Back to Journals » Nature and Science of Sleep » Volume 14
Persistent Treatment-Emergent Central Sleep Apnea (TECSA) Following Hypoglossal Nerve Stimulation
Authors Wang Y ![]() , Penzel T
, Penzel T ![]() , Salanitro M
, Salanitro M ![]() , Arens P
, Arens P ![]()
Received 2 August 2022
Accepted for publication 11 December 2022
Published 22 December 2022 Volume 2022:14 Pages 2227—2236
DOI https://doi.org/10.2147/NSS.S382710
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Yan Wang,1 Thomas Penzel,1 Matthew Salanitro,1 Philipp Arens2
1Interdisciplinary Sleep Medicine Center Charité – Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin and Humboldt-Universitätzu Berlin, Berlin, Germany; 2Department of Otorhinolaryngology, Campus Virchow Klinikum Charité – Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Berlin, Germany
Correspondence: Philipp Arens, Department of Otorhinolaryngology, Campus Virchow Klinikum Charité – Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Berlin, Germany, Email [email protected]
Purpose: Since 2001, hypoglossal nerve stimulators (HNS) have been used worldwide to treat patients with obstructive sleep apnea (OSA). Recently, a few studies reported treatment-emergent central sleep apnea (TECSA) with spontaneous resolution following HNS. However, the evidence of persistent development of TECSA during long-term care visits was lacking. As a result, this study first report two patients with persistent TECSA and describe their development phenotype during more than two years of follow-up visits to help explore the influencing factors and underlying mechanisms.
Patients and Methods: This retrospective study included twenty-seven patients who underwent HNS implantation from 2016 to 2021. Their demographic data, pre- and postoperative sleep study characteristics, and device use settings were collected. The possible factors associated with post-operative elevated CSA (central apnea index ≥ 5) were evaluated. Moreover, the development phenotype of the TECSA was observed and followed up with a titration trial study.
Results: Among overall 27 patients with OSA, 3 patients with an increased preoperative Epworth Sleepiness Score (ESS) got an elevated CSA (CAI ≥ 5). Two of these 3 patients developed a persistent TECSA with a significant negative correlation between obstructive apnea index (OAI) and central and mixed sleep apnea index (CMAI) (R = − 0.745, P = 0.021). These development phenotypes might be associated with different stimulation amplitudes of the HNS device. Furthermore, the following titration trial study also suggested that different amplitudes would influence the development of TECSA following HNS.
Conclusion: OSA patients with severe daytime sleepiness are more likely to have elevated CSA following HNS. An inappropriate stimulation amplitude might influence the development course of TECSA in such patients.
Keywords: hypoglossal nerve stimulation, obstructive sleep apnea, treatment-emergent central sleep apnea, stimulation amplitude, daytime sleepiness
Introduction
Hypoglossal nerve stimulator (HNS) has been demonstrated to be a safe and effective treatment for patients with OSA in several large multicenter prospective clinical trials, improving both objective respiratory and subjective quality-of-life measures without uncommon adverse events.1 Nevertheless, a few case reports and one retrospective study reported elevated central sleep apnea (CSA), which has been indicated as an independent predictor of heart failure and could lead to significant comorbidity and an increased risk of adverse cardiovascular outcomes.2–5
In 2020, the International Classification of Sleep Disorders-third edition introduced the term “TECSA” (Treatment-Emergent Central Sleep Apnea) and defined it as the presence of primary OSA at the initial diagnostic sleep study, significant resolution of obstructive events with CPAP titration followed by emergence or persistence of central events during PAP treatment with a central apnea index (CAI) ≥5/h, >50% of events being central, and symptoms that cannot be explained in a better manner by another CSA disorder.6
However, the evidence of TECSA following HNS is limited, especially for the long-term observations. Therefore, this study aims to first report persistent TECSA following HNS in two patients with OSA, describe their development phenotype during long-term visit and discuss the possible influencing factors.
Materials and Methods
This study was a retrospective cohort study. Between 2016 and 2021, all 27 patients who underwent implantation of an HNS system (Inspire Medical Systems Inc. USA) at the otolaryngology department at Charité Universität, Berlin were enrolled. Each patient underwent either an in-lab PSG or HSAT before the implantation and during the follow-up. These recordings were manually scored in accordance with the American Academy of Sleep Medicine (AASM) manual recommendations. HNS device recordings were collected retrospectively from the patient’s medical records. Their clinical data, including demographic data, sleep characteristics, and device configurations, were collected and stored in Charité’s internal database. This study was approved by the ethics committee of the university (Charité—Universitätsmedizin Berlin approval Number EA2/068/22) and adhered to the tenets of the Declaration of Helsinki.
