Back to Archived Journals » Open Access Surgery » Volume 16
Perioperative Nutrition Support for Elective Surgical Cancer Patients: A Narrative Review
Authors Mulatie Zewudie M, Yaregal Melesse D ![]() , Dereje Filatie T, Getahun AB
, Dereje Filatie T, Getahun AB ![]() , Adie Admass B
, Adie Admass B ![]()
Received 24 January 2023
Accepted for publication 9 May 2023
Published 12 May 2023 Volume 2023:16 Pages 33—45
DOI https://doi.org/10.2147/OAS.S405799
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Luigi Bonavina
Misgan Mulatie Zewudie,1 Debas Yaregal Melesse,2 Tesera Dereje Filatie,2 Amare Belete Getahun,2 Biruk Adie Admass2
1Department of Anesthesia, College of Medicine and Health Sciences, Injibara University, Injibara, Ethiopia; 2Department of Anesthesia, College of Medicine and Health Science, University of Gondar, Gondar, Ethiopia
Correspondence: Debas Yaregal Melesse, Tel +251948814731, Email [email protected]
Objective: This review of the literature’s current types of suggestions regarding perioperative nutrition support for surgical cancer patients was its primary goal.
Methods: Appropriate kinds of literature were searched from the databases and other sources based on the process applied in a narrative review. The following databases like SCOPUS, PubMed, science direct, Google scholar, Cochrane library, MEDLINE, and Embase with Boolean operators including OR, AND, with medical heading subjects (MeSH) (preoperative AND nutrition AND cancer, malnutrition OR under-nutrition AND prevention AND management, cancer AND surgery AND analgesia, nutrition AND perioperative AND oncologic surgery, optimization AND perioperative AND nutrition AND cancer, oncological surgery AND frailty, sarcopenia AND perioperative malnutrition AND optimization, prehabilitation AND nutritional support AND cancer AND cachexia) were used. Endnote reference manager was used to remove duplications of extracted kinds of literature from different sources.
Results: The total number of articles identified through database and website searches was 34,292. Of these references, 1030 duplicates were removed. Nine hundred literatures were excluded in the screening phase with the human and published periods. Eighty-nine (89) references were included in the final version of this review.
Conclusion: Cancer-related malnutrition can be diagnosed using the criteria of the Global Leadership Initiative on Malnutrition (GLIM). A daily caloric consumption of 20– 35 kcal/kg, with glucose and lipids, as well as electrolytes, trace elements, and vitamins, is advised for malnutrition in cancer patients.
Keywords: cancer, frailty, nutrition support, optimization, perioperative, sarcopenia
Introduction
Malnutrition is defined as a significant loss in body weight and other body weight components that affects quality of life and the prognosis of a particular illness.1 Early screening of cancer patients for malnutrition enables early detection and treatment.2
Internationally recognised and validated screening tools such as the Malnutrition Universal Screening Tool (MUST), the Nutritional Risk Screening (NRS) and the Patient-Generated Subjective Global Assessment (PG-SGA) can be used to assess the risk of malnutrition.3–5
The following criteria (at least one criterion met): severe weight loss (> 10–15% in 6 months), low body mass index (BMI < 18.5 kg/m2), or serum albumin < 30 g/L (in the absence of liver or kidney failure) are the standards used to identify cancer patients at a high risk of malnutrition and suggest preoperative nutrition therapy.3,4,6–8
The Global Leadership Initiative on Malnutrition (GLIM) ranked the top five criteria, with three phenotypic criteria—non-voluntary weight loss, a low body mass index, and decreased muscle mass—as well as two aetiological criteria—reduced food intake or assimilation and inflammation or disease burden. To determine malnutrition, at least one phenotypic and one aetiological indicator must be present. We suggest two levels of malnutrition severity: level 1 (moderate) and level 2 (severe). It is suggested that the aetiological parameters be used to direct intervention and anticipated outcomes. Malnutrition associated with chronic diseases with inflammation, malnutrition associated with chronic diseases with little to no apparent inflammation, malnutrition associated with acute diseases or injuries with severe inflammation, and malnutrition associated with starvation are the four aetiological diagnostic groups.9,10
The clinical features of malnutrition can be measured by inadequate energy intake, loss of fat, weight and muscle, fluid accumulation and reduced grip strength, which should allow prediction of outcomes such as morbidity and mortality, physical function, quality of life, readmissions and hospitalisations, and health care costs.11–13
Cachexia is a multifactorial syndrome prevalent in chronic diseases and is now thought to be a comorbidity of cancer. Cancer-related malnutrition can cause it. It is characterized by a significant, involuntary loss of skeletal muscle mass, along with or without a loss of fat mass, and a heightened inflammatory reaction throughout the body.14
The global incidence of malnutrition in the course of cancer ranges from 30 to 90%, depending on the type, location, grade and stage of the tumour, tumour spread and cancer treatment, but also individual susceptibility.15 In 20–50% of cancer patients having surgery, malnutrition is one of the independent causes of post-operative complications.16
Nearly two-thirds of patients with colorectal cancer who were scheduled for surgical resection required other nutritional therapy, and about 1 in 5 required critical nutritional intervention. Every component of measured health-related quality of life (HRQoL) was worse in patients whose diet was compromised than in those who did not need a dietary intervention, including depression, anxiety, pain, social function, overall physical health, overall mental health and overall quality of life.17
According to recommendations made by the European Society for Clinical Nutrition and Metabolism (ESPEN) expert group, nutritional care for cancer patients should be based on three key procedures: screening all cancer patients for nutritional risks early in their treatment without taking into account their body mass index or weight history; incorporating measures of anorexia, body composition, inflammatory biomarkers, resting energy expenditure, and physical performance into nutritional assessment methods; Utilizing multimodal dietary interventions with customized treatment plans, such as care aimed at boosting calorie consumption, lowering inflammation and hypermetabolic stress, and boosting physical activity.18
In patients with colon cancer, preoperative albumin level was a predictor of prognosis, and low albumin level is linked to a worse outcome in these patients.19
Preoperative nutritional interventions to optimise nutritional status with enteral and parenteral nutrition have shown that enteral nutrition was superior to parenteral nutrition in reducing postoperative complications.20 Although there are well-known, internationally recognised guidelines for the management of perioperative malnutrition, too little attention is paid to it in clinical practise.21 Since there is no argument in the treatment of malnutrition in cancer patients, inadequate nutritional therapy for these patients should be considered unethical.22
In patients with cancer of any type and location, multimodal care, including nutritional therapy, should be consistent with the principle of improved recovery after surgery (ERAS).23
According to one study, current data suggests that both types of neoadjuvant therapy (chemoradiation and perioperative chemotherapy) have similar outcomes of interest.24 Another important component of perioperative care for these patients has just been introduced into prehabilitation practise, which aims to reduce the occurrence of adverse events and improve nutritional and health status during the perioperative period.25 Considering that malnutrition and underfeeding are risk factors for postoperative complications, early enteral nutrition is important for all surgical patients at risk of malnutrition.26 The nutritional care process was found to be beneficial by nutrition and dietetics professionals.27
The purpose of this literature review was to thoroughly examine the available literature in order to obtain recommendations for enhancing nutrition in cancer patients undergoing elective surgery.
