Back to Journals » Cancer Management and Research » Volume 18

Perioperative FLOT versus Definitive 50.4 Gy Chemoradiotherapy in Siewert II Esophagogastric Junction Adenocarcinoma: A Multicenter Retrospective Cohort Study
Authors Dinc Sonusen S ![]() , Sucuoglu Isleyen Z
, Sucuoglu Isleyen Z ![]() , Aydin O
, Aydin O ![]() , Erciyestepe M
, Erciyestepe M ![]() , Sakin A, Gurdal N
, Sakin A, Gurdal N ![]() , Urun M, Mermit Ercek B, Bilici M, Gurbuz HS, Gunenc S
, Urun M, Mermit Ercek B, Bilici M, Gurbuz HS, Gunenc S ![]() , Akyel R
, Akyel R ![]() , Celik E, Erturk K
, Celik E, Erturk K ![]() , Atci MM
, Atci MM
Received 21 November 2025
Accepted for publication 10 April 2026
Published 20 April 2026 Volume 2026:18 583473
DOI https://doi.org/10.2147/CMAR.S583473
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Chien-Feng Li
Sermin Dinc Sonusen,1 Zehra Sucuoglu Isleyen,1 Okan Aydin,1 Mert Erciyestepe,1 Abdullah Sakin,1 Necla Gurdal,2 Muslih Urun,3 Berrak Mermit Ercek,3 Mehmet Bilici,4 Halide Sena Gurbuz,4 Senar Gunenc,5 Resit Akyel,6 Emir Celik,1 Kayhan Erturk,1 Muhammed Mustafa Atci1
1Department of Medical Oncology, Prof. Dr. Cemil Tascioglu City Hospital, Istanbul, Turkey; 2Department of Radiation Oncology, Prof. Dr. Cemil Tascioglu City Hospital, Istanbul, Turkey; 3Department of Medical Oncology, Van Yuzuncu Yil University Faculty of Medicine, Van, Turkey; 4Department of Medical Oncology, Ataturk University Faculty of Medicine, Erzurum, Turkey; 5Department of Radiation Oncology, Yedikule Chest Diseases and Chest Surgery Training and Research Hospital, Istanbul, Turkey; 6Department of Nuclear Medicine, Yedikule Chest Diseases and Chest Surgery Training and Research Hospital, Istanbul, Turkey
Correspondence: Sermin Dinc Sonusen, Department of Medical Oncology, Prof. Dr. Cemil Tascioglu City Hospital, Darulaceze Cd. No: 27, Sisli, Istanbul, 34384, Turkey, Tel +90 212 314 55 55, Email [email protected]
Background: Optimal multimodal treatment for esophagogastric junction adenocarcinoma remains debated. While the ESOPEC trial supports perioperative FLOT, real-world evidence is limited, particularly for Siewert type II tumors.
Aim: To compare survival and treatment outcomes of perioperative FLOT versus definitive-dose chemoradiotherapy in non-metastatic Siewert II esophagogastric junction adenocarcinoma.
Methods: Siewert type II esophagogastric junction adenocarcinoma was defined as tumors with an epicenter located between 1 cm above and 2 cm below the esophagogastric junction. We retrospectively identified patients with non-metastatic Siewert type II esophagogastric junction adenocarcinoma treated between January 2015 and December 2024 at three tertiary cancer centers. Patients received either perioperative FLOT chemotherapy or concurrent chemoradiotherapy with weekly carboplatin–paclitaxel and 50.4 Gy radiotherapy, delivered as definitive therapy or neoadjuvantly prior to planned surgery. Clinical characteristics, treatment delivery, pathological response, survival outcomes, and treatment-related toxicities were analyzed.
Results: Seventy patients were included (FLOT, n=50; concurrent chemoradiotherapy, n=20). Surgery was performed in 45/50 (90%) FLOT patients and 7/20 (35%) concurrent chemoradiotherapy patients, representing a major difference between treatment groups. Median follow-up was 53.7 months. Median overall survival was 43.0 months in the FLOT group and 48.6 months in the concurrent chemoradiotherapy group (p=0.498). Median event-free survival was 34.2 months and 35.0 months, respectively (p=0.548). No pathological complete response occurred in the FLOT group; one patient (14.3%) in the concurrent chemoradiotherapy group achieved pathological complete response. Grade 3– 4 toxicities were more frequent with FLOT (26% vs. 5%). Distant relapse was the predominant recurrence pattern in both groups.
Conclusion: Despite a substantial difference in surgical resection rates between groups, perioperative FLOT and concurrent chemoradiotherapy showed comparable survival outcomes in this real-world cohort of patients with Siewert type II EGJ adenocarcinoma. These findings should be interpreted with caution, as treatment selection and baseline differences may have influenced outcomes. Treatment decisions should be individualized based on patient characteristics and clinical context.
Plain Language Summary: Siewert type II esophagogastric junction adenocarcinoma is a challenging disease with limited real-world comparative data. In this multicenter study, we compared two common treatment approaches: perioperative FLOT chemotherapy and chemoradiotherapy using a standard, full-course radiation treatment (50.4 Gy). Despite higher surgical rates in the FLOT group, survival outcomes were comparable between the two strategies. Pathological complete response was rare, and distant metastasis was the most common pattern of recurrence. FLOT was associated with higher grade 3– 4 toxicities. These findings suggest that treatment should be individualized, and that organ-preserving approaches such as chemoradiotherapy may be a reasonable option for selected patients with Siewert type II EGJ adenocarcinoma in clinical practice.
