Back to Journals » Cancer Management and Research » Volume 17

Peritoneal Metastasis in Non-Small Cell Lung Cancer: A Systematic Review of Clinical Features, Molecular Profiles, Diagnostic Approaches, and Outcomes
Authors Ohta R ![]() , Ryu Y, Tanaka K
, Ryu Y, Tanaka K ![]() , Sano C, Hayashi H
, Sano C, Hayashi H ![]()
Received 22 May 2025
Accepted for publication 8 September 2025
Published 19 September 2025 Volume 2025:17 Pages 2127—2141
DOI https://doi.org/10.2147/CMAR.S542123
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Antonella D'Anneo
Ryuichi Ohta,1– 3 Yoshinori Ryu,1 Kaoru Tanaka,2 Chiaki Sano,3 Hidetoshi Hayashi2
1Department of Community Care, Unnan City Hospital, Unnan City, Shimane, Japan; 2Department of Medical Oncology, Kindai University Faculty of Medicine, Osaka-Sayama City, Osaka, Japan; 3Community Medicine Management, Shimane University Faculty of Medicine, Izumo City, Shimane, Japan
Correspondence: Ryuichi Ohta, Department of Community Care, Unnan City Hospital, Unnan, Shimane, Japan, Email [email protected]
Introduction: Peritoneal metastasis is an uncommon but clinically significant manifestation of non-small cell lung cancer (NSCLC). While traditionally associated with gastrointestinal or ovarian malignancies, emerging reports suggest that NSCLC, particularly adenocarcinoma with driver mutations, can also exhibit peritoneal dissemination. This systematic review aims to synthesize current evidence on the clinical characteristics, diagnostic modalities, molecular profiles, treatment strategies, and outcomes of NSCLC patients with peritoneal metastasis.
Methods: A systematic literature search was conducted in PubMed, Embase, and Web of Science from inception through April 2025. Studies were eligible if they reported peritoneal metastasis in histologically confirmed NSCLC patients. Data on histopathology, molecular alterations, diagnosis, treatment, and survival were extracted. The review was conducted in accordance with PRISMA 2020 guidelines.
Results: Twenty-seven studies met inclusion criteria, comprising 19 case-based reports and seven retrospective cohort studies. Adenocarcinoma was the predominant histologic type (93%), and EGFR mutations were the most frequently reported molecular alteration. Diagnosis was primarily established via ascitic cytology, imaging, or intraoperative findings. Targeted therapy (eg, EGFR- or BRAF-directed TKIs) yielded temporary disease control in selected cases. However, median overall survival after peritoneal metastasis ranged from 2.0 to 5.2 months. Prognostic factors included poor performance status, absence of actionable mutations, and concurrent pleural metastasis.
Conclusion: Peritoneal metastasis in NSCLC is rare but associated with poor prognosis. Molecular-guided therapies offer transient benefit, underscoring the need for early recognition and individualized treatment approaches. Prospective studies are warranted to better define predictors and optimal management strategies for this atypical metastatic pattern.
Keywords: non-small cell lung cancer, peritoneal neoplasms, neoplasm metastasis, targeted therapy, molecular diagnostic techniques, prognosis
Introduction
Non-small cell lung cancer (NSCLC) accounts for approximately 85% of all lung cancer cases and is often diagnosed at an advanced stage with distant metastasis.1 Common sites of metastasis include the brain, bones, liver, and adrenal glands, and these patterns have been extensively studied.2 In contrast, peritoneal metastasis (PM) in NSCLC is considered rare and remains poorly characterized in incidence, clinical features, diagnostic approach, prognosis, and treatment strategies.3
PM is more frequently encountered in gastrointestinal malignancies such as gastric, colorectal, and pancreatic cancers, where it is often associated with widespread peritoneal dissemination.4 However, in NSCLC, the diagnosis of PM is challenging due to nonspecific clinical symptoms such as abdominal pain, ascites, and gastrointestinal complaints.5,6 These symptoms often mimic those of other advanced cancers, resulting in delayed diagnosis and limited therapeutic options. Imaging techniques such as CT, MRI, and PET-CT can detect peritoneal involvement, but early identification remains difficult.7 Furthermore, definitive diagnosis may require pathological confirmation through ascitic fluid cytology or peritoneal biopsy.
Although several case reports and cohort studies suggest that PM frequency in NSCLC ranges from 1% to 5%, the data remain fragmented, and the associated risk factors are not fully elucidated.4 Emerging therapies, including targeted agents and immune checkpoint inhibitors (ICIs), may influence metastatic patterns in NSCLC.8 For instance, patients with EGFR (Epidermal Growth Factor Receptor) mutations or ALK (Anaplastic Lymphoma Kinase) rearrangements are known to exhibit distinct metastatic profiles. Yet, their association with PM is not well understood.9,10 Similarly, the impact of novel therapies on PM progression and response is unclear.
Given these gaps in the literature, there is an urgent need to synthesize existing evidence regarding histopathological features, diagnostic characteristics, risk factors, treatment approaches, and prognosis of PM in NSCLC patients. This systematic review, conducted following PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, aims to consolidate and evaluate current knowledge, thereby providing a comprehensive understanding that can inform clinical decision-making.11
Methods
Study Design
This study is a systematic review of published literature investigating the frequency and associated factors of PM in NSCLC. This manuscript reports the methodology of the systematic review component.
Protocol Registration
The International Prospective Register of Systematic Reviews (PROSPERO) has registered the review protocol. The registered number was CRD420251016924.
Search Strategy
A comprehensive literature search was conducted using the following databases: PubMed, Embase, and Web of Science. Additional databases, including the Cochrane Library and Scopus, were considered where necessary. The search period was restricted to studies published between January 2000 and March 2025. The search strategy included both MeSH terms and keyword variants as follows:
- (“non-small cell lung cancer” OR “NSCLC” OR “lung adenocarcinoma”) AND
- (“peritoneal metastasis” OR “peritoneal dissemination” OR “peritoneal carcinomatosis”)
Only English-language articles were included. Abstracts, conference proceedings, and non-peer-reviewed studies were excluded to ensure data quality.
Study Selection
Two independent reviewers screened the titles and abstracts of retrieved studies. Full-text articles were then reviewed for eligibility based on the following criteria. Inclusion Criteria are studies involving NSCLC patients with confirmed PM by imaging (CT, MRI, PET-CT) or pathological diagnosis (ascitic cytology or peritoneal biopsy), original research articles, including case reports, cohort studies, cross-sectional studies, or case-control studies and reports providing data on frequency, clinical characteristics, risk factors, treatment, or prognosis of PM. Exclusion criteria include non-human or basic science studies, studies lacking clear diagnostic criteria for PM, duplicated data (where the most recent or comprehensive study was selected), and non-peer-reviewed data, editorials, or opinion pieces. Disagreements were resolved through discussion or by a third reviewer. The study selection process was documented using a PRISMA flow diagram.
