Back to Journals » Advances in Medical Education and Practice » Volume 17
Personalized Learning in Health Professions Education: A Comprehensive Review
Authors Salih S, Alkatheeri A ![]() , Jacob NC, El-Sobkey SB, Hammoud E, Abdul Razak W
, Jacob NC, El-Sobkey SB, Hammoud E, Abdul Razak W ![]() , Kamil N, Sachdeva M, Hasaneen M
, Kamil N, Sachdeva M, Hasaneen M ![]() , Shaik BB
, Shaik BB ![]() , Nordin MN
, Nordin MN
Received 25 March 2026
Accepted for publication 19 June 2026
Published 9 July 2026 Volume 2026:17 612028
DOI https://doi.org/10.2147/AMEP.S612028
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Suliman Salih,1,2 Ajnas Alkatheeri,1 Ninan Cherry Jacob,1 Salwa B El-Sobkey,3 Emne Hammoud,3 Wuni Abdul Razak,1 Noon Kamil,4 Monika Sachdeva,4 Mohamed Hasaneen,1 Balkhis Banu Shaik,3 Mohd Nazmi Nordin1
1Radiography and Medical Imaging Department, Fatima College of Health Sciences, Abu Dhabi, 3798, United Arab Emirates; 2College of Medicine, Wad Medani University, Wad Madani, Sudan; 3Physiotherapy Department, Fatima College of Health Sciences, Abu Dhabi, 3798, United Arab Emirates; 4Pharmacy Department, Fatima College of Health Sciences, Abu Dhabi, 3798, United Arab Emirates
Correspondence: Ajnas Alkatheeri, Email [email protected]
Abstract: In response to the limitations of traditional one-size-fits-all models, health professions education is increasingly adopting personalized learning approaches that recognize individual learner differences. This review examines personalized learning in health professions education, focusing on its key principles, implementation strategies, and impact on learning outcomes. Literature searches were performed using PubMed, Scopus, and Google Scholar using specific keywords: “Personalized learning; Health professions education; education, Key principles; strategies for fostering personalized learning, learning outcomes; were reviewed by the authors. The key principles of personalized learning in health professions education centres are based on learner agency, learner-centeredness, self-Regulated learning and metacognition, and mastery-driven instruction tailored to individual needs. These strategies for implementing personalized learning include curriculum design, instructional methodologies, assessment methods, faculty development, and the integration of real-world clinical scenarios. Studies included in the current review have suggested several strategies to foster personalized learning in health professions education. The implementation of these strategies will enhance educational outcomes by improving knowledge retention, increasing learner engagement, strengthening overall academic performance, and better preparing students for clinical practice. In conclusion, Personalized learning in health professions education integrates learner-centered principles with competency-based progression, adaptive instruction, and continuous feedback to create responsive academic and clinical training environments. When implemented through structured curricular and assessment strategies, it enhances engagement, knowledge retention, clinical skill development, and long-term professional competence.
Keywords: personalized learning, health professions education, key principles, strategies for fostering personalized learning, learning outcomes
Introduction
Health professions education (HPE) has traditionally relied on teacher-centred, standardised instructional models designed to ensure content coverage, regulatory compliance, and minimum competency attainment. Personalized learning refers to instructional models that adapt content, pacing, feedback, and assessment based on learner performance data and developmental needs, while the traditional learning approach is characterised by didactic lectures, fixed curricular sequencing, uniform pacing, and summative assessments applied consistently across learner cohorts. The conventional method generally entails direct, in-person training, wherein medical students acquire clinical examination skills by practicing on healthy individuals or actual patients under the guidance of seasoned clinicians or medical educators.1 Evaluation of blended learning method versus traditional learning method of clinical examination skills in physiology among undergraduate medical students in an Indian medical college.2,3
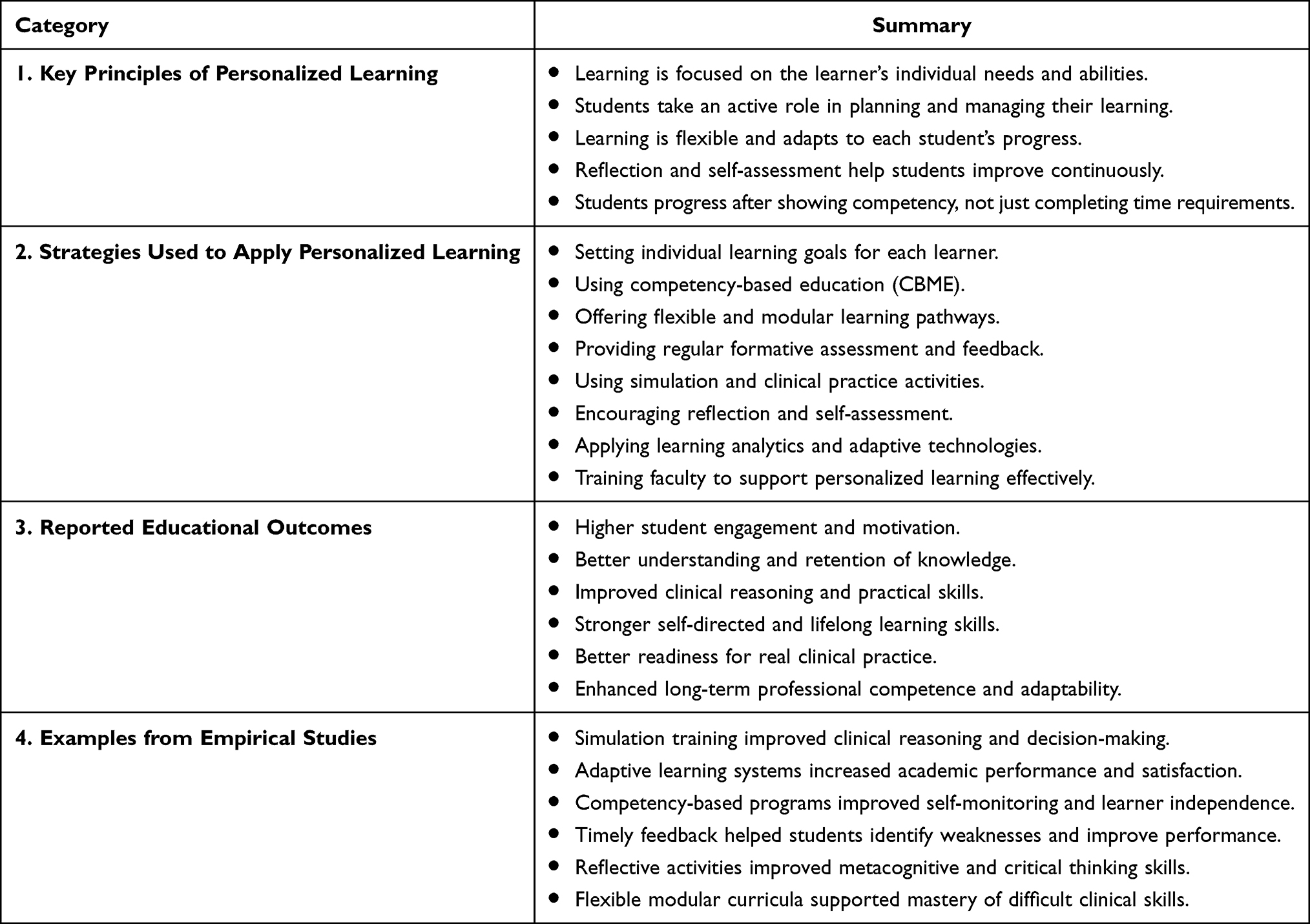 |
Table 1 Result Summary Table |
Within this framework, all learners are expected to progress through predetermined content irrespective of prior knowledge, learning needs, or performance variation. In clinical education, learning opportunities are often opportunistic rather than systematically mapped to developmental milestones.4 While this approach has historically supported standardisation in professional preparation, it assumes learner homogeneity and emphasises content transmission over adaptive competence development. Despite its longstanding use, the traditional model presents several limitations in contemporary healthcare education. Fixed pacing and standardised delivery may inadequately address individual differences in cognitive processing, motivation, and clinical reasoning development.5 Additionally, summative-dominant assessment structures restrict continuous formative feedback and iterative skill refinement. As healthcare systems become increasingly complex and technologically integrated, graduates must demonstrate adaptive expertise, interprofessional competence, and lifelong learning capacity.6 Traditional pedagogical models may insufficiently cultivate self-regulated learning and reflective practice—1 skills essential for sustained professional growth.7 Self-regulated learning defined as (SRL) refers to the process through which learners actively plan, monitor, control, and evaluate their own learning in order to achieve personal and academic goals.7 These limitations underscore the need for more flexible, learner-responsive educational paradigms.