Keywords: esophagogastric junction, siewert type II, FLOT, chemoradiotherapy, adenocarcinoma
Introduction
According to GLOBOCAN 2022, esophageal cancer ranks as the eleventh most common malignancy worldwide, with approximately 511,000 new cases and 445,000 deaths annually.1 Esophageal cancer comprises two main histological subtypes: adenocarcinoma and squamous cell carcinoma.2 The predominance of each subtype varies according to geographic region, etiological factors, and tumor location.2
Esophagogastric junction (EGJ) cancer represents a relatively uncommon entity, typically manifesting as adenocarcinoma, and is managed as either esophageal or gastric cancer depending on its anatomical location.3,4 The Siewert classification categorizes EGJ adenocarcinomas into three subtypes: type I, arising 1–5 cm above the EGJ; type II, centered between 1 cm above and 2 cm below the EGJ; and type III, originating 2–5 cm below the EGJ with invasion of the junction.3,4 Siewert type I and II tumors are staged and managed according to esophageal cancer protocols, whereas Siewert type III tumors are classified and treated as gastric cancer.5,6
Locally advanced resectable EGJ adenocarcinomas are treated with multimodal strategies combining systemic therapy, radiotherapy (RT), and surgery in various sequences to optimize oncologic outcomes. The MAGIC trial established the role of perioperative chemotherapy by demonstrating that perioperative epirubicin, cisplatin, and fluorouracil (ECF) significantly improved survival compared with surgery alone.7 This benefit was further enhanced by the FLOT4-AIO trial, which showed that perioperative fluorouracil, leucovorin, oxaliplatin, and docetaxel (FLOT) improved overall survival compared with ECF, thereby setting a new standard of care.8 In parallel, the CROSS trial demonstrated a survival advantage with neoadjuvant concurrent chemoradiotherapy (CCRT) followed by surgery in patients with esophageal and EGJ tumors.9 More recently, the Phase III ESOPEC trial directly compared these two strategies and found that perioperative FLOT conferred a significant overall survival benefit over neoadjuvant CCRT.10
However, Siewert type II tumors represent a particularly challenging subgroup because they lie at the anatomical interface between the distal esophagus and the proximal stomach, resulting in ongoing debate regarding the optimal treatment strategy. Consequently, these tumors may be managed according to either esophageal or gastric cancer treatment paradigms in clinical practice. Moreover, Siewert type II tumors have been underrepresented in large prospective trials, and real-world data directly comparing perioperative FLOT and CCRT approaches remain limited. In a subset of patients unable to tolerate perioperative chemotherapy or who decline surgery, definitive CCRT continues to represent a valid alternative, supported by the long-term outcomes of the landmark RTOG 85–01 trial.11 In recent years, several retrospective real-world studies have also examined distal esophageal, EGJ, and gastric cardia tumors, further supporting the applicability of multimodal treatment strategies in routine clinical practice.12,13 More recently, the integration of immunotherapy into multimodal treatment strategies has further reshaped the therapeutic landscape of EGJ adenocarcinoma. Trials such as CheckMate-577 and MATTERHORN have demonstrated improved disease-free survival and pathological response rates with the addition of immune checkpoint inhibitors in selected settings.14,15
Therefore, this multicenter retrospective study aimed to compare real-world outcomes in patients with non-metastatic (localized and locally advanced) Siewert type II EGJ adenocarcinoma treated with perioperative FLOT versus definitive or preoperative CCRT.
Methods
Patient Selection
The medical records of patients newly diagnosed with distal esophageal or EGJ adenocarcinoma between January 2015 and December 2024 were retrospectively reviewed at three tertiary oncology centers. Eligibility criteria included histopathologically confirmed EGJ adenocarcinoma classified as Siewert type II; clinical stage cT2N0, cT1b-cT2 N+ or cT3-cT4a with any N disease without evidence of distant metastasis; age ≥ 18 years; and planned treatment with either perioperative FLOT or CCRT, administered as definitive therapy or as neoadjuvant treatment prior to planned surgery. Staging procedures included endoscopic ultrasound, contrast-enhanced computed tomography (CT) of the chest, abdomen, and pelvis, fluorodeoxyglucose positron emission tomography (FDG-PET), and diagnostic laparoscopy. Patients were excluded if they had a concurrent active malignancy or a history of prior chemotherapy or radiotherapy.
Perioperative FLOT
The perioperative FLOT regimen consisted of docetaxel 50 mg/m2, oxaliplatin 85 mg/m2, leucovorin 200 mg/m2, and 5-fluorouracil 2600 mg/m2 administered as a continuous 24-hour intravenous infusion. All agents were administered on day 1 of each 14-day cycle. Treatment was planned for a total of eight cycles (four preoperative and four postoperative), whenever feasible. Granulocyte colony-stimulating factor (G-CSF) was routinely prescribed as primary prophylaxis for all patients in this group.
Concurrent Chemoradiotherapy
In the CCRT group, all patients underwent CT simulation in the supine position with a slice thickness of 3 mm for radiotherapy planning. The gross tumor volume was defined based on the primary tumor and involved lymph nodes identified on imaging modalities and PET-CT. The clinical target volume was defined by expanding the gross tumor volume, with additional margins of 3–4 cm in the craniocaudal direction and 1–1.5 cm in the axial plane to encompass areas at risk of microscopic tumor spread, including submucosal longitudinal extension, and a planning target volume was subsequently generated by adding appropriate margins to account for setup uncertainties and internal organ motion. For the lymphatic regions, the clinical target volume included metastatic lymph nodes as well as the relevant regional lymphatic drainage areas according to tumor location and extent, including the periesophageal, lower mediastinal, perigastric, and/or celiac lymphatics. The determination of these margins was based on established protocols that consider anatomical site–specific patterns of microscopic spread as well as organ and tumor motion related to swallowing, respiration, and other physiological movements. Treatment planning was performed using volumetric-modulated arc therapy (VMAT), with strict adherence to dose–volume constraints for organs at risk. Radiotherapy was delivered using a RapidArc–Trilogy linear accelerator (Varian Medical Systems, Palo Alto, CA, USA) to a total dose of 50.4 Gy in 1.8 Gy daily fractions. Concurrent chemotherapy consisted of weekly paclitaxel 50 mg/m2 and carboplatin at an area under the curve (AUC) of 2, administered intravenously on day 1 of each treatment week during the 5-week course of radiotherapy. Neoadjuvant or definitive CCRT was administered according to clinical indication, and surgery was performed in eligible patients following neoadjuvant therapy.
Assessment of Staging, Treatment Response, and Toxicity
Demographic, clinical, and treatment-related data, including clinical stage, treatment modality (FLOT or CCRT), performance status (PS), comorbidities, surgical status, postoperative pathological stage (ypTNM), postoperative treatments, and recurrence status were collected from electronic medical records. PS was evaluated using the Eastern Cooperative Oncology Group (ECOG) performance scale.16 Tumor staging was based on the 8th edition (2017) of the American Joint Committee on Cancer (AJCC) TNM classification.17
The primary objective of this study was to compare overall survival (OS) between patients with non-metastatic, operable Siewert type II EGJ adenocarcinoma treated with perioperative FLOT or CCRT. OS was calculated from the date of diagnosis to death or last follow-up. Secondary objectives included comparisons of event-free survival (EFS), objective response rate (ORR), pathological complete response (pCR) rate, and treatment-related toxicities between the two treatment groups. EFS was defined as the time from initiation of first-line anticancer therapy (chemotherapy in the FLOT group or chemoradiotherapy in the CCRT group) to radiologically confirmed disease recurrence or death, whichever occurred first.
Tumor response was assessed using contrast-enhanced CT of the chest and abdomen and 18F-FDG PET according to the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1 and the PET Response Criteria in Solid Tumors (PERCIST).18,19 Tumor responses were categorized as complete response (CR), partial response (PR), stable disease (SD), or progressive disease (PD). The ORR was defined as the combined rate of CR and PR.20,21
In both treatment groups, pathological tumor regression was graded using the modified Ryan system.22 This system classifies response as Grade 0 (no viable cancer cells; complete response), Grade 1 (single cells or rare small groups of cancer cells; near complete response), Grade 2 (residual cancer with evidence of tumor regression; partial response), or Grade 3 (extensive residual cancer with no evident tumor regression; poor or no response). pCR was defined as Grade 0, indicating the absence of viable tumor cells in both the primary tumor and regional lymph nodes. Pathological assessments were performed by experienced local pathologists at each participating center according to institutional practice.
