biomarker research.
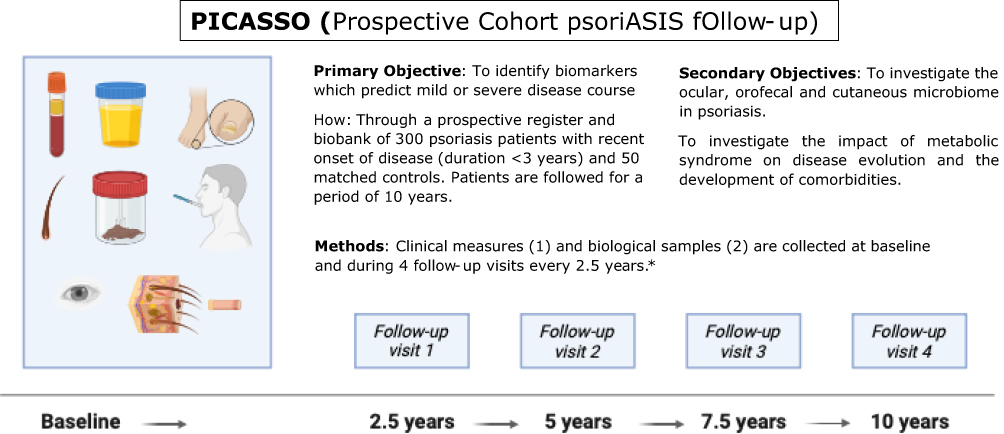 |
Figure 1 Study design (created with BioRender.com). Eligible patients (disease duration < 3 years) are screened at baseline and every 2.5 years thereafter. *A baseline blood test, blood (serum, plasma, DNA), urine (metabolomics), nails and hair (DNA), faeces, saliva, ocular, psoriatic and healthy skin swabs (microbiome) and tape stripping (mRNA). The samples are preserved at −80°C. Ultrasound measurement of carotid intima media thickness as a cardiovascular risk substitute, oral examination and a skin biopsy are optional. |
More than 70 patients are currently included and a data lock is planned for first analyses (eg. microbiome). Further recruitment aims to include 300 patients.
Conclusion
The ambition of personalized medicine in psoriasis should transcend the choice between equally effective biologics. Instead, it must deliver tools that allow clinicians to identify and intervene early in high-risk individuals, prevent comorbidities, and modify the disease course itself. Achieving this will require integrating clinical cohorts like PICASSO with global consortia and adopting machine learning approaches to identify reproducible biomarker panels rather than single candidate molecules.
The PICASSO project is one step toward the future, and we encourage international collaboration to accelerate this endeavor by reaching out to the research team.
Funding
The PICASSO project is supported by: Abbvie, Almirall, Amgen, Avène, Cerave, EG, Eli Lilly, Johnson & Johnson, La Roche Posay, Leo Pharma, Novartis, Pierre Fabre, UCB, Vichy.
Disclosure
Prof. Dr. Tom Hillary reports grants from Almirall, Amgen, J&J, EG, Leo Pharma, Eli Lilly, UCB, Novartis, Abbvie, during the conduct of the study; the author reports no other conflicts of interest in this work.
References
1. Bhamidipati D, Schram AM. Emerging tumor-agnostic molecular targets. Mol Cancer Ther. 2024;23(11):1544–3.
2. Schäkel K, Reich K, Asadullah K, et al. Early disease intervention with guselkumab in psoriasis leads to a higher rate of stable complete skin clearance (‘clinical super response’): week 28 results from the ongoing phase IIIb randomized, double-blind, parallel-group, GUIDE study. J Eur Acad Dermatol Venereol. 2023;37(10):2016–2027. doi:10.1111/jdv.19236
3. Gordon KB, Foley P, Krueger JG, et al. Bimekizumab efficacy and safety in moderate to severe plaque psoriasis (BE READY): a multicentre, double-blind, placebo-controlled, randomised withdrawal Phase 3 trial. Lancet. 2021;397(10273):475–486. doi:10.1016/S0140-6736(21)00126-4
4. Blauvelt A, Leonardi CL, Gooderham M, et al. Efficacy and safety of continuous risankizumab therapy vs treatment withdrawal in patients with moderate to severe plaque psoriasis: a phase 3 randomized clinical trial. JAMA Dermatol. 2020;156(6):649–658. doi:10.1001/jamadermatol.2020.0723
5. Eyerich K, Krueger J, Stahle M, et al. An international delphi consensus to define a clinically appropriate definition of disease modification for plaque psoriasis. J Eur Acad Dermatol Venereol. 2024;38(5):e424–e427. doi:10.1111/jdv.19652
6. Thomas SE, Barenbrug L, Hannink G, Seyger MMB, de Jong E, van den Reek J. Drug survival of IL-17 and IL-23 inhibitors for psoriasis: a systematic review and meta-analysis. Drugs. 2024;84(5):565–578. doi:10.1007/s40265-024-02028-1
7. Anzengruber F, Ghosh A, Maul JT, Drach M, Navarini AA. Limited clinical utility of HLA-Cw6 genotyping for outcome prediction in psoriasis patients under ustekinumab therapy: a monocentric, retrospective analysis. Psoriasis. 2017;8:7–11. doi:10.2147/PTT.S161437
8. Guo H, Gao J, Gong L, Wang Y. Multi-omics analysis reveals novel causal pathways in psoriasis pathogenesis. J Transl Med. 2025;23(1):100. doi:10.1186/s12967-025-06099-w
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.