Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Personalized Biologic Therapy for Refractory Bullous Pemphigoid: Sequential Omalizumab, Dupilumab, and Rituximab
Authors Yu L, Hu G, Zhang Q ![]() , Zhu Y
, Zhu Y ![]() , Chen L, Chen J
, Chen L, Chen J ![]()
Received 28 January 2026
Accepted for publication 30 May 2026
Published 17 July 2026 Volume 2026:19 599596
DOI https://doi.org/10.2147/CCID.S599596
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Lang Yu,1,* Gang Hu,1,* Quanhong Zhang,2,* Yue Zhu,2 Liuqing Chen,2,3 Jinbo Chen2,3
1Jianghan University School of Medicine, Wuhan, People’s Republic of China; 2Department of Dermatology, Traditional Chinese and Western Medicine Hospital of Wuhan, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China; 3Department of Dermatology, Wuhan No.1 Hospital, Wuhan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jinbo Chen, Department of Dermatology, Wuhan No.1 Hospital, No. 215, Zhongshan Avenue, Wuhan, People’s Republic of China, Email [email protected]
Abstract: Bullous pemphigoid (BP) is an autoimmune subepidermal blistering disease that predominantly affects elderly individuals. Systemic corticosteroids remain a mainstay of therapy but are often limited by comorbidities and treatment-related adverse effects. We report a 73-year-old man with refractory BP and multiple comorbidities who underwent sequential biologic therapy with omalizumab, dupilumab, and rituximab. The diagnosis was supported by typical clinical manifestations, subepidermal blistering, markedly elevated anti-BP180 antibody levels, peripheral eosinophilia, and elevated total IgE, although direct immunofluorescence was negative and indirect immunofluorescence was not performed. Omalizumab did not produce an early clinical response within two weeks, but its efficacy could not be fully evaluated because of the short treatment duration. Dupilumab induced the most rapid clinical improvement; however, relapse occurred after treatment discontinuation due to financial constraints. Rituximab was subsequently administered and contributed to sustained disease control and corticosteroid tapering. This case highlights the complexity of individualized biologic selection in refractory BP and suggests that clinical phenotype, serological profile, treatment response, corticosteroid-sparing needs, safety considerations, and economic accessibility should be integrated when developing personalized treatment strategies.
Keywords: Bullous pemphigoid, rituximab, omalizumab, dupilumab
Bullous pemphigoid (BP) is a common autoimmune subepidermal blistering disease that predominantly affects elderly individuals. With population aging, the clinical burden of BP has increased, and management is often complicated by diabetes, infection risk, osteoporosis, neurological disease, and other age-related comorbidities.1 Systemic corticosteroids remain the cornerstone of treatment for moderate-to-severe BP, but prolonged or high-dose corticosteroid therapy may be difficult to sustain in elderly patients with multiple comorbidities.
In recent years, biologic agents targeting different immunological pathways have emerged as potential options for refractory BP. These include omalizumab, which targets IgE-mediated inflammation; dupilumab, which inhibits interleukin-4 and interleukin-13 signaling; and rituximab, which depletes CD20-positive B cells and reduces autoantibody-producing B-cell populations.2 Although individual biologics have been reported in BP,3 evidence regarding the sequential use of multiple biologics in a single refractory patient remains limited. Here, we report a case of refractory BP treated sequentially with omalizumab, dupilumab, and rituximab, highlighting diagnostic challenges, differences in treatment response, and the need to integrate disease mechanisms, comorbidities, drug accessibility, and patient-specific circumstances when individualizing therapy.
A 73-year-old male presented with a 3-month history of widespread erythema, tense blisters, erosions, and intense pruritus involving the trunk and limbs. Prior treatment with methylprednisolone and cyclosporine at a local hospital provided insufficient disease control. He was admitted to Wuhan No.1 Hospital and initially received prednisone 40 mg/day (0.67 mg/kg/day). However, tapering prednisone to 25 mg/day because of poorly controlled diabetes mellitus led to disease recurrence.
Past medical history included lung tumor, type 2 diabetes mellitus, cataracts, cerebral atherosclerosis, left acromioclavicular joint fracture, and remote pulmonary tuberculosis. The patient had no history of immune checkpoint inhibitor therapy, including PD-1, PD-L1, or CTLA-4 inhibitors, and had not received dipeptidyl peptidase-4 (DPP-4) inhibitors before the onset of blistering lesions. Physical examination revealed extensive erythema, tense blisters, and erosions on the trunk and limbs, with minor oral erosions (Figure 1A). The Bullous Pemphigoid Disease Area Index (BPDAI) score was 38, and the Numerical Rating Scale (NRS) score for pruritus was 9.