Methods
Appropriate types of literature were searched in databases and other sources based on the procedure used in a systematic review. The following databases such as SCOPUS, PubMed, science direct, Google scholar, Cochrane library, MEDLINE and Embase were searched using Boolean operators such as OR, AND and medical keywords (MeSH) (preoperative AND nutrition AND cancer, malnutrition OR malnutrition AND prevention AND management, cancer AND surgery AND analgesia, nutrition AND perioperative AND oncological surgery, optimisation AND perioperative AND nutrition AND cancer, oncological surgery AND frailty, sarcopenia AND perioperative malnutrition AND optimisation, prehabilitation AND nutritional support AND cancer) were used. A critical appraisal of the literature was conducted to screen papers. Endnote Reference Manager was used to remove duplicates of extracted literature types from different sources. The review process was conducted following the Preferred Reporting Elements for Systematic Reviews and Meta-Analyses (PRISMA) 202028,29 (Figure 1).
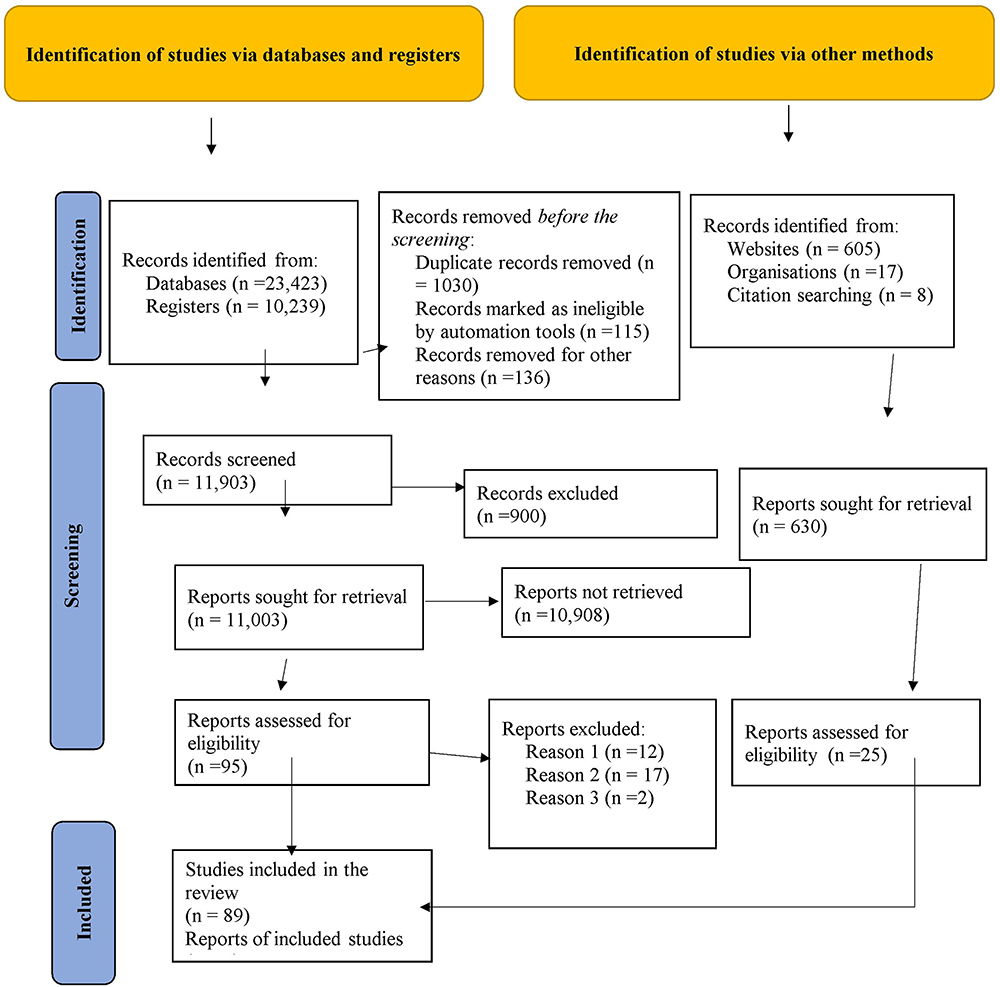 |
Figure 1 Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) 2020. Adapted from Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ (Clinical research ed). 2021;372:n71.29 |
Conclusions and recommendations were drawn by directing the assessment towards perioperative optimisation of cancer patients with malnutrition. The studies were summarised by weighing the advantages and disadvantages of the alternative management strategies based on the currently available literature.
Inclusion and Exclusion Criteria
In this literature review, we considered randomised controlled trials, systematic reviews, meta-analyses and observational studies of perioperative (preoperative, intraoperative and postoperative) nutritional support or therapy in elective surgical cancer patients worldwide published in English at any time point, in any age group and in both men and women. Duplicate studies, reports, commentaries, articles without full text, short communications irrelevant to our topic, and letters to the editor were excluded from this literature review.
Results
Identification of Studies and Characteristics of Included Studies
We identified a total of 34,292 studies from databases, registries, websites, organisations and citations. After removing duplicates and reviewing titles and abstracts, 88 studies were considered for full text review.
The total number of literature identified through database and website searches was 23,423 and 10,239 respectively. Of these scraps of literature, 1030 duplicates were removed. Nine hundred (900) pieces of literature were excluded during the screening phase with humans. Eighty-nine (89) pieces of literature were included in the final version of this literature review.
Out of the total 89 studies, twelve (12) different studies were selected as the sample for the summary of the literature review based on the grading of recommendations, assessment, development and evaluations (GRADE) of each type of literature for the conclusions (Table 1).
