Back to Journals » International Journal of General Medicine » Volume 15
Peripherally Inserted Central Catheter by Interventional Nephrologists: Experiences from a Single Center
Authors Kim AY, Do JY ![]() , Cho KH, Park JW, Kang SH
, Cho KH, Park JW, Kang SH ![]()
Received 11 February 2022
Accepted for publication 13 May 2022
Published 23 May 2022 Volume 2022:15 Pages 5123—5131
DOI https://doi.org/10.2147/IJGM.S362146
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
A Young Kim, Jun Young Do, Kyu Hyang Cho, Jong Won Park, Seok Hui Kang
Division of Nephrology, Department of Internal Medicine, College of Medicine, Yeungnam University, Daegu, Republic of Korea
Correspondence: Seok Hui Kang, Division of Nephrology, Department of Internal Medicine, College of Medicine, Yeungnam University, Daegu, Republic of Korea, Tel +82-53-620-3836, Fax +82-53-654-8386, Email [email protected]
Purpose: As the number of patients with chronic kidney disease increases, nephrologist activities are gradually expanding. This study evaluated the safety and success of peripherally inserted central catheter (PICC) performed by nephrologists.
Patients and Methods: We retrospectively analyzed the medical records of a medical center. All patients underwent a PICC procedure by two nephrologists. The reasons for catheter removal were classified as accidental removal; treatment termination; catheter occlusion; vessel thrombosis; catheter-related infection, or patient death. Overall catheter complications were defined as catheter occlusion, vessel thrombosis, or catheter-related infection.
Results: A total of 335 catheterizations among 286 patients were performed. Overall, catheter removal was required during follow-up in 251 of 335 cases. The catheter was removed in 48 out of 251 (19.1%) cases with catheter-related complications. In univariate and multivariate analyses, diabetes mellitus was associated with catheter-related infection. The catheter survival rates were 85.3% at 1 month. In univariate and multivariate analyses, diabetes mellitus and fluoroscopy-guided insertion were associated with favorable catheter survival.
Conclusion: The results of our study showed high success and low complication rates for PICC insertion by nephrologists. These findings indicate that interventional nephrologists already skilled in other procedures can expand their field of activity and profit.
Keywords: catheter-related complication, catheter survival, fluoroscopy, interventional nephrology, peripheral inserted central catheter
Introduction
As the number of patients with chronic kidney disease increases, nephrologist activities are gradually expanding. Interventional nephrology has emerged as a subspecialty in nephrology.1 The interventions include kidney biopsy, hemodialysis/peritoneal dialysis catheter insertion, and percutaneous endovascular procedures.1 Previous studies have shown no differences in safety and success when nephrologists perform these procedures.2,3 However, there are limited data on peripherally inserted central catheter (PICC) insertion by nephrologists. While the PICC puncture occurs at a peripheral site, the catheter tip is finally located in the central vein. As life expectancy is increasing, many elderly patients have various comorbidities resulting in poor peripheral vein status. In addition, the number of patients requiring chemotherapeutic agents is increasing. Thus, the number of PICC insertions has been increasing in recent years.4,5 The risk of complications that can occur during procedures, such as pneumothorax or hemothorax is low, and venous access is sustainable.5 PICC insertion is relatively easy and has fewer side effects than central catheter insertion. In addition, interventional nephrologists have experience with ultrasound, fluoroscopy, vein puncture, and safety and success in several interventions. Therefore, interventional nephrologists can also perform PICC insertion. This study evaluated the safety and success of PICC performed by nephrologists.
Patients and Methods
Study Population
We retrospectively analyzed the medical records of a tertiary medical center in Korea. All patients underwent a PICC procedure by two nephrologists between March 2019 and June 2020. Among the patients admitted to the internal medicine of the intensive care unit as well as the general ward, those requiring catheterization were targeted. If catheter insertion was required in each department of internal medicine, the procedure was performed after consultation with the nephrology department. Among 293 patients, 7 in whom catheter insertion failed were excluded. A total of 335 catheterizations among 286 patients were performed and evaluated. This study was approved by the Institutional Review Board of Yeungnam University Hospital (2021-02-029), which waived the requirement for informed consent. Informed consent was not obtained from the patients since the records and information of the participants were anonymized and de-identified prior to the analysis. The study was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Data Collection and Assessments
We collected data on patient age, sex, underlying disease, and reasons for catheter insertion or removal. Underlying comorbidities were evaluated using the age-adjusted Charlson comorbidity index as previously described.6 Renal function at the time of PICC insertion was evaluated based on the estimated glomerular filtration rate (eGFR, mL/min/1.73 m2) using the Chronic Kidney Disease Epidemiology Collaboration equation.7 Chronic kidney disease was defined as an eGFR of <60 mL/min/1.73 m2.8 Dialysis patients were defined as those who underwent maintenance peritoneal dialysis or hemodialysis.
