Back to Journals » Psychology Research and Behavior Management » Volume 18
Personality Traits and Social Support: Their Role in Postpartum Depression
Authors Richa S, Parveen S, Abullais SS, Mahmood SE ![]() , Alsamghan A, Alshaikh AA
, Alsamghan A, Alshaikh AA
Received 3 February 2025
Accepted for publication 9 July 2025
Published 10 August 2025 Volume 2025:18 Pages 1685—1699
DOI https://doi.org/10.2147/PRBM.S507701
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Saumya Richa,1,* Sumaila Parveen,2,* Shahabe Saquib Abullais,3,* Syed Esam Mahmood,4,* Awad Alsamghan,4,* Ayoub Ali Alshaikh4,*
1Department of Psychology, Lovely Professional University, Phagwara, Punjab, India; 2Department of Anesthesia and Operations, College of Applied Medical Sciences, King Khalid University, Muhayil Asir, Saudi Arabia; 3Department of Periodontics and Community Dental Science, College of Dentistry, King Khalid University, Abha, Saudi Arabia; 4Department of Family & Community Medicine, College of Medicine, King Khalid University, Abha, Saudi Arabia
*These authors contributed equally to this work
Correspondence: Syed Esam Mahmood, Department of Family and Community Medicine, College of Medicine, King Khalid University, Al-Qaraa Campus, P.O. Box 641, Abha, 62529, Saudi Arabia, Email [email protected]
Introduction: Postpartum depression (PPD) is a significant mood disorder occurring within the first year after childbirth, characterized by persistent sadness, fatigue, and bonding difficulties. This study focuses on mothers in Aurangabad, Bihar—a region with limited health-care facilities, high poverty, low education, and strong cultural beliefs about motherhood and mental health. We hypothesized that positive Big Five personality traits correlate with lower PPD levels, and that social support enhances this protective effect.
Methods: This cross-sectional survey involved 300 mothers of children aged 1– 2 years, recruited via convenience sampling between February and April 2023. Data collection used face-to-face interviews with the Big Five Inventory (BFI), Multidimensional Scale of Perceived Social Support (MSPSS), and Edinburgh Postnatal Depression Scale (EPDS). Analyses included descriptive statistics, correlation analysis, moderation testing with PROCESS macro (SPSS v4.2), and Structural Equation Modeling (SEM).
Results: The average EPDS score was 7.9 (SD = 4.3), indicating generally low to moderate levels of PPD. Higher depression scores were significantly associated with neuroticism (r = 0.51, p < 0.01), lower extraversion, older mothers’ age, and lower income. Perceived social support did not directly predict PPD but marginally moderated the relationship between personality traits and depression (interaction p = 0.0995), with reduced effect at higher levels of support (p = 0.2245). SEM supported partial indirect effects but did not indicate strong mediation.
Conclusion: Personality traits, particularly neuroticism, are key predictors of PPD in this population. While social support shows a limited moderating effect, it may offer modest protective benefits under certain conditions. The findings underscore the need for early psychological screening, especially for neuroticism, and tailored support interventions for new mothers. Given the cross-sectional design and sampling method, results should be interpreted cautiously. Longitudinal studies are recommended for further validation.
Keywords: postpartum depression, personality traits, social support, Big Five Inventory, cross-sectional study, perceived social support, moderation analysis, structural equation modeling
Introduction
Postpartum depression (PPD) is a psychological condition increasingly recognized for its profound impact on new parents, particularly mothers. Occurring within the first year after childbirth, PPD is a mood disorder characterized by persistent symptoms such as overwhelming sadness, mood swings, hopelessness, fatigue, and difficulty bonding with the infant. Unlike the transient “baby blues”, which typically resolve within two weeks, PPD is more severe and enduring, often requiring professional intervention. If untreated, it can persist for months, significantly affecting the parent, child, and family dynamics.1,2
The Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5), classifies PPD under the broader term “postpartum depression”, encompassing depressive episodes that begin during pregnancy or within four weeks postpartum. However, PPD symptoms may not manifest until much later, with some individuals experiencing symptoms as late as one year after childbirth. This condition, often overlooked or misunderstood, affects approximately 13% of women globally, with rates rising to 20% in developing countries.3
PPD is a multifactorial disorder influenced by biological, psychological, and social factors. Hormonal changes, previous depressive episodes, significant life stressors, and a lack of social support are key contributors to its development. Additional risk factors include young maternal age, emergency cesarean sections, multiple births, immigrant status, obesity, and specific personality traits. For instance, sensitive personality traits have been positively correlated with a heightened likelihood of developing PPD.4,5
Social support plays a critical role in mitigating the risk of PPD. Insufficient support from partners, family, and friends significantly exacerbates the likelihood of depressive symptoms. Research has consistently demonstrated that social support reduces psychological distress and improves new mothers’ well-being while navigating parenthood challenges.6–8 Furthermore, experiences of abuse, unplanned pregnancies, and the absence of culturally competent services have been associated with increased maternal depressive symptoms.9–12
The Big Five personality traits—Neuroticism, Extraversion, Agreeableness, Conscientiousness, and Openness to Experience13—significantly influence how individuals respond to emotional and environmental stimuli. Neuroticism, in particular, has been consistently linked to a higher risk of developing PPD, while Conscientiousness, Extraversion, Openness, and Agreeableness are associated with a lower risk.14–17 The decision to focus on the Big Five personality traits in this study is grounded in their comprehensive nature, offering a robust framework for understanding the psychological predispositions that influence emotional regulation, stress responses, and coping strategies—all of which are crucial during the postpartum period. These five broad traits (Neuroticism, Extraversion, Openness, Agreeableness, and Conscientiousness) capture stable, cross-culturally validated dimensions of personality13 and have been consistently linked to mental health outcomes, including depression risk. Importantly, the interaction between these personality traits and the level of social support available to new mothers may moderate the development of postpartum depression (PPD), making this an important and underexplored area of research. The role of social support in postpartum mental health has been well documented, with numerous studies demonstrating that perceived support buffers against the negative effects of stress and reduces the risk of PPD.18 Over the past 30 years, research has repeatedly emphasized that social support—whether emotional, instrumental, or informational—plays a protective role in maintaining maternal mental well-being during and after pregnancy. The stress-buffering hypothesis, originally proposed by Cohen and Wills,19 provides a strong theoretical foundation for this investigation. It posits that social support, through the provision of psychological and material resources by one’s social network, can lessen the adverse behavioral and biological effects of stress, thereby reducing health risks over time. Despite the growing body of research on personality and postpartum mental health, limited attention has been paid to how the interaction between personality traits and social support shapes PPD outcomes. This study aims to address this gap by exploring the relationship between personality traits and PPD, examining the moderating role of perceived social support in this relationship, and assessing both direct and indirect effects using Structural Equation Modeling (SEM). By doing so, the study seeks to provide a deeper understanding of the complex interplay between individual differences and social resources in shaping postpartum experiences and maternal mental health outcomes.