The criteria for implantation and inclusion in the study were participants aged >18 years, who had an apnea and hypopnea index (AHI) between 15 and 65 with <25% central events, and those who failed to accept or adhere to continuous positive airway pressure (CPAP) therapy. Patients with body mass index >35 kg/m2 were excluded.
HNS
HNS maintains the upper airway opening by stimulating the protrusion branches of the hypoglossal nerve during the collapse-prone portion of the respiratory cycle.7 In this research, the standard procedure to implant an HNS stimulator was performed by the same physician.8 Four to eight weeks after implantation, the HNS device is normally activated with standard settings (bipolar electrode configuration, pulse width 90 µs, frequency 33 Hz) and the amplitude of stimulation is titrated individually. During follow-up, device configuration, including stimulation amplitude, frequency, pulse width, and electrode configuration, is adjusted to optimal values during office titrations and sleep lab titrations.
Statistical Analysis
The SPSS software (IBM SPSS Statistics, version 26.0. Armonk, NY, IBM Corp.) was used for statistical analysis. The overall demographic data is presented as mean ± standard deviation (range). To evaluate the possible factors associated with elevated CSA (CAI ≥ 5), Fisher’s exact test and χ2 test were used to compare categorical variables. Mann–Whitney tests were used to compare continuous variable data. Spearman rank correlation was used to analyze the correlation between OAI and central and mixed sleep apnea index (CMAI) in patients with TECSA. Differences were considered statistically significant at P < 0.05.
Results
Patient Characteristics
This study included 27 patients with OSA who underwent HNS implantation from 2016 to 2021. There were 22 male patients (81.5%), 4 female patients and 1 transsexual (trans male) patient; all patients are Caucasians. The mean age at the time of HNS activation was 57 ± 7.5 years, with a mean pre-operative ESS score of 12.2 ± 6.0 and a mean BMI of 29.7 ± 3.2 (range, 20–34.5). The mean CCI was 1 ± 1 (range, 0–4), and hypertension was the most common comorbidity among all patients (44.4%). At baseline,14 patients had polysomnography, and 13 received home sleep apnea testing (HSAT).