The reasons for catheter removal were classified as accidental removal by problems such as delirium, dementia, or non-cooperation; treatment termination; catheter occlusion; vessel thrombosis; catheter-related infection, or patient death. Overall catheter complications were defined as catheter occlusion, vessel thrombosis, or catheter-related infection. Catheter occlusion was defined as a state in which fluid did not pass through the lumen or blood did not flow back. Vessel thrombus was classified as cases confirmed by vascular ultrasonography or computed tomography. Catheter-related infection was defined as cases in which bacteria were cultured from the blood or skin around the insertion site showing clinical findings, such as redness and tenderness.
Catheter survival duration was defined as the period from the time of PICC insertion to removal. The catheter function was maintained; however, if the patient died or was lost to follow-up, the date were considered the end-point and censored data. If the cause of the catheter removal was accidental removal or treatment termination, the catheter was also considered to be catheter survival until the point of catheter removal.
Methods of Catheter Insertion
The procedure was performed in one of two places, depending on the patient’s general condition. If the patient’s general condition was unstable, such as in an intensive care unit or requiring vasopressor use, the catheter was inserted at the bedside without fluoroscopic guidance. If the patient’s general condition was stable, fluoroscopy was performed in an imaging room. The PICC was usually inserted into the non-dominant arm and the upper arm above the elbow. However, if an appropriate position for the procedure was not established due to surgery or trauma, arm saving was required owing to a history of breast cancer surgery or the need for a fistula, the procedure was performed on the dominant arm. Electrocardiography (ECG) monitoring was maintained, and we checked the location by ultrasound to identify the vessel in which the catheter was inserted. The aseptic procedure included betadine sterilization and cover with a surgical gown. We used a pre-packed Mini Access Kit (Merit Medical Systems, Utah, USA), which contained the introducer needle (21 G, 7 cm), nitinol guidewire (0.46 mm, 40 cm), and coaxial introducer (4 F, 10 cm). Using ultrasound, the introducer needle was inserted into the vessel (basilic, brachial, or cephalic veins), in which the catheter was to be placed. The nitinol guidewire was passed into the needle and the introducer needle was removed. The coaxial introducer was then inserted, the nitinol guidewire was removed, and the syringe was connected to the coaxial introducer. A syringe was used to check the patency. The method was the same whether the procedure is performed in the imaging room or at the bedside. Next, we used a pre-packed PICC kit (Bard, Inc., Salt Lake City, Utah, USA), which included a guidewire (0.018-inch, 135 cm) and the dual lumen catheter (5 F, 55 cm). The guidewire was inserted into the introducer while the fluoroscopy image was checked. The wire was introduced in the direction of the inferior vena cava. An ECG monitor was used to check the direction of the guidewire if the procedure is performed at the bedside. If premature ventricular contraction repeatedly appeared on the ECG monitor, we assumed the guidewire had entered the right atrium or ventricle, and attempted repositioning. After the guidewire was properly inserted, the coaxial introducer was removed and the vessel dilator was inserted. The proper catheter tip position and length were measured at the junction of the superior vena cava and right atrium, and the proper length was checked under fluoroscopy. When performing the procedure at the bedside, we measured the length of the catheter at approximately the 3rd intercostal space through the passage of the vein. We then cut the catheter to fit the length and inserted it along the guidewire. We next removed the dilator sheath and secured the PICC to the arm using StatLock. If the procedure was performed at the bedside, chest radiography was performed to confirm the correct catheter tip position before use. To evaluate whether the PICC insertion was successful, a syringe was connected to its two lumens and regurgitation was checked. It was also evaluated whether the catheter tip was located between the superior vena cava and the middle portion of the right atrium on chest radiography or fluoroscopy.
