Back to Journals » Drug Design, Development and Therapy » Volume 19
Perioperative Dexmedetomidine Exposure and One-Year Mortality Risk After Video-Assisted Thoracoscopic Surgery: A Multi-Institutional Study
Authors Hung KC ![]() , Chang LC, Lai YC, Wu JY
, Chang LC, Lai YC, Wu JY ![]() , Chen IW
, Chen IW ![]()
Received 12 August 2025
Accepted for publication 18 November 2025
Published 25 November 2025 Volume 2025:19 Pages 10495—10506
DOI https://doi.org/10.2147/DDDT.S560044
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Solomon Tadesse Zeleke
Kuo-Chuan Hung,1,2 Li-Chen Chang,3 Yi-Chen Lai,1,2 Jheng-Yan Wu,4 I-Wen Chen5
1Department of Anesthesiology, Chi Mei Medical Center, Tainan, Taiwan; 2School of Medicine, College of Medicine, National Sun Yat-sen University, Kaohsiung, Taiwan; 3Department of Anesthesiology, E-Da Hospital, I-Shou University, Kaohsiung, Taiwan; 4Department of Nutrition, Chi Mei Medical Center, Tainan, Taiwan; 5Department of Anesthesiology, Chi Mei Medical Center, Liouying, Tainan, Taiwan
Correspondence: I-Wen Chen, Department of Anesthesiology, Chi Mei Medical Center, Liouying, Tainan, Taiwan, Tel +886-6-281-2811, Fax +886-6-283-3806, Email [email protected]
Purpose: To evaluate the association between perioperative dexmedetomidine exposure and one-year mortality risk following video-assisted thoracoscopic surgery (VATS).
Patients and Methods: We conducted a multi-institutional retrospective cohort study using the TriNetX Research Network. Adult patients aged ≥ 18 years who underwent elective VATS between January 2010 and December 2024 were included in the study. Patients were categorized into dexmedetomidine or midazolam (control) groups based on perioperative medication exposure. Midazolam was selected as the active comparator as it represents a standard perioperative sedative with different pharmacological properties than dexmedetomidine. After applying the exclusion criteria, 1:1 propensity score matching was performed using demographic variables, comorbidities, and laboratory parameters. The primary outcome was all-cause mortality within one year; and the secondary outcome was overall major complications (composite of sepsis, acute respiratory failure, acute myocardial infarction, cerebral infarction, and acute kidney failure).
Results: After propensity matching, 6387 patients were included in each group with balanced baseline characteristics. Patients receiving dexmedetomidine had significantly lower one-year mortality compared to midazolam (4.1% vs 5.4%; hazard ratio [HR]: 0.80, 95% confidence interval [CI]: 0.68– 0.94; p=0.007). This mortality difference was observed during the later follow-up period (31– 365 days: HR:0.80; p=0.008) rather than the early postoperative period (1– 30 days: HR:0.89; p=0.695). No difference was observed in overall major complications between groups (12.7% each; HR 1.05; p=0.289). Sensitivity and subgroup analyses confirmed these findings.
Conclusion: Perioperative dexmedetomidine administration is associated with reduced one-year mortality following VATS compared to midazolam. The mortality benefit appears during the later follow-up period without differences in major complication rates. Future prospective randomized trials are needed to confirm these findings and determine optimal dosing strategies.
Keywords: dexmedetomidine, video-assisted thoracoscopic surgery, mortality, perioperative care, thoracic surgery, propensity score matching
Introduction
Video-assisted thoracoscopic surgery (VATS) has revolutionized thoracic surgical practice by offering patients a minimally invasive alternative to traditional open thoracotomy procedures, fundamentally changing how surgeons approach complex intrathoracic pathologies.1–3 This technological advancement allows for smaller incisions, reduced tissue trauma, and faster recovery times than conventional open approaches.4,5 Despite significant advances in surgical techniques, enhanced recovery protocols, and perioperative care optimization, VATS still carries substantial mortality risks, with 90-day mortality rates ranging from 2.5% to 12.05%.6–8 The choice of perioperative anesthetic agent plays a crucial role in patient outcomes, as these medications can influence hemodynamic stability, inflammatory responses, stress hormone release, and overall physiological resilience during the critical perioperative period.9–12 Understanding how different anesthetic agents affect both short-term recovery and long-term survival has become increasingly important as clinicians strive to optimize patient care and reduce mortality risk following thoracic surgery through evidence-based medication selection.
Dexmedetomidine, a highly selective alpha-2 adrenergic receptor agonist, has emerged as an intriguing perioperative medication with properties that extend beyond traditional sedation and anesthesia.13,14 Unlike conventional sedatives such as midazolam, dexmedetomidine offers unique pharmacological benefits, including sympatholytic effects, anti-inflammatory properties, and potential organ-protective mechanisms.14–16 These characteristics may theoretically translate into improved patient outcomes by reducing perioperative stress responses, minimizing inflammatory cascades, and preserving end-organ function during surgical procedures. Clinical evidence also supports these potential benefits. A Bayesian meta-analysis of 44 RCTs found improved postoperative quality of recovery and reduced chronic pain, albeit with increased bradycardia and hypotension.17 In a meta-analysis of 31 studies, perioperative dexmedetomidine reduced 30-day mortality, the incidence of delirium, atrial fibrillation, and cardiac arrest in cardiac surgery patients, although the benefits were less pronounced in noncardiac surgery.18 A large cohort study also linked its use to improved 5-year survival after cardiac surgery.19
Current evidence suggests that perioperative dexmedetomidine may reduce pain, anesthetic consumption, and improve pulmonary outcomes, such as lowering the incidence of atelectasis and hypoxemia in patients undergoing thoracoscopic and thoracic surgery.20,21 Despite these potential benefits, no large-scale study has specifically evaluated its effect on mortality after VATS. Patients undergoing VATS are particularly susceptible to perioperative pulmonary complications, hemodynamic fluctuations, and heightened sympathetic stress responses due to one-lung ventilation and surgical manipulation of thoracic structures. These physiological challenges make this population especially relevant for evaluating the potential organ-protective and sympatholytic properties of dexmedetomidine. We hypothesized that perioperative dexmedetomidine use is associated with improved long-term survival compared to midazolam use in patients undergoing VATS. Therefore, this multi-institutional study aimed to address these knowledge gaps by employing a propensity-matched design to compare one-year mortality outcomes between patients receiving perioperative dexmedetomidine versus midazolam during VATS procedures.