During treatment, patients in the perioperative FLOT group were evaluated by a physician every two weeks, whereas patients in the CCRT group were assessed weekly throughout the course of chemoradiotherapy. After completion of treatment, patients were followed at 3-month intervals, provided that no disease progression or new clinical symptoms were detected. Follow-up evaluations included clinical assessment (medical history and physical examination), complete blood count, serum biochemistry tests, and carcinoembryonic antigen (CEA) levels, as well as contrast-enhanced CT of the thorax, abdomen, and pelvis. Positron emission tomography (PET-CT) was performed when clinically indicated.
Treatment-related toxicities were defined as adverse events occurring during or after treatment that were considered at least possibly related to the administered therapy and were graded according to the Common Terminology Criteria for Adverse Events (CTCAE), version 5.0. Grade 3–4 treatment-related toxicities of interest included hematologic (neutropenia, anemia, thrombocytopenia) and non-hematologic adverse events such as esophagitis, nausea/vomiting, diarrhea, and fatigue. Toxicities were managed according to institutional clinical practice, including dose modifications, treatment delays, and supportive care as appropriate.
Statistical Analysis
Statistical analyses were conducted using IBM SPSS Statistics software. Continuous variables were reported as median (range) or mean ± standard deviation, categorical variables as frequencies and percentages. Survival curves were estimated using the Kaplan–Meier method and compared using the Log rank test. Univariate and multivariate Cox proportional hazards regression analyses were performed to identify factors associated with EFS and OS. Variables with a p-value <0.20 in univariate analysis were included in the multivariate model. Hazard ratios (HRs) with 95% confidence intervals (CIs) were calculated. Statistical significance was set at two-tailed p < 0.05. The statistical methods of this study were reviewed by an independent biomedical statistician. Given the retrospective design of the study, potential treatment-selection bias was considered. Due to the relatively limited sample size, particularly in the CCRT group, advanced weighting methods such as inverse-probability-of-treatment weighting (IPTW) or standardized mortality ratio weighting (SMRW) were not applied, as these approaches may yield unstable estimates in small cohorts. Therefore, survival outcomes were analyzed using conventional methods and interpreted with caution.
Results
Baseline Characteristics
A total of 100 potentially eligible patients were screened. Thirty patients with Siewert type I or III tumors were excluded, leaving 70 patients diagnosed between January 2015 and December 2024 for inclusion in the final analysis. Among them, 50 patients (71.4%) received perioperative chemotherapy, while 20 patients (28.6%) were treated with CCRT. Baseline characteristics are summarized in Table 1.
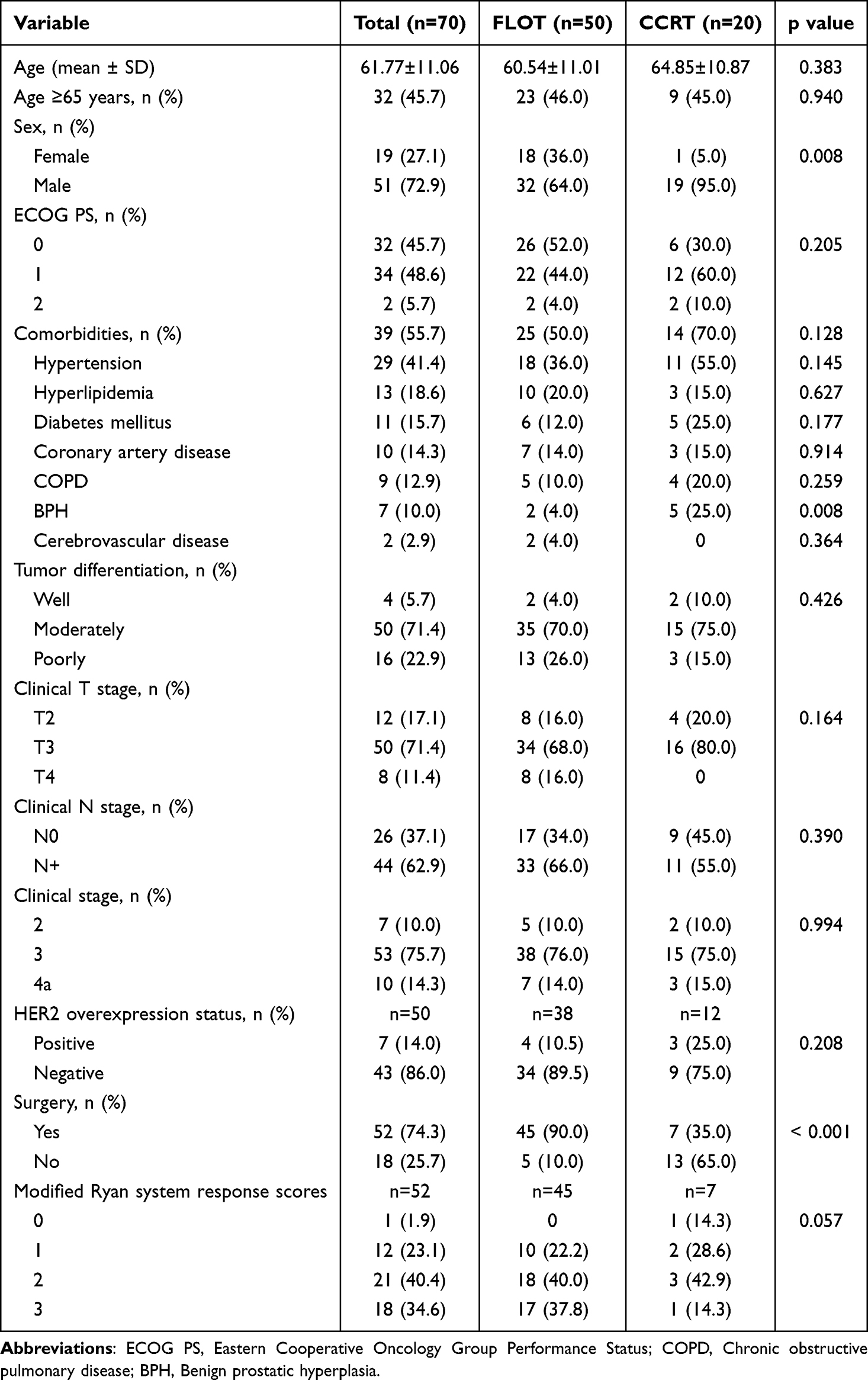 |
Table 1 Baseline Demographic, Clinicopathologic Characteristics and Pathological Response Rates |
Patients in the CCRT group were, on average, older than those in the perioperative FLOT group. The proportion of patients with an ECOG-PS of 0 was higher in the FLOT group, whereas most patients in the CCRT group had a PS of 1. Comorbidities were also more common in the CCRT group. However, there were no statistically significant differences between the groups in terms of mean age, proportion of patients aged ≥65 years, ECOG-PS, or comorbidity status. Similarly, no significant differences were observed regarding tumor differentiation, clinical T stage, clinical N stage, or overall clinical stage.
