Back to Journals » Pharmacogenomics and Personalized Medicine » Volume 16
Personalized Approaches to Antiplatelet Treatment for Cardiovascular Diseases: An Umbrella Review
Authors Oliva A ![]() , Cao D, Spirito A
, Cao D, Spirito A ![]() , Nicolas J, Pileggi B
, Nicolas J, Pileggi B ![]() , Kamaleldin K, Vogel B, Mehran R
, Kamaleldin K, Vogel B, Mehran R
Received 7 March 2023
Accepted for publication 21 August 2023
Published 3 November 2023 Volume 2023:16 Pages 973—990
DOI https://doi.org/10.2147/PGPM.S391400
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Angelo Oliva,1,2 Davide Cao,1,3 Alessandro Spirito,1 Johny Nicolas,1 Brunna Pileggi,1,4 Karim Kamaleldin,1 Birgit Vogel,1 Roxana Mehran1
1The Zena and Michael A. Wiener Cardiovascular Institute, Icahn School of Medicine at Mount Sinai, New York City, NY, USA; 2Cardio Center, Humanitas Research Hospital IRCCS Rozzano, Milan, Italy; 3Department of Biomedical Sciences, Humanitas University, Pieve Emanuele (MI), Italy; 4Department of Cardiopneumonology, Heart Institute of the University of Sao Paulo, Sao Paulo, Brazil
Correspondence: Roxana Mehran, Tel +1-212-659-9649, Email [email protected]
Abstract: Antiplatelet therapy is the cornerstone of antithrombotic prevention in patients with established atherosclerosis, since it has been proven to reduce coronary, cerebrovascular, and peripheral thrombotic events. However, the protective effect of antiplatelet agents is counterbalanced by an increase of bleeding events that impacts on patients’ mortality and morbidity. Over the last years, great efforts have been made toward personalized antithrombotic strategies according to the individual bleeding and ischemic risk profile, aiming to maximizing the net clinical benefit. The development of risk scores, consensus definitions, and the new promising artificial intelligence tools, as well as the assessment of platelet responsiveness using platelet function and genetic testing, are now part of an integrated approach to tailored antithrombotic management. Moreover, novel strategies are available including dual antiplatelet therapy intensity and length modulation in patients undergoing myocardial revascularization, the use of P2Y12 inhibitor monotherapy for long-term secondary prevention, the implementation of parenteral antiplatelet agents in high-ischemic risk clinical settings, and combination of antiplatelet agents with low-dose factor Xa inhibitors (dual pathway inhibition) in patients suffering from polyvascular disease. This review summarizes the currently available evidence and provides an overview of the principal risk-stratification tools and antiplatelet strategies to inform treatment decisions in patients with cardiovascular disease.
Keywords: antiplatelet therapy, cardiovascular disease, P2Y12 inhibitor, aspirin
Introduction
Antiplatelet therapy is the cornerstone of antithrombotic prevention in patients with established atherosclerosis, including those with coronary artery disease (CAD).1–3 Although antiplatelet therapy is highly effective in reducing ischemic events and thrombotic complications, it invariably increases bleeding occurrence which may have a detrimental impact on patient mortality and morbidity.4,5 Understanding the bleeding and ischemic risks balance is critical to inform decisions on antiplatelet therapy and efforts have been made toward finding the optimal compromise between prevention of thrombotic events and avoidance of bleeding complications.6 Current guidelines stress the importance of risk stratification according to baseline characteristics and clinical presentation to identify those who could benefit from shorter or less intense antiplatelet therapy, and vice versa.1–3 The aim of the present review is to summarize the evidence on antiplatelet therapy in patients with cardiovascular disease, providing an overview of the principal risk-stratification tools and antithrombotic available strategies, including novel emerging approaches (Figure 1). Given the preeminent role of antiplatelet therapy in patients with coronary artery disease undergoing percutaneous revascularization, we initially focused on this broad subset of patients; additionally, we also provided insights about personalized antiplatelet approaches in patients suffering from other specific cardiovascular conditions, including cerebrovascular and polyvascular disease.
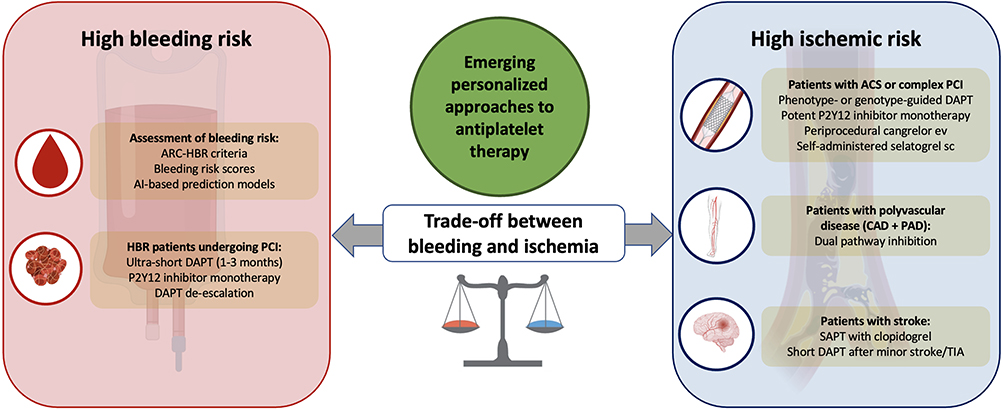 |
Figure 1 Emerging personalized approaches to antiplatelet therapy. |
Antiplatelet Therapy in Patients with Coronary Artery Disease Undergoing Percutaneous Coronary Intervention
In the past years, dual antiplatelet therapy (DAPT), consisting of aspirin plus a P2Y12-receptor inhibitor, was recommended for at least 12 months after percutaneous coronary intervention (PCI).7 This default strategy was primarily driven by concerns about the risk of stent thrombosis with first-generation drug-eluting stents (DES) but gave little consideration to individual patient characteristics and risk factors. More recently, several randomized controlled trials (RCTs) have evaluated the safety and effectiveness of different DAPT strategies, tailoring the length and intensity of DAPT to optimize net clinical outcomes. Novel antithrombotic strategies, such as short DAPT followed by P2Y12 inhibitor monotherapy and platelet function-guided or genotype-guided de-escalation or escalation of P2Y12 inhibition, have been investigated. Moreover, in the context of antiplatelet therapy, risk scores have been developed to assess the risk of bleeding or ischemic events and inform decision-making on antiplatelet therapy. Assessment of bleeding and ischemic risks is achieved by the evaluation of clinical variables, including patient history, frailty, comorbidities, and laboratory examinations. In the PCI setting, procedural and technical features also play an important role in determining the subsequent ischemic or bleeding risks and should be taken into consideration.8
Stratification of Bleeding and Thrombotic Risk
The PARIS risk model is one of the first validated tools for prediction of out-of-hospital thrombotic and bleeding events in patients undergoing PCI with DES.9 It consists of two different prediction models, one for coronary thrombotic events and the other for BARC (Bleeding Academic Research Consortium) 3 or 5 major bleeding, used to develop integer-based risk scores that categorize patients into three risk groups (low risk: <3, moderate risk: 3–7, and high risk: ≥8 points). Independent predictors of thrombotic complications included acute coronary syndrome (ACS), prior revascularization, diabetes mellitus, renal dysfunction, and current smoking. Independent predictors of major bleeding included older age, body mass index, concomitant use of anticoagulant at discharge, anemia, current smoking, and renal dysfunction. Each model displayed modest discrimination and adequate calibration. Other alternative scores assessing the long-term bleeding or thrombotic risk are summarized in Table 1 and include BleeMACS, the Dutch aspirin score, the PRECISE-DAPT score, the DAPT score, and the REACH score.10–14 The PRECISE-DAPT score is a five-item risk score that incorporates the following clinical features: age, creatinine clearance, hemoglobin, white-blood-cell count, and previous spontaneous bleeding.14 It provides a tool for the prediction of out-of-hospital TIMI (thrombolysis in myocardial infarction) major or minor bleeding during DAPT in patients undergoing PCI and has been endorsed by current guidelines.1 The DAPT score was developed from 11,648 patients enrolled in the DAPT trial who tolerated DAPT during the first year post PCI without major adverse cardiovascular events (MACE) or bleeding. The DAPT score aimed to identify patients who could derive benefit from DAPT extension (beyond 1 year and up to 30 months) without bleeding-related harm and includes a combination of ischemic and bleeding predictors: age, heart failure/low left ventricular ejection fraction, vein graft stenting, myocardial infarction (MI) at presentation, prior MI or PCI, diabetes, stent diameter <3 mm, smoking, and paclitaxel-eluting stent.11 The DAPT score has been externally validated in several studies with conflicting results.15–18
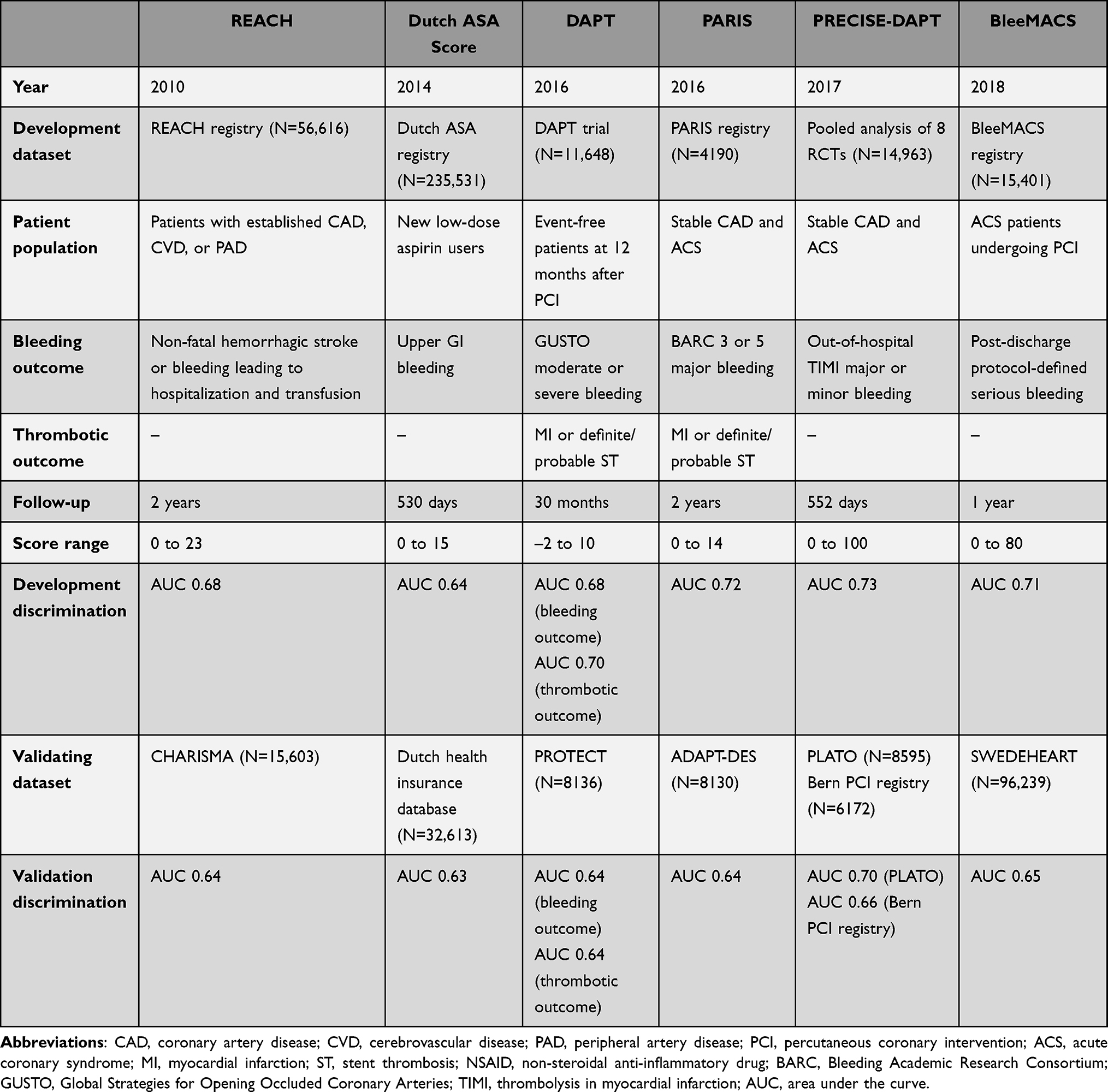 |
