Back to Journals » Neuropsychiatric Disease and Treatment » Volume 22
Peripheral Nerve Conduction in Alzheimer’s vs. Late-Life Depression: A Comparative Study
Authors Li X, Zhao X, Huang Y, Tang J
Received 26 March 2026
Accepted for publication 21 May 2026
Published 4 June 2026 Volume 2026:22 611214
DOI https://doi.org/10.2147/NDT.S611214
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rakesh Kumar
Xiaojuan Li,1,* Xing Zhao,2,* Yongpan Huang,3 Jiayu Tang1
1Department of Neurology, Brain Hospital of Hunan Province (The Second People’s Hospital of Hunan Province), Changsha, Hunan, 410007, People’s Republic of China; 2Department of Rehabilitation, Changsha Central Hospital, Changsha, Hunan, People’s Republic of China; 3Medicine School, Changsha Social Work College, Changsha, Hunan, 410004, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yongpan Huang, Medicine School, Changsha Social Work College, Changsha, Hunan, 410004, People’s Republic of China, Email [email protected]
Background: Alzheimer’s disease (AD) and late-life depression (LLD) patients both exhibit peripheral motor nerve conduction impairments, but with distinct patterns, highlighting divergent neurophysiological mechanisms in these aging-related disorders.
Objective: To compare peripheral nerve conduction function among normal cognition (NC), older adults with AD, and LLD.
Methods: All the participants were enrolled and assigned to AD, LLD and aged-matched NC controls (all ≥ 60 years, n=60, respectively). Sensory conduction of the median and sural nerves, and motor conduction of the median and common peroneal nerves, were assessed. Key parameters included latency, amplitude, and conduction velocity. Group differences were analyzed after adjusting for gender, age, education, height, and comorbid medical conditions.
Results: By controlling gender, age, height, education level, and somatic diseases with inter-group differences, compared with NC group, the median nerve motor conduction in AD group showed prolonged proximal latency (3.21 vs. 3.65 ms, P=0.023), reduced amplitude (proximal: 7.30± 2.02 vs. 3.89± 0.57 mV; distal: 6.13± 2.17 vs. 4.12± 2.38 mV, both P< 0.001), and slowed conduction velocity (56.46± 5.18 vs. 49.29± 6.27 m/s, P=0.002). LLD group exhibited more pronounced latency prolongation (proximal: 3.21 vs. 4.06 ms; distal: 7.18 vs. 7.98 ms, both P< 0.001) and greater amplitude reduction (proximal: 7.30± 2.02 vs. 3.65± 0.66 mV; distal: 6.13± 2.17 vs. 3.18± 1.88 mV, both P< 0.001). In terms of the common peroneal nerve motor conduction, function AD group had significantly slower conduction velocity (48.88± 5.82 vs. 42.85± 5.27 m/s, P=0.033). LLD group showed prolonged proximal latency (4.25 vs. 5.77 ms, P< 0.001). No significant differences were found in sensory conduction parameters across groups after adjustment.
Conclusion: Both AD and LLD groups were associated with peripheral motor neuropathy, but the pattern of impairment differs. AD is marked by generalized conduction slowing, while LLD shows more severe latency delays and amplitude loss, suggesting distinct pathophysiological pathways. These findings provide new insights into the peripheral nervous system’s involvement in age-related neurocognitive and mood disorders.
Keywords: nerve motor conduction, nerve sensory conduction, nerve conduction velocity, late-life depressive disorder, Alzheimer’s disease
Introduction
Alzheimer’s disease (AD) and late-life depression (LLD) are two major neuropsychiatric disorders in the elderly, with increasing prevalence amid global population aging.1,2 AD, the most common neurodegenerative disease, is characterized by progressive cognitive decline and memory impairment, severely affecting patients’ daily functioning and imposing substantial socioeconomic burdens.3,4 LLD, a prevalent mood disorder among older adults, manifests as persistent low mood, anhedonia, and sleep disturbances, and is associated with cognitive deterioration and multiple adverse health outcomes.5,6 Recent study highlights a complex interplay between AD and LLD, exhibiting LLD often presents with cognitive deficits, with some cases progressing to AD, while depressive symptoms are common in AD, may act as early markers or comorbid conditions.7 However, these underlying neurobiological mechanisms differ, AD is defined by neuronal loss, β-amyloid plaques, and neurofibrillary tangles, whereas LLD involves neurotransmitter imbalances, neuroendocrine dysregulation, and impaired neuroplasticity.8
Peripheral nerve dysfunction has been observed in both conditions. Electrophysiological studies consistently demonstrate impaired motor nerve conduction velocity and reduced sensory nerve action potential amplitude in AD patients, suggesting that peripheral nervous system abnormalities are integral to the disease’s pathogenesis.9,10 A parallel exists in diabetic neuropathy (DN), a common complication of diabetes mellitus where peripheral nerve impairment directly results from metabolic disturbances like chronic hyperglycemia, dyslipidemia, and oxidative stress. Similar to the AD-LLD link, studies show a strong correlation between peripheral nerve impairment in DN and the emergence of depressive symptoms, establishing a direct and clinically relevant link between somatic nerve damage and mood disturbance.11 This hints at a plausible mechanistic link to LLD that may involve shared pathways of systemic inflammation, oxidative stress, or neuroendocrine disruption. Notably, however, no systematic investigation has yet compared peripheral nerve conduction profiles between AD and LLD cohorts. This study hypothesizes that although AD, LLD, and conditions like diabetic neuropathy may all impair peripheral nerve function, the patterns and electrophysiological signatures of motor and sensory deficits differ based on their distinct etiologies. By comprehensively comparing detailed neurophysiological parameters, including motor conduction velocity and sensory wave amplitude, among AD patients, LLD patients, patients with diabetic neuropathy and depression, and cognitively healthy older adults, this study aims to identify these distinct neuroconduction profiles. This will help clarify their underlying pathophysiological mechanisms and, crucially, provide actionable insights for improved differential clinical diagnosis and the development of more targeted, mechanism-based interventions that address both neurological and psychiatric dimensions, ultimately aiming for greater therapeutic impact.