Treatment Information
In the perioperative FLOT group, five patients did not undergo surgery. Among them, two experienced disease progression after four cycles of chemotherapy, one declined surgery despite completing eight cycles, one was deemed inoperable due to congestive heart failure and an abdominal aortic aneurysm, and one died from COVID-19 pneumonia after completing eight cycles.
Among the 45 patients who underwent surgery in the perioperative FLOT group, 35 completed the planned perioperative treatment (eight cycles of FLOT and surgery). Seven patients completed all eight cycles preoperatively. In the postoperative setting, five patients were unable to complete chemotherapy due to toxicity or deterioration in performance status, and one discontinued treatment because of disease progression. Based on pathological findings, one patient with inadequate treatment response and two patients with positive surgical margins received postoperative chemoradiotherapy instead of completing perioperative FLOT. In total, six patients received postoperative chemoradiotherapy.
In the CCRT group, all patients received definitive-dose radiotherapy. Seven subsequently underwent surgery, while 13 were managed non-surgically following completion of CCRT. One patient achieved a pCR. Of the six without pCR, one received adjuvant nivolumab and another received six cycles of adjuvant XELOX; the remaining four were followed up without adjuvant treatment.
Response Rates
In surgically treated patients, treatment response was radiologically assessed using thoracoabdominal CT and/or FDG-PET prior to surgery, whereas in non-surgical CCRT patients, evaluations were performed following treatment completion. The results are summarized in Table 2.
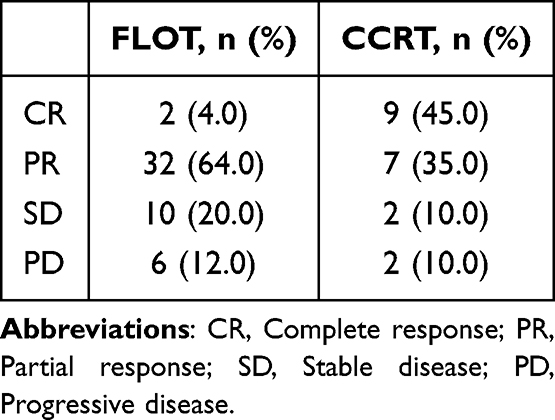 |
Table 2 Radiologic Response to Neoadjuvant Treatment |
In the perioperative FLOT group, radiologic response rates were as follows: CR in 4%, PR in 64%, SD in 20%, and PD in 12%. In the CCRT group, CR was observed in 45%, PR in 35%, SD in 10%, and PD in 10%. The rate of radiologic CR was notably higher in the CCRT group. The ORR was 68% for perioperative FLOT and 80% for CCRT (p = 0.315).
The distributions of clinical and pathological stages are summarized in Table 3. Among patients who underwent surgery, none in the FLOT group achieved pCR, whereas one of seven patients (14.3%) in the CCRT group achieved pCR. According to the modified Ryan tumor regression grading system, the proportions of Grades 0, 1, 2 and 3 in the perioperative FLOT group were 0%, 22.2%, 40.0% and 37.8%, respectively, compared with 14.3%, 28.6%, 42.9% and 14.3% in the CCRT group (p = 0.057).
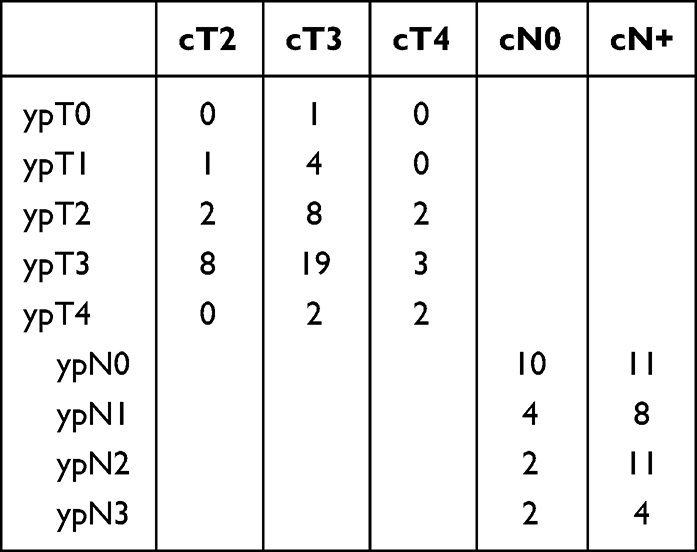 |
Table 3 Distribution of Clinical and Pathological Stages |
Survival Analysis
The median follow-up duration was 53.7 months. The median OS was 43.0 months (95% CI, 3.85–82.15) in the perioperative FLOT group and 48.6 months (95% CI, 5.48–91.72) in the CCRT group (p = 0.498). The median EFS was 34.2 months (95% CI, 2.33–78.49) for FLOT and 35.0 months (95% CI, 2.43–70.27) for CCRT (p = 0.548). No statistically significant differences were observed between the two groups for either OS or EFS.
Kaplan–Meier survival curves for OS and EFS are presented in Figures 1 and 2. The 12-, 24- and 36-month OS rates were 95%, 72% and 52% in the FLOT group, compared with 75%, 58% and 51% in the CCRT group, respectively. The 12-, 24- and 36-month EFS rates were 80%, 57% and 48% in the FLOT group, and 70%, 54% and 47% in the CCRT group. The OS and EFS rates for both groups at 12-, 24- and 36-months are summarized in Figure 3.