Materials and Methods
Design
All participants provided informed consent before being included in the study, and responses were kept anonymous throughout the research procedure. Eligible participants were recruited using a convenience sampling method. Mothers attending postnatal clinics or residing in nearby communities were invited to participate, provided they met the specified inclusion criteria. The inclusion criteria specified that mothers must have children aged one to two years, provide informed consent to participate in the study, and have no history of severe physical illness. A “history of severe physical disease” was defined as any chronic or debilitating medical condition requiring prolonged hospitalisation or ongoing medical intervention, such as cancer, severe cardiovascular conditions, or end- stage renal disease. The research question aimed to understand how these personality traits influence postpartum depression (PPD) and how social support impacts this relationship. We hypothesised that there is a positive correlation between beneficial Big Five traits (like extraversion and agreeableness) and lower PPD levels, and that social support enhances the positive effects of these traits in reducing PPD. The investigation involved the administration of postnatal surveys conducted in various health-care facilities. Researchers and qualified medical professionals administered the surveys during clinic visits or in postnatal wards. Mothers were invited to participate in face- to- face interviews using validated instruments, including the Big Five Personality Traits Inventory to assess personality dimensions, the Edinburgh Postnatal Depression Scale (EPDS) to measure the severity of postpartum depressive symptoms, and the Multidimensional Scale of Perceived Social Support (MSPSS) to evaluate perceived availability of social support. A demographic questionnaire was also included to collect age, education, occupation, and socioeconomic status data. Data collection was conducted offline via face-to-face interactions to ensure accurate responses. Interviews were held in private settings within the health-care facilities to encourage participants’ comfort. For mothers who had not completed the survey during their initial interaction or had yet to reach the required postpartum period, follow- up was conducted through reminder phone calls. This approach helped maximize response rates and included mothers whose children were one to two years old. Initially, 500 mothers were recruited for the study. After excluding incomplete or invalid responses—such as questionnaires with missing data or inconsistencies, a final sample of 300 participants was included in the analysis. The study team ensured data reliability and participant adherence to survey completion. This study was conducted in accordance with the ethical principles of the Declaration of Helsinki. Before the data collection began, the Institutional Review Board of Lovely Professional University ethical approval (LPU/IEC-LPU/2024/3/4) was obtained.
Study Participants
Participants were eligible if they met the following requirements: 1) could understand English; 2) had given birth within one to two years; 3) had no history of severe physical diseases; 4) signed an informed consent form and agreed to participate in the survey. Mothers with more than four deliveries or any other severe postpartum illnesses were excluded. Pregnant women who declined to take part in the study or withdrew midway were also excluded.
Measurements
Sociodemographic and Obstetrical Characteristics Questionnaire
This questionnaire was created to gather primary participant data based on previous studies. Information collected included age, location, qualifications, average monthly family income, work status, substance abuse, delivery type, birth order, place of childbirth, partner and in-law relationships, family and marriage types, post-marriage motherhood experiences, conception preparation, method of conception, and pregnancy complications. Data about the infant’s gender, birth mode, and breastfeeding habits were collected for the first two years following delivery.
The Edinburgh Postpartum Depression Scale (EPDS)
Cox et al20 developed the Edinburgh Postpartum Depression Scale. There are ten brief remarks on the scale. Based on the severity of the ailment, responses are given a score of 0, 1, 2, or 3. Reverse scoring applies to items 3, 5, and 10 (ie, 3, 2, 1, and 0). The EPDS had an internal consistency rating of 0.83.21
Multidimensional Social Support (MSPSS)
A 12-item self-report survey with three subscales— Zimet et al22 developed the Multidimensional Scale of Perceived Social Support (MSPSS), which measures support from family, friends, and significant others. More points correspond to more social support being perceived. Its test–retest reliability and internal consistency are good (α = 0.85–0.91).23
Big Five Personality Scale (Big5)
The Big Five Personality Inventory-10 (BFI-10), a shorter version developed by Rammstedt and John in 2007, was used with some adaptations. In under a minute, the personality assessment is a condensed 10-item German and English version of the Big Five Inventory. According to Rammstedt & John, the ultrashort versions of the BFI preserve notable validity and reliability, which is essential when conducting surveys in a constrained amount of time.24
Data Collection
Mothers in Aurangabad, Bihar, India, participated in a cross-sectional survey using a convenience sample conducted between 1st February 2023 and 30th April 2023 across multiple clinics and wards. All participants provided informed consent at the start of the survey after being informed about the study’s purpose, content, duration, and voluntary nature. Information regarding withdrawal rights, potential risks and benefits, confidentiality, and results dissemination was also presented. Written informed consent was obtained from each participant before proceeding. Participants were guided on how to complete the questionnaire to ensure accurate data collection. Of the 500 mothers initially approached, 450 consented to participate. The survey included the BFI-10, EPDS, MSPSS, and a demographic questionnaire. After screening, 150 mothers were excluded due to incomplete surveys or failure to meet inclusion criteria. Offline follow-ups were conducted to finalize data collection. Three hundred complete responses were retained, yielding a 60% response rate.
Data Analysis
Data were analyzed using IBM SPSS Statistics 27.0 and AMOS Graphics 26.0. Descriptive statistics, including frequencies, means, percentages, and standard deviations, were utilised to evaluate sociodemographic data, Big Five personality traits, EPDS scores, and MSPSS scores. Pearson correlation coefficients assessed the relationships between postpartum depression, personality traits, perceived social support, and demographic variables. Additionally, the internal consistency of the measurement tools was re-evaluated. Socio-demographic factors such as age, education, income, and qualifications were examined for their association with postpartum depression (PPD). Following these analyses, personality traits and social support were analysed as predictors. Structural Equation Modeling (SEM) explored the relationships between personality traits, social support, and PPD. Mediation effects were assessed using the product of coefficients method and bootstrapping with 5000 samples. The bootstrap method generated 95% confidence intervals for the mediation effects. Model fit was evaluated using various indices, including the Tucker-Lewis Index (TLI), degrees of freedom (df), Goodness-of-Fit Index (GFI), Adjusted GFI (AGFI), Comparative Fit Index (CFI), Chi-square statistics (CMIN), and the Root Mean Square Error of Approximation (RMSEA). A two-tailed significance level of 0.05 was applied for all analyses.
To ensure adequate statistical power for our SEM analyses, we conducted an a priori power analysis using Daniel Soper’s (2025) online sample size calculator for SEM.25 Our model comprises 32 observed variables and 3 latent constructs. Assuming a medium effect size (f² = 0.30) as recommended by Cohen (1988), with an alpha level of 0.05 and a desired power of 0.80, the minimum required sample size was approximately 190 participants. Our actual sample of 300 participants exceeds this threshold, providing sufficient power to detect both direct and indirect effects. Additionally, in accordance with Kline’s (2016) guidelines for SEM, models of moderate complexity26,27 should include at least 200 cases to ensure parameter stability and reliable estimation. Our sample comfortably surpasses this recommendation, further supporting the robustness of our findings.
Results
Participants Characteristics
A total of 300 mothers participated in the survey. Their age at childbirth ranged from 18 to 40 years, with a mean age of 27.37 years (SD = 4.3). Table 1 presents the sociodemographic profile of the participants.