Subjects
A total of 60 patients with AD and 60 patients with LLD were consecutively recruited from the outpatient clinics and inpatient wards of the Department of Neurology and Department of Psychiatry at Brain Hospital of Hunan Province (The Second People’s Hospital of Hunan Province) between June 2024 and June 2025. Meanwhile, 60 cognitively normal elderly individuals were enrolled as the control group during the same period, who underwent routine health check-ups at the hospital’s Health Management Center. All participants were strictly screened based on predefined inclusion and exclusion criteria to ensure the homogeneity of the study cohorts. The study protocol was reviewed and approved by the Medical Ethics Committee of Hunan Brain Hospital (Approval No. [2025K002]) and Geriatric Friendly Hospital (2024001), and written informed consent was obtained from each participant or their legal guardian prior to any study-related procedures (Due to the partial learning and memory deficits of some participants, they required the presence of a legal guardian to participate in this study).
Inclusion Criteria for AD Group
Both sexes were eligible, with age ≥60 years. Diagnosis of AD according to the International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10), confirmed by a three-tier clinical review. Eligibility criteria included meeting the diagnostic criteria for AD as specified in the Chinese Guidelines for the Diagnosis and Treatment of Alzheimer’s Disease Dementia (2020 Edition), a Mini-Mental State Examination score ranging from 10 to 24, and evidence of hippocampal atrophy or temporoparietal hypometabolism confirmed by cranial MRI or CT. Ability to comply with study procedures and neurophysiological testing.
Exclusion Criteria for AD Group
History of Parkinson’s disease, essential tremor, peripheral neuropathy, bilateral carpal tunnel syndrome, or metabolic disorders including diabetes (HbA1c≥6.5%), hyperthyroidism, or hypothyroidism; Significant comorbidities involving the cardiovascular, pulmonary, hepatic, renal, or hematopoietic systems; History of organic brain disease, traumatic brain injury, or craniotomy; Coexisting psychiatric disorders, substance abuse, intoxication, or genetic diseases; Positive findings on neurological examination (including abnormalities in light touch, pain/temperature sensation, proprioception, or deep tendon reflexes in all four limbs); Inability to complete the study protocol or adhere to study requirements. A total of 60 AD patients were enrolled.
Inclusion Criteria for LLD Group
Both sexes were eligible, with age ≥65 years. Diagnosis of major depressive disorder according to ICD-10, confirmed by a three-tier clinical review. Meeting the diagnostic criteria for depressive episode or recurrent depressive disorder per ICD-10; voluntary participation with written informed consent from the subject or legal guardian. Ability to comply with study procedures and neurophysiological testing.
Exclusion Criteria for LLD Group
Identical to those applied to the AD group. A total of 60 LLD patients were enrolled.
Inclusion Criteria for NC Group
Matched for sex and age with the AD and LLD groups; Confirmed normal cognitive function based on standardized neuropsychological assessment; Ability to comply with study procedures and neurophysiological testing.
Exclusion Criteria for NC Group
Identical to those applied to the AD group. A total of 60 cognitively normal elderly individuals were enrolled.
This study was approved by the Medical Ethics Committee of Hunan Brain Hospital (Approval No. [2025K002]). Written informed consent was obtained from all participants or their legally authorized representatives prior to enrollment.
Methods
General Demographic and Clinical Information
General demographic information, including sex, age, and years of education, was collected. Clinical information included physical comorbidities (hypertension, heart disease, hyperlipidemia, cerebral infarction), height, and body mass index (BMI). Data for the AD and LLD groups were extracted from inpatient medical records, while data for the NC group were obtained from a health examination cohort of cognitively normal older adults at our hospital’s health examination center.
Neurophysiological Testing
Neuroconduction studies were performed by trained resident physicians blinded to diagnostic group assignments, using a NicoletTM EDX electromyography/nerve conduction system. Sensory nerve conduction was assessed in the median nerve (upper limb) and sural nerve (lower limb); motor nerve conduction was assessed in the median nerve (upper limb) and common peroneal nerve (lower limb). Testing for AD and LLD groups was conducted in hospital wards, while data for NC group were retrieved from a pre-existing cohort database; all three groups followed identical procedural protocols. Prior to testing, the dominant hand side was evaluated; if contraindications such as history of fracture, carpal tunnel syndrome, or other unsuitable conditions were present on the dominant side, the contralateral limb was tested instead. During testing, participants were positioned supine in a room maintained at 22–24°C, with skin temperature stabilized at approximately 32–34°C. Recording, reference, and stimulating electrodes were placed along the standardized surface anatomical pathways of the target nerves. A rectangular electrical stimulus of 0.1 ms duration was applied, with intensity gradually increased from 10 mA in incremental steps, not exceeding 30 mA.