Statistical Methods
Data were analyzed using IBM SPSS Statistics for Windows, version 25.0 (IBM Corp., Armonk, NY, USA). Categorical data are expressed as counts and percentages, and continuous data are presented as means ± standard deviation. Survival curve analysis was performed using the Kaplan-Meier method. Logistic and Cox regression analyses were used to analyze the risk factors for catheter survival and complications. The multivariate analysis was adjusted for sex, age, diabetes mellitus, hypertension, cancer, chronic kidney disease, use of antiplatelet or anticoagulant agents, insertion site, and use of fluoroscopy. Statistical significance was set at P < 0.05.
Results
Characteristics of the Patients and Procedures
Among 335 cases (293 patients) of catheterization, 328 were successful (97.9%). Among the 7 cases of failure, 4 were due to the patient’s inability to cooperate due to their general condition or underlying disease such as dementia, 2 were due to catheter malposition, and 1 was due to failed venous puncture. The study enrolled a total of 286 patients, with 152 (53.1%) male patients (Table 1). The average patient age was 68.2 ± 14.0 years. The age-adjusted Charlson comorbidity index was 7.5 ± 3.0. Thirty-five (12.2%) patients had chronic kidney disease, 28 of whom did not undergo dialysis and had a short life expectancy to consider arteriovenous fistula due to the exacerbation of underlying diseases such as metastatic cancer or old age. Seven patients had poor vein status and required a venous line for treatment. Among these, four patients required intensive care for severe diseases such as heart failure, peritonitis, and hepatic encephalopathy due to liver cirrhosis. The other three patients required an intravenous infusion of antibiotics owing to severe diabetic foot wounds. The PICCs were inserted, and the patients were discharged without any complications.
 |
Table 1 Characteristics of the Patients and Procedures |
The two main reasons for catheter insertion were the administration of medication such as total parenteral nutrition or antibiotics (241 (87.8%) patients) and the prevention of extravasation during chemotherapy (94 (28.1%) patients). Fluoroscopy was used in 270 (80.6%) cases, while 65 (19.4%) cases did not use fluoroscopy. The catheters were inserted in the right and left arms in 117 (34.9%) and 218 (65.1%) cases, respectively.
Catheter Complications
Overall, catheter removal was required during follow-up in 251 of 335 cases (74.9%). A total of 84 (25.1%) cases had a catheter until the end of follow-up or were lost to follow-up after discharge. The most common cause of catheter removal was death (Table 2). The catheter was removed in 48 out of 251 (19.1%) cases with catheter-related complications. No patients died due to catheter-related complications. Catheter were removed in 29 (11.6%) cases due to infection. Among them, blood culture tests of 17 cases showed no growth, three showed Candida albicans, three showed Staphylococcus epidermis, one showed Staphylococcus aureus, and one showed Staphylococcus capitis. Three cases showed Enterococcus faecium and one showed Pseudomonas aeruginosa. In multivariate analysis, patients with diabetes mellitus had an odds ratio (OR) of 3.32 (95% confidence interval [CI], 1.46–7.56; P = 0.004) for catheter-related infection compared to those without diabetes mellitus (Table 3). A total of 13 (5.2%) cases required catheter removal due to occlusion. In multivariate analysis, female patients had an OR of 4.12 (95% CI, 1.11–15.25; P = 0.034) for catheter occlusion compared to male patients. Six (2.4%) cases required catheter removal for vessel thrombus. There was no significant association between the use of antiplatelet or anticoagulant agents and catheter occlusion or vessel thrombus (P = 0.228 and P = 0.452, respectively).