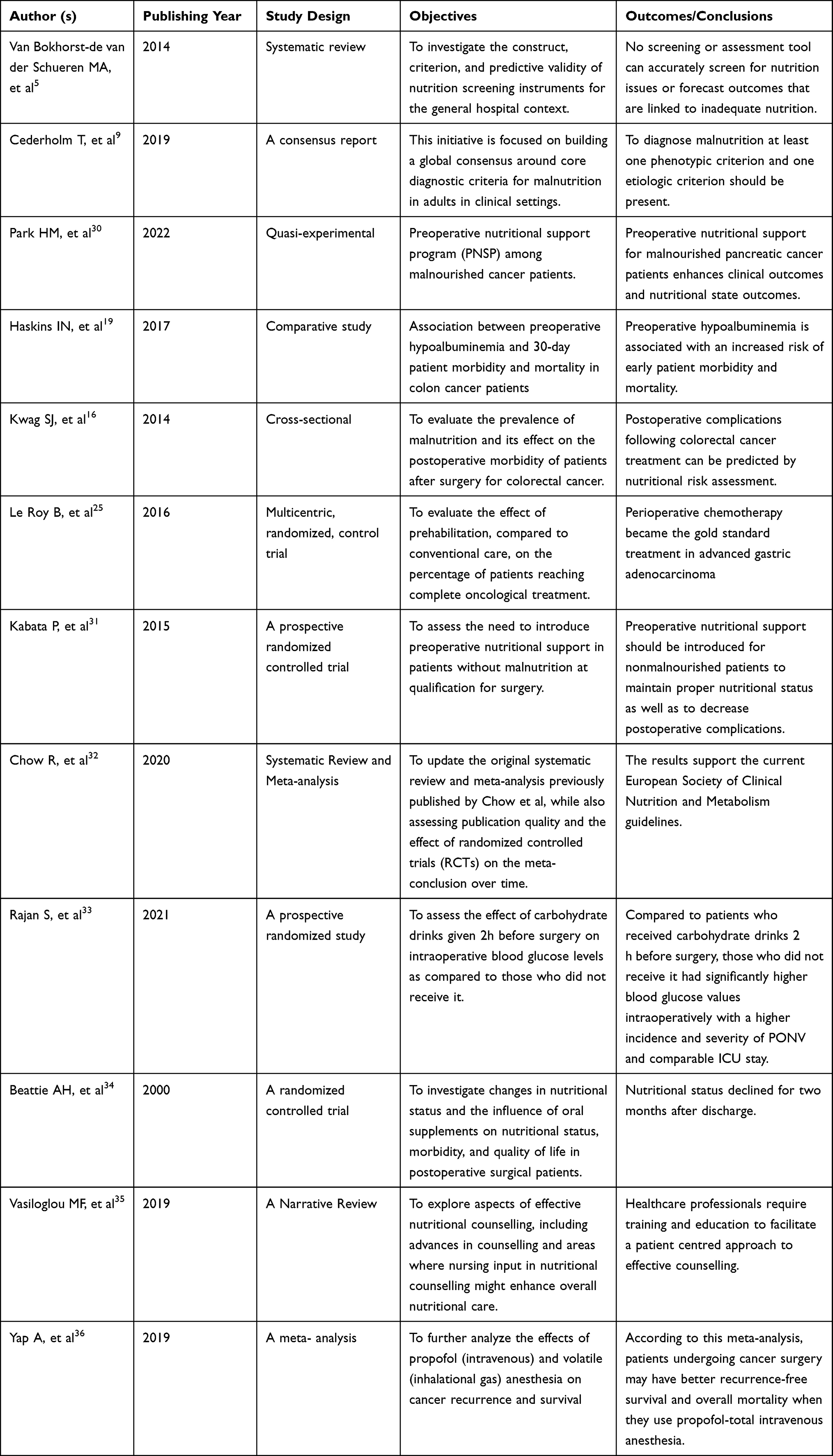 |
Table 1 A List of Examples of Literature That Was Used in the Findings |
Discussion
Perioperative nutritional support can improve positive patient outcomes by reducing hospital stay, morbidity and postoperative mortality.37 It is well known that the preoperative nutritional status of the patient is a decisive factor for the postoperative outcome in surgical oncology cases.38 A systematic review and meta-analysis concluded that preoperative body composition assessment helps to identify patients who need nutritional support.39
The aim of this literature review was to discuss the currently available literature on perioperative nutrition therapy in surgical cancer patients by dividing it into different subcategories.
Preoperative Counseling and Education
In addition to an examination of general medical conditions, the preoperative medical evaluation of cancer patients should include nutritional status, functional status, and symptom control (especially with reference to cancer-related pain). It’s also important to take into account the cancer’s natural course as well as the effects of any earlier radiation or chemotherapy. Older people can experience cancer surgery with comparable short- and long-term results as younger ones. Considerations for treatment should be made in light of functional status rather than chronological age.40
Detailed formal education and counselling in the preoperative period are invaluable in reducing reducible factors such as smoking, malnutrition, alcohol consumption and anaemia.41
Outcomes after colorectal surgery have been measured by various indicators such as length of stay, morbidity, mortality, overall survival, disease-free survival, and time to first bowel movement or time to first oral intake. However, many of these indicators are of limited relevance to frail older people, who may be more concerned about anticipated disability and dependency than a cancer diagnosis or a reduction in life expectancy.42–44
A randomised clinical trial (RCT) concluded that integrated palliative care models (PC) for cancer patient caregivers lead to good patient outcomes and improve the caregiver experience.45
Another study on the use of complementary and alternative medicine in cancer patients concluded that communication with patients about the use of complementary and alternative medicine (CAM) in cancer treatment plays a crucial role for a positive outcome.46
Nutritional counselling, usually carried out by dieticians, is considered the best way to stabilise various chronic diseases.35
Preoperative Medical Optimization
A study conducted by Grocott MP et al concluded that early perioperative contact between patients and physicians improved patients’ surgical and medical conditions, such as hypertension, anaemia and diabetes, as well as physical activity and cessation of smoking and drug or alcohol abuse.47
Promoting exercise, correcting malnutrition, psychological support and optimising medical conditions are areas of prehabilitation that improve the postoperative outcome of cancer patients.48 Preoperative correction of malnutrition and metabolic abnormalities before major surgery has been shown to reduce postoperative complications.6
The Society for Perioperative Assessment and Quality Improvement (SPAQI), an interdisciplinary society made up of perioperative medicine professionals, has published recommendations for the preoperative management of frailty. It states that teams should actively screen for frailty before surgery and that pathways, including geriatric comanagement, shared decision-making and multimodal prehabilitation, should be embedded in routine care to improve patient outcomes.49
These standards include preoperative screening for common geriatric complexities such as delirium risk and social vulnerabilities, addressing polypharmacy and nutritional needs, improving communication with patients and families, and providing care that is consistent with patients’ goals.50 Significant changes in postoperative functional capacity are more likely to be achieved with a prehabilitation programme than with rehabilitation.51 Structured and personalised prehabilitation programmes with moderate exercise protocols, combined with optimised nutrition and appropriate psychological support, can improve postoperative outcomes in these individuals. This is an important, targeted and rapidly developing area of clinical research.52
Preoperative Bowel Preparation
Routine preoperative mechanical bowel preparation with antibiotics reduced postoperative anastomotic leakage in patients undergoing elective surgery for colorectal resection of cancer.53 The other systematic review introduced that the addition of oral antibiotics decreases the development of infection and nutritional obsoleting during the preoperative period is outdated.54
The other study, which focused on rectal cancer surgery, concluded that preoperative enemas only led to postoperative complications.55
A meta-analysis of randomised controlled clinical trials comparing mechanical bowel preparation with oral and systemic antibiotics with mechanical bowel preparation and systemic antibiotics alone found that surgical wound infections were significantly reduced in patients receiving the former intervention.56
Preoperative Nutritional Support in Cancer Patients and Preoperative Fasting
One of the most important components of surgical care is preoperative nutritional support.57
Essential components of perioperative care are the combination of nutritional components with the general management of the patient, reduced preoperative fasting, resumption of oral nutrition as early as possible postoperatively, especially in high-risk patient groups, metabolic control and early mobilisation according to the recommendations for surgical cancer patients.26 Preoperative nutritional therapy can also be used in non-malnourished patients to maintain an adequate nutritional status and reduce postoperative adverse events.31 We can improve the nutritional status of elective surgical cancer patients through oral nutritional support and immunostimulatory formulas.37 A preoperative nutritional support program (PNSP) was formed to improve perioperative nutritional status and clinical outcomes among malnourished patients with cancer.30 It is well researched that preoperative oral nutritional supplements (ONS) improve the postoperative outcomes of surgical patients.58