TECSA
As shown in Figure 1, 3 patients developed newly elevated CSA (CAI ≥ 5) after HNS activation. Univariate analysis was performed to compare differences between preoperative findings and the postoperative CAI ≥ 5 and CAI < 5 groups. The difference in preoperative ESS score and mixed apnea index between two groups was significant (P < 0.01). However, there was no significant difference (P > 0.05) between age, BMI, AHI or other sleep architectures (Table 1). Also, the differences in average use time/week and the initial stimulation configuration were not significant (p > 0.05).
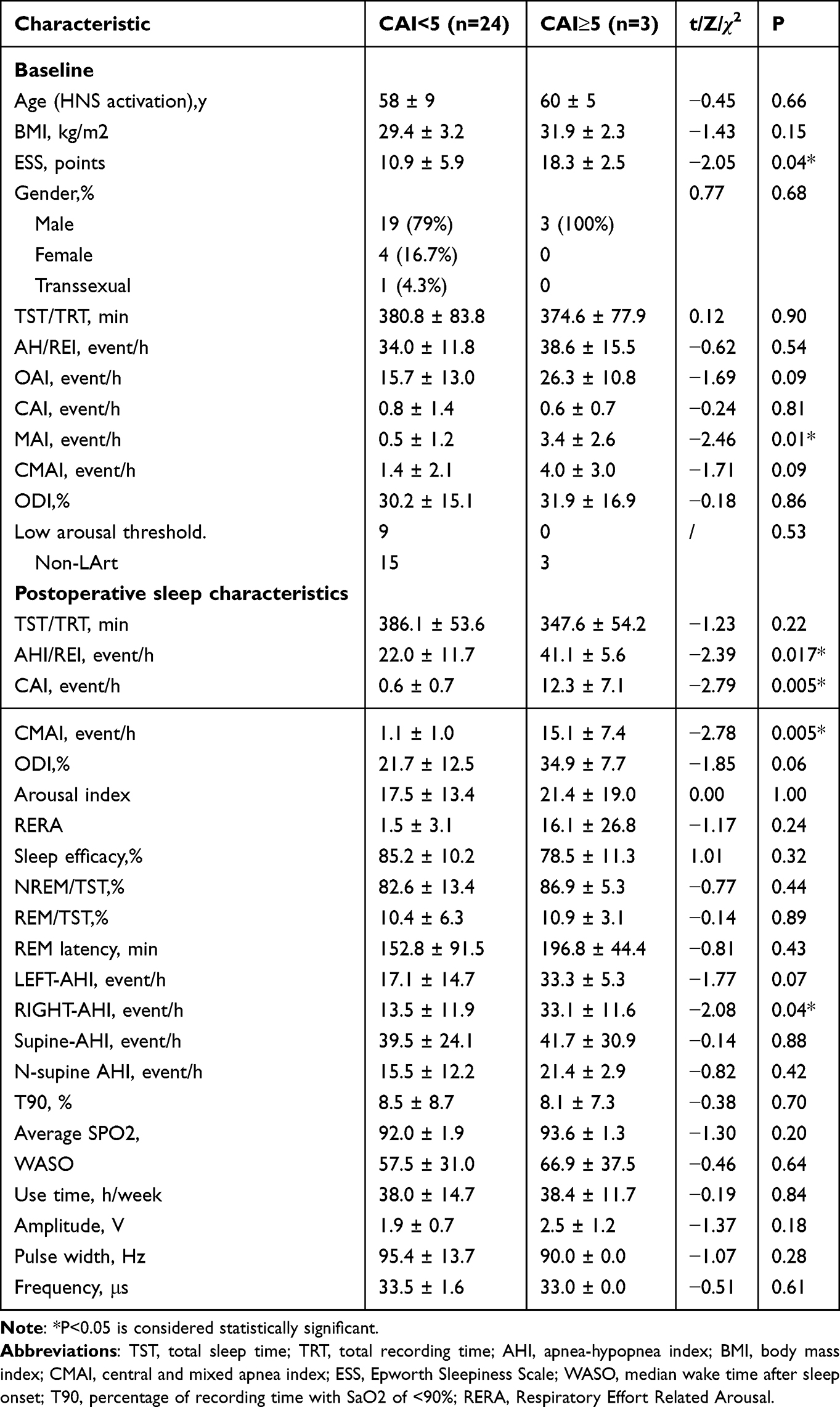 |
Table 1 Preoperative and Postoperative Data Including Patient Demographics, Sleep Study Data Base of CAI ≥5 (CAI <5 and CAI ≥5) |
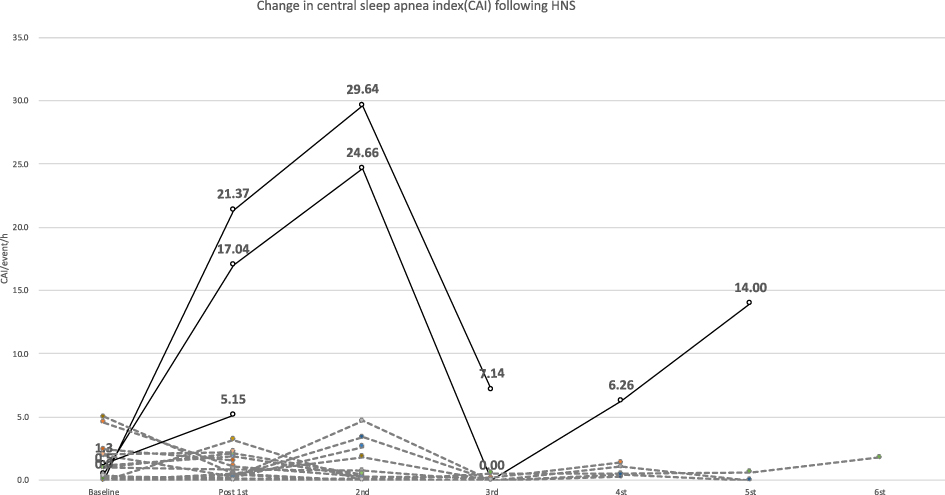 |
Figure 1 Change in central apnea index (CAI) following HNS. Note: Patients who had an increased CSA of CAI ≥5 following HNS (n = 3) are indicated by a dashed line, and patients with a CAI <5 following HNS (n = 24) are indicated by a solid line. |
As one of 3 patients lacked long-term follow-up, 2 patients (7.4%) were diagnosed with persistent TECSA during visits over a 2-year time span, whose baseline CAI < 5 events/h demonstrated a CMAI of ≥5 events/h becoming prominent. As shown in Table 2, both patients were men with mild obesity and had severe daytime sleepiness. Patient 1 had a medical history of hypertension, while patient 2 had coronary heart disease. Following HNS, OAI of patient 1 decreased from 37.1 event/h to 11.5 event/h, with CAI increasing from 0.5 to 12.4 event/h. Patient 2 had a baseline AHI of 15.6 event/h which improved to 6.5, while CAI increased from 0 to 19.4 event/h. Both patients reported noticeable improvement in sleep quality and resolution of OSA symptoms; their bed partners also reported a marked change in snoring and breathing.