Table 1 Risk Scores for Evaluating Baseline Bleeding and/or Thrombotic Risk Among Patients with CAD |
When interpreting risk scores, it must be remembered that they are all intrinsically influenced by the characteristics of the study populations used for their development and may not be applicable to the general population. In order to overcome these limitations, in 2019 an Academic Research Consortium (ARC) initiative proposed a consensus definition of high bleeding risk (HBR) patients based on the presence of well-recognized major and minor risk criteria in a PCI setting.19 Patients should be considered HBR if at least 1 major or 2 minor criteria are met. A 1-year incidence of BARC 3 or 5 bleeding ≥4% or intracranial hemorrhage ≥1% has been arbitrarily proposed as a cut-off to define true HBR patients. The 2023 European guidelines for the management of ACS endorsed the use of ARC-HBR criteria to guide decisions on DAPT and, following the same approach, criteria for defining patients at high or moderate thrombotic risk were provided (Table 2).
 |
Table 2 High Bleeding (ARC-HBR) and Thrombotic (ESC Guideline) Risk Definitions |
Another well-known limitation of risk scores is that they are usually derived by applying classical statistic regression models and tend to underestimate interactions between variables in complex scenarios, especially when a large number of clinical, anatomical, and procedural features may be reciprocally influenced.20 Novel opportunities may reside in the ability of artificial intelligence (AI) in generating decision pathways truly individualized for every single patient.21 As an example, the PRAISE score, a risk score aimed to predict 1-year post-discharge all-cause death, myocardial infarction, and major bleeding, was recently derived using a machine learning model trained on a cohort of 19,826 ACS patients from the BleeMACS and RENAMI registries.22 AI-based approaches hold the promise of improving predictive model performance and could represent a turning point in the field of precision medicine; however, bigger studies and more evidence are warranted to implement their use in the clinical practice.
Strategies for Thrombotic Risk Reduction
Extended DAPT
In the early years after the spread of first-generation DES, safety concerns about the risk of late stent thrombosis were raised, highlighting the need for a more intense and prolonged DAPT.23,24 The advent of newer-generation DES, associated with a very low incidence of stent thrombosis (<1%/year), mitigated this clinical issue.25 However, the observation that patients with CAD remain at risk for recurrent spontaneous ischemic events provided the rationale for investigations on prolonged DAPT duration, even beyond one year.26 To date, 9 RCTs have compared extended DAPT (up to 48 months) with standard 6–12-month DAPT (Table 3).26–34 Most trials failed to demonstrate a clear benefit of extended DAPT, and pooled analyses showed that the reduction in myocardial infarction and stent thrombosis did not result in improved survival.35 The DAPT study was the first large-scale, randomized clinical trial that evaluated a strategy of 30-month DAPT versus standard 12-month DAPT among 9961 participants with either stable CAD or ACS.26 Extended DAPT significantly reduced the incidence of MACE and stent thrombosis, but at the expense of increased bleeding and mortality.
 |
Table 3 RCTs Comparing Extended versus Standard DAPT Regimens in Patients with CAD Undergoing PCI |
Altogether, these studies support an extended DAPT course in selected patients in whom thrombotic risk outweighs bleeding risk, but careful evaluation, especially in frail and older patients, is needed to avoid potential harm.1–3
Strategies for Bleeding Risk Reduction
Short DAPT Followed by Aspirin Monotherapy
Twelve RCTs have explored the risks and benefits of short DAPT followed by aspirin as compared with standard DAPT (Table 4).36–47 Eight trials compared 6-month versus 12-month DAPT, three trials 3-month versus 12-month DAPT, and one trial 1-month versus 6–12-month DAPT. Although most of these studies showed that early discontinuation of the P2Y12 inhibitor reduces bleeding without a significant increase in thrombotic complications, caution should be exercised given the low ischemic risk profile of the patients enrolled, the lower-than-expected event rates, and the lack of power for hard ischemic endpoints for some RCTs. Overall, it seems reasonable to reserve a short DAPT duration followed by aspirin monotherapy to stable patients undergoing non-complex procedures.1–3
 |
Table 4 RCTs Comparing Short DAPT Followed by Aspirin Monotherapy versus Standard DAPT in Patients with CAD Undergoing PCI |
Ultra-short DAPT durations (1–3 months) have also been tested in HBR patients undergoing PCI with newer-generation DES platforms. Although bare-metal stents have been historically considered safer for HBR patients receiving an abbreviated DAPT, contemporary RCTs have challenged this practice.48–51 The MASTER DAPT trial was the first large study testing different DAPT durations in a cohort of 4434 HBR patients undergoing implantation of a biodegradable-polymer sirolimus-eluting Ultimaster stent.52 A short DAPT (1 month) regimen was shown to be non-inferior to standard DAPT with regard to net adverse clinical events and MACE. A recent meta-analysis comparing abbreviated (1–3 months) with standard (≥6 months) DAPT among 9006 HBR patients from 11 RCTs showed a significant reduction in major bleeding and cardiovascular mortality in HBR patients assigned to short DAPT.53
Short DAPT Followed by P2Y12 Inhibitor Monotherapy
A strategy of P2Y12 inhibitor monotherapy after a short DAPT has recently been proposed for PCI patients. RCTs comparing P2Y12 inhibitor monotherapy versus DAPT are summarized in Table 5.47,54–58 Clopidogrel monotherapy after 1-to-3 month DAPT was investigated as an alternative to standard 12-month DAPT in patients undergoing PCI in three different trials: SMART-CHOICE, STOPDAPT-2, and STOPDAPT-2 ACS.47,57,59 In a pooled analysis of nearly 6000 patients, clopidogrel monotherapy was non-inferior to 12-month DAPT for the composite of cardiovascular death, MI, definite stent thrombosis, or any stroke, while it significantly reduced TIMI major or minor bleeding.60 However, a numerical increase in cardiovascular events was noted among ACS on 1-month DAPT, warning about a possible safety issue in high ischemic risk patients.
 |
Table 5 RCTs Comparing Short DAPT Followed by P2Y12 Inhibitor Monotherapy versus Standard DAPT in Patients with CAD Undergoing PCI |
With the advent of ticagrelor and prasugrel, pharmacodynamic studies have questioned the incremental antiplatelet effect of aspirin in the presence of potent P2Y12 inhibitors, especially with ticagrelor.61 GLOBAL LEADERS was the first trial to test a strategy of open-label 1-month DAPT followed by 23-month ticagrelor monotherapy versus 12-month DAPT followed by aspirin monotherapy among nearly 16,000 patients (of whom 46.9% had ACS).54 The trial failed to meet its primary endpoint of reduction in all-cause death and non-fatal Q-wave MI despite a favorable numerical trend; meanwhile, no significant differences were observed in terms of site-reported BARC 3 or 5 bleeding. Opposing these negative results, the double-blind, placebo-controlled TWILIGHT trial enrolled high-risk PCI patients who completed an initial course of DAPT with ticagrelor for 3 months, and randomized them to ticagrelor monotherapy versus ticagrelor plus aspirin for an additional 12 months.55 Ticagrelor monotherapy significantly reduced the primary outcome of BARC 2, 3, or 5 bleeding at 12 months and the key composite ischemic endpoint met the non-inferiority criterion. Results were consistent among subgroups of high-risk patients such as those with diabetes mellitus, ACS, and HBR, and those undergoing complex PCI.62–64 Finally, the TICO trial included only ACS patients who were randomized to 3-month DAPT followed by ticagrelor monotherapy or 12-month aspirin and ticagrelor.65 Ticagrelor monotherapy significantly reduced the composite of death, MI, stent thrombosis, stroke, target vessel revascularization, or TIMI major bleeding at 12 months, a difference that was mainly driven by a reduction in TIMI major bleeding.