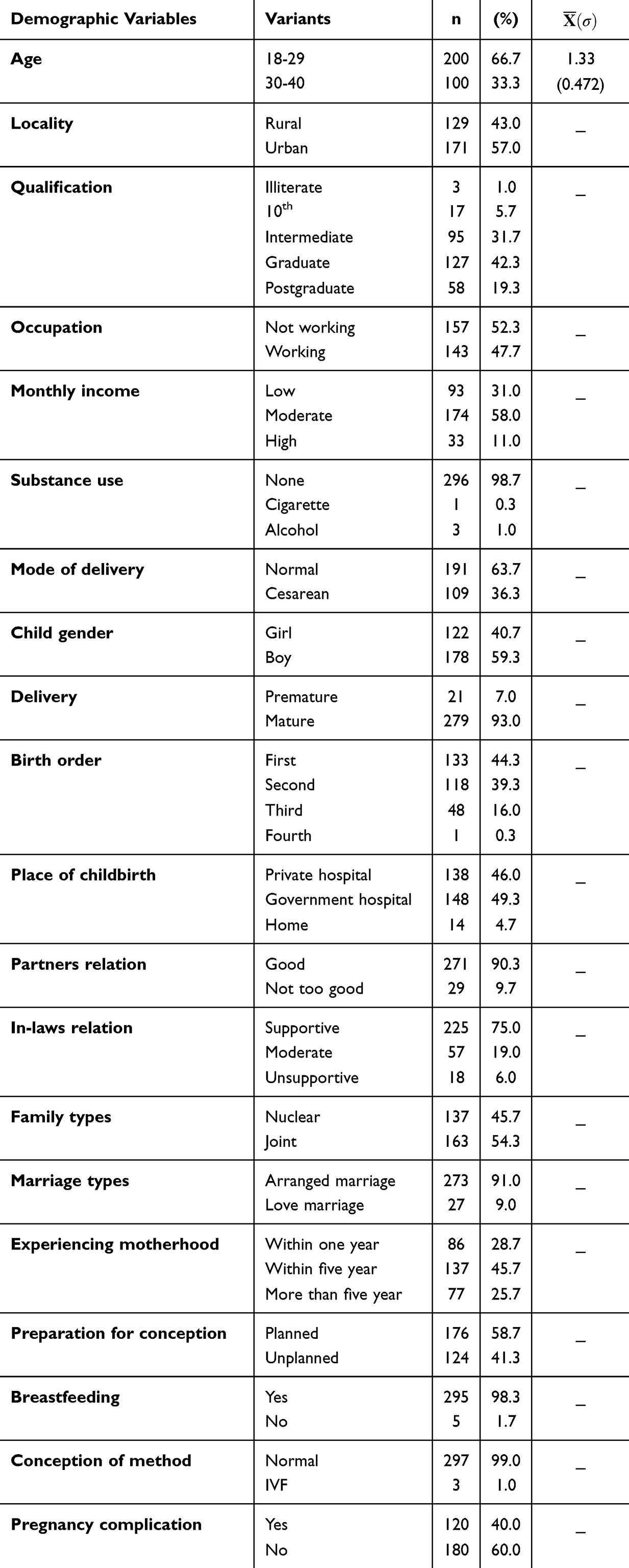 |
Table 1 Participants’ Sociodemographic Details |
Descriptive Statistics of the Measurements
Table 2 presents the descriptive statistics for postpartum depression, perceived social support, and Big Five personality traits. The mean EPDS (Edinburgh Postnatal Depression Scale) score was 13.14 (SD = 4.15), with a range of 24, indicating that a substantial number of participants reported moderate to high levels of postpartum depressive symptoms. Notably, 142 out of 300 participants (47.3%) scored above the clinical threshold of 13, suggesting a high likelihood of postpartum depression symptoms in nearly half of the sample. Perceived social support was measured using the Multidimensional Scale of Perceived Social Support (MSPSS), yielding a total mean score of 16.13 (SD = 3.67, range = 18), indicating a moderate level of perceived support. Based on the scale response descriptors by Zimet et al,28 mean scale scores from 1 to 2.9 indicate low support, 3 to 5 indicate moderate support, and 5.1 to 7 reflect high support. Accordingly, the subscale means reflect high perceived support from each source: Family (eg, immediate family) = 5.50 (SD = 1.42), Friends (peers/social circle) = 5.19 (SD = 1.41), and Significant Others (partners/spouses) = 5.43 (SD = 1.32). These results suggest that participants generally experienced strong support across all three domains, with Family emerging as the most prominent source. The composite Big Five personality traits score averaged 30.22 (SD = 3.17), with a range of 16.00. Among the individual traits, Extraversion showed the highest mean score (6.39, SD = 1.79, range = 8.00), followed by Openness = 6.08 (SD = 1.93, range = 8.00). Neuroticism had a mean of 5.98 (SD = 1.06), which is notable due to its documented link with postpartum depression. Conscientiousness scored 5.89 (SD = 1.06), Agreeableness scored 5.62 (SD = 0.89), and the smallest variability was observed in Agreeableness and Conscientiousness.
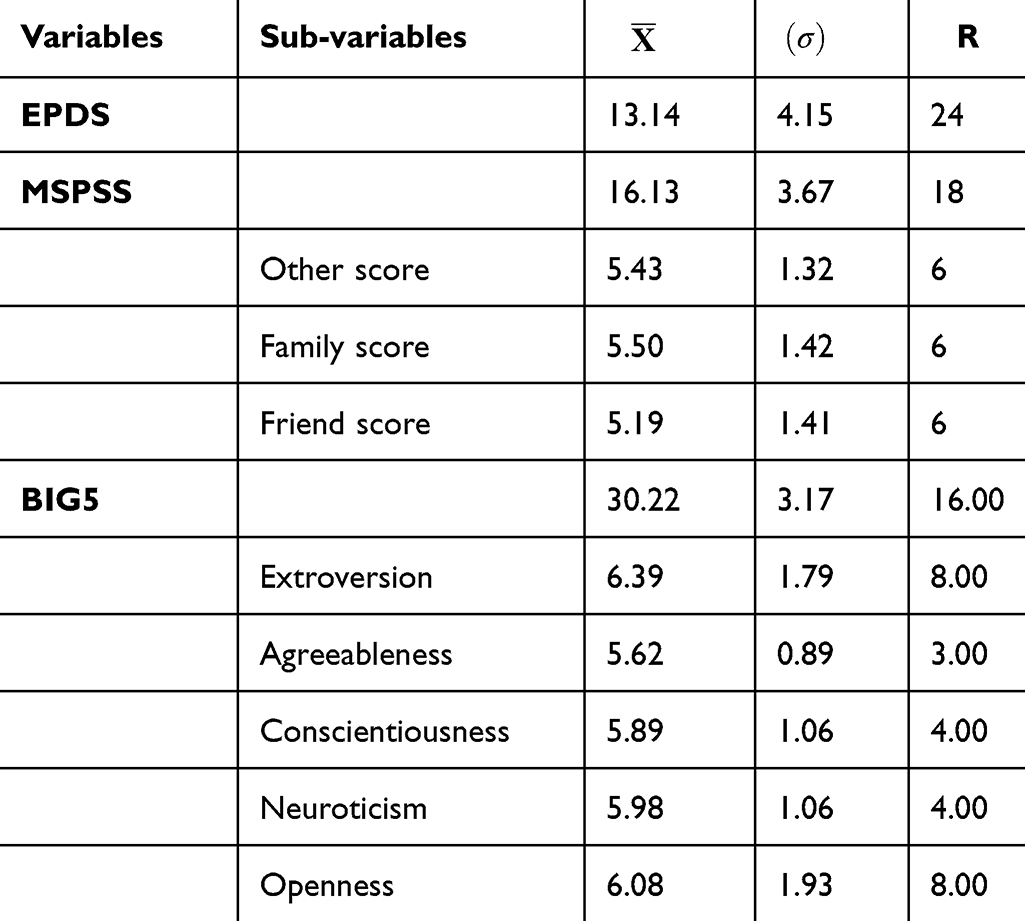 |
Table 2 Questionnaire Data Descriptive Statistics (N = 300) |
Correlation Analysis
Table 3 presents a refined correlation matrix illustrating significant relationships among postpartum depression (PPD), social support (SS), personality traits, and various contextual factors. A strong negative correlation was observed between perceived social support and PPD (r = –0.572, p < 0.01), emphasizing the protective role of social support in maternal mental health. Similarly, healthier relationships with partners (r = –0.244, p < 0.01) and in-laws (r = –0.247, p < 0.01) were associated with lower levels of depressive symptoms. Living in a joint family structure also showed a significant inverse association with PPD (r = –0.315, p < 0.01), suggesting that extended family systems may buffer emotional distress after childbirth. Additional contextual variables, such as locality (urban vs rural; r = –0.136, p < 0.05), and the quality of familial relationships, were meaningfully associated with maternal mental health. In contrast, PPD was positively correlated with certain personality traits (r = 0.292, p < 0.01), maternal age (r = 0.190, p < 0.01), and experiencing motherhood after marriage (r = 0.160, p < 0.01), indicating increased vulnerability in these contexts. Social support was significantly higher among urban residents (r = 0.239, p < 0.01), employed mothers (r = 0.249, p < 0.01), and individuals living in joint family arrangements (r = 0.257, p < 0.01). However, strained relationships within the family appeared to reduce perceived support. Further associations revealed that mode of delivery was significantly related to pregnancy complications (r = –0.204, p < 0.01), with vaginal births associated with fewer complications. Institutional childbirth showed a strong negative association with normal delivery (r = –0.550, p < 0.01), suggesting that medical settings are often linked with planned or medically guided deliveries. Lastly, marriage type (arranged vs love marriage) was modestly associated with place of childbirth (r = –0.178, p < 0.01), possibly reflecting sociocultural influences on birth practices.