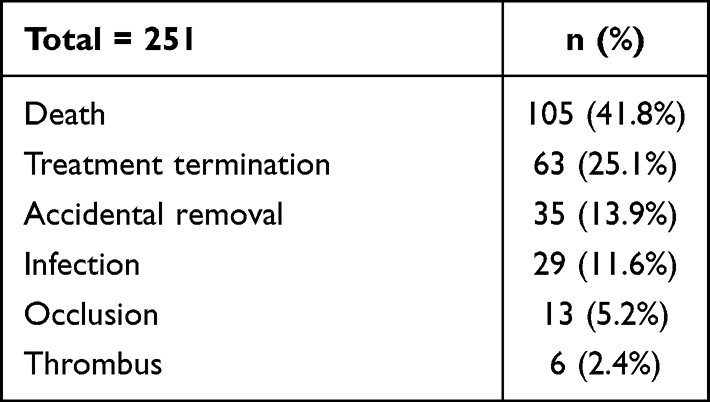 |
Table 2 Causes of Catheter Removal |
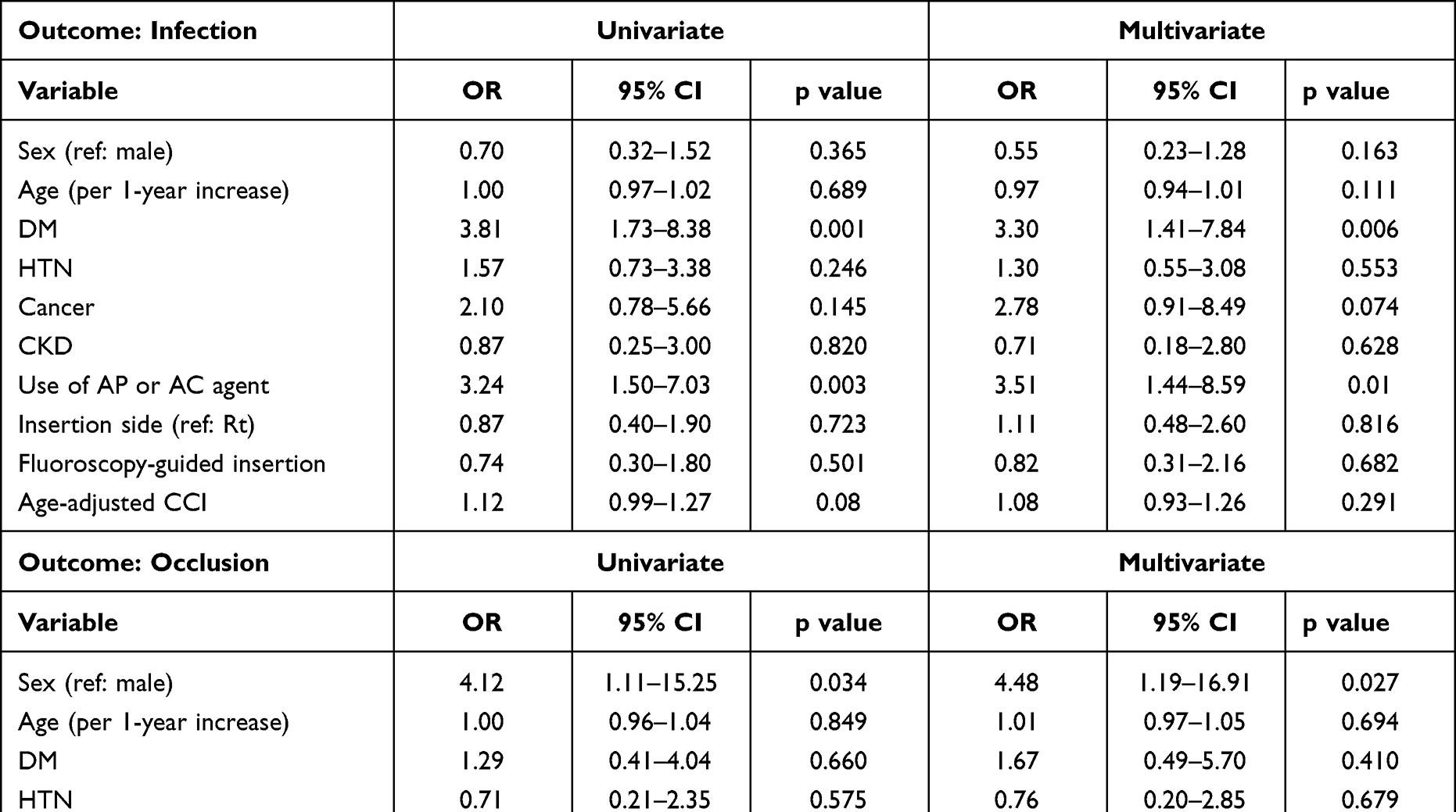 |
Table 3 Logistic Regression Analyses of Factors Contributing to Catheter-Related Complications |
Catheter Survival
The catheter survival rates were 85.3% at 1 month and 76.8% at 3 months. The mean catheter duration was 42.0 ± 51.7 days. There were no significant associations between sex, age, and catheter survival (Table 4). In univariate and multivariate analyses, diabetic patients had hazard ratios (HRs) of 2.54 and 2.48, respectively, compared to non-diabetic patients. Right or left-side catheter location was not significantly associated with catheter survival (multivariate, HR=1.01, 95% CI [0.55–1.86], P = 0.969). Fluoroscopy-guided insertion was associated with favorable catheter survival (multivariate, HR=0.51, 95% CI [0.27–0.98], P = 0.042).