Methods
Study Design and Data Source
We conducted a multi-institutional, longitudinal, retrospective cohort study utilizing the TriNetX Research Network, a global federated health research platform that provides access to de-identified electronic health records from participating healthcare organizations. This real-world dataset enables access to a wide range of structured clinical information, including patient demographics, diagnoses, procedures, laboratory results, and medication prescriptions, across diverse healthcare settings. The TriNetX platform ensures patient privacy by removing all patient identifiers while maintaining data integrity for research purposes. This platform has been extensively validated and widely used for clinical research across multiple medical disciplines.22–25
As the data were fully de-identified and involved a retrospective analysis of existing medical records, informed consent was not required. This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki and was approved by the Institutional Review Board of Chi Mei Medical Center (IRB number: 11406-E02), which granted a waiver for informed consent in compliance with the observational research regulations.
Study Population and Inclusion Criteria
This study included adult patients aged 18 years and older who underwent elective VATS between January 1, 2010, and December 31, 2024. The index date was defined as the date of the thoracoscopic procedure. Patients were categorized into two groups based on perioperative medication exposure: the dexmedetomidine (DEX) group comprised patients who received dexmedetomidine on the same index date, while the control group consisted of patients who received midazolam on the same index date. Midazolam was selected as the comparator because it represents a commonly used benzodiazepine sedative in perioperative anesthesia practice. Unlike dexmedetomidine, which provides both sedative and sympatholytic effects, midazolam lacks α2-adrenergic activity and serves as an appropriate active control to isolate the potential survival benefit associated with unique pharmacological profile of dexmedetomidine.
Exclusion Criteria
To strengthen internal validity and minimize confounding bias, we applied a series of prespecified exclusion criteria. First, patients with any documented diagnosis of COVID-19, corrected QT interval prolongation (>500ms), sepsis, acute kidney injury, acute respiratory failure, critical care service utilization, or end-stage renal disease within one month prior to the index date were excluded to ensure that study participants had relatively stable baseline conditions. Second, individuals with a documented history of heart transplantation, cardiac surgery, pacemaker implantation, or ventricular arrhythmias at any time prior to the index date were excluded to eliminate patients with significant preexisting cardiovascular interventions that could confound mortality outcomes. Third, to exclude patients undergoing emergency procedures, we excluded those who had visited the emergency department within three days prior to surgery. To reduce misclassification bias and ensure that dexmedetomidine exposure was truly perioperative rather than related to postoperative intensive care unit management, we excluded patients who received dexmedetomidine between postoperative days 2–14.
Data Collection and Variable Definitions
Patient characteristics and clinical information were extracted from electronic medical records spanning two years prior to the index date. Demographic variables included age at surgery, sex, race/ethnicity, and body mass index. Comorbidity data encompassed cardiovascular diseases (eg, ischemic heart disease, hypertension, heart failure, and myocardial infarction), cerebrovascular disease, diabetes mellitus, chronic obstructive respiratory diseases, chronic kidney disease, liver disease, and malignancy. The laboratory parameters collected included hemoglobin levels, glycated hemoglobin (HbA1c), serum albumin concentrations, and C-reactive protein.
Propensity Score Matching
To minimize selection bias and balance baseline characteristics between the treatment groups, we employed propensity score matching using a 1:1 ratio with a greedy nearest-neighbor approach without replacement. The propensity model incorporated demographic variables (age, sex, race, and body mass index), comorbidity profiles (Supplementary Table 1), and laboratory parameters as matching variables. Considering that baseline inflammation status may be associated with mortality risk, we specifically included C-reactive protein (CRP) levels as a matching variable. The effectiveness of propensity score matching was assessed using standardized mean differences (SMDs), with values <0.1 considered indicative of adequate balance between cohorts. Propensity score distributions were visually examined to verify appropriate overlap between the groups.
Outcome Definitions
The primary outcome was all-cause mortality within one year following the index surgical procedure. The secondary outcomes included the overall risk of major complications. Overall major complications were defined as a composite endpoint, including sepsis (ICD-10 code A41), acute respiratory failure (J96.0), acute and chronic respiratory failure (J96.2), acute myocardial infarction (I21), cerebral infarction (I63), and acute kidney failure (N17).
To provide temporal granularity, outcome events were stratified into early and late onset, defined as those occurring within 1–30 days and 31–365 days post-surgery, respectively. This stratification allows for differentiation between immediate perioperative complications and longer-term adverse events potentially related to surgical intervention or anesthetic management.
Sensitivity Analyses
To evaluate the robustness of our findings and address potential confounding factors, we conducted two prespecified sensitivity analyses. The first sensitivity analysis excluded patients who received perioperative blood transfusion, defined as transfusion occurring within one week following surgery, to eliminate the potential impact of transfusion-related complications on patient outcomes. The second sensitivity analysis excluded patients with preoperative anemia to address this important prognostic factor. These sensitivity analyses were designed specifically to account for the well-established association between anemia and blood transfusion as potential predictors of postoperative morbidity and mortality, ensuring that our primary findings were not confounded by hematologic factors that could independently influence patient outcomes following thoracic surgery.
Statistical Analysis
Descriptive analyses were employed to characterize the baseline demographic and clinical features of the study population. Continuous variables are presented as means with standard deviations (SDs), while categorical variables are summarized using frequencies and percentages. The effectiveness of propensity score matching was evaluated by calculating the SMDs between matched cohorts. For time-to-event outcomes, Kaplan-Meier survival curves were constructed and compared using the Log rank test to assess differences in event-free survival between the treatment groups. Cox proportional hazards regression models were applied to estimate hazard ratios (HRs) and assess the risk of outcomes over time after matching for selected covariates, including demographics, comorbidities, and laboratory variables. Additionally, multivariate Cox proportional hazards regression was used to identify independent risk factors for 1-year mortality, adjusting for relevant demographics (eg, age) and comorbidities (eg, anemia, malnutrition).
Subgroup analyses were performed to explore potential effect modification by clinically relevant patient characteristics, specifically age (18–65 years versus ≥66 years), sex (male versus female), and the presence of malignant lung cancer (yes vs no) for one-year mortality. All statistical procedures were executed using the built-in analytical functions of the TriNetX research platform, ensuring the reproducibility and standardization of the analytical approaches. To evaluate the robustness of the observed associations to potential unmeasured confounding, an E-value analysis was performed for the one-year mortality outcome. The E-value represents the minimum strength of association that an unmeasured confounder would need to have with both the exposure and the outcome, above and beyond measured covariates, to fully explain the observed effect estimate.26
Results
Patient Selection and Baseline Characteristics
The patient selection process using the TriNetX database is illustrated in Figure 1. After excluding patients with significant comorbidities that could confound mortality outcomes (eg, recent COVID-19 infections, critical care utilization, or major cardiovascular interventions prior to surgery), we successfully identified 34,248 patients who underwent VATS with either dexmedetomidine (DEX group, n=6390) or midazolam exposure (control group, n=27858). Before matching, there were notable imbalances between the DEX and control groups, as evidenced by the distinct propensity score distributions (Figure 2). However, after implementing 1:1 propensity score matching, we achieved an excellent covariate balance with 6387 patients in each group, and the propensity score distributions showed substantial overlap, indicating successful matching (Figure 2). The baseline characteristics after matching revealed a well-balanced cohort (Table 1). Both groups had similar mean ages (approximately 58 years), with a slightly higher number of female patients. Importantly, the prevalence of major comorbidities was well balanced between the groups, including neoplasms (66.0% vs 64.7%), essential hypertension (43.5% vs.42.0%), and lung malignancy (34.6% vs 33.9%). The standardized mean differences for all variables were below 0.1, confirming adequate balance.