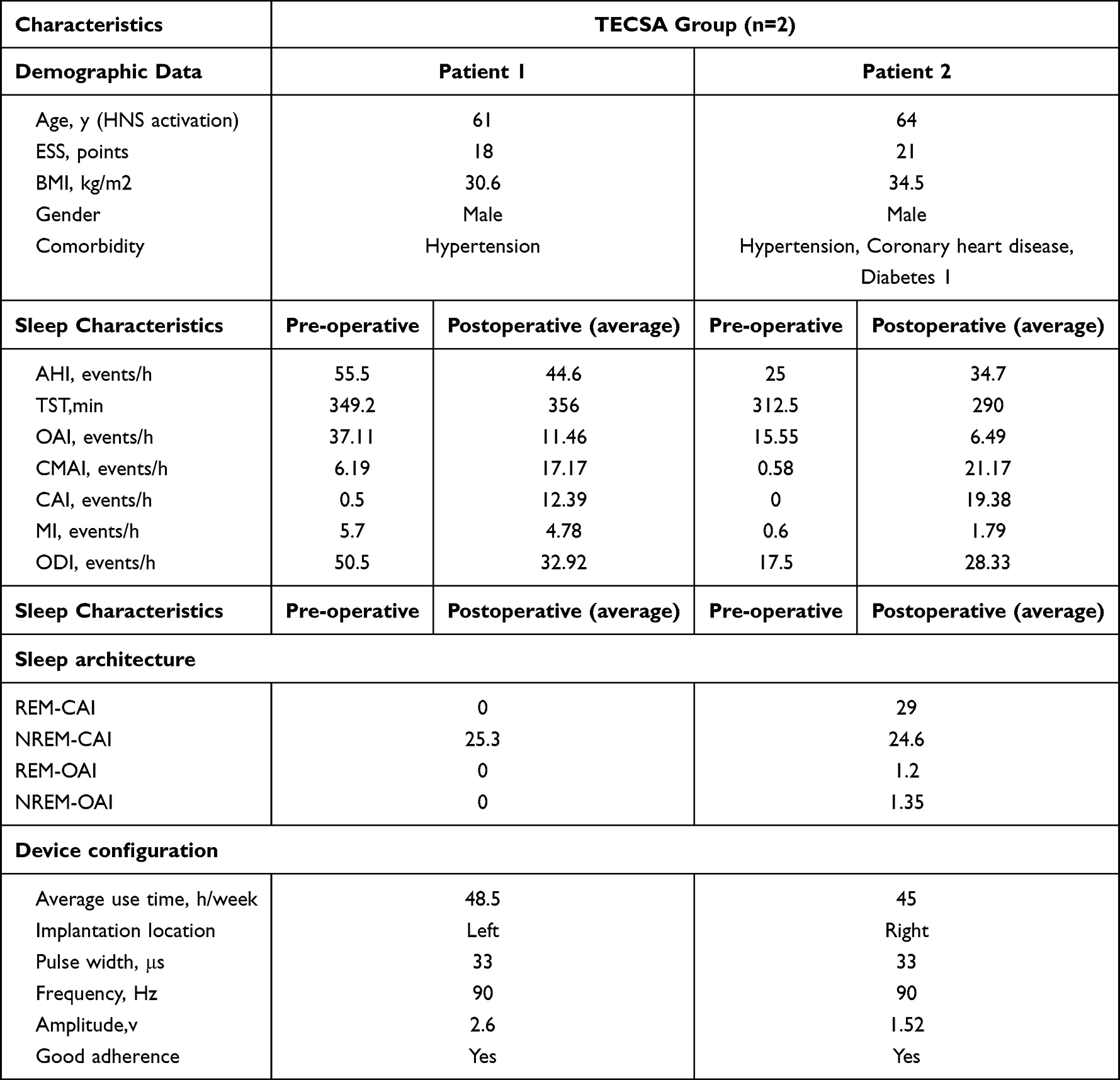 |
Table 2 Demographic, Sleep Study and Stimulation Configuration of 2 Patients with TECSA |
Moreover, their development phenotype of TECSA included a persistent course during follow-up visits, and there is a strong negative correlation between OA and CA and sleep phase-related characteristics. The data in Figures 2 and 3 demonstrate that OSA was resolved with different stimulation amplitudes while central and mixed sleep apnea increased. While the CMAI decreased, the OAI increased significantly. Spearman correlation was performed and found that the correlation coefficient between OAI and CMAI was −0.75, which indicates a significant, strong negative correlation between CA and OA in the two patients with TECSA (Table 3). Moreover, the PSG investigation found that in the two patients with TECSA, OSA occurred primarily during the night’s first half and CSA in the second half of the night. The respiratory events were also related to changes in the sleep phase, and OSA events frequently occurred during REM sleep, whereas CSA occurred during NREM sleep. However, this study did not observe the position dependence of TECSA and other patterns.