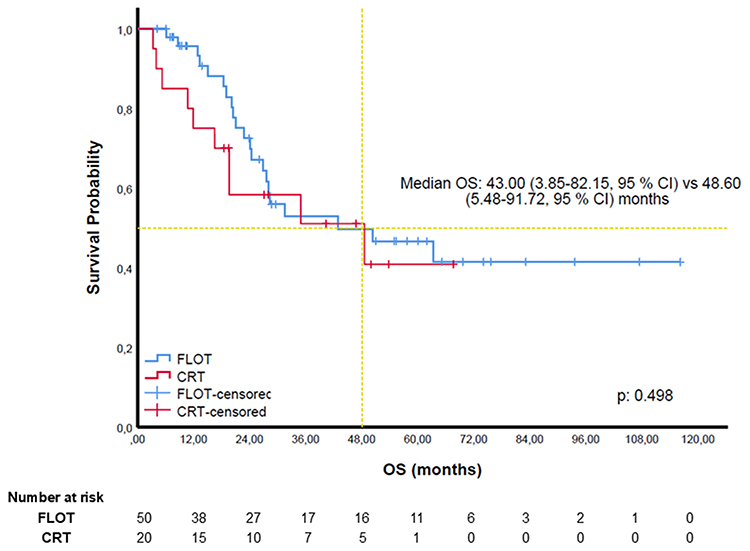 |
Figure 1 Kaplan–Meier overall survival (OS) curves comparing perioperative FLOT versus CCRT in patients with Siewert type II esophagogastric junction adenocarcinoma. Median OS: 43.0 vs 48.6 months (p = 0.498). Abbreviations: OS, overall survival; CI, confidence interval; FLOT, fluorouracil/leucovorin/oxaliplatin/docetaxel; CCRT, concurrent chemoradiotherapy. |
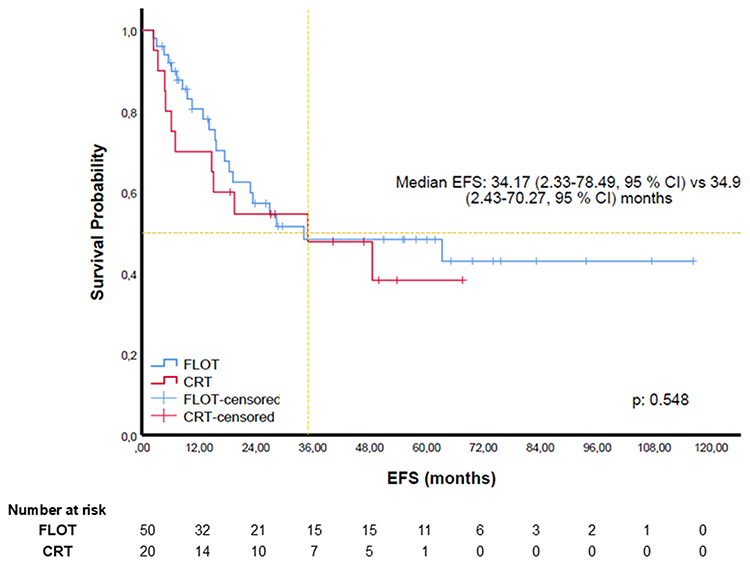 |
Figure 2 Kaplan–Meier event-free survival (EFS) curves comparing perioperative FLOT and CCRT. Median EFS: 34.17 vs 34.97 months (p = 0.548). Abbreviations: EFS, event-free survival; CI, confidence interval; FLOT, fluorouracil/leucovorin/oxaliplatin/docetaxel; CCRT, concurrent chemoradiotherapy. |
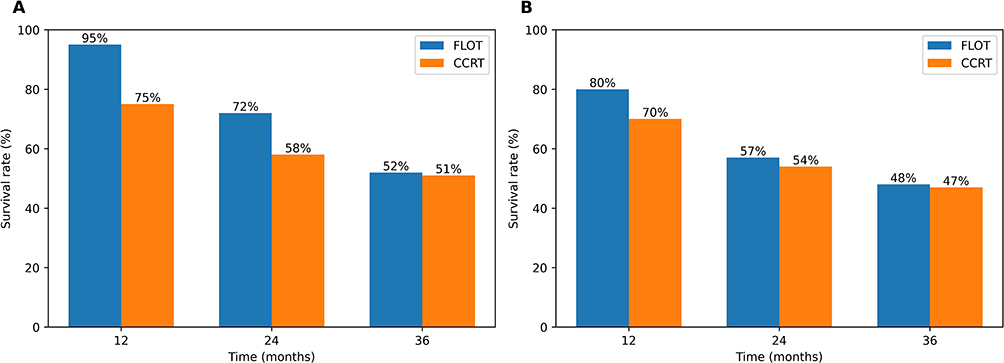 |
Figure 3 (A) One-, two-, and three-year overall survival (OS) rates for each treatment cohort. (B) One-, two-, and three-year event-free survival (EFS) rates for each treatment cohort. Abbreviations: OS, overall survival; EFS, event-free survival; FLOT, fluorouracil/leucovorin/oxaliplatin/docetaxel; CCRT, concurrent chemoradiotherapy. |
To further evaluate factors associated with survival outcomes, univariate and multivariate Cox proportional hazards regression analyses were performed for both EFS and OS (Table 4). In the multivariate analysis for EFS, male sex (HR: 2.85, 95% CI: 1.08–7.52, p = 0.035), ECOG performance status 1–2 (HR: 2.34, 95% CI: 1.05–5.21, p = 0.037), and advanced clinical stage (stage 3: HR: 5.94, p = 0.017; stage 4a: HR: 18.36, p = 0.011) were independently associated with worse EFS. For OS, ECOG performance status 1–2 (HR: 2.25, 95% CI: 1.00–5.06, p = 0.049) and clinical stage 4a (HR: 12.44, 95% CI: 1.37–112.81, p = 0.025) remained independent predictors of poorer survival. Treatment modality (perioperative FLOT vs. CCRT) was not independently associated with either EFS (HR: 0.71, p = 0.424) or OS (HR: 0.80, p = 0.621).
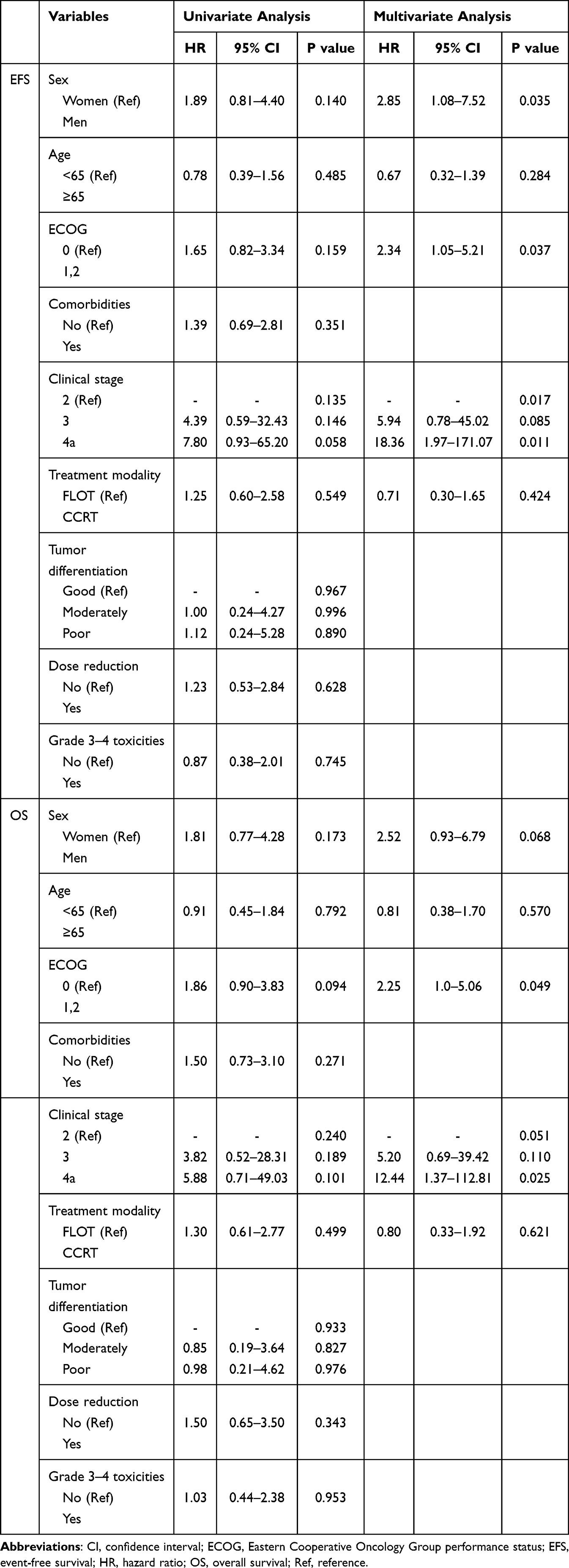 |
Table 4 Univariate and Multivariate Cox Regression Analyses for Event-Free Survival and Overall Survival |
Recurrence
In the perioperative FLOT group, recurrence occurred in 27% of the 45 surgically treated patients. In the CCRT group, recurrence was observed in 42% of the 7 patients who underwent surgery and in 38% of the 13 patients managed non-surgically. Among patients with recurrence, distant metastases accounted for 93.3% of relapses in the FLOT group and 75.0% in the CCRT group. Although the CCRT group exhibited a numerically higher rate of locoregional relapse, the overall recurrence patterns did not differ significantly between the groups (p = 0.214). Among patients who developed recurrence, 30.4% did not receive any subsequent treatment.