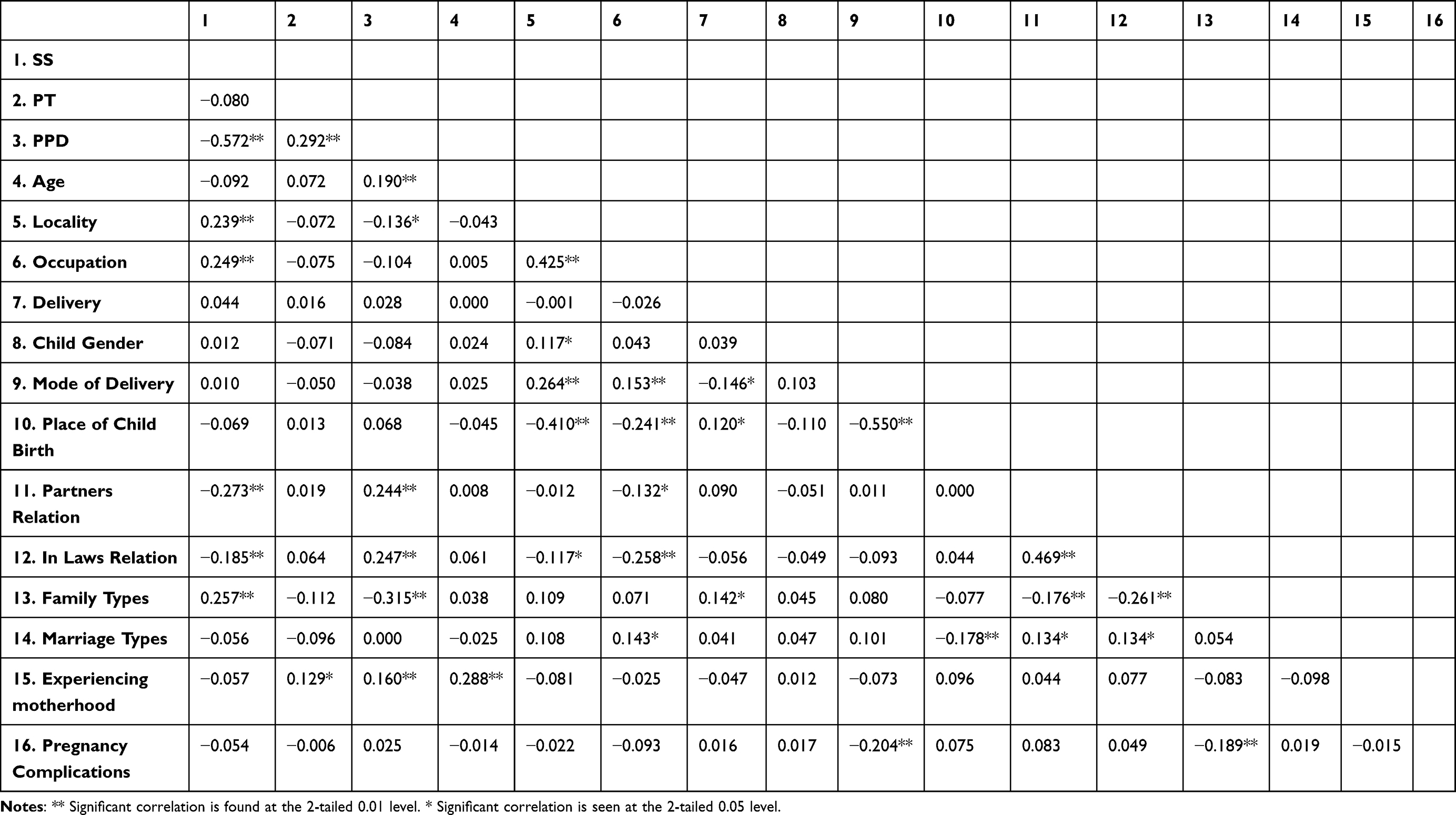 |
Table 3 Pearson Correlation for the Risk Factor, EPDS, MSPSS, and Big5 (N = 300) |
The Moderate Effect of Social Support
Table 4 shows the moderation analysis using PROCESS SPSS (version 4.2) was conducted with 300 participants to examine the relationship between Big Five personality traits, perceived social support, and postnatal depression. The overall regression model was significant (F = 5.954, p = 0.0006), explaining 5.7% of the variance in postnatal depression (EPDS) scores. Big Five personality traits significantly predicted EPDS scores (p = 0.0193), indicating that higher Big Five scores are associated with an increased risk of postpartum depression. However, perceived social support did not independently predict EPDS scores (p = 0.1052), suggesting that social support alone does not influence postnatal depression. The interaction between Big Five traits and social support was marginally significant (p = 0.0995), indicating a potential moderation effect. Table 5 shows the conditional effects analysis showed that the impact of Big Five traits on EPDS scores varied depending on social support levels. When social support was low, higher Big Five scores were significantly associated with higher EPDS scores (p = 0.0193). The relationship remained positive at average levels of social support but was marginally significant (p = 0.0500). At high levels of social support, the relationship became negative, though not significant (p = 0.2245), suggesting that higher perceived social support may reduce the influence of Big Five traits on postnatal depression.