Data Extraction and Synthesis
Data were extracted systematically from each eligible study, including frequency of PM in NSCLC, patient demographics and clinical features, histological subtypes and molecular characteristics (eg, EGFR, ALK, KRAS (Kirsten Rat Sarcoma Viral Oncogene Homolog) mutations), diagnostic modalities used, co-existing distant metastasis, treatment strategies and outcomes (eg, chemotherapy, targeted therapy, ICIs), overall survival (OS) and progression-free survival (PFS). Risk of bias was assessed using the Newcastle-Ottawa Scale for observational studies or the Cochrane Risk of Bias tool, as appropriate.
A narrative synthesis was performed due to expected heterogeneity. Where possible, pooled analyses of frequency and prognostic outcomes were conducted using weighted means. Hazard ratios (HRs) and odds ratios (ORs) were calculated to evaluate the association between clinical variables and PM.
Statistical Analysis
No formal meta-analysis was conducted due to substantial heterogeneity in study design, patient populations, outcome reporting, and methodological quality among the included studies. Instead, a narrative synthesis approach was employed to summarize findings across the 27 studies qualitatively. Extracted data were categorized by histopathological subtype, molecular profile, diagnostic method, treatment strategy, and reported outcomes, including overall survival and treatment response.
Where feasible, descriptive statistics such as counts and proportions were used to illustrate the distribution of key clinical and molecular characteristics (eg, the prevalence of adenocarcinoma, frequency of EGFR mutations). However, pooled effect estimates (eg, hazard ratios, odds ratios) were not calculated. Due to the nature of the included literature—primarily case reports and small retrospective cohorts—statistical comparisons or subgroup analyses were not performed. All results are presented descriptively; no statistical software was used in the data synthesis.
Study quality was appraised based on study design. The Joanna Briggs Institute (JBI) Critical Appraisal Checklists were used for case reports and case series. For retrospective cohort studies, the NIH Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies was applied. Two reviewers independently assessed all studies, and discrepancies were resolved through discussion. Quality ratings were not used for exclusion but were considered in the interpretation of findings.
Results
Study Selection
A total of 665 records were identified through database searches, including 578 from Embase, 48 from Web of Science, and 39 from PubMed. After 74 duplicates were removed—73 by Covidence and one manually—591 records remained for screening. Title and abstract screening yielded 100 relevant studies for full-text review (Figure 1).
 |
Figure 1 PRISMA Flow Diagram of Study Selection. The diagram depicts the selection process of studies included in this systematic review, based on PRISMA 2020 guidelines. Blue bolded values represent the number of studies at each respective step of the PRISMA screening process. Adapted from Page M J, McKenzie J E, Bossuyt P M, Boutron I, Hoffmann T C, Mulrow C D et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021; 372:n71. Creative Commons. |
Of these, 13 articles were excluded after full-text assessment due to the following reasons: wrong setting (n = 4), wrong outcomes (n = 2), wrong intervention (n = 1), wrong study design (n = 2), and wrong patient population (n = 4). Ultimately, 27 studies were included in the systematic review (Table 1).
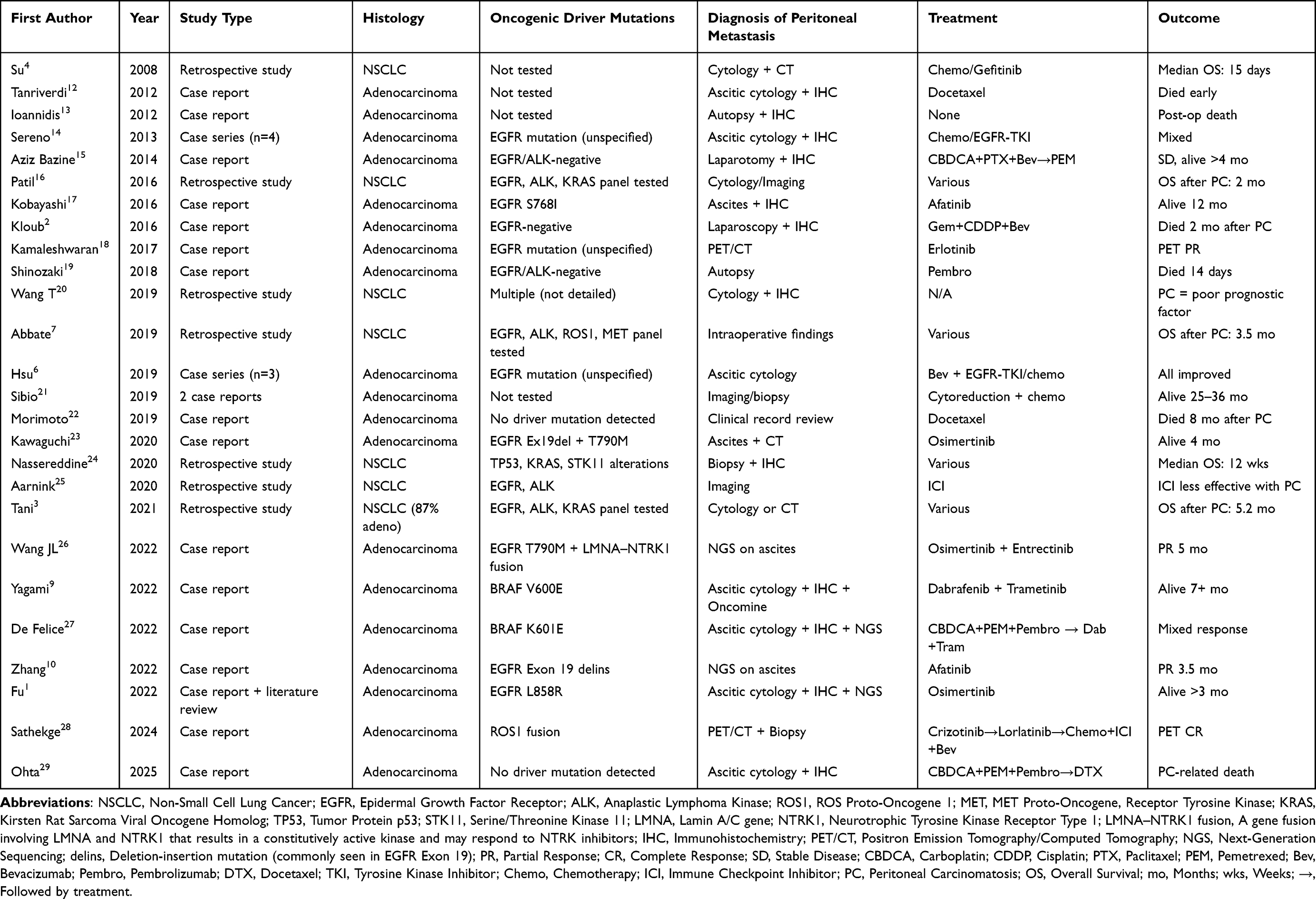 |
Table 1 The Characteristics of the Included Articles |
Characteristics of the Included Articles
The included studies comprised 19 case reports or series and seven retrospective cohort studies. All studies described patients with histologically confirmed NSCLC who developed peritoneal metastasis, confirmed by imaging, cytology, or histopathology. These reports provided detailed information regarding diagnostic strategies, treatment modalities—including chemotherapy, immune checkpoint inhibitors, and targeted therapies—and patient outcomes (Table 1).