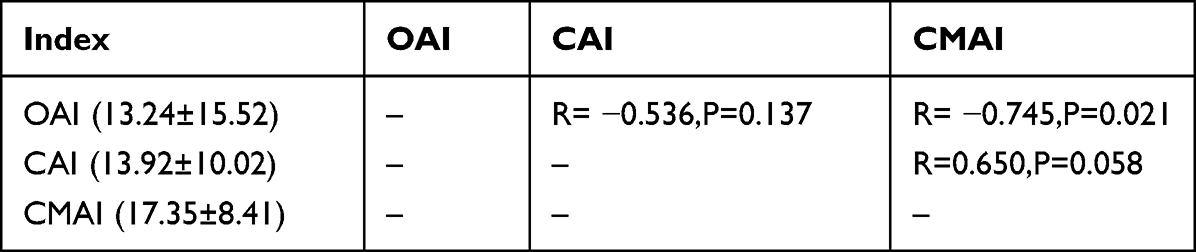 |
Table 3 Spearman Correlation Between CAI, CMAI and OAI |
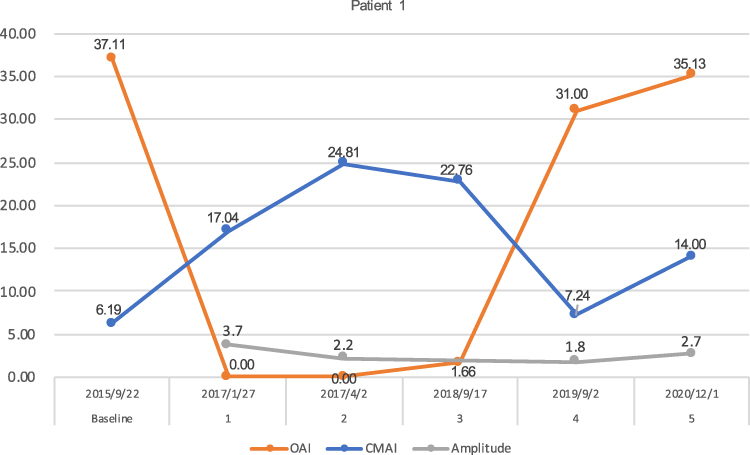 |
Figure 2 Changes of CMAI, OAI, use time during Patient 1 follow-up visits. |
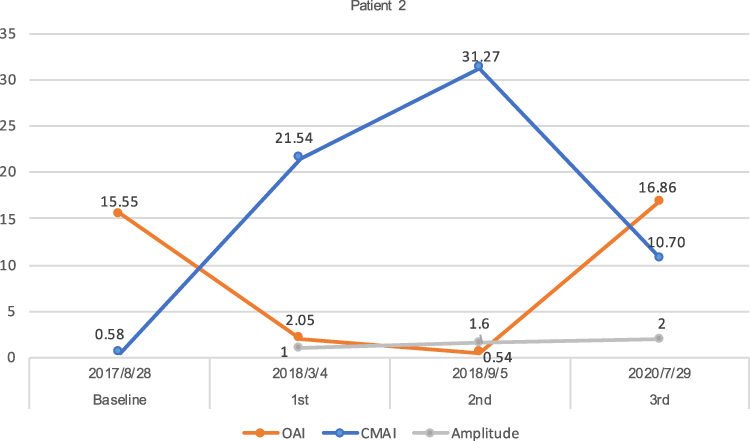 |
Figure 3 Changes of CMAI, OI, stimulation amplitude during Patient 1 follow-up visits. |
Titration Trial Study
Based on the development phenotype of TECSA during visit, this study found that it might be associated with different stimulation amplitudes of the HNS stimulator. OSA occurred at a higher stimulation amplitude, while CSA developed at a lower one. When the stimulation amplitude was adjusted to approximately 1.66 V −2V, both CSA and OSA achieved a satisfactory level. Therefore, a titration trial was performed to test this hypothesis. Three conditions were stimulated by adjusting the device amplitude at different levels (off, low, standard, and high amplitudes) (ineffective treatment, appropriate treatment, and overstimulation). The changes in sleep respiratory events under 3 different conditions were observed.