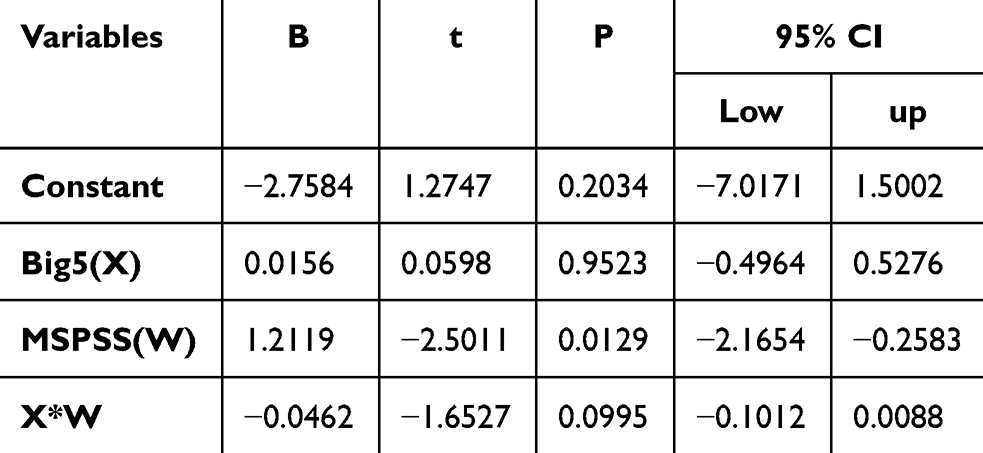 |
Table 4 Moderated Regression Analysis Summary Predicting EPDS |
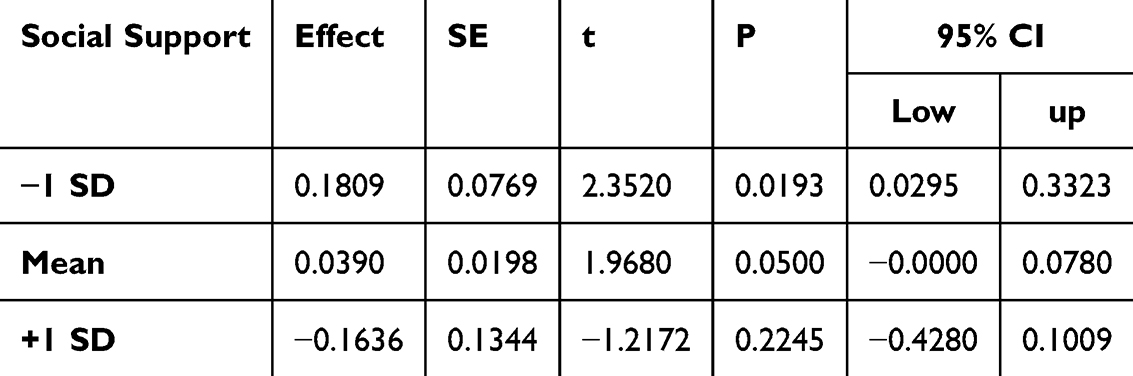 |
Table 5 Conditional Effects of Big Five Personality Trait (Big5) on EPDS at Different Levels of Social Support (MSPSS) |
Figure 1 shows this interaction plot illustrates the moderating role of perceived social support in the relationship between Big Five personality traits and depressive symptoms, as measured by the Edinburgh Postnatal Depression Scale (EPDS). The graph depicts three levels of social support (low = 12.47, average = 16.14, high = 19.81) and their corresponding associations between personality trait scores and depressive symptoms. As shown, individuals with low social support exhibit a steeper positive slope, indicating that higher personality vulnerability (eg, higher neuroticism) is associated with significantly increased postpartum depression symptoms. In contrast, the slope becomes flatter at average and high levels of social support, suggesting a buffering effect. At high support, the association between personality traits and depression becomes weak or even negligible. These visual trends are consistent with the results from the PROCESS moderation analysis (interaction term B = −0.1216, p = 0.0995), indicating a marginally significant interaction. Despite the modest statistical significance, the plot clearly supports the hypothesis that social support reduces the psychological risks associated with vulnerable personality traits in the postpartum period.
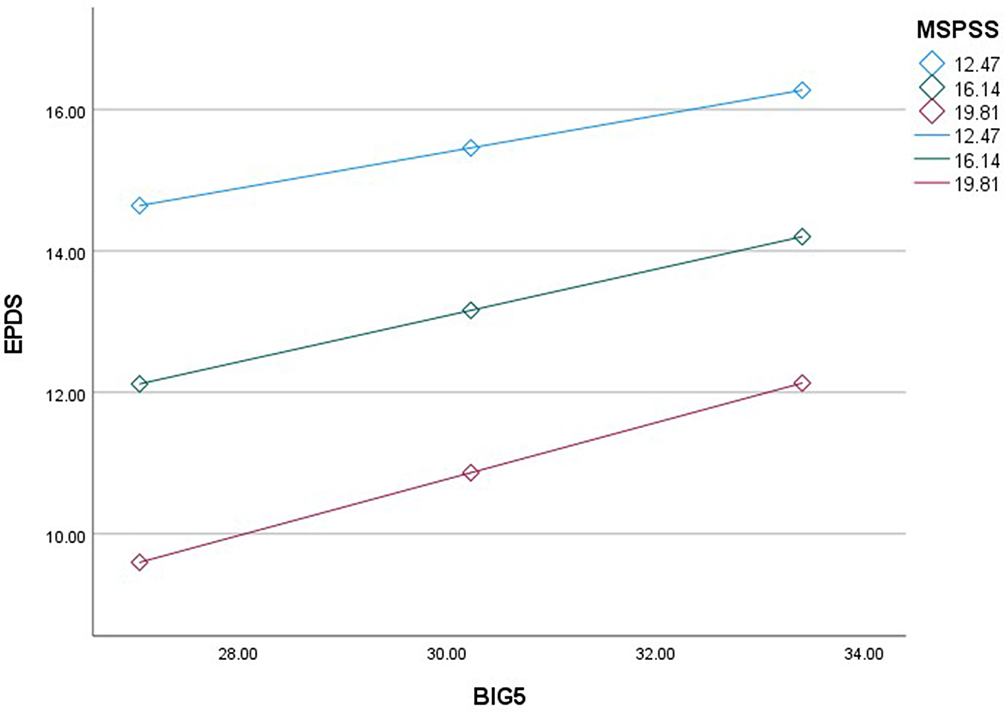 |
Figure 1 Association between Depression (EPDS), Social Support (MSPSS) and Big5 Personality traits. |
Table 6 shows this study examined the relationship between Big Five personality traits (B 5), social support (SS), and postpartum depression (PPD) using Structural Equation Modeling (SEM) with 5, 000 bootstrap samples. The total effect of personality traits on postpartum depression was 0.517 (95% CI [0.276, 0.758]), indicating a significant impact. Social support partially mediated this relationship, with an indirect effect of 0.106 (95% CI [0.040, 0.172]) and a direct effect of 0.411 (95% CI [0.206, 0.626]). Personality traits significantly predicted social support (0.350, 95% CI [0.242, 0.458]), which, in turn, had a strong negative effect on postpartum depression (−0.479, 95% CI [- 0.559, −0.400]).