For sensory conduction, compound action potentials were averaged across successive stimuli until the mean amplitude plateaued or the participant reported intolerance to stimulation. For motor conduction, stimulation of the median nerve elicited thumb flexion, and stimulation of the common peroneal nerve elicited great toe dorsiflexion; recordings were terminated when the single evoked action potential amplitude stabilized or intolerance occurred. Latency, amplitude, and conduction velocity were recorded for all nerves (Figure 1).
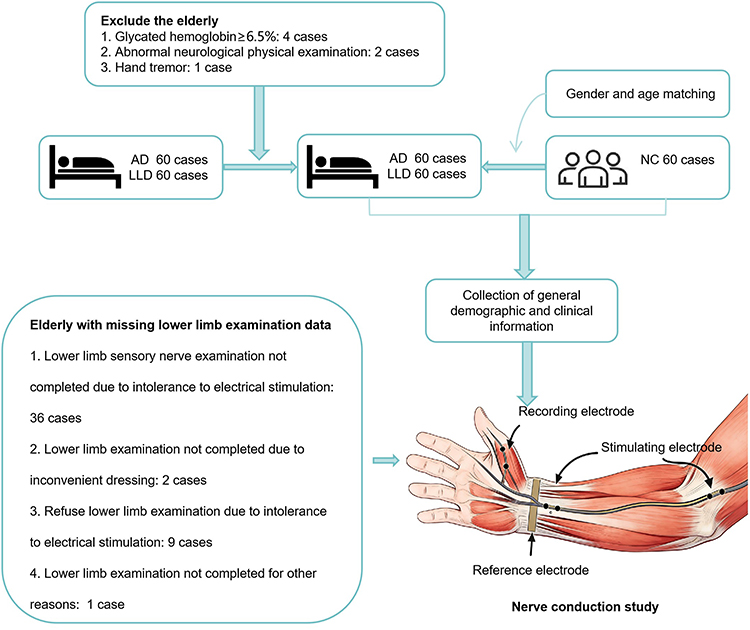 |
Figure 1 Flow chart of the study (using median nerve motor conduction as an example). |
Statistical Analysis
Data were analyzed using SPSS 26.0 (IBM Corp., Armonk, NY, USA). Categorical variables such as sex and history of chronic diseases were described using frequency (percentage), and intergroup comparisons were performed using the χ2-test or Fisher’s exact test. Normality was assessed using the Kolmogorov–Smirnov test. Normally distributed continuous variables, such as BMI and nerve conduction velocities, were expressed as mean ± standard deviation, and intergroup comparisons were conducted using one-way ANOVA, with post hoc pairwise comparisons performed using the Bonferroni correction. In cases of heterogeneity of variance, Welch’s test and Games-Howell post hoc test were applied. Non-normally distributed continuous variables, including age, years of education, height, sensory nerve conduction latency, and amplitude, were presented as median, and intergroup differences were examined using the Kruskal–Wallis H-test, followed by Bonferroni-corrected pairwise comparisons. To account for potential confounding factors that might influence intergroup comparisons of nerve conduction function, a two-step analysis of covariance (ANCOVA) was further conducted: Model 1 adjusted for sex, age, years of education, and height as covariates; Model 2 further adjusted for hypertension, hyperlipidemia, heart disease, and cerebral infarction in addition to Model 1. Post hoc comparisons for both ANCOVA models were performed using the Bonferroni correction. The significance level was set at α = 0.05, and two-tailed tests were used.
Results
Demographic and Clinical Profiles in AD and LLD
To identify the balance or differences in key variables between study groups, thereby providing a basis for subsequent analysis. As shown in Table 1, the results indicated that no statistically significant differences were observed among AD, LLD, and NC groups in terms of sex (χ2=3.086, P=0.195), age (H=3.075, P=0.186), years of education (H=1.361, P=0.513) or body mass index (BMI) (F=2.010, P=0.141). However, a statistically significant difference in height was detected among the three groups (H=10.791, P=0.004), with AD group exhibiting greater height than both LLD group and NC group. Regarding comorbidities, significant intergroup differences were found for hypertension (χ2=11.035, P=0.002), hyperlipidemia (χ2=23.455, P=0.001), and cerebral infarction (χ2=7.161, P=0.025).