Histopathological Features
Among the 27 studies in this review, histological subtype was reported in all 20 case-based reports and six retrospective cohort studies. Pulmonary adenocarcinoma was the most prevalent histologic subtype, identified in 25 of the 27 studies (93%), encompassing all individual case reports and case series. Across these studies, adenocarcinoma was explicitly described in at least 34 patients, drawn from case-based and cohort-derived data.
Only a single case of squamous cell carcinoma with confirmed peritoneal involvement was identified, reported in a retrospective analysis by Patil et al (2016).16 No large-cell carcinoma, adenosquamous carcinoma, or pleomorphic carcinoma were noted in the included literature. Prominent examples of adenocarcinoma-associated peritoneal metastasis include the following.
- Morimoto et al (2019), Kawaguchi et al (2020), Yagami et al (2022), Wang JL et al (2022), and Shinozaki et al (2018), all of whom reported cases with histologically confirmed lung adenocarcinoma followed by clinically or radiologically diagnosed peritoneal carcinomatosis.9,19,22,23,26
- In a small case series, Sereno et al (2013) described four patients with lung adenocarcinoma, each of whom subsequently developed peritoneal metastasis.14
- Nassereddine et al (2020) reported a retrospective pathology-based cohort of 12 patients with peritoneal carcinomatosis, among whom 11 had confirmed adenocarcinoma.24
- Large multicenter cohorts by Abbate et al (2019) and Tani et al (2021) demonstrated a similarly high prevalence of adenocarcinoma in patients with peritoneal spread, accounting for 80% to 87% of reported cases.3,7
The overrepresentation of adenocarcinoma among NSCLC patients with peritoneal metastasis may reflect its well-documented tendency toward hematogenous dissemination and serosal surface invasion. In multiple instances, such as those described by Kobayashi et al (2016), Zhang et al (2022) and Ohta et al (2025), peritoneal carcinomatosis was the initial or isolated site of metastatic recurrence, occurring even after prior systemic disease control10,17,29 (Table 2).
 |
Table 2 Histological Subtypes of NSCLC with Peritoneal Metastasis |
Molecular Characteristics
Molecular profiling was available in 23 of the 27 included studies, providing important insights into the relationship between oncogenic drivers and peritoneal dissemination in NSCLC. Among these, EGFR mutations were the most frequently reported, identified in at least 11 patients across 10 studies. These included classical sensitizing variants such as Exon 19 deletions, L858R, and resistance mutations like T790M, as well as less common alterations such as S768I and deletion-insertion mutation in EGFR Exon 19.
Multiple case reports demonstrated clinical benefit from EGFR-targeted therapy in the context of peritoneal metastasis. For instance, Kawaguchi et al (2020) and Kobayashi et al (2016) described favorable responses to osimertinib and afatinib, respectively, in EGFR-mutated adenocarcinoma patients with symptomatic peritoneal involvement.17,23 Zhang et al (2022) reported partial radiologic response to afatinib in a patient harboring a rare Exon 19 delinsIP mutation, and Fu et al (2022) documented temporary disease control in a patient with EGFR L858R mutation treated with osimertinib.1,10 Additionally, Hsu et al (2019) reported three EGFR-positive patients with malignant ascites who experienced clinical improvement following bevacizumab-based therapy, with or without tyrosine kinase inhibitors.6
Beyond EGFR, other actionable mutations were less common but notable BRAF mutations were identified in two cases: V600E (Yagami et al, 2022) and K601E (De Felice et al, 2022), both treated with dabrafenib + trametinib, with partial or mixed responses.9,27,30 A particularly rare acquired LMNA–NTRK1 fusion was detected post-osimertinib resistance in a case by Wang JL et al (2022), and was managed with entrectinib plus rechallenge EGFR-TKI. Sathekge et al (2024) presented a patient with ROS1 fusion-positive NSCLC and peritoneal metastasis who achieved complete metabolic response on PET following sequential targeted therapy.26,28
In contrast, Ohta et al (2025) described a case of adenocarcinoma without oncogenic driver mutation, confirmed through ascitic cytology and immunohistochemistry (IHC), in which platinum-doublet chemotherapy plus pembrolizumab, followed by docetaxel, failed to prevent progression of peritoneal carcinomatosis.29
Cohort studies by Nassereddine et al (2020) and Abbate et al (2019) further revealed frequent alterations in TP53, KRAS, and STK11 in patients with aggressive clinical courses; however, these analyses did not specifically correlate mutational subtypes with peritoneal spread.7,24
In summary, oncogenic driver mutations—particularly EGFR and BRAF—appear to influence not only therapeutic responsiveness but may also correlate with a propensity for peritoneal dissemination. While most responses to targeted agents were transient, these findings suggest that molecular subtypes may shape unique metastatic trajectories, warranting further investigation in larger, molecularly stratified cohorts (Table 3).
 |
Table 3 Molecular Alterations and Clinical Features in NSCLC with Peritoneal Metastasis |
Diagnosis of Peritoneal Metastasis
Diagnostic approaches for identifying peritoneal metastasis in NSCLC patients varied considerably across the included studies, reflecting the clinical urgency and available diagnostic infrastructure in each case. The most frequent method of diagnosis was cytological analysis of ascitic fluid, used in at least 20 individual reports. Malignant cells with adenocarcinomatous features were identified in ascitic samples, providing the initial evidence of peritoneal carcinomatosis.
Imaging studies played a pivotal role in both diagnosis and disease monitoring. Contrast-enhanced CT and 18F-fluorodeoxyglucose positron emission tomography/computed tomography (FDG PET/CT) were frequently employed to detect characteristic findings such as diffuse peritoneal nodules, omental caking, and FDG-avid ascites, as described in studies by Sathekge et al (2024) and Kamaleshwaran et al (2017).18,28 In some cases, peritoneal metastasis was suspected solely based on PET imaging in asymptomatic patients.