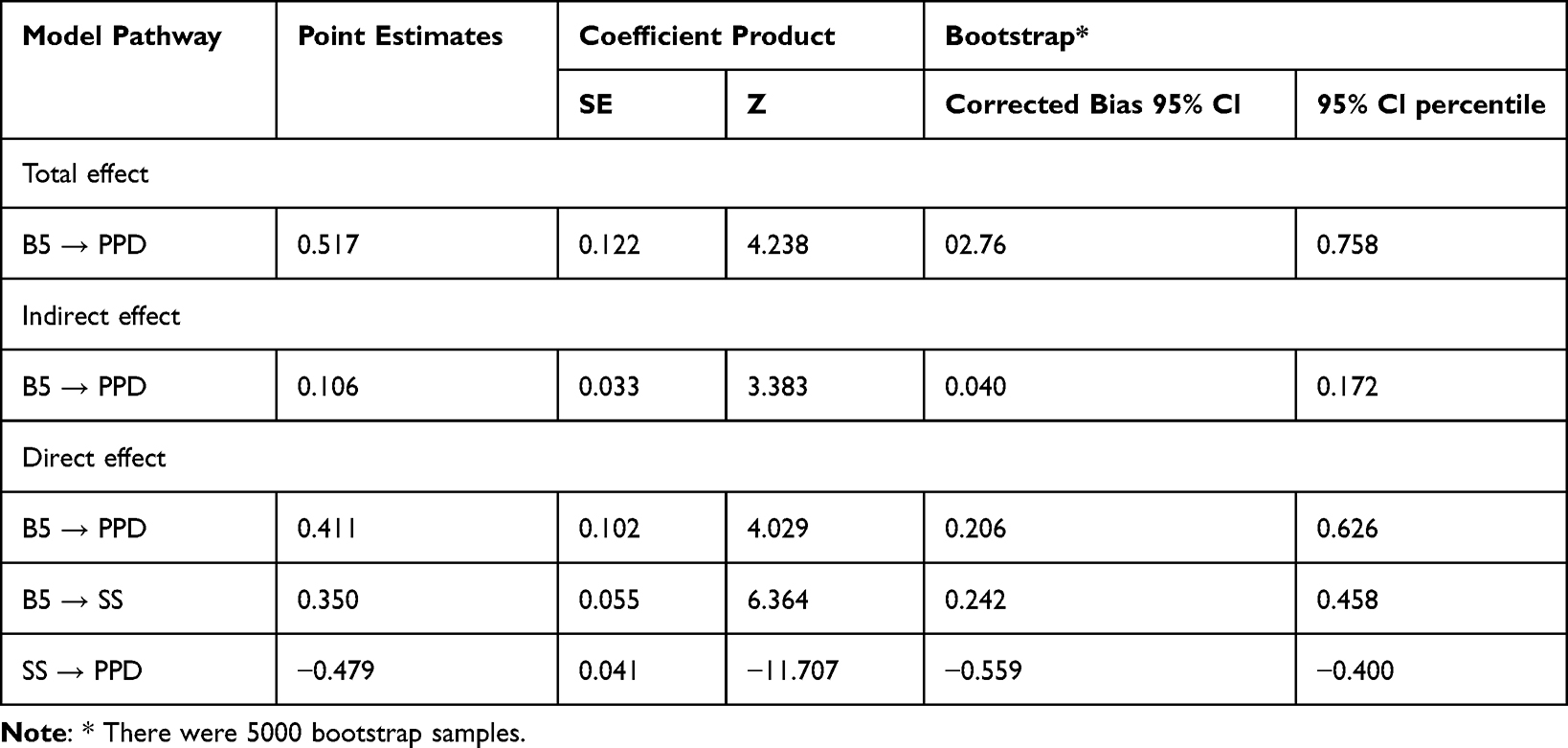 |
Table 6 Social Support, Personality Traits, and Postpartum Depression: The Standardized Total, Indirect, and Direct Effects of Mediation Model (N = 300) |
Figure 2 demonstrates that social support moderates the relationship between personality traits and postpartum depression. Higher social support weakens the negative effects of vulnerable personality traits, thereby reducing the likelihood of postpartum depression. Conversely, lower social support increases the risk, especially for individuals with high neuroticism. Social support was identified as a significant protective factor against postpartum depression (β = −0.479, p < 0.001). Neuroticism was the strongest predictor of postpartum depression, followed by extraversion and agreeableness. However, personality traits did not significantly predict social support (p = 0.178), indicating that other external factors may influence the availability and perception of social support.
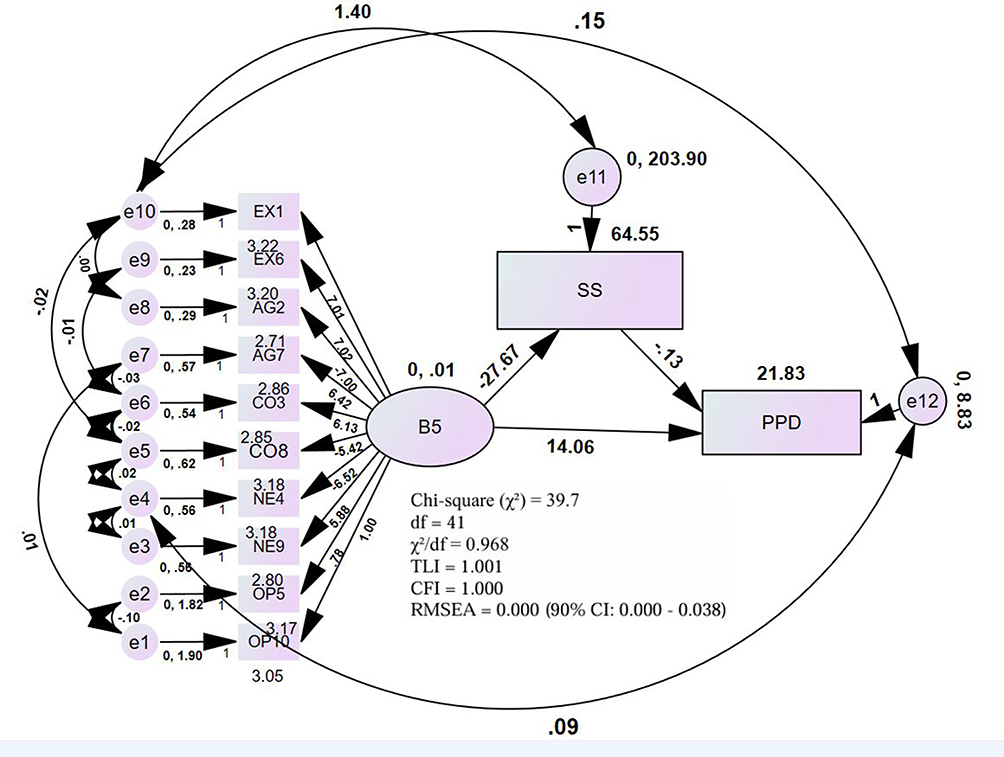 |
Figure 2 Social support’s moderating function in vulnerable personality traits and postpartum depression is modeled using structural equations. Abbreviations: B5, big five personality traits; PPD, postpartum depression; SS, social support. |
The structural equation model was assessed using model fit criteria. A good- fitting model is accepted when CMIN/df < 5, and when the Tucker- Lewis Index (TLI) and the Comparative Fit Index (CFI) exceed 0.90 (Hair et al, 2010; Bentler, 1990). The Root Mean Square Error of Approximation (RMSEA) should be between 0.05 and 0.08 (Hair et al, 2010). The model fit indices were as follows: CMIN/df = 0.968 (acceptable, <5), TLI = 1.001 (>0.90, excellent), CFI = 1.000 (>0.90, excellent), and RMSEA = 0.000 (90% CI: [0.000, 0.038], excellent). Given that CMIN/df < 5, TLI and CFI > 0.90, and RMSEA < 0.05, the model demonstrates an excellent overall fit.
Discussion
The findings from this study provide valuable insights into the intricate relationships between personality traits, social support, and postpartum depression (PPD) among new mothers. The study was guided by several vital hypotheses primarily supported by the results.
PPD affects the mother-child bond, making it difficult for the mother to bond emotionally, breastfeed, and respond to her child’s needs. According to Slomian et al,29 infants whose mothers suffer from postpartum depression (PDD) tend to be less active, cry more intensely, experience anxiety, or have abnormal sleep and wake habits. Furthermore, research shows that PPD exacerbates the mother’s suffering, degrades her well-being, and raises the possibility of marital discord.27 These findings were consistent with the outcomes of this study, where PPD was strongly linked to negative emotional and relational outcomes for both mothers and their infants.
The results of the research supported the theory that personality factors have a significant influence on postpartum depression (PPD). In particular, a strong correlation was found between PPD and the Big Five personality traits, which include extraversion, Conscientiousness, Neuroticism, Agreeableness, and Openness. The results indicated a positive connection (B = 0.1808, p = 0.0193) between the number of PPD symptoms and higher overall Big Five trait scores. This implies that certain people may be more susceptible to PPD than others due to particular personality traits. The Big Five qualities had a positive association with Edinburgh Postnatal Depression Scale (EPDS) scores (r = 0.196, p < 0.01), indicating the significant influence of personality features on postpartum mental health outcomes.