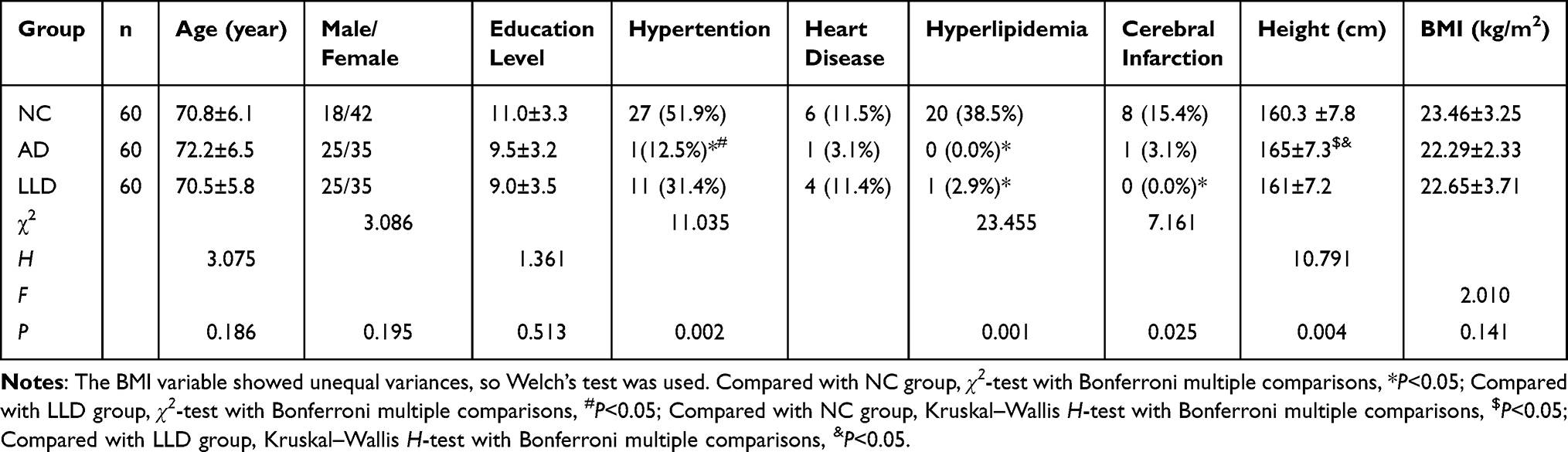 |
Table 1 The Demographic and Clinical Data in Participants |
Altered Peripheral Sural Nerve Sensory Conduction Profiles in AD Versus LLD
To investigate the characteristics of sensory nerve conduction differences between patients with AD and LLD, this study sequentially examined the basic features of sural nerve sensory conduction. As shown in Table 2, the results exhibited that among sensory nerve conduction indices, a statistically significant difference was observed in the latency of the sural nerve across the three groups (H=11.366, P=0.015). Specifically, AD group showed prolonged latency compared to both NC group and LLD group, while no significant difference was found between NC and LLD groups. No other nerve conduction measures showed significant differences between groups (P>0.05).
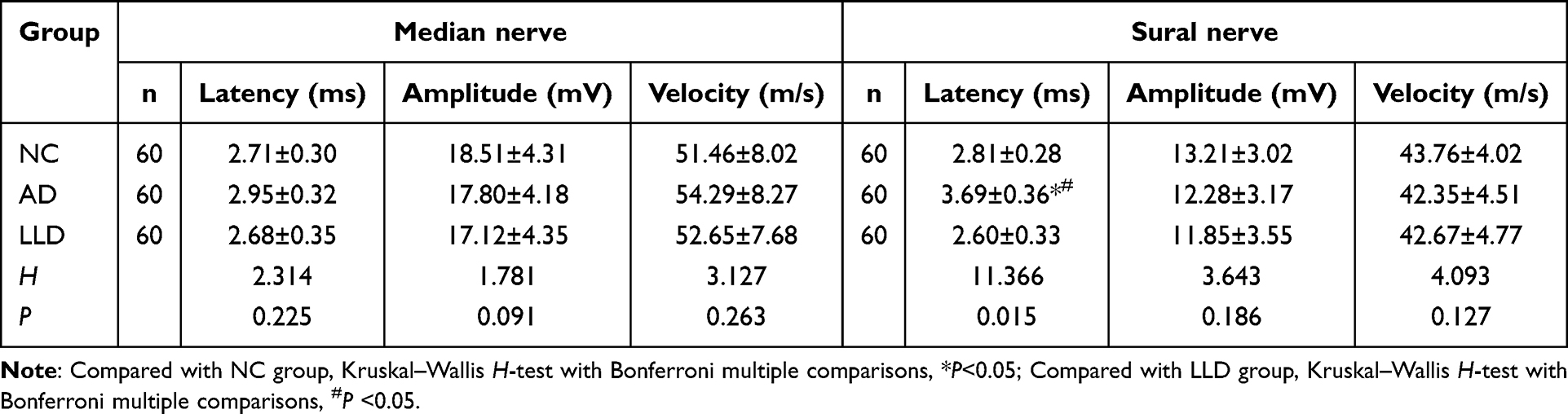 |
Table 2 Comparison of Peripheral Sensory Nerve Conduction Test Results Among the Three Participant Groups |
Altered Peripheral Median and Common Peroneal Nerve Motor Profiles in AD versus LLD
To investigate the characteristics of motor nerve conduction differences between patients with AD and LLD, this study sequentially examined the basic features of median and common peroneal nerve motor conduction. As shown in Table 3, the results indicated that significant intergroup differences were observed among AD, LLD, and NC groups in median nerve motor conduction latency, amplitude, and conduction velocity. Compared with NC group, both AD and LLD groups exhibited prolonged proximal and distal latencies (proximal: F=26.729, P=0.023; distal: F=15.106, P=0.001), as well as reduced amplitudes at both proximal and distal sites (proximal: F=23.716, P=0.001; distal: F=13.826, P=0.001). However, no statistically significant differences were found between AD and LLD groups in latency or amplitude (P<0.001). AD group showed significantly slower conduction velocity than NC group (F=6.862, P=0.002), but no significant difference was observed between AD and LLD groups (P<0.001). Additionally, there was no significant difference in conduction velocity between LLD and NC groups (Table 3).