 |
Table 4 Cox Regression Analyses of Factors Contributing Catheter Survival |
Discussion
As interventional nephrology is becoming a subspecialty of nephrology, interventional nephrologists are expanding their field of activity.9 Nephrologists can perform kidney biopsy, insert a dialysis catheter, and perform angioplasty and thrombolysis of grafts and fistulas.9 Previous studies have reported no differences in safety and success when nephrologists perform such procedures.2,3 Beathard et al reported an overall success rate of 94.9% and a major side effect rate of 0.3% for procedures including tunneled catheter insertion, angioplasty, and thrombectomy.9 Interventional nephrologists are familiar with vascular access and anatomy through these procedures. Because PICC is relatively easy and has few side effects, it is more easily accessed.
Cho et al reported a PICC insertion success rate of 93.9–97.6% in 224 cases.10 Their success rate was similar to our results, and they evaluated the outcomes of the same interventional nephrology procedures. However, the primary aim of their study was to compare PICC procedures without versus with fluoroscopy, and there were no data for catheter survival or related factors. Our study differs from the Cho study in that we also examined other factors that could affect catheter survival as well as the place of procedure. Additional data for catheter survival–related factors would help maintain long-term catheter survival.
PICC use has been increasing recently.4,5 It is considered standard care when mid-to-long-term intravenous therapy is required in both the general ward and intensive care units.11 Fluoroscopy and chest radiography are classical methods for determining proper tip navigation and position. Some central catheterizations were performed without fluoroscopy guidance; the procedure is associated with a high rate of catheter malposition. In addition to fluoroscopy, various methods can increase procedural accuracy and success rates. Previous studies demonstrated that ultrasound and intracavitary electrocardiography can be used for tip location and navigation.12,13 The sensitivity and success rate were higher in the group using these devices than in that using anatomical landmarks to confirm the catheter tip location.13 Although these methods completely avoid the need for fluoroscopy and/or chest radiography, these methods can be safe and useful options for assessing PICC at non-applicable status to fluoroscopy or emergency.
Despite the increasing use of PICC and several devices that increase the success rate, there are situations in which the catheter requires removal. The rates of catheter removal due to global complications varied between 15.9% and 40.7%.14–16 In our study, 19.1% of cases required catheter removal due to complications, comparable to the rates reported by previous studies on interventional radiologists.14–16 In the present study, 13.9% of cases removed their catheters by accident, which was the second most common cause of catheter removal. Grua et al reported an accidental catheter removal rate of PICC inserted by a radiologist of 8.9%.17 However, the authors had sutured the PICC to the skin, while we fixed the catheters using a StatLock, which is easier to remove, which may explain our higher rate of accidental catheter removal. However, in terms of skin irritation or reduction of bacterial colonization, StatLock is superior to suturing.18
In our study, the three major causes of catheter removal were patient death, treatment termination, and accidental removal. These can inform some issues for PICC insertion. First, the demand for PICC was largely occupied by patients requiring terminal or palliative care as well as care for acute lesions. PICC insertion as first choice may be advantageous in terms of decreasing patient pain or inconvenience rather than effort to maintain a venous line from a poor peripheral vein. Second, some PICC cases would be required by needed for parenteral nutrition, antibiotics, or the presence of a poor peripheral vein. Timely catheter removal, when not absolutely necessary, would decrease the development of catheter-related complications. Finally, the PICC can be easily removed by spontaneous traction. Clinicians should always provide information to caregivers, nurses, or the patient about the possibility of self-removal and protection against traction.