This meta-analysis showed that the risk of infection, complications and all-cause mortality after gastrointestinal cancer surgery was reduced in patients receiving a preoperative diet in a low-to middle-income country (LMIC).58 This report shows that some dietary factors have an impact on mortality and on the risk of recurrence or second primary cancer in cancer patients. Therefore, high-risk nutritional states may occur in certain cancers: From diagnosis and throughout the course of treatment, weight loss (lung and oesophageal cancers), malnutrition (lung, oesophageal, colorectal, pancreatic, stomach and liver cancers), weight gain (colorectal, breast and kidney cancers) and alcohol consumption (upper aerodigestive and oesophageal cancers) should be monitored; and after cancer treatments, obesity should be detected (colorectal, breast and kidney cancers).59 The prudent pattern was characterised by a high intake of fruits and vegetables, poultry and fish, while the western pattern was characterised by a high intake of meat, fat, refined grains and desserts. Patients were followed up for cancer recurrence or death. Higher consumption of Western dietary patterns may be associated with a higher risk of recurrence and mortality in patients with stage III colon cancer treated with surgery and adjuvant chemotherapy.60
Compared to usual hospital nutrition without nutritional support, individual nutritional support reduced the risk of death and improved functional outcomes and quality of life in cancer patients at increased nutritional risk.61 Safe management of anastomotic leaks after gastric cancer surgery with enteral feeding via a naso-intestinal tube.62
Preoperative nutritional support reduces the incidence of surgical wound complications in oncology patients.63 Post-discharge ONS nutritional counselling in patients at nutritional risk after gastric cancer surgery improved nutritional outcomes, skeletal muscle preservation, chemotherapy tolerance and some quality of life variables.64 Preoperative nutrition care is often overlooked because of the urgency of operating on a cancer patient.65 The negative consequences are a longer hospital stay, higher levels of treatment-related toxicity, lower response to cancer treatment, lower activity levels, lower quality of life and a poorer overall prognosis.66
A systematic review and meta-analysis by Ronald Chow et al concluded that neither parenteral (PN) nor enteral (EN) nutrition is superior in terms of nutritional support and postoperative complication rates.67 A daily intake of 20–35 kcal/kg, with a balanced contribution of glucose and lipids, and of 0.2–0.35 g nitrogen/kg is recommended both for EN and PN, with an adequate provision of electrolytes, trace elements and vitamins. A balanced contribution of glucose and lipids, or slightly more glucose than fat (60% glucose, 40% fat) is generally recommended. Needless to say, the nutrition must be supplemented, especially in the case of parenteral nutrition, with electrolytes, trace elements and vitamins.68,69
Preoperative nutritional assistance is crucial for patients with gastrointestinal and abdominal cancer, even if there is no risk of malnutrition. This method lessens postoperative issues, especially anastomotic dehiscence and leaking.31
Patients undergoing oncologic surgery should receive oral preoperative carbohydrate therapy to lessen perioperative discomfort, including worry. There was no increase in the risk of aspiration after preoperative delivery of an 800 mL carbohydrate drink the night before surgery and 400 mL right before surgery on the day of surgery.70 A study that evaluated preoperative oral carbohydrate loading and its impact on “intraoperative blood glucose levels, postoperative nausea and vomiting, and intensive care unit stay” found that patients who consumed carbohydrates two hours prior to surgery had lower blood sugar levels than those who did not, and that preoperative carbohydrate loading also reduced the frequency and severity of postoperative nausea and vomiting (PONV).33
If the patient is thought to have been unable to consume for longer than five days, preoperative nutritional therapy should be initiated. It is also advised for patients who are anticipated to have low oral intake and who are unable to sustain intake levels above 50% for longer than seven days. It is advised to immediately begin nutritional treatment in such cases.71
Preoperative fasting from midnight is not required, according to the European Society for Clinical Nutrition and Metabolism’s (ESPEN) practical recommendation. As a result, patients who are thought to have no particular risk of aspiration can consume clear liquids up to two hours before induction and foods up to six hours before induction.26
Several studies have lately questioned the advantages of 6 to 8 hours of preoperative fasting to reduce the risk for pulmonary aspiration of gastric content.72,73 Traditional fasting is frequently extended when operation takes longer than expected. Due to the heightened systemic response to surgical tissue damage, the recommended prior fasting period can be prolonged by 10 to 16 hours. This has a negative impact on the recovery process.73
Anesthesia Considerations
Anesthesia and/or analgesia are used for diagnostic, therapeutic, or palliative measures in up to 80% of oncological patients.74 Total intravenous anesthetic may enhance sufferers’ survival without recurrence and lower overall mortality, according to current systematic reviews and meta-analyses.36,75 Clinical practitioners have begun using local anesthetics in the treatment of a variety of inflammation-related conditions and diseases due to their potent anti-inflammatory properties, which are superior in several ways to traditional anti-inflammatory agents of the non-steroidal anti-inflammatory drugs (NSAIDs) and steroid groups and have fewer side effects.76 Regional anesthesia may be advantageous because it protects cell-mediated immunity and lowers the surgical neuroendocrine stress response by blocking afferent neural transmission that stimulates the hypothalamic-pituitary-adrenal axis and sympathetic nervous system. This could reduce the need for opioids and volatile anesthetics, which would reduce the risk of cancer recurrence.77,78
Postoperative Nutritional Care
Prescriptions for postoperative oral nutritional supplements for 8 weeks are clearly advantageous for malnourished patients in terms of nutritional healing, protein economy, and quality of life.34 Long-term bed rest reduces muscular strength, pulmonary function, and tissue oxygenation in addition to increasing insulin resistance and muscle loss.79
Immuno-enhanced nutrition (IEN) can be the chosen management, but using parenteral nutrition support should be given to indicated patients like patients with intolerance to it. Preoperative enteral nutrition significantly reduces the postoperative adverse events in patients with digestive system cancer.80 Perioperative nutritional support has been shown to decrease morbidity, death, and length of hospital stay.37
There are many restrictions with this literature review. This literature review’s absence of a meta-analysis of the types of literature with particular issue bases was one of its limitations. The statistics were not quantitatively analyzed, which was another drawback. The current review’s limitations included all kinds of papers with various publication dates, research designs, and the size of the global population.