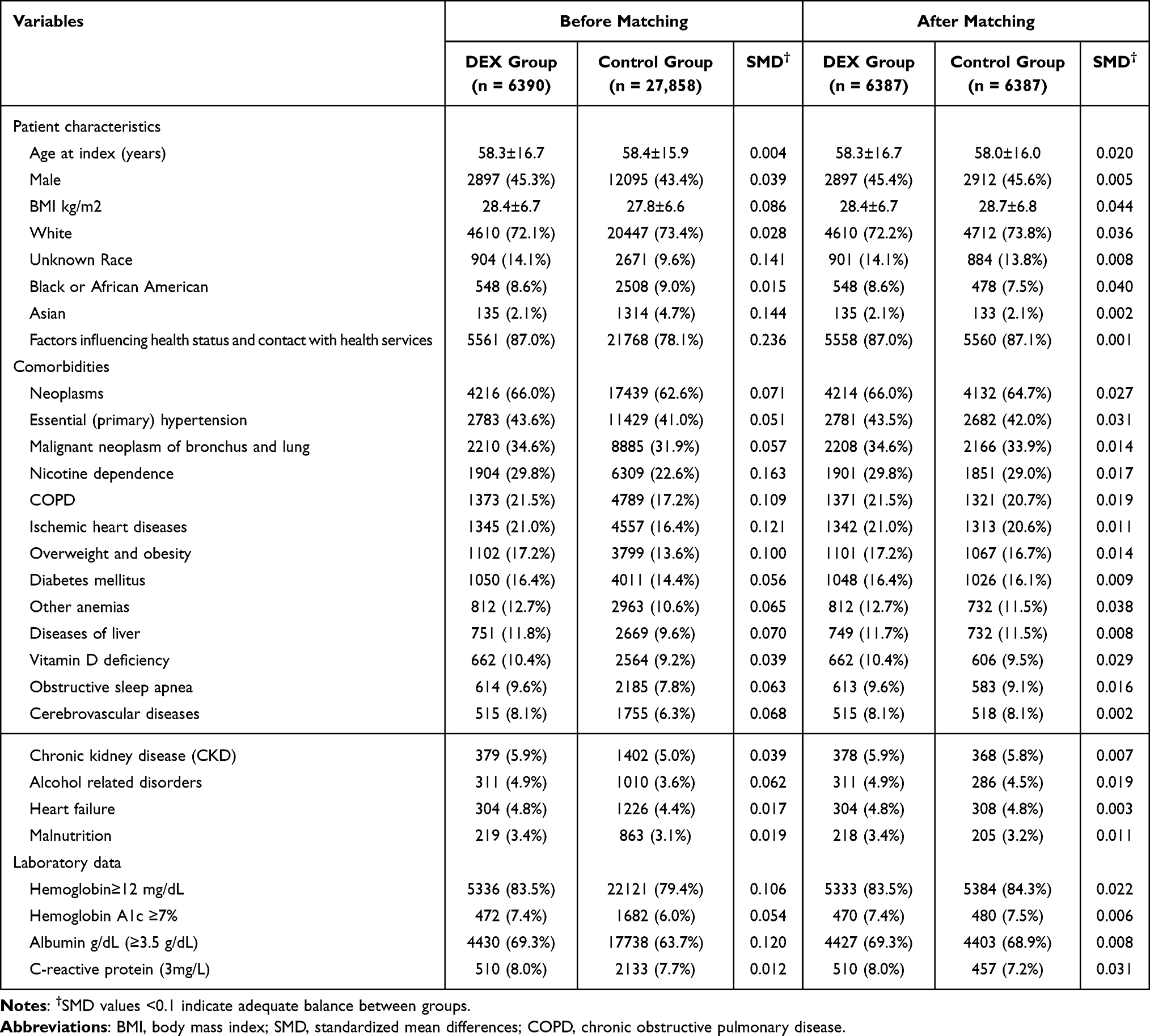 |
Table 1 Baseline Characteristics of Patients Before and After Propensity Score Matching |
 |
Figure 1 Patient selection flowchart from the TriNetX database. The flowchart illustrates the systematic exclusion process applied to identify eligible patients using dexmedetomidine (DEX group) or midazolam (control group). Abbreviations: HCOs, Healthcare Organizations; VATS, video-assisted thoracoscopic surgery. |
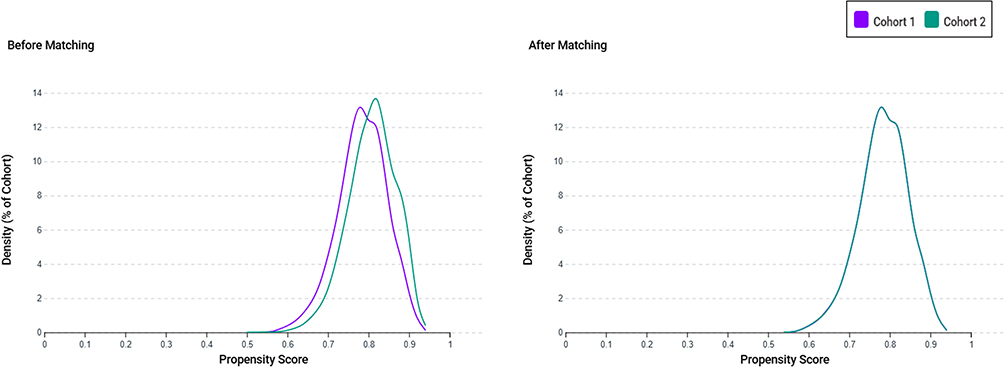 |
Figure 2 Propensity score density distributions before and after matching. The left panel shows the distribution of propensity scores between the dexmedetomidine (DEX) group (Cohort 1, purple) and the control group (Cohort 2, green) before matching, indicating a noticeable imbalance. The right panel shows improved overlap and covariate balance after 1:1 propensity score matching using age, sex, race, laboratory data, and comorbidities. |
Association Between Dexmedetomidine Exposure and 1-Year Outcomes
The primary analysis demonstrated a statistically significant association between perioperative dexmedetomidine exposure and improved 1-year survival (Table 2). Patients receiving dexmedetomidine had a 20% lower risk of 1-year mortality than those receiving midazolam (4.1% vs 5.4%; HR 0.80, 95% CI 0.68–0.94; p=0.007). In the E-value analysis for one-year mortality, the E-value was 1.81 for the point estimate and 1.32 for the lower limit of the 95% CI, suggesting that an unmeasured confounder would need to have a relatively strong association with both dexmedetomidine use and mortality to nullify the observed association. Temporal stratification of the mortality data revealed that this survival benefit did not emerge in the early postoperative period (1–30 days: HR 0.89; p=0.695) but became evident during the later follow-up interval (31–365 days: HR 0.80; p=0.008). This delayed effect suggests that the benefit of dexmedetomidine may not lie in mitigating immediate postoperative complications, but rather in promoting long-term physiological recovery. Notably, dexmedetomidine did not reduce the overall 1-year incidence of major complications (12.7% in both groups; HR, 1.05; p=0.289).