Treatment-Related Toxicities
Treatment-related toxicities are summarized in Table 5. When all-grade adverse events were considered, no statistically significant differences were observed between the two groups, except for diarrhea and peripheral neuropathy, which were significantly more frequent in the perioperative FLOT group. Esophagitis occurred in two patients in the CCRT group.
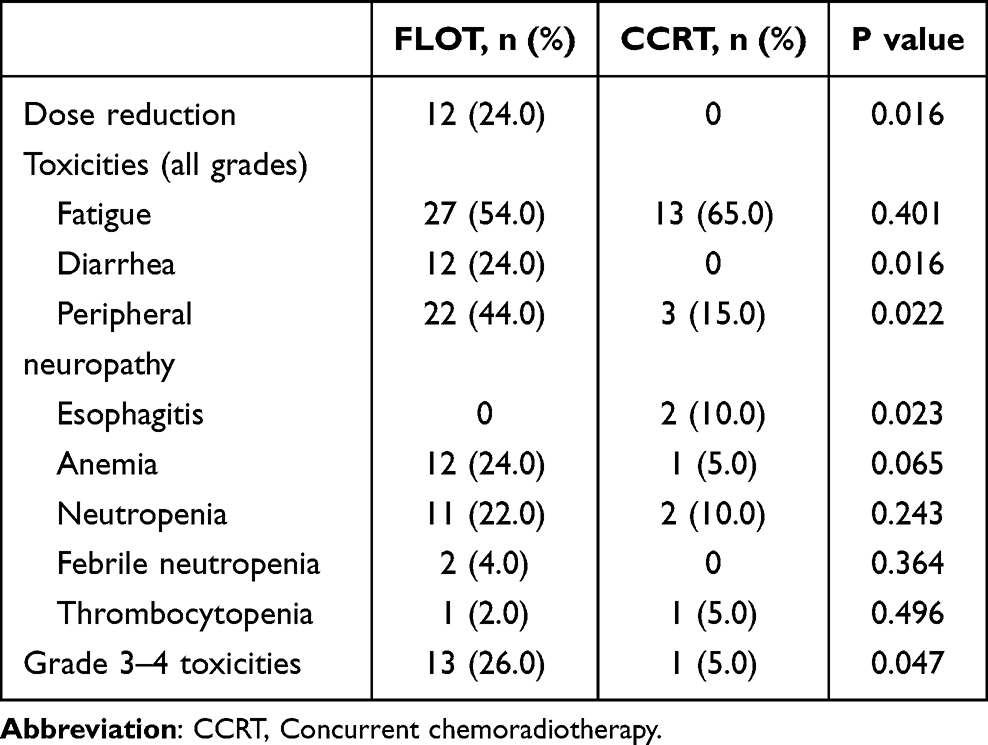 |
Table 5 Distribution of Treatment-Related Toxicities |
Dose reductions were required in 24% of patients in the perioperative FLOT group. Grade 3–4 toxicities occurred significantly more often in the FLOT group compared with the CCRT group (26% vs. 5%).
Discussion
In this multicenter retrospective study of patients with locally advanced, resectable Siewert type II EGJ adenocarcinoma, we found no significant difference in survival outcomes between perioperative FLOT and either definitive or preoperative CCRT. The median OS was 43.0 months in the FLOT group versus 48.6 months in the CCRT group (p = 0.498), while the median EFS was 34.2 and 35.0 months, respectively (p = 0.548). Although a higher proportion of patients in the FLOT cohort underwent surgery (45/50 compared with 7/20 in the CCRT cohort), none achieved a pCR, whereas one patient (14.3%) in the CCRT surgery subgroup did. Notably, grade 3–4 treatment-related toxicities were significantly more frequent with FLOT, reflecting the higher intensity and cumulative burden of the perioperative chemotherapy regimen.
When reviewing the literature, we observed that most real-world studies on chemoradiotherapy included both adenocarcinoma and squamous cell carcinoma histologies, and that tumor location often varied between perioperative chemotherapy and chemoradiotherapy cohorts.12,13,23 This heterogeneity in histopathology and anatomical distribution can complicate the interpretation of comparative outcomes across retrospective studies. To reduce confounding and allow a more accurate assessment of therapeutic strategies, our study focused exclusively on Siewert type II adenocarcinoma, thereby ensuring a more homogeneous cohort both anatomically and biologically.
Several retrospective real-world studies have reported comparable survival outcomes between perioperative FLOT and CROSS-based chemoradiotherapy in esophageal and EGJ adenocarcinomas.12,13,23 However, the phase III ESOPEC trial demonstrated a clear survival advantage with perioperative FLOT over preoperative chemoradiotherapy (66 months vs. 37 months, respectively).10 Approximately one-third of the ESOPEC trial participants had Siewert type II tumors. While multiple retrospective and randomized studies have compared perioperative chemotherapy and neoadjuvant chemoradiotherapy in esophageal or EGJ adenocarcinoma, data focusing specifically on Siewert type II tumors treated with a definitive 50.4 Gy chemoradiotherapy backbone remain limited. Our cohort, therefore, provides valuable real-world data in this distinct subgroup. The pronounced survival advantage observed in ESOPEC was not replicated in our real-world cohort, likely due to differences in study design, patient selection, sample size, and treatment delivery. A recent multicenter retrospective study similarly demonstrated improved survival with perioperative FLOT compared to CROSS-based chemoradiotherapy in patients with cT2N0 esophageal and EGJ adenocarcinoma, though that analysis was limited to patients who underwent surgery.24
The pCR rate in our cohort was also lower than those reported in major prospective trials. In FLOT4-AIO, pCR was achieved in approximately 16% of patients receiving perioperative FLOT, whereas the CROSS trial reported a 23% pCR rate among patients with esophageal or EGJ adenocarcinoma treated with preoperative chemoradiotherapy.8,9 Likewise, ESOPEC documented pCR rates of 16.7% for FLOT and 10.1% for CROSS-type chemoradiotherapy.10 It is important to emphasize that these trials compared perioperative FLOT with preoperative chemoradiotherapy delivered according to the CROSS protocol. In contrast, clinical practice in our region more commonly employs a definitive-dose chemoradiotherapy approach using 50.4 Gy rather than the 41.4 Gy neoadjuvant regimen used in CROSS. Consequently, our findings reflect real-world treatment patterns and provide insights into outcomes with a higher-dose radiation backbone, which is frequently adopted outside of trial settings. In addition, the observed difference in pCR rates between the CCRT and perioperative FLOT groups (14.3% vs 0%) should be interpreted with caution. The retrospective design of the study and the limited sample size may have contributed to an overestimation of this difference. In addition, variability in the interval between neoadjuvant treatment and surgery, as well as differences in surgical specimen handling and pathological assessment across centers, may have further influenced pCR outcomes.