Personalized learning has emerged as a transformative approach aimed at tailoring education to individual learner characteristics, progression patterns, and competency gaps. Personalized learning refers to instructional models that adapt content, pacing, feedback, and assessment based on learner performance data and developmental needs.8 Within health professions education, personalized learning aligns closely with competency-based medical education (CBME), deliberate practice theory, and adaptive learning systems.9,10 It incorporates formative analytics, simulation-based mastery learning, structured mentorship, and adaptive digital platforms to support individualized progression toward clearly defined competencies.11 Unlike traditional models, personalized learning emphasizes mastery-based advancement, learner agency, and continuous feedback loops.
Although personalized learning is increasingly discussed in higher education, its implementation in health professions education remains conceptually fragmented and methodologically heterogeneous. A recent scoping review in health sciences education reported wide variability in definitions, frameworks, and evaluation strategies related to personalized learning interventions.12 Much of the literature focuses on technological tools rather than comprehensive pedagogical redesign, and robust evidence linking personalization to sustained clinical competence remains limited. There is a notable gap in synthesised scholarship examining the core principles of personalized learning, structured implementation strategies in both academic and clinical settings, and measurable educational outcomes relevant to professional practice. Addressing this gap is critical as HPE transitions toward competency-based, data-informed, and digitally enhanced models of training.Accordingly, this study aims to explore personalized learning in health professions education by examining: (1) the key principles underpinning personalized learning; (2) strategies for fostering personalized learning within academic and clinical environments; and (3) the impact of personalized learning approaches on learning outcomes.
Literature Review Strategy
A structured literature search was conducted to identify relevant studies examining personalized learning within health professions education. The search was performed using the electronic databases PubMed, Scopus, and Google Scholar to capture peer-reviewed journal articles, reviews, and relevant theoretical papers. These databases were selected to ensure broad coverage of medical, health sciences, and educational research literature. The collected literatures was from 1983 to 2025.
Search terms were developed based on the conceptual domains of the review and combined using Boolean operators. The primary keywords included: “personalized learning,” “health professions education,” “medical education,” “learner-centered,” “competency-based education,” “self-regulated learning,” “formative feedback,” “learning analytics,” “strategies for fostering personalized learning,” “key principles,” and “learning outcomes.” Search strings were adapted to the indexing structure of each database, and reference lists of included studies were manually screened to identify additional relevant publications.
Inclusion Criteria Comprised
- Peer-reviewed articles published in English
- Peer-reviewed articles that addressed personalized, adaptive, or competency-based learning approaches within academic or clinical health professions education contexts.
- Both empirical studies (quantitative, qualitative, and mixed methods) and high-quality reviews were considered.
Exclusion Criteria Included
- Opinion pieces without conceptual grounding,
- Non-health education settings,
- Studies lacking clear relevance to personalization principles or outcomes, and non-English publications.
The retrieved literature was screened by two of the authors based on title and abstract, followed by a full-text review to determine eligibility, after that, another 2 authors were revised to eliminate the bais from paper selection. The literature screening was in period from October 2025 to February 2026. Studies were then thematically analyzed (Line-by-Line Coding) and categorized according to three domains guiding this review: (1) key principles of personalized learning, (2) strategies for fostering personalized learning in academic and clinical environments, and (3) impact on educational outcomes.
Results
Key Principles of Personalized Learning in Health Professions Education
Personalized learning in health professions education is grounded in pedagogical principles that shift instruction from uniform content delivery toward adaptive competence development. Core principles include learner agency, learner-centered design, continuous formative feedback, self-regulated learning, and adaptive progression. Together, they enable educators to align learning experiences with performance evidence while maintaining professional standards.
Learner Agency and Autonomy
A central principle of personalized learning is learner agency, defined as the capacity to actively direct one’s learning through goal setting, monitoring, and strategic decision-making. The theoretical foundations of learner agency derive from social-cognitive theory, which emphasizes self-efficacy and intentional action as drivers of motivation and performance.13 In educational settings, autonomy-supportive environments enhance intrinsic motivation, engagement, and persistence.14
Within health professions education, the agency supports the transition from passive knowledge acquisition to active professional formation. When learners participate in selecting clinical cases, determining learning priorities, or adjusting learning pathways, they demonstrate stronger ownership of learning and improved academic outcomes. However, autonomy must be developmentally calibrated. Excessive freedom without structured guidance may increase cognitive load, especially for novice learners navigating complex clinical reasoning tasks. Therefore, personalized learning models must combine learner autonomy with explicit scaffolding and performance standards.