Prior research has emphasized the significance of various characteristics, specifically Neuroticism, as a potential risk factor for PPD. In 17 of the 18 studies that analyzed, for example, they discovered that Neuroticism was a significant predictor of PPD. The odds ratio (OR) varied greatly, ranging from 1.05 to 7.90, depending on the research population and methodology. The current study’s results are consistent with this corpus of literature, highlighting the direct and indirect risks of PPD that people with high neuroticism face due to their influence on social support.28
The study results are consistent with the theory that social support plays a significant role in PPD. In the regression study, social support did not show statistical significance as a predictor of PPD (p = 0.1052). However, it was clear that social support acted as a mediator between personality factors and PPD. With an indirect impact of B = 0.106 (p < 0.05), the study found that social support strongly mediates the association between the Big Five personality traits and PPD. This indicates that certain personality qualities may negatively affect postpartum mental health, but that social support can act as a buffer, mitigating such impacts.
Social support is protective against PPD in several studies. For instance, research by Chien et al30 and Brown et al8 revealed a correlation between lower PPD ratings and higher levels of social support. In a similar vein, Qi et al31 proposed that healthy interpersonal connections—especially with family members—are essential for lowering postpartum depression and enhancing the quality of sleep for new mothers. These results are in line with the current study, which emphasizes how crucial it is to improve social support as a component of postpartum treatment to lower the incidence of PPD.
However, it is important to interpret the moderation results with caution. While the conditional effects analysis suggested that the impact of personality traits on PPD varied by the level of social support, the interaction effect approached but did not reach conventional levels of statistical significance (p = 0.0995). Therefore, claims that social support serves as a strong protective buffer against PPD should be qualified and not overstated. These relationships are associative, not causal, and the cross-sectional design limits the ability to draw firm conclusions about directionality or mechanisms.
These findings from Structural Equation Modeling (SEM) emphasize the crucial role of social support in reducing postpartum depression, particularly among individuals with vulnerable personality traits. While personality traits significantly influence postpartum depression, social support serves as a key protective factor that mitigates its effects. The SEM model further clarifies these relationships, demonstrating that positive personality traits such as extraversion, openness, agreeableness, and conscientiousness are associated with higher social support, which in turn lowers postpartum depression. This suggests that individuals with these personality traits may be more likely to seek, perceive, or receive social support, ultimately reducing their risk of postpartum depression. Strengthening social support systems may therefore be an effective intervention strategy to improve postpartum mental health, especially for those with personality profiles that naturally enhance social connectedness. Conversely, Neuroticism lowers social support, which raises the risk of PPD both directly and indirectly. The findings align with previous studies showing that higher neuroticism scale scores were a strong predictor of postpartum depression in females32 and that Neuroticism and introversion were strong predictors of PPD during the first year after childbirth.30
Postpartum depression (PPD) is highly impacted by the Big Five personality traits (B5). The overall substantial (0.517) effect of B5 on PPD is partially mediated by social support (SS). While B5’s direct impact on PPD, without SS, is still significant (0.411), its indirect effect on PPD through SS is significant (0.106). B5 has a favorable impact on SS (0.350), and SS has a noteworthy adverse influence on PPD (−0.479). This shows that social support, especially for qualities like Neuroticism that negatively impair SS, has a vital role in lowering PPD, even though B5 directly influences PPD.
This study established the considerable influence of demographic factors on personality traits, social support, and postpartum depression (PPD). In line with earlier studies showing the impact of socioeconomic position and prior delivery experience on postpartum mental health, older age, poorer income, and being a first-time mother were linked to higher PPD scores.33 Moreover, mothers who had cesarean sections also reported having more depressive symptoms, which supports studies demonstrating that postpartum depression (PPD) can be more likely in patients who have greater recovery demands after surgery.34
Level of education and marital status also had an impact; PPD and social support were higher among single mothers and those with lower educational attainment.35 These findings highlight the necessity for postpartum care providers to take demographic factors into account to manage and reduce the risk of PPD effectively.
Limitations and Future Research
This study has several limitations. Its cross-sectional design prevents causal conclusions, so the reported associations between personality, social support, and postpartum depression (PPD) should be interpreted cautiously. The scales were used in English that could pose an issue for reliability among non-English-speaking participants. However, for participants who were not fully proficient in English, the items were translated orally into the local language by trained field researchers. Care was taken to ensure that the translated content retained the original meaning and intent of the items. Participants were only included if they demonstrated sufficient understanding of the translated version. This approach helped maintain the reliability and validity of the responses across the sample. The sampling method (convenience sampling) introduces selection bias and reduces generalizability. The sample size, while adequate for analysis, may limit generalizability. The study timeframe is relatively short for examining postpartum depression, which can fluctuate over time. A longitudinal design is preferable, as postpartum depression symptoms can evolve beyond the one-to-two-year postpartum period analyzed in our study. Future research should use larger, more diverse samples and longitudinal designs to clarify causal pathways. Additionally, unmeasured factors such as prior mental health, marital quality, and socioeconomic or cultural influences may have affected the findings and should be considered in future studies. While the SEM model fit indices (TLI, CFI, RMSEA) indicate an acceptable level of model fit, it is important to acknowledge that potential overfitting related to the sample size has not been explicitly addressed. Additionally, the study does not examine issues such as collinearity among variables or explore alternative model specifications, which could have further strengthened the robustness and validity of the findings. Future research should consider these aspects to ensure more comprehensive model evaluation.
Conclusion
This research suggests that certain personality traits—especially high neuroticism and low extraversion—are linked to a heightened risk of postpartum depression (PPD) in new mothers. While the presence of social support seemed to influence the connection between personality and PPD, this effect was only marginally significant and lessened with increased support levels. As a result, any conclusions regarding its potential protective role should be approached with care. Moreover, demographic elements such as age, income, and education also impacted postpartum mental health outcomes, with older and lower-income mothers showing a greater risk of PPD. These results enhance the understanding of how psychosocial and demographic factors interrelate to affect mothers mental health after childbirth. However, the study’s cross-sectional nature prevents causal inferences. To confirm these associations and better understand the temporal dynamics involved, further longitudinal research is necessary. Practical implications suggest that personality assessments and customized support strategies could be beneficial in postpartum care, though additional work is essential to develop and assess these interventions. Increasing transparency about limitations, like sampling methods and potential social desirability bias, would improve the study’s generalizability and relevance in practical contexts in future.
Clinical Implication
Despite the insightful information obtained, this study has several limitations. Although sufficient for the analyses, the sample size can restrict how broadly the results can be applied. Furthermore, causal relationships cannot be established because of the study’s cross-sectional nature. Longitudinal studies and larger sample size studies that monitor changes in personality, social support, and PPD over time would benefit future research. Furthermore, investigating additional potential modifiers like socioeconomic position or cultural characteristics might offer a more thorough comprehension of the dynamics at work.
Acknowledgment
The authors extend their appreciation to the Deanship of Scientific Research at King Khalid University for supporting this work through Large group Project RGP-2/504/45.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Deanship of Scientific Research at King Khalid University through the Large Group Project (Grant No. RGP-2/504/45).
Disclosure
All authors have no competing interests.