Results from studies investigating P2Y12 inhibitor monotherapy versus standard DAPT, including those conducted among patients receiving coronary bypass, were pooled in a recent individual patient-level meta-analysis of nearly 24,000 patients. P2Y12 inhibitor monotherapy significantly reduced bleeding without increasing the risk of death, myocardial infarction, or stroke.66 Meta-analysis restricted to ticagrelor monotherapy RCTs yielded similar results.67 Based on the available evidence, P2Y12 inhibitor monotherapy after an initial short DAPT should be considered as an alternative to standard DAPT, especially when bleeding risk is a concern. In ACS patients, however, early DAPT discontinuation followed by clopidogrel monotherapy may not provide sufficient antithrombotic protection; thus, ticagrelor should remain the agent of choice.
Phenotype-Guided or Genotype-Guided Antiplatelet Strategies
Clopidogrel is a prodrug and requires conversion to an active metabolite by the hepatic cytochrome P450 enzyme (CYP2C19). Up to 30% of Caucasian patients show inadequate response to clopidogrel that can be partly explained by loss-of-function (LOF) polymorphisms of CYP2C19 alleles.68 Carriers of LOF alleles exhibit high on-treatment platelet reactivity (HPR) that increases the risk of thrombotic events, MACE, and stent thrombosis; conversely, patients with low-platelet reactivity seem to have a higher risk for bleeding.69 Because such genetic polymorphisms do not alter the pharmacokinetics of prasugrel and ticagrelor, it has been suggested that carriers of CYP2C19 LOF mutations might derive greater benefit from more potent P2Y12 inhibitors. The impact of CYP2C19 genotype on clinical outcomes with ticagrelor or prasugrel compared with clopidogrel was recently evaluated in a meta-analysis including 15,949 patients from 7 RCTs. Prasugrel or ticagrelor were shown to reduce major ischemic events in CYP2C19 LOF carriers, whereas no difference was observed in non-carriers.70
From a phenotype perspective, on-treatment platelet inhibition can be measured with dedicated essays. In vitro platelet function tests predict patients’ clinical response to clopidogrel and have been shown to correlate with the risk of subsequent thrombosis and bleeding.71 Theoretically, based on these tests, DAPT can be modulated choosing between more or less potent agents, depending on the predicted response to clopidogrel. Therefore, it is possible to define a functional-guided escalation (eg the use of a more potent P2Y12 inhibitors in the setting of high platelet reactivity on clopidogrel) or de-escalation (eg, maintenance of clopidogrel in case of adequate platelet inhibition). At present, however, randomized trials assessing the clinical utility of standardized platelet function tests have generated contradictory results, and there is no consensus on the definition of resistance to antiplatelet therapy.72–74
In the TROPICAL-ACS trial, a platelet functional guided de-escalation strategy resulted non-inferior in terms of net-clinical benefit as compared with conventional therapy of DAPT with prasugrel among 2610 randomized ACS patients.72 The rates of ischemic events were similar in the two groups and a numerical trend, albeit not significant, toward less bleeding in the platelet function-guided group was evident.
Non-inferiority for net clinical benefit was also met in the POPULAR GENETICS trial, in which a total of 2488 patients undergoing primary PCI for ST-elevation myocardial infarction (STEMI) were randomized to a genotype-guided DAPT strategy where carriers of CYP2C19 LOF alleles received ticagrelor or prasugrel and non-carriers received clopidogrel versus standard treatment with either ticagrelor or prasugrel.73 The genotype-guided strategy was also associated with a significant reduction in major or minor bleeding, mainly driven by a reduction in minor bleeding.
Finally, in the TAILOR PCI trial, 5302 patients undergoing PCI for ACS (82%) or stable angina (18%) were randomized to standard treatment or use of a point-of-care genotyping test for the selection of ticagrelor or clopidogrel.74 The genotype-guided strategy resulted in a numerically, but not statistically significant reduction of the primary endpoint, a composite of cardiovascular death, myocardial infarction, stroke, stent thrombosis, or severe recurrent ischemia at 12 months; however, the secondary endpoint of major or minor bleeding did not differ between the two study groups. The ABCD-GENE (age, body mass index, chronic kidney disease, diabetes mellitus, and genotyping) risk score was subsequently derived from a post-hoc analysis of the trial, to identify patients with HPR on clopidogrel at increased risk for adverse ischemic events, who may benefit from escalation of DAPT.75
Overall, in a large meta-analysis including 20,743 patients from 11 RCTs and 3 observational studies, a strategy of guided selection of antiplatelet therapy by means of genotyping or platelet function tests was associated with improved clinical outcomes.76 Despite this significative piece of evidence and the potential role among HBR patients and patients with a recent ACS, routine adoption of phenotype-guided or genotype-guided antithrombotic therapies in clinical practice remains limited.
Long-Term Secondary Antithrombotic Prevention
Aspirin and DAPT
Aspirin is universally considered the foundation of life-long secondary prevention in patients with cerebrovascular, coronary, or peripheral artery disease and remains the drug of choice after discontinuation of DAPT post-PCI or ACS.1,77 However, long-term aspirin use carries potential side-effects, including a well-established risk of gastrointestinal bleeding. In this setting, P2Y12 inhibitors offer an alternative for chronic maintenance therapy. Initially, long-term maintenance therapy with P2Y12 inhibitor was tested in combination with aspirin. In the PEGASUS-TIMI 54 trial, 21,162 high-risk patients presenting 1–3 years after ACS (54% STEMI) were randomized in a double-blind 1:1:1 fashion to ticagrelor 90 mg twice daily, ticagrelor 60 mg twice daily, or placebo, on top of aspirin.31 At 3 years, ticagrelor 60 mg on top of aspirin was the most favorable regimen in terms of overall net benefit, and has therefore been endorsed by recent guidelines for long-term secondary prevention. The high-risk clinical features (age ≥65 years, diabetes mellitus, recurrent MI, multivessel disease, or chronic kidney disease) adopted as inclusion criteria in the PEGASUS-TIMI 54 trial serve to identify patients that may derive a clinical benefit from extended DAPT with low-dose of ticagrelor. On the other hand, in the setting of high-risk stable CAD, the THEMIS trial randomized 19,271 diabetic patients to ticagrelor 60 mg and aspirin versus aspirin alone.34 At a median follow-up of 40 months, ticagrelor was associated with a borderline reduction in MACE and a 2-fold increase in TIMI major bleeding. When the analysis was restricted to patients with previous PCI, ticagrelor seemed to yield a greater net benefit than in those without prior PCI.78
P2Y12Inhibitor Monotherapy
More recently, several RCTs have compared P2Y12 inhibitor monotherapy against aspirin for secondary prevention in patients with established atherosclerosis, yielding mixed results. A comprehensive meta-analysis encompassing 42,108 patients from 9 RCTs showed a significant, yet clinically modest, risk reduction in myocardial infarction with P2Y12 inhibitor versus aspirin monotherapy, with no differences in death, stroke, and major bleeding.79 In the HOST-EXAM trial, clopidogrel monotherapy was associated with a significant reduction in both thrombotic and bleeding events up to 5 years as compared to low-dose aspirin, among 5438 patients who were free from ischemic and bleeding adverse events 12 months after PCI.80,81 These promising results were confirmed by an individual patient data meta-analysis of 7 large RCTs – including HOST-EXAM – with an overall population of nearly 35,000 patients with established coronary disease. P2Y12 inhibitor monotherapy, including clopidogrel (62%) and ticagrelor (38%), showed a significant reduction of cardiovascular death, MI, or stroke with similar rate of major bleeding, as compared to aspirin, at a median follow-up of 552 days.82 Despite the uncertain cost-effectiveness and the relatively low effect size of P2Y12 inhibitor monotherapy, the use P2Y12 inhibitors now represents a valid alternative to aspirin, especially in patients with coronary artery disease who are intolerant to aspirin or have experienced adverse events.