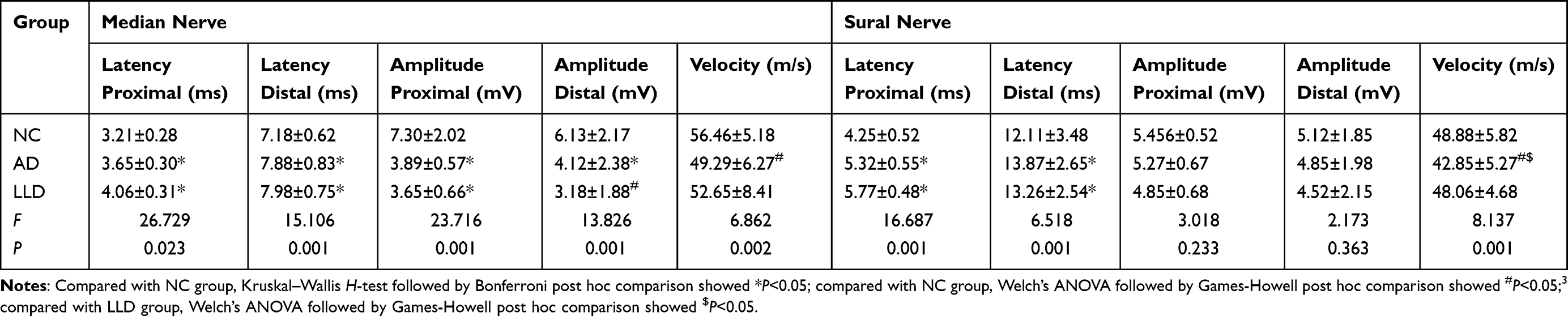 |
Table 3 Comparison of Peripheral Motor Nerve Conduction and Sural Nerve Conduction Detection Among the Three Groups |
Furthermore, we investigated the characteristics of common peroneal nerve motor conduction and found that common peroneal nerve motor conduction latency (proximal: F=16.687, P=0.001; distal: F=6.518, P=0.001) and conduction velocity (F=8.137, P<0.001), but not in amplitude (proximal: F=3.018, P=0.233; distal: F=2.173, P=0.363), there exhibited significant differences among the three groups compared with NC group, both AD and LLD groups had longer proximal and distal latencies. No significant difference was observed between AD and LLD groups in either proximal or distal latency. AD group exhibited significantly slower conduction velocity (F=8.137, P<0.001) than both NC group and LLD group, whereas no significant difference was found between NC and LLD groups (P>0.05) (Table 3).
Confounding Effects on the Intergroup Comparison of Nerve Conduction Function in AD and LLD
We established Model 1 with gender, age, years of education, and height as covariates to analyze median nerve motor conduction, adjusting for potential inter-group confounding factors. As presented in Table 4, the findings of Model 1 for median nerve motor conduction revealed statistically significant inter-group differences in latency (proximal: F=14.537, P<0.001; distal: F=7.481, P<0.001), amplitude (proximal: F=25.613, P<0.001; distal: F=14.235, P<0.001), and conduction velocity (F=4.826, P=0.016). When compared with NC group, both AD and LLD groups showed prolonged proximal latency (P<0.001) and reduced amplitudes at both proximal and distal sites (proximal: F=25.613, P=0.001; distal: F=14.235, P<0.001). LLD group exhibited prolonged distal latency relative to NC group (P<0.001), while no such significant difference was detected between AD and NC groups. Additionally, AD group had slower conduction velocity than NC group (F=4.826, P=0.016), yet no significant difference was observed between LLD and NC groups. Notably, no statistically significant differences were identified between AD and LLD groups across all measured parameters.
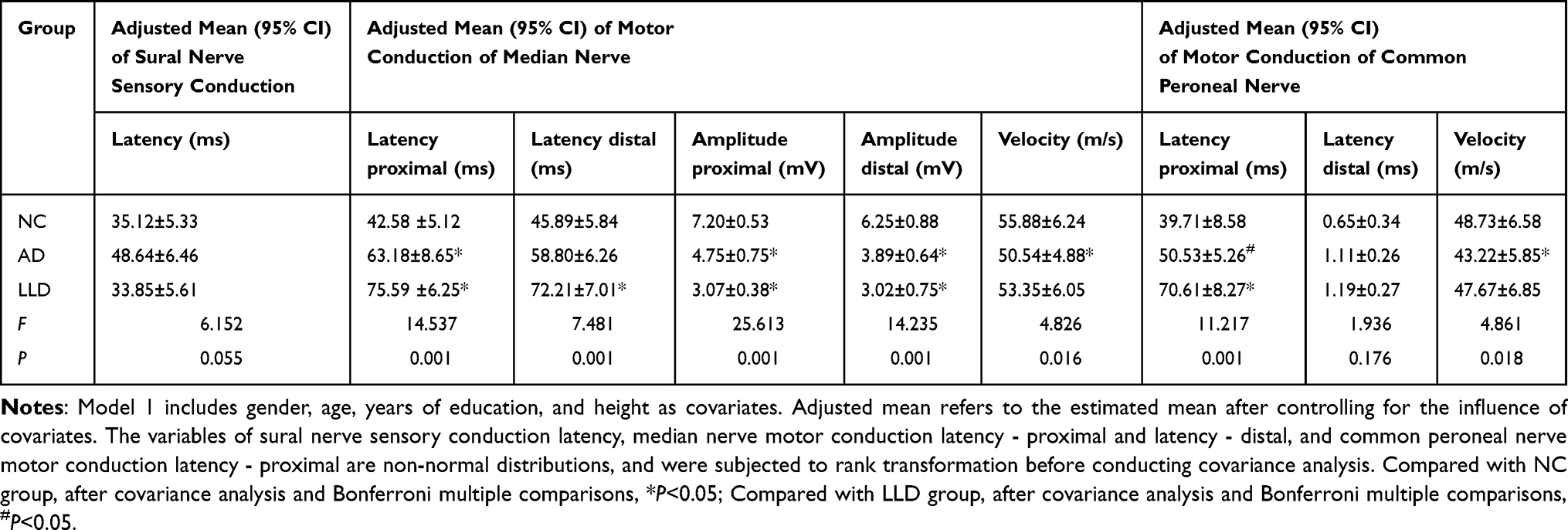 |
Table 4 ANCOVA Analysis in Sural Nerve Sensory Conduction, Median Nerve Motor Conduction and Common Peroneal Nerve Conduction Among Groups - Model 1 |
For common peroneal nerve motor conduction, significant inter-group differences were found in proximal latency (proximal: F=11.217, P<0.001) and conduction velocity (F=4.861, P=0.018), whereas no significant difference emerged in distal latency (F=1.936, P=0.176). Specifically, LLD group had significantly longer proximal latency than both NC (P<0.001) and AD groups (P=0.035), while no significant difference was seen between AD and NC groups (P=0.387). The AD group demonstrated slower conduction velocity compared with NC group (P=0.018), yet no significant difference was found between LLD and NC groups (P>0.05).