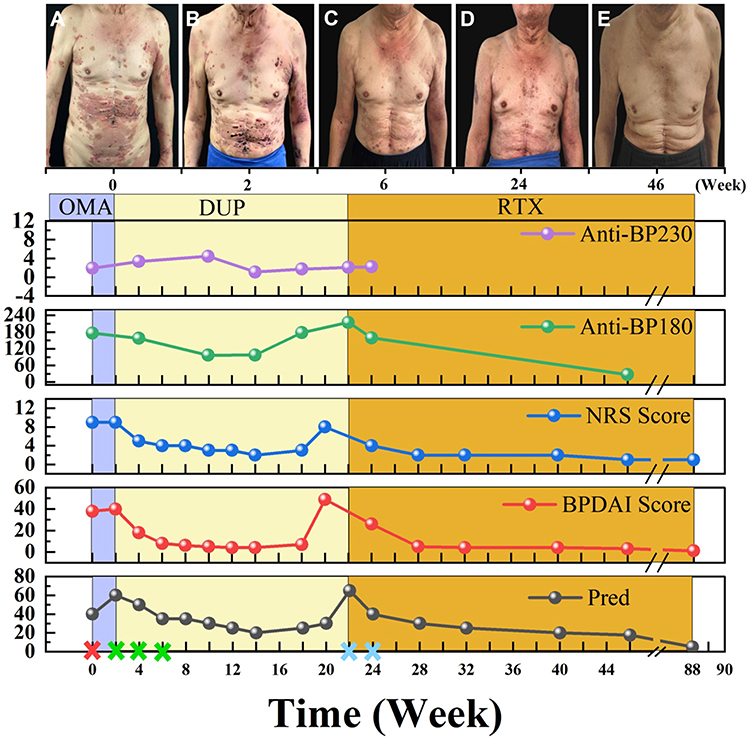 |
Figure 1 Clinical course and laboratory parameters during sequential biologic therapy. (A–E) Representative clinical photographs at the indicated time points shown on the timeline: baseline before biologic therapy (A), week 2 during dupilumab treatment (B), week 6 during dupilumab treatment (C), week 24 after relapse and rituximab initiation (D), and week 46 during follow-up after rituximab treatment (E). The lower panels show changes in anti-BP230 antibody levels, anti-BP180 antibody levels, pruritus severity assessed by the Numerical Rating Scale (NRS), disease activity assessed by the Bullous Pemphigoid Disease Area Index (BPDAI), and daily prednisone() dose over time. Treatment phases are indicated by background colors: omalizumab (OMA), dupilumab (DUP), and rituximab (RTX). Injection time points are marked on the timeline. Abbreviations: BPDAI, Bullous Pemphigoid Disease Area Index; DUP, dupilumab; NRS, Numerical Rating Scale; OMA, omalizumab; RTX, rituximab. |
Histopathological examination demonstrated subepidermal blistering with neutrophilic infiltration and perivascular lymphocytic and neutrophilic infiltrates in the superficial dermis (Figure 2). Direct immunofluorescence was negative for IgG, C3, IgA, and IgM. Indirect immunofluorescence was not performed. Baseline laboratory examination showed markedly elevated anti-BP180 antibody levels (118.12 U/mL; cut-off <9 U/mL), whereas anti-BP230 antibody levels remained below the cut-off value (1.91 U/mL; cut-off <9 U/mL). Peripheral blood eosinophil count was elevated at 1.0 × 109/L, and total IgE(cut-off < 200 IU/mL) was increased to 348 IU/mL. IGRA was positive. Hepatitis B serology showed positive HBsAb and HBcAb.