There was a significant increase in catheter infection in cases of antiplatelet or anticoagulant use. Some studies reported that platelets have a direct effect on the immune system, such as innate and adaptive immunity.19,20 Platelets have protective action against vascular injury, produce antibodies, and release bactericidal agents.21 We cautiously speculated that taking antiplatelets may inhibit the action of platelets and affect catheter infections. However, insufficient studies have been examined the association between catheter infection and these drugs, for which further studies are needed. In previous studies performed by physician and nurse PICC teams, the incidence rates of catheter occlusion were 2.4% to 6%,22,23 compared to the rate in the present study (5.2%). Our study showed a higher OR for catheter occlusion in women than in men. Although not a PICC, several articles have reported a higher proportion of women than men with intravenous catheter occlusion.24,25 Although few studies have reported causes of high catheter occlusion rates in women, we carefully speculate that the sex-based differences in vessel diameter may affect the results. However, the issue is beyond the scope of our study; thus, further studies of sex-based differences in catheter occlusion would be interesting.
In other studies, the catheter-related infection rates ranged from 5.7% to 20%,15,16,26 compared to 11.6% in our study. Bacteria were not cultured from the blood of 17 of 29 cases. Local infection does not necessarily indicate a systemic infection.27 If fever occurs, the catheter is often removed preemptively. A reported 80–90% of causes of fever are non-catheter-related, and we determined that the culture rate was low due to these factors.28 There is a significant correlation between catheter-related infections and diabetes mellitus. Zhang et al reported that diabetes mellitus was a risk factor for PICC-related infections among patients in the intensive care unit.29 In terms of catheter survival, were observed a significant difference between the diabetic and non-diabetic groups of cases. We also observed a significant relationship between diabetes and catheter-related infection, which also likely affected catheter survival. While studies have shown that diabetes mellitus increases the risk of infection with certain pathogens or specific disease groups, evidence to support the assumption that diabetes mellitus increases the risk of infection is lacking.30 Therefore, further research is needed on the direct correlation between diabetes mellitus, PICC-related infection, and catheter survival.
Among the complications, nephrologists should pay attention to thrombosis or vessel injury. In our study, the incidence of thrombosis was 2.4%, while other studies reported rate ranging from 1.5% to 4.5%.15,17 Marnejon et al reported that vessel thrombosis occurs more than two-fold more often in patients with chronic kidney disease than in patients with normal kidney function.31 El Ters et al reported significantly reduced arteriovenous fistula function in patients with previous PICC insertion.32 Due to immaturity of the arteriovenous fistula, the Nephrology Society discourages PICC insertion in patients with chronic kidney disease.33 Chronic kidney disease is a risk factor for central catheter-related complications or poor catheter survival, but our results showed a non-association between chronic kidney disease and catheter survival or complications. Thus, we inserted a PICC only after considering a patient’s situation, which may have influenced the results. Furthermore, we removed the PICC when it was not absolutely necessary. When patients are properly selected by a nephrologist, procedures can be performed safely and without delay in those who need it. Nevertheless, our study findings should not be interpreted as PICC implantation in chronic kidney disease patients being safe in all cases. Shingarev et al suggested including a nephrologist in the decision-making process before PICC insertion in a patient with chronic kidney disease.33 PICC performed by an intervention nephrologist may decrease this unnecessary process and prevent delay in performing the procedure.
PICC procedures can expand the field of nephrologist’s activities and generate revenue. We anticipate profits at no additional cost if fluoroscopy or ultrasound is already available. If the procedure is performed using fluoroscopy, in Korea, the profit, excluding the material cost, is $209 per case. Without fluoroscopy, the profit is $115 per case. The annual revenue in our center was approximately $53,827.
Our study has several limitations. First, the sample size was relatively small, and this was a single-center study. Second, the rate of catheter removal due to patient death was high, which may limit data interpretation. In addition, further research may be needed if there are differences in the incidence of catheter-related complications and catheter survival depending on the vessel.
Conclusion
The results of our study showed high success and low complication rates for PICC insertion by nephrologists. These findings indicate that interventional nephrologists already skilled in other procedures can expand their field of activity and profit.