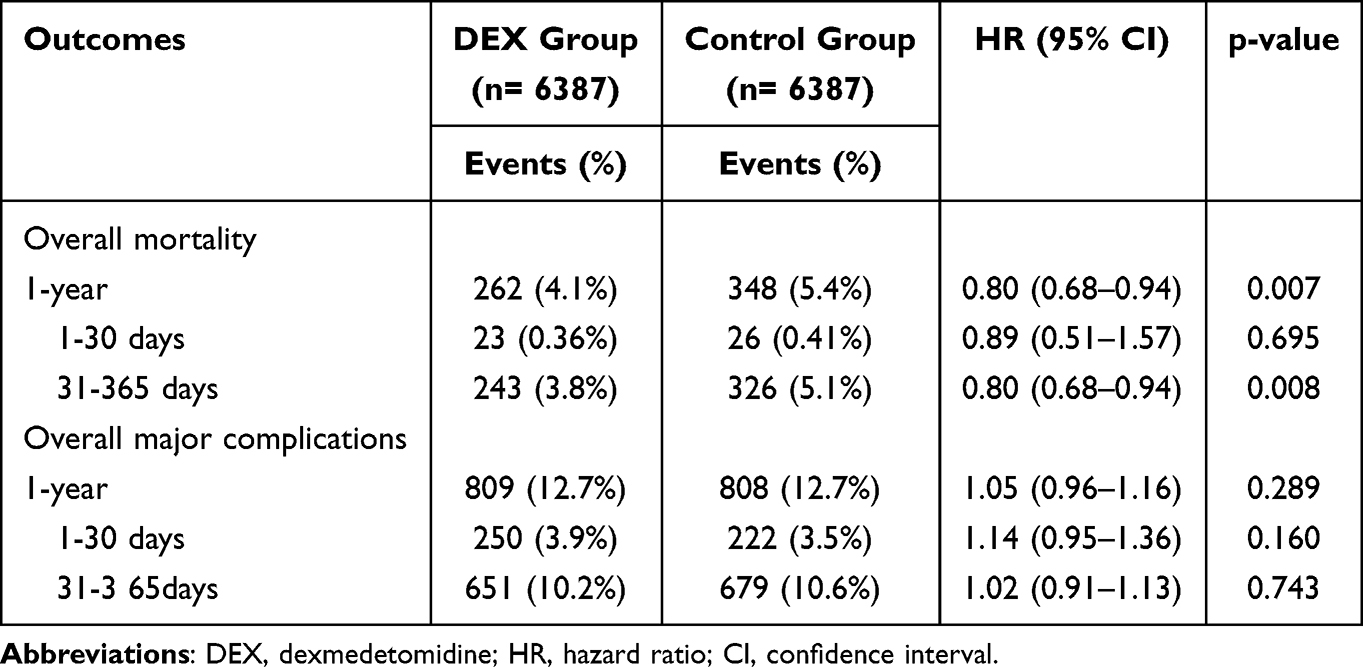 |
Table 2 Association Between Dexmedetomidine and 1-year Risk of Mortality Following Thoracic Surgery |
Sensitivity Analyses
The robustness of our primary findings was supported by two prespecified sensitivity analyses designed to address potential confounding factors (Table 3). First, after excluding patients who received perioperative blood transfusions (n=6332 per group), the mortality benefit associated with dexmedetomidine became more pronounced, with a 23% reduction in 1-year mortality (HR 0.77, 95% CI 0.66–0.91; p=0.001). This strengthened association suggests that the primary findings are not confounded by transfusion-related complications and may underestimate the true protective effect of dexmedetomidine. Second, when patients with preoperative anemia were excluded (n=5685 per group), the protective effect of dexmedetomidine persisted (HR 0.80, 95% CI 0.67–0.96; p=0.018). Importantly, in this anemia-free subgroup, a significant reduction in early mortality was observed (1–30 days: HR, 0.52; p=0.021), indicating that dexmedetomidine may confer additional short-term survival benefits in patients without anemia. Together, these sensitivity analyses confirm that the observed association between dexmedetomidine and improved survival is not driven by confounding from perioperative transfusion or preoperative anemia, two well-established risk factors for adverse postoperative outcomes. The consistency of the findings across multiple analytic strategies enhances the validity and credibility of the observed protective effects.