As shown in Figure 4, patient 1 with TECSA was observed to have all-night evident and severe CSA even with the HNS device off (AHI of 59.6, CAI of 55.5 and OAI of 1 event/h). Patient 2 had no CSA with the device off. After 2 hours of steady sleep, the night PSG technologists changed the stimulation amplitude from 1.8 V-1.4 V −2.0 V every 2 hours to evaluate the changes in central and obstructive apnea events. The results of the titration study showed that respiratory events, including OSA, CSA, arousal, and sleep efficacy, were all influenced by the stimulation amplitude. The finding of the titration trial is summarized in Figure 5, which supports our hypothesis that an appropriate stimulation amplitude could influence the development of TECSA.
 |
Figure 4 The titration sleep study report of patient 1 in the TECSA group. |
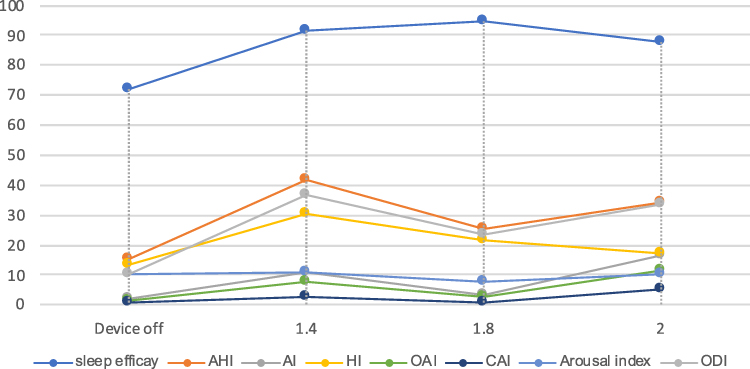 |
Figure 5 The changes in sleep study characteristics at different stimulation amplitudes of patient 1 in the TECSA group. |
Discussion
Based on the developmental phenotype of persistent TECSA and titration trial studies, we hypothesize that patients with severe daytime sleepiness might be more likely to develop an elevated CSA following HNS. An insufficient or excessive stimulation amplitude might influence the development of TECSA for such patients. As a result, precise patient selection and scheduled clinical monitoring to determine the appropriate stimulation amplitude are necessary to prevent or resolve TECSA.9
In 2018, Chan et al first observed that one patient had a significantly increased CSA during titration. Both OSA and CSA were resolved after the patient’s device configuration was changed to unipolar stimulation and amplitude was calibrated from 0.6 to 1.6 V. In 2019, Sarber et al3 reported a patient with mixed sleep apnea (CAI of 12.5 event/h) who presented with a TECSA (CAI of 78.9 event/h) and obstructive apnea and hypopnea index of 4.9 event/h with Cheyne-Stokes breathing (CSB) after implantation of HNS. During follow-up, the CSA and CSB continued throughout the study without HNS activation. In 2020, Patel et al conducted a prospective cohort study with 5 of 141 patients who underwent TECSA. Three patients presented with spontaneous resolution after continued use of HNS, and another 2 patients had a resolution of CSA-related symptoms after configuration adjustment or discontinued HNS due to severe and persistent CSA.2 They hypothesized that after UAS device activation, the resolution of sleep-related obstruction and restoration of normal lower nocturnal values of partial pressure of carbon dioxide (PCO2) with decreased receptor chemosensitivity might result in TECSA. After continuous treatment and progressive adaptation of chemoreceptors to new levels of nocturnal PCO2, CSA decreased gradually.5
Unlike the spontaneous resolution of TECSA observed in the above studies, this study found a persistent development and a strong negative correlation between central apnea and obstructive apnea. With the patient’s device configuration being changed to optimize the effect continually, central apneas occurred and persisted with the resolution of OSA at an excessive stimulation amplitude. And vice versa, obstructive apnea events increased, and central apnea decreased at insufficient stimulation.10 When the range of stimulation amplitude was adjusted to approximately 1.66–2V, both CSA and OSA achieved satisfactory levels. With other configuration defaults unchangeable during the visit, pulse width and frequency were 90 μs and 33 Hz, respectively, with bipolar configuration, which indicates that determining an effective range of stimulation amplitude might be able to solve TECSA. Furthermore, this result of the titration study strongly supports our hypothesis that an appropriate stimulation amplitude could solve TECSA. During the titration study for patient 2, no elevated CSA was observed (CAI of 2.21 event/h) with the device off. While the stimulation amplitude increased from 1.4, 1.8 to 2.0V, CAI was 2.6, 0.7, and 5.33 event/h, respectively. Notably, the minimum CAI, OAI, AHI, best sleep efficacy, and ODI were observed at 1.8 V.