Personalized Approaches in Specific Cardiovascular Conditions
Complex PCI
Up to 30% of PCI procedures can be classified as complex owing to technical challenges and high rates of periprocedural complications, especially when multiple complexity features are present.8,83 The definition of PCI complexity generally refers to coronary artery disease extent or lesion difficulty, but may also extend to patient comorbidities and frailty. Notably, bleeding and ischemic risk factors often coincide (eg, age, chronic kidney disease, anemia) and a large proportion (up to 45%) of patients undergoing complex PCI are at high-bleeding risk, making the management of DAPT even more challenging.84
In a pivotal study by Giustino et al, complex PCI was defined by the presence of at least one of the following criteria: 3 vessels treated, ≥3 lesions treated, ≥3 stents implanted, bifurcation with 2 stents implanted, total stent length >60 mm, or chronic total occlusion as the target lesion.8 Using data from 6 RCTs and 9577 patients, the authors showed that long-term (≥12 months) versus short-term (3–6 months) DAPT significantly reduced MACE in complex PCI patients but not in those without complex features. On the other hand, long DAPT was associated with more major bleeding, irrespective of PCI complexity. A subsequent similar study, which accounted for not only PCI complexity but also HBR features, showed that long-term DAPT reduces ischemic events after complex PCI only when HBR features are not present.85 Recently, in the ALPHEUS trial, 1910 elective high-risk PCI patients were randomized to DAPT with ticagrelor versus clopidogrel for 30 days after the procedure. Ticagrelor did not reduce the primary outcome, a composite of PCI-related type 4 myocardial infarction or major myocardial injury; major bleeding did not differ between the two groups, but minor bleeding was more frequent with ticagrelor at 30 days.86 Finally, two different study-level meta-analyses and one patient-level meta-analysis evaluated the safety and efficacy of P2Y12 inhibitor monotherapy among patients undergoing complex PCI including subgroup analysis from 5 different RCTs.87–89 A short course of 1–3-month DAPT followed by P2Y12 inhibitor monotherapy with either clopidogrel or ticagrelor was found to reduce bleeding complications without increasing ischemic events, irrespective of PCI complexity. On the basis of the available evidence, P2Y12 inhibitor monotherapy after a short DAPT can be a valid alternative to standard and/or prolonged DAPT, especially in HBR patients.
Parenteral Antiplatelet Therapy
Glycoprotein IIb/IIIa Receptor Inhibitors
Glycoprotein IIb/IIIa receptor inhibitors (GPIs) were the first available intravenous antiplatelet agents providing nearly complete inhibition of platelet aggregation.90 GPIs were first used in the acute setting to reduce the risk of ischemic complications during ACS or PCI. After the introduction of more potent oral P2Y12 inhibitors and given the bleeding concerns associated with GPIs, their routine use has significantly decreased in clinical practice. Nowadays, GPIs are limited to a bailout use, in the presence of a large thrombus burden, slow flow, or “no reflow” complications of PCI.90
Cangrelor
Cangrelor is an intravenous direct reversible P2Y12 receptor antagonist with a quick onset and a rapid offset of action after infusion discontinuation. Compared to oral P2Y12 inhibitors, cangrelor achieves fast and consistent platelet inhibition, and it is effective in reducing periprocedural thrombotic complication of PCI.90 In the CHAMPION PHOENIX trial, among 11,145 P2Y12 inhibitor-naive patients undergoing PCI for stable CAD or non-ST-segment elevation ACS, pre-treatment with cangrelor reduced the primary endpoint of death, MI, ischemia-driven revascularization, or stent thrombosis at 48 h, with no significant difference in severe bleeding, as compared to an oral loading dose of clopidogrel.91 In a post-hoc analysis, cangrelor showed a greater absolute risk reduction of 48-h MACE and stent thrombosis in patients with high-risk periprocedural features, suggesting a greater benefit–risk profile in patients with complex coronary anatomies.92 According to the current evidence, candidates for cangrelor administration include patients undergoing complex PCI who are not pretreated with oral P2Y12 inhibitors. Those presenting with ACS who undergo emergency PCI can also be considered for cangrelor use. In the setting of STEMI and/or hemodynamic instability, the slow gut transit, morphine use, and presence of nausea, vomiting, intubation, or cardiogenic shock may impair absorption and efficacy of oral P2Y12 inhibitors, making cangrelor a valid option to overcome the latency of an oral P2Y12 inhibitor.93 However, since cost and availability may limit its use, alternative strategies including parenteral administration of enoxaparin have been tested in this setting, with promising results.94 Finally, given its rapid onset and offset of action, use of cangrelor is an attractive option for patients at high ischemic risk requiring non-deferrable surgery and in whom discontinuation of oral P2Y12 inhibition is necessary.95–97
Selatogrel
A novel fascinating concept has been introduced with the development of the new parenteral P2Y12 inhibitor, selatogrel. Selatogrel can be administered subcutaneously and has a rapid onset/offset effect, providing immediate platelet inhibition in patients with acute ischemic events including MI, stroke, or acute limb ischemia. As it is available in the form of an injector for self-administration, patients with very high ischemic risk could hypothetically derive benefit from an early self-administration when the first symptoms of ongoing ischemia are recognized.98 Recently, a single subcutaneous administration of selatogrel was tested in a small phase 2 exploratory study among patients presenting with acute MI scheduled for an invasive strategy, showing a profound, rapid, and dose-related antiplatelet inhibition, with a good safety profile.99 However, studies are needed to establish the efficacy and safety of selatogrel in patients with suspected MI.
Concomitant Oral Anticoagulation
Patients with an indication to chronic oral anticoagulation (OAC), mainly because of atrial fibrillation, represent a sizeable portion of those undergoing PCI and are by definition considered at HBR. Guidelines and consensus recommendations on the management of OAC and DAPT after PCI or ACS have changed significantly over the last years with introduction of non-vitamin K antagonist oral anticoagulants (NOACs) and with results of their respective RCTs: rivaroxaban (PIONEER AF-PCI), dabigatran (REDUAL-PCI), apixaban (AUGUSTUS), and edoxaban (ENTRUST-AF-PCI).100–103 In order to minimize the risk of bleeding, a default strategy of triple antithrombotic therapy, consisting of aspirin, P2Y12 inhibitor, and NOAC, should be given for one week (or up until hospital discharge) after PCI, followed by a combination of NAOC and a single antiplatelet agent (preferably, the P2Y12 inhibitor clopidogrel) up to 12 months.104 After 12 months, a single long-term therapy with NOAC alone should be the treatment of choice.105 However, this strategy should be modulated according to the individual ischemic and bleeding risk of the patient. If thrombotic risk is a concern, the triple therapy may be extended up to one month after PCI and the use of more potent P2Y12 inhibitors instead of clopidogrel may be considered in patients at low bleeding risk. Meanwhile, if bleeding risk prevails, earlier discontinuation of dual antithrombotic therapy and transition to OAC alone after 3–6 months may be considered.
Cerebrovascular Disease
Anticoagulants represent the cornerstone of primary and secondary prevention among patients suffering from atrial fibrillation or atrial flutter at high risk for cardioembolic stroke. Nevertheless, in the absence of such indication to anticoagulation, antiplatelet therapy remains the treatment of choice for the secondary prevention of patients with a history of ischemic stroke or transient ischemic attack (TIA), and treatment initiation immediately after the acute event is essential for preventing recurrences.106 The benefit of aspirin in this setting is well-established after it was tested in more than 40,000 patients, in the randomized CAST and IST studies.107,108 Based on the results of the CAPRIE trial and subsequent meta-analysis of several studies, clopidogrel monotherapy was even more effective than aspirin in reducing ischemic stroke recurrence.109,110 Similar rates of recurrent stroke were observed with the combination of aspirin plus dipyridamole versus clopidogrel in the PROFESS study.110–112 Conversely, ticagrelor monotherapy failed to show superiority to aspirin in the SOCRATES trial, enrolling nearly 13,000 patients with non-severe ischemic stroke or high-risk TIA.113 DAPT with aspirin and clopidogrel has been tested for long-term prevention after a stroke or TIA in the MATCH and SPS3 trials and in a subset of the CHARISMA trial, but it did not show better outcomes than monotherapy in terms of recurrent ischemic events, and was rather associated with increased bleeding.111,114,115 By contrast, a short course of DAPT with clopidogrel has shown some advantages over monotherapy in patients with minor stroke or TIA in the CHANCE and POINT RCTs, probably due to the increased probability of reoccurrence of a major stroke, often disabling, within the first weeks after a minor event. On the other hand, DAPT with ticagrelor compared with aspirin alone significantly reduced the risk of 1-month stroke or death, at the expense of higher incidence of severe bleeding, among 11,016 patients enrolled in the THALES trial.116
For these reasons, current guidelines suggest short-term (up to 3 weeks) DAPT for patients with recent TIA or minor stroke, whereas antiplatelet monotherapy with clopidogrel over aspirin is recommended after moderate-to-severe strokes due to the potential risk of hemorrhagic transformation; antiplatelet monotherapy, or as alternative a combination of aspirin and dipyridamole, is warranted for long-term ischemic stroke secondary prevention.