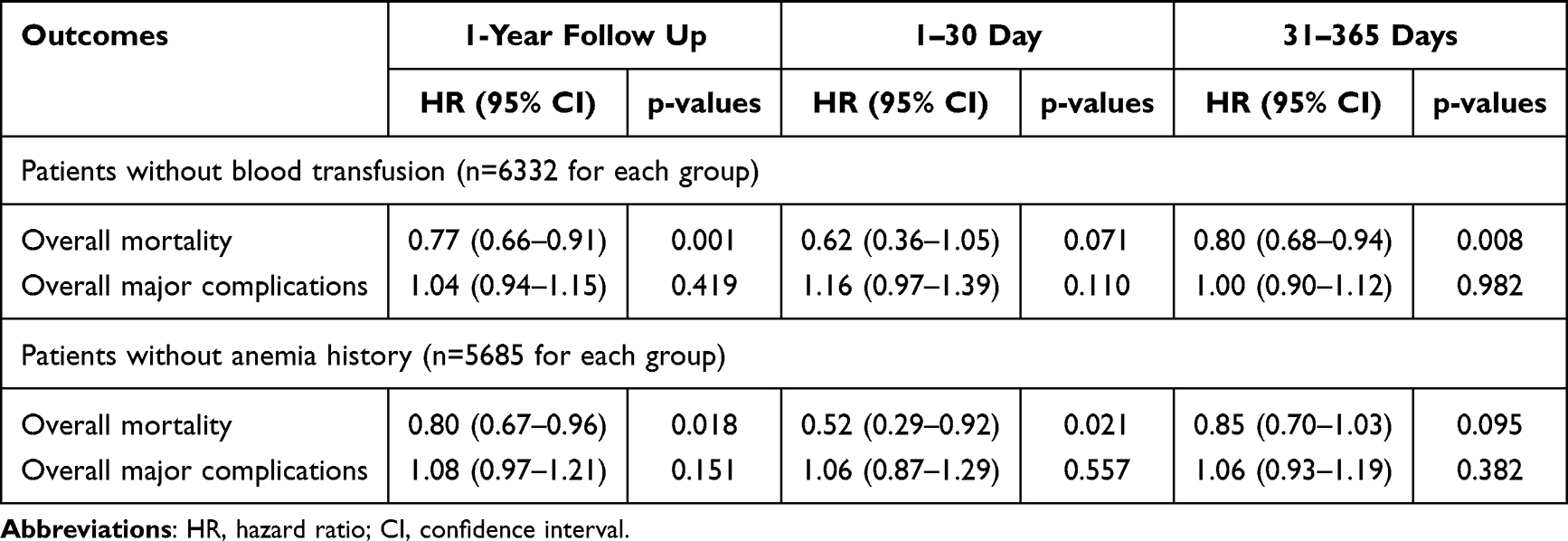 |
Table 3 Sensitivity Analysis |
Subgroup Analysis
Subgroup analyses were conducted to evaluate whether the survival benefit of dexmedetomidine varied among clinically relevant populations (Table 4). No statistically significant interaction effects were detected, indicating that the protective effect of dexmedetomidine was consistent across all the examined subgroups. Although male patients (HR 0.71, p = 0.002) appeared to derive a greater benefit than female patients (HR 0.79, p = 0.086), the non-significant interaction p-value (p = 0.556) indicates that this difference is likely attributable to chance. Similarly, both younger (18–65 years: HR 0.81, p=0.144) and older patients (>66 years: HR 0.75, p=0.003) experienced comparable benefits, with an interaction p-value of 0.675. Among patients with lung malignancy (HR 0.67, p<0.001) and those without (HR 0.83, p=0.084), no significant effect modification was observed (interaction p=0.193). These findings confirm that the protective effect of dexmedetomidine is broadly applicable across sex, age, and cancer status, supporting its use in a wide range of patients undergoing VATS.
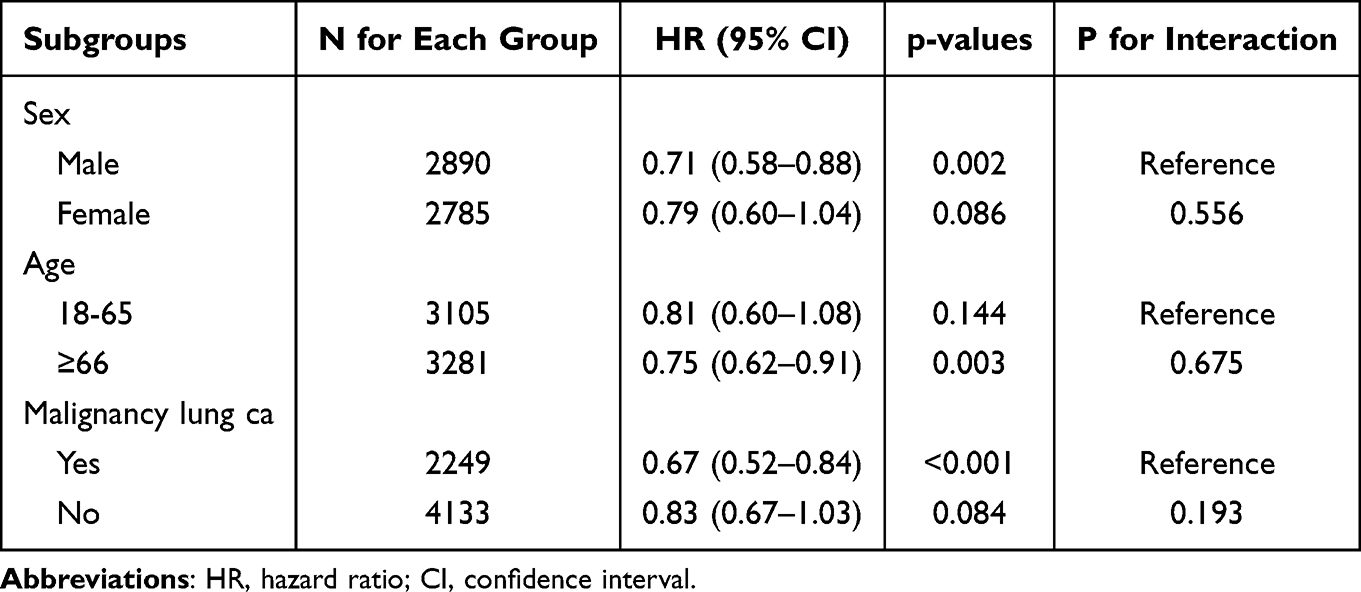 |
Table 4 Subgroup Analysis for 1-Year Mortality Risk |
Multivariable Analysis for Risk Factor Identification
The multivariate Cox proportional hazards model identified dexmedetomidine as an independent protective factor for 1-year mortality after adjusting for a wide range of demographic and clinical variables (Table 5). Dexmedetomidine exposure remained significantly associated with a 25% reduction in mortality risk (HR 0.75, 95% CI 0.66–0.85; p<0.001), confirming the robustness of its effect beyond baseline patient characteristics. Several predictors were used to validate the model. Male sex was associated with a higher risk of 1-year mortality (HR, 1.49; p<0.001), and increasing age also conferred a greater risk, with each additional year linked to a 2% increase in mortality (HR, 1.02; p<0.001). Among the comorbidities, malnutrition had the strongest association (HR, 3.13; p<0.001), followed by heart failure (HR, 2.03; p<0.001) and anemia (HR, 1.62; p<0.001), underscoring the importance of nutritional and cardiovascular optimization before surgery. Interestingly, conditions such as chronic obstructive pulmonary disease and ischemic heart disease were not significant predictors, possibly reflecting the homogeneous nature of the VATS population or effective baseline balancing. Overall, these findings further support the independent and consistent benefit of dexmedetomidine on long-term survival.