Recommendations
Perioperative Management
Prior to surgery, anesthetists and surgeons should conduct a physical examination, thorough medical history, and laboratory tests to assess the patient’s overall health. They should also pay particular attention to the patient’s nutritional status, type of surgery, and anesthesia, as well as the patient’s stage of cancer, the severity of their malnutrition, and any opportunistic infections they may have. The group should take malnourished patients with any kinds of cancer into account when predicting the perioperative risk category.
Regional anesthesia is frequently the preferred technique when it is not prohibited, such as in thrombocytopenic patients. The chance of neuropathies, local infections, or abnormalities in blood clotting must nevertheless be considered. All preventive and supportive management is still in effect during the intraoperative period. Malnourished patients who also have cancer should receive extra care, counseling, and multimodal treatments. Regional techniques for postoperative pain control are reliant on the patient’s hemodynamic condition, coagulation profile, and resource availability as part of multimodal therapies. Additionally, early nutritional support and antibiotics should be included in postoperative concerns for those patients.
Conclusions
Cancer-related malnutrition can be diagnosed using the criteria of the Global Leadership Initiative on Malnutrition (GLIM). A daily caloric consumption of 20–35 kcal/kg, with glucose and lipids, as well as electrolytes, trace elements, and vitamins, is advised for malnutrition in cancer patients (Figures 2–4).
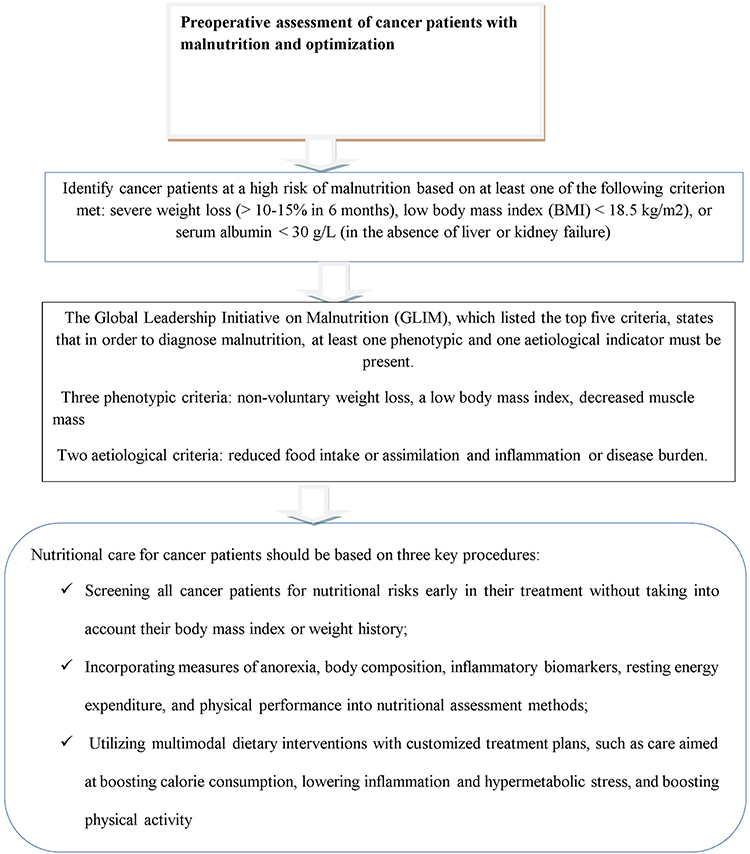 |
Figure 2 Preoperative assessment of cancer patients with malnutrition and optimization. |
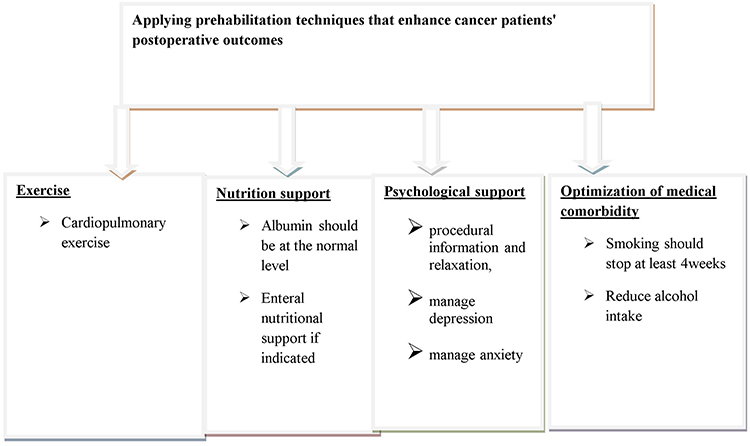 |
Figure 3 Components of perioperative prehabilitation of surgical cancer patients. |
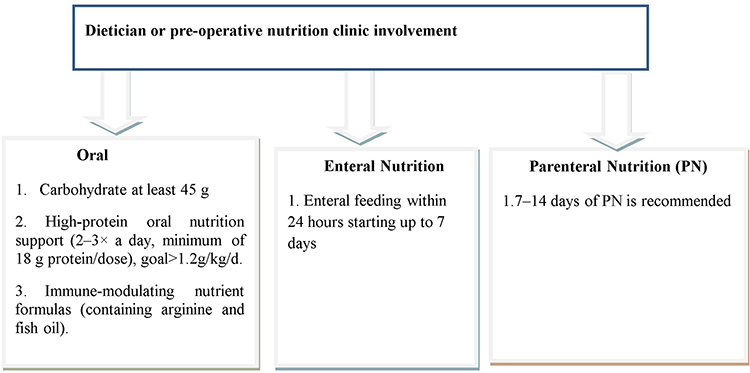 |
Figure 4 Preoperative nutrition support recommendations. |
Acknowledgment
We would like to acknowledge the University of Gondar.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declares no conflict of interest in this work.