Polyvascular Disease
A significant proportion of patients with CAD also have peripheral artery disease (PAD).117 Presence of polyvascular disease renders these patients at increased risk of thrombotic events which may justify an intensified antithrombotic strategy.117 Among patients with symptomatic PAD, single antiplatelet therapy with either aspirin or clopidogrel has been shown to reduce ischemic complications.117 The effects of a more profound platelet inhibition with clopidogrel-based DAPT was evaluated in a post-hoc analysis of the CHARISMA trial among 3096 patients with PAD. DAPT was found to reduce the rate of MI and hospitalization for ischemic events at the cost of increased bleeding, and with no difference in ischemic limb events.118 The newer P2Y12 inhibitor ticagrelor failed to show a clinical benefit over clopidogrel among 13,885 patients with symptomatic PAD enrolled in the EUCLID trial.119
Taken together, the available evidence suggests that, despite a theoretical benefit of DAPT in PAD patients with a low bleeding risk being hypothesized, monotherapy with clopidogrel or aspirin remains the preferred approach. More recently, a new strategy of dual-pathway inhibition (DPI) consisting of a combination of an antiplatelet agent with a low-dose anticoagulant to achieve a synergistic antithrombotic effect has been proposed for patients with a high atherosclerotic burden. The COMPASS trial was the first study to investigate the use of low-dose NOAC in addition to antiplatelet therapy in stable atherosclerotic cardiovascular disease. A total of 27,395 patients were randomly assigned to rivaroxaban 2.5 mg twice daily plus aspirin (DPI group), rivaroxaban 5.0 mg twice daily alone, or aspirin alone. Patients assigned to a DPI strategy had fewer MACE but more major bleeding compared with those assigned to aspirin alone.120 Among 7749 patients with a history of PAD, DPI with rivaroxaban plus aspirin reduced the occurrence of major adverse limb events including major amputation.121 The benefit of DPI was even greater in terms of major adverse limb events, total vascular amputations, and peripheral vascular interventions when considering a restricted subgroup of 6391 patients with lower-extremity PAD.121 The benefit of low-dose rivaroxaban in addition to aspirin in reducing major thrombotic vascular events was also demonstrated in PAD patients undergoing peripheral revascularization from the VOYAGER PAD trial, with a significant reduction in thrombotic events with no apparent trade-off in major bleeding.122 Therefore, adding “vascular protection” low-dose rivaroxaban to aspirin has been endorsed by recent expert consensus and guidelines as a feasible option in patients with PAD not deemed to be at HBR.117
Conclusions
Antiplatelet therapy has dramatically evolved over the last decades, aiming to reduce the risk of thrombotic complications while minimizing the risk of bleeding among patients with established cardiovascular disease. Among those with CAD undergoing PCI, different strategies are now available and include prolonging, shortening, escalating, or de-escalating DAPT, in a guided or unguided manner. P2Y12 inhibitor monotherapy is a novel approach focused on reducing the bleeding risk perhaps maintaining ischemic protection. The use of parenteral antiplatelet agents, such as intravenous cangrelor or subcutaneous selatogrel, are emerging approaches to ensure adequate platelet inhibition in high-ischemic risk clinical settings. Finally, DPI can provide vascular protection in patients suffering from a complex, multidistrict polyvascular disease. However, a comprehensive assessment of the ischemic and bleeding risk profile, as well as of individual clinical features and possibly responsiveness to antiplatelet agents by the use of platelet function and genetic testing, is now crucial in defining the optimal regimen. The use of risk scores, consensus definitions, and the new promising AI tools is part of an integrated approach aimed to personalize the selection of the most appropriate antiplatelet therapy for each patient.
Funding
There is no funding to report.
Disclosure
Dr. Spirito reports grants from Swiss National Science Foundation, outside the submitted work. Dr. Pileggi reports a research grant from the Brazilian Federal Foundation for Support and Evaluation of Graduate Education (CAPES). Dr. Mehran reports institutional research grants from Abbott, Abiomed, Applied Therapeutics, Arena, AstraZeneca, Bayer, Biosensors, Boston Scientific, Bristol-Myers Squibb, CardiaWave, CellAegis, CERC, Chiesi, Concept Medical, CSL Behring, DSI, Insel Gruppe AG, Medtronic, Novartis Pharmaceuticals, OrbusNeich, Philips, Transverse Medical, and Zoll; personal fees from ACC, Boston Scientific, California Institute for Regenerative Medicine (CIRM), Cine-Med Research, Janssen, WebMD, and SCAI; consulting fees paid to the institution from Abbott, Abiomed, AM-Pharma, Alleviant Medical, Bayer, Beth Israel Deaconess, CardiaWave, CeloNova, Chiesi, Concept Medical, DSI, Duke University, Idorsia Pharmaceuticals, Medtronic, Novartis, and Philips; equity <1% in Applied Therapeutics, Elixir Medical, STEL, and CONTROLRAD (spouse); and Scientific Advisory Board for AMA, Biosensors (spouse). The other authors have no relevant conflicts of interest to disclose for this work.
References
1. Valgimigli M, Bueno H, Byrne RA, et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: the task force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European. Eur Heart J. 2018;39(3):213–260. doi:10.1093/eurheartj/ehx419
2. Neumann FJ, Sousa-Uva M, Ahlsson A, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2019;40(2):87–165. doi:10.1093/eurheartj/ehy394
3. Byrne RA, Xavier Rossello JJC, Barbato E, et al. Roberto E, ESC Scientific Document Group, 2023 ESC guidelines for the management of acute coronary syndromes: developed by the task force on the management of acute coronary syndromes of the European Society of Cardiology (ESC), Eur Heart J. 2023; ehad191. doi: 10.1093/eurheartj/ehad191
4. Piccolo R, Oliva A, Avvedimento M, et al. Mortality after bleeding versus myocardial infarction in coronary artery disease: a systematic review and meta-analysis. EuroIntervention. 2021;17(7):550–560.
5. Valgimigli M, Costa F, Lokhnygina Y, et al. Trade-off of myocardial infarction vs. bleeding types on mortality after acute coronary syndrome: lessons from the Thrombin Receptor Antagonist for Clinical Event Reduction in Acute Coronary Syndrome (TRACER) randomized trial. Eur Heart J. 2017;38(11):804–810. doi:10.1093/EURHEARTJ/EHW525
6. Capodanno D, Bhatt DL, Gibson CM, et al. Bleeding avoidance strategies in percutaneous coronary intervention. Nat Rev Cardiol. 2021;19(2):117–132. doi:10.1038/s41569-021-00598-1
7. Cao D, Chandiramani R, Chiarito M, Claessen BE, Mehran R. Evolution of antithrombotic therapy in patients undergoing percutaneous coronary intervention: a 40-year journey. Eur Heart J. 2021;42(4):339–351. doi:10.1093/eurheartj/ehaa824
8. Giustino G, Chieffo A, Palmerini T, et al. Efficacy and safety of dual antiplatelet therapy after complex PCI. J Am Coll Cardiol. 2016;68(17):1851–1864. doi:10.1016/J.JACC.2016.07.760
9. Baber U, Mehran R, Giustino G, et al. Coronary Thrombosis and major bleeding after PCI with drug-eluting stents: risk scores from Paris. J Am Coll Cardiol. 2016;67(19):2224–2234. doi:10.1016/J.JACC.2016.02.064
10. Raposeiras-Roubín S, Faxén J, Íñiguez-romo A, et al. Development and external validation of a post-discharge bleeding risk score in patients with acute coronary syndrome: the BleeMACS score. Int J Cardiol. 2018;254:10–15. doi:10.1016/J.IJCARD.2017.10.103
11. De Groot NL, Hagenaars MP, Smeets HM, Steyerberg EW, Siersema PD, Van Oijen MGH. Primary non-variceal upper gastrointestinal bleeding in NSAID and low-dose aspirin users: development and validation of risk scores for either medication in two large Dutch cohorts. J Gastroenterol. 2014;49(2):245–253. doi:10.1007/S00535-013-0817-Y
12. Yeh RW, Secemsky EA, Kereiakes DJ, et al. Development and validation of a prediction rule for benefit and harm of dual antiplatelet therapy beyond 1 year after percutaneous coronary intervention. JAMA. 2016;315(16):1735–1749. doi:10.1001/JAMA.2016.3775
13. Ducrocq G, Wallace JS, Baron G, et al. Risk score to predict serious bleeding in stable outpatients with or at risk of atherothrombosis. Eur Heart J. 2010;31(10):1257–1265. doi:10.1093/EURHEARTJ/EHQ021
14. Costa F, van Klaveren D, James S, et al. Derivation and validation of the predicting bleeding complications in patients undergoing stent implantation and subsequent dual antiplatelet therapy (PRECISE-DAPT) score: a pooled analysis of individual-patient datasets from clinical trials. Lancet. 2017;389(10073):1025–1034. doi:10.1016/S0140-6736(17)30397-5
15. Brener SJ, Kirtane AJ, Rinaldi MJ, et al. Prediction of ischemic and bleeding events using the dual antiplatelet therapy score in an unrestricted percutaneous coronary intervention population: analysis from the ADAPT-DES registry. Circ Cardiovasc Interv. 2018;11(10). doi:10.1161/CIRCINTERVENTIONS.118.006853
16. Harada Y, Michel J, Lohaus R, et al. Validation of the DAPT score in patients randomized to 6 or 12 months clopidogrel after predominantly second-generation drug-eluting stents. Thromb Haemost. 2017;117(10):1989–1999. doi:10.1160/TH17-02-0101
17. Ueda P, Jernberg T, James S, et al. External validation of the DAPT score in a nationwide population. J Am Coll Cardiol. 2018;72(10):1069–1078. doi:10.1016/J.JACC.2018.06.023
18. Witberg G, Zusman O, Yahav D, Perl L, Vaknin-Assa H, Kornowski R. Meta-analysis of studies examining the external validity of the dual antiplatelet therapy score. Eur Heart J Cardiovasc Pharmacother. 2020;6(5):285–291. doi:10.1093/EHJCVP/PVZ075
19. Urban P, Mehran R, Colleran R, et al. Defining high bleeding risk in patients undergoing percutaneous coronary intervention: a consensus document from the academic research consortium for high bleeding risk. Eur Heart J. 2019;40(31):2632–2653. doi:10.1093/eurheartj/ehz372
20. Chiarito M, Luceri L, Oliva A, Stefanini G, Condorelli G. Artificial intelligence and cardiovascular risk prediction: all that glitters is not gold. Eur Cardiol Rev. 2022. doi:10.15420/ECR.2022.11
21. Krittanawong C, Zhang HJ, Wang Z, Aydar M, Kitai T. Artificial intelligence in precision cardiovascular medicine. J Am Coll Cardiol. 2017;69(21):2657–2664. doi:10.1016/J.JACC.2017.03.571
22. D’Ascenzo F, De Filippo O, Gallone G, et al. Machine learning-based prediction of adverse events following an acute coronary syndrome (PRAISE): a modelling study of pooled datasets. Lancet. 2021;397(10270):199–207. doi:10.1016/S0140-6736(20)32519-8
23. Pfisterer M, Brunner-La Rocca HP, Buser PT, et al. Late clinical events after clopidogrel discontinuation may limit the benefit of drug-eluting stents: an observational study of drug-eluting versus bare-metal stents. J Am Coll Cardiol. 2006;48(12):2584–2591. doi:10.1016/J.JACC.2006.10.026
24. Serruys PW, Daemen J. Stent thrombosis late after implantation of first-generation drug-eluting stents: a cause for concern. Circulation. 2007;115(11):1455. doi:10.1161/CIRCULATIONAHA.106.666800
25. Piccolo R, Bonaa KH, Efthimiou O, et al. Drug-eluting or bare-metal stents for percutaneous coronary intervention: a systematic review and individual patient data meta-analysis of randomised clinical trials. Lancet. 2019;393(10190):2503–2510.