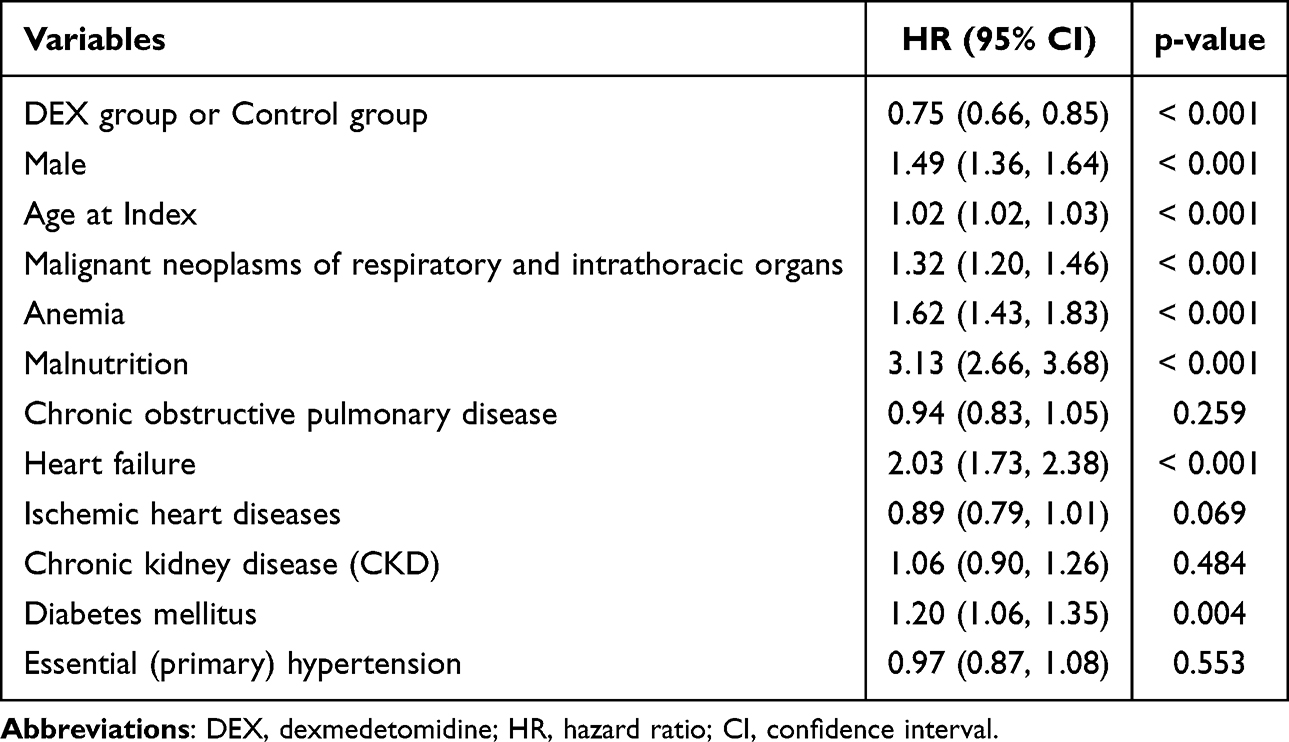 |
Table 5 Variables for 1-Year Mortality Prediction |
Discussion
This multi-institutional study examined 12,774 patients undergoing VATS to compare one-year mortality risk between those receiving perioperative dexmedetomidine versus midazolam. Our results revealed a 20% reduction in one-year mortality risk for patients receiving dexmedetomidine compared to midazolam. Importantly, this survival benefit emerged during the later follow-up period (31–365 days post-surgery) rather than immediately after surgery, suggesting that the protective effects of dexmedetomidine may relate to longer-term physiological recovery rather than prevention of immediate complications. Interestingly, both groups experienced identical rates of major complications (12.7%), indicating that dexmedetomidine’s mortality benefit operates through mechanisms beyond preventing overt clinical events, such as sepsis or respiratory failure. Sensitivity analyses confirmed that these findings remained robust even after excluding patients with blood transfusions or preoperative anemia, and the protective effect was consistent across different patient subgroups regardless of age, sex, or cancer status.
Based on current evidence, dexmedetomidine has demonstrated significant progress in preventing postoperative mortality, although this benefit appears to be most pronounced in specific surgical populations. Ji et al27 demonstrated that perioperative dexmedetomidine reduced in-hospital, 30-day, and 1-year mortality in patients undergoing coronary artery bypass surgery. Similarly, Cheng et al28 found significantly decreased in-hospital mortality and operative mortality in elderly cardiac surgery patients. These findings were corroborated by Peng et al18 in a comprehensive meta-analysis of cardiac surgery patients, which demonstrated a 65% reduction in the 30-day mortality risk. However, the benefits of noncardiac surgery remain less consistent, as the same meta-analysis by Peng et al18 found that 30-day mortality advantages were not significant in noncardiac surgical populations.
In the current study, the observed reduction in one-year mortality associated with perioperative dexmedetomidine represents a clinically significant finding that extends well beyond the immediate perioperative period. The temporal pattern of this survival benefit is particularly intriguing, as it became evident only during the intermediate to late follow-up period rather than in the first month after surgery. This delayed emergence of benefits suggests that the protective effects of dexmedetomidine may not be primarily related to preventing immediate surgical complications but rather to enhancing the body’s capacity for long-term recovery and adaptation following the physiological stress of thoracic surgery. In addition, these findings were supported by sensitivity and subgroup analyses. However, because perioperative blood transfusion is both an indicator of surgical complexity and an independent predictor of adverse outcomes,29,30 it may confound the association between dexmedetomidine use and mortality. As excluding transfused patients may preferentially remove those with greater baseline risk or intraoperative instability, this result should be interpreted with caution.
This study revealed a notable paradox: despite comparable 30-day complication and mortality rates between groups, a significant divergence in survival emerged between 31 and 365 days postoperatively. This temporal dissociation suggests that the survival benefit of dexmedetomidine is unlikely to result from reduced perioperative complications but rather from enhanced postoperative physiological resilience. Although unmeasured confounders such as surgeon skill, institutional volume, intraoperative blood loss, or adherence to enhanced recovery protocols were not available in the database, these factors primarily influence short-term risk of complications or morbidity. The consistent 30-day complication rates between groups therefore suggest that such variables were likely balanced and are unlikely to explain the delayed divergence in long-term mortality.
As a highly selective alpha-2 adrenergic receptor agonist, dexmedetomidine exerts potent sympatholytic effects that may attenuate the excessive stress response associated with major surgery, thereby reducing the cascade of inflammatory mediators and stress hormones that can contribute to organ dysfunction and adverse outcomes.14–16 The well-documented anti-inflammatory properties of the drug may play a particularly important role in thoracic surgery patients, where inflammatory responses can significantly impact respiratory function and wound healing. Additionally, the potential neuroprotective and cardioprotective effects of dexmedetomidine, mediated through preconditioning mechanisms and preservation of cellular energy metabolism, may help maintain vital organ function during periods of physiological stress.15,31 Such modulation of systemic homeostasis may explain the delayed mortality benefit observed in our cohort and highlights the potential for pharmacologic interventions to influence long-term surgical outcomes beyond the prevention of discrete adverse events.