In patients presenting with acute abdomen, ileus, or bowel obstruction, surgical exploration—either by laparoscopy or laparotomy—allows for both diagnostic confirmation and therapeutic intervention. For example, Sibio et al (2019) and Bazine et al (2014) reported cases where intraoperative findings led to diagnosis and subsequent cytoreductive surgery.15,21
Post-mortem examination was the definitive diagnostic tool in rapidly deteriorating cases or those with unclear etiology. Shinozaki et al (2018) and Ioannidis et al (2012) both described cases where peritoneal carcinomatosis was confirmed at autopsy after unexpected clinical decline.13,19
To confirm the pulmonary origin of metastatic peritoneal lesions, immunohistochemical (IHC) staining was essential. TTF-1 and CK7 were consistently positive across studies, while gastrointestinal markers such as CK20 and CDX2 remained negative. These staining patterns effectively distinguished lung adenocarcinoma from gastrointestinal primaries in peritoneal deposits, especially in cytology-only diagnoses.
In several recent reports, next-generation sequencing (NGS) or targeted mutation were applied to cell blocks or cytospin preparations derived from ascites, enabling the detection of key molecular alterations such as EGFR, BRAF, or NTRK mutations. This approach not only provided diagnostic confirmation but also facilitated personalized therapy selection, as illustrated in the cases by Wang JL et al (2022), Zhang et al (2022), Yagami et al (2022), Fu et al (2022), and De Felice et al (2022).1,9,10,26,27 Cases such as Ohta et al (2025) highlight that diagnosis based solely on ascitic cytology and IHC remains clinically relevant in settings where molecular profiling is unavailable.29
The combination of cytological, radiographic, surgical, and molecular methods underscores the complexity of diagnosing peritoneal metastasis in NSCLC. Importantly, early and accurate identification of PC has meaningful implications for prognosis and treatment selection (Table 4).
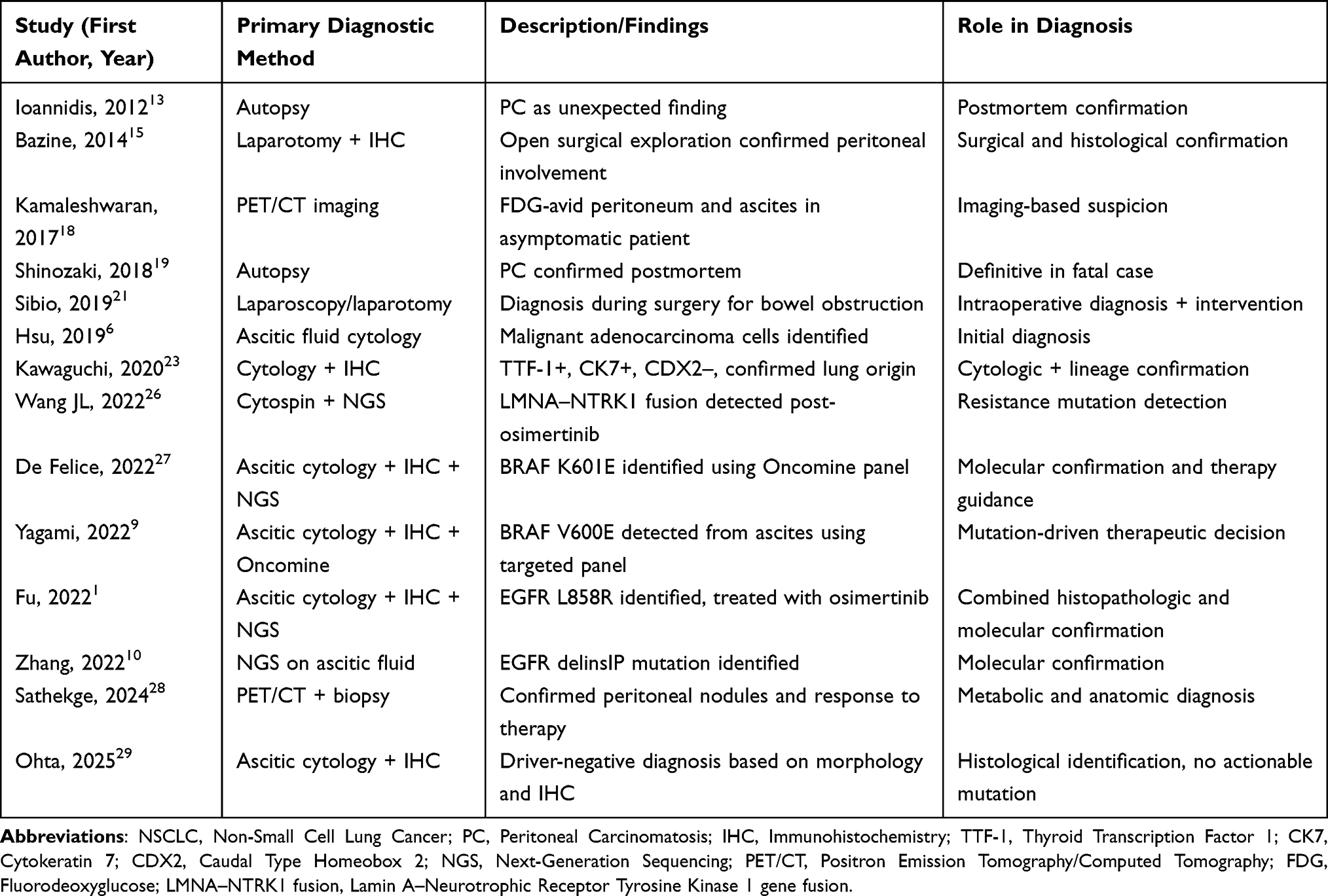 |
Table 4 Diagnostic Modalities for Peritoneal Metastasis in NSCLC |
Targeted Therapies
Most patients with known oncogenic drivers received tyrosine kinase inhibitors (TKIs), resulting in variable but frequently favorable responses. EGFR-mutated cases were typically managed with osimertinib, afatinib, or erlotinib, demonstrating radiologic regression of ascites or symptomatic improvement. For instance, Kawaguchi et al (2020) and Kobayashi et al (2016) reported improved performance status and resolution of malignant ascites following osimertinib and afatinib treatment, respectively.17,23,31 Similarly, Zhang et al (2022) and Fu et al (2022) described favorable responses to afatinib and osimertinib in patients harboring uncommon EGFR variants, including Exon 19 delinsIP and L858R mutations.1,10
Hsu et al (2019) also reported that all three EGFR-mutant patients in their series responded to bevacizumab-based therapy with or without EGFR-TKIs.6 Beyond EGFR, BRAF-mutated cases responded to combination therapy with dabrafenib and trametinib, as reported in Yagami et al (2022) and De Felice et al (2022).9,27
A unique molecular evolution was noted by Wang JL et al (2022), who reported a patient with acquired LMNA–NTRK1 fusion following osimertinib resistance. The patient was subsequently treated with a combination of entrectinib and rechallenge osimertinib, achieving transient disease control.26
Additionally, Sathekge et al (2024) documented a ROS1-positive patient who achieved a complete metabolic response after sequential treatment with crizotinib, lorlatinib, and combination chemotherapy, immune checkpoint inhibitors (ICIs), and bevacizumab.28
Chemotherapy and Immunotherapy
For patients lacking actionable mutations or with deteriorated performance status, systemic chemotherapy—commonly platinum-based regimens—was frequently utilized. Regimens such as carboplatin plus pemetrexed, often combined with immune checkpoint inhibitors (eg, pembrolizumab) or anti-angiogenic agents (eg, bevacizumab), were typical.