Funding
This work was supported by the Medical Research Center Program (2015R1A5A2009124) through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT and Future Planning.
Disclosure
The authors report no conflict of interest in this work.
References
1. Efstratiadis G, Platsas I, Koukoudis P, Vergoulas G. Interventional nephrology: a new subspecialty of nephrology. Hippokratia. 2007;11:22–24.
2. Brescia M, Cimino J, Appel K, Hurwich B. Chronic hemodialysis using venipuncture and a surgically created arteriovenous fistula. N Engl J Med. 1966;275(20):1089–1092. doi:10.1056/NEJM196611172752002
3. Asif A, Merrill D, Brouwer D, Roth D, Ash S. Procedural nephrology: changing the face of renal disease care. Dial Transplant. 2004;33:258–260.
4. Gibson C, Connolly BL, Moineddin R, Mahant S, Filipescu D, Amaral JG. Peripherally inserted central catheters: use at a tertiary care pediatric center. J Vasc Interv Radiol. 2013;24:1323–1331. doi:10.1016/j.jvir.2013.04.010
5. Vineet C, David R, Latoya K, Tracy L, Carol C, Sarah K. PICC-associated bloodstream infections: prevalence, Patterns, and Predictors. Am J Med. 2014;127:319–328. doi:10.1016/j.amjmed.2014.01.001
6. Frenkel WJ, Jongerius EJ, Mandjes-van Uitert MJ, van Munster BC, de Rooij SE. Validation of the Charlson Comorbidity Index in acutely hospitalized elderly adults: a prospective cohort study. J Am Geriatr Soc. 2014;62:342–346. doi:10.1111/jgs.12635
7. Matsushita K, Mahmoodi BK, Woodward M, et al. Comparison of risk prediction using the CKD-EPI equation and the MDRD study equation for estimated glomerular filtration rate. JAMA. 2012;307:1941–1951. doi:10.1001/jama.2012.3954
8. Levey AS, Eckardt KU, Tsukamoto Y, et al. Definition and classification of chronic kidney disease: a position statement from kidney disease: improving Global Outcomes (KDIGO). Kidney Int. 2005;67:2089–2100. doi:10.1111/j.1523-1755.2005.00365.x
9. Beathard GA, Litchfield T. Physician operators forum of RMS Lifeline, Inc. Effectiveness and safety of dialysis vascular access procedures performed by interventional nephrologists. Kidney Int. 2004;66:1622–1632. doi:10.1111/j.1523-1755.2004.00928.x
10. Cho S. Peripherally inserted central catheter procedure at the bedside by a nephrologist is safe and successful. Kidney Res Clin Pract. 2021;40:153–161. doi:10.23876/j.krcp.20.119
11. Loewenthal MR, Dobson PM, Starkey RE, Dagg SA, Petersen A, Boyle MJ. The peripherally inserted central catheter (PICC): a prospective study of its natural history after cubital fossa insertion. Anaesth Intensive Care. 2002;30:21–24. doi:10.1177/0310057X0203000103
12. Greca A, Lacobone E, Elisei D, et al. ECHOTIP: a structured protocol for ultrasound-based tip navigation and tip location during placement of central venous access devices in adult patients. J Vasc Access;2021. 11297298211044325. doi:10.1177/11297298211044325
13. Yin YX, Gao W, Li WY, et al. Insertion of peripherally inserted central catheters with intracavitary electrocardiogram guidance: a randomized multicenter study in China. J Vasc Access. 2019;20:524–529. doi:10.1177/1129729818819732
14. Vidal V, Muller C, Jacquier A, et al. Prospective evaluation of PICC line related complications. J Radiol. 2008;89:495–498. doi:10.1016/S0221-0363(08)71453-7
15. Yap YS, Karapetis C, Lerose S, Iyer S, Koczwara B. Reducing the risk of peripherally inserted central catheter line complications in the oncology setting. Eur J Cancer Care. 2006;15:342–347. doi:10.1111/j.1365-2354.2006.00664.x
16. Leroyer C, Lashéras A, Marie V, et al. Prospective follow-up of complications related to peripherally inserted central catheters. Med Mal Infect. 2013;43(8):350–355. doi:10.1016/j.medmal.2013.06.013