As shown in Figure 6, this study hypothesized that the underlying mechanism of the persistent TECSA might be a combination of a high loop gain and an upper airway effect. The endotypes of OSA include the passive critical closing pressure (Pcrit), arousal threshold, loop gain and muscle responsiveness, arousal leads to ventilatory compensation resulting in significant CO2 expulsion, which reduces respiratory drive and can cause apnea and central respiratory instability.11–13 In 2014, Edwards et al14 indicated clinical predictor of respiratory arousal threshold in OSA patients, LAT score + (AHI < 30 events/h)/(SpO2 nadir > 82.5%) + (F hypopneas > 58.3%). Accordingly, both patients with TECSA had a low Arth, the endotype of OSA should be studied further to explore the underlying mechanisms in the future.15,16
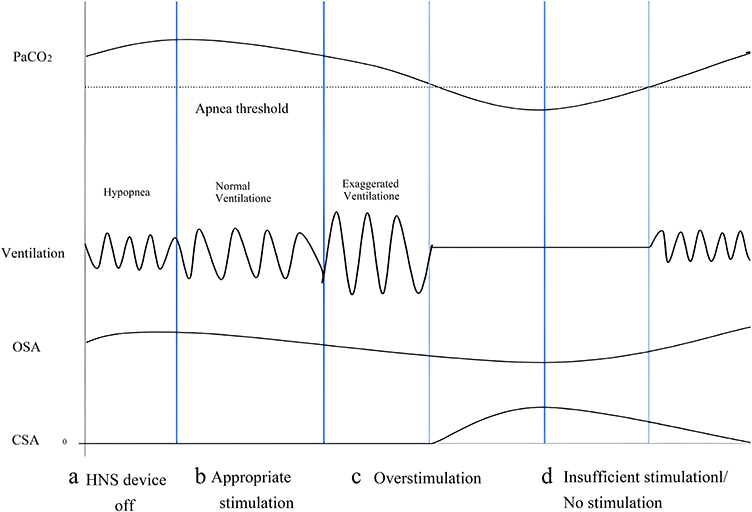 |
Figure 6 The possible mechanism of TECSA following HNS. Abbreviations: PaCO2, prevailing partial pressure of carbon dioxide; AT, dotted line, apnea threshold; VE, minute ventilation, ventilation; AT, apnea threshold. Notes: (A) While the device is off, the prevailing PaCO2 exceeds the AT, there is an improvement of OSA and no CSA occurs; (B) While the HNS is set at an optimal stimulation amplitude to treat upper airway obstruction, the prevailing PaCO2 exceeds the AT with normal ventilation, CSA will not occur while OSA is solved; (C) When HNS overstimulates the upper airway, OSA and inspiratory flow. |
The main limitations of our study are the small sample, retrospective study characteristics and lack of complete clinical data to evaluate the possible postoperative clinical indicators, and the results and hypothesis are exploratory. Moreover, the underlying mechanisms of TECSA still need more evidence and scheduled follow-up in the future.
Conclusion
In summary, this study suggested that OSA patients who have severe daytime sleepiness are more likely to develop TECSA following HNS. The stimulation amplitude of HNS might influence the development phenotype of TECSA. Moreover, multiple underlying mechanisms might be a combination of a high loop gain and upper airway effects in such patients.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Acknowledgments
The authors appreciate Peter Ambros contributing to data collecting, Dr. Nadine Richter (Inspire Medical Systems, Inc.) for help with data extraction and Mr. Mike Mutschelknaus with the language editing.
Funding
This study was funded by the Charité – Universitätsmedizin Berlin.
Disclosure
Philipp Arens received financial support from ImThera Inc. and Apnex Medical Inc. within the framework of research projects related to hypoglossal nerve stimulation therapy. Philipp Arens received a speaker’s fee for an invited talk on behalf of Inspire Medical Inc. and an honorarium for a surgical proctoring. He also reports personal fees from Verlag für Printmedien und PR, XM Consult, and RG Gesellschaft für Information und Organisation mbH, outside the submitted work. Prof. Dr. Thomas Penzel reports unrestricted study grants from Cidelec, grants for consultation and study from Bayer Healthcare, consultation for Philips, grants, personal fees from Löwenstein Medical, personal fees from Neuwirth, Jazz Pharma, Idorsia, National Sleep Foundation, Cerebra, consultation and devices for Sleepimage, outside the submitted work. He also owns shares of Advanced Sleep Research GmbH, The Siestagroup GmbH, Nukute. Other authors report no conflicts of interest in this work.