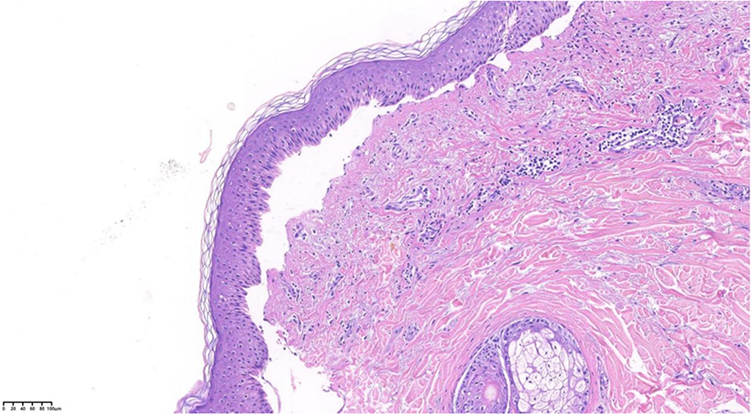 |
Figure 2 Histopathological findings. Histopathological examination showed subepidermal blister formation with neutrophilic infiltration within the blister cavity and perivascular lymphocytic and neutrophilic infiltrates in the superficial dermis. Hematoxylin and eosin staining. |
Based on the patient’s typical clinical presentation, subepidermal blistering on histopathology, markedly elevated anti-BP180 antibody levels, peripheral eosinophilia, and elevated total IgE level, a diagnosis of BP was made. The negative direct immunofluorescence result may have been related to prior systemic treatment, biopsy timing, or sampling factors. The absence of indirect immunofluorescence testing represents a limitation of the diagnostic work-up.
The patient received prednisone 60 mg/day (1 mg/kg/day) for one week without significant improvement in pruritus or skin lesions. Because of the elevated total IgE level and persistent disease activity, omalizumab 300 mg was added. After two weeks, no early clinical improvement was observed (BPDAI 40, NRS 9). Given the limited response and the need to reduce prolonged high-dose corticosteroid exposure in a patient with poorly controlled diabetes and multiple comorbidities, therapy was switched to dupilumab. However, because omalizumab was administered for only two weeks, its therapeutic efficacy could not be fully evaluated, and the lack of early response in this patient should not be interpreted as definitive omalizumab failure.
Dupilumab was administered as a 600 mg loading dose followed by 300 mg every two weeks. Within two weeks, the skin lesions markedly improved (Figure 1B), with BPDAI and NRS scores decreasing to 18 and 5, respectively. Anti-BP180 antibody levels were 157.55 U/mL, whereas anti-BP230 antibody levels remained below the cut-off value (3.36 U/mL). After four doses of dupilumab, treatment was discontinued because of financial constraints. The disease remained controlled during subsequent follow-up while prednisone was tapered from 40 mg/day to 20 mg/day (BPDAI 6, NRS 4; Figure 1C). Anti-BP180 antibody levels decreased to 96.76 U/mL, and anti-BP230 antibody levels remained below the cut-off value (1.93 U/mL).
At week 16 after dupilumab therapy, following prednisone reduction to 20 mg/day, the disease relapsed with recurrent erythema, vesicles, and pruritus (BPDAI 49, NRS 8). Anti-BP180 antibody levels increased to 215.01 U/mL, while anti-BP230 antibody levels remained below the cut-off value (2.10 U/mL). Increasing prednisone to 65 mg/day failed to adequately control the disease (Figure 1D). Rituximab was subsequently selected after consideration of recurrent disease activity, the need for corticosteroid-sparing treatment, comorbidities, treatment accessibility, and the patient’s economic circumstances. Rituximab was administered at 200 mg for two infusions.4 Gradual healing of erosions was observed. Two weeks after the second rituximab infusion, BPDAI and NRS scores improved to 26 and 4, respectively. Systemic corticosteroids were successfully tapered to a maintenance dose of 5 mg/day (Figure 1E). The patient remained in remission without adverse events during 14 months of follow-up.
This case is important because it illustrates both the potential and the limitations of sequential biologic therapy in refractory BP. The patient had advanced age, diabetes mellitus, a history of lung tumor, remote pulmonary tuberculosis, and other comorbidities, making prolonged high-dose corticosteroid therapy undesirable. The clinical course showed different response patterns to three biologics: dupilumab produced the most rapid improvement in skin lesions and pruritus, whereas rituximab was associated with more durable disease control and corticosteroid tapering after relapse. Therefore, the present case supports an individualized approach rather than a fixed biologic sequence.
The diagnosis of BP in this patient warrants careful interpretation. BP is usually diagnosed by integrating clinical manifestations, histopathology, direct immunofluorescence, and serological testing.1 In this case, the diagnosis was supported by typical tense blisters and erosions with severe pruritus, subepidermal blistering on histopathology, markedly elevated anti-BP180 antibody levels, peripheral eosinophilia, and elevated total IgE. However, direct immunofluorescence was negative, and indirect immunofluorescence was not performed. We therefore acknowledge that the negative direct immunofluorescence result and absence of indirect immunofluorescence limited the diagnostic certainty. Possible explanations for the negative direct immunofluorescence include previous systemic treatment, biopsy timing, or sampling factors. In addition, anti-BP230 antibody levels remained below the cut-off value throughout the disease course and should not be interpreted as positive.