Building on Model 1, we developed Model 2 by further adjusting for hypertension, hyperlipidemia, heart disease, and cerebral infarction to assess motor nerve conduction in the median and common peroneal nerves, with Bonferroni correction applied for post-hoc multiple comparisons. As outlined in Table 5, Model 2’s analysis of median nerve motor conduction revealed statistically significant inter-group differences in latency (proximal: F=12.261, P=0.022; distal: F=6.911, P=0.002), amplitude (proximal: F=22.218, P<0.001; distal: F=14.861, P<0.001), and conduction velocity (F=6.210, P=0.002). Relative to NC group, both AD and LLD groups exhibited prolonged proximal latency and reduced amplitudes at both proximal and distal sites. LLD group also showed prolonged distal latency compared with NC group (P<0.001), while no such significant difference was detected between AD and NC groups. Additionally, AD group demonstrated significantly slower conduction velocity than NC group, yet no significant difference was observed between LLD and NC groups. Notably, no statistically significant differences were identified between AD and LLD groups across all measured parameters.
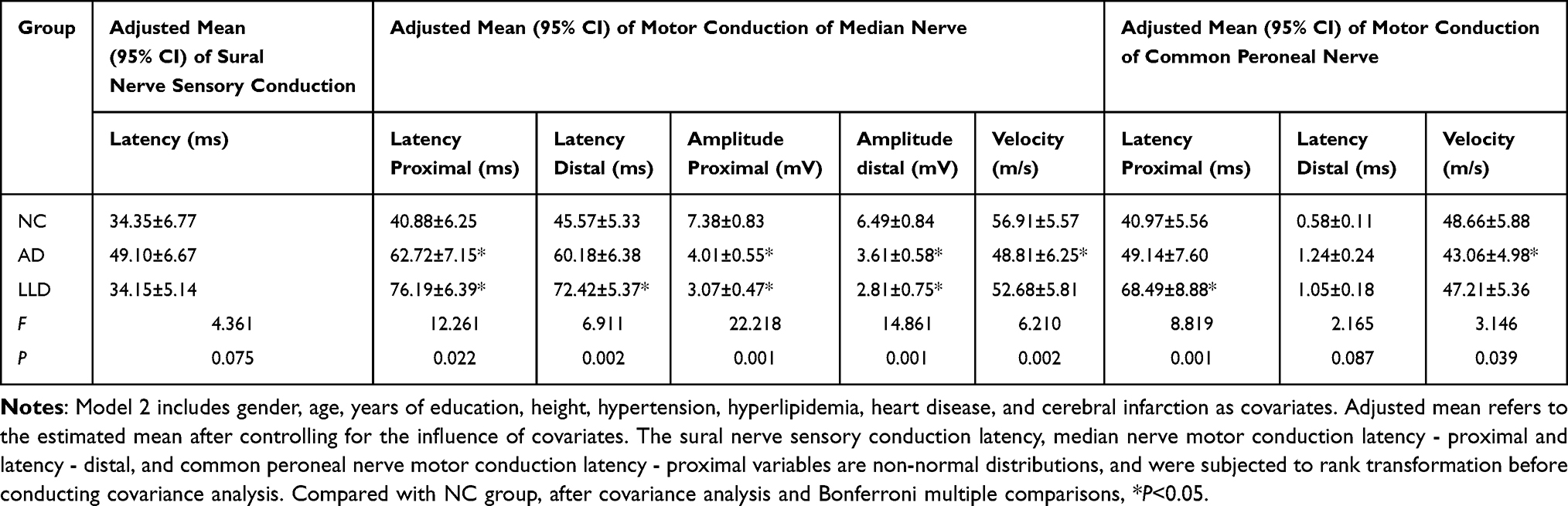 |
Table 5 ANCOVA Analysis in Sural Nerve Sensory Conduction, Median Nerve Motor Conduction and Common Peroneal Nerve Conduction Among Groups- Model 2 |
For common peroneal nerve motor conduction under Model 2, significant inter-group differences were found in proximal latency (proximal: F=8.819, P<0.001) and conduction velocity (F=3.146, P=0.039), whereas no significant difference emerged in distal latency (F=2.165, P=0.087). Specifically, LLD group had significantly longer proximal latency than NC group (P<0.001), while no significant difference was seen between AD and NC groups (P=0.863). AD group exhibited slower conduction velocity compared to NC group (P=0.028), yet no significant differences were detected between LLD and NC groups, or between AD and LLD groups, across any of the measured parameters (P>0.05).