17. Grau D, Clarivet B, Lotthé A, Bommart S, Parer S. Complications with peripherally inserted central catheters (PICCs) used in hospitalized patients and outpatients: a prospective cohort study. Antimicrob Resist Infect Control. 2017;6(1):18. doi:10.1186/s13756-016-0161-0
18. Yamamoto AJ, Solomon JA, Soulen MC, et al. Sutureless securement device reduces complications of peripherally inserted central venous catheters. J Vasc Interv Radiol. 2002;13(1):77–81. doi:10.1016/S1051-0443(07)60012-8
19. Zarbock A, Polanowska-Grabowska RK, Ley K. Platelet-neutrophil-interactions: linking hemostasis and inflammation. Blood Rev. 2007;21(2):99–111. doi:10.1016/j.blre.2006.06.001
20. Elzey BD, Sprague DL, Ratliff TL. The emerging role of platelets in adaptive immunity. Cell Immunol. 2005;238(1):1–9. doi:10.1016/j.cellimm.2005.12.005
21. Blasco-Colmenares E, Perl TM, Guallar E, et al. Aspirin plus clopidogrel and risk of infection after coronary artery bypass surgery. Arch Intern Med. 2009;169(8):788–796. doi:10.1001/archinternmed.2009.42
22. Valbousquet Schneider L Jr, Duron S, Arnaud FX, et al. Evaluation of PICC complications in orthopedic inpatients with bone infection for long-term intravenous antibiotics therapy. J Vasc Access. 2015;16:299–308. doi:10.5301/jva.5000389
23. Bertoglio S, Faccini B, Lalli L, Cafiero F, Bruzzi P. Peripherally inserted central catheters (PICCs) in cancer patients under chemotherapy: a prospective study on the incidence of complications and overall failures. J Surg Oncol. 2016;113:708–714. doi:10.1002/jso.24220
24. Wallis MC, McGrail M, Webster J, et al. Risk factors for peripheral intravenous catheter failure: a multivariate analysis of data from a randomized controlled trial. Infect Control Hosp Epidemiol. 2014;35(1):63–68. doi:10.1086/674398
25. Abolfotouh MA, Salam M, Ala’a Bani Mustafa DW, Balkhy HH, Balkhy H. Prospective study of incidence and predictors of peripheral intravenous catheter-induced complications. Ther Clin Risk Manag. 2014;10:993–1001. doi:10.2147/TCRM.S74685
26. Smith JR, Friedell ML, Cheatham ML, Martin SP, Cohen MJ, Horowitz JD. Peripherally inserted central catheters revisited. Am J Surg. 1998;176:208–211. doi:10.1016/S0002-9610(98)00121-4
27. Mermel LA, Farr BM, Sherertz RJ, et al. Guidelines for the management of intravascular catheter related infections. Clin Infect Dis. 2001;32:1249–1272. doi:10.1086/320001
28. Ryan JA Jr, Abel RM, Abbott WM, et al. Catheter complications in total parenteral nutrition: a prospective study of 200 consecutive patients. N Engl J Med. 1974;290:757–761. doi:10.1056/NEJM197404042901401
29. Zhang S, Sun X, Lei Y. The microbiological characteristics and risk factors for PICC-related bloodstream infections in intensive care unit. Sci Rep. 2017;7:15074. doi:10.1038/s41598-017-10037-2
30. Jackson LA. Evaluating diabetes mellitus as risk factor for community acquired infections. Clin Infect Dis. 2005;41:289–290.
31. Marnejon T, Angelo D, Abu Abdou A, Gemmel D. Risk factors for upper extremity venous thrombosis associated with peripherally inserted central venous catheters. J Vasc Access. 2012;13:231–238. doi:10.5301/jva.5000039
32. El Ters M, Schears GJ, Taler SJ, et al. Association between prior peripherally inserted central catheters and lack of functioning arteriovenous fistulas: a case-control study in hemodialysis patients. Am J Kidney Dis. 2012;60:601–608.
33. Shingarev R, Allon M. Peripherally inserted central catheters and other intravascular devices: how safe are they for hemodialysis patients? Am J Kidney Dis. 2012;60:510–513. doi:10.1053/j.ajkd.2012.07.003
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.