Drug-induced BP was also considered. This was particularly relevant because the patient had a history of lung tumor and type 2 diabetes mellitus, and immune checkpoint inhibitors and DPP-4 inhibitors have been implicated in BP-like eruptions or BP induction. A detailed medication history showed no previous exposure to PD-1, PD-L1, or CTLA-4 inhibitors and no use of DPP-4 inhibitors before the onset of blistering lesions. These findings made immune checkpoint inhibitor-associated BP and DPP-4 inhibitor-associated BP less likely in this case.
The selection of omalizumab was supported by the patient’s elevated total IgE level and by the role of IgE-mediated inflammation in BP.5 Omalizumab, a recombinant humanized anti-IgE monoclonal antibody, binds circulating IgE and reduces FcεRI-mediated activation of mast cells and basophils. Its efficacy may involve reduction of FcεRI-positive and IgE-positive inflammatory cells in lesional skin.6 A French multicenter retrospective study reported favorable outcomes with omalizumab in BP resistant to first-line therapy.7 In the present case, however, omalizumab did not produce an early clinical response within two weeks. Because the exposure duration was short, we have avoided describing this as definitive omalizumab failure. Rather, the result should be interpreted as a lack of early response under the specific treatment conditions of this patient.
Dupilumab produced the most rapid clinical improvement in this case. Dupilumab blocks the interleukin-4 receptor alpha subunit and inhibits IL-4 and IL-13 signaling, thereby suppressing type 2 inflammation, which is increasingly recognized in BP pathogenesis. Emerging evidence supports dupilumab as a safe and effective option for BP.8 In this patient, skin lesions and pruritus improved within two weeks of dupilumab initiation, and disease activity remained controlled for a period after treatment discontinuation. However, relapse occurred during corticosteroid tapering after discontinuation of dupilumab due to financial constraints. These findings suggest that dupilumab was clinically effective for early disease control, but sustained treatment may have been necessary to maintain remission.
Rituximab was selected after relapse and inadequate control despite prednisone escalation. Rituximab targets CD20-positive B lymphocytes and can reduce pathogenic B-cell populations involved in autoantibody production.9 Systematic reviews have suggested that rituximab, omalizumab, and dupilumab may all provide clinical benefit in BP, although the evidence base remains dominated by retrospective studies, case series, and case reports.10 In this patient, rituximab contributed to sustained disease control and allowed prednisone tapering to 5 mg/day, which was clinically meaningful given the patient’s diabetes and comorbidities. Compared with dupilumab, rituximab did not appear to produce the fastest initial improvement, but it was associated with longer-term corticosteroid-sparing disease control after relapse.
The present case should not be interpreted as establishing a standard sequential strategy of omalizumab followed by dupilumab and then rituximab. Several limitations should be emphasized. First, direct immunofluorescence was negative and indirect immunofluorescence was not performed, limiting diagnostic certainty. Second, omalizumab was used for only two weeks, preventing full assessment of its efficacy. Third, the decision not to restart dupilumab after relapse was influenced by financial constraints and treatment accessibility, rather than by lack of efficacy. Fourth, concomitant systemic corticosteroids may have contributed to disease control and complicate attribution of the observed responses to individual biologics. Despite these limitations, the case highlights how clinical phenotype, serological profile, treatment response, safety considerations, corticosteroid-sparing needs, and economic accessibility can influence biologic selection in refractory BP.
In this patient with refractory BP and multiple comorbidities, dupilumab produced rapid clinical improvement, whereas rituximab contributed to sustained disease control and corticosteroid tapering after relapse. Omalizumab did not produce an early response, but its efficacy could not be fully evaluated because of the short treatment duration. This case does not establish a standard biologic sequence for BP. Instead, it underscores the need for individualized decision-making based on diagnostic certainty, immunological features, treatment response, comorbidities, safety concerns, and economic feasibility.
Data Sharing Statement
The raw data supporting the conclusions of this article will be made available by the corresponding authors.
Consent Statement
Written informed consent was obtained from the individual for the publication of any potentially identifiable images or data included in this article.
Acknowledgments
Lang Yu, Gang Hu, and Quanhong Zhang are co-first authors for this study. This work was supported by the Major Clinical Collaboration Project on Integrated Traditional Chinese and Western Medicine for Refractory Diseases (Bullous Pemphigoid) (ZDYN-2024-A-144), Shizhen Talent Program of Hubei Province for Scientific Research (Grant No: Hubei Health Document [2024] No. 256) and the Top talent project of Hubei Health Commission (China).