Discussion
Present study focuses on peripheral nerve conduction function, and preliminarily reveals the similarities and differences in peripheral nerve conduction impairments between patients with LLD and AD. Compared with NC group, both patient cohorts exhibited striking similarities in electrophysiological alterations of the median nerve: specifically, there was a marked prolongation of proximal motor latency and a significant reduction in motor conduction amplitude. Notably, sensory nerve conduction function was preserved across all patient groups. AD patients had reduced motor conduction velocities in the median and common peroneal nerves, while LLD patients did not. In contrast, LLD patients showed prolonged distal motor latency in the median nerve and prolonged proximal motor latency in the common peroneal nerve, while findings absent in AD patients.
The pathogenesis of AD is characterized by progressive changes that involve both central and peripheral neural systems. Accumulation of amyloid-β (Aβ) and tau-protein alterations are recognized as early steps, initiating a cascade of neural injury.12,13 While these processes contribute to central neurodegeneration, similar changes in Aβ and tau can also be observed in peripheral nerves, where they may lead to local stress and gradual structural impairment affecting nerve conduction.14 Concomitant cerebrovascular changes in AD patients further weaken neural control of peripheral function, compounding the peripheral dysfunction.15,16
Peripheral nerve studies in AD have consistently shown reduced motor conduction velocities, consistent with the view that alterations of the myelin structure play a role in the disease’s clinical expression.17–19 This pattern differs from that seen in major depressive disorder in later life (LLD), where motor deficits can occur without marked slowing of conduction speed.20–23
Motor slowing in LLD has previously been interpreted largely in terms of neurotransmitter dysregulation within the brain, but the present study observed measurable changes in peripheral motor latencies, supporting the idea that LLD-related motor impairment involves both central and peripheral nerves. Crucially, conduction velocity remains largely preserved in LLD, a finding that contrasts with AD. Both AD and LLD patients demonstrated reduced motor amplitudes, pointing toward a possible shared pathway, such as glutamate-related stress and cellular energy dysfunction, that could partly explain motor deficits in both conditions.24,25 These results broaden our understanding of the neurological correlates of motor dysfunction in aging-related cognitive and mood disorders.
This investigation represents a preliminary, small-sample exploration of peripheral nerve function in AD and LLD, and thus has several important limitations that warrant consideration. First, the assessment of confounding factors was incomplete: while we attempted to control for major medications and comorbidities known to affect peripheral nerve conduction, our screening did not capture all potential modifiers, including subtle metabolic abnormalities, subclinical vitamin deficiencies, or chronic low-grade inflammatory states. Additionally, the selection of tested nerves was restricted to the median and common peroneal nerves, limiting our ability to characterize the full topography of peripheral nerve involvement in these populations. Second, variability in participant cooperation and tolerance to neurophysiological testing introduced technical challenges. Some subjects exhibited reduced amplitude responses or incomplete data acquisition due to discomfort from electrical stimulation, particularly among older adults with sensory hypersensitivity or cognitive impairment. These missing or attenuated signals may have introduced bias in the interpretation of conduction velocity and latency measurements, potentially masking subtle differences between groups.
Collectively, this preliminary study identified distinct patterns of peripheral nerve conduction impairment in patients with AD and LLD. After adjusting for covariates, AD patients exhibited slowed motor conduction velocity, most notably in the median and common peroneal nerves, a finding indicative of potential demyelinating pathology. In contrast, LLD patients presented with prolonged motor latency and reduced amplitude while maintaining preserved conduction velocity, suggesting underlying axonal or synaptic dysfunction rather than demyelination. Notably, sensory nerve conduction in the median and sural nerves was preserved in both groups following adjustment. These exploratory findings confirm peripheral nerve involvement in both conditions, highlighting distinct neurophysiological signatures that may aid in differential diagnosis. They further underscore the value of integrating peripheral nerve evaluation into clinical assessments of elderly patients with neurocognitive or mood disorders, though larger-scale studies are needed to validate these conclusions and explore their clinical implications in greater depth.
Data Sharing Statement
The data underlying the results presented in the study are available upon request from the corresponding author if there are legal or ethical restrictions on sharing data publicly.
Consent for Publication
Consent to publish statements must confirm that the details of any image, video, or recording can be published. All authors provided copies of the signed consent forms to the journal editorial office if requested.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the funding of Hunan University of Chinese Medicine (HUCMS) University-Hospital Joint Fund (2024XYLH209). The funder supported study design, data collection and analysis, decision to publish, and preparation of the manuscript.
Disclosure
The authors report no competing interests in this work.
References
1. Li J, Haj Ebrahimi A, Ali AB. Advances in therapeutics to alleviate cognitive decline and neuropsychiatric symptoms of Alzheimer’s disease. Int J Mol Sci. 2024;25(10):5169.