Learner-Centeredness
Personalized learning is fundamentally learner-centered, meaning instructional design begins with learner characteristics rather than curriculum structure. Learner-centered approaches emphasize responsiveness to prior knowledge, readiness, and professional development needs, thereby aligning educational experiences with individual trajectories rather than uniform timelines.8
In health professions education, this principle is particularly relevant because learners enter training with diverse prior experiences and learning needs. Learner-centered approaches enable educators to tailor learning tasks, feedback, and support mechanisms so that each learner can progress toward competence at an appropriate pace. This orientation transforms education from content delivery into competence development. Rather than assuming uniform readiness, learner-centered models recognize variability as a normal feature of professional development and use it to inform adaptive instruction.
Self-Regulated Learning and Metacognition
Self-regulated learning (SRL) constitutes another foundational principle of personalized learning. SRL involves the ability to plan, monitor, and evaluate one’s learning processes, thereby enabling learners to adapt strategies based on performance feedback.7 Within health professions education, SRL is essential because professional competence requires continuous adaptation beyond formal training. Evidence from the reviewed studies indicates that strategies such as reflective practice, structured debriefing, and self-assessment tools promote metacognitive awareness and support individualized learning adjustments.
Structured reflection is particularly important in clinical training. Guided reflective exercises allow learners to reconstruct reasoning processes, identify cognitive biases, and align future actions with professional standards, thereby strengthening adaptive expertise and long-term professional development.4,9
Adaptation to Individual Needs
The defining feature of personalized learning is the capacity to adapt instruction to individual learner needs. Adaptation may involve adjustments in pacing, learning modalities, instructional resources, or remediation strategies. In health professions education, adaptation is often operationalized through competency frameworks that allow progression based on demonstrated mastery rather than time spent in training.9 Such adaptive models support safe competence development by ensuring that learners address gaps before advancing to more complex clinical responsibilities.
The literature emphasizes that adaptation to individual needs is a central principle of personalized learning in health education. Personalized learning approaches recognize that students differ in their prior knowledge, learning pace, motivation, professional goals, and preferred learning strategies. Consequently, educational programs should provide flexible and learner-centered experiences that allow students to progress according to their individual needs and competencies rather than through a uniform curriculum.15
Several studies highlight the role of adaptive learning technologies in supporting individualized education. Adaptive systems use learner data, performance analytics, and feedback mechanisms to tailor educational content, assessments, and learning pathways to each student’s level of understanding and progress. These approaches have been associated with improved academic performance, engagement, and learner satisfaction because students receive targeted support and appropriately challenging material.16
The literature also links adaptation to individual needs with the development of self-directed and lifelong learning skills. In health professions education, personalized learning encourages students to identify their own learning gaps, set goals, and take responsibility for continuous professional development. This is particularly important in modern healthcare systems where knowledge and technologies evolve rapidly.15 In addition, scholars argue that effective personalized education requires educators to acknowledge learner variability and design instruction that is responsive to students’ cognitive, emotional, and professional development needs. Flexible curricula, individualized feedback, and competency-based progression are viewed as essential components of adaptive education models.17 Overall, the literature suggests that adapting education to individual learner needs enhances engagement, promotes deeper learning, supports competency development, and prepares healthcare graduates for continuous adaptation within complex healthcare environments.
Strategies for Fostering Personalized Learning in Health Professions Education
Health professions education is on the edge of a transformative shift towards personalized learning, where individualized approaches cater to the diverse needs and preferences of learners. Recognizing that no two learners are alike, educators in health professions education are increasingly embracing implementation adapting strategies that foster personalized learning environments. These strategies include curriculum design, instructional methodologies, assessment methods, faculty development, and integration of real-world clinical scenarios. Studies included in the current review indicated that several strategies have been suggested to foster personalized learning in health professions education.
Curriculum Design
Curriculum design acts as a framework for implementing personalized learning in health professions education. At the program level, curriculum structure determines whether personalization is systematically incorporated rather than applied inconsistently. Several studies have discussed curriculum-level strategies that facilitate personalized learning.
Personalized Learning Goals
The central curricular strategy is to align learning goals with individual learner needs. In this context, personalized models and learning objectives should be adapted to reflect unique needs and goals. Evidence suggests a significant enhancement in student achievement when implementing individualized goal-setting practices based on the learner profiles.8 Moreover, in health professions education, Frank et al 2010 demonstrates that competency frameworks make individualized goal setting concrete and measurable.9 This can be achieved when competencies are clearly defined, and remediation is targeted to specific competency gaps.9 From a self-regulated learning perspective, Zimmerman et al 2002 showed that individualized goals create a reference point for monitoring and self-correction.7
However, studies have indicated that even when personalized goal setting is implemented alone, it does not guarantee achievement gains unless learners understand how to set effective goals.7 Moreover, flexibility without clear competency boundaries may increase ambiguity and cognitive load among learners.18 Therefore, personalization of goals must occur within clearly defined curricular expectations.
Competency-Based Progression and Mastery Learning
Competency-based progression is defined when the progress of each student toward clearly defined goals is continuously assessed, and when a student is ready to demonstrate competency.9 In the medical context, Frank et al 2010 describe Competency-Based Medical Education (CBME) as an outcomes-based model where progression depends on demonstrated competency rather than time.9 This strategy aligns strongly with personalized learning principles by emphasizing mastery rather than time-based progression. In addition, it has significant implications for the planning of medical curricula by enhancing lifelong learning readiness, emphasizing observable competencies, requiring self-monitoring, and integrating frequent formative assessment and adaptive expertise.8,9 Furthermore, this strategy inherently supports SRL by encouraging goal setting, performance tracking, and self-evaluation.7,9
Autonomy-Supportive Learning Environment
Autonomy and self-regulated learning are widely implemented in professional health academia. As described by Bandura et al.14 This strategy can promote SRL by granting learners control over pacing, sequencing, and modality of instruction. It also enhances intrinsic motivation, goal orientation, and strategic engagement. So, instruction becomes flexible and responsive to individual needs.7,13,19
Personalized learning environments shift the learner from passive recipient to active decision-maker by putting specific goals, controlling learning, and personalizing their ownership. Moreover, autonomy-supportive learning design can be interpreted in many ways and might include a self-directed learning module, choice of cases/topics, and flexible pacing in online components, which enhance intrinsic motivation and self-regulation because learners engage more deeply when tasks align with readiness and goals.8,14,19,20
From a theoretical perspective, Zimmerman et al suggested that autonomy-supportive environments activate SRL through three phases, which include the forethought phase, performance phase, and self-reflection phase.7 This model suggests a strong planner, strong monitoring, and deep reflection, which have a positive impact on the SRL strategy.7,19 Despite all these positive effects, autonomy requires structured support and should be developmentally calibrated. Literature suggests that autonomy without structured instructional support like clear learning objectives, step-by-step guidance, and regular feedback – especially early in training- may overwhelm novice learners, particularly in complex clinical settings (diagnosis, patient management, ICU), where the cognitive load is already high.21 Therefore, personalization must be balanced with structured guidance.