References
1. Löser C, Fruehauf S, Müller M, et al. Moderne Ernährungstherapie bei onkologischen Patienten – ein Positionspapier. Aktuelle Ernährungsmedizin. 2014;39(02):127–131. doi:10.1055/s-0034-1369885
2. Silva F, de Oliveira MGOA, Souza ASR, Figueroa JN, Santos CS. Factors associated with malnutrition in hospitalized cancer patients: a croos-sectional study. Nutr J. 2015;14(1):1–8. doi:10.1186/s12937-015-0113-1
3. Kondrup J, Allison SP, Elia M, Vellas B, Plauth M. ESPEN guidelines for nutrition screening 2002. Clin Nutr. 2003;22(4):415–421. doi:10.1016/S0261-5614(03)00098-0
4. Skipper A, Ferguson M, Thompson K, Castellanos VH, Porcari J. Nutrition screening tools: an analysis of the evidence. JPEN J Parenter Enteral Nutr. 2012;36(3):292–298. doi:10.1177/0148607111414023
5. van Bokhorst-de van der Schueren MA, Guaitoli PR, Jansma EP, de Vet HC. Nutrition screening tools: does one size fit all? A systematic review of screening tools for the hospital setting. Clin Nutr. 2014;33(1):39–58. doi:10.1016/j.clnu.2013.04.008
6. Steenhagen E. Preoperative nutritional optimization of esophageal cancer patients. J Thorac Dis. 2019;11(Suppl 5):S645. doi:10.21037/jtd.2018.11.33
7. Cederholm T, Bosaeus I, Barazzoni R, et al. Diagnostic criteria for malnutrition - an ESPEN consensus statement. Clin Nutr. 2015;34(3):335–340. doi:10.1016/j.clnu.2015.03.001
8. Valentini L, Volkert D, Schütz T, et al. Leitlinie der Deutschen Gesellschaft für Ernährungsmedizin (DGEM). Aktuelle Ernährungsmedizin. 2013;38(02):97–111. doi:10.1055/s-0032-1332980
9. Cederholm T, Jensen GL, Correia M, et al. GLIM criteria for the diagnosis of malnutrition - A consensus report from the global clinical nutrition community. Clin Nutr. 2019;38(1):1–9. doi:10.1016/j.clnu.2018.08.002
10. Jensen GL, Cederholm T, Correia M. GLIM criteria for the diagnosis of malnutrition: a consensus report from the global clinical nutrition community. J Cachexia Sarcopenia Muscle. 2019;43(1):32–40.
11. Hand RK, Murphy WJ, Field LB, et al. Validation of the academy/A.S.P.E.N. Malnutrition clinical characteristics. J Acad Nutr Diet. 2016;116(5):856–864. doi:10.1016/j.jand.2016.01.018
12. White JV, Guenter P, Jensen G, Malone A, Schofield M. Consensus statement: Academy of Nutrition and Dietetics and American Society for Parenteral and Enteral Nutrition: characteristics recommended for the identification and documentation of adult malnutrition (undernutrition). JPEN J Parenter Enteral Nutr. 2012;36(3):275–283. doi:10.1177/0148607112440285
13. White JV, Guenter P, Jensen G, Malone A, Schofield M. Consensus statement of the Academy of Nutrition and Dietetics/American Society for Parenteral and Enteral Nutrition: characteristics recommended for the identification and documentation of adult malnutrition (undernutrition). J Acad Nutr Diet. 2012;112(5):730–738. doi:10.1016/j.jand.2012.03.012
14. Muscaritoli M, Corsaro E, Molfino A. Awareness of cancer-related malnutrition and its management: analysis of the results from a survey conducted among medical oncologists. Front Oncol. 2021;11. doi:10.3389/fonc.2021.682999
15. Nitenberg G, Raynard B. Nutritional support of the cancer patient: issues and dilemmas. Crit Rev Oncol Hematol. 2000;34(3):137–168. doi:10.1016/S1040-8428(00)00048-2
16. Kwag SJ, Kim JG, Kang WK, Lee JK, Oh ST. The nutritional risk is a independent factor for postoperative morbidity in surgery for colorectal cancer. Ann Surg Treat Res. 2014;86(4):206–211. doi:10.4174/astr.2014.86.4.206
17. Gillis C, Richer L, Fenton TR, et al. Colorectal cancer patients with malnutrition suffer poor physical and mental health before surgery. Surgery. 2021;170(3):841–847. doi:10.1016/j.surg.2021.04.003
18. Arends J, Baracos V, Bertz H, et al. ESPEN expert group recommendations for action against cancer-related malnutrition. Clin Nutr. 2017;36(5):1187–1196. doi:10.1016/j.clnu.2017.06.017
19. Haskins IN, Baginsky M, Amdur RL, Agarwal S. Preoperative hypoalbuminemia is associated with worse outcomes in colon cancer patients. Clin Nutr. 2017;36(5):1333–1338. doi:10.1016/j.clnu.2016.08.023
20. Brennan GT, Ha I, Hogan C, et al. Does preoperative enteral or parenteral nutrition reduce postoperative complications in Crohn’s disease patients: a meta-analysis. Eur J Gastroenterol Hepatol. 2018;30(9):997–1002. doi:10.1097/MEG.0000000000001162
21. Sandrucci S, Beets G, Braga M, Dejong K, Demartines N. Perioperative nutrition and enhanced recovery after surgery in gastrointestinal cancer patients. A position paper by the Esso task force in collaboration with the ERAS society (ERAS coalition). Eur J Surg Oncol. 2018;44(4):509–514. doi:10.1016/j.ejso.2017.12.010
22. Caccialanza R, Cotogni P, Cereda E, et al. Nutritional support in cancer patients: update of the Italian Intersociety Working Group practical recommendations. J Cancer. 2022;13(9):2705–2716. doi:10.7150/jca.73130
23. Ciacio O, Voron T, Pittau G, et al. Interest of preoperative immunonutrition in liver resection for cancer: study protocol of the PROPILS trial, a multicenter randomized controlled Phase IV trial. BMC Cancer. 2014;14(1):1–10. doi:10.1186/1471-2407-14-980
24. Laxague F, Schlottmann F. Esophagogastric junction adenocarcinoma: preoperative chemoradiation or perioperative chemotherapy? World J Clin Oncol. 2021;12(7):557–564. doi:10.5306/wjco.v12.i7.557
25. Le Roy B, Pereira B, Bouteloup C, et al. Effect of prehabilitation in gastro-oesophageal adenocarcinoma: study protocol of a multicentric, randomised, control trial—the PREHAB study. BMJ open. 2016;6(12):e012876. doi:10.1136/bmjopen-2016-012876
26. Weimann A, Braga M, Carli F, et al. ESPEN practical guideline: clinical nutrition in surgery. Clin Nutr. 2021;40(7):4745–4761. doi:10.1016/j.clnu.2021.03.031
27. Kikomeko PK, Ochola S, Kaaya AN, Ogada I, Birungi TL, Nakitto P. Stakeholders’ perceptions of the nutrition and dietetics needs and the requisite professional competencies in Uganda: a cross-sectional mixed methods study. BMC Health Serv Res. 2021;21(1):92. doi:10.1186/s12913-021-06090-3
28. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. 2021;88:105906. doi:10.1016/j.ijsu.2021.105906
29. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
30. Park HM, Kang YH, Lee DE, Kang MJ, Han -S-S, Park S-J. Effect of preoperative nutritional support in malnourished patients with pancreatobiliary cancer: a quasi-experimental study. BMC Nutr. 2022;8(1):61. doi:10.1186/s40795-022-00555-2
31. Kabata P, Jastrzębski T, Kąkol M, et al. Preoperative nutritional support in cancer patients with no clinical signs of malnutrition--prospective randomized controlled trial. Support Care Cancer. 2015;23(2):365–370. doi:10.1007/s00520-014-2363-4
32. Chow R, Bruera E, Arends J, et al. Enteral and parenteral nutrition in cancer patients, a comparison of complication rates: an updated systematic review and (cumulative) meta-analysis. Support Care Cancer. 2020;28(3):979–1010. doi:10.1007/s00520-019-05145-w
33. Rajan S, Rahman AA, Kumar L. Preoperative oral carbohydrate loading: effects on intraoperative blood glucose levels, post-operative nausea and vomiting, and intensive care unit stay. J Anaesthesiol Clin Pharmacol. 2021;37(4):622–627. doi:10.4103/joacp.JOACP_382_19
34. Beattie AH, Prach AT, Baxter JP, Pennington CR. A randomised controlled trial evaluating the use of enteral nutritional supplements postoperatively in malnourished surgical patients. Gut. 2000;46(6):813–818. doi:10.1136/gut.46.6.813
35. Vasiloglou MF, Fletcher J, Poulia KA. Challenges and perspectives in nutritional counselling and nursing: a narrative review. J Clin Med. 2019;8(9):1489. doi:10.3390/jcm8091489
36. Yap A, Lopez-Olivo MA, Dubowitz J, et al. Anesthetic technique and cancer outcomes: a meta-analysis of total intravenous versus volatile anesthesia. Can J Anesth. 2019;66(5):546–561. doi:10.1007/s12630-019-01330-x
37. Martínez-Ortega AJ, Piñar-Gutiérrez A, Serrano-Aguayo P, et al. Perioperative nutritional support: a review of current literature. Nutrients. 2022;14(8):1601. doi:10.3390/nu14081601
38. Cerantola Y, Grass F, Cristaudi A, Demartines N, Schafer M, Hubner M. Perioperative nutrition in abdominal surgery: recommendations and reality. Gastroenterol Res Pract. 2011;2011:739347. doi:10.1155/2011/739347
39. Kamarajah SK, Bundred J, Tan BH. Body composition assessment and sarcopenia in patients with gastric cancer: a systematic review and meta-analysis. Gastric Cancer. 2019;22(1):10–22. doi:10.1007/s10120-018-0882-2
40. Ramesh HS, Pope D, Gennari R, Audisio RA. Optimising surgical management of elderly cancer patients. World J Surg Oncol. 2005;3(1):17. doi:10.1186/1477-7819-3-17
41. Kearney DE, Liska D, Holubar SD. Preoperative instructions and postoperative care in the 21 st century. Ann Laparoscop Endoscopic Surg. 2019;4. doi:10.21037/ales.2019.08.02
42. Montroni I, Rostoft S, Spinelli A, et al. GOSAFE - Geriatric Oncology Surgical Assessment and Functional Recovery after Surgery: early analysis on 977 patients. J Geriatr Oncol. 2020;11(2):244–255. doi:10.1016/j.jgo.2019.06.017
43. Montroni I, Ugolini G, Saur NM, et al. Personalized management of elderly patients with rectal cancer: expert recommendations of the European Society of Surgical Oncology, European Society of Coloproctology, International Society of Geriatric Oncology, and American College of Surgeons Commission on Cancer. Eur J Surg Oncol. 2018;44(11):1685–1702. doi:10.1016/j.ejso.2018.08.003
44. Saur NM, Davis BR, Montroni I, et al. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the perioperative evaluation and management of frailty among older adults undergoing colorectal surgery. Dis Colon Rectum. 2022;65(4):473–488. doi:10.1097/DCR.0000000000002410
45. El‐Jawahri A, Greer JA, Pirl WF, et al. Effects of early integrated palliative care on caregivers of patients with lung and gastrointestinal cancer: a randomized clinical trial. Oncologist. 2017;22(12):1528–1534. doi:10.1634/theoncologist.2017-0227
46. Jazieh AR, Al Sudairy R, Abulkhair O, et al. Use of complementary and alternative medicine by patients with cancer in Saudi Arabia. J Alternat Complement Med. 2012;18(11):1045–1049. doi:10.1089/acm.2011.0266
47. Grocott MP, Plumb JO, Edwards M, Fecher-Jones I, Levett DZ. Re-designing the pathway to surgery: better care and added value. Perioperat Med. 2017;6(1):1–7. doi:10.1186/s13741-017-0065-4
48. Robson M, Alexopoulou P. Pre-optimisation of the cancer patient. Digest Med Res. 2020;3:29. doi:10.21037/dmr-20-48
49. Alvarez-Nebreda ML, Bentov N, Urman RD, et al. Recommendations for preoperative management of frailty from the Society for Perioperative Assessment and Quality Improvement (SPAQI). J Clin Anesth. 2018;47:33–42. doi:10.1016/j.jclinane.2018.02.011
50. Cooper L, Abbett SK, Feng A, et al. Launching a Geriatric Surgery Center: recommendations from the Society for perioperative assessment and quality improvement. J Am Geriatr Soc. 2020;68(9):1941–1946. doi:10.1111/jgs.16681
51. Gillis C, Li C, Lee L, et al. Prehabilitation versus rehabilitation: a randomized control trial in patients undergoing colorectal resection for cancer. Anesthesiology. 2014;121(5):937–947. doi:10.1097/ALN.0000000000000393
52. Scheede-Bergdahl C, Minnella EM, Carli F. Multi-modal prehabilitation: addressing the why, when, what, how, who and where next? Anaesthesia. 2019;74(Suppl 1):20–26. doi:10.1111/anae.14505
53. Ambe PC, Zarras K, Stodolski M, Wirjawan I, Zirngibl H. Routine preoperative mechanical bowel preparation with additive oral antibiotics is associated with a reduced risk of anastomotic leakage in patients undergoing elective oncologic resection for colorectal cancer. World J Surg Oncol. 2019;17(1):20. doi:10.1186/s12957-019-1563-2
54. Kumar AS, Kelleher DC, Sigle GW. Bowel Preparation before Elective Surgery. Clin Colon Rectal Surg. 2013;26(3):146–152. doi:10.1055/s-0033-1351129