26. Mauri L, Kereiakes DJ, Yeh RW, et al. Twelve or 30 months of dual antiplatelet therapy after drug-eluting stents. Engl J Med. 2014;371(23):2155–2166. doi:10.1056/NEJMoa1409312
27. Valgimigli M, Campo G, Monti M, et al. Short- versus long-term duration of dual-antiplatelet therapy after coronary stenting: a randomized multicenter trial. Circulation. 2012;125(16):2015–2026. doi:10.1161/CIRCULATIONAHA.111.071589
28. Collet JP, Silvain J, Barthélémy O, et al. Dual-antiplatelet treatment beyond 1 year after drug-eluting stent implantation (Arctic-Interruption): a randomised trial. Lancet. 2014;384(9954):1577–1585. doi:10.1016/S0140-6736(14)60612-7
29. Lee CW, Ahn JM, Park DW, et al. Optimal duration of dual antiplatelet therapy after drug-eluting stent implantation: a randomized, controlled trial. Circulation. 2014;129(3):304–312. doi:10.1161/CIRCULATIONAHA.113.003303
30. Helft G, Steg PG, Le Feuvre C, et al. Stopping or continuing clopidogrel 12 months after drug-eluting stent placement: the OPTIDUAL randomized trial. Eur Heart J. 2016;37(4):365–374. doi:10.1093/eurheartj/ehv481
31. Bonaca MP, Bhatt DL, Cohen M, et al. Long-term use of ticagrelor in patients with prior myocardial infarction. Engl J Med. 2015;372(19):1791–1800. doi:10.1056/NEJMoa1500857
32. Gilard M, Barragan P, Noryani AAL, et al. 6- versus 24-month dual antiplatelet therapy after implantation of drug-eluting stents in patients nonresistant to aspirin: the randomized, multicenter ITALIC trial. J Am Coll Cardiol. 2015;65(8):777–786. doi:10.1016/j.jacc.2014.11.008
33. Nakamura M, Iijima R, Ako J, et al. Dual antiplatelet therapy for 6 versus 18 months after biodegradable polymer drug-eluting stent implantation. JACC Cardiovasc Interv. 2017;10(12):1189–1198. doi:10.1016/j.jcin.2017.04.019
34. Steg PG, Bhatt DL, Simon T, et al. Ticagrelor in patients with stable coronary disease and diabetes. N Engl J Med. 2019;381(14):1309–1320. doi:10.1056/NEJMOA1908077
35. Palmerini T, Benedetto U, Bacchi-Reggiani L, et al. Mortality in patients treated with extended duration dual antiplatelet therapy after drug-eluting stent implantation: a pairwise and Bayesian network meta-analysis of randomised trials. Lancet. 2015;385(9985):2371–2382. doi:10.1016/S0140-6736(15)60263-X
36. Gwon HC, Hahn JY, Park KW, et al. Six-month versus 12-month dual antiplatelet therapy after implantation of drug-eluting stents: the Efficacy of Xience/Promus Versus Cypher to Reduce Late Loss After Stenting (EXCELLENT) randomized, multicenter study. Circulation. 2012;125(3):505–513. doi:10.1161/CIRCULATIONAHA.111.059022
37. Kim BK, Hong MK, Shin DH, et al. A new strategy for discontinuation of dual antiplatelet therapy: the RESET trial (REal Safety and efficacy of 3-month dual antiplatelet therapy following endeavor zotarolimus-eluting stent implantation). J Am Coll Cardiol. 2012;60(15):1340–1348. doi:10.1016/j.jacc.2012.06.043
38. Feres F, Costa RA, Abizaid A, et al. Three vs twelve months of dual antiplatelet therapy after zotarolimus-eluting stents: the OPTIMIZE randomized trial. JAMA. 2013;310(23):2510–2522. doi:10.1001/jama.2013.282183
39. Colombo A, Chieffo A, Frasheri A, et al. Second-generation drug-eluting stent implantation followed by 6- versus 12-month dual antiplatelet therapy: the SECURITY randomized clinical trial. J Am Coll Cardiol. 2014;64(20):2086–2097. doi:10.1016/j.jacc.2014.09.008
40. Schulz-Schüpke S, Byrne RA, ten Berg JM, et al. ISAR-SAFE: a randomized, double-blind, placebo-controlled trial of 6 vs. 12 months of clopidogrel therapy after drug-eluting stenting. Eur Heart J. 2015;36(20):1252–1263. doi:10.1093/eurheartj/ehu523
41. Han Y, Xu B, Xu K, et al. Six versus 12 months of dual antiplatelet therapy after implantation of biodegradable polymer sirolimus-eluting stent: randomized substudy of the I-LOVE-IT 2 trial. Circ Cardiovasc Interv. 2016;9(2). doi:10.1161/CIRCINTERVENTIONS.115.003145
42. Hong SJ, Shin DH, Kim JS, et al. 6-month versus 12-month dual-antiplatelet therapy following long everolimus-eluting stent implantation: the IVUS-XPL randomized clinical trial. JACC Cardiovasc Interv. 2016;9(14):1438–1446. doi:10.1016/j.jcin.2016.04.036
43. Hahn JY, Song YB, Oh JH, et al. 6-month versus 12-month or longer dual antiplatelet therapy after percutaneous coronary intervention in patients with acute coronary syndrome (SMART-DATE): a randomised, open-label, non-inferiority trial. Lancet. 2018;391(10127):1274–1284. doi:10.1016/S0140-6736(18)30493-8
44. Kedhi E, Fabris E, Van Der Ent M, et al. Six months versus 12 months dual antiplatelet therapy after drug-eluting stent implantation in ST-elevation myocardial infarction (DAPT-STEMI): randomised, multicentre, non-inferiority trial. BMJ. 2018;363. doi:10.1136/BMJ.K3793
45. Lee BK, Kim JS, Lee OH, et al. Safety of six-month dual antiplatelet therapy after second-generation drug-eluting stent implantation: OPTIMA-C randomised clinical trial and OCT substudy. EuroIntervention. 2020;13(16):1923–1930.
46. de Luca G, Damen SA, Camaro C, et al. Final results of the randomised evaluation of short-term dual antiplatelet therapy in patients with acute coronary syndrome treated with a new-generation stent (REDUCE trial). EuroIntervention. 2019;15(11):E990–E998. doi:10.4244/EIJ-D-19-00539
47. Watanabe H, Domei T, Morimoto T, et al. Effect of 1-month dual antiplatelet therapy followed by clopidogrel vs 12-month dual antiplatelet therapy on cardiovascular and bleeding events in patients receiving PCI: the STOPDAPT-2 randomized clinical trial. JAMA. 2019;321(24):2414–2427. doi:10.1001/jama.2019.8145
48. Urban P, Meredith IT, Abizaid A, et al. Polymer-free drug-coated coronary stents in patients at high bleeding risk. Engl J Med. 2015;373(21):2038–2047. doi:10.1056/NEJMOA1503943/SUPPL_FILE/NEJMOA1503943_DISCLOSURES.PDF
49. Windecker S, Latib A, Kedhi E, et al. Polymer-based or polymer-free stents in patients at high bleeding risk. Engl J Med. 2020;382(13):1208–1218. doi:10.1056/NEJMOA1910021/SUPPL_FILE/NEJMOA1910021_DATA-SHARING.PDF
50. Varenne O, Cook S, Sideris G, et al. Drug-eluting stents in elderly patients with coronary artery disease (SENIOR): a randomised single-blind trial. Lancet. 2018;391(10115):41–50. doi:10.1016/S0140-6736(17)32713-7
51. Mehran R, Cao D, Angiolillo DJ, et al. 3- or 1-month DAPT in patients at high bleeding risk undergoing everolimus-eluting stent implantation. JACC Cardiovasc Interv. 2021;14(17):1870–1883. doi:10.1016/j.jcin.2021.07.016
52. Valgimigli M, Frigoli E, Heg D, et al. Dual antiplatelet therapy after PCI in patients at high bleeding risk. Engl J Med. 2021;385(18):1643–1655. doi:10.1056/NEJMOA2108749/SUPPL_FILE/NEJMOA2108749_DATA-SHARING.PDF
53. Costa F, Montalto C, Branca M, et al. Dual antiplatelet therapy duration after percutaneous coronary intervention in high bleeding risk: a meta-analysis of randomized trials. Eur Heart J. 2022. doi:10.1093/EURHEARTJ/EHAC706
54. Vranckx P, Valgimigli M, Jüni P, et al. Ticagrelor plus aspirin for 1 month, followed by ticagrelor monotherapy for 23 months vs aspirin plus clopidogrel or ticagrelor for 12 months, followed by aspirin monotherapy for 12 months after implantation of a drug-eluting stent: a multicentre, open-label, randomised superiority trial. Lancet. 2018;392(10151):940–949. doi:10.1016/S0140-6736(18)31858-0
55. Mehran R, Baber U, Sharma SK, et al. Ticagrelor with or without aspirin in high-risk patients after PCI. Engl J Med. 2019;381(21):2032–2042. doi:10.1056/NEJMOA1908419/SUPPL_FILE/NEJMOA1908419_DATA-SHARING.PDF
56. Lee SJ, Lee YJ, Kim BK, et al. Ticagrelor monotherapy versus ticagrelor with aspirin in acute coronary syndrome patients with a high risk of ischemic events. Circ Cardiovasc Interv. 2021;14:e010812.