From a clinical perspective, the potential survival benefit associated with dexmedetomidine use may justify its higher acquisition cost, particularly if future studies confirm long-term improvements in recovery and quality of life. Furthermore, these findings could contribute to the development of evidence-based perioperative management guidelines incorporating dexmedetomidine as a component of multimodal anesthesia strategies for thoracic surgery. However, the implementation of these findings in clinical practice should be balanced with individual patient factors, contraindications, and institutional protocols. The broad applicability of the survival benefit across different patient subgroups suggests that the protective effects of dexmedetomidine may benefit the general population undergoing thoracic surgery. These results also highlight the importance of considering long-term outcomes, not just immediate perioperative complications, when evaluating the effectiveness of different anesthetic approaches.
The absence of any significant difference in major complications between the dexmedetomidine and control groups indicates that the protective effects of dexmedetomidine do not operate primarily through the prevention of overt clinical events such as sepsis, respiratory failure, myocardial infarction, or acute kidney injury. However, dexmedetomidine may influence the severity or clinical course of complications in ways that do not change their incidence but improve their outcomes. This pattern underscores the complexity of perioperative medicine and highlights how medication can influence patient outcomes through pathways that extend beyond the prevention of easily measurable clinical endpoints. Nevertheless, the absence of difference in the overall complication rate should be interpreted with caution. The composite definition used in this study may not have captured all clinically relevant adverse events, and differences in complication detection or reporting across institutions could have influenced the results. In our initial analysis, individual complications were examined separately; however, no significant differences were observed between patients with or without dexmedetomidine exposure. To avoid excessive reporting of non-significant findings and to present a concise yet clinically meaningful summary, we therefore used an overall composite endpoint of major complications. This approach also reflects the limitation of ICD-10–based data, which capture diagnostic categories but not the severity of each event.
Given the relatively high proportion of patients with malignancy in our cohort, the findings should be interpreted within the context of a predominantly oncologic VATS population, and caution is warranted when generalizing to non-cancer surgical settings. In clinical practice, dexmedetomidine is commonly administered as an initial bolus followed by continuous intraoperative infusion to maintain hemodynamic stability and sedation. Although our database did not capture the specific administration details, this limitation is unlikely to substantially affect the interpretation of our findings, as the typical perioperative use pattern is relatively standardized. However, because detailed information on the specific dosing regimen, timing (eg, pre-induction, intraoperative, or postoperative), infusion duration of dexmedetomidine, or concomitant anesthetics was unavailable, we were unable to assess potential dose–response relationships or identify threshold effects that might influence efficacy or adverse events. These factors may influence its physiological and clinical effects; therefore, our results should be interpreted as reflecting general perioperative exposure rather than a specific administration protocol.
Several important limitations of this study must be acknowledged when interpreting these findings. First, the retrospective observational design cannot establish causality and may be subject to unmeasured confounding factors (such as physician preference, surgical complexity, intraoperative events, hemodynamic stability, expected surgery duration, or severity of comorbidities) that could influence both treatment selection and outcomes. Second, our composite endpoint of major complications did not include granular subclassifications, and variations in postoperative follow-up completeness among institutions could have introduced minor ascertainment bias. These factors may partly account for the residual uncertainty in interpreting the magnitude and mechanisms of the observed survival benefit. Third, the study population was limited to patients who received either dexmedetomidine or midazolam, potentially excluding those who received other sedative agents, which limits our ability to draw broader conclusions regarding optimal perioperative management. Fourth, the inherent limitations of the TriNetX database, including potential variability in diagnostic coding accuracy, missing data, and the lack of granular clinical details such as medication dosing or surgical complexity, may affect the internal validity of our findings. In addition, the TriNetX database does not capture the specific causes of mortality, precluding differentiation between disease-related and non–disease-related deaths. Finally, while our follow-up period of one year provides valuable long-term data, even longer follow-up periods might reveal different patterns of benefit or delayed adverse effects not apparent in our analysis timeframe.
Conclusion
This multi-institutional study demonstrates that perioperative dexmedetomidine administration is associated with a reduction in one-year mortality following VATS. This survival benefit appears to emerge through mechanisms that extend beyond the prevention of immediate postoperative complications, suggesting that dexmedetomidine may enhance physiological resilience and recovery capacity during the critical postoperative period. However, given the absence of detailed information on drug dosing, timing, and protocol adherence, the present study should be viewed as hypothesis-generating rather than practice-guiding. Future randomized controlled trials are required to validate these observations and define optimal perioperative use parameters.
Data Sharing Statement
The data that support the findings of this study are available from the TriNetX Research Network, but restrictions apply to the availability of these data, which were used under a collaboration agreement for the current study and so are not publicly available. Data are however available from the author (Kuo-Chuan Hung) upon reasonable request and with permission of TriNetX. Access to the de-identified data requires either TriNetX network mem-bership or establishment of a collaborative agreement with TriNetX.
Ethics Approval Statement
The study protocol was approved by the Institutional Review Board of Chi Mei Medical Center, which granted a waiver of informed consent in compliance with observational research regulations (IRB number: 11406-E02).
Patient Consent Statement
Informed consent was not required for this retrospective study, as it involved secondary analysis of pre-existing data without any interventions or direct participant interaction.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Ikeda N. Updates on minimally invasive surgery in non-small cell lung cancer. Curr Treat Options Oncol. 2019;20:16. doi:10.1007/s11864-019-0614-9
2. Jiang Y, Su Z, Liang H, Liu J, Liang W, He J. Video-assisted thoracoscopy for lung cancer: who is the future of thoracic surgery? J Thorac Dis. 2020;12:4427–4433. doi:10.21037/jtd-20-1116
3. Jindal R, Nar AS, Mishra A, Singh RP, Aggarwal A, Bansal N. Video-assisted thoracoscopic surgery versus open thoracotomy in the management of empyema: a comparative study. J Minim Access Surg. 2021;17:470–478. doi:10.4103/jmas.JMAS_249_19
4. Wang Z, Pang L, Tang J, et al. Video-assisted thoracoscopic surgery versus muscle-sparing thoracotomy for non-small cell lung cancer: a systematic review and meta-analysis. BMC Surg. 2019;19:144. doi:10.1186/s12893-019-0618-1
5. Lodhia JV, Konstantinidis K, Papagiannopoulos K. Video-assisted thoracoscopic surgery in trauma: pros and cons. J Thorac Dis. 2019;11:1662–1667. doi:10.21037/jtd.2019.03.55
6. Lin CW, Huang KY, Lin CH, et al. Video-assisted thoracoscopic surgery in community-acquired thoracic empyema: analysis of risk factors for mortality. Surg Infect. 2022;23:191–198. doi:10.1089/sur.2021.191
7. Brunelli A, Dinesh P, Woodcock-Shaw J, Littlechild D, Pompili C. Ninety-day mortality after video-assisted thoracoscopic lobectomy: incidence and risk factors. Ann Thorac Surg. 2017;104:1020–1026. doi:10.1016/j.athoracsur.2017.02.083
8. McKenna RJ, Benditt JO, DeCamp M, et al. Safety and efficacy of median sternotomy versus video-assisted thoracic surgery for lung volume reduction surgery. J Thorac Cardiovasc Surg. 2004;127:1350–1360.