Modular and Flexible Learning Pathways
A modular curriculum is an educational structure in which the program is organized into discrete, self-contained modules, each with clearly defined learning outcomes, assessment criteria, and progression requirements. This strategy allows learners to engage with content according to their readiness and need, and targets mastery of specific competencies.22 This type of curriculum is a learning pathway that becomes responsive to individual readiness and performance data by allowing the learners to focus on specific weak domains and target remediation to specific modules.
Studies have demonstrated improvements in engagement and retention when applying adaptive and modular learning approaches in higher education.23,24 In health professions education, a modular curriculum supports safe mastery development by enhancing clinical education practice and allowing the students to repeat complex practice skills in simulation modules. Therefore, this strategy allows learners to revisit complex domains while progressing in areas of strength.5
Modular flexibility enables personalization; however, flexible learning pathways must be balanced with structured guidance and competency alignment. Without structured academic learning support, this flexible strategy may provoke negative risks, such as fragmentation of the curriculum, loss of integration between competencies, and cognitive overload from too many choices.21 Accordingly, modularization must remain aligned with competency frameworks to preserve professional standards.
Structured Reflective Practice and Debriefing
Structured reflective practice is a guided and systematic process in which learners critically analyze their actions, decisions, and underlying reasoning using explicit prompts or facilitated discussion to improve future performance.25 In health professions education, reflective practice represents a key metacognitive strategy because it allows learners to adjust reasoning during performance by reconstructing their reasoning steps, identifying errors or biases, and comparing performance to standards. Structured reflection promotes personalization because reflection aligns learning adjustments with individual cognitive needs, such as giving individualized feedback that helps the learners to identify their own specific performance gaps. In clinical education, simulation-based training with guided debriefing has demonstrated positive effects on clinical reasoning and reflective capacity.5
However, research indicates that active learning improves performance only if accompanied by structured reflection. Without a good structure, learning remains superficial and episodic rather than developmental.26 Thus, personalization must incorporate structured reflection prompts and guided feedback.
Assessment Strategies
Formative Assessment
Assessment strategies are a fundamental component that influences personalized learning in health professions education. It provides continuous performance data, assessment mechanisms that enable individualized progression, targeted remediation, and metacognitive regulation. A holistic approach to learner assessment integrates a blend of formative and summative assessments. Formative assessment guides learning while summative assessment judges learning.27 Formative assessment functions as a core mechanism for personalization by generating ongoing information about learner performance. Unlike summative assessments, formative strategies provide developmental opportunities for learners to identify knowledge gaps and adjust learning strategies before high-risk evaluation.27 By embracing a multifaceted approach to assessment, educators can provide meaningful feedback, foster critical thinking, and support continuous improvement among.27
In health professions education, performance-based assessment supports competence development. It includes simulation-based assessments, workplace-based assessments, OSCE with feedback, clinical logbooks, and other structured clinical skills evaluations, which serve a formative purpose.5,28 In the same context, studies also demonstrated that formative assessment enhances performance monitoring and supports adaptive learning behaviors, especially when it is timely addressed.27 During simulation and clinical training, this structured feedback enables learners to identify knowledge gaps, adjust learning strategies, and monitor performance trajectories, which strengthens reflective practice and performance regulation.3,5
Although formative assessment is very important, its quality may be influenced by the assessment tool used.21 For instance, internet-based tools alone do not guarantee learning gains, and analytics data alone do not guarantee a behavioral change. Furthermore, the risks of over-assessment and passive compliance rather than reflection might influence the data results unless learners are trained to interpret and apply feedback effectively.21,29
Timely and Actionable Feedback
Timely feedback is a comment that should be delivered soon after performance. It should be specific, linked to predefined competencies, and include clear guidance for improvement. Timely feedback supports personalization by identifying individual performance gaps, enabling targeted remediation, and aligning improvement with competency standards.30 In this context, learning adjustments become individualized rather than generalized and serve as an external regulator that strengthens internal regulation.7,30
In simulation and clinical education, feedback transforms clinical performance into learning episodes because it shows a positive impact on enhancing clinical reasoning and clarifying diagnostic errors.5 A study by Hattie 2007 showed that effective feedback should answer three main questions: Where am I going? How am I going? And what next? This strategy is used to help the learner to focus on the task, not the person, and consequently guides the strategic planning.30 Nevertheless, literature showed that delayed feedback loses impact and generic comments lack direction. Thus, the quality and pedagogical framing of the feedback matter more than frequency and determine its personalization value.29
Self-Assessment Strategy
Self-assessment represents a strategy for fostering metacognitive awareness when learners become evaluators of their own competence. This tool includes many items, such as reflective portfolios and competency checklists, which encourage learners to evaluate their own performance by comparing it against predefined standards and documenting strengths and weaknesses. Self-assessment supports personalized learning by fostering the instructional adjustments that originate not only from the faculty but also from the learner. This can be interpreted when the progress tracking becomes individualized, and the improvement goals become self-generated.7
Within the competency-based medical education domain, the self-assessment is frequently based on structured competencies that provide reference points for accurate self-evaluation, such as milestone progression systems and documentation that support progression decisions.9 When guided by clear criteria, self-assessment strengthens SRL, by enabling learners to compare performance to explicit criteria, identify discrepancies, and revise goals.7 The major limitation of this strategy is that, without external calibration, such as good feedback, learners often overestimate or underestimate their competence, which puts the accuracy of this tool in question.31
Learning Analytics and Feedback Loops
Learning analytics provides learners with visual representations of performance trends, fostering metacognitive awareness of strengths and weaknesses. This strategy makes learning progress visible and measurable. Studies suggest that this strategy can identify individual performance patterns, detect learning gaps early, provide meaningful data-informed progression decisions, and allow the faculty to tailor adequate and personalized support to the learner. In addition, studies also indicate that learning analytics strategy cannot be effective unless learners are trained to interpret data, faculty guide the interpretation, and it is integrated into structured feedback systems.24,32,33
However, learning analytics should follow the pedagogic and ethical rules. Without pedagogical mediation, data visibility alone does not change behavior and does not guarantee improved learning outcomes.29 In addition, ethical issues such as risk of data profiling and privacy concerns might be a source of limitation and should also be considered.34