57. Watanabe H, Morimoto T, Natsuaki M, et al. Comparison of clopidogrel monotherapy after 1 to 2 months of dual antiplatelet therapy with 12 months of dual antiplatelet therapy in patients with acute coronary syndrome: the STOPDAPT-2 ACS randomized clinical trial. JAMA Cardiol. 2022;7(4):407–417. doi:10.1001/JAMACARDIO.2021.5244
58. Choi KH, Park YH, Song B, et al. Long-term effects of P2Y12 inhibitor monotherapy after percutaneous coronary intervention: 3-year follow-up of the SMART-CHOICE randomized clinical trial. JAMA Cardiol. 2022;7(11):1100–1108. doi:10.1001/JAMACARDIO.2022.3203
59. Hahn JY, Song YB, Oh JH, et al. Effect of P2Y12 inhibitor monotherapy vs dual antiplatelet therapy on cardiovascular events in patients undergoing percutaneous coronary intervention: the SMART-CHOICE randomized clinical trial. JAMA. 2019;321(24):2428–2437. doi:10.1001/JAMA.2019.8146
60. Obayashi Y, Watanabe H, Morimoto T, et al. Clopidogrel monotherapy after 1-month dual antiplatelet therapy in percutaneous coronary intervention: from the STOPDAPT-2 total cohort. Circ Cardiovasc Interv. 2022;15(8):E012004. doi:10.1161/CIRCINTERVENTIONS.122.012004
61. Armstrong PCJ, Leadbeater PD, Chan MV, et al. In the presence of strong P2Y12 receptor blockade, aspirin provides little additional inhibition of platelet aggregation. J Thromb Haemost. 2011;9(3):552–561. doi:10.1111/J.1538-7836.2010.04160.X
62. Angiolillo DJ, Baber U, Mehran R. Ticagrelor monotherapy in patients with diabetes mellitus undergoing percutaneous coronary interventions: insights from the TWILIGHT trial. Cardiovasc Res. 2020;116(7):E70–E72. doi:10.1093/CVR/CVAA120
63. Escaned J, Cao D, Baber U, et al. Ticagrelor monotherapy in patients at high bleeding risk undergoing percutaneous coronary intervention: TWILIGHT-HBR. Eur Heart J. 2021;42(45):4624–4634. doi:10.1093/EURHEARTJ/EHAB702
64. Dangas G, Baber U, Sharma S, et al. Ticagrelor with or without aspirin after complex PCI. J Am Coll Cardiol. 2020;75(19):2414–2424. doi:10.1016/J.JACC.2020.03.011
65. Kim BK, Hong SJ, Cho YH, et al. Effect of ticagrelor monotherapy vs ticagrelor with aspirin on major bleeding and cardiovascular events in patients with acute coronary syndrome: the TICO randomized clinical trial. JAMA. 2020;323(23):2407–2416. doi:10.1001/jama.2020.7580
66. Valgimigli M, Gragnano F, Branca M, et al. P2Y12 inhibitor monotherapy or dual antiplatelet therapy after coronary revascularisation: individual patient level meta-analysis of randomised controlled trials. BMJ. 2021;373:n1332. doi:10.1136/bmj.n1332
67. Valgimigli M, Mehran R, Franzone A, et al. Ticagrelor monotherapy versus dual-antiplatelet therapy after PCI: an individual patient-level meta-analysis. JACC Cardiovasc Interv. 2021;14(4):444–456.
68. Mega JL, Simon T, Collet JP, et al. Reduced-function CYP2C19 genotype and risk of adverse clinical outcomes among patients treated with clopidogrel predominantly for PCI: a meta-analysis. JAMA. 2010;304(16):1821–1830. doi:10.1001/JAMA.2010.1543
69. Aradi D, Kirtane A, Bonello L, et al. Bleeding and stent thrombosis on P2Y12-inhibitors: collaborative analysis on the role of platelet reactivity for risk stratification after percutaneous coronary intervention. Eur Heart J. 2015;36(27):1762–1771. doi:10.1093/EURHEARTJ/EHV104
70. Pereira NL, Rihal C, Lennon R, et al. Effect of CYP2C19 genotype on ischemic outcomes during oral P2Y12 inhibitor therapy: a meta-analysis. JACC Cardiovasc Interv. 2021. doi:10.1016/j.jcin.2021.01.024
71. Sibbing D, Aradi D, Alexopoulos D, et al. Updated expert consensus statement on platelet function and genetic testing for guiding P2Y12 receptor inhibitor treatment in percutaneous coronary intervention. JACC Cardiovasc Interv. 2019;12(16):1521–1537. doi:10.1016/j.jcin.2019.03.034
72. Sibbing D, Aradi D, Jacobshagen C, et al. Guided de-escalation of antiplatelet treatment in patients with acute coronary syndrome undergoing percutaneous coronary intervention (TROPICAL-ACS): a randomised, open-label, multicentre trial. Lancet. 2017;390(10104):1747–1757. doi:10.1016/S0140-6736(17)32155-4
73. Claassens DMF, Vos GJA, Bergmeijer TO, et al. A genotype-guided strategy for oral P2Y12 inhibitors in primary PCI. N Engl J Med. 2019;1(1):1. doi:10.1056/NEJMoa1907096
74. Pereira NL, Farkouh ME, So D, et al. Effect of genotype-guided oral P2Y12 inhibitor selection vs conventional clopidogrel therapy on ischemic outcomes after percutaneous coronary intervention: the TAILOR-PCI randomized clinical trial. JAMA. 2020;324(8):761–771. doi:10.1001/jama.2020.12443
75. Capodanno D, Angiolillo DJ, Lennon RJ, et al. ABCD-GENE score and clinical outcomes following percutaneous coronary intervention: insights from the TAILOR-PCI trial. J Am Heart Assoc. 2022;11(4):24156. doi:10.1161/JAHA.121.024156
76. Galli M, Benenati S, Capodanno D, et al. Guided versus standard antiplatelet therapy in patients undergoing percutaneous coronary intervention: a systematic review and meta-analysis. Lancet. 2021;397(10283):1470–1483. doi:10.1016/S0140-6736(21)00533-X
77. Antithrombotic Trialists’ Collaboration. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ. 2002;324(7329):71–86. doi:10.1136/bmj.324.7329.71
78. Bhatt DL, Steg PG, Mehta SR, et al. Ticagrelor in patients with diabetes and stable coronary artery disease with a history of previous percutaneous coronary intervention (THEMIS-PCI): a Phase 3, placebo-controlled, randomised trial. Lancet. 2019;394(10204):1169–1180. doi:10.1016/S0140-6736(19)31887-2
79. Chiarito M, Sanz-Sánchez J, Cannata F, et al. Monotherapy with a P2Y12 inhibitor or aspirin for secondary prevention in patients with established atherosclerosis: a systematic review and meta-analysis. Lancet. 2020;395(10235):1487–1495. doi:10.1016/S0140-6736(20)30315-9
80. Koo BK, Kang J, Park KW, et al. Aspirin versus clopidogrel for chronic maintenance monotherapy after percutaneous coronary intervention (HOST-EXAM): an investigator-initiated, prospective, randomised, open-label, multicentre trial. Lancet. 2021;397(10293):2487–2496. doi:10.1016/S0140-6736(21)01063-1
81. Kang J, Park KW, Lee H, et al. Aspirin versus clopidogrel for long-term maintenance monotherapy after percutaneous coronary intervention: the HOST-EXAM extended study. Circulation. 2023;147(2):108–117. doi:10.1161/CIRCULATIONAHA.122.062770
82. Valgimigli M. P2Y12 inhibitor or aspirin monotherapy as secondary prevention in patients with coronary artery disease: an individual participant data meta-analysis of randomised controlled trials.
83. Baber U, Kini AS, Sharma SK. Stenting of complex lesions: an overview. Nat Rev Cardiol. 2010;7(9):485–496. doi:10.1038/NRCARDIO.2010.116
84. Yamamoto K, Shiomi H, Morimoto T, et al. Ischemic and bleeding risk after complex percutaneous coronary intervention in patients with or without high bleeding risk. Catheter Cardiovasc Interv. 2021;97(6):E758–E770. doi:10.1002/CCD.29335
85. Costa F, Van Klaveren D, Feres F, et al. Dual antiplatelet therapy duration based on ischemic and bleeding risks after coronary stenting. J Am Coll Cardiol. 2019;73(7):741–754.