Disclosure
Lang Yu, Gang Hu, and Quanhong Zhang contributed equally to this work and should be considered co-first authors. The authors report no conflicts of interest in this work.
References
1. Powers CM, Thakker S, Gulati N, et al. Bullous pemphigoid: a practical approach to diagnosis and management in the modern era. J Am Acad Dermatol. 2025;92(6):1337–5. doi:10.1016/j.jaad.2025.01.086
2. Karakioulaki M, Eyerich K, Patsatsi A. Advancements in bullous pemphigoid treatment: a comprehensive pipeline update. Am J Clin Dermatol. 2024;25(2):195–212. doi:10.1007/s40257-023-00832-1
3. Le ST, Herbert S, Haughton R, et al. Rituximab and omalizumab combination therapy for bullous pemphigoid. JAMA Dermatol. 2024;160(1):107–109. doi:10.1001/jamadermatol.2023.4508
4. Chen Q, Hu B, Wan L, et al. Three cases of refractory bullous pemphigoid in the elderly treated successfully with ultra-low-dose rituximab. J Dermatol. 2023;50(4):561–564. doi:10.1111/1346-8138.16668
5. van Beek N, Lüttmann N, Huebner F, et al. Correlation of serum levels of IgE autoantibodies against BP180 with bullous pemphigoid disease activity. JAMA Dermatol. 2017;153(1):30–38. doi:10.1001/jamadermatol.2016.3357
6. Seyed Jafari SM, Gadaldi K, Feldmeyer L, Yawalkar N, Borradori L, Schlapbach C. Effects of omalizumab on FcepsilonRI and IgE expression in lesional skin of bullous pemphigoid. Front Immunol. 2019;10:1919. doi:10.3389/fimmu.2019.01919
7. Chebani R, Lombart F, Chaby G, et al. Omalizumab in the treatment of bullous pemphigoid resistant to first-line therapy: a French national multicentre retrospective study of 100 patients. Br J Dermatol. 2024;190(2):258–265. doi:10.1093/bjd/ljad369
8. Zhao L, Wang Q, Liang G, et al. Evaluation of dupilumab in patients with bullous pemphigoid. JAMA Dermatol. 2023;159(9):953–960. doi:10.1001/jamadermatol.2023.2428
9. Tovanabutra N, Payne AS. Clinical outcome and safety of rituximab therapy for pemphigoid diseases. J Am Acad Dermatol. 2020;82(5):1237–1239. doi:10.1016/j.jaad.2019.11.023
10. Cao P, Xu W, Zhang L. Rituximab, omalizumab, and dupilumab treatment outcomes in bullous pemphigoid: a systematic review. Front Immunol. 2022;13:928621. doi:10.3389/fimmu.2022.928621
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Case Report: Omalizumab Successfully Treated Recalcitrant Bullous Pemphigoid in an Elderly Patient with Multiple Comorbidities
Liu J, Xiang T, Wang W, Bu Z
Clinical, Cosmetic and Investigational Dermatology 2022, 15:1391-1396
Published Date: 21 July 2022
Characterization of Severe Uncontrolled Asthma in Japan: Analysis of Baseline Data from the PROSPECT Study
Koya T, Asai K, Iwanaga T, Hara Y, Takahashi M, Makita N, Hayashi N, Tashiro N, Tohda Y
Journal of Asthma and Allergy 2023, 16:597-609
Published Date: 2 June 2023
Successful Treatment of Immune Checkpoint Inhibitor–Induced Bullous Pemphigoid with Omalizumab: A Case Report and Review of the Literature
Chen J, Xu D, He Z, Ma S, Liu J, Dai X, Luo Y, Ye X
Clinical, Cosmetic and Investigational Dermatology 2024, 17:2865-2874
Published Date: 14 December 2024
Dupilumab as Immunomodulatory Rescue for Severe Recalcitrant Pemphigus Vulgaris: A Case Report and Literature Review
Boonpethkaew S, Chanprapaph K
Clinical, Cosmetic and Investigational Dermatology 2025, 18:1775-1782
Published Date: 25 July 2025
Corticosteroid-Sparing Control of Bullous Pemphigoid with Dupilumab and Tripterygium Glycosides: A Real-World Cohort with Longitudinal Transcriptomics
Wang SH, Li SZ, Li YR, Zhang J, Wang Y, Zuo YG
Journal of Inflammation Research 2026, 19:596205
Published Date: 1 May 2026