References
1. Serati M, Redaelli M, Buoli M, Altamura AC. Perinatal major depression biomarkers: a systematic review. J Affect Disord. 2016;193:391–404. doi:10.1016/j.jad.2016.01.027
2. Radoš SN, Akik BK, Žutić M, et al. Diagnosis of peripartum depression disorder: a state-of-the-art approach from the COST action riseup-PPD. Compr Psychiatry. 2024;130(Cc):152456. doi:10.1016/j.comppsych.2024.152456
3. Elmuttalut M, Alfahal MS. View of key risk factors contributing to postpartum depression_ Literature Review.pdf.
4. Dennis CLE, Janssen PA, Singer J. Identifying women at-risk for postpartum depression in the immediate postpartum period. Acta Psychiatr Scand. 2004;110(5):338–346. doi:10.1111/j.1600-0447.2004.00337.x
5. Felger JC, Lotrich FE. Inflammatory cytokines in depression: neurobiological mechanisms and therapeutic implications. Neuroscience. 2013;246:199–229. doi:10.1016/j.neuroscience.2013.04.060
6. Saharoy R, Potdukhe A, Wanjari M, Taksande AB. Postpartum depression and maternal care: exploring the complex effects on mothers and infants. Cureus. 2023;15(7). doi:10.7759/cureus.41381
7. Wills TA, Ainette MC. Social networks and social support. In: Handbook of Health Psychology,
8. Brown JD, Harris SK, Woods ER, Buman MP, Cox JE. Longitudinal study of depressive symptoms and social support in adolescent mothers. Matern Child Health J. 2012;16(4):894–901. doi:10.1007/s10995-011-0814-9
9. Bayrampour H, McDonald S, Tough S. Risk factors of transient and persistent anxiety during pregnancy. Midwifery. 2015;31(6):582–589. doi:10.1016/j.midw.2015.02.009
10. Nylen KJ, Williamson JA, O’Hara MW, Watson D, Engeldinger J. Validity of somatic symptoms as indicators of depression in pregnancy. Arch Womens Ment Health. 2013;16(3):203–210. doi:10.1007/s00737-013-0334-2
11. Valentine JM, Rodriguez MA, Lapeyrouse LM, Zhang M. Recent intimate partner violence as a prenatal predictor of maternal depression in the first year postpartum among Latinas. Arch Womens Ment Health. 2011;14(2):135–143. doi:10.1007/s00737-010-0191-1
12. Choudhury N, Moran AC, Alam MA, Ahsan KZ, Rashid SF, Streatfield PK. Beliefs and practices during pregnancy and childbirth in urban slums of Dhaka, Bangladesh. BMC Public Health. 2012;12(1):1. doi:10.1186/1471-2458-12-791
13. Costa PT, McCrae RR. The five-factor model of personality and its relevance to personality disorders. J Pers Disord. 1992;6(4):343–359. doi:10.1521/pedi.1992.6.4.343
14. Podolska MZ, Bidzan M, Majkowicz M, Podolski J, Sipak-Szmigiel O, Ronin-Walknowska E. Personality traits assessed by the NEO five-factor inventory (NEO-FFI) as part of the perinatal depression screening program. Case Reports Clin Pract Rev. 2010;16(9):77–81.
15. Verkerk GJM, Denollet J, Van Heck GL, Van Son MJM, Pop VJM. Personality factors as determinants of depression in postpartum women: a prospective 1-year follow-up study. Psychosom Med. 2005;67(4):632–637. doi:10.1097/01.psy.0000170832.14718.98
16. Hengartner MP. Developmental course of child personality traits and their associations with externalizing psychopathology: results from a longitudinal multi-informant study in a representative cohort. J Res Pers. 2018;73:164–172. doi:10.1016/j.jrp.2017.12.001
17. Ormel J, Jeronimus BF, Kotov R, et al. Neuroticism and common mental disorders: meaning and utility of a complex relationship. Clin Psychol Rev. 2013;33(5):686–697. doi:10.1016/j.cpr.2013.04.003
18. White LK, Kornfield SL, Himes MM, et al. The impact of postpartum social support on postpartum mental health outcomes during the COVID-19 pandemic. Arch Womens Ment Health. 2023;26(4):531–541. doi:10.1007/s00737-023-01330-3
19. Cohen S, Stress WTA. Social support, and the buffering hypothesis. Psychol Bull. 1985;98(2):310–357. doi:10.1037/0033-2909.98.2.310
20. Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression: development of the 10-item Edinburgh postnatal depression scale. Br J Psychiatry. 1987;150(JUNE):782–786. doi:10.1192/bjp.150.6.782
21. Bunevicius R, Kusminskas L, Bunevicius A, Nadisauskiene RJ, Jureniene K, Pop VJM. Psychosocial risk factors for depression during pregnancy. Acta Obstet Gynecol Scand. 2009;88(5):599–605. doi:10.1080/00016340902846049
22. Zimet GD, Dahlem NW, Zimet SG, Farley GK. The multidimensional scale of perceived social support. J Pers Assess. 1988;52(1):30–41. doi:10.1207/s15327752jpa5201_2
23. Kaur K, Beri N. Psychometric properties of multidimensional scale of perceived social support (MSPSS): Indian adaptation. Int J Sci Technol Res. 2019;8(11):2796–2801.
24. Rammstedt B, John OP. Measuring personality in one minute or less: a 10-item short version of the Big Five Inventory in English and German. J Res Pers. 2007;41(1):203–212. doi:10.1016/j.jrp.2006.02.001
25. Zimet G. Multidimensional Scale of Perceived Social Support (MSPSS) - scale items and scoring information; 2016.
26. Slomian J, Honvo G, Emonts P, Reginster JY, Bruyère O. Consequences of maternal postpartum depression: a systematic review of maternal and infant outcomes. Women’s Health. 2019;15. doi:10.1177/1745506519844044
27. Stewart DE, Vigod SN. Postpartum depression: pathophysiology, treatment, and emerging therapeutics. Annu Rev Med. 2019;70:183–196. doi:10.1146/annurev-med-041217-011106
28. Tian T, Li Y, Xie D, et al. Clinical features and risk factors for post-partum depression in a large cohort of Chinese women with recurrent major depressive disorder. J Affect Disord. 2012;136(3):983–987. doi:10.1016/j.jad.2011.06.047
29. Chien LY, Tai CJ, Yeh MC. Domestic decision-making power, social support, and postpartum depression symptoms among immigrant and native women in Taiwan. Nurs Res. 2012;61(2):103–110. doi:10.1097/NNR.0b013e31824482b6
30. Udovičić S. Big Five Personality traits and social support as predictors of postpartum depression. J Eur Psychol Students. 2014;5(3):66–73. doi:10.5334/jeps.ck
31. Qi W, Liu Y, Lv H, et al. Effects of family relationship and social support on the mental health of Chinese postpartum women. BMC Pregnancy Childbirth. 2022;22(1):1–10. doi:10.1186/s12884-022-04392-w
32. Lee DTS, Yip ASK, Chiu HFK, Leung TYS, Chung TKH. A psychiatric epidemiological study of postpartum Chinese women. Am J Psychiatry. 2001;158(2):220–226. doi:10.1176/appi.ajp.158.2.220
33. Goyal D, Gay C, Lee KA. How much does low socioeconomic status increase the risk of prenatal and postpartum depressive symptoms in first-time mothers? Women’s Heal Issues. 2010;20(2):96–104. doi:10.1016/j.whi.2009.11.003
34. Sword W, Kurtz Landy C, Thabane L, et al. Is mode of delivery associated with postpartum depression at 6 weeks: a prospective cohort study. BJOG an Int J Obstet Gynaecol. 2011;118(8):966–977. doi:10.1111/j.1471-0528.2011.02950.x
35. Dennis CL, Letourneau N. Global and relationship-specific perceptions of support and the development of postpartum depressive symptomatology. Soc Psychiatry Psychiatr Epidemiol. 2007;42(5):389–395. doi:10.1007/s00127-007-0172-5
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.