2. Samtani S, Mahalingam G, Lam BCP, et al. Emotional and instrumental social support and older adults’ depressive symptoms: collaborative individual participant data meta-analysis of 11 population-based studies of aging. Am J Epidemiol. 2025;194(10):3041–11. doi:10.1093/aje/kwaf137
3. Hardy J. Alzheimer’s disease: treatment challenges for the future. J Neurochem. 2025;169(8):e70176. doi:10.1111/jnc.70176
4. Ruthirakuhan M, Guan DX, Mortby M, Gatchel J, Babulal GM. Updates and future perspectives on neuropsychiatric symptoms in Alzheimer’s disease. Alzheimers Dement. 2025;21(3):e70079. doi:10.1002/alz.70079
5. Nelson JC, Gandelman JA, Mackin RS. A systematic review of antidepressants and psychotherapy commonly used in the treatment of late life depression for their effects on cognition. Am J Geriatr Psychiatry. 2025;33(3):287–304. doi:10.1016/j.jagp.2024.08.015
6. Pozuelo Moyano B, Gomez Bautista D, Porras Ibarra KJ, et al. Systematic review of clinical effectiveness of interventions for treatment resistant late-life depression. Ageing Res Rev. 2025;107:102710. doi:10.1016/j.arr.2025.102710
7. Teixeira AL, Gregg A, Gentry MT, et al. Cognitive deficits in late-life depression: from symptoms and assessment to therapeutics. Focus. 2025;23(2):183–194. doi:10.1176/appi.focus.20240046
8. Alghafri RM, Gatt A, Formosa C. Depression symptoms in patients with diabetic peripheral neuropathy. Rev Diabet Stud. 2020;16(1):35–40. doi:10.1900/RDS.2020.16.35
9. Qiu Q, Yang M, Gong D, Liang H, Chen T. Potassium and calcium channels in different nerve cells act as therapeutic targets in neurological disorders. Neural Regen Res. 2025;20(5):1258–1276. doi:10.4103/NRR.NRR-D-23-01766
10. Leon-Ariza JS, Mosquera MA, Siomin V, et al. The vagus nerve somatosensory-evoked potential in neural disorders: systematic review and illustrative vignettes. Clin EEG Neurosci. 2022;53(3):256–263.
11. Zhou X, Zhu Y, Wang Z, et al. Rate-dependent depression: a predictor of the therapeutic efficacy in treating painful diabetic peripheral neuropathy. Diabetes. 2022;71(6):1272–1281. doi:10.2337/db21-0960
12. Ding X, Hu Y, Feng X, et al. Enhanced blood-brain barrier penetrability of BACE1 SiRNA-loaded prussian blue nanocomplexes for Alzheimer’s disease synergy therapy. Exploration. 2025;5(4):e20230178. doi:10.1002/EXP.20230178
13. Vecchio FL, Bisceglia P, Imbimbo BP, et al. Are apolipoprotein E fragments a promising new therapeutic target for Alzheimer’s disease? Ther Adv Chronic Dis. 2022;13:20406223221081605. doi:10.1177/20406223221081605
14. Al-Amin MM, Kim B, Karahan H, et al. Apolipoprotein epsilon4 exacerbates white matter impairment in a mouse model of Abeta amyloidosis by decreasing actively myelinating oligodendrocytes. Alzheimers Dement. 2025;21(10):e70791. doi:10.1002/alz.70791
15. Eid SA, Rumora AE, Beirowski B, et al. New perspectives in diabetic neuropathy. Neuron. 2023;111(17):2623–2641. doi:10.1016/j.neuron.2023.05.003
16. Xi C, Zhang J, Huang Z, et al. EGR2 maintains neuropathic pain by promoting microglial phagocytosis. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2025;50(4):586–601. doi:10.11817/j.issn.1672-7347.2025.240270
17. Ciaccio M. Biochemical biomarkers and neurodegenerative diseases. Brain Sci. 2021;11(7):940. doi:10.3390/brainsci11070940
18. Janelidze S, Ashton NJ, Orduña Dolado A, et al. A comparison of p-tau assays for the specificity to detect tau changes in Alzheimer’s disease. Alzheimers Dement. 2025;21(4):e70208. doi:10.1002/alz.70208
19. Parvez F. Immune crosstalk in Alzheimer’s and Parkinson’s disease: insights from Drosophila models into the brain–peripheral immune axis. Front Immunol. 2026;17:1725046. doi:10.3389/fimmu.2026.1725046
20. Murri MB, Triolo F, Coni A, et al. Instrumental assessment of balance and gait in depression: a systematic review. Psychiatry Res. 2020;284:112687. doi:10.1016/j.psychres.2019.112687
21. Wang Y, Wang J, Liu X, Zhu T. Detecting depression through gait data: examining the contribution of gait features in recognizing depression. Front Psychiatry. 2021;7(12):661213. doi:10.3389/fpsyt.2021.661213
22. Bogdanova D. Gait disorders in unipolar and bipolar depression. Heliyon. 2023;9(5):e15864. doi:10.1016/j.heliyon.2023.e15864
23. Van Cauwenberge MGA, Casteele TV, Laroy M, et al. Motor dysfunction in late life depression: a mood or movement disorder?. J Affect Disord. 2025;15(381):680–691.
24. Kessler EM, Kleinke K, Engel JV, Forstmeier S. Age-sensitive telehealth group therapy for depression in older adults with and without comorbid anxiety (VISION-AGE): study protocol for a randomized controlled trial in an embedded mixed-methods design. BMC Psychiatry. 2026;26(1):215. doi:10.1186/s12888-026-07851-2
25. Hunjan G, Aran KR. Role of mGluR7 in Alzheimer’s disease: pathophysiological insights and therapeutic approaches. Inflammopharmacology. 2025;33(6):2977–2995. doi:10.1007/s10787-025-01765-3
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.