Outcomes, however, were generally poor after the establishment of peritoneal carcinomatosis. For example, Ohta et al (2025) and Morimoto et al (2019) both reported rapid disease progression despite aggressive platinum-based therapy and second-line docetaxel.22,29
Nonetheless, isolated exceptional responses were observed. Sathekge et al (2024) described a case where carboplatin + pemetrexed + atezolizumab + bevacizumab led to complete metabolic response on PET, though relapse occurred subsequently.28 Other supportive examples include Bazine et al (2014), who reported stable disease exceeding 4 months with combination chemotherapy and anti-VEGF therapy, and Sibio et al (2019), who documented long-term survival (25–36 months) following cytoreductive surgery and systemic chemotherapy in two highly selected patients with isolated peritoneal metastasis.15,21
Additionally, Tanriverdi et al (2012) and Shinozaki et al (2018) exemplified the limited effectiveness of monotherapy (eg, docetaxel or pembrolizumab) in rapidly deteriorating patients with advanced disease burden.12,19 These findings underscore the need for early molecular characterization and aggressive intervention prior to performance status decline.
Surgical Intervention
Surgical treatment was rarely pursued but yielded encouraging outcomes in two carefully selected patients described by Sibio et al (2019).21 Both underwent cytoreductive surgery (including bowel resection and omentectomy) for symptomatic peritoneal disease and survived 25 and 36 months, respectively. These cases underscore the potential role of surgery in highly selected individuals with isolated peritoneal metastasis and preserved performance status21 (Table 5).
 |
Table 5 Surgical Management and Outcomes |
Overall Outcomes
Despite advances in targeted and immunotherapy, the prognosis after the diagnosis of peritoneal carcinomatosis remained poor in most reports. Reported survival ranged from as little as 2 weeks to 12 months, with retrospective studies such as those by Abbate et al (2019) and Tani et al (2021) estimating median OS between 2.0 and 5.2 months.3,7 Patients with driver mutations who received appropriate targeted therapy generally had more favorable outcomes, albeit with a limited duration of disease control (Figure 2).
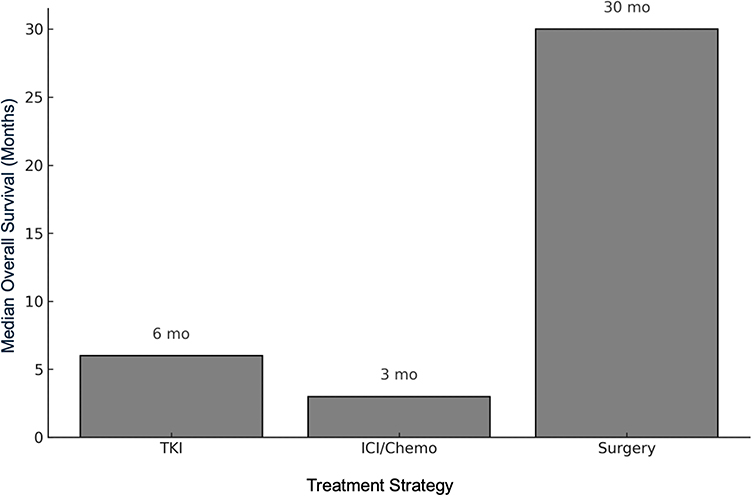 |
Figure 2 Estimated median overall survival by treatment strategy in NSCLC patients with peritoneal metastasis. Bar chart illustrates the approximate median overall survival (OS) in months according to major treatment strategies reported in the literature. Patients who received tyrosine kinase inhibitors (TKIs) for targetable mutations demonstrated modest survival prolongation (median ~6 months), while those treated with chemotherapy and/or immune checkpoint inhibitors (ICIs) had shorter survival (median ~3 months). Surgical intervention, although rarely performed, was associated with the longest survival in selected patients with isolated peritoneal involvement (median ~30 months). These findings underscore the heterogeneity of outcomes based on treatment modality. Abbreviations: TKI, Tyrosine Kinase Inhibitor; ICI, Immune Checkpoint Inhibitor; OS, Overall Survival; mo, Months. |
Prognostic Indicators
The prognosis for patients with NSCLC and peritoneal metastasis was generally poor across the included studies. However, several clinical and molecular factors consistently emerged as potential outcome indicators (Table 6).
 |
Table 6 Prognostic Factors and Reported Outcomes in NSCLC with Peritoneal Metastasis |
Poor performance status, particularly an Eastern Cooperative Oncology Group (ECOG) score of ≥2, was frequently associated with rapid deterioration and limited treatment eligibility. In multiple case reports, patients who were bedridden at the time of PC diagnosis either received best supportive care or failed to complete systemic therapy, leading to death within weeks. For example, Shinozaki et al (2018) described a patient who died within 14 days of initiating ICI therapy, later confirmed at autopsy to have extensive peritoneal metastasis.19
The presence of concurrent pleural metastasis further worsened the prognosis. A retrospective analysis by Aarnink et al (2020) demonstrated that pleuroperitoneal involvement was an independent predictor of reduced PFS and OS in patients treated with ICIs, with a hazard ratio of 2.1 (p < 0.05).25 This suggests extensive serosal dissemination reflects a biologically aggressive tumor phenotype, potentially less responsive to immunotherapy.
Another key prognostic variable was the absence of targetable mutations. Patients without actionable oncogenic drivers—such as EGFR, BRAF, ROS1, or NTRK fusions—had limited systemic treatment options and often experienced poor responses to chemotherapy or immunotherapy. By contrast, patients harboring EGFR mutations or other actionable alterations, as reported in studies by Kawaguchi et al (2020) and Wang JL et al (2022), showed improved disease control and symptom relief when treated with appropriate tyrosine kinase inhibitors.23,26 Nonetheless, these responses were often transient, and peritoneal progression ultimately led to clinical decline in most cases.
Finally, several patients were unable to receive adequate systemic therapy due to rapid clinical deterioration or comorbidities, underscoring the importance of early recognition and intervention. The narrow therapeutic window between the diagnosis of peritoneal metastasis and functional decline may limit opportunities for aggressive treatment (Figure 3).