Although the 50.4 Gy regimen used in our CCRT cohort (1.8 Gy daily fractions) could theoretically improve local control, current evidence shows that escalating the dose beyond 41.4 Gy does not provide a survival advantage when surgery follows. Several retrospective analyses have reported comparable pCR and survival outcomes between neoadjuvant 41.4 Gy and 50.4 Gy regimens.25,26 Unlike the CROSS and ESOPEC populations—where most patients proceeded to surgery—65% of our CCRT group ultimately did not undergo resection, effectively receiving definitive chemoradiotherapy. This difference in treatment intent may partially explain why the median OS in our CCRT cohort (48.6 months) was numerically higher than that of the ESOPEC CROSS arm (37.0 months), despite a lower surgical resection rate.9,10
Although the ESOPEC trial strongly supports perioperative FLOT in this patient population, our findings contribute to growing real-world evidence suggesting comparable survival outcomes between perioperative FLOT and chemoradiotherapy.10,12,13 The similar survival observed with both strategies in our study should be interpreted with caution, as treatment selection was likely influenced by baseline patient characteristics such as frailty, comorbidities, and surgical fitness. Therefore, the apparent comparability of outcomes may partly reflect treatment-selection bias rather than true equivalence between treatment modalities. Importantly, treatment modality was not identified as an independent predictor of survival in multivariate analysis, suggesting that survival outcomes in this cohort may be more strongly driven by baseline patient and disease characteristics rather than treatment strategy alone. CCRT may serve as an organ-preserving strategy for patients who are unfit for surgery or who decline surgical intervention. However, the long-term oncologic outcomes of organ preservation remain uncertain, and such approaches should be reserved for carefully selected cases. Therefore, multidisciplinary tumor board discussions remain essential when determining the optimal management strategy, considering overall patient status, surgical fitness, and tumor features.
With regard to toxicity, grade 3–4 adverse events were more frequent in the perioperative FLOT group compared with the CCRT group. In the FLOT arm, 70% of patients were able to complete the entire course of treatment (eight cycles plus surgery), whereas all patients in the CCRT group completed their planned regimen (with or without surgery). These findings align with previous randomized controlled trials. In both the FLOT4-AIO and ESOPEC trials, approximately half of patients completed all eight planned FLOT cycles,8,10 whereas treatment completion rates were notably higher in the chemoradiotherapy arms of ESOPEC and CROSS.9,10
This study has several limitations. An important methodological consideration is the imbalance in surgical rates between the treatment groups. A substantially higher proportion of patients in the perioperative FLOT group underwent surgery compared with those in the CCRT group (90% vs 35%), likely reflecting differences in baseline patient characteristics such as frailty, comorbidities, and surgical fitness rather than treatment effect alone. Consequently, our analysis represents a comparison of treatment strategies rather than directly comparable modalities, introducing treatment-selection bias and limiting the comparability of outcomes. Importantly, this comparison should not be interpreted as an evaluation of equivalent preoperative strategies, but rather as a comparison of two distinct clinical treatment pathways reflecting differences in treatment intent and patient fitness. Therefore, survival results should be interpreted with caution and should not be considered as evidence of causal superiority. The limited sample size and relatively short follow-up may also reduce statistical power and increase the risk of Type II error. Larger studies are needed to confirm these findings. In addition, pathological response assessment was performed locally without central blinded review, which may have introduced variability, although a standardized modified Ryan grading system was used. Finally, inclusion of patients treated prior to the integration of immunotherapy may limit generalizability. In recent years, phase III trials have demonstrated that integrating immunotherapy into multimodal treatment strategies can further enhance clinical outcomes. The MATTERHORN trial showed that adding durvalumab to perioperative FLOT significantly increased pCR rates and yielded a meaningful improvement in EFS.14 Similarly, the CheckMate-577 study demonstrated that one year of adjuvant nivolumab following neoadjuvant chemoradiotherapy and surgery significantly prolonged disease-free survival in patients with residual disease, including both esophageal and EGJ adenocarcinomas.15 These emerging data suggest that immunotherapy-based multimodal regimens may redefine the standard of care in this disease setting.
Conclusion
In this real-world study, perioperative FLOT and definitive 50.4 Gy chemoradiotherapy showed comparable survival in Siewert II EGJ adenocarcinoma. However, these findings should be interpreted within the context of a non-randomized cohort with a high proportion of patients not undergoing surgery in the CCRT group and the use of a definitive-dose (50.4 Gy) radiotherapy approach, introducing potential surgical selection bias. Notably, despite a substantially lower resection rate in the CCRT group, survival outcomes remained comparable, which may support the feasibility of organ-preserving strategies in selected patients. Therefore, the observed comparable survival should not be generalized to populations treated according to CROSS or ESOPEC protocols, where treatment strategies and surgical rates differ substantially. Individualized multidisciplinary decision-making remains essential to balance organ preservation, treatment tolerance, and long-term outcomes in the era of immunotherapy. For patients who decline surgery, or are unfit for surgical intervention, definitive 50.4 Gy chemoradiotherapy continues to represent a meaningful and clinically relevant treatment option.
Strobe Statement
This study was conducted and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement.
Abbreviations
AUC, area under the curve; AJCC, American Joint Committee on Cancer; CCRT, concurrent chemoradiotherapy; CEA, carcinoembryonic antigen; CI, confidence interval; CR, complete response; CROSS, Chemoradiotherapy for Oesophageal Cancer Followed by Surgery; CT, computed tomography; CTCAE, Common Terminology Criteria for Adverse Events; ECOG, Eastern Cooperative Oncology Group; ECF, epirubicin, cisplatin, fluorouracil; EGJ, esophagogastric junction; EFS, event-free survival; FDG-PET, fluorodeoxyglucose positron emission tomography; FLOT, fluorouracil, leucovorin, oxaliplatin, docetaxel; G-CSF, granulocyte colony-stimulating factor; Gy, gray; HR, hazard ratio; ORR, objective response rate; OS, overall survival; pCR, pathological complete response; PD, progressive disease; PET-CT, positron emission tomography–computed tomography; PERCIST, PET Response Criteria in Solid Tumors; PR, partial response; PS, performance status; RECIST, Response Evaluation Criteria in Solid Tumors; RT, radiotherapy; SD, stable disease; TNM, tumor, node, metastasis; VMAT, volumetric-modulated arc therapy; XELOX, capecitabine plus oxaliplatin.