86. Silvain J, Lattuca B, Beygui F, et al. Ticagrelor versus clopidogrel in elective percutaneous coronary intervention (ALPHEUS): a randomised, open-label, phase 3b trial. Lancet. 2020;396(10264):1737–1744. doi:10.1016/S0140-6736(20)32236-4
87. Oliva A, Castiello DS, Franzone A, et al. P2Y12 inhibitors monotherapy in patients undergoing complex vs non-complex percutaneous coronary intervention: a meta-analysis of randomized trials. Am Heart J. 2023;255:71–81. doi:10.1016/J.AHJ.2022.10.006
88. Nicolas J, Dangas G, Chiarito M, et al. Efficacy and safety of P2Y12 inhibitor monotherapy after complex PCI: a collaborative systematic review and meta-analysis. Eur Heart J Cardiovasc Pharmacother. 2022. doi:10.1093/EHJCVP/PVAC071
89. Gragnano F, Mehran R, Branca M, et al. P2Y12 inhibitor monotherapy or dual antiplatelet therapy after complex percutaneous coronary interventions. J Am Coll Cardiol. 2023;81(6):537–552. doi:10.1016/J.JACC.2022.11.041
90. Capodanno D, Milluzzo RP, Angiolillo DJ. Intravenous antiplatelet therapies (glycoprotein IIb/IIIa receptor inhibitors and cangrelor) in percutaneous coronary intervention: from pharmacology to indications for clinical use. Ther Adv Cardiovasc Dis. 2019;13. doi:10.1177/1753944719893274/ASSET/IMAGES/LARGE/10.1177_1753944719893274-FIG2.JPEG
91. Bhatt DL, Stone GW, Mahaffey KW, et al. Effect of platelet inhibition with cangrelor during PCI on ischemic events. N Engl J Med. 2013;368(14). doi:10.1056/NEJMOA1300815
92. Stone GW, Généreux P, Harrington RA, et al. Impact of lesion complexity on peri-procedural adverse events and the benefit of potent intravenous platelet adenosine diphosphate receptor inhibition after percutaneous coronary intervention: core laboratory analysis from 10 854 patients from the CHAMPION Phoenix trial. Eur Heart J. 2018;39(46):4112–4121. doi:10.1093/EURHEARTJ/EHY562
93. Franchi F, Rollini F, Rivas A, et al. Platelet inhibition with cangrelor and crushed ticagrelor in patients with ST-segment-elevation myocardial infarction undergoing primary percutaneous coronary intervention. Circulation. 2019;139(14):1661–1670. doi:10.1161/CIRCULATIONAHA.118.038317
94. Sumaya W, Parker WAE, Fretwell R, et al. Pharmacodynamic effects of a 6-hour regimen of enoxaparin in patients undergoing primary percutaneous coronary intervention (PENNY PCI study). Thromb Haemost. 2018;118(7). doi:10.1055/s-0038-1657768
95. Angiolillo DJ, Firstenberg MS, Price MJ, et al. Bridging antiplatelet therapy with cangrelor in patients undergoing cardiac surgery: a randomized controlled trial. JAMA. 2012;307(3):265–274. doi:10.1001/JAMA.2011.2002
96. Cao D, Chandiramani R, Capodanno D, et al. Non-cardiac surgery in patients with coronary artery disease: risk evaluation and periprocedural management. Nat Rev Cardiol. 2021;18(1):37–57. doi:10.1038/S41569-020-0410-Z
97. Rossini R, Tarantini G, Musumeci G, et al. A multidisciplinary approach on the perioperative antithrombotic management of patients with coronary stents undergoing surgery: surgery after stenting 2. JACC Cardiovasc Interv. 2018;11(5):417–434. doi:10.1016/J.JCIN.2017.10.051
98. Parker WAE, Storey RF. Pharmacology and potential role of selatogrel, a subcutaneous platelet P2Y12 receptor antagonist. Expert Opin Emerg Drugs. 2020;25(1):1–6. doi:10.1080/14728214.2020.1729121
99. Sinnaeve P, Fahrni G, Schelfaut D, et al. Subcutaneous selatogrel inhibits platelet aggregation in patients with acute myocardial infarction. J Am Coll Cardiol. 2020;75(20):2588–2597. doi:10.1016/J.JACC.2020.03.059
100. Gibson CM, Mehran R, Bode C, et al. Prevention of bleeding in patients with atrial fibrillation undergoing PCI. Engl J Med. 2016;375(25):2423–2434. doi:10.1056/NEJMOA1611594/SUPPL_FILE/NEJMOA1611594_DISCLOSURES.PDF
101. Cannon CP, Bhatt DL, Oldgren J, et al. Dual antithrombotic therapy with dabigatran after PCI in atrial fibrillation. Engl J Med. 2017;377(16):1513–1524. doi:10.1056/NEJMOA1708454/SUPPL_FILE/NEJMOA1708454_DISCLOSURES.PDF
102. Lopes RD, Heizer G, Aronson R, et al. Antithrombotic therapy after acute coronary syndrome or PCI in atrial fibrillation. Engl J Med. 2019;380(16):1509–1524. doi:10.1056/NEJMOA1817083/SUPPL_FILE/NEJMOA1817083_DATA-SHARING.PDF
103. Vranckx P, Valgimigli M, Eckardt L, et al. Edoxaban-based versus vitamin K antagonist-based antithrombotic regimen after successful coronary stenting in patients with atrial fibrillation (ENTRUST-AF PCI): a randomised, open-label, phase 3b trial. Lancet. 2019;394(10206):1335–1343. doi:10.1016/S0140-6736(19)31872-0
104. Yasuda S, Kaikita K, Akao M, et al. Antithrombotic therapy for atrial fibrillation with stable coronary disease. Engl J Med. 2019;381(12):1103–1113. doi:10.1056/NEJMOA1904143/SUPPL_FILE/NEJMOA1904143_DATA-SHARING.PDF
105. Angiolillo DJ, Bhatt DL, Cannon CP, et al. Antithrombotic therapy in patients with atrial fibrillation treated with oral anticoagulation undergoing percutaneous coronary intervention. Circulation. 2021;143(6):583–596. doi:10.1161/CIRCULATIONAHA.120.050438
106. Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2019;50(12):E344–E418. doi:10.1161/STR.0000000000000211
107. Chen ZM. CAST: randomised placebo-controlled trial of early aspirin use in 20,000 patients with acute ischaemic stroke. Lancet. 1997;349(9066):1641–1649. doi:10.1016/S0140-6736(97)04010-5
108. Sandercock PAG. The International Stroke Trial (IST): a randomised trial of aspirin, subcutaneous heparin, both, or neither among 19 435 patients with acute ischaemic stroke. Lancet. 1997;349(9065):1569–1581. doi:10.1016/S0140-6736(97)04011-7
109. Gent M. A randomised, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events (CAPRIE). Lancet. 1996;348(9038):1329–1339. doi:10.1016/S0140-6736(96)09457-3
110. Paciaroni M, Ince B, Hu B, et al. Benefits and risks of clopidogrel vs. aspirin monotherapy after recent ischemic stroke: a systematic review and meta-analysis. Cardiovasc Ther. 2019;2019. doi:10.1155/2019/1607181
111. Diener PHC, Bogousslavsky PJ, Brass PLM, et al. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or transient ischaemic attack in high-risk patients (MATCH): randomised, double-blind, placebo-controlled trial. Lancet. 2004;364(9431):331–337. doi:10.1016/S0140-6736(04)16721-4
112. Sacco RL, Diener HC, Yusuf S, et al. Aspirin and extended-release dipyridamole versus clopidogrel for recurrent stroke. Engl J Med. 2008;359(12):1238–1251. doi:10.1056/NEJMOA0805002
113. Johnston SC, Amarenco P, Albers GW, et al. Ticagrelor versus aspirin in acute stroke or transient ischemic attack. Engl J Med. 2016;375(1):35–43. doi:10.1056/NEJMOA1603060
114. Fergus IV. Effects of clopidogrel added to aspirin in patients with recent lacunar stroke. Cardiol Rev. 2012;28(6). doi:10.1056/NEJMOA1204133
115. Bhatt DL, Fox KAA, Hacke W, et al. Clopidogrel and aspirin versus aspirin alone for the prevention of atherothrombotic events. Engl J Med. 2006;354(16):1706–1717. doi:10.1056/NEJMOA060989
116. Johnston SC, Amarenco P, Denison H, et al. Ticagrelor and aspirin or aspirin alone in acute ischemic stroke or TIA. Engl J Med. 2020;383(3):207–217. doi:10.1056/NEJMOA1916870/SUPPL_FILE/NEJMOA1916870_DATA-SHARING.PDF
117. Aboyans V, Bauersachs R, Mazzolai L, et al. Antithrombotic therapies in aortic and peripheral arterial diseases in 2021: a consensus document from the ESC working group on aorta and peripheral vascular diseases, the ESC working group on thrombosis, and the ESC working group on cardiovascular pharma. Eur Heart J. 2021. doi:10.1093/eurheartj/ehab390
118. Bhatt DL, Flather MD, Hacke W, et al. Patients with prior myocardial infarction, stroke, or symptomatic peripheral arterial disease in the CHARISMA trial. J Am Coll Cardiol. 2007;49(19):1982–1988. doi:10.1016/j.jacc.2007.03.025
119. Hiatt WR, Fowkes FGR, Heizer G, et al. Ticagrelor versus clopidogrel in symptomatic peripheral artery disease. Engl J Med. 2017;376(1):32–40. doi:10.1056/NEJMOA1611688
120. Eikelboom JW, Connolly SJ, Bosch J, et al. Rivaroxaban with or without aspirin in stable cardiovascular disease. Engl J Med. 2017;377(14):1319–1330. doi:10.1056/NEJMoa1709118
121. Anand SS, Bosch J, Eikelboom JW, et al. Rivaroxaban with or without aspirin in patients with stable peripheral or carotid artery disease: an international, randomised, double-blind, placebo-controlled trial. Lancet. 2018;391(10117):219–229. doi:10.1016/S0140-6736(17)32409-1
122. Bonaca MP, Bauersachs RM, Anand SS, et al. Rivaroxaban in peripheral artery disease after revascularization. Engl J Med. 2020;382(21):1994–2004. doi:10.1056/NEJMOA2000052
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Budget Impact of Cangrelor in the UK for the Treatment of Out-of-Hospital Cardiac Arrest Patients Who Require Percutaneous Coronary Intervention
Modi B, Cain R, Stork R, Barwood C, Tarpey G, Colucciello A
ClinicoEconomics and Outcomes Research 2025, 17:189-197
Published Date: 15 March 2025