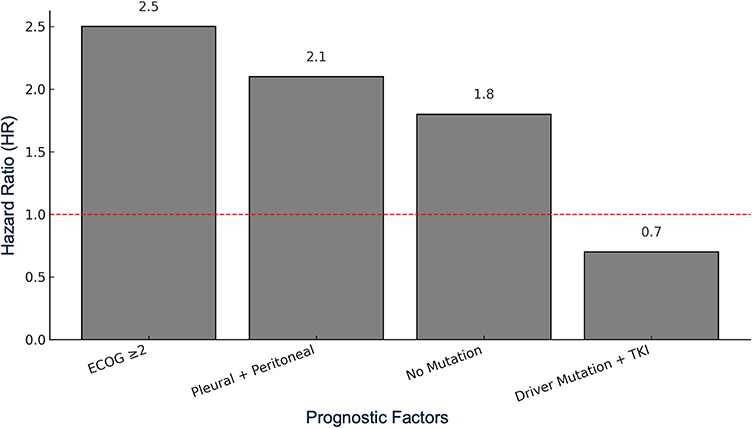 |
Figure 3 Estimated impact of prognostic factors on overall survival (OS) in NSCLC patients with peritoneal metastasis. Bar plot shows the estimated hazard ratios (HR) associated with key prognostic indicators identified across included studies. Poor performance status (ECOG ≥2), concurrent pleural metastasis, and absence of actionable driver mutations (eg, EGFR, BRAF, ROS1, NTRK) were associated with worse survival outcomes (HR >1). Conversely, the presence of driver mutations with administration of targeted therapies was associated with more favorable prognosis (HR <1). The red dashed line indicates the HR baseline of 1.0. Abbreviations: ECOG, Eastern Cooperative Oncology Group; HR, Hazard Ratio; TKI, Tyrosine Kinase Inhibitor; ICI, Immune Checkpoint Inhibitor; OS, Overall Survival. |
Quality Assessment Results
Among the 27 included studies, case reports and case series generally fulfilled core JBI criteria, though follow-up duration and outcome clarity were inconsistently reported. Retrospective studies were of moderate quality overall, with limitations in outcome reporting and selection criteria noted in some. Detailed assessments are available in Supplementary Table 1.
Discussion
Summary of the Study
This systematic review synthesized evidence from 27 studies reporting peritoneal metastasis in patients with NSCLC, encompassing 19 case-based publications and seven retrospective cohort studies. The findings highlight that PC, although rare in NSCLC, is a clinically significant manifestation associated with poor prognosis. Pulmonary adenocarcinoma was the predominant histologic subtype, present in 93% of included studies, and frequently associated with driver mutations such as EGFR and BRAF. Peritoneal metastasis was often diagnosed by cytology, imaging, or surgery, and occasionally confirmed at autopsy. Targeted therapies, especially EGFR TKIs, were associated with symptomatic relief and short-term disease control. However, median OS following PC diagnosis remained poor, generally between 2.0 and 5.2 months in retrospective cohorts.
Comparison with Other Studies
Previous large-scale epidemiologic reports have estimated the incidence of peritoneal metastasis in NSCLC to be less than 1%, primarily based on autopsy data or population registries.1,32 The present review expands on these findings by providing granular clinical, pathological, and molecular details. Compared to earlier systematic overviews, this study identifies an increasing number of recent reports using advanced diagnostics such as NGS on ascitic fluid to guide therapy—a method rarely documented before 2015. Additionally, while historical perspectives have emphasized hematogenous and lymphatic spread in NSCLC, our findings support that serosal dissemination, particularly in adenocarcinoma, may be under-recognized, especially in patients with long-standing systemic control of thoracic disease.33
Our results also align with recent literature suggesting that patients with actionable mutations may be at increased risk of atypical metastatic presentations, including leptomeningeal and peritoneal spread.34,35 However, whether molecular drivers such as EGFR mutations directly predispose to peritoneal involvement remains unclear and warrants further mechanistic investigation.
Strengths of the Study
This review represents the most comprehensive synthesis of clinical reports describing peritoneal metastasis in NSCLC. Including individual patient-level data and cohort-level outcomes offers an integrative perspective on clinical characteristics, diagnostic patterns, molecular alterations, and treatment responses. The inclusion of contemporary case reports from the post-2015 era ensures the relevance of newer diagnostic and therapeutic approaches, such as liquid biopsy, IHC-guided diagnosis, and precision oncology strategies using TKIs or BRAF/MEK inhibitors. Furthermore, the PRISMA-guided methodology and rigorous inclusion criteria improve the reliability of the findings.
Limitations
This study has several limitations inherent in it. First, most publications included case reports or small series, which are subject to publication bias, favoring atypical or successful cases. As this review heavily relies on case reports and small series, there is a potential for overrepresentation of unusual or favorable outcomes, which could introduce publication bias. Although our findings highlight an association between driver mutations and peritoneal metastasis, the data remain hypothesis-generating, and no mechanistic link has been established. Prospective molecular studies are warranted to clarify causality. Second, the retrospective nature of all included studies precludes any causal inference or robust prognostic modeling. Most included case reports lacked long-term follow-up and standardized reporting of treatment response metrics such as progression-free survival or RECIST criteria. This hinders comparison and limits conclusions regarding treatment durability. Third, heterogeneity in diagnostic definitions, treatment regimens, and follow-up duration across studies limited quantitative synthesis or meta-analysis. Additionally, few retrospective cohort studies stratified patients based on peritoneal involvement, which restricted our ability to assess prognostic differences between PM-positive and PM-negative populations robustly. Lastly, survival data were inconsistently reported, and formal quality assessments of individual studies were not feasible due to the nature of the source literature. The overall methodological quality of the included studies was variable. While most case reports regarding clinical presentation and treatment were well documented, many lacked standardized outcome reporting or long-term follow-up. Similarly, several retrospective cohort studies showed moderate risk of bias due to retrospective design, small sample sizes, and incomplete data. Although quality assessment tools (JBI and NIH) were used to guide interpretation, given the observational and descriptive nature of most studies, including case reports, the synthesized findings should be interpreted as hypothesis-generating. Quality assessments were conducted but not used for exclusion due to inherent limitations in study design.
Conclusion
Peritoneal metastasis in NSCLC, though uncommon, represents a clinically meaningful manifestation associated with poor prognosis and limited therapeutic options. Pulmonary adenocarcinoma, particularly in patients with driver mutations such as EGFR or BRAF, appears more frequently associated with this metastatic pattern. Targeted therapy can provide short-term disease control, but long-term outcomes remain unsatisfactory. Timely diagnosis—supported by cytology, imaging, and molecular testing—and individualized treatment planning are essential to optimize care. Future prospective studies are needed to better understand the pathophysiology, identify predictive biomarkers for peritoneal tropism, and evaluate the efficacy of novel systemic treatments in this understudied subgroup.