55. Kim YW, Choi EH, Kim IY, Kwon HJ, Ahn SK. The impact of mechanical bowel preparation in elective colorectal surgery: a propensity score matching analysis. Yonsei Med J. 2014;55(5):1273–1280. doi:10.3349/ymj.2014.55.5.1273
56. Chen M, Song X, Chen L-Z, Lin Z-D, Zhang X-I. Comparing mechanical bowel preparation with both oral and systemic antibiotics versus mechanical bowel preparation and systemic antibiotics alone for the prevention of surgical site infection after elective colorectal surgery. Dis Colon Rectum. 2016;59(1):70–78. doi:10.1097/DCR.0000000000000524
57. Gillis C, Wischmeyer PE. Pre-operative nutrition and the elective surgical patient: why, how and what? Anaesthesia. 2019;74(S1):27–35. doi:10.1111/anae.14506
58. Knight SR, Qureshi AU, Drake TM, et al. The impact of preoperative oral nutrition supplementation on outcomes in patients undergoing gastrointestinal surgery for cancer in low- and middle-income countries: a systematic review and meta-analysis. Sci Rep. 2022;12(1):12456. doi:10.1038/s41598-022-16460-4
59. Salas S, Cottet V, Dossus L. Nutritional factors during and after cancer: impacts on survival and quality of life. Nutrients. 2022;14(14):2958. doi:10.3390/nu14142958
60. Meyerhardt JA, Niedzwiecki D, Hollis D, et al. Association of dietary patterns with cancer recurrence and survival in patients with stage III colon cancer. JAMA. 2007;298(7):754–764. doi:10.1001/jama.298.7.754
61. Bargetzi L, Brack C, Herrmann J, et al. Nutritional support during the hospital stay reduces mortality in patients with different types of cancers: secondary analysis of a prospective randomized trial. Ann Oncol. 2021;32(8):1025–1033. doi:10.1016/j.annonc.2021.05.793
62. Akashi Y, Hiki N, Nunobe S, Jiang X, Yamaguchi T. Safe management of anastomotic leakage after gastric cancer surgery with enteral nutrition via a nasointestinal tube. Langenbeck’s Archiv Surg. 2012;397(5):737–744. doi:10.1007/s00423-012-0935-7
63. Mudarra García N, Naranjo Peña I, Olivares Pizarro SP, et al. Pre-surgical nutrition support reduces the incidence of surgical wound complications in oncological patients. Nutr Cancer. 2020;72(5):801–807. doi:10.1080/01635581.2019.1653473
64. Meng Q, Tan S, Jiang Y, et al. Post-discharge oral nutritional supplements with dietary advice in patients at nutritional risk after surgery for gastric cancer: a randomized clinical trial. Clin Nutr. 2021;40(1):40–46. doi:10.1016/j.clnu.2020.04.043
65. Baji DB, Patel JP, Srinivasa NKK, Gande A, Anusha M, Dar H. Nutrition care in cancer surgery patients: a narrative review of nutritional screening and assessment methods and nutritional considerations. Cureus. 2022;14(12). doi:10.7759/cureus.33094
66. Van Cutsem E, Arends J. The causes and consequences of cancer-associated malnutrition. Eur J Oncol Nurs. 2005;9(Suppl 2):S51–S63. doi:10.1016/j.ejon.2005.09.007
67. Nygren J, Thacker J, Carli F, et al. Guidelines for perioperative care in elective rectal/pelvic surgery: enhanced Recovery After Surgery (ERAS®) Society recommendations. Clin Nutr. 2012;31(6):801–816. doi:10.1016/j.clnu.2012.08.012
68. Hyltander A, Warnold I, Edén E, Lundholm K. Effect on whole-body protein synthesis after institution of intravenous nutrition in cancer and non-cancer patients who lose weight. Eur J Cancer. 1991;27(1):16–21. doi:10.1016/0277-5379(91)90051-E
69. Merrick HW, Long CL, Grecos GP, Dennis RS, Blakemore WS. Energy requirements for cancer patients and the effect of total parenteral nutrition. JPEN J Parenter Enteral Nutr. 1988;12(1):8–14. doi:10.1177/014860718801200108
70. Yuill KA, Richardson RA, Davidson HI, Garden OJ, Parks RW. The administration of an oral carbohydrate-containing fluid prior to major elective upper-gastrointestinal surgery preserves skeletal muscle mass postoperatively--a randomised clinical trial. Clin Nutr. 2005;24(1):32–37. doi:10.1016/j.clnu.2004.06.009
71. Hammerlid E, Wirblad B, Sandin C, et al. Malnutrition and food intake in relation to quality of life in head and neck cancer patients. Head Neck. 1998;20(6):540–548. doi:10.1002/(SICI)1097-0347(199809)20:6<540::AID-HED9>3.0.CO;2-J
72. Ajmal M. Role of the acidity (pH) and volume of gastric fluid in obstetric anaesthesia. Eur J Anaesthesiol. 2021;38:200. doi:10.1097/EJA.0000000000001364
73. Akbuğa GA, Başer M. Effect of preoperative oral liquid carbohydrate intake on blood glucose, fasting-thirst, and fatigue levels: a randomized controlled study. Brazilian J Anesthesiol. 2021;71:247–253. doi:10.1016/j.bjane.2021.02.053
74. Longhini F, Bruni A, Garofalo E, et al. Anesthetic strategies in oncological surgery: not only a simple sleep, but also impact on immunosuppression and cancer recurrence. Cancer Manag Res. 2020;12:931–940. doi:10.2147/CMAR.S237224
75. Soltanizadeh S, Degett TH, Gögenur I. Outcomes of cancer surgery after inhalational and intravenous anesthesia: a systematic review. J Clin Anesth. 2017;42:19–25. doi:10.1016/j.jclinane.2017.08.001
76. Cassuto J, Sinclair R, Bonderovic M. Anti-inflammatory properties of local anesthetics and their present and potential clinical implications. Acta Anaesthesiol Scand. 2006;50(3):265–282. doi:10.1111/j.1399-6576.2006.00936.x
77. Cata JP, Hernandez M, Lewis VO, Kurz A. Can regional anesthesia and analgesia prolong cancer survival after orthopaedic oncologic surgery? Clin Orthop Related Res. 2014;472:1434–1441. doi:10.1007/s11999-013-3306-y
78. Fodale V, D’Arrigo MG, Triolo S, Mondello S, La Torre D. Anesthetic techniques and cancer recurrence after surgery. Scientific World J. 2014;2014. doi:10.1155/2014/328513
79. Kehlet H, Wilmore DW. Multimodal strategies to improve surgical outcome. Am J Surg. 2002;183(6):630–641. doi:10.1016/s0002-9610(02)00866-8
80. Yan X, Zhou FX, Lan T, et al. Optimal postoperative nutrition support for patients with gastrointestinal malignancy: a systematic review and meta-analysis. Clin Nutr. 2017;36(3):710–721. doi:10.1016/j.clnu.2016.06.011
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.