Faculty Development and Capacity-Building
Faculty Training for Personalization, Feedback, Analytics Use, and Facilitation
The successful implementation of personalized learning strategies in health professions education depends essentially on faculty competence in instructional design, feedback delivery, and data interpretation. Personalization only functions when faculty can mediate it, and without faculty mediation, the systems remain technical, the students may not understand expectations, and the feedback loses impact.9
In order to achieve personalized learning goals, the faculty must be trained to align learning objectives with competency frameworks, break down competencies into teachable milestones, and structure modular or flexible pathways coherently. This requires the faculty member to shift from the traditional content delivery mode, such as content transmitter and lecture-based delivery, toward coaching performer and learning designer.9
Faculty coaching skills must also include the ability to deliver feedback that is specific and performance-based and engaging learners in reflective dialogue.2 Faculty member should know how to guide simulation debriefings and use reflection prompts strategically as well as help learners in interpreting data analytics, understand dashboards and indicators, and explain performance trends.5,25,29,33 Studies indicate that faculty development influences not only educator behavior but also learner performance. The faculty development strategies improve feedback quality, enhance assessment alignment, promote reflective teaching practices, and indirectly improve learner outcomes.35,36
The rigidity of the faculty members toward this training causes superficial personalization strategies, affects the quality of feedback, and leads to the misuse or misinterpretation of the data. For this reason, faculty development should not be considered as optional but as a structural infrastructure. Therefore, as a professional development strategy, institutions must provide structured faculty development programs, allocate protected time for training, offer training in feedback literacy, provide analytics training workshops, and create communities of practice.3,21
Implementation Support and Change Management
Personalized learning strategies are structurally complex, interdependent, and have multilevel status (curriculum, instruction, assessment, technology). For this reason, they cannot function in isolation but require system-level alignment.9,37 Along with individual faculty training and skills, institutional infrastructure and change management processes are critical for achieving the personalized learning goals and embedding personalized learning sustainably; otherwise, the curriculum may not align with assessment, and analytics may not align with competencies. This support should include: 1. curricular Infrastructure such as clear competency frameworks and integrated assessment systems 2. Technological Infrastructure, such as reliable learning management systems and analytics dashboards, 3. Administrative Infrastructure such as faculty workload adjustment and leadership endorsement.9
In health professions education, personalization initiatives need structural changes and often require revising assessment policies, adjusting faculty teaching loads, and training faculty in analytics use. Without systematic planning, the feedback may lose quality, the learners might be confused, and the curriculum design remains fragmented.21 In addition, an ethical site should also be considered because sustainable personalization requires ethical governance. Institutions must establish transparent data policies, clear consent procedures, and ethical review mechanisms.34 Thus, sustainable personalized learning requires both pedagogical capacity-building and institutional change management strategies.
Impact on Educational Outcomes
The adoption of personalized learning principles in health professions education leads to enhanced educational outcomes in the form of increased engagement, improved learning outcomes, and enhanced readiness for clinical practice.12 Health professions education is significantly impacted by learner background diversity, varying prior learning experiences, and diverse learning preferences. Personal learning allows for increased autonomy in learning journeys, enabling learners to take charge of their learning and make choices regarding activities that suit their preferences and needs. Furthermore, health professions educators can also implement flexible and adaptable learning experiences based on the principles of personal learning.12
Learner Engagement
Engagement is a central outcome of personalized learning and a key predictor of knowledge retention.26 By placing the learner at the centre of the educational experience, personalized learning fosters autonomy and ownership, which in turn promote voluntary, active participation in learning activities.38 This sense of control strengthens intrinsic motivation and sustains engagement, contributing to deeper retention of learned material.20,26 In health professions education specifically, allowing learners to choose among instructional modalities — lectures, simulation, case-based work, or self-paced modules — has been linked to better educational outcomes.39
Knowledge Retention
Knowledge retention is a powerful learning outcome because it enables learners to draw on previously learned information when faced with new challenges or questions. Personalised learning experiences in bespoke learning environments can significantly enhance knowledge retention. Knowledge retention can be strengthened through personalized learning experiences that incorporate smart technology and adaptive instruction technology. These technologies are some of the characteristic features of personal learning.24 Clinical skills development is one of the most fundamental outcomes of health professions education. It is essential to ensure that health professionals have the skills to provide high-quality patient care. Personal learning approaches create stratagems suited to developing these skills.40 Simulation increases clinical skills development in traditional and bespoke educational settings.40 Simulation–based training refers to computer-based training and case-based assessments that mimic real-world clinical training scenarios.28,40 These trainings offer learners valuable clinical training experiences while protecting them and ensuring that they are prepared for the challenges and difficulties that can be found in actual clinical practice.41 Evidence indicates that simulation-based training increases clinical skills development because it enables professionals to practice over and over again, receiving feedback each time and the opportunity for deliberate practice.37 Numerous scenarios can be simulated, including patient interactions, training in procedures, and making clinical decisions with the feedback of trained educators and peers.40
Individualized Instruction also enhances the development of clinical skills in learners when combined with other learning experiences. In medical education for example, early clinical training experiences are important for the development of practical clinical skills.20 Inserting clinical training experiences into the curriculum from the start can expose learners to a great variety of patients in diverse health service settings.16 Furthermore, incorporating diverse and plentiful clinical training experiences into the early phase of the medical education curriculum exposes learners to a variety of patient needs, cases, and challenges in various phases of life.
Long-Term Professional Competence
Long-term professional competence is an important educational outcome in health professions education because it ensures that health professionals have the knowledge and skills they need to perform their jobs well, even if there are changes in their profession. Personal Learning approaches create stratagems that enhance this outcome.42 Personal Learning approaches used in addition to competency-Based education also enhance long-term professional competence because they account for changes in practices among medical professionals over time. Medical professionals encounter numerous changes in their careers that render their current level of knowledge insufficient for their practice. Changes in practice occur at a fast pace. New innovations can emerge in a short period and become established practices. These changes can make previous learning obsolete.