Abbreviations
ALK, Anaplastic Lymphoma Kinase; BRAF, B-Raf Proto-Oncogene; CDX2, Caudal Type Homeobox 2; CBDCA, Carboplatin; CDDP, Cisplatin; CK7, Cytokeratin 7; CK20, Cytokeratin 20; CR, Complete Response; ECOG, Eastern Cooperative Oncology Group; EGFR, Epidermal Growth Factor Receptor; FDG, Fluorodeoxyglucose; HR, Hazard Ratio; IHC, Immunohistochemistry; ICI, Immune Checkpoint Inhibitor; LMNA–NTRK1 fusion, Lamin A/Nuclear Envelope Gene fused with Neurotrophic Receptor Tyrosine Kinase 1; MET, MET Proto-Oncogene, Receptor Tyrosine Kinase; mo, Months; NGS, Next-Generation Sequencing; NSCLC, Non-Small Cell Lung Cancer; OS, Overall Survival; PC, Peritoneal Carcinomatosis; PCR, Polymerase Chain Reaction; PEM, Pemetrexed; PET/CT, Positron Emission Tomography/Computed Tomography; PFS, Progression-Free Survival; PR, Partial Response; ROS1, ROS Proto-Oncogene 1; SD, Stable Disease; SCC, Squamous Cell Carcinoma; STK11, Serine/Threonine Kinase 11; TKI, Tyrosine Kinase Inhibitor; TTF-1, Thyroid Transcription Factor 1; VEGF, Vascular Endothelial Growth Factor; wks, Weeks.
Data Sharing Statement
This study is a systematic review based on previously published articles. No new data were generated or analyzed.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
Dr Kaoru Tanaka reports personal fees from Astrazeneca, Bristol-Myers Squibb, ONO PHARMACEUTICAL, CHUGAI PHARMACEUTICAL, MSD, Eisai, Novartis Pharma, Taiho Pharmaceutical, outside the submitted work. Professor Hidetoshi Hayashi reports grants and/personal fees from IQVIA Services JAPAN K.K., SYNEOS HEALTH CLINICAL K.K., EP-CRSU CO., LTD., EPS Corporation., Otsuka Pharmaceutical Co., Ltd., Takeda Pharmaceutical Co.,Ltd., MSD K.K., Amgen Inc., Chugai Pharmaceutical Co.,Ltd., Nippon Boehringer Ingelheim Co.,Ltd., Janssen Pharmaceutical K.K., Astellas Pharma Inc, Eisai Co., Ltd., Shionogi & Co., Ltd., Nippon Kayaku Co.,Ltd, GlaxoSmithKline K.K., Sanofi K.K., Taiho Pharmaceutical Co.,Ltd., Bristol Myers Squibb Company, SRL Medisearch Inc., PRA Health Sciences Inc., CMIC CO., Ltd., Pfizer R&D Japan G.K., Ascent Development Services, Labcorp Development Japan K.K., Kobayashi Pharmaceutical Co., Ltd., Pfizer Japan Inc., grants, AbbVie Inc., A2 Healthcare Corp., Eli Lilly Japan K.K., Kyowa Kirin Co.,Ltd., Sysmex Corporation, Clinical Research Support Center Kyushu, Kyushu Study group of Clinical Cancer, Public Health Research Foundation, Thoracic Oncology Research Group, Japan Clinical Cancer Research Organization, Eisai Inc., grants from Bayer Yakuhin, Ltd, AstraZeneca K.K., Daiichi Sankyo Co., Ltd., Novartis Pharma K.K., Merck Biopharma Co., Ltd, Medpace Japan K.K., ICON Japan K.K., PPD-SNBL K.K., Mochida Pharmaceutical Co., Ltd., Japanese Gastric Cancer Association, West Japan Oncology Group, Comprehensive Support Project for Oncological Research of Breast Cancer, Ono Pharmaceutical Co., Ltd., Reno. Medical K.K., Hisamitsu Pharmaceutical Co., Inc., Novocure K.K., 3H Clinical Trial Inc., Ishiyaku Publishers,Inc., Care Net, Inc., Guardant Health Japan Corp, and Medical Review Co., Ltd., during the conduct of the study. The authors declare no other competing interests in this work.
References
1. Fu JX, Wang XJ, Xia M, Wang XJ. Peritoneal carcinomatosis secondary to metastatic lung cancer complicated with acute suppurative appendicitis: a case report and literature review. Medicine. 2022;101:e31866. doi:10.1097/md.0000000000031866
2. Hanane K, Salma B, Khadija B, et al. Peritoneal carcinomatosis, an unusual and only site of metastasis from lung adenocarcinoma. Pan Afr Med J. 2016;23:60. doi:10.11604/pamj.2016.23.60.8910
3. Tani T, Nakachi I, Ikemura S, et al. Clinical characteristics and therapeutic outcomes of metastatic peritoneal carcinomatosis in non-small-cell lung cancer. Cancer Manag Res. 2021;13:7497–7503. doi:10.2147/cmar.S330103
4. Su HT, Tsai CM, Perng RP. Peritoneal carcinomatosis in lung cancer. Respirology. 2008;13:465–467. doi:10.1111/j.1440-1843.2008.01268.x
5. Kazakova V, Alarcon Velasco SV, Perepletchikov A, Lathan CS. ROS1-rearranged lung adenocarcinoma with peritoneal carcinomatosis on initial presentation. BMJ Case Rep. 2020;13:e233864. doi:10.1136/bcr-2019-233864
6. Hsu JF, Lee YL, Chang HL, et al. Clinical efficacy of concurrent bevacizumab for malignant ascites in nonsquamous cell carcinoma of the lung. Asia Pac J Clin Oncol. 2019;15:e126–e131. doi:10.1111/ajco.13131
7. Abbate MI, Cortinovis DL, Tiseo M, et al. Peritoneal carcinomatosis in non-small-cell lung cancer: retrospective multicentric analysis and literature review. Future Oncol. 2019;15:989–994. doi:10.2217/fon-2018-0469
8. Araghi M, Mannani R, Heidarnejad Maleki A, et al. Recent advances in non-small cell lung cancer targeted therapy; an update review. Cancer Cell Int. 2023;23:162. doi:10.1186/s12935-023-02990-y
9. Yagami Y, Nakahara Y, Manabe H, et al. Promising response to Dabrafenib plus trametinib in a patient with peritoneal carcinomatosis from non small lung cancer harboring BRAF V600E mutation. Onco Targets Ther. 2022;15:1369–1374. doi:10.2147/ott.S375246
10. Zhang L, Yang L, Sun B, et al. Case report: afatinib sensitivity in rare EGFR E746_L747delinsIP mutated LUAD with peritoneal metastases. Front Oncol. 2022;12:861271. doi:10.3389/fonc.2022.861271
11. Matthew JP, Joanne EM, Patrick MB, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
12. Tanriverdi O, Barutca S, Meydan N. Relapse with isolated peritoneal metastasis in lung adenocarcinoma: case report and review of the literature. Contemp Oncol. 2012;16:586–589. doi:10.5114/wo.2012.32495
13. Ioannidis O, Iordanidis F, Paraskevas G, et al. Omental metastases from primary lung adenocarcinoma. Rev Invest Clin. 2012;64:308–310.