Data Sharing Statement
The datasets generated and analyzed during the current study are not publicly available due to institutional restrictions but are available from the corresponding author upon reasonable request.
Ethical Approval
This retrospective study was approved by the Prof. Dr. Cemil Tascioglu City Hospital Ethics Committee (Approval No: 25.08.2025/203). The requirement for informed consent was waived due to the retrospective nature of the study. All patient data were anonymized and handled confidentially. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the 1964 Helsinki Declaration and its later amendments.
Consent for Publication
No identifying patient information is included in this manuscript; therefore, consent for publication was not required.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for this research.
Disclosure
The authors declare that they have no financial or non-financial competing interests.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74:229–14. doi:10.3322/caac.21834
2. Arnold M, Ferlay J, Van Berge MI, Soerjomataram I. Global burden of oesophageal and gastric cancer by histology and subsite in 2018. Gut. 2020;69:1564–1571. doi:10.1136/gutjnl-2020-321600
3. Li J, Wang QB, Liang YB, et al. Tumor-associated lymphatic vessel density is a reliable biomarker for prognosis of esophageal cancer after radical resection: a systemic review and meta-analysis. Front Immunol. 2024;15:1453482. doi:10.3389/fimmu.2024.1453482
4. Miao W, Feng Y, Jiang B, et al. Projections of esophageal cancer incidence trend in Jiangsu Province, China: a Bayesian modeling study. J Natl Cancer Cent. 2024;5:149–155. doi:10.1016/j.jncc.2024.11.004
5. Siewert JR, Stein HJ. Classification of adenocarcinoma of the oesophagogastric junction. Br J Surg. 1998;85:1457–1459. doi:10.1046/j.1365-2168.1998.00940.x
6. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®). Esophageal and Esophagogastric Junction Cancers. Version 4.2025. National Comprehensive Cancer Network. Available from: https://www.nccn.org/professionals/physician_gls/pdf/esophageal.pdf.
7. Cunningham D, Allum WH, Stenning SP, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med. 2006;355:11–20. doi:10.1056/NEJMoa055531
8. Al-Batran SE, Homann N, Pauligk C, et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): a randomised, Phase 2/3 trial. Lancet. 2019;393:1948–1957. doi:10.1016/S0140-6736(18)32557-1
9. Van Hagen P, Hulshof MC, Van Lanschot JJB, et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med. 2012;366:2074–2084. doi:10.1056/NEJMoa1112088
10. Hoeppner J, Brunner T, Schmoor C, et al. Perioperative chemotherapy or preoperative chemoradiotherapy in esophageal cancer. N Engl J Med. 2025;392:323–335. doi:10.1056/NEJMoa2409408
11. Herskovic A, Martz K, Al-Sarraf M, et al. Combined chemotherapy and radiotherapy compared with radiotherapy alone in patients with cancer of the esophagus. N Engl J Med. 1992;326:1593–1598. doi:10.1056/NEJM199206113262403
12. Shahnam A, Nindra U, McNamee N, et al. Real-world outcomes of FLOT versus CROSS regimens for patients with oesophagogastric cancers. Gastrointest Tumors. 2023;10:19–28. doi:10.1159/000531536
13. Wonglhow J, Wong HL, Duong C, et al. Real-World Outcomes Between Perioperative Chemotherapy (FLOT) and Preoperative Concurrent Chemoradiotherapy (CROSS) in Localized Esophageal and Esophagogastric Junction Adenocarcinoma: a Retrospective Cohort Study. Cancers. 2025;17. doi:10.3390/cancers17182962
14. Janjigian YY, Al-Batran SE, Wainberg ZA, et al. Perioperative durvalumab in gastric and gastroesophageal junction cancer. N Engl J Med. 2025;393:217–230. doi:10.1056/NEJMoa2503701
15. Kelly RJ, Ajani JA, Kuzdzal J, et al. Adjuvant nivolumab in resected esophageal or gastroesophageal junction cancer. N Engl J Med. 2021;384:1191–1203. doi:10.1056/NEJMoa2032125
16. Oken MM, Creech RH, Tormey DC, et al. Toxicity and response criteria of the Eastern cooperative oncology group. Am J Clin Oncol. 1982;5:649–655.
17. Amin MB, Greene FL, Edge SB, et al. The Eighth Edition AJCC Cancer Staging Manual: continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J Clin. 2017;67:93–99. doi:10.3322/caac.21388
18. Subbiah V, Chuang HH, Gambhire D, Kairemo K. Defining clinical response criteria and early response criteria for precision oncology: current state-of-the-art and future perspectives. Diagnostics. 2017;7. 10.3390/diagnostics7010010.
19. Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45:228–247. doi:10.1016/j.ejca.2008.10.026
20. Li J, Liang YB, Wang QB, et al. Rechallenge with immune checkpoint inhibitors in patients with hepatocellular carcinoma: a narrative review. Liver Cancer. 2025. doi:10.1159/000549355
21. Kudo M, Ueshima K, Tsuchiya K, et al. Primary analysis of a Phase II study of atezolizumab plus bevacizumab for TACE-unsuitable patients with tumor burden beyond up-to-seven criteria in intermediate-stage hepatocellular carcinoma: REPLACEMENT study. Liver Cancer. 2025;15:104–116. doi:10.1159/000546899
22. Ryan R, Gibbons D, Hyland JMP, et al. Pathological response following long-course neoadjuvant chemoradiotherapy for locally advanced rectal cancer. Histopathology. 2005;47:141–146. doi:10.1111/j.1365-2559.2005.02176.x
23. Karadag I, Karakaya S, Ates O, Berna O, Oksuzoglu C. CROSS or FLOT in distal esophageal and gastroesophageal cancer. J Coll Physicians Surg Paki. 2021;31:326–329. doi:10.29271/jcpsp.2021.03.326
24. Wirsik NM, Schmidt T, Kooij CD, et al. Comparison of pretreatment strategies for cT2cN0 staged adenocarcinoma of the esophagus and the gastroesophageal junction: a european high-volume center cohort analysis. Ann Surg Oncol. 2025;32:10128–10136. doi:10.1245/s10434-025-18311-8
25. Haltmeier T, Brazerol J, Borbely Y, et al. Preoperative chemoradiotherapy for esophageal or gastroesophageal junction cancer: results from a retrospective study using extended CROSS regimen. Radiat Oncol. 2025;20:71. doi:10.1186/s13014-025-02637-4
26. Nehlsen AD, Lehrer EJ, Resende-Salgado L, Rosenzweig KE, Buckstein M. Comparison of pathologic complete response rates and oncologic outcomes in patients with surgically resectable esophageal cancer treated with neoadjuvant chemoradiation to 50.4 Gy vs 41.4 Gy. Cureus. 2021;13:e19233. doi:10.7759/cureus.19233
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.