Personalised learning environments enhance learners’ long-term professional competence because they account for changes that occur over the course of medical practitioners’ careers. Using innovative pedagogical methods and digital resources available anytime and anywhere, Personalised learning environments ensure that learners always have access to information relevant to the practices that recently emerged. Even if participants in learning engagements may not be currently practicing medicine, custom learning experiences improve their ability to perform well if they resume their practice in the future. These experiences have been demonstrated and validated through research. In summary, the evidence indicates that individualized instruction indeed enhances the learning outcomes reported by health profession learners in many areas.
Discussion
This review approached personalized learning in health professions education (HPE) not as a single intervention but also as a pedagogical orientation that crosses curriculum design, assessment, faculty practice, and learning technology. The underlying principles are consistent, but the terminology is not. The strategies differ in how well they are supported by evidence (Table 1). Furthermore, most outcome claims are based on short-term measures rather than long-term ones. This discussion takes each principle in turn, sets the findings against prior literature, and ends by returning to a question raised in the introduction: whether the field has converged on what personalized learning actually is.
Key Principles: Convergence and Unresolved Tensions
The principles identified in this review are learner agency, learner-centred design, formative feedback, self-regulated learning, and adaptive progression, and they are aligned largely with those reported in other studies of student-centred and adaptive learning.19,24 These findings suggest that even though the terminology varies across studies, the conceptual frame remains the same.12
Based on the literature, two principles seem to compete: autonomy and feedback. The first principle (Autonomy), based on Bandura’s theory, holds that people perform well when they believe in their own ability and when they intentionally choose what to do13. This is supported by many studies in health sciences programs showing that when students are given structured ways to direct their own learning, they take greater ownership of it.14,43 On the other hand, studies based on cognitive load theory show that excessive flexibility burdens new learners, especially when they have to manage complex diagnostic tasks.44 In our opinion, this can be resolved by matching the approach to the learner’s stage of development, giving learners independence with support structures in place at the beginning of their training and gradually handing over decision-making as they become more skilled. Unfortunately, most studies do not clearly state what level of learner they studied, which makes it difficult to compare findings across the literature.12
The second principle concerns feedback. Formative feedback is widely mentioned in the literature as the driving mechanism of personalization.27 However, its value depends on three main properties: timing, alignment with competencies, and practical usability, which many primary studies fail to document.30 The principle itself is widely accepted, but precisely when and how it personalizes learning has not been clearly demonstrated.
Strategies: What the Evidence Supports and What It Presumes
The reviewed studies show that three groups of strategies are most strongly evidenced: competency-based progression with formative assessment, simulation training that combines deliberate skill practice with tailored feedback sessions, and the performance analytics that shape instructional decisions.5,9,29 A fourth strategy concerning the faculty role redefinition is commonly recommended but less well evidenced.35
Frank et al (2010) showed that competency-based progression aligns advancement with demonstrated mastery rather than time-based completion9 Furthermore, Harden et al (1999) found that outcome-based frameworks enable focused remediation of identified weaknesses22 Among personalization strategies, competency-based progression represents the most established evidence base in HPE. Previous studies showed that when a modular curriculum is built on this idea, it might allow learners to revisit challenging topics while advancing in others;5 however, modularization without a competency framework can also fragment rather than personalize.21
Literature shows that simulation accounts for most of the procedural-skills literature,40,41 but isolating what personalization itself is challenging because the simulation’s design focuses on practice with individualized feedback, which is already a form of personalization. So “simulation works” and “personalization works” become impossible to separate. The honest reading here is that simulation evidence supports adaptive instruction broadly; whether it validates “personalized learning” as a distinct construct is less clear.
Among all these strategies, learning analytics offer the most novel implementation pathway, but their educational value depends on pedagogical mediation and ethical governance, not on the platforms themselves.29,34 The literature we reviewed focuses more on analytics platforms than on how teaching with analytics affects learning, and this represents an important direction for future studies.
Lastly, despite many studies’ recommendations for faculty to shift from content transmitters to performance coaches,35,36 HPE evidence remains mostly descriptive rather than evaluative. Long-term implementation will require faculty training programmes to be evaluated using learner outcomes as well as institutional commitment, supporting infrastructure, and managed organizational change, as mentioned by Damschroder et al’s study.37
Interpreting the Outcome Evidence
The outcomes reported in the reviewed literature, including better engagement, stronger retention, sharper clinical reasoning, and greater readiness for practice, appear consistently across diverse educational contexts, although careful reading is needed before adopting this.12,24
Most of the reviewed studies focus on immediate outcomes such as satisfaction, perceived engagement, and short-term recall rather than long-term outcomes like clinical performance two years post-graduation and patient outcomes. This is significant because the theoretical promise of personalized learning lies in long-term professional adaptability, not short-term test gains, yet evidence for those long-term outcomes is limited.20,26
A second contradiction emerges in the literature. Studies that emphasize learner autonomy report higher engagement14,43 while studies of beginners show mental overload when autonomy is introduced before readiness.44 In our opinion, personalization functions differently at different stages of expertise; however, this distinction is rarely articulated in the primary literature, which often treats personalization as a uniform intervention. Future studies should specify the stage of training of participants and the level of structured support provided, rather than presenting personalization as a single concept.
A third concept is that much of the procedural-skills literature comes from simulation studies,16,40–42 describe environments that are already highly individualized and deliberate practice with adaptive feedback. It is therefore not possible, with the available research, to determine whether the reported gains come from the personalization only or from the broader pedagogical design of simulation training itself. This is a meaningful confound when interpreting effect sizes in the field.
Revisiting the Conceptual Variability Problem
At the beginning of this review, we used Ali et al’s study, stating that there is substantial heterogeneity in how personalized learning is defined, structured, and measured across health sciences research.12 What our study adds is confirmation, but not resolution.
Across the studies reviewed, the term “personalized learning” was attached to interventions as adaptive e-learning platforms,24,39 mentor-guided personal goal-setting, modular curriculum structures, and simulation-based deliberate practice.40,41 Some of these share a pedagogical core such as learner agency, formative feedback and mastery-orientation, whereas others are linked by terminology alone.