14. Sereno M, Rodriguez-Esteban I, Gomez-Raposo C, et al. Lung cancer and peritoneal carcinomatosis. Oncol Lett. 2013;6:705–708. doi:10.3892/ol.2013.1468
15. Bazine A, Fetohi M, Khmamouch MR, Namad T, Ichou M, Errihani H. An unusual case of isolated peritoneal metastases from lung adenocarcinoma. Case Rep Oncol. 2014;7:600–604. doi:10.1159/000366293
16. Patil T, Aisner DL, Noonan SA, et al. Malignant pleural disease is highly associated with subsequent peritoneal metastasis in patients with stage IV non-small cell lung cancer independent of oncogene status. Lung Cancer. 2016;96:27–32. doi:10.1016/j.lungcan.2016.03.007
17. Kobayashi H, Wakuda K, Takahashi T. Effectiveness of Afatinib in lung cancer with paralytic ileus due to peritoneal carcinomatosis. Respirol Case Rep. 2016;4:e00197. doi:10.1002/rcr2.197
18. Kamaleshwaran KK, Joseph J, Kalarikal RK, Shinto AS. Image findings of rare case of peritoneal carcinomatosis from non small cell lung cancer and response to erlotinib in F-18 FDG positron emission tomography/computed tomography. Indian J Nucl Med. 2017;32:140–142. doi:10.4103/0972-3919.202239
19. Shinozaki T, Iwami E, Ikemura S, et al. A case of pulmonary adenocarcinoma showing rapid progression of peritoneal dissemination after immune checkpoint inhibitor therapy. BMC Cancer. 2018;18:620. doi:10.1186/s12885-018-4549-5
20. Wang T, Lu R, Lai S, et al. Development and validation of a nomogram prognostic model for patients with advanced non-small-cell lung cancer. Cancer Inform. 2019;18:1176935119837547. doi:10.1177/1176935119837547
21. Sibio S, Sica GS, Di Carlo S, et al. Surgical treatment of intraperitoneal metastases from lung cancer: two case reports and a review of the literature. J Med Case Rep. 2019;13:262. doi:10.1186/s13256-019-2178-5
22. Morimoto K, Date K, Kawano H. A case of lung cancer with peritoneal carcinomatosis effectively treated with docetaxel. Japanese J Lung Cancer. 2019;59:71–75. doi:10.2482/haigan.59.71
23. Kawaguchi Y, Hanaoka J, Hayashi H, et al. Clinical efficacy of osimertinib for a patient with ileus due to peritoneal carcinomatosis. Clin Case Rep. 2020;8:347–350. doi:10.1002/ccr3.2645
24. Nassereddine H, Sannier A, Brosseau S, et al. Clinicopathological and molecular study of peritoneal carcinomatosis associated with non-small cell lung carcinoma. Pathol Oncol Res. 2020;26:2795–2800. doi:10.1007/s12253-019-00713-1
25. Aarnink A, Fumet JD, Favier L, Truntzer C, Ghiringhelli F. Role of pleural and peritoneal metastasis in immune checkpoint inhibitors efficacy patients with non-small cell lung cancer: real-world data from a large cohort in France. J Cancer Res Clin Oncol. 2020;146:2699–2707. doi:10.1007/s00432-020-03262-2
26. Wang JL, Wang LS, Zhu JQ, Ren J, Wang D, Luo M. Survival benefit of combinatorial osimertinib rechallenge and entrectinib in an EGFR-mutant NSCLC patient with acquired LMNA-NTRK1 fusion following osimertinib resistance. Respirol Case Rep. 2022;10:e01054. doi:10.1002/rcr2.1054
27. De Felice M, Pisapia P, Pepe F, et al. Unusual clinical experience in BRAF Exon 15 p.K601E-mutated lung cancer: a case report and brief review of the literature. Appl Sci. 2022;12:7552. doi:10.3390/app12157552
28. Sathekge T, Boktor RR, Berlangieri S, Lee ST. Flourine-18 fluorodeoxyglucose positron emission tomography/computed tomography imaging of peritoneal carcinomatosis in lung cancer: a case study. World J Nucl Med. 2024;23:202–206. doi:10.1055/s-0044-1778708
29. Ohta R, Tanaka K, Miyata M, Tanizaki J, Hayashi H. Peritoneal metastasis mimicking chemotherapy-induced complications in lung adenocarcinoma: a diagnostic challenge of a case report. Cureus. 2025;17:e82530. doi:10.7759/cureus.82530
30. Mendoza DP, Dagogo-Jack I, Chen T, et al. Imaging characteristics of BRAF-mutant non-small cell lung cancer by functional class. Lung Cancer. 2019;129:80–84. doi:10.1016/j.lungcan.2019.01.007
31. Kazushi Y, Inoue A, Sugawara S, et al. Overall survival (OS) of EGFR mutation-positive non-small cell lung cancer (NSCLC) patients: real-world treatment patterns of 1,660 Japanese patients (pts). J Clin Oncol. 2016;34:e20503–e20503. doi:10.1200/JCO.2016.34.15_suppl.e20503
32. Satoh H, Ishikawa H, Yamashita YT, Kurishima K, Ohtsuka M, Sekizawa K. Peritoneal carcinomatosis in lung cancer patients. Oncol Rep. 2001;8:1305–1307. doi:10.3892/or.8.6.1305
33. Dela Cruz CS, Tanoue LT, Matthay RA. Lung cancer: epidemiology, etiology, and prevention. Clin Chest Med. 2011;32:605–644. doi:10.1016/j.ccm.2011.09.001
34. Sener U, Kumthekar P, Boire A. Advances in the diagnosis, evaluation, and management of leptomeningeal disease. Neurooncol Adv. 2021;3:v86–v95. doi:10.1093/noajnl/vdab108
35. Ozcan G, Singh M, Vredenburgh J. Leptomeningeal metastasis from non-small cell lung cancer and current landscape of treatments. Clin Cancer Res. 2022;29. doi:10.1158/1078-0432.CCR-22-1585
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.