9. Boavista Barros Heil L, Leme Silva P, Ferreira Cruz F, Pelosi P, Rieken Macedo Rocco P. Immunomodulatory effects of anesthetic agents in perioperative medicine. Minerva Anestesiol. 2020;86:181–195. doi:10.23736/S0375-9393.19.13627-9
10. Konstantis G, Katsadouros I, Tsaousi G, Grosomanidis V, Pourzitaki C. Immunomodulatory effects of anesthetic techniques in lung cancer surgery: a systematic review and meta-analysis. Medicina. 2025;61:1263. doi:10.3390/medicina61071263
11. Ivascu R, Torsin LI, Hostiuc L, Nitipir C, Corneci D, Dutu M. The surgical stress response and anesthesia: a narrative review. J Clin Med. 2024;13:3017. doi:10.3390/jcm13103017
12. Santander Ballestín S, Lanuza Bardaji A, Marco Continente C, Luesma Bartolomé MJ. Antitumor anesthetic strategy in the perioperatory period of the oncological patient: a review. Front Med. 2022;9:799355. doi:10.3389/fmed.2022.799355
13. Gerlach AT, Dasta JF. Dexmedetomidine: an updated review. Ann Pharmacother. 2007;41:245–252. doi:10.1345/aph.1H314
14. Liu X, Li Y, Kang L, Wang Q. Recent advances in the clinical value and potential of dexmedetomidine. J Inflamm Res. 2021;14:7507–7527. doi:10.2147/JIR.S346089
15. Bao N, Tang B. Organ-protective effects and the underlying mechanism of dexmedetomidine. Mediators Inflamm. 2020;2020:6136105. doi:10.1155/2020/6136105
16. Wang K, Wu M, Xu J, et al. Effects of dexmedetomidine on perioperative stress, inflammation, and immune function: systematic review and meta-analysis. Br J Anaesth. 2019;123:777–794. doi:10.1016/j.bja.2019.07.027
17. Verret M, Le JBP, Lalu MM, et al. Effectiveness of dexmedetomidine on patient-centred outcomes in surgical patients: a systematic review and Bayesian meta-analysis. Br J Anaesth. 2024;133:615–627. doi:10.1016/j.bja.2024.06.007
18. Peng K, Ji FH, Liu HY, Zhang J, Chen QC, Jiang YH. Effects of perioperative dexmedetomidine on postoperative mortality and morbidity: a systematic review and meta-analysis. Clin Ther. 2019;41:138–54.e4. doi:10.1016/j.clinthera.2018.10.022
19. Peng K, Shen YP, Ying YY, et al. Perioperative dexmedetomidine and 5-year survival in patients undergoing cardiac surgery. Br J Anaesth. 2021;127:215–223. doi:10.1016/j.bja.2021.03.040
20. Zorrilla-Vaca A, Grant MC, Law M, Messinger CJ, Pelosi P, Varelmann D. Dexmedetomidine improves pulmonary outcomes in thoracic surgery under one-lung ventilation: a meta-analysis. J Clin Anesth. 2024;93:111345. doi:10.1016/j.jclinane.2023.111345
21. Song C, Lu Q. Effect of dexmedetomidine supplementation for thoracoscopic surgery: a meta-analysis of randomized controlled trials. J Cardiothorac Surg. 2022;17:70. doi:10.1186/s13019-022-01803-z
22. Chen IW, Chang LC, Ho CN, et al. Association between COVID-19 and the development of chronic kidney disease in patients without initial acute kidney injury. Sci Rep. 2025;15:10924. doi:10.1038/s41598-025-96032-4
23. Hung KC, Chang LC, Chang YJ, et al. Vitamin D deficiency and diabetic retinopathy risk in patients with newly diagnosed type 2 diabetes mellitus: a retrospective analysis. Front Nutr. 2025;12:1614287. doi:10.3389/fnut.2025.1614287
24. Chen IW, Chang LC, Wu JY, et al. Impact of SGLT2 inhibitors use on risk of postoperative acute kidney injury following metabolic and bariatric surgery: a retrospective study. Obes Surg. 2025;35:3599–3607. doi:10.1007/s11695-025-08002-4
25. Lai YC, Yu TS, Hung KC, et al. Zinc deficiency as a contributor to acute kidney injury in patients with chronic kidney disease: a propensity score-matched retrospective analysis. Front Nutr. 2025;12:1658308. doi:10.3389/fnut.2025.1658308
26. VanderWeele TJ, Ding P. Sensitivity analysis in observational research: introducing the E-value. Ann Intern Med. 2017;167:268–274. doi:10.7326/M16-2607
27. Ji F, Li Z, Nguyen H, et al. Perioperative dexmedetomidine improves outcomes of cardiac surgery. Circulation. 2013;127:1576–1584. doi:10.1161/CIRCULATIONAHA.112.000936
28. Cheng H, Li Z, Young N, et al. The effect of dexmedetomidine on outcomes of cardiac surgery in elderly patients. J Cardiothorac Vasc Anesth. 2016;30:1502–1508. doi:10.1053/j.jvca.2016.02.026
29. Lu Q, Zhang J, Gao WM, Lv Y, Zhang XF, Liu XM. Intraoperative blood transfusion and postoperative morbidity following liver resection. Med Sci Monit. 2018;24:8469–8480. doi:10.12659/MSM.910978
30. Inoue Y, Ishii M, Fujii K, et al. The effects of allogeneic blood transfusion in hepatic resection. Am Surg. 2021;87:228–234. doi:10.1177/0003134820950285
31. Unchiti K, Leurcharusmee P, Samerchua A, Pipanmekaporn T, Chattipakorn N, Chattipakorn SC. The potential role of dexmedetomidine on neuroprotection and its possible mechanisms: evidence from in vitro and in vivo studies. Eur J Neurosci. 2021;54:7006–7047. doi:10.1111/ejn.15474
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.