Unless researchers settle on a common definition that distinguishes personalization from similar approaches such as adaptive learning, self-directed learning, competency-based education, evidence reviews will continue to merge fundamentally different interventions and prevent identification of what actually causes the reported benefits. The dynamic model recently proposed by Tetzlaff et al17 provides a rational starting point, but consensus across professional educational bodies like AMEE, ASME, or equivalent would benefit the field more at this stage than additional outcome studies from individual settings.
Limitation
Although the reviewed literature generally reports positive outcomes associated with personalized learning in health professions education, several methodological limitations should be considered when interpreting these findings. Many studies relied heavily on self-reported data, such as learner satisfaction, perceived engagement, or self-assessed competence, which may introduce response and social desirability bias. In addition, numerous studies used short follow-up periods, limiting the ability to evaluate the long-term impact of personalized learning on clinical competence, professional performance, and lifelong learning behaviors. Several studies also lacked robust experimental designs, including the absence of control groups or randomization, making it difficult to determine whether reported improvements were directly attributable to personalized learning interventions rather than external factors. Furthermore, variations in study settings, sample sizes, educational technologies, and assessment methods reduced comparability across studies and limited the generalizability of findings. The literature also showed inconsistency in defining personalized learning, adaptive learning, and competency-based education, which may affect conceptual clarity and interpretation of outcomes.
Although this review provides useful insights into personalized learning in health professions education, several limitations related to the study selection process should be noted. The inclusion and exclusion criteria may have introduced selection bias. The review was also limited by the choice of databases and search terms, which could have led to the omission of relevant studies. Restricting studies to English languages also have introduced language and availability bias, reducing the diversity of included evidence. Finally, variation in definitions and approaches to personalized learning across studies created heterogeneity, making comparison and synthesis more challenging.
Recommendation
To enhance the personalised learning in health profession education it is recommended to redesign the curricula to be more oriented about around competency-based and modular structures and ensure alignment between learning objectives, assessments, and clinical competencies to support individualized learning pathways, it is necessary allowing flexible, learner-paced progression with clearly defined learning outcomes.
Also, Implementation structured faculty development programs focused on feedback literacy, coaching skills, and use of learning analytics. Train educators to deliver timely, specific, and actionable feedback and to support reflective and self-regulated learning in students. Invest in integrated digital learning infrastructure (eg., LMS, simulation platforms, analytics dashboards) and establish clear policies for data use and ethical governance. Promote institutional change management strategies that support sustainable adoption of personalized learning approaches.
Conclusion
This narrative literature review examined Personalised learning in health professions education’s theoretical foundations, implementation methodologies, and educational outcomes. Personalized learning shifts from uniform instruction to adaptive, learner-centered educational models that match teaching strategies to individual learner needs, competencies, and professional development trajectories, according to the analysis. Personalized learning integrates learner agency, self-regulated learning, adaptive progression, competency-based assessment, and ongoing formative feedback. Collectively, these concepts foster introspective, independent health workers who can navigate complex clinical contexts and changing healthcare demands.
The review found various evidence-based options for application of individualized learning in academic and clinical training. Adaptive learning platforms, intelligent tutoring, competency-based curriculum, learning analytics–driven feedback, simulation-based education, and structured mentorship models are examples. These methods let educators customize learning routes, track student progress, and give targeted support to address strengths and learning gaps when carefully incorporated into educational frameworks. Personalized learning should not replace stringent competency standards; rather, it enables flexible pathways to professional competencies, according to the literature.
In the studied literature, personalized learning approaches led to favorable educational outcomes. Better learner engagement, knowledge retention, academic motivation, clinical reasoning, and professional practice preparedness. In quickly changing clinical and technology landscapes, tailored learning environments promote deeper reflective practice and lifetime learning competencies, which healthcare workers need. The literature notes persisting issues with teacher preparation, technical infrastructure, curricular alignment, and institutional support, notwithstanding these promising results. Unplanned institutional tactics can divide personalized learning into separate educational initiatives.The strategic integration of personalized learning in health professions education requires curriculum redesign, faculty development, investment in digital learning technologies, and alignment with competency-based education frameworks. Personalized learning treatments should be empirically evaluated in longitudinal and multi-institutional studies that analyze educational and clinical practice results, rather than descriptive descriptions.
Finally, personalised learning transforms health professions education by meeting individual learner requirements while preserving professional competency standards. Personalised learning can improve learner engagement, clinical competence, and future healthcare professionals’ readiness for modern healthcare systems when integrated into academic and clinical training.
Abbreviations
HPE, Health professions education; CBME, Competency-Based Medical Education; SRL, Self-regulated learning.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Juhi A, Pinjar MJ, Marndi G, Hungund BR, Mondal H. Evaluation of blended learning method versus traditional learning method of clinical examination skills in physiology among undergraduate medical students in an Indian medical college. Cureus. 2023;15(4):e37061. doi:10.7759/cureus.37061
2. Harden RM. The integration ladder: a tool for curriculum planning and evaluation. Med Educ. 2000;34(7):551–14.
3. Spencer JA, Jordan RK. Learner centred approaches in medical education. BMJ. 1999;318(7193):1280–1283. doi:10.1136/bmj.318.7193.1280
4. Irby DM. Excellence in clinical teaching: knowledge transformation and development required. Med Educ. 2010;44(8):776–784.
5. Cook DA, Hatala R, Brydges R, et al. Technology-enhanced simulation for health professions education: a systematic review and meta-analysis. JAMA. 2011;306(9):978–988. doi:10.1001/jama.2011.1234
6. Frenk J, Chen L, Bhutta ZA, et al. Health professionals for a new century: transforming education to strengthen health systems in an interdependent world. Lancet. 2010;376(9756):1923–1958. doi:10.1016/S0140-6736(10)61854-5
7. Zimmerman BJ. Becoming a self-regulated learner: an overview. Theory Pract. 2002;41(2):64–70. doi:10.1207/s15430421tip4102_2
8. Pane JF, Steiner ED, Baird MD, Hamilton LS. Continued Progress: Promising Evidence on Personalized Learning. RAND Corporation; 2015.