References
1. Strollo PJ, Soose RJ, Maurer JT, et al. STAR Trial Group. Upper-airway stimulation for obstructive sleep apnea. N Engl J Med. 2014;370(2):139–149. PMID: 24401051. doi:10.1056/NEJMoa1308659
2. Patel J, Daniels K, Bogdan L, Huntley C, Boon M. Elevated central and mixed apnea index after upper airway stimulation. Otolaryngol Head Neck Surg. 2020;162(5):767–772. PMID: 32178573. doi:10.1177/0194599820912740
3. Sarber KM, Ishman SL, Patil RD. Emergence of Cheyne-Stokes breathing after hypoglossal nerve stimulator implant in a patient with mixed sleep apnea. JAMA Otolaryngol Head Neck Surg. 2019;145(4):389–390. PMID: 30763424. doi:10.1001/jamaoto.2018.4077
4. Testani E, De Corso E, Losurdo A, et al. Treatment-emergent central sleep apnoea after surgery for obstructive sleep apnoea. Acta Otorhinolaryngol Ital. 2018;38(5):476–479. PMID: 30498277; PMCID: PMC6265664. doi:10.14639/0392-100X-1476
5. Weitzman ED, Kahn E, Pollak CP. Quantitative analysis of sleep and sleep apnea before and after tracheostomy in patients with the hypersomnia-sleep apnea syndrome. Sleep. 1980;3(3–4):407–423. PMID: 7221348. doi:10.1093/sleep/3.3-4.407
6. Aasm, American Academy of Sleep Medicine (AASM). International Classification of Sleep Disorders.
7. Wray CM, Thaler ER. Hypoglossal nerve stimulation for obstructive sleep apnea: a review of the literature. World J Otorhinolaryngol Head Neck Surg. 2016;2(4):230–233. PMID: 29204571; PMCID: PMC5698546. doi:10.1016/j.wjorl.2016.11.005
8. Heiser C, Thaler E, Boon M, Soose RJ, Woodson BT. Updates of operative techniques for upper airway stimulation. Laryngoscope. 2016;126(Suppl 7):S12–6. PMID: 27572119. doi:10.1002/lary.26158
9. Dedhia RC, Strollo PJ, Soose RJ. Upper airway stimulation for obstructive sleep apnea: past, present, and future. Sleep. 2015;38(6):899–906. doi:10.5665/sleep.4736
10. Zhang J, Wang L, Guo HJ, Wang Y, Cao J, Chen BY. Treatment-emergent central sleep apnea: a unique sleep-disordered breathing. Chin Med J. 2020;133(22):2721–2730. PMID: 33009018; PMCID: PMC7725531. doi:10.1097/CM9.0000000000001125
11. Zhu Z, Hofauer B, Wirth M, Heiser C. Long-term changes of stimulation intensities in hypoglossal nerve stimulation. J Clin Sleep Med. 2020;16(10):1775–1780. doi:10.5664/jcsm.8320
12. Eckert DJ. Phenotypic approaches to obstructive sleep apnoea - New pathways for targeted therapy. Sleep Med Rev. 2018;37:45–59. doi:10.1016/j.smrv.2016.12.003
13. Aishah A, Eckert DJ. Phenotypic approach to pharmacotherapy in the management of obstructive sleep apnoea. Curr Opin Pulm Med. 2019;25(6):594–601. doi:10.1097/MCP.0000000000000628
14. Carberry JC, Amatoury J, Eckert DJ. Personalized management approach for OSA. Chest. 2018;153(3):744–755. doi:10.1016/j.chest.2017.06.011
15. Edwards BA, Eckert DJ, McSharry DG, et al. Clinical predictors of the respiratory arousal threshold in patients with obstructive sleep apnea. Am J Respir Crit Care Med. 2014;190(11):1293–1300. doi:10.1164/rccm.201404-0718OC
16. Baptista PM, Costantino A, Moffa A, Rinaldi V, Casale M. Hypoglossal nerve stimulation in the treatment of obstructive sleep apnea: patient selection and new perspectives. Nat Sci Sleep. 2020;12:151–159. doi:10.2147/NSS.S221542
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.