9. Frank JR, Snell LS, Cate OT, et al. Competency-based medical education: theory to practice. Med Teach. 2010;32(8):638–645. doi:10.3109/0142159X.2010.501190
10. Ericsson KA. Deliberate practice and the acquisition and maintenance of expert performance in medicine and related domains. Acad Med. 2004;79(10):S70–S81. doi:10.1097/00001888-200410001-00022
11. Cook DA, Triola MM. What is the role of e-learning? Looking past the hype. Med Educ. 2014;48(9):930–937. doi:10.1111/medu.12484
12. Ali M, Wahab IBA, Huri HZ, Yusoff MSB. Personalised learning in higher education for health sciences: a scoping review. BMC Med Educ. 2025;25(1):969. doi:10.1186/s12909-025-07565-1
13. Bandura A. Toward a psychology of human agency. Perspect Psychol Sci. 2006;1(2):164–180. doi:10.1111/j.1745-6916.2006.00011.x
14. Vansteenkiste M, Niemiec CP, Soenens B. The development of the five mini-theories of self-determination theory. Advances in Motivation and Achievement. 2009;16:105–165.
15. Wilkes S, Maggio LA, Martin PC, Melton J, Zheng B. Self-directed learning in health professions education: a systematic review and meta-analysis. Perspect Med Educ. 2026;15(1):37–52. PMID: 41626409; PMCID: PMC12857615. doi:10.5334/pme.2128
16. Giles E, Guerrero K. A simulated clinic to build interprofessional and authentic learning opportunities for shaping future practice in medical radiation professionals. J Med Imaging Radiat Sci. 2024;55(3):101437. doi:10.1016/j.jmir.2024.101437
17. Tetzlaff L, Schmiedek F, Brod G. Developing personalized education: a dynamic framework. Educ Psychol Rev. 2021;33:863–882. doi:10.1007/s10648-020-09570-w
18. Södersved Källestedt ML, Hidefjäll P. Self-directed learning in clinical practice using a mobile skills training system: a mixed methods study. BMC Med Educ. 2025;25:1515. doi:10.1186/s12909-025-08127-1
19. Metsälä E, Törnroos S. Benefits and outcomes of student-centred learning strategies in a healthcare higher education institution setting: a scoping review. Am J Nurs Stud. 2021;2(1):1008.
20. Deci EL, Ryan RM. The “what” and “why” of goal pursuits: human needs and the self-determination of behavior. Psychol Inq. 2000;11(4):227–268. doi:10.1207/S15327965PLI1104_01
21. Cook DA, Levinson AJ, Garside S, Dupras DM, Erwin PJ, Montori VM. Internet-based learning in the health professions: a meta-analysis. JAMA. 2008;300(10):1181–1196. doi:10.1001/jama.300.10.1181
22. Harden RM, Crosby JR, Davis MH. Outcome-based education: part 1—an introduction to outcome-based education. Med Teach. 1999;21(1):7–14. doi:10.1080/01421599979969
23. Koedinger KR, Corbett AT. Technology brings learning sciences to the classroom. In: Sawyer RK, editor. The Cambridge Handbook of the Learning Sciences.
24. du Plooy E, Casteleijn D, Franzsen D. Personalized adaptive learning in higher education: a scoping review of key characteristics and impact on academic performance and engagement. Heliyon. 2024;10(21):e39630. doi:10.1016/j.heliyon.2024.e39630
25. Schön DA. The Reflective Practitioner: How Professionals Think in Action. Basic Books; 1983.
26. Freeman S, Eddy SL, McDonough M, et al. Active learning increases student performance in science, engineering, and mathematics. Proc Natl Acad Sci U S A. 2014;111(23):8410–8415. doi:10.1073/pnas.1319030111
27. Black P, Wiliam D. Developing the theory of formative assessment. Educ Assess Eval Account. 2009;21(1):5–31. doi:10.1007/s11092-008-9068-5
28. Kononowicz AA, Woodham LA, Edelbring S, et al. Virtual patient simulations in health professions education: systematic review. J Med Internet Res. 2019;21(7):e14676. doi:10.2196/14676
29. Macfadyen LP, Dawson S. Numbers are not enough: why e-learning analytics failed to inform an institutional strategic plan. Educ Technol Soc. 2012;15(3):149–163.
30. Hattie J, Timperley H. The power of feedback. Rev Educ Res. 2007;77(1):81–112. doi:10.3102/003465430298487
31. Eva KW, Regehr G. Self-assessment in the health professions: a reformulation and research agenda. Acad Med. 2005;80(10):S46–S54. doi:10.1097/00001888-200510001-00015
32. Bienkowski M, Feng M, Means B. Enhancing Teaching and Learning Through Educational Data Mining and Learning Analytics. U.S. Department of Education; 2014.
33. Viberg O, Hatakka M, Bälter O, Mavroudi A. The current landscape of learning analytics in higher education. Comput Human Behav. 2018;89:98–110. doi:10.1016/j.chb.2018.07.027
34. Slade S, Prinsloo P. Learning analytics: ethical issues and dilemmas. Am Behav Sci. 2013;57(10):1510–1529. doi:10.1177/0002764213479366
35. Steinert Y, Mann K, Centeno A, et al. A systematic review of faculty development initiatives. Med Teach. 2016;38(8):769–786. doi:10.1080/0142159X.2016.1181851
36. Steinert Y. Faculty development in competency-based medical education. Med Teach. 2019;41(4):362–369.
37. Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice. Implement Sci. 2009;4:50. doi:10.1186/1748-5908-4-50
38. Weimer M. Learner-Centered Teaching: Five Key Changes to Practice. Jossey-Bass; 2013.
39. El-Sabagh HA. Adaptive e-learning environment based on learning styles and its impact on development students’ engagement. Int J Educ Technol High Educ. 2021;18:53. doi:10.1186/s41239-021-00289-4
40. Hicke Y, Geathers J, Rajashekar N, et al. MedSimAI: simulation and formative feedback generation to enhance deliberate practice in medical education. arXiv. 2025.
41. Kassutto S, Clancy C, Harbison S, Tsao S. A virtual simulation-based clinical skills course. Clin Teach. 2024;21(4). doi:10.1111/tct.13727
42. Xue H, Lu Y, Liu L. Efficacy of problem-based learning in enhancing health education skills, self-directed learning, and critical thinking among nursing interns: a prospective cohort study. BMC Med Educ. 2025;25:1406. doi:10.1186/s12909-025-07936-8
43. Finn A, Fitzgibbon C, Fonda N, Gosling CM. Self-directed learning and the student learning experience in undergraduate clinical science programs: a scoping review. Adv Health Sci Educ. 2025;30:973–1005. doi:10.1007/s10459-024-10383-7
44. Van Nooijen CCA, de Koning BB, Bramer WM, Van Gog T. A cognitive load theory approach to understanding expert scaffolding of visual problem-solving tasks: a scoping review. Educ Psychol Rev. 2024;36:12. doi:10.1007/s10648